Embed Size (px)
Citation preview

m
w
i
c
i
m
c
t
p
t
e
c
n
Ttceasbt
amtmwsddfi
e(alis
rt
S
PP
J
Esmolol Reduces Perioperative Ischemia in Cardiac Surgery:A Meta-analysis of Randomized Controlled Studies
Alberto Zangrillo, MD, Stefano Turi, MD, Giuseppe Crescenzi, MD, Alessandro Oriani, MD,
Francesco Distaso, MD, Fabrizio Monaco, MD, Elena Bignami, MD, and Giovanni Landoni, MDc
r
t
r
a
2
n
t
[
s
5
v
i
b
©
K
Objective: �-Blockers were associated with a reduction of
ortality and morbidity in noncardiac surgery until recently
hen the POISE trial showed that �-blockers could be harmful
n the perioperative period because of hypotension and brady-
ardia. Esmolol is an ultra–short-acting �-blocker mostly used
n emergency and high-risk patients. The authors performed a
eta-analysis to evaluate the clinical effects of esmolol in
ardiac surgery.
Design: Meta-analysis.
Setting: Hospitals.
Participants: A total of 778 patients from 20 randomized
rials.
Interventions: None.
Measurements and Main Result: Three investigators inde-
endently searched BioMedCentral and PubMed. Inclusion cri-
eria were random allocation to treatment and comparison of
smolol versus other drugs, placebo, or standard of care in
ardiac surgery. Exclusion criteria were duplicate publications,
ubMed search strategy was designed to be highly comprehensive and
shfeAdivlw
S
iwnwmaalwcad
D
s
V
AO
ournal of Cardiothoracic and Vascular Anesthesia, Vol 23, No 5 (October)
omes. The use of esmolol was associated with a significant
eduction of myocardial ischemia episodes (15/122 [12.2%] in
he esmolol group v 36/140 [25.7%] in the control arm, odds
atio [OR] �0.42 [0.23-0.79], p � 0.007) and development of
rrhythmias after cardiopulmonary bypass (15/65 [23.07%] v
3/64 [35.9%], OR � 0.42 [0.18-1.01], p � 0.05). The authors did
ot find a reduction in the use of inotropic drugs in esmolol-
reated patients (29/153 [18.9%] v 48/146 [32.8%], OR � 0.43
0.16-1.10], p � 0.08). Esmolol-treated patients had more epi-
odes of bradycardia (19/129 [14.72%] v 3/133 [2.25%], OR �.49 [2.21-13.62], p � 0.0002) and hypotension (28/113 [24.77%]
14/119 [11.76%], OR � 2.73 [0.83-9.04], p � 0.10).
Conclusions: Esmolol reduces the incidence of myocardial
schemia and arrhythmias in cardiac surgery. An increase in
radycardia was noted as well.
2009 Elsevier Inc. All rights reserved.
EY WORDS: esmolol, cardiac surgery, cardiac anesthesia,
onhuman experimental studies, and no data on clinical out- �-blocker, cardiac protection, anesthesia
HE USE AND THE IMPORTANCE OF �-blockers in theperioperative period are widely accepted in high-risk pa-
ients undergoing noncardiac surgery,1 a context in which theyould reduce morbidity and mortality.2,3 In cardiac surgery, thefficacy of �-blockers is limited to the prevention of postoper-tive atrial fibrillation in coronary artery bypass graft (CABG)urgery,4 and only one observational analysis suggested a smallut consistent survival benefit for patients receiving �-blockerherapy and undergoing CABG surgery.5
Esmolol is an ultra–short-acting �-blocker; its half-life ispproximately 2 minutes, its time to peak effect is about 6 to 10inutes after administration, and its washout time is considered
o be 9 minutes after stopping infusion.6 All these propertiesake this �-blocker the first-choice drug in critical patients inhom possible side effects such as cardiac failure, hypoten-
ion, or bradycardia make a rapid and immediate interruption ofrug administration necessary. Usually it is used as a loadingose followed by a continuous infusion.7 These clinically use-ul pharmacologic characteristics have led to the use of esmololn the prevention of a sympathetic response in cardiac surgery.
Numerous underpowered studies suggested that esmolol prop-rties are useful to treat arrhythmias after cardiopulmonary bypassCPB), as an alternative or additive to traditional cardioplegicgents, or to reduce the hemodynamic responses associated witharyngoscopy, intubation, and extubation.8-37 However, clinical stud-es showing the efficacy of esmolol in patients undergoing cardiacurgery have been sparse and limited by small sample sizes.
To address this problem, the authors conducted a systematiceview and meta-analysis of all the existing trials to determinehe impact of esmolol on patients undergoing cardiac surgery.
METHODS
earch Strategy
Pertinent studies were independently searched in BioMedCentral andubMed (updated April 13, 2008) by 3 trained investigators. The
ensitive, including as key words “esmolol AND surgery.” Furtherand or computerized searches involved the recent (2006-2007) con-erence proceedings from the International Anesthesia Research Soci-ty, American Heart Association, American College of Cardiology,merican Society of Anesthesiologists, and European Society of Car-iology congresses. In addition, the authors used backward snowball-ng (ie, scanning of reference of retrieved articles and pertinent re-iews) and contacted international experts for further studies. Noanguage restriction was enforced and non–English-language articlesere translated before further analysis.
