Embed Size (px)
Citation preview

ORIGINAL ARTICLE: Experimental Endoscopy
Endoscopic closure of colon perforation compared to surgery ina porcine model: a randomized controlled trial (with videos)
Gottumukkala S. Raju, MD, Annette Fritscher-Ravens, MD, Richard I. Rothstein, MD, Paul Swain, MD,Andres Gelrud, MD, Ijaz Ahmed, MD, Guillermo Gomez, MD, Markus Winny, MD,Thomas Sonnanstine, MD, Maria Bergstrom, MD, PhD, Per-Ola Park, MD, PhD
Galveston, Texas, Lebanon, New Hampshire, Cincinnati, Ohio, Florence, Kentucky, USA, London, United Kingdom,Hannover, Germany, Goteborg, Sweden
Background: Endoscopic closure of inadvertent or intentional colon perforations might be valuable if compa-rable to surgical closure.
Objective: The aim of this study was to compare endoscopic closure of a 4-cm colon perforation in a porcinemodel with surgical closure in a multicenter study.
Setting: University hospitals in the United States and Europe.
Design and Interventions: After creating a 4-cm linear colon perforation, the animals were randomized toeither endoscopic or surgical closure. The total procedure time from the beginning of perforation to the com-pletion of procedure was measured. The animals were euthanized after 2 weeks to evaluate healing, unless therewas a complication.
Results: Fifty-four animals were randomized to either surgical or endoscopic closure of colon perforation. Eightanimals developed complications, and 7 of these were euthanized before 2 weeks. Twenty-three animals in eachgroup survived for 2 weeks. Surgical closure of the perforation was successful in all animals in that group, andendoscopic closure was successful in 25 of the 27 animals. The median procedure time was shorter in the sur-gery group compared to the endoscopy group (35 vs 44 minutes, P Z.016). Peritonitis, local adhesions, and leaktest results were comparable in both groups. Distant adhesions were less frequent in the endoscopic closuregroup (26.1% vs 56.5%, P Z .03). Five of the 186 T-tags (2.7%) were noted in the adjacent viscera.
Limitation: This porcine study does not mimic clean colon perforation in humans; it mimics dirty colon per-foration in humans.
Conclusions: Endoscopic closure of a 4-cm colon perforation was comparable to surgery, and this technique can bepotentially used for closure of intentional or inadvertent colon perforations. (Gastrointest Endosc 2008;68:324-32.)
Inadvertent instrumental perforation is a serious com-plication of colonoscopy.1-9 Management and outcome de-pends on prompt surgical closure of perforation to limitleakage of colonic contents and prevent peritonitis.4 De-spite the best efforts, peritonitis occurs in half of the pa-tients because of the inevitable delay in arranging forsurgery. Fecal diversion followed by secondary repairmay be required in those with diffuse peritonitis.1,2,4,6,10-12
Abbreviations: IMCA, InScope Multi-Clip Applier; TAS, Tissue Apposition
System.
Copyright ª 2008 by the American Society for Gastrointestinal Endoscopy
0016-5107/$32.00
doi:10.1016/j.gie.2008.03.006
324 GASTROINTESTINAL ENDOSCOPY Volume 68, No. 2 : 2008
Colonoscopic perforations after polypectomy are small(1-2 cm), whereas those after mechanical injury can ex-tend up to 6 cm.4 Recently, experimental studies havedemonstrated that GI perforations can be closed by endos-copy without the need for surgery.13-22 Even 4-cm colonperforations can be closed successfully by endoscopic su-turing.13 Encouraged by this experience, we compared en-doscopic closure of a 4-cm colon perforation with surgicalclosure in a randomized controlled trial with a porcinemodel.
MATERIALS AND METHODS
Five academic centers in the United States and Europeparticipated in the study after approval of the protocol
www.giejournal.org

Raju et al Endoscopic closure of colon perforation
from the Institutional Animal Care and Use Committees.Before participation in the study, all the endoscopists prac-ticed endoscopic closure of GI perforations in live pigs withat least 4 sutures and 4 clips. Experienced general surgeonsundertook surgical closure of colon perforations.
The colon of each pig was cleaned by using a combina-tion of liquid diet, Visicol tablets (InKline PharmaceuticalCompany, Blue Bell, Pa) or glauber salt, and Fleets Phos-pho-Soda enema (C. B. Fleet Company, Inc, Lynchburg,Va) before the colonoscopy.23 After endoscopic clearingof the stools from the distal colon, the endoscope wasnot cleaned before the creation of colon perforation. A4-cm colon perforation was then made at 20 cm from theanus by using a double-channel colonoscope under generalanesthesia, as shown in Video 1 (available online atwww.giejournal.org). A biopsy forceps with a 4-cm markwas used to measure the length of the perforation. Afterpuncturing the colon wall with a needle-knife, an insu-lated-tip knife was introduced through the puncture to cre-ate a 4-cm colon perforation. The endoscope was routinelypassed into the peritoneal cavity to confirm the perfora-tion. After withdrawal of the endoscope back into thebowel (Video 1), the animals were randomized to either en-doscopic or surgical closure by opening a sealed envelope.
Endoscopic closure groupEndoscopic closure of the colon perforation was under-
taken either with sutures alone or a combination ofsutures and clips (Videos 2 to 4, available online atwww.giejournal.org). First, endoscopic suturing was usedto approximate the gaping perforation. Next, either su-tures or clips were used to complete the closure.
