Embed Size (px)
Citation preview

International Journul of Cardioloa, 22 (1989) 329-338
Elsevier
329
IJC 00818
Immunosuppressive treatment in myocarditis
A. Salvi, A. Di Lenarda, L. Dreas, F. Silvestri ’ and F. Camerini
Department of Cardlologv und of ’ Patholoy,,. Ospedule Mcrggiore and University of Trieste, Trleste, Itu(l
(Received 15 June 1988; revision accepted 22 August 1988)
Salvi A, Di Lenarda A, Dreas L, Silvestri F, Camerini F. Immunosuppressive treatment in myocarditis. Int J Cardiol 1989;22:3299338.
Twenty patients (13 males and seven females) with a biopsy-proven diagnosis of myocarditis underwent a period of treatment with prednisone and azathioprine. The primary objective of the study was the
observation of histologic changes which occur during treatment and after treatment withdrawal. The
secondary objective was the detection, if any, of changes in left ventricular ejection fraction. Multiple endomyocardial biopsies were obtained and the treatment was adjusted in order to achieve complete
disappearance of the myocardial inflammation. The histologic status was improved in all patients, although complete disappearance of the signs of active disease was seen in 15 patients only. Two patients died during
the observation period. A clear relationship between histologic status and immunosuppression was estab- lished in some patients (50% of all cases showed a worsening after withdrawal from the treatment). An
overall improvement of the ejection fraction was observed (from 0.37 k 0.14 to 0.46 k 0.17), but a direct effect of the treatment on the recovery of ventricular function cannot be stated. In some patients, however, a direct relationship between the histological changes and the changes in ejection fraction was seen. These
data suggest that treatment with prednisone and azathioprine may be beneficial in some patients with biopsy-proven myocarditis and depressed ventricular function.
Key words: Endomyocardial biopsy; Myocarditis: Immunosuppression
Introduction
Myocarditis is clinically suspected when con- gestive heart failure, atrioventricular block, or ventricular arrhythmias develop rapidly in a previ- ously normal subject, particularly, after a viral illness [l-3].
Various non-invasive diagnostic tests may help in the clinical diagnosis [4-71 but only since the
Correspondence to: A. S&i. Department of Cardiology,
Ospedale Maggiore. Piazza Ospedale 1, 34129 Trieste, Italy.
Presented as a Communication at the international Sym-
posium “New Concepts in Viral Heart Disease”. Munich, 25-28 May. 1988.
technique of endomyocardial biopsy has become available [8], it is possible to obtain histologic confirmation of the disease in vivo.
The similarity between the histologic picture in acute myocarditis and that seen in acute cardiac rejection suggested that immunosuppression might benefit both conditions. and some authors have already reported their observations [9-131. A be- neficial effect of immunosuppression in acute myocarditis is, however, still unproven. The aim of our study was to evaluate the effect of immuno- suppressive treatment with prednisone and azathioprine on both histology and left ventricular function in 20 patients with biopsy-proven acute myocarditis.
0167.5273/89/$03.50 li’ 1989 Elsewer Science Publishers B.V. (Biomedical Division)

330
Patients
Up to January 1988. endomyocardial biopsy was performed in 420 patients admitted to our institution for the investigation of a suspected myocardial disease. Myocarditis was diagnosed histologically in 38 patients. Twenty patients in whom the diagnosis was made within the last four years. and who entered a protocol on the effects of immunosuppressive treatment in myocarditis of unknown etiology, are the basis of this study. This group consists of 13 males and 7 females with an age range of 16-66 years (mean 33.6).
Clinical picture
The clinical presentation was congestive heart failure in 16 patients, persistent atria1 tachycardia and ventricular premature complexes in two and typical angina pectoris at rest in two others.
A history compatible with a viral illness in the preceding four months was found in nine patients. In four patients the illness was diagnosed within two months after delivery. Seventeen patients had the histologic diagnosis made within five months of clinical presentation (mean 2.2 months, range O-5).