tudy Selection
References obtained from database and literature searches were firstndependently examined at the title/abstract level by 3 investigators,ith divergences resolved by consensus and then, if potentially perti-ent, retrieved as complete articles. The following inclusion criteriaere used for potentially relevant studies: random allocation to treat-ent, comparison of an esmolol versus a control treatment or placebo,
nd performed on cardiac surgical patients with no restriction in dosend time of administration. The exclusion criteria were duplicate pub-ications (in this case, only the article reporting the longest follow-upas abstracted), nonhuman experimental studies, and studies with no
linical outcome. Two investigators independently assessed compli-nce to selection criteria and selected studies for the final analysis, withivergences finally resolved by consensus.
ata Abstraction and Study Characteristics
Baseline, procedural, and outcome data were independently ab-tracted by 3 trained investigators with divergences resolved by con-
From the Department of Anesthesia and Intensive Care, Universitàita-Salute San Raffaele, Milan, Italy.Address reprint request to Giovanni Landoni, MD, Department of
nesthesia and Intensive Care, Istituto Scientifico San Raffaele, vialgettina 60, Milano 20132, Italy. E-mail: [email protected]© 2009 Elsevier Inc. All rights reserved.1053-0770/09/2305-0007$36.00/0
doi:10.1053/j.jvca.2009.01.003625, 2009: pp 625-632

setd
aa
p
3
626 ZANGRILLO ET AL
ensus (Tables 1 and 2). Specifically, the authors extracted studyndpoints and main outcomes, study design (including patient selec-ion, randomization, single-/multicenter design, and open or single-/ouble-blind design), clinical setting, population, additional treatments,
Table 1. Randomized Controlled Studies Included in the Met
Drug Ad
Authors Journal YearPatients
(Esmolol)
Boldt J Anesth Analg 2004 21
Scorsin M J Thorac Cardiovasc Surg 2003 23Deng YK Circ J 2002 12Balcetyte-Harris N Ann Noninvasive Electrocardiol 2002 27Kurian SM Anaesthesia 2001 34Rinne T Acta Anaesthesiol Scand 2000 20Mooss AN Am Heart J 2000 15
Mehlhorn U Eur J Cardiothorac Surg 2000 10Chauhan S Indian J Med Res 1999 30Tempe D Indian Heart J 1999 15Mehlhorn U Cardiovasc Surg 1999 30Kuhn-Regnier F Eur J Cardiothorac Surg 1999 30Cork CR Anesth Analg 1995 15Cork CR Anesth Analg 1995 16
Neustein SM J Cardiothorac Vasc Anesth 1994 17Reves JG J Thorac Cardiovasc Surg 1990 16Harrison L Anesthesiology 1987 15De Brujin Anesth Analg 1987 19Girare D Anesthesiology 1986 11Newsome LR Anesth Analg 1986 10
TOTAL 386
Table 2. Details on the Type of Surgery and the
Author Groups Surgery
Boldt J 2 CABG Esmolol anScorsin M 2 Aortic stenosis Esmolol inDeng YK 2 Mitral valve replacement Esmolol
Balcetyte-Harris N 2 CABG EsmololKurian SM 2 CABG EsmololRinne T 2 CABG Esmolol adMooss AN 2 CABG/Valve Replacement EsmololMehlhorn U 2 CABG Esmolol adChauhan S 2 Off-pump CABG EsmololTempe D 2 CABG EsmololMehlhorn U 2 CABG Esmolol ad
cardiopleKuhn-Regnier F 2 CABG Normother
as myocCork RC 2 CABG EsmololCork RC 2 CABG/Valve replacement EsmololNeustein SM 2 CABG EsmololReves JG 2 CABG EsmololHarrison L 2 CABG EsmololDe Brujin NP 2 CABG EsmololGirare D 2 CABG EsmololNewsome LR 3 CABG Esmolol
nd adverse events. At least 2 separate attempts at contacting originaluthors were made in the case of missing data.
The primary endpoint of the present review was the rate oferioperative ischemia as per author definition, whereas the copri-
lysis With the Number of Patients and Timing of the Study
tration
ientstrols) Administration
21 After anesthesia induction until the morning of the firstpostoperative day
18 After aortic cross-clamping12 Before CPB23 6-18 hours after surgery for up to 24 hours38 Intensive care unit until 3 hours after extubation20 During cardioplegia15 After diagnosis of atrial fibrillation in the postoperative
period10 During cardioplegia30 During cardioplegia15 30-45 minutes after CPB30 During cardioplegia30 During cardioplegia14 During CPB, up to 10 min after release of aortic cross-clamp14 Just before CPB, up to 10 min after release of aortic cross-
clamp23 Before entering into the operating room14 Before induction of anesthesia15 Before induction of anesthesia21 Before induction of anesthesia
9 Before induction of anesthesia20 Before induction up to 5 min after sternotomy
92
cteristics of the Treatment and Control Groups
reatment Group Control Group
ximone Placeboas cardioplegia Potassium in blood as cardioplegia
Normothermia cardiopulmonarybypass
Oral �-blockersPlacebo
to blood cardioplegia Blood cardiolplegiaDiltiazem
to warm blood cardioplegia Buckberg cardioplegiaDiltiazemPlacebo
to normothermic blood Bretschneider cardioplegia
lood enriched with esmololprotection
Buckberg cardioplegia
PlaceboPlaceboPlaceboPlaceboPlaceboPlaceboPlaceboPlacebo
a-ana
minis
Pat(Con
Chara
T
d enoblood
dition
dition
ditiongia
mic bardial
Usual antihypertensive medication

mipoepd
I
pib
D
ativoefmostpmms
ojpfb
si
evaM
ytasdltdefi
S
eMs2Cabct
to
627ESMOLOL AND CARDIAC SURGERY
ary endpoints were perioperative use of inotropic drugs and thencidence of arrhythmias after CPB. Other relevant secondary end-oints were perioperative incidence of myocardial infarction, lengthf hospital stay and intensive care unit stay, mortality, cardiacvents (at the longest follow-up available for each study), and theresence of possible side effects such as hypotension and bra-ycardia.