Suture closure. The Tissue Apposition System (TAS)(Ethicon Endo-Surgery, Inc, Cincinnati, Ohio) consists of 3components: a 3.0 polypropylene thread attached to a metalT-tag that can be top-loaded into a needle catheter (a longhollow needle enclosed in a plastic sheath) with a stylet todislodge the T-tag, and a thread-locking-cutting deviceloaded with a plastic ring and pin (collet and sleeve method).An endoscope with a standard accessory channel of at least2.8-mm diameter is required for insertion of this device.21,22
Three steps are involved in the endoscopic suturing:(1) needle puncture of one edge of the perforation, fol-lowed by the release of a T-tag, thus anchoring the threadbeyond the wall; (2) repeat of the procedure to place an-other T-tag on the opposite edge of perforation; and (3)knot tying of the two threads and suture cutting in a singlestep to complete suturing. Using a 1-cm exposed needle,we inserted T-tags at 0.5- to 1-cm intervals from the prox-imal end to the distal end of perforation.
Clip closure. The InScope Multi-Clip Applier (IMCA)(Ethicon Endo-Surgery, Inc, Cincinnati, Ohio) is loadedwith 4 clips that can be applied quickly during one inser-tion. The device has a locking mechanism that enables theendoscopist to lock on the target pathology, assess the ap-plication of clip before its deployment, and reposition the
www.giejournal.org
Capsule Summary
What is already known on this topic
d Peritonitis, resulting from inadvertent perforation duringcolonoscopy, may be prevented by endoscopic closureof the perforation immediately after it is recognized.
What this study adds to our knowledge
d In a comparison of endoscopic closure with surgicalclosure of a 4-cm colon perforation in a porcine model,the procedure was successful in 100% of the surgicalgroup and in 93% of the endoscopy group.
d Peritonitis, local adhesions, and leak test results werecomparable; median procedure time was shorter in thesurgery group, and distant adhesions were less frequentin the endoscopy group.
device, if desired. The rotatable end of the device enablesthe endoscopist to accurately position the device rightacross the perforation (Video 3).
Surgical closure groupSurgery was performed after the creation of the perfo-
ration and randomization, without any delay. Under sterileconditions, a midline laparotomy was used to explore theperitoneal cavity and identify the perforation site, whichwas closed with a running 4-0 resorbable monofilamentsuture. The peritoneum was not closed because sutureclosure of the peritoneum is shown to increase adhe-sions.24,25 The abdominal fascia was closed with a 2-0 run-ning monofilament resorbable suture. The skin was closedwith a 3-0 running nonresorbable suture.
Clinical assessment - 2 weeksAfter recovery from the procedure, the animals were
given nothing by mouth with free access to water forthe first 24 hours. Liquid diet was allowed for the next24 hours, and then regular diet was resumed. All the ani-mals received enrofloxacin 5 mg/kg daily for 2 weeks afterthe procedure. A veterinarian closely monitored the ani-mals twice a day for 2 weeks to detect any signs of distress.
NecropsyEuthanasia was performed on day 14, unless the ani-
mals demonstrated distress. After midline incision of theabdominal cavity, the peritoneum was closely inspectedfor peritonitis, abscesses, and adhesions. A methylene-blue dye leak test was performed to assess healing ofthe perforation.
Peritonitis. The peritoneal inflammation was gradedon a scale of 0 to 2 (0 Z no peritonitis, glistening perito-neum; 1 Z mild and focal fibrinous deposits; 2 Z severeand diffuse fibrinous deposits).
Volume 68, No. 2 : 2008 GASTROINTESTINAL ENDOSCOPY 325

Endoscopic closure of colon perforation Raju et al
Pericolonic abscess and fecal peritonitis. The par-acolic gutters and pelvic cavity were examined for free fluidand fecal matter. The site of colon perforation was observedfor any pericolonic inflammation and abscess formation.
Adhesions. Local adhesions at the site of perforationwere graded on a scale of 0 to 2 (0 Z no adhesions,thin serosal scar; 1 Z thin adhesion band; 2 Z thickband of adhesion). Distant adhesions away from the siteof perforation, extending between loops of bowels, bowelto adjacent viscera, or bowel to anterior abdominal wallwere recorded and were graded on a scale of 0 to 2(0 Z no adhesions between the abdominal wall and intes-tines; 1 Z single, thin adhesion between abdominal walland intestines; 2 Z multiple, dense adhesions betweenabdominal wall and intestines and other viscera).
Methylene-blue dye leak test. The segment of colonwith perforation was isolated and cross-clamped at one end,and through the other end methylene-blue dye was injectedunder pressure until maximum distension of colon was ob-served. The perforation site was closely inspected for leak-age of dye on the bench and under water.
MeasurementsThree parameters were compared between the
endoscopic and surgical closure groups: (1) success oftechnical closure and survival for 14 days without compli-cations; (2) procedure time, defined as the time requiredfor creating a perforation and subsequently closing it; and(3) necropsy on day 14 for peritonitis, pericolonic abscess,adhesions, T-tag injury to adjacent organs, and quality ofhealing by a dye leak test.
Statistical analysisThe outcome of surgery and endoscopy on colon per-
foration closuredperitonitis, pericolonic abscess, fecalperitonitis, and local and distant adhesionsdwas analyzedby using SAS version 9.1.3 (SAS Institute, Cary, NC)through a Fisher exact test. The analysis of the total pro-cedure time was done by using a 2-sample equal variancet test.
