Embed Size (px)
Citation preview
Circulation Journal Vol.77, May 2013
Circulation JournalOfficial Journal of the Japanese Circulation Societyhttp://www.j-circ.or.jp
increased risk of cardiovascular events in patients with CAD.2,11 A combination of LGE and myocardial perfusion-MR can provide structural and physiological information12 that helps in the diagnosis of CAD4 and has been applied clinically. On the other hand, cine MRI provides accurate and reproducible measurements of cardiac function and is currently regarded as the reference standard.13 Currently, tagged MR offers a repro-ducible measure of regional myocardial strain that can be used for a detailed analysis of regional ventricular function with high spatial resolution and accuracy.14,15
Adenosine triphosphate (ATP) induces hyperemia in nor-mal coronary arteries and relative hypoperfusion in stenotic coronary arteries. Its effect on myocardial wall motion has been studied,16 but the effect on myocardial strain has not been elucidated quantitatively by tagged MR and has not been used
ardiovascular magnetic resonance (CMR) is a valuable imaging modality that can be used to investigate ven-tricular function, myocardial perfusion, viability, and
coronary artery anatomy during a single examination, without radiation exposure.1–8 Stress myocardial perfusion-magnetic resonance (MR), using a gadolinium-based contrast agent, is a sensitive method for detecting coronary artery disease (CAD) with good specificity. Recently, several studies have tested the accuracy of stress perfusion-MR for the detection of CAD and have shown equal or improved results compared with single-photon emission computed tomography (SPECT).9,10 Late gad-olinium enhancement (LGE) MR imaging (MRI), with its high spatial resolution and high contrast-to-noise ratio, can also de-tect myocardial infarcts with high diagnostic accuracy. How-ever, the presence and extent of LGE is associated with an
C
Received August 24, 2012; revised manuscript received December 3, 2012; accepted January 6, 2013; released online February 6, 2013 Time for primary review: 24 days
Department of Radiology (Tomoyuki K., Teruhito K., A.K., M.M., T.M.), Department of Cardiovascular Internal Medicine (A.O.), Ehime University Graduate School of Medicine, Toon; Department of Molecular Imaging & Diagnosis, Graduate School of Medical Sciences, Kyushu University, Fukuoka (M.N.), Japan
Mailing address: Tomoyuki Kido, MD, Department of Radiology, Ehime University Graduate School of Medicine, Shitsukawa, Toon 791-0295, Japan. E-mail: [email protected]
ISSN-1346-9843 doi: 10.1253/circj.CJ-12-1106All rights are reserved to the Japanese Circulation Society. For permissions, please e-mail: [email protected]
Stress/Rest Circumferential Strain in Non-Ischemia, Ischemia, and Infarction
– Quantification by 3 Tesla Tagged Magnetic Resonance Imaging –Tomoyuki Kido, MD; Michinobu Nagao, MD; Teruhito Kido, MD, PhD; Akira Kurata, MD, PhD;
Masao Miyagawa, MD, PhD; Akiyoshi Ogimoto, MD, PhD; Teruhito Mochizuki, MD, PhD
Background: Adenosine triphosphate (ATP) induces relative hypoperfusion in significantly stenotic coronary arter-ies, but its effect on myocardial strain has not been used clinically for the detection of ischemia. The purpose of this study was to quantify ATP-stress-induced contractile impairment as altered myocardial strain in coronary artery disease (CAD) using tagged magnetic resonance (MR) and to evaluate its diagnostic capability in comparison with ATP-stress myocardial perfusion-MR.
Methods and Results: Tagged MR and perfusion-MR under ATP-stress and rest conditions and late gadolinium enhancement (LGE) MR imaging were performed in 22 patients with suspected CAD. The peak absolute value of the circumferential strain (C-strain) was measured in 12 segments. Myocardial segments were categorized as non-ischemic (n=201), ischemic (n=42), or infarcted (n=21) according to the perfusion-MR and LGE MR imaging results. The absolute C-strain was significantly greater under ATP-stress (19±13%) (mean ± SD) than under at-rest (15±11%, P<0.001) conditions in non-ischemic segments. Conversely, the absolute C-strain was significantly lower under ATP-stress (10±13%) than under at-rest (16±6%, P<0.01) conditions in ischemic segments. Optimal cutoff values for stress C-strain (–17.5%) could successfully differentiate segments with ischemia or infarction from non-ischemic ones with a sensitivity of 86%, a specificity of 65%, and an area under the curve of 0.79.
Conclusions: C-strain analysis using tagged MR could detect ATP-stress-induced contractile impairment in isch-emic myocardium. (Circ J 2013; 77: 1235 – 1241)
Key Words: Magnetic resonance imaging; Myocardial infarction; Myocardial ischemia; Myocardial perfusion imag-ing; Ventricular function
ORIGINAL ARTICLEImaging
Circulation Journal Vol.77, May 2013
1236 KIDO T et al.
4 women; mean age, 28±3 years) were enrolled as a control group. For the controls, tagged MR under ATP-stress and at-rest conditions was performed using the same imaging param-eters as for the patient group.