nternal Validity and Risk of Bias Assessment
The internal validity and risk of bias of included trials were ap-raised according to The Cochrane Collaboration methods38 by 2ndependent reviewers (G.L. and G.B.-Z.), with divergences resolvedy consensus.
ata Analysis and Synthesis
Computations were performed with SPSS 11.0 (SPSS, Chicago, IL)nd RevMan 4.2 (a freeware available from The Cochrane Collabora-ion).38 Statistical heterogeneity and inconsistency were measured us-ng, respectively, Cochran Q tests and I2. Binary outcomes from indi-idual studies were analyzed in order to compute individual and pooleddds ratios (ORs), with pertinent 95% confidence intervals (CIs, withquivalence set at 1, OR �1 favoring the first treatment, and OR �1avoring the second treatment), by means of the Peto fixed-effectethod in case of low statistical inconsistency (I2 �25%) and by means
f a random-effect method (which better accommodates clinical andtatistical variations) in case of moderate or high statistical inconsis-ency (I2 �5%). Weighted mean differences and 95% CI were com-uted for continuous variables, again by means of a fixed-effectethod in case of low statistical inconsistency (I2 �25%) and byeans of a random-effect method in case of moderate or high
tatistical inconsistency (I2 �25%).39
The risk of small study bias (including publication bias; ie, the riskf small nonsignificant studies being selectively rejected by medicalournals) was assessed by visual inspection of funnel plots and com-uting the Egger test. The authors assessed the robustness of findingsrom the primary analysis to the effects of study population andaseline risk for any of the primary outcomes through a series of
Table 3.
Authors Esmolol Dosage
Boldt J 0.5-mg/kg bolus, 2.5 �g/kg/min ciScorsin M 250-300 mg infused in 2-3 minutesDeng YK 1-mg/kg bolus, ci to have heart rate betweeBalcetyte-Harris N 0.5 mg/kg bolus, 0.05 �g/kg/min ciKurian SM 500-�g/kg bolus, ci to have hr between 55-6Rinne T 15 mg/min in cardioplegic solutionsMooss AN 500-�g/kg bolus, 25-50 �g/kg/min ciMehlhorn U 100-mg bolus, 15 mg/min ciChauhan S 500-�g/kg bolus, 100 �g/kg/h ciTempe D 500-�g/kg bolus, 100 �g/kg/min ciMehlhorn U 100-mg bolus, 15 mg/min ciKuhn-Regnier F 100-mg bolus, 15 mg/min ciCork CR 2-mg/kg bolus, 300 �g/kg/min ciCork CR 2-mg/kg bolus, 300 �g/kg/min ciNeustein SM 1-mg/kg bolus, 100 �g/kg/min ciReves JG 80-mg bolus, 12 mg/min ciHarrison L 500 �g/kg/min (4 min), 300 �g/kg/min ciDe Brujin NP 500 �g/kg/min ciGirare D 500 �g/kg/min (2 min), 200 �g/kg/min ciNewsome LR 500 �g/kg/min (2 min), 200 �g/kg/min ci
Abbreviation: ci, continous infusion.
ensitivity analyses, including random-effects model and by withdraw-ng one study at a time.
Statistical significance was set at the 2-tailed 0.05 level for hypoth-sis testing and at 0.10 for heterogeneity testing, and unadjusted palues are reported throughout. This study was performed in compli-nce with The Cochrane Collaboration and the Quality of Reporting ofeta-Analyses guidelines.39,40
RESULTS
Database searches, snowballing, and contacts with expertsielded a total of 336 citations. Excluding 306 nonpertinentitles or abstracts, 30 studies were retrieved in complete formnd assessed according to the selection criteria. A total of 10tudies were further excluded because of their nonexperimentalesign and the use of historic controls13,25 and duplicate pub-ication21,22; 2 were excluded because they were crossoverrials35,37; and 4 studies because they did not have significantata for the major outcomes.19,28,29,34 The authors identified 20ligible randomized clinical trials, which were included in thenal analysis8-12,14-18,20,23,24,26,27,30-33,36 (Table 1).
tudy Characteristics
The 20 included trials randomized 778 patients (386 tosmolol and 392 receiving a control drug or placebo) (Table 1).ost studies were performed on patients undergoing CABG
urgery, 4 on valvular or combined procedures8,10,11,14 (Table). Esmolol was administered at anesthesia induction, beforePB, in the cardioplegia solution or as a cardioplegic agent, ort extubation as shown in Table 1. Esmolol was administeredy a single-dose bolus (usually 500 �g/kg) followed by aontinuous infusion (between 100 and 300 �g/kg/min or ti-rated in order to maintain low heart rates) (Table 3).
All the studies had a single-center design and studied popula-ions that were too small to allow for significant results in clinicalutcome variables. All studies were published as full articles.