RESULTS
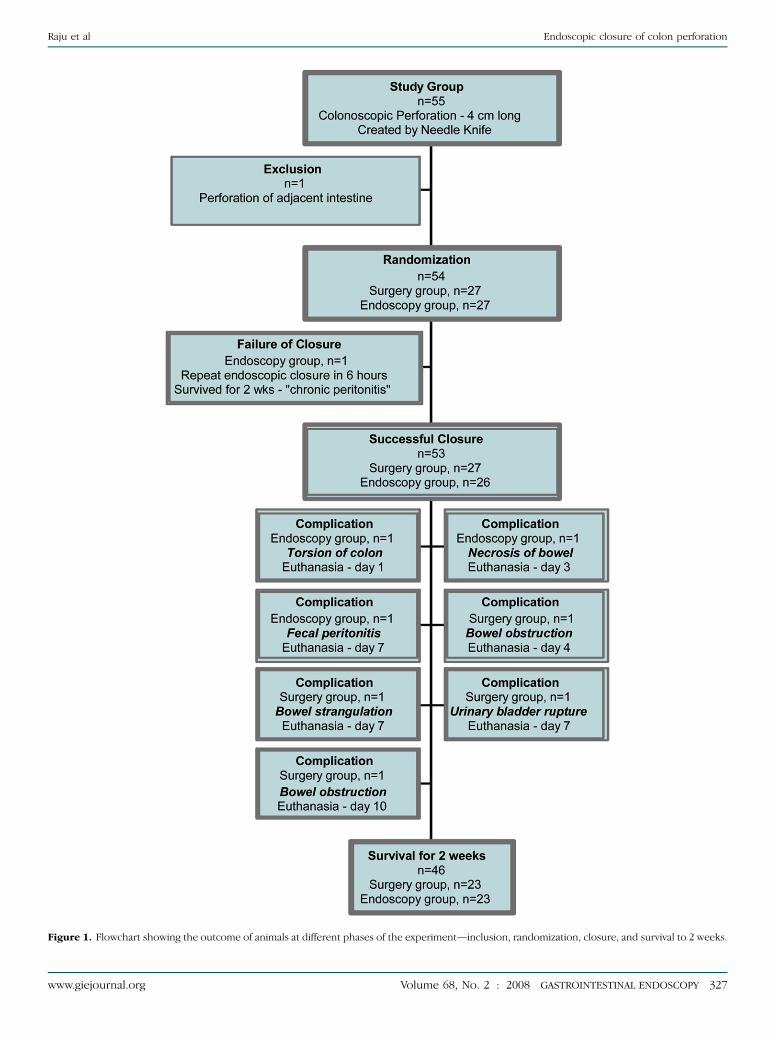
Fifty-five animals (center 1: 12 animals; center 2: 12 an-imals; center 3: 12 animals; center 4: 13 animals; and cen-ter 5: 6 animals) were enrolled in the study. In one animal,accidental needle-knife perforation of the adjacent smallbowel was observed, and the animal was therefore ex-cluded. The remaining 54 animals with colon perforationwere randomized to either surgical (n Z 27) or endo-scopic (n Z 27) closure (Fig. 1).
Procedure timeThe median procedure times in the endoscopic and
surgical closure groups were 44 (range 23-87) and 35(range: 14-70) minutes, respectively (P Z .016).
326 GASTROINTESTINAL ENDOSCOPY Volume 68, No. 2 : 2008
Surgical closureSurgical closure of perforation was successful in all 27
animals in that group. In the first animal randomized tosurgery, methylene blue was injected through the rectumto identify the perforation site. In another animal, a smallperforation of the adjacent bowel was noted that was su-tured as well.
Endoscopic closureEndoscopic closure of perforation was successful in 26
of the 27 animals. Sutures alone were used for perforationclosure in 12 animals (median number: 5 sutures; range: 3to 9 sutures). Both sutures and clips were used for perfo-ration closure in 15 animals (median number: 2 sutures þ4 clips; range: 1 suture þ 4 clips to 4 sutures þ 4 clips).
One animal failed to recover quickly after endoscopicclosure of perforation; repeated endoscopic closure wasattempted within 6 hours. This animal failed to eat nor-mally until day 11. Necropsy on day 14 revealed chronicdiffuse peritonitis, well-healed perforation, and an inad-vertent placement of a T-tag in the adjacent small bowel.
Follow-upOf the remaining 53 animals that underwent successful
closure of colon perforation, euthanasia was performed in7 animals before 2 weeks: 6 in the first week (surgerygroup, n Z 3; endoscopy group, n Z 3) and 1 in thesecond week (surgery group, nZ1).The remaining 46 an-imals (surgery group, n Z 23; endoscopy group, n Z 23)survived 2 weeks without complications.
Seven animals (endoscopy group, n Z 3 and surgerygroup, n Z 4) were euthanized before 2 weeks. In the en-doscopy group, bowel necrosis required euthanasia onday 3 in one animal due to T-tag insertion into the mesen-tery, fecal peritonitis required euthanasia on day 7 due toslippage of clips, and torsion of the colon required eutha-nasia on day 1. In the surgery group, bowel obstructionfrom dense peritoneal adhesions required euthanasia in3 animals on days 4, 7, and 10, respectively, and one ani-mal developed bladder rupture from accidental ligationof urethra during abdominal wall closure, requiring eutha-nasia on day 7.