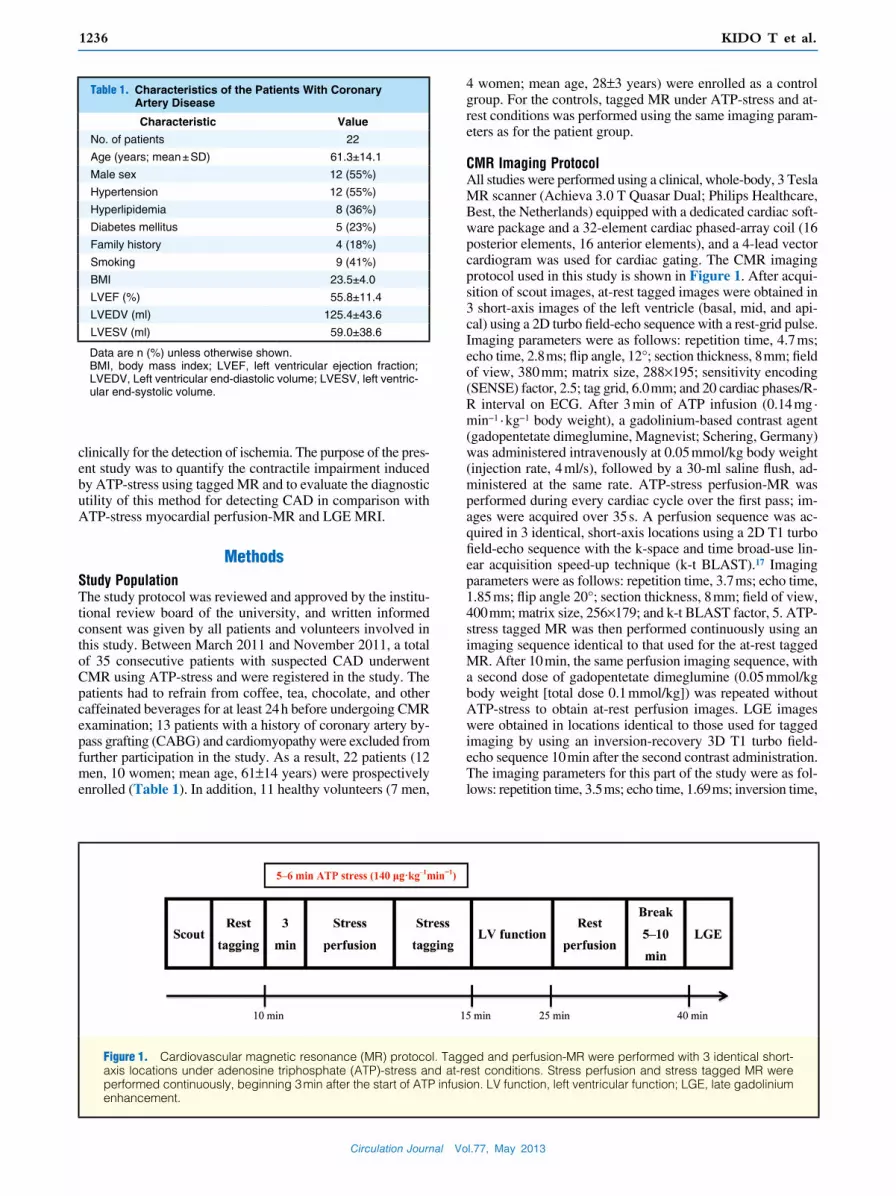
CMR Imaging ProtocolAll studies were performed using a clinical, whole-body, 3 Tesla MR scanner (Achieva 3.0 T Quasar Dual; Philips Healthcare, Best, the Netherlands) equipped with a dedicated cardiac soft-ware package and a 32-element cardiac phased-array coil (16 posterior elements, 16 anterior elements), and a 4-lead vector cardiogram was used for cardiac gating. The CMR imaging protocol used in this study is shown in Figure 1. After acqui-sition of scout images, at-rest tagged images were obtained in 3 short-axis images of the left ventricle (basal, mid, and api-cal) using a 2D turbo field-echo sequence with a rest-grid pulse. Imaging parameters were as follows: repetition time, 4.7 ms; echo time, 2.8 ms; flip angle, 12°; section thickness, 8 mm; field of view, 380 mm; matrix size, 288×195; sensitivity encoding (SENSE) factor, 2.5; tag grid, 6.0 mm; and 20 cardiac phases/R-R interval on ECG. After 3 min of ATP infusion (0.14 mg · min−1 · kg−1 body weight), a gadolinium-based contrast agent (gadopentetate dimeglumine, Magnevist; Schering, Germany) was administered intravenously at 0.05 mmol/kg body weight (injection rate, 4 ml/s), followed by a 30-ml saline flush, ad-ministered at the same rate. ATP-stress perfusion-MR was performed during every cardiac cycle over the first pass; im-ages were acquired over 35 s. A perfusion sequence was ac-quired in 3 identical, short-axis locations using a 2D T1 turbo field-echo sequence with the k-space and time broad-use lin-ear acquisition speed-up technique (k-t BLAST).17 Imaging parameters were as follows: repetition time, 3.7 ms; echo time, 1.85 ms; flip angle 20°; section thickness, 8 mm; field of view, 400 mm; matrix size, 256×179; and k-t BLAST factor, 5. ATP-stress tagged MR was then performed continuously using an imaging sequence identical to that used for the at-rest tagged MR. After 10 min, the same perfusion imaging sequence, with a second dose of gadopentetate dimeglumine (0.05 mmol/kg body weight [total dose 0.1 mmol/kg]) was repeated without ATP-stress to obtain at-rest perfusion images. LGE images were obtained in locations identical to those used for tagged imaging by using an inversion-recovery 3D T1 turbo field-echo sequence 10 min after the second contrast administration. The imaging parameters for this part of the study were as fol-lows: repetition time, 3.5 ms; echo time, 1.69 ms; inversion time,
clinically for the detection of ischemia. The purpose of the pres-ent study was to quantify the contractile impairment induced by ATP-stress using tagged MR and to evaluate the diagnostic utility of this method for detecting CAD in comparison with ATP-stress myocardial perfusion-MR and LGE MRI.