Dosage
Control Drug Dosage
PlaceboPotassium, 0.2 g/mL, at a total dose of 1.2 g
nd 50 beats/min PlaceboOral �-blockers (metoprolol 50 mg/d)PlaceboPlaceboDiltiazem, 0.25 mg/kg then 5 mg/hPlaceboDiltiazem, 0.15 mg/kg then 5 mg/hPlaceboPlaceboPlaceboPlaceboPlaceboPlaceboPlaceboPlaceboPlaceboPlaceboPlacebo
Drug
n 30 a
0 bpm
boaclf
Q
pom[
I(fF
rp14r00(e
s
628 ZANGRILLO ET AL
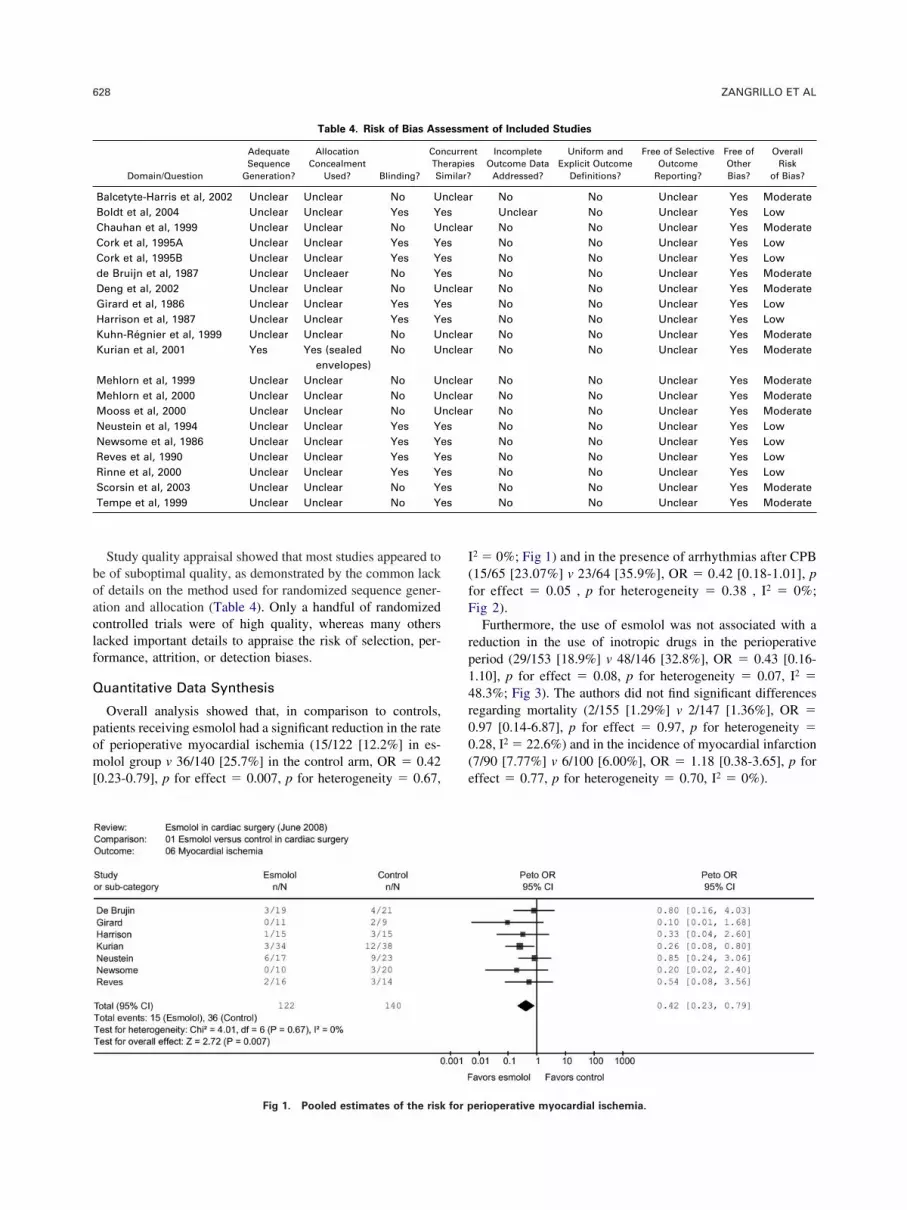
Study quality appraisal showed that most studies appeared toe of suboptimal quality, as demonstrated by the common lackf details on the method used for randomized sequence gener-tion and allocation (Table 4). Only a handful of randomizedontrolled trials were of high quality, whereas many othersacked important details to appraise the risk of selection, per-ormance, attrition, or detection biases.
uantitative Data Synthesis
Overall analysis showed that, in comparison to controls,atients receiving esmolol had a significant reduction in the ratef perioperative myocardial ischemia (15/122 [12.2%] in es-olol group v 36/140 [25.7%] in the control arm, OR � 0.42
0.23-0.79], p for effect � 0.007, p for heterogeneity � 0.67,
Table 4. Risk of Bias Ass
Domain/Question
AdequateSequence
Generation?
AllocationConcealment
Used? Blinding?