Necropsy at 2 weeksTwenty-three animals in each group underwent nec-
ropsy at 2 weeks.Peritonitis. In the endoscopy closure group, the peri-
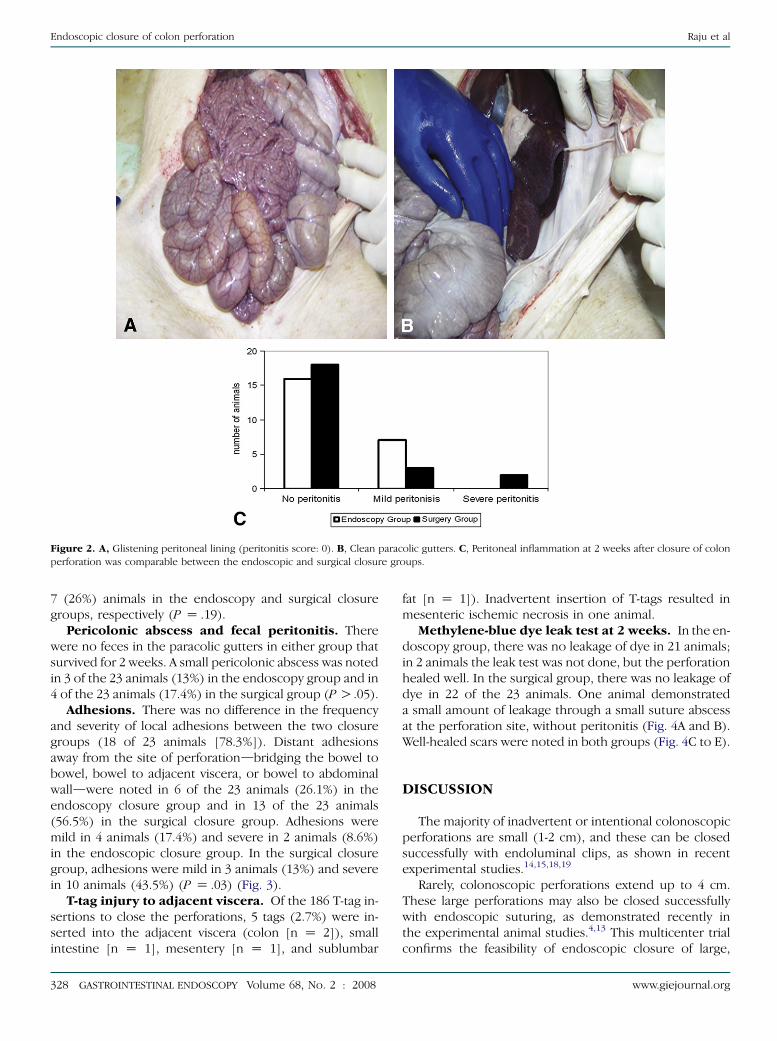
toneal cavity was normal in 16 of the 23 animals (69.6%),and mild fibrinous deposits were noted in 7 animals(30.4%). In the surgical closure group, the peritoneal cav-ity was normal in 18 of the 23 animals (78.3%), there weremild fibrinous deposits in 3 animals (13.0%), and severefibrinous deposits in 2 animals (8.7%) (P O .05) (Fig. 2).
By including all the animals from randomization (27 ineach group), peritonitis was observed in 10 (37%) and
www.giejournal.org
Raju et al Endoscopic closure of colon perforation
Figure 1. Flowchart showing the outcome of animals at different phases of the experimentdinclusion, randomization, closure, and survival to 2 weeks.
www.giejournal.org Volume 68, No. 2 : 2008 GASTROINTESTINAL ENDOSCOPY 327
Endoscopic closure of colon perforation Raju et al
Figure 2. A, Glistening peritoneal lining (peritonitis score: 0). B, Clean paracolic gutters. C, Peritoneal inflammation at 2 weeks after closure of colon
perforation was comparable between the endoscopic and surgical closure groups.
7 (26%) animals in the endoscopy and surgical closuregroups, respectively (P Z .19).
Pericolonic abscess and fecal peritonitis. Therewere no feces in the paracolic gutters in either group thatsurvived for 2 weeks. A small pericolonic abscess was notedin 3 of the 23 animals (13%) in the endoscopy group and in4 of the 23 animals (17.4%) in the surgical group (P O.05).