MethodsStudy PopulationThe study protocol was reviewed and approved by the institu-tional review board of the university, and written informed consent was given by all patients and volunteers involved in this study. Between March 2011 and November 2011, a total of 35 consecutive patients with suspected CAD underwent CMR using ATP-stress and were registered in the study. The patients had to refrain from coffee, tea, chocolate, and other caffeinated beverages for at least 24 h before undergoing CMR examination; 13 patients with a history of coronary artery by-pass grafting (CABG) and cardiomyopathy were excluded from further participation in the study. As a result, 22 patients (12 men, 10 women; mean age, 61±14 years) were prospectively enrolled (Table 1). In addition, 11 healthy volunteers (7 men,
Table 1. Characteristics of the Patients With Coronary Artery Disease
Characteristic Value
No. of patients 22
Age (years; mean ± SD) 61.3±14.1
Male sex 12 (55%)
Hypertension 12 (55%)
Hyperlipidemia 8 (36%)
Diabetes mellitus 5 (23%)
Family history 4 (18%)
Smoking 9 (41%)
BMI 23.5±4.0
LVEF (%) 55.8±11.4
LVEDV (ml) 125.4±43.6
LVESV (ml) 59.0±38.6
Data are n (%) unless otherwise shown.BMI, body mass index; LVEF, left ventricular ejection fraction; LVEDV, Left ventricular end-diastolic volume; LVESV, left ventric-ular end-systolic volume.
Figure 1. Cardiovascular magnetic resonance (MR) protocol. Tagged and perfusion-MR were performed with 3 identical short-axis locations under adenosine triphosphate (ATP)-stress and at-rest conditions. Stress perfusion and stress tagged MR were performed continuously, beginning 3 min after the start of ATP infusion. LV function, left ventricular function; LGE, late gadolinium enhancement.

Circulation Journal Vol.77, May 2013
12373 Tesla Tagged MR to Detect CAD
was defined as an area with a perfusion defect (>25% of wall thickness) under ATP-stress, normal perfusion at rest, and non-LGE in delayed images (Figure 3). An infarcted segment was defined as an area with a perfusion defect under ATP-stress and the presence of LGE (>25% of wall thickness). A non-ischemic segment was defined as an area with normal perfu-sion under ATP-stress and at-rest, and non-LGE in delayed images. If the same segment was deemed both ischemic and infarcted, the determination was based on views on either side. Control segments corresponded to those in normal volunteers; the 11 volunteers did not show any non-ischemic segments.
Statistical AnalysisContinuous data are expressed as means ± SD. The differences in the C-strain values between ATP-stress and at-rest tagged images in each group were analyzed using the Wilcoxon signed-rank test. The differences in the C-strain values between any 2 of the 4 groups were analyzed using the Steel-Dwass test. The diagnostic capability of the C-strain for CAD was ana-
400–500 ms (adjusted to the null signal of the normal myocar-dium using the “Look Locker sequence”18); flip angle, 15°; section thickness, 6 mm; field of view, 350 mm; matrix size, 224×157; and SENSE factor, 2.
MR Data AnalysisTag analysis was performed using open source software (Osirix inTag; http://www.osirix-viewer.com) and the sine-wave mod-eling method.19 The peak negative value of the subendocar-dial C-strain during a cardiac cycle was measured for 4 seg-ments (anterior, septal, inferior, and lateral) of the basal, mid, and apical left ventricle using short-axis tagged images during ATP-stress and at-rest conditions; the obtained value was used as an estimate of contraction (Figure 2). The myocardial seg-ment was categorized as being ischemic, infarcted, or non-ischemic according to the ATP-stress perfusion and LGE MRI. The perfusion and LGE images were visually analyzed by 2 individuals, experienced in reading CMR images; both were blinded to the results of tagged analysis. An ischemic segment
Figure 2. Tagged images and time-curves of circumferential-strain (C-strain) under adenosine triphosphate (ATP)-stress and at-rest conditions in a 28-year-old healthy female volunteer. Short-axis, mid-ventricular view of tagging at-rest (A) and under stress (B) at end-systole. The x-axis indicates the time frames (20 frames/cycle) and the y-axis indicates the C-strain values (C,D). Tagged images show an increase in wall motion and the absolute peak C-strain value becomes elevated under ATP-stress conditions.