ConThS
Balcetyte-Harris et al, 2002 Unclear Unclear No UBoldt et al, 2004 Unclear Unclear Yes YeChauhan et al, 1999 Unclear Unclear No UCork et al, 1995A Unclear Unclear Yes YeCork et al, 1995B Unclear Unclear Yes Yede Bruijn et al, 1987 Unclear Uncleaer No YeDeng et al, 2002 Unclear Unclear No UGirard et al, 1986 Unclear Unclear Yes YeHarrison et al, 1987 Unclear Unclear Yes YeKuhn-Régnier et al, 1999 Unclear Unclear No UKurian et al, 2001 Yes Yes (sealed
envelopes)No U
Mehlorn et al, 1999 Unclear Unclear No UMehlorn et al, 2000 Unclear Unclear No UMooss et al, 2000 Unclear Unclear No UNeustein et al, 1994 Unclear Unclear Yes YeNewsome et al, 1986 Unclear Unclear Yes YeReves et al, 1990 Unclear Unclear Yes YeRinne et al, 2000 Unclear Unclear Yes YeScorsin et al, 2003 Unclear Unclear No YeTempe et al, 1999 Unclear Unclear No Ye
Fig 1. Pooled estimates of the risk for p
2 � 0%; Fig 1) and in the presence of arrhythmias after CPB15/65 [23.07%] v 23/64 [35.9%], OR � 0.42 [0.18-1.01], por effect � 0.05 , p for heterogeneity � 0.38 , I2 � 0%;ig 2).Furthermore, the use of esmolol was not associated with a
eduction in the use of inotropic drugs in the perioperativeeriod (29/153 [18.9%] v 48/146 [32.8%], OR � 0.43 [0.16-.10], p for effect � 0.08, p for heterogeneity � 0.07, I2 �8.3%; Fig 3). The authors did not find significant differencesegarding mortality (2/155 [1.29%] v 2/147 [1.36%], OR �.97 [0.14-6.87], p for effect � 0.97, p for heterogeneity �.28, I2 � 22.6%) and in the incidence of myocardial infarction7/90 [7.77%] v 6/100 [6.00%], OR � 1.18 [0.38-3.65], p forffect � 0.77, p for heterogeneity � 0.70, I2 � 0%).
ent of Included Studies
nts
IncompleteOutcome Data
Addressed?
Uniform andExplicit Outcome
Definitions?
Free of SelectiveOutcome
Reporting?
Free ofOtherBias?
OverallRisk
of Bias?
No No Unclear Yes ModerateUnclear No Unclear Yes LowNo No Unclear Yes ModerateNo No Unclear Yes LowNo No Unclear Yes LowNo No Unclear Yes ModerateNo No Unclear Yes ModerateNo No Unclear Yes LowNo No Unclear Yes LowNo No Unclear Yes ModerateNo No Unclear Yes Moderate
No No Unclear Yes ModerateNo No Unclear Yes ModerateNo No Unclear Yes ModerateNo No Unclear Yes LowNo No Unclear Yes LowNo No Unclear Yes LowNo No Unclear Yes LowNo No Unclear Yes ModerateNo No Unclear Yes Moderate
essm
curreerapieimilar?
nclears
nclearsss
nclearss
nclearnclear
nclearnclearnclearsssss
erioperative myocardial ischemia.

r[eb[Ivhfeh5pm
A
a1rrd
baafimssr
pneCbdpt
a3f
incid
629ESMOLOL AND CARDIAC SURGERY
The authors searched for the presence of possible side effectselated to the use of a �-blocker such as hypotension (28/11324.77%] v 14/119 [11.76%], OR � 2.73 [0.83-9.04], p forffect � 0.10, p for heterogeneity � 0.13, I2 � 43.3%; Fig 4)radycardia (19/129 [14.72%] v 3/133 [2.25%], OR � 5.492.21-13.62], p for effect � 0.0002, p for heterogeneity � 0.48,2 � 0%; Fig 5) and low output cardiac syndrome (8/77 [10.38%]8/73 [10.95%], OR � 0.99 [0.34-2.89], p for effect � 0.98, p foreterogeneity � 0.59, I2 � 0%). No significant differences wereound regarding the length of stay in the intensive care unit (p forffect � 0.39, p for heterogeneity � 0.007, I2 � 71.6%) and theospital (p for effect � 0.41, p for heterogeneity � 0.12, I2 �3.0%). All the episodes of bradycardia were reversed with atro-ine or pacing, and the authors reported no association withorbidity or mortality. No author reported data on stroke.
dditional Analyses
The robustness and applicability of the present findings weressessed through a series of sensitivity analyses (ie, excluding
study at a time and switching from a fixed-effect to aandom-effect model). All subanalyses performed excluding 1andomized controlled trial at a time remained in the sameirection and magnitude of statistical significance (if applica-
Fig 2. Pooled estimates of the
Fig 3. Pooled estimates of the use o
le) as in the overall analysis. Similarly, random-effect meta-nalyses confirmed the robustness of the primary analyses. Theuthors also appraised the robustness and validity of the presentndings by exploring the likelihood of small study bias byeans of funnel plot inspection, finding no major evidence of
uch bias. Finally, disagreements between reviewers at studyelection or appraisal were uncommon (�5%) and quicklyesolved during agreement discussions.
DISCUSSION
A meta-analysis of pooled data from several small, under-owered studies was performed and showed that esmolol sig-ificantly decreases the rate of perioperative myocardial isch-mia and the development of arrhythmias at the end of thePB. No differences in reduction in the use of inotropic drugsetween the 2 groups were found. Although significantly un-erpowered, most studies included in this analysis showedositive trends, consistent with the overall positive results ofhe present meta-analysis.
The use of esmolol during cardiac surgery also was associ-ted with bradycardia (19/129 [14.72%] in the esmolol group v/133 [2.25%], OR � 5.49 [2.21-13.62] in the control group, por effect � 0.0002), but all of these episodes, as stated by
ence of arrhythmias after CPB.
f perioperative inotropic drugs.