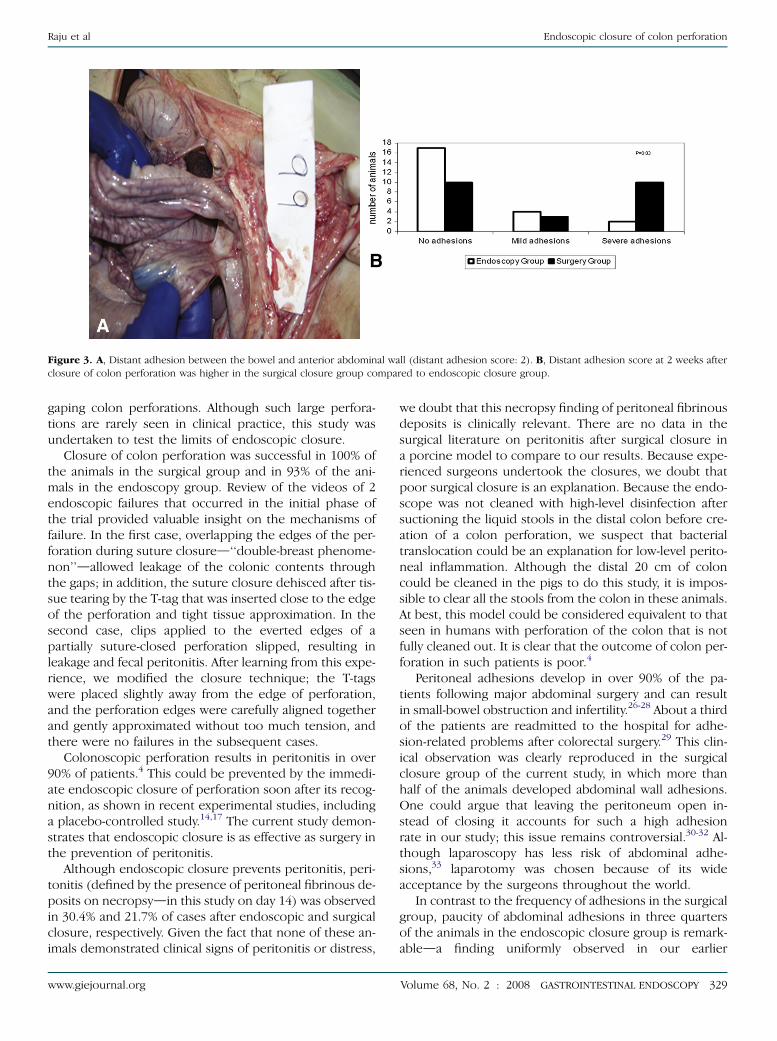
Adhesions. There was no difference in the frequencyand severity of local adhesions between the two closuregroups (18 of 23 animals [78.3%]). Distant adhesionsaway from the site of perforationdbridging the bowel tobowel, bowel to adjacent viscera, or bowel to abdominalwalldwere noted in 6 of the 23 animals (26.1%) in theendoscopy closure group and in 13 of the 23 animals(56.5%) in the surgical closure group. Adhesions weremild in 4 animals (17.4%) and severe in 2 animals (8.6%)in the endoscopic closure group. In the surgical closuregroup, adhesions were mild in 3 animals (13%) and severein 10 animals (43.5%) (P Z .03) (Fig. 3).
T-tag injury to adjacent viscera. Of the 186 T-tag in-sertions to close the perforations, 5 tags (2.7%) were in-serted into the adjacent viscera (colon [n Z 2]), smallintestine [n Z 1], mesentery [n Z 1], and sublumbar
328 GASTROINTESTINAL ENDOSCOPY Volume 68, No. 2 : 2008
fat [n Z 1]). Inadvertent insertion of T-tags resulted inmesenteric ischemic necrosis in one animal.
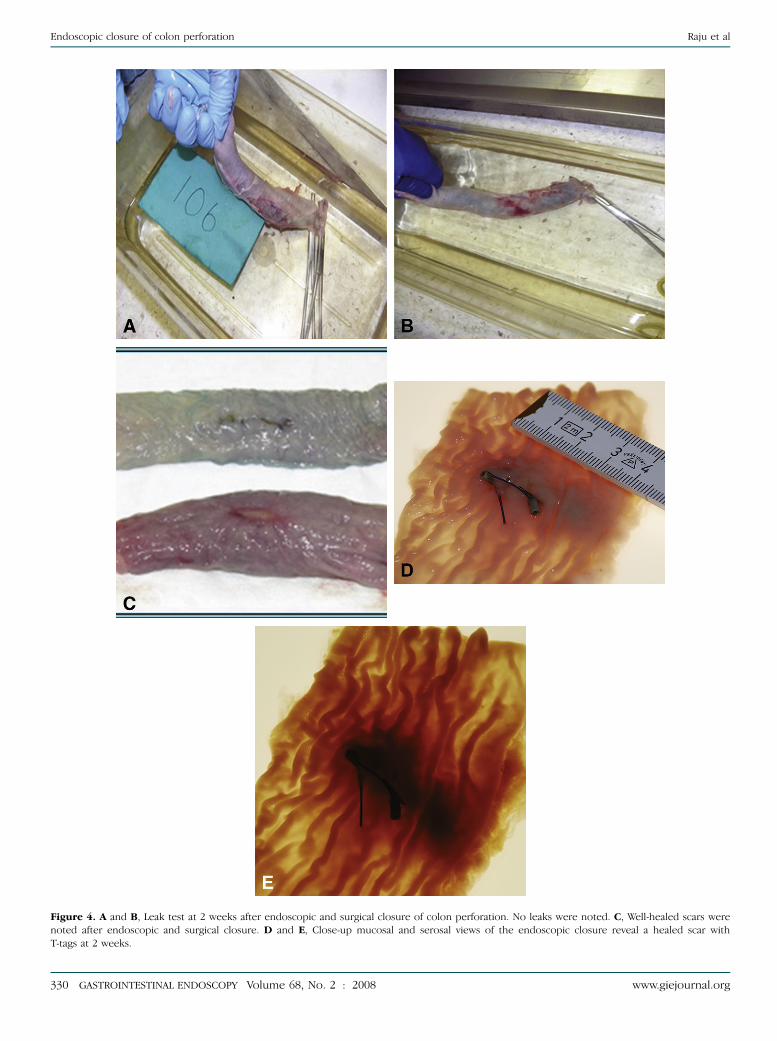
Methylene-blue dye leak test at 2 weeks. In the en-doscopy group, there was no leakage of dye in 21 animals;in 2 animals the leak test was not done, but the perforationhealed well. In the surgical group, there was no leakage ofdye in 22 of the 23 animals. One animal demonstrateda small amount of leakage through a small suture abscessat the perforation site, without peritonitis (Fig. 4A and B).Well-healed scars were noted in both groups (Fig. 4C to E).