Circulation Journal Vol.77, May 2013
1238 KIDO T et al.
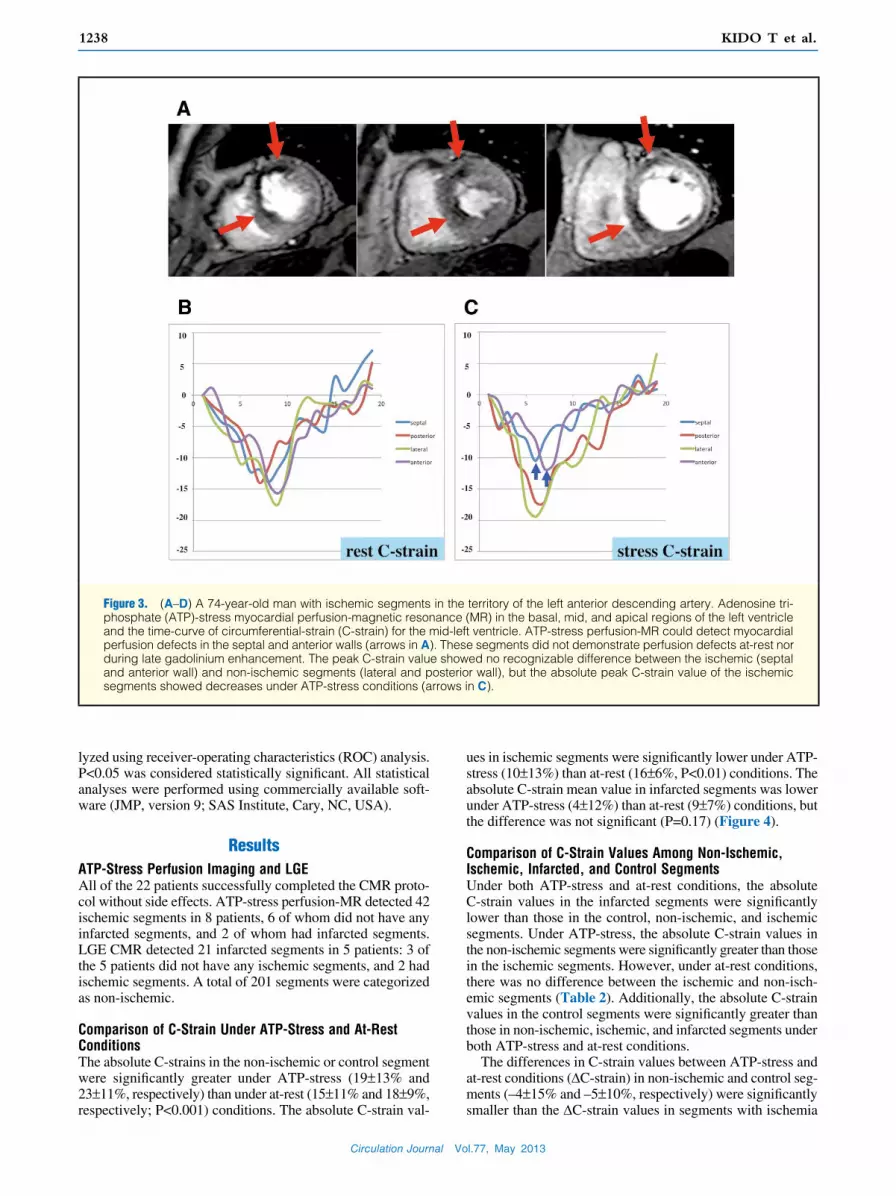
ues in ischemic segments were significantly lower under ATP-stress (10±13%) than at-rest (16±6%, P<0.01) conditions. The absolute C-strain mean value in infarcted segments was lower under ATP-stress (4±12%) than at-rest (9±7%) conditions, but the difference was not significant (P=0.17) (Figure 4).
Comparison of C-Strain Values Among Non-Ischemic, Ischemic, Infarcted, and Control SegmentsUnder both ATP-stress and at-rest conditions, the absolute C-strain values in the infarcted segments were significantly lower than those in the control, non-ischemic, and ischemic segments. Under ATP-stress, the absolute C-strain values in the non-ischemic segments were significantly greater than those in the ischemic segments. However, under at-rest conditions, there was no difference between the ischemic and non-isch-emic segments (Table 2). Additionally, the absolute C-strain values in the control segments were significantly greater than those in non-ischemic, ischemic, and infarcted segments under both ATP-stress and at-rest conditions.
The differences in C-strain values between ATP-stress and at-rest conditions (∆C-strain) in non-ischemic and control seg-ments (–4±15% and –5±10%, respectively) were significantly smaller than the ∆C-strain values in segments with ischemia
lyzed using receiver-operating characteristics (ROC) analysis. P<0.05 was considered statistically significant. All statistical analyses were performed using commercially available soft-ware (JMP, version 9; SAS Institute, Cary, NC, USA).
ResultsATP-Stress Perfusion Imaging and LGEAll of the 22 patients successfully completed the CMR proto-col without side effects. ATP-stress perfusion-MR detected 42 ischemic segments in 8 patients, 6 of whom did not have any infarcted segments, and 2 of whom had infarcted segments. LGE CMR detected 21 infarcted segments in 5 patients: 3 of the 5 patients did not have any ischemic segments, and 2 had ischemic segments. A total of 201 segments were categorized as non-ischemic.