asgncb
mermdhp
matbao
da
btpcpltcti
spmo
tc
of ep
630 ZANGRILLO ET AL
uthors, were reversible. The incidences of low-output cardiacyndrome and hypotension were not different between the 2roups, suggesting that the concerns connected to a possibleegative inotropic effect after the use of a �-blocker duringardiac surgery are not a real problem if esmolol is used26
ecause it is an ultra–short-acting �-blocker.High catecholamine concentrations are cytotoxic to cardiacyocytes. Killingsworth et al41 showed that plasma cat-
cholamines, an indirect measure of myocardial catecholamines,ise markedly with cardiac arrest to a level that can increaseyocardial oxygen demand, aggravate myocardial ischemia, in-
uce malignant arrhythmias, and be cytotoxic. Animal studiesave suggested that adrenergic-receptor blockade may decreaseostresuscitation myocardial dysfunction and improve survival.41
Patients with coronary artery disease are more susceptible toajor and minor perioperative myocardial injury. Proper man-
gement begins preoperatively, with optimization of the pa-ient’s antianginal drug regimen. �-Blockers, calcium channellocking therapy, and intravenous nitroglycerin, if that is beingdministered, should be continued until the patient comes to theperating room.42 Particular attention to avoidance of myocar-
Fig 4. Pooled estimates
Fig 5. Pooled estimates of e
ial ischemia is necessary during the induction of anesthesiand in the period before CPB.43
The ultra–short-acting �-blocker esmolol is probably theest choice of a �-blocker in the perioperative period of pa-ients undergoing cardiac surgery. In the studies included in theresent meta-analysis, esmolol was used in 3 different clinicalonditions: (1) preventing the hemodynamic response to somerocedures (in particular extubation), (2) treatment and prophy-axis of atrial fibrillation at the end of CPB, and (3) adminis-ration during surgery (in many cases just before and during theardioplegia) in order to reach or improve myocardial protec-ion. Numerous studies showed how an increase of tachycardias strongly connected to episodes of myocardial ischemia.44,45
Kurian et al12 showed that esmolol was associated with aignificant reduction of ST-segment changes when extubatingatients undergoing cardiac surgery procedures. Esmolol wasore efficacious in controlling heart rate when compared with
ther agents such as magnesium19 and diltiazem.24
During the phase of cardiac arrest and aortic cross-clamping,here is an increase in the catecholamine circulating levels thatan be dangerous to cardiac function. Cork et al8,26 suggested
isodes of hypotension.
pisodes of bradycardia.

teoorrmas
trlteacsofr
aodcsfC
00mrsdn
sstwcf1
s
spwm
sm
eCp
e1
bs
ps
bN
c
A
g
bi1
ad
631ESMOLOL AND CARDIAC SURGERY
hat �-blockers can reduce this kind of damage through differ-nt mechanisms such as a reduction in the myocardial metab-lism, a decrease of intracellular lipase activity, and a decreasef fatty acid injury after reperfusion.46 In animal models, �-ad-energic antagonists increase blood flow to ischemic regions,esulting in a better balance between oxygen supply and de-and,47 and they prevent or attenuate the fracture of vulnerable
therosclerotic plaques, thereby reducing coronary thrombo-is.48
Many authors in the present meta-analysis demonstrated thathe infusion of esmolol during CPB was associated with aeduction of the expression of some inflammatory moleculesike ICAM-I, the heat shock protein 70, or nitric oxide syn-hase; lower values of lactate concentrations; and less cellulardema with better lymphatic drainage.10,15-17,49 Recent studiesnd meta-analysis showed how the use of �-blockers in non-ardiac surgical patients was associated with reductions ofhort-term complications and mortality,2 and an improvementf the long-term outcome.50 In cardiac surgery, few data wereound regarding mortality, underscoring the need for largeandomized controlled studies in high-risk populations.
A recent meta-analysis found similar results.3 Wiesbauer etl3 reviewed the evidence regarding the effectiveness of peri-perative �-blockers for improving patient outcomes after car-iac and noncardiac surgery of 69 randomized, controlled trialsomparing perioperative �-blockers with either placebo or thetandard of care; in cardiac surgery, �-blockers reduced therequency of ventricular tachyarrhythmias (OR � 0.28; 95%
I, 0.13-0.57), atrial fibrillation/flutter (OR � 0.37; 95% CI, tREN
ioplegia. J Cardiothorac Vasc Surg 125:1022-1029, 2003
a6
it5
cC
va
ms
�a
vJ
ha
mc
s
.28-0.48), and myocardial ischemia (OR � 0.49; 95% CI,
.17-1.4), whereas the length of hospitalization, mortality, andyocardial infarction were not reduced. Even if the present
esults are similar, this meta-analysis is different because ittudied only esmolol (an ultra–short-acting �-blocker) and up-ated the analysis to April 2008, including 15 articles that wereot included in the Wiesbauer meta-analysis.In a recent large randomized controlled study, the POISE
tudy group51 analyzed 8,351 patients receiving metoprololuccinate in the perioperative period of noncardiac surgery. Inhese patients, the perioperative �-blockade was associatedith a reduction in myocardial infarction but also with in-
reases in mortality and stroke. In cardiac surgery, the authorsound few and nonsignificant data regarding mortality.8-
0,16,17,23,26 No episodes of stroke were reported in the analyzedtudies.
LIMITATIONS
The inclusion of different ways to administer esmolol in thetudies included in this meta-analysis could have weakened theresent study’s conclusions. Few clinically relevant outcomesere reported by the authors of the 20 trials included in theeta-analysis (eg, no author reported perioperative stroke).
CONCLUSIONS
The authors conclude that the use of esmolol in cardiacurgery is associated with reductions in ischemia and arrhyth-ias. More studies with a large cohort of patients are necessary
o support these positive and promising results.