DISCUSSION
The majority of inadvertent or intentional colonoscopicperforations are small (1-2 cm), and these can be closedsuccessfully with endoluminal clips, as shown in recentexperimental studies.14,15,18,19
Rarely, colonoscopic perforations extend up to 4 cm.These large perforations may also be closed successfullywith endoscopic suturing, as demonstrated recently inthe experimental animal studies.4,13 This multicenter trialconfirms the feasibility of endoscopic closure of large,
www.giejournal.org
Raju et al Endoscopic closure of colon perforation
Figure 3. A, Distant adhesion between the bowel and anterior abdominal wall (distant adhesion score: 2). B, Distant adhesion score at 2 weeks after
closure of colon perforation was higher in the surgical closure group compared to endoscopic closure group.
gaping colon perforations. Although such large perfora-tions are rarely seen in clinical practice, this study wasundertaken to test the limits of endoscopic closure.
Closure of colon perforation was successful in 100% ofthe animals in the surgical group and in 93% of the ani-mals in the endoscopy group. Review of the videos of 2endoscopic failures that occurred in the initial phase ofthe trial provided valuable insight on the mechanisms offailure. In the first case, overlapping the edges of the per-foration during suture closured‘‘double-breast phenome-non’’dallowed leakage of the colonic contents throughthe gaps; in addition, the suture closure dehisced after tis-sue tearing by the T-tag that was inserted close to the edgeof the perforation and tight tissue approximation. In thesecond case, clips applied to the everted edges of apartially suture-closed perforation slipped, resulting inleakage and fecal peritonitis. After learning from this expe-rience, we modified the closure technique; the T-tagswere placed slightly away from the edge of perforation,and the perforation edges were carefully aligned togetherand gently approximated without too much tension, andthere were no failures in the subsequent cases.
Colonoscopic perforation results in peritonitis in over90% of patients.4 This could be prevented by the immedi-ate endoscopic closure of perforation soon after its recog-nition, as shown in recent experimental studies, includinga placebo-controlled study.14,17 The current study demon-strates that endoscopic closure is as effective as surgery inthe prevention of peritonitis.
Although endoscopic closure prevents peritonitis, peri-tonitis (defined by the presence of peritoneal fibrinous de-posits on necropsydin this study on day 14) was observedin 30.4% and 21.7% of cases after endoscopic and surgicalclosure, respectively. Given the fact that none of these an-imals demonstrated clinical signs of peritonitis or distress,
www.giejournal.org
we doubt that this necropsy finding of peritoneal fibrinousdeposits is clinically relevant. There are no data in thesurgical literature on peritonitis after surgical closure ina porcine model to compare to our results. Because expe-rienced surgeons undertook the closures, we doubt thatpoor surgical closure is an explanation. Because the endo-scope was not cleaned with high-level disinfection aftersuctioning the liquid stools in the distal colon before cre-ation of a colon perforation, we suspect that bacterialtranslocation could be an explanation for low-level perito-neal inflammation. Although the distal 20 cm of coloncould be cleaned in the pigs to do this study, it is impos-sible to clear all the stools from the colon in these animals.At best, this model could be considered equivalent to thatseen in humans with perforation of the colon that is notfully cleaned out. It is clear that the outcome of colon per-foration in such patients is poor.4
Peritoneal adhesions develop in over 90% of the pa-tients following major abdominal surgery and can resultin small-bowel obstruction and infertility.26-28 About a thirdof the patients are readmitted to the hospital for adhe-sion-related problems after colorectal surgery.29 This clin-ical observation was clearly reproduced in the surgicalclosure group of the current study, in which more thanhalf of the animals developed abdominal wall adhesions.One could argue that leaving the peritoneum open in-stead of closing it accounts for such a high adhesionrate in our study; this issue remains controversial.30-32 Al-though laparoscopy has less risk of abdominal adhe-sions,33 laparotomy was chosen because of its wideacceptance by the surgeons throughout the world.
In contrast to the frequency of adhesions in the surgicalgroup, paucity of abdominal adhesions in three quartersof the animals in the endoscopic closure group is remark-ableda finding uniformly observed in our earlier
Volume 68, No. 2 : 2008 GASTROINTESTINAL ENDOSCOPY 329
Endoscopic closure of colon perforation Raju et al
Figure 4. A and B, Leak test at 2 weeks after endoscopic and surgical closure of colon perforation. No leaks were noted. C, Well-healed scars were
noted after endoscopic and surgical closure. D and E, Close-up mucosal and serosal views of the endoscopic closure reveal a healed scar with
T-tags at 2 weeks.
330 GASTROINTESTINAL ENDOSCOPY Volume 68, No. 2 : 2008 www.giejournal.org

Raju et al Endoscopic closure of colon perforation
studies.13-15,17 Endoluminal closure is associated with fewadhesions because it can be accomplished easily; there isno additional peritoneal trauma, either tissue dissectionor manipulation, to identify the perforation site comparedto laparotomy.
Although the rate of complications was equal in the en-doscopic and surgical closure groups, the type of complica-tions deferred-bowel obstruction was the predominantcomplication after surgery, whereas leakage and peritonitisor necrosis occurred after endoscopic closure. Further re-finements in endoscopic closure should be made to ensuresuccessful closure. In clinical practice, any deteriorationafter closure of perforation mandates emergent surgicalre-exploration and appropriate therapy. The incidence ofpostsurgical complications (15%)d3 with bowel obstruc-tion and 1 with perforation of the bladderdappears highin this animal study. Despite extensive search of the litera-ture, there are no prior data with which to compare.
Adjacent organ injury can occur during T-tag inser-tion.34 In the current study, inadvertent insertion of theT-tags into the adjacent viscera was observed in 5 of 186attempts (2.7%), resulting in bowel obstruction and mes-enteric vascular insufficiency in one case. Use of a modifiedtechnique of withdrawing the needle by 0.5 cm prior toT-tag deployment in our recent studies (instead of deploy-ing the T-tag immediately after puncture with a 1-cm nee-dle) has been encouraging.