Comparison of C-Strain Under ATP-Stress and At-Rest ConditionsThe absolute C-strains in the non-ischemic or control segment were significantly greater under ATP-stress (19±13% and 23±11%, respectively) than under at-rest (15±11% and 18±9%, respectively; P<0.001) conditions. The absolute C-strain val-
Figure 3. (A–D) A 74-year-old man with ischemic segments in the territory of the left anterior descending artery. Adenosine tri-phosphate (ATP)-stress myocardial perfusion-magnetic resonance (MR) in the basal, mid, and apical regions of the left ventricle and the time-curve of circumferential-strain (C-strain) for the mid-left ventricle. ATP-stress perfusion-MR could detect myocardial perfusion defects in the septal and anterior walls (arrows in A). These segments did not demonstrate perfusion defects at-rest nor during late gadolinium enhancement. The peak C-strain value showed no recognizable difference between the ischemic (septal and anterior wall) and non-ischemic segments (lateral and posterior wall), but the absolute peak C-strain value of the ischemic segments showed decreases under ATP-stress conditions (arrows in C).

Circulation Journal Vol.77, May 2013
12393 Tesla Tagged MR to Detect CAD
ditions. ATP is a naturally occurring vasodilator that has been used to induce maximal coronary hyperemia. It also induces an elevated heart rate and may lead to hyperkinesis. Coronary hyperemia induced by ATP infusion has been reported to re-sult in hyperkinetic wall motion in normal myocardium.20 The increase in C-strain under ATP-stress in non-ischemic and control segments, as indicated in Figure 4, correlates with the physiological status under ATP-stress conditions.
or infarction (7±12% and 5±10%, respectively; P<0.001). There was no significant difference in the ∆C-strain values between non-ischemic and control segments, or between isch-emic and infarcted segments (Figure 5).
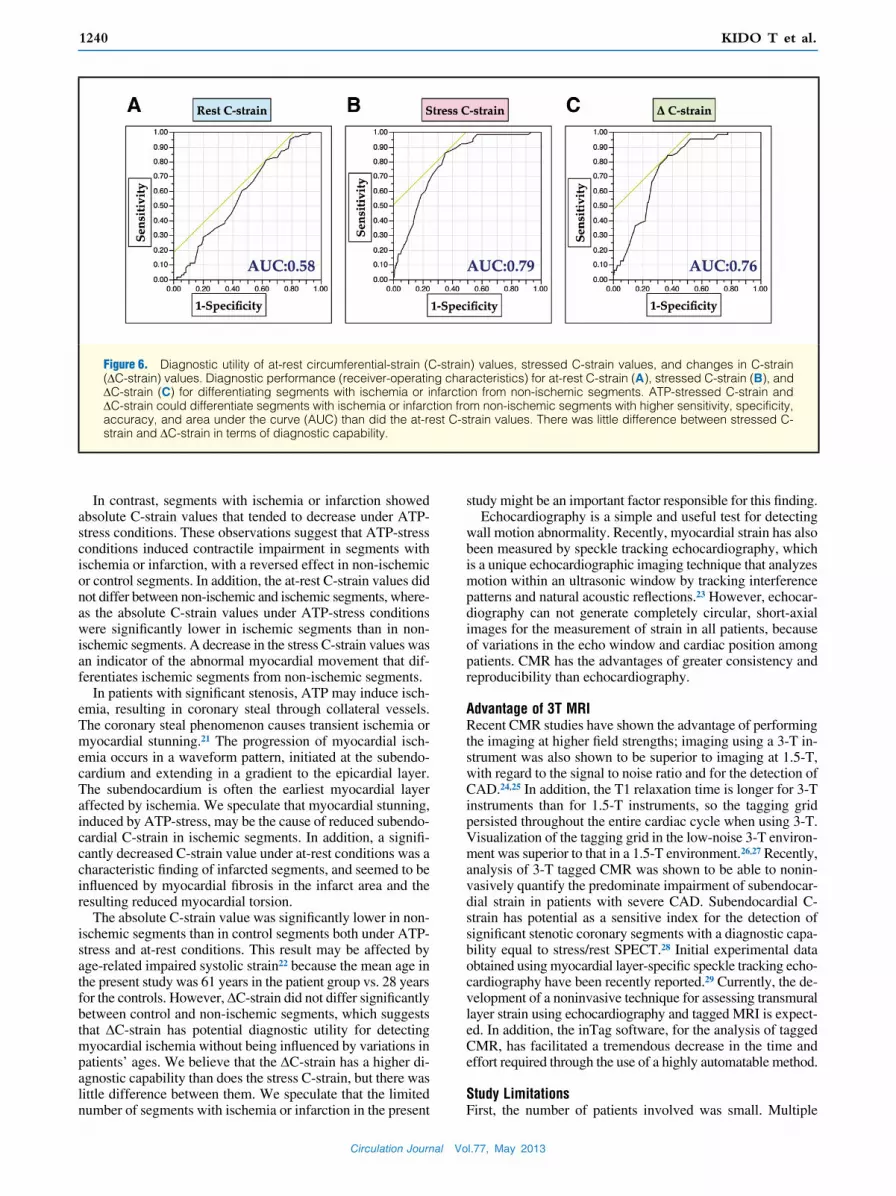
Diagnostic Capability of C-StrainA cutoff value of –19.0% for the at-rest C-strain value allowed differentiation between segments with ischemia or infarction from non-ischemic segments, with a sensitivity of 81%, spec-ificity of 37%, and accuracy of 44%; area under the curve (AUC) =0.58. A cutoff value of –17.5% for the ATP-stress C-strain value could make the same differentiation between segments, with a sensitivity of 86%, specificity of 65%, and accuracy of 68%; AUC=0.79. Similarly, a cutoff value of –0.05% for the ∆C-strain value could differentiate segments with ischemia or infarction from non-ischemic segments with a sensitivity of 84.1%, specificity of 63.1%, and accuracy of 66.4%; AUC =0.76 (Figure 6).