Seventeen patients showed a depressed (less than 0.50) left ventricular ejection fraction at diag- nosis. Two patients with a history of angina and one with a history of atria1 tachycardia had nor- mal or minimally depressed ejection fraction (nor- mal values for ejection fraction in our laboratory are 0.67 f 0.09). Selective coronary arteriography. in order to exclude coronary artery disease was performed in all patients over 25 years of age, except in two women aged 34 years who presented with congestive heart failure. Both coronary arteries were opacified during aortography in the three youngest patients.
Methods
Endomyocardial biopsy
Four or five samples of tissue were obtained from the right or the left ventricle with a King’s
endomyocardial bioptome [14] or the Cordis adap- tation of this instrument [15] and immediately fixed in 10% buffered formalin. Multiple 5 pm thick sections were made, stained with haema- toxylin eosin. Masson’s trichrome and Weigertt Van Gieson and examined by light microscopy.
Histologic classification
The methods suggested by a panel of patholo- gists who met at Dallas in 1984 [16] were used for the diagnosis of myocarditis. All cases were retro- spectively examined and the diagnosis was accepted when two different observers agreed. Subsequent biopsies were classified according to the above mentioned paper.
Immunosuppressive treatment protocol
Immunosuppressive treatment consisted of oral azathioprine, 75 mg per square metre per day for at least six months (unless the white blood cells count fell below 4000/mm7) and oral prednisone 50 mg per square metre per day for two weeks. then tapered until withdrawal of the drug after at least six months of treatment. In patients admitted to the study after June 1985, the prednisone dose of 0.3 mg per kilogram per day. when reached, was maintained for approximately four months. In the event of persistent active myocarditis during treatment or reactivation after interruption, the prednisone dosage was increased either to the initial dose or to the one previously demonstrated effective.
In all patients. the interval between the onset of symptoms and the beginning of treatment was at least one month.
The usual means of treatment of congestive heart failure. arrhythmias, diabetes and hyperten- sion were continued in addition to the immuno- suppression.
Treatment with digoxin. diuretics. vasodilators and amiodarone, when already present. was con- tinued. In seven patients, metoprolol 50-700 mg per day was added during the period of observa- tion for either persistent sinus tachycardia at rest (five cases) or hypertension (two cases).
331
Patients’ assessment Results
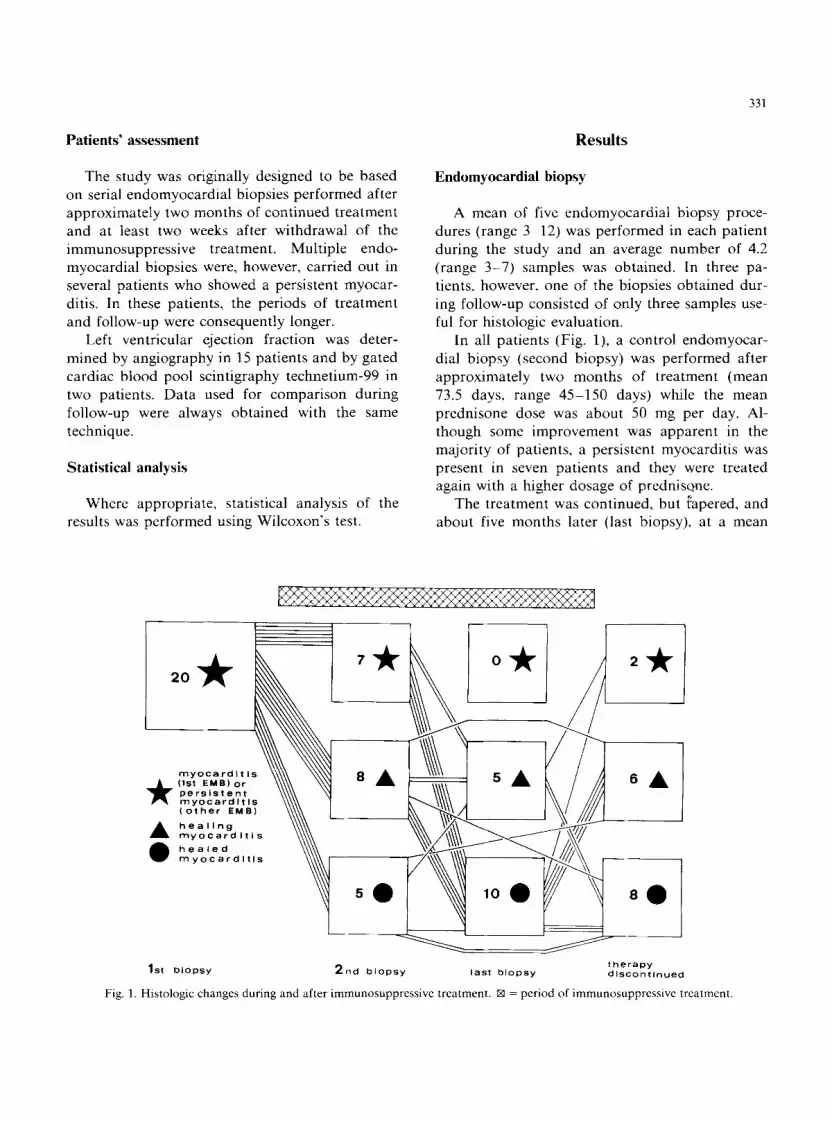