REFE
1. ACC/AHA: 2007 guidelines on perioperative cardiovascularvaluation and care for non cardiac surgery: A report of Americanollege of Cardiology/American Heart Association Task Force onractice guidelines. Anesth Analg 1063:685-712, 2008
2. McGory ML, Maggard MA, Ko CY: A meta-analysis of periop-rative beta-blockade: What is the actual risk reduction? Surgery 138:71-179, 2005
3. Weisbauer F, Schagler O, Domanovits H, et al: Perioperativeeta-blockers for preventing surgery related mortality and morbidity: Aystematic review and meta-analysis. Anesth Analg 104:27-41, 2007
4. Crystal E, Garfinkle MS, Connolly SS, et al: Interventions forreventing postoperative atrial fibrillation in patients undergoing hearturgery. Cochrane Database Syst Rev 18:CD 003611, 2004
5. Ferguson TB Jr, Coombs LP, Peterson ED: Preoperative beta-locker use and mortality and morbidity following CABG surgery inorth America. JAMA 287:2221-2227, 2002
6. Fita G, Gomar C, Rovira I: Esmolol in anaesthesiology: Pharma-ology and indications. Rev Esp Anestesiol Reanim 46:401-414, 1999
7. Ravussin P: Characteristics and clinical use of esmolol. Minervanestesiol 58:77-79, 1992 (suppl 1)
8. Cork R, Kramer TH, Dreischmeier B, et al: The effect of esmololiven during cardiopulmonary bypass. Anesth Analg 80:28-40, 19959. Boldt J, Brosch C, Lehmann A, et al: The prophylactic use of the
eta-blocker esmolol in combination with phosphodiesterase III inhib-tor enoximone in elderly cardiac surgery patients. Anesth Analg 99:009-1017, 200410. Scorsin M, Mebazaa A, Al Attar N, et al: Efficacy of esmolol asmyocardial protective agent during continuous retrograde blood car-
CES
11. Deng YK, Wei F, Li ZL, et al: Esmolol protects the myocardiumnd facilitates intracardiac operation with a beating heart. Circulation6:715-717, 200212. Kurian SM, Evans R, Fernandes NO, et al: The effect of an
nfusion of esmolol on the incidence of myocardial ischaemia duringracheal extubation following coronary artery surgery. Anaesthesia6:1163-1168, 200113. Mehlhorn U, Fattah M, Kuhn-Regnier F, et al: Impact of myo-
ardial protection during coronary bypass surgery on patient outcome.ardiovasc Surg 9:482-486, 200114. Mooss AN, Wurdeman RL, Mohiuddin SY, et al: Esmolol
ersus diltiazem in the treatment of postoperative atrial fibrillation/trial flutter after open heart surgery. Am Heart J 140:176-180, 2000
15. Mehlhorn U, Blochb W, Krahwinkelb A, et al: Activation ofyocardial constitutive nitric oxide synthase during coronary artery
urgery. Eur J Cardiothorac Surg 17:305-311, 200716. Mehlhorn U, Sauer H, Kuhn-Regnier F, et al: Myocardial
-blockade as an alternative to cardioplegic arrest during coronaryrtery surgery. Cardiovasc Surg 7:549-557, 1999
17. Kuhn-Regnier F, Natour E, Dheind S, et al: Beta-blockadeersus Buckberg blood-cardioplegia in coronary bypass operation. EurCardiothorac Surg 15:67-74, 199918. Newsome LR, Roth JV, Hug CC Jr, et al: Esmolol attenuates
ernodynamic responses during fentanyl-pancuronium anesthesia forortocoronary bypass surgery. Anesth Analg 65:451-456, 1986
19. Arar C, Colak A, Alagol A, et al: The use of esmolol andagnesium to prevent haemodynamic responses to extubation after
oronary artery grafting. Eur J Anesthesiol 24:826-831, 200720. Balcetyte-Harris N, Tamis JE, Homel P, et al: Randomized
tudy of early intravenous esmolol versus oral beta-blockers in pre-

vsE
vta
dC
u4
ao
ncC
gf1
it
eh
tp1
un
o1
on
ts5
ai1
h
th
aC
Rr
oQ3
won
bv2
sp
AbTA
cA
ht1
A
gl
p9
cc
ar(
s
632 ZANGRILLO ET AL
enting post-CABG atrial fibrillation in high risk patients identified byignal-averaged ECG: Results of a pilot study. Ann Noninvasivelectrocardiol 7:86-91, 200221. Maniar PB, Balcetyte-Harris N, Tamis JE, et al: Intravenous
ersus oral beta-blockers for prevention of post-CABG atrial fibrilla-ion in high-risk patients identified by signal-averaged ECG: lessons ofpilot study. Cardiac Electrophysiol Rev 7:158-161, 200322. Hilleman DE, Reyes AP, Mooss AN, et al: Esmolol versus
iltiazem in atrial fibrillation following coronary bypass graft surgery.urr Med Res Opin 19:376-382, 200323. Rinne T, Hairmonen A, Kaukinen S: Esmolol cardioplegia in
nstable coronary revascularisation patients. Acta Anesthesiol Scand4:727-732, 200024. Chahuan S, Saxena N, Rao BH, et al: A comparison of esmolol
nd diltiazem for heart rate control during coronary revascularisationn beating heart. Indian J Med Res 110:174-177, 199925. Hekamt K, Clemens RM, Mehlhorn U, et al: Emergency coro-
ary artery surgery after failed PTCA: Myocardial protection withontinuous coronary perfusion of beta-blocker enriched blood. Thoracardiovasc Surg 46:333-338, 199826. Cork RC, Azari DM, McQueen KAK, et al: Effect of esmolol