A cutoff value of –13.5% for the at-rest C-strain value could differentiate infarcted segments from ischemic segments with a sensitivity of 76.2%, specificity of 71.4%, and accuracy of 73%; AUC =0.8.
DiscussionTo our knowledge, this is the first clinical study to quantita-tively analyze contractile impairment in coronary arteries in-duced by ATP-stress in segments with ischemia or infarction using ATP-stress tagged MR. By using this approach, we found that, in the non-ischemic or control segments, the absolute C-strain values increased significantly under ATP-stress con-ditions compared with determinations made under at-rest con-
Figure 4. Absolute circumferential-strain (C-strain) differences between stressed and at-rest tagged images. Bars and horizontal lines indicate means and standard deviations. *P<0.01, **P<0.001.
Table 2. Absolute Peak C-Strain Values During ATP-Stress and At-Rest CMR Imaging Conditions Among Ischemic, Non-Ischemic, and Infarcted Segments
Segment No. of segments Rest C-strain (%) P value Stress C-strain (%) P value
Non-ischemic 201 14.6±10.8 18.6±13.0
Ischemic 42 16.4±6.2 NS 9.7±13.2 <0.001
Infarcted 21 8.6±6.7 <0.01 3.9±11.5 <0.001
P value: difference with respect to non-ischemic segments. ATP, adenosine triphosphate; CMR, cardiovascular magnetic resonance; C-strain, circumferential strain.
Figure 5. Changes in the circumferential-strain (∆C-strain) among ischemic, non-ischemic, infarcted, and control seg-ments. Bars and horizontal lines indicate means and standard deviations. *P<0.001.
Circulation Journal Vol.77, May 2013
1240 KIDO T et al.
study might be an important factor responsible for this finding.Echocardiography is a simple and useful test for detecting
wall motion abnormality. Recently, myocardial strain has also been measured by speckle tracking echocardiography, which is a unique echocardiographic imaging technique that analyzes motion within an ultrasonic window by tracking interference patterns and natural acoustic reflections.23 However, echocar-diography can not generate completely circular, short-axial images for the measurement of strain in all patients, because of variations in the echo window and cardiac position among patients. CMR has the advantages of greater consistency and reproducibility than echocardiography.
Advantage of 3T MRIRecent CMR studies have shown the advantage of performing the imaging at higher field strengths; imaging using a 3-T in-strument was also shown to be superior to imaging at 1.5-T, with regard to the signal to noise ratio and for the detection of CAD.24,25 In addition, the T1 relaxation time is longer for 3-T instruments than for 1.5-T instruments, so the tagging grid persisted throughout the entire cardiac cycle when using 3-T. Visualization of the tagging grid in the low-noise 3-T environ-ment was superior to that in a 1.5-T environment.26,27 Recently, analysis of 3-T tagged CMR was shown to be able to nonin-vasively quantify the predominate impairment of subendocar-dial strain in patients with severe CAD. Subendocardial C-strain has potential as a sensitive index for the detection of significant stenotic coronary segments with a diagnostic capa-bility equal to stress/rest SPECT.28 Initial experimental data obtained using myocardial layer-specific speckle tracking echo-cardiography have been recently reported.29 Currently, the de-velopment of a noninvasive technique for assessing transmural layer strain using echocardiography and tagged MRI is expect-ed. In addition, the inTag software, for the analysis of tagged CMR, has facilitated a tremendous decrease in the time and effort required through the use of a highly automatable method.
Study LimitationsFirst, the number of patients involved was small. Multiple
In contrast, segments with ischemia or infarction showed absolute C-strain values that tended to decrease under ATP-stress conditions. These observations suggest that ATP-stress conditions induced contractile impairment in segments with ischemia or infarction, with a reversed effect in non-ischemic or control segments. In addition, the at-rest C-strain values did not differ between non-ischemic and ischemic segments, where-as the absolute C-strain values under ATP-stress conditions were significantly lower in ischemic segments than in non-ischemic segments. A decrease in the stress C-strain values was an indicator of the abnormal myocardial movement that dif-ferentiates ischemic segments from non-ischemic segments.
In patients with significant stenosis, ATP may induce isch-emia, resulting in coronary steal through collateral vessels. The coronary steal phenomenon causes transient ischemia or myocardial stunning.21 The progression of myocardial isch-emia occurs in a waveform pattern, initiated at the subendo-cardium and extending in a gradient to the epicardial layer. The subendocardium is often the earliest myocardial layer affected by ischemia. We speculate that myocardial stunning, induced by ATP-stress, may be the cause of reduced subendo-cardial C-strain in ischemic segments. In addition, a signifi-cantly decreased C-strain value under at-rest conditions was a characteristic finding of infarcted segments, and seemed to be influenced by myocardial fibrosis in the infarct area and the resulting reduced myocardial torsion.