The study was originally designed to be based on serial endomyocardial biopsies performed after approximately two months of continued treatment and at least two weeks after withdrawal of the immunosuppressive treatment. Multiple endo- myocardial biopsies were, however, carried out in several patients who showed a persistent myocar- ditis. In these patients, the periods of treatment and follow-up were consequently longer.
Endomyocardial biopsy
A mean of five endomyocardial biopsy proce- dures (range 3312) was performed in each patient during the study and an average number of 4.2 (range 3-7) samples was obtained. In three pa- tients, however, one of the biopsies obtained dur- ing follow-up consisted of only three samples use- ful for histologic evaluation.
Left ventricular ejection fraction was deter-
mined by angiography in 15 patients and by gated cardiac blood pool scintigraphy technetium-99 in two patients. Data used for comparison during follow-up were always obtained with the same technique.
Statistical analysis
In all patients (Fig. l), a control endomyocar- dial biopsy (second biopsy) was performed after approximately two months of treatment (mean 73.5 days, range 45-150 days) while the mean prednisone dose was about 50 mg per day. Al- though some improvement was apparent in the majority of patients, a persistent myocarditis was present in seven patients and they were treated again with a higher dosage of prednisone.
Where appropriate, statistical analysis of the results was performed using Wilcoxon’s test.
The treatment was continued, but fapered, and about five months later (last biopsy), at a mean
myocardl t Is (1st EMB) or persistent myocardltls (other EMB)
A healing myocardltls healed myocardltls
1 st biopsy 2nd biopsy last biopsy therapy dlSConflnued
Fig. 1. Histologic changes during and after immunosuppressive treatment. IXI = period of immunosuppressive treatment.

332
lzF% 45: 40-
35-
30-
25-
20-
Fig. 2. Changes of histology and ejection fraction and relationship with the immunohupprsssive treatment in one patient. *. A. and l as in Fig. 1.
1 St 2nd dlscontinuatlon dlscontlnuatlon of therapy of therapy
mean 300 days maan 502 days
3 rd dlscontlnuatlon Of therapy
mean 795 days
Fig. 3. Histologic changes during and after Immunosuppressive treatment in seven patients who needed reinstitution of therapy after first discontinuation (one died before being rebiopsied). *, A. 0 and IXI as in Fig. 1.
prednisone dose of 25 mg per day. the results were definitely better and all patients examined showed a clear reduction of the histologic signs of activity. It has to be noted. however. that data for compari- son were available in 15 patients only. Four pa- tients with healing or healed myocarditis after two months of therapy reduced the drug dosages as scheduled but refused a subsequent biopsy during maintainance. In one patient, the treatment was stopped after four months when he presented with appendicitis complicated by peritonitis.