A number of suturing methods are currently under inves-tigation.21,35-37 Compared to the suturing devices that requireremoving the endoscope from the operating field, loading itwith a suturing device, and reinserting the endoscope-sutur-ing device assembly through a conduit, the TAS can be in-serted through the endoscope channel easily. This allowsthe endoscopist to stay in the operating field, continually suc-tion the colonic contents, and prevent leakage.13,21,35-37
Although our experimental study design of immediateclosure of the colon perforation without any delay favoredsurgery by limiting the time for colonic leakage and peri-toneal contamination, the results of endoscopic closurewere comparable to surgical closure. Whether the encour-aging results observed in endoscopic closure of a healthydistal colon will hold up in the proximal colon with liquidstools, in the setting of colitis, or in the colon with extrin-sic adhesions requires further study.
In summary, this large multicenter randomized studydemonstrates that endoscopic closure is effective in clos-ing large perforations of the colon. If endoscopic closurecan be perfected to the point of avoiding any failuresand T-tag injury to adjacent viscera, this may serve as a ba-sis for future developments in endoluminal colon surgery.
DISCLOSURE
The following authors report that they have no disclo-sures relevant to this publication: I. Ahmed, G. Gomez,
www.giejournal.org
M. Winny. The following authors have disclosed actual orpotential conflicts: G. S. Raju, A. Fritscher-Ravens, R. I.Rothstein, P. Swain, A. Gelrud, Thomas Sonnanstine,M. Bergstrom, and P-O Park served as consultants toEthicon Endosurgery, Inc for this project and receivedresearch support for this study. A. Fritscher-Ravens andP. Swain hold patents on the insulated-tip knife. TheUniversity of Texas Medical Branch (UTMB) Experimen-tal Endoscopy Laboratory was supported by PentaxMedical, Inc. with endoscopy equipment. OlympusAmerica, Inc. provided the IT knives to UTMB for thestudy.
REFERENCES
1. Luning TH, Keemers-Gels ME, Barendregt WB, et al. Colonoscopic per-
forations: a review of 30,366 patients. Surg Endosc 2007;21:994-7.
2. Tulchinsky H, Madhala-Givon O, Wasserberg N, et al. Incidence and
management of colonoscopic perforations: 8 years’ experience. World
J Gastroenterol 2006;12:4211-3.
3. Levin TR, Zhao W, Conell C, et al. Complications of colonoscopy in an
integrated health care delivery system. Ann Intern Med 2006;145:
880-6.
4. Iqbal CW, Chun YS, Farley DR. Colonoscopic perforations: a retrospec-
tive review. J Gastrointest Surg 2005;9:1229-35, discussion 1236.
5. Misra T, Lalor E, Fedorak RN. Endoscopic perforation rates at a Ca-
nadian university teaching hospital. Can J Gastroenterol 2004;18:
221-6.
6. Cobb WS, Heniford BT, Sigmon LB, et al. Colonoscopic perforations: in-
cidence, management, and outcomes. Am Surg 2004;70:750-7, discus-
sion 757–8.
7. Viiala CH, Zimmerman M, Cullen DJ, et al. Complication rates of
colonoscopy in an Australian teaching hospital environment. Intern
Med J 2003;33:355-9.
8. Korman LY, Overholt BF, Box T, et al. Perforation during colonoscopy
in endoscopic ambulatory surgical centers. Gastrointest Endosc
2003;58:554-7.
9. Gatto NM, Frucht H, Sundararajan V, et al. Risk of perforation after
colonoscopy and sigmoidoscopy: a population-based study. J Natl
Cancer Inst 2003;95:230-6.
10. Ker TS, Wasserberg N, Beart RW Jr. Colonoscopic perforation and
bleeding of the colon can be treated safely without surgery. Am
Surg 2004;70:922-4.
11. Araghizadeh FY, Timmcke AE, Opelka FG, et al. Colonoscopic perfora-
tions. Dis Colon Rectum 2001;44:713-6.
12. Farley DR, Bannon MP, Zietlow SP, et al. Management of colonoscopic
perforations. Mayo Clin Proc 1997;72:729-33.
13. Raju GS, Shibukawa G, Ahmed I, et al. Endoluminal suturing may over-
come the limitations of clip closure of a gaping wide colon perforation
(with videos). Gastrointest Endosc 2007;65:906-11.
14. Raju GS, Pham B, Xiao SY, et al. A pilot study of endoscopic closure of
colonic perforations with endoclips in a swine model. Gastrointest
Endosc 2005;62:791-5.
15. Raju GS, Ahmed I, Xiao SY, et al. Controlled trial of immediate
endoluminal closure of colon perforations in a porcine model by
use of a novel clip device (with videos). Gastrointest Endosc
2006;64:989-97.
16. Raju GS, Ahmed I, Shibukawa G, et al. Endoluminal clip closure of
a circular full-thickness colon resection in a porcine model (with
videos). Gastrointest Endosc 2007;65:503-9.
17. Raju GS, Ahmed I, Brining D, et al. Endoluminal closure of large perfo-
rations of colon with clips in a porcine model (with video). Gastroint-
est Endosc 2006;64:640-6.
Volume 68, No. 2 : 2008 GASTROINTESTINAL ENDOSCOPY 331

Endoscopic closure of colon perforation Raju et al
18. Pai RD, Fong DG, Bundga ME, et al. Transcolonic endoscopic cholecys-
tectomy: a NOTES survival study in a porcine model (with video). Gas-
trointest Endosc 2006;64:428-34.