The absolute C-strain value was significantly lower in non-ischemic segments than in control segments both under ATP-stress and at-rest conditions. This result may be affected by age-related impaired systolic strain22 because the mean age in the present study was 61 years in the patient group vs. 28 years for the controls. However, ∆C-strain did not differ significantly between control and non-ischemic segments, which suggests that ∆C-strain has potential diagnostic utility for detecting myocardial ischemia without being influenced by variations in patients’ ages. We believe that the ∆C-strain has a higher di-agnostic capability than does the stress C-strain, but there was little difference between them. We speculate that the limited number of segments with ischemia or infarction in the present
Figure 6. Diagnostic utility of at-rest circumferential-strain (C-strain) values, stressed C-strain values, and changes in C-strain (∆C-strain) values. Diagnostic performance (receiver-operating characteristics) for at-rest C-strain (A), stressed C-strain (B), and ∆C-strain (C) for differentiating segments with ischemia or infarction from non-ischemic segments. ATP-stressed C-strain and ∆C-strain could differentiate segments with ischemia or infarction from non-ischemic segments with higher sensitivity, specificity, accuracy, and area under the curve (AUC) than did the at-rest C-strain values. There was little difference between stressed C-strain and ∆C-strain in terms of diagnostic capability.
Circulation Journal Vol.77, May 2013
12413 Tesla Tagged MR to Detect CAD
CC, et al. Cardiovascular magnetic resonance and single-photon emis-sion computed tomography for diagnosis of coronary heart disease (CE-MARC): A prospective trial. Lancet 2012; 379: 453 – 460.
11. Kwong RY, Chan AK, Brown KA, Chan CW, Reynolds HG, Davis ST. Impact of unrecognized myocardial scar detected by cardiac mag-netic resonance imaging on event-free survival in patients presenting with signs or symptoms of coronary artery disease. Circulation 2006; 113: 2733 – 2743.
12. Mahrholdt H, Klem I, Sechtem U. Cardiovascular MRI for detection of myocardial viability and ischaemia. Heart 2007; 93: 122 – 129.
13. Bellenger NG, Marcus NJ, Rajappan K, Yacoub M, Banner NR, Pennell DJ. Comparison of techniques for the measurement of left ventricular function following cardiac transplantation. J Cardiovasc Magn Reson 2002; 4: 255 – 263.
14. Gotte MJ, van Rossum AC, Twisk JWR, Kuijer JPA, Marcus JT, Visser CA. Quantification of regional contractile function after in-farction: Strain analysis superior to wall thickening analysis in dis-criminating infarct from remote myocardium. J Am Coll Cardiol 2001; 37: 808 – 817.
15. Kuijpers D, Ho KY, van Dijkman PR, Vliegenthart R, Oudkerk M. Dobutamine cardiovascular magnetic resonance for the detection of myocardial ischemia with the use of myocardial tagging. Circulation 2003; 107: 1592 – 1597.
16. Paetsch I, Jahnke C, Wahl A, Gebker R, Neuss M, Fleck E, et al. Comparison of dobutamine stress magnetic resonance, adenosine stress magnetic resonance, and adenosine stress magnetic resonance perfusion. Circulation 2004; 110: 835 – 842.
17. Tsao J, Boesiger P, Pruessmann KP. k-t BLAST and k-t SENSE: Dynamic MRI with high frame rate exploiting spatiotemporal cor-relations. Magn Reson Med 2003; 50: 1031 – 1042.
18. Look DC, Locker DR. Time saving in measurement of NMR and EPR relaxation times. Rev Sci Instrum 1970; 41: 250 – 251.
19. Arts T, Prinzen FW, Delhaas T, Milles JR, Rossi AC, Clarysse P. Mapping displacement and deformation of the heart with local sine-wave modeling. IEEE Trans Med Imag 2010; 29: 1114 – 1123.
20. Ran H, Zhang PY, Fang LL, Ma XW, Wu WF, Feng WF. Clinic value of two-dimensional speckle tracking combined with adenosine stress echocardiography for assessment of myocardial viability. Echocar-diography 2012; 29: 688 – 694.
21. Druz RS, Akinboboye OA, Grimson R, Nichols LJ, Reichek N. Post-ischemic stunning after adenosine vasodilator stress. J Nucl Cardiol 2004; 11: 534 – 541.
22. Cheng S, Fernandes RS, Bluemke DA, Mcclelland RL, Kronmal RA, Lima AC. Age-related left ventricular remodeling and associated risk for cardiovascular outcomes: The Multi-Ethnic Study of Atheroscle-rosis. Circ Cardiovasc Imaging 2009; 2: 191−198.
23. Helle-Valle T, Crosby J, Edvardsen T, Lyseggen E, Amundsen BH, Smith HJ, et al. New non invasive method for assessment of left ventricular rotation: Speckle tracking echocardiography. Circulation 2005; 112: 3149 – 3156.
24. Strach K, Meyer C, Thomas D, Naehle CP, Schmitz C, Litt H, et al. High-resolution myocardial perfusion imaging at 3 T: Comparison to 1.5 T in healthy volunteers. Eur Radiol 2007; 17: 1829 – 1835.
25. Araoz PA, Glockner JF, McGee KP, Potter DD Jr, Valeti VU, Stanley DW, et al. 3 Tesla MR imaging provides improved contrast in first-pass myocardial perfusion imaging over a range of gadolinium doses. J Cardiovasc Magn Reson 2005; 7: 559 – 564.