In 16 patients. the histologic status was reas- sessed two weeks after withdrawal of treatment and about nine months (mean 285 days, range 120-510 days) after entry into the study (Fig. 1). One patient died before being restudied and three refused further invasive investigations. A worsen- ing of histology was seen in about 50% of the patients who had improved during treatment and two showed a severe reactivation. All were treated at doses previously demonstrated effective or even
EM 70
50 ! 40
30
20
333
higher, except one who died shortly after. The treatment, very prolonged in some patients (Fig. 2) was eventually associated with histology of healing or healed myocarditis (Fig. 3).
Left ventricular ejection fraction
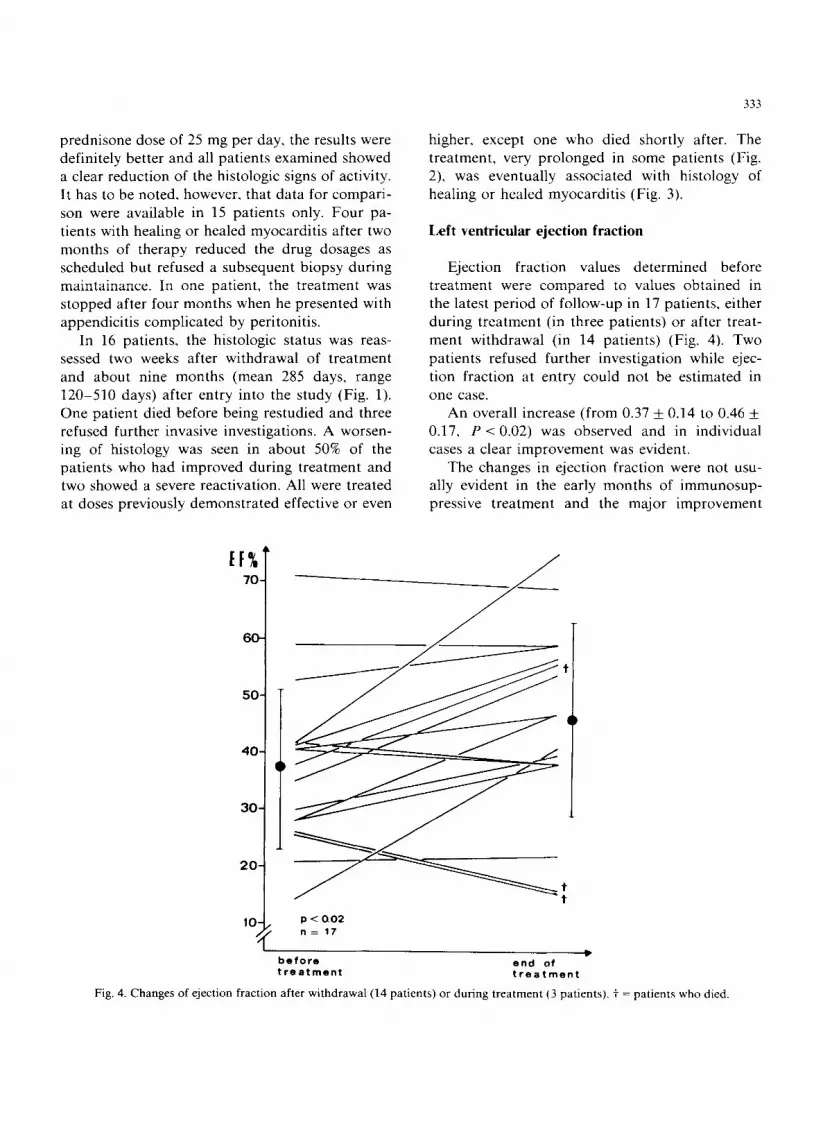
Ejection fraction values determined before treatment were compared to values obtained in the latest period of follow-up in 17 patients, either during treatment (in three patients) or after treat- ment withdrawal (in 14 patients) (Fig. 4). Two patients refused further investigation while ejec- tion fraction at entry could not be estimated in one case.
An overall increase (from 0.37 k 0.14 to 0.46 + 0.17, P < 0.02) was observed and in individual cases a clear improvement was evident.