19. Fong DG, Pai RD, Thompson CC. Transcolonic endoscopic abdominal
exploration: a NOTES survival study in a porcine model. Gastrointest
Endosc 2007;65:312-8.
20. Park PO, Bergstrom M, Ikeda K, et al. Experimental studies of transgas-
tric gallbladder surgery: cholecystectomy and cholecystogastric anas-
tomosis (videos). Gastrointest Endosc 2005;61:601-6.
21. Bergstrom M, Ikeda K, Swain P, et al. Transgastric anastomosis by us-
ing flexible endoscopy in a porcine model (with video). Gastrointest
Endosc 2006;63:307-12.
22. Ikeda K, Fritscher-Ravens A, Mosse CA, et al. Endoscopic full-thickness
resection with sutured closure in a porcine model. Gastrointest Endosc
2005;62:122-9.
23. Raju GS, Rex DK, Kozarek RA, et al. A novel shape-locking guide for
prevention of sigmoid looping during colonoscopy. Gastrointest En-
dosc 2004;59:416-9.
24. Kyzer S, Bayer I, Turani H, et al. The influence of peritoneal closure on
formation of intraperitoneal adhesions: an experimental study. Int
J Tissue React 1986;8:355-9.
25. Tulandi T, Al-Jaroudi D. Nonclosure of peritoneum: a reappraisal. Am
J Obstet Gynecol 2003;189:609-12.
26. Liakakos T, Thomakos N, Fine PM, et al. Peritoneal adhesions: etiology,
pathophysiology, and clinical significance. Recent advances in preven-
tion and management. Dig Surg 2001;18:260-73.
27. Ellis H. Intraabdominal and postoperative peritoneal adhesions. J Am
Coll Surg 2005;200:641-4.
28. Holmdahl L. Making and covering of surgical footprints. Lancet
1999;353:1456-7.
29. Parker MC, Ellis H, Moran BJ, et al. Postoperative adhesions: ten-year
follow-up of 12,584 patients undergoing lower abdominal surgery.
Dis Colon Rectum 2001;44:822-9, discussion 829–30.
30. Duffy DM, diZerega GS. Is peritoneal closure necessary? Obstet Gyne-
col Surv 1994;49:817-22.
31. Cheong YC, Bajekal N, Li TC. Peritoneal closuredto close or not to
close. Hum Reprod 2001;16:1548-52.
32. Zareian Z, Zareian P. Non-closure versus closure of peritoneum during
cesarean section: a randomized study. Eur J Obstet Gynecol Reprod
Biol 2006;128:267-9.
332 GASTROINTESTINAL ENDOSCOPY Volume 68, No. 2 : 2008
33. Hansen AJ, Tessier DJ, Anderson ML, et al. Laparoscopic repair of co-
lonoscopic perforations: indications and guidelines. J Gastrointest
Surg 2007;11:655-9.
34. Sumiyama K, Gostout CJ, Rajan E, et al. Transgastric cholecystectomy:
transgastric accessibility to the gallbladder improved with the SEMF
method and a novel multibending therapeutic endoscope. Gastroint-
est Endosc 2007;65:1028-34.
35. Pham BV, Raju GS, Ahmed I, et al. Immediate endoscopic closure of
colon perforation by using a prototype endoscopic suturing device:
feasibility and outcome in a porcine model (with video). Gastrointest
Endosc 2006;64:113-9.
36. Fritscher-Ravens A, Mosse CA, Mills TN, et al. A through-the-scope de-
vice for suturing and tissue approximation under EUS control. Gastro-
intest Endosc 2002;56:737-42.
37. Sclabas GM, Swain P, Swanstrom LL. Endoluminal methods for gastro-
tomy closure in natural orifice transenteric surgery (NOTES). Surg In-
nov 2006;13:23-30.
Received December 5, 2007. Accepted March 3, 2008.
Current affiliations: Department of Medicine and Surgery (G.S.R., I.A., G.G.),
University of Texas Medical Branch, Galveston, Texas, USA; Department of
Medicine (A.F-R.), Homerton University Hospital, London, United
Kingdom; Department of Medicine (R.I.R.), Dartmouth-Hitchcock Medical
Center, Lebanon, New Hampshire, USA; Department of Medicine (P.S.),
Royal London Hospital, London, United Kingdom; Department of
Medicine (A.G.), University of Cincinnati Medical Center, Cincinnati, Ohio,
USA; Department of Surgery (M.K.), Hannover Medical School, Hannover,
Germany; Tristate Surgical Weight Loss Center (T.S.), St. Luke Hospitals,
Florence, Kentucky, USA; Department of Surgery (M.B., P-O.P.),
Sahlgrenska University Hospital, Goteborg, Sweden.
Presented at the Presidential Plenary Session of ASGE, Digestive Disease
Week 2007, May 20-23, 2007, Washington, DC (Gastrointest Endosc
2007;65:AB128).
Reprint requests: G.S. Raju, MD, Center for Endoscopic Research, Training,
and Innovation (CERTAIN), 4.106 McCullough Building, 301 University
Blvd, University of Texas Medical Branch, Galveston, TX 77555.
www.giejournal.org






















![[I Brazilian consensus of endoscopic ultrasonography]](https://img.dokumen.tips/doc/110x75/634ac5bce2b881b8bf0189bc/i-brazilian-consensus-of-endoscopic-ultrasonography.jpg)