26. Gutberlet M, Schwinge K, Freyhardt P, Spors B, Grothoff M, Denecke T, et al. Influence of high magnetic field strengths and parallel acqui-sition strategies on image quality in cardiac 2D CINE magnetic reso-nance imaging: Comparison of 1.5 T vs 3.0 T. Eur Radiol 2005; 15: 1586 – 1597.
27. Valeti VU, Chun W, Potter DD, Araoz PA, McGee KP, Glockner JF, et al. Myocardial tagging and strain analysis at 3 Tesla: Comparison with 1.5 Tesla imaging. J Magn Reson Img 2006; 23: 477 – 480.
28. Nagao M, Hatakenaka M, Matsuo Y, Kamitani T, Higuchi K, Shikata F, et al. Subendocardial contractile impairment in chronic ischemic myocardium: Assessment by strain analysis of 3T tagged CMR. J Cardiovasc Magn Reson 2012; 14: 14 – 21.
29. Nishimura K, Okayama H, Inoue K, Saito M, Yoshii T, Hiasa G, et al. Direct measurement of radial strain in the inner-half layer of the left ventricular wall in hypertensive patients. J Cardiol 2012; 59: 64 – 71.
30. Yu CM, Lin H, Yang H, Kong SL, Zhang Q, Lee SW. Progression of systolic abnormalities in patients with “isolated” diastolic heart failure and diastolic dysfunction. Circulation 2002; 105: 1195 – 1201.
comparisons should be interpreted with caution given the small sample size. Second, the mixture of ischemic, infarct, and non-ischemic myocardium in a single segment could affect the results. Third, in patients with CAD, the subendocardial lon-gitudinal myofiber is vulnerable and susceptible in the areas of myocardial hypoperfusion; thus, it is prone to earlier dam-age leading to impaired longitudinal function.30 Because of limitations in the longitudinal tagged CMR scan, longitudinal myocardial strain was not calculated in our analysis. Finally, conventional coronary angiography was not performed to con-firm ischemic and infarcted segments or coronary artery ste-nosis. However, previous study has reported stress perfusion-CMR as a valuable alternative to SPECT for CAD detection, with equal or better performance than SPECT in this regard.9 We believe that ATP-stress perfusion-MR provides a diagno-sis for ischemic segments comparable to that using conven-tional coronary angiography.
ConclusionIn conclusion, C-strain analysis (ie, quantitative analysis of ATP-stress tagged MR) showed contractile impairment in non-ischemic, ischemic, and infarcted segments in patients with suspected CAD. Under ATP stress, a greater decrease in C-strain was a candidate factor for differentiating ischemic seg-ments from non-ischemic segments. A significantly decreased C-strain value at rest was useful for differentiating infarcted segments from ischemic segments.
DisclosuresMichinobu Nagao: Bayer Healthcare Japan, Modest, Research Grant; Philips Electronics Japan, Modest, Research Grant.
References 1. Wu KC. Variation on a theme: CMR as the “one-stop shop” for risk
stratification after infarction? J Am Coll Cardiol 2009; 2: 843 – 845. 2. Kim RJ, Wu E, Rafael A, Chen EL, Parker MA, Simonetti O, et al.
The use of contrast-enhanced magnetic resonance imaging to iden-tify reversible myocardial dysfunction. N Engl J Med 2000; 343: 1445 – 1453.
3. Kim WY, Danias PG, Stuber M, Flamm SD, Plein S, Nagel E, et al. Coronary magnetic resonance angiography for the detection of coro-nary stenoses. N Engl J Med 2001; 45: 1863 – 1869.
4. Klem I, Heitner JF, Shah DJ, Sketch MH, Behar V, Weinsaft J, et al. Improved detection of coronary artery disease by stress perfusion cardiovascular magnetic resonance with the use of delayed enhance-ment infarction imaging. J Am Coll Cardiol 2006; 47: 1630 – 1638.
5. Kwong RY, Schussheim AE, Rekhraj S, Aletras AH, Geller N, Davis J, et al. Detecting acute coronary syndrome in the emergency depart-ment with cardiac magnetic resonance imaging. Circulation 2003; 107: 531 – 537.
6. Cheung SC, Chan CW. Cardiac magnetic resonance imaging: Choice of the year: Which imaging modality is best for evaluation of myo-cardial ischemia? (MRI-side). Circ J 2011; 75: 724 – 730.
7. Ishida M, Kato S, Sakuma H. Cardiac MRI in ischemic heart disease. Circ J 2009; 73: 1577 – 1588.
8. Kirschbaum SW, Nieman K, Springeling T, Weustink AC, Ramcharitar S, Mieghem C, et al. Non-invasive diagnostic workup of patients with suspected stable angina by combined computed tomography coronary angiography and magnetic resonance perfusion imaging. Circ J 2011; 75: 1678 – 1684.
9. Schwitter J, Wacker CM, van Rossum AC, Lombardi M, Al-Saadi N, Ahlstom H, et al. MR-IMPACT: Comparison of perfusion-cardiac magnetic resonance with single-photon emission computed tomog-raphy for the detection of coronary artery disease in a multicentre, multivendor, randomized trial. Eur Heart J 2008; 9: 480 – 489.
10. Greenwood JP, Maredia N, Younger JF, Brown JM, Nixon J, Everett





