The changes in ejection fraction were not usu- ally evident in the early months of immunosup- pressive treatment and the major improvement
/
p -z 0.02
before I
end of treatment treatment
Fig. 4. Changes of ejection fraction after withdrawal (14 patients) or during treatment (3 patients). t = patients who died.

334
Fig. 5 Changes of
60
SO.
40
30.
20.
10 4 n= 17
0 3 6 9 12 15 18 21 24 27 months
ejection fraction during prolonged period of immunosuppressive treatment in seventeen patients.
died.
was often observed after several months of con- tinuous treatment or sometimes after several un- successful attempts of treatment withdrawal (Figs.
2, 5).
Immunosuppressive treatment and side effects
All patients became clinically “cushingoid” with the doses of prednisone employed. Two of the oldest patients developed hypertension which re- quired treatment with metoprolol and captopril and in one of them insulin was given to control a previously unknown diabetes mellitus. In the same case, suboptimal doses of azathioprine were used due to recurrent leukopenia. The same patient developed, after two years of treatment, oral candidiasis and epididymitis, which were con- trolled with short courses of topical mycostatin and oral tetracyclin. In one patient, the treatment was stopped after four months with the onset of an acute peritonitis as a complication of a previ- ously known chronic appendicitis which perfo-
i= patients who
rated. Interestingly, he had normal white blood cell counts during the period of treatment which raised, with normal differentials, during the acute infection. He was surgically treated and made an uneventful recovery. Immunosuppression was not restarted because myocarditis was demonstrated to be completely healed by endomyocardial biopsy one year later.
Mortality
Two patients died. Both had low ejection frac- tion which deteriorated slowly during the observa- tion period (in both from 0.26 to 0.16). Another patient died after the end of treatment for non- cardiac causes (cerebral haemorrhage during anti- coagulant treatment).
Discussion
Myocarditis is defined “as a process char- acterized by an inflammatory infiltrate of the

myocardium with necrosis and/or degeneration of adjacent myocytes not typical of the ischemic damage associated with coronary artery disease”
P61. Although different organisms (bacteria, viruses,
rickettsia, fungi, parasites) may cause the disease. in most cases a viral etiology is generally sus- pected [17,18].
The clinical diagnosis of myocarditis is often difficult and sometimes impossible. The disease may be suspected when congestive heart failure, ventricular arrhythmias or atrioventricular block [l-3,19.20] develop rapidly in a previously normal subject. Another. although rare, presentation is that of acute myocardial infarction in a young patient, particularly, after a viral illness [21].
It has been claimed that different noninvasive diagnostic tests [4,7] may help or even confirm [5,6] the clinical suspect. However. it is possible to obtain histologic confirmation of the disease in vivo, only since the technique of endomyocardial biopsy has become available [S].
Efforts aimed at the identification of viruses in the myocardium of patients with myocarditis al- most invariably failed [22,23]. This is at variance
335
with the evidence for a viral implication in up to 40% of cases of myocarditis and pericarditis [17] and with the finding of rising serum titres for coxsackie B virus neutralizing antibodies in up to 50% of patients with biopsy proven myocarditis [12]. The concept of an immune-mediated damage, after viral infection, based on the experimental work of Wilson [24] and Woodruff and Woodruff [25] was therefore suggested also in the pathogene- sis of human myocarditis.
From this concept and from the observation that a similarity exists between the histologic aspect of myocarditis and that of cardiac allograft rejection. in which immunosuppressive drugs are beneficial, comes the rationale for this form of treatment.
After the initial report of the Stanford group [9] several other authors published their results in the treatment of myocarditis with immunosuppres- sives [lo-13,26,27].
Different histologic criteria for the diagnosis of myocarditis were, however, used and great caution should be exercised when interpreting the results. The need for a more uniform diagnostic and clas- sification system was therefore felt.
Fig. 6. Endomyocardial biopsy (haematoxylin and eosin, original magnification X 100). Diffuse mononuclear - cells infiltrate with
loss and necrosis of myocytes.