iven during cardiopulmonary bypass on fractional area of contractionrom transesophageal echocardiography. Anesth Analg 81:219-224,99527. Neustein SM, Bronheim DS, Lasker S, et al: Esmolol and
ntraoperative myocardial ischemia: A double-blind study. J Cardio-horac Vasc Anesth 8:273-277, 1994
28. Boylan JF, O’Leary J, Weisel RD, et al: A comparison ofsmolol, diltiazem, nifedipine and nitroprusside therapy of post-CABGypertension. Can J Anesth 37:s156, 199029. Kling D, Boldt J, Zickmann B, et al: The hemodynamic effect of
reatment with beta-receptor blockers during coronary surgery. A com-arison between acebutolol and esmolol. Anaesthesist 39:264-268,99030. Harrison L, Ralley FE, Wynands E, et al: The role of an
ltra-short adrenergic blocker (esmolol) in patients undergoing coro-ary artery bypass surgery. Anesthesiology 66:413-418, 198731. Girard D, Shulman BJ, Thys DM, et al: The safety and efficacy
f esmolol during myocardial revascularisation. Anesthesiology 65:57-164, 198632. De Brujin NP, Croughwell N, Reves JG: Hemodynamic effects
f esmolol in chronically beta-blocked patients undergoing aortocoro-ary bypass surgery. Anesth Analg 66:137-141, 198733. Tempe DK, Mulchandani P, Tandon SM, et al: Control of
achycardia and hypertension following coronary artery bypass grafturgery: Efficacy and haemodynamic effects of esmolol. Indian Heart J1:294-300, 199934. O’Dwyer JP, Yorukoglu D, Harris MNE: The use of esmolol to
ttenuate the haemodynamic response when extubating patients follow-ng cardiac surgery—A double blind controlled study. Eur Heart J4:701-704, 199335. Gray RJ, Bateman TM, Czer LSC, et al: Use of esmolol in
ypertension after cardiac surgery. Am J Cardiol 56:49F-56F, 1985 r
36. Reves JG, Croughwell ND, Hawkins E, et al: Esmolol forreatment of intraoperative tachycardia and/or hypertension in patientsaving cardiac operations. J Cardiovasc Surg 100:221-227, 199037. Gray RJ, Bateman TM, Czer LSC, et al: Comparison of esmolol
nd nitroprusside for acute post-cardiac surgery hypertension. Am Jardiol 59:887-891, 198738. Higgins JPT, Green S: The Cochrane Handbook for Systematic
eviews of Interventions 4.2.5. Available at: http://www.cochrane.org/esources/handbook/hbook.htm. Accessed October 10, 2005
39. Moher D, Cook DJ, Eastwood S, et al: Improving the qualityf reports of meta-analyses of randomised controlled trials: TheUOROM statement. Quality of reporting of meta-analyses. Lancet54:1896-1900, 199940. Biondi-Zoccai GG, Lotrionte M, Abbate A, et al: Compliance
ith QUOROM and quality of reporting of overlapping metaanalysisn the role of acetylcysteine in the prevention of contrast associatedephropathy: Case study. BMJ 332:202-209, 200641. Killingsworth CR, Wei CC, Dell’Italia LJ, et al: Shorting-acting
eta-adrenergic antagonist esmolol given at reperfusion improves sur-ival after prolonged ventricular fibrillation. Circulation 109:2469-474, 200442. Rosenfeld DM, Trentman TL, Hentz JG, et al: Patients under-
tanding of the importance of the beta-blocker use in the perioperativeeriod. J Cardiothorac Vasc Anesth 21:325-329, 200743. A report of the American College of Cardiology/American Heart
ssociation ACC/AHA guidelines and indications for coronary arteryypass graft surgery. Task Force on Assessment of Diagnostic andherapeutic Cardiovascular Procedures (Subcommittee on Coronaryrtery Bypass Graft Surgery). Circulation 83:1125-1173, 199144. Landoni G, Pappalardo F, Calabrò MG, et al: Myocardial ne-
rosis biomarkers after different cardiac surgical operations. Minervanestesiol 73:49-56, 200745. Beattie WS, Wijeysundera DN, Karkouti K, et al: Does tight
eart rate control improve beta-blocker efficacy? An update analysis ofhe noncardiac surgical randomized trials. Anesth Analg 106:1025-030, 200846. Opie LH: Myocardial infarct size. Part 1. Basic considerations.
m Heart J 100:355-372, 198047. Becker LC, Fortuin NJ, Pitt B: Effect of ischemia and antian-
inal drugs on the distribution of radioactive microspheres in the canineeft ventricle. Circ Res 28:263-269, 1971
48. Frishman WH, Chang CM: Beta-adrenergic blockade in therevention of myocardial infarction: A new theory. J Hypertens Suppl:531-534, 199149. Heringlake M, Bahlmann L, Misfeld M, et al: High myocardial
oncentration is associated with poor myocardial function prior toardiopulmonary bypass. Minerva Anestesiol 71:775-783, 2005
50. Feringa HH, Bax JJ, Boersma E, et al: High dose beta-blockersnd tight heart rate control reduce myocardial ischemia and troponin Telease in vascular surgery patients. Circulation 114:1344-1349, 2006suppl)
51. POISE Study Group: Effects of extended-release metoprololuccinate in patients undergoing noncardiac surgery (POISE trial): A
andomised controlled trial. Lancet 371:1839-1847, 2008




