336
Fig. 7. Endomyocardial biopsy (haematoxylin and eosin, original magnification x 100). Diffuse mononuclear - cells infiltrate closely applied to the sarcolemma with irregular cellular outlines and necroslr of myocytes.
A Multi Centre Myocarditis Trial, based on uniform and strict histologic criteria, known as the Dallas criteria [16], was therefore designed [28] in order to clarify the role of immunosuppression in myocarditis, not convincingly defined by the ini- tial experiences. Until the results of this trial are available, it may be useful to report our observa- tions.
All patients included in this study showed on their initial endomyocardial biopsy “both an in- flammatory infiltrate and damage of the adjacent myocytes . . in the form of frank necrosis (Fig. 6) myocyte vacuolization, irregular cellular outlines or cellular disruption with lymphocytes closely applied to the sarcolemma” (Fig. 7) [16].
After a retrospective analysis of cases initially reported [29], two patients were excluded due to the fact that the histologic findings were consid- ered insufficient for a definite diagnosis of active myocarditis.
During follow-up, myocarditis was classified as persistent, healing or healed [16]. The study was primarily designed to follow the histologic changes during and after an immunosuppressive treatment with prednisone and azathioprine and to observe
if any change in left ventricular ejection fraction takes place during follow-up.
Six months was the originally planned duration of treatment, but the histologic response led to adjustments in dosage and duration of immuno- suppression. Most patients had a period of follow- up longer than six months and some were treated for as long as two years.
An important limitation is that it cannot be stated whether the observed changes were sec- ondary to the immunosuppression or spontaneous. This problem could be probably solved by the randomized study which is presently in progress [28,30]. The behaviour of individual patients (Fig. 2) and the fact that 50% of patients who healed histologically during therapy showed a worsening after interruption of the treatment (Fig. 1). how- ever, suggests a direct link between immunosup- pressive drug regimen and the histologic findings observed.
These data suggest also that treatment should not be carried out according to rigid protocols but rather modulated according to histology. After two months of high continuous prednisone ther- apy, one-third of the cases was still unchanged. It

may be noted also that at the second control biopsy, performed during a low prednisone dose after approximately seven months of treatment, none of the patients showed signs of persistent myocarditis. A benefit related to a prolonged period of treatment at low maintainance doses as in other immuno-mediated disease [31] is therefore
postulated. Most previous reports on immunosuppression
in myocarditis did not provide an objective and reliable evaluation of ventricular function in all
patients [9-11,271. In the study of Hosenpud et al.
]131, who did not observe any improvement, ventricular function was assessed by right heart catheterization and M-mode echo data, but Daly et al. [12] provided evidence for an improvement of ventriculographic ejection fraction after treat- ment. Whether this improvement is secondary to the treatment is, however, still undefined, because Kawamura et al. [32] have shown that 38% of patients with biopsy-proven myocarditis improve spontaneously and because other authors [26] have also noted a spontaneous improvement of ejection fraction in patients in whom myocarditis, al- though unequivocally diagnosed, was not treated with immunosuppression.
An overall significant improvement of ejection fraction was observed in our patients. Interest- ingly, this was more evident in cases treated for longer periods, because of frequent reactivation of myocarditis (Fig. 5). The behaviour of individual cases (Fig. 2) may suggest a direct effect of the immunosuppression both on histologic healing, and on recovery of ventricular function. This is in accordance with some other observations of Ma- son et al. [9], Daly et al. 1121 and Dee et al. [26] and suggests that there is a subset of patients who improve as a result of the immunosuppression and show a relapse when the drugs are reduced or discontinued.
One limitation of this study is that it was not conceived as a controlled trial, although the need for a randomized study to assess this form of treatment had already been suggested [12].
Another potential limitation is that the autoim- mune pathogenesis of human myocarditis has be- come less convincing after the experimental work of Bowles et al. [33]. These authors [33] were able
In conclusion, (1) Immunosuppressive treatment is usually associated with a reduction of histologic signs of active myocarditis. (2) Reduction or inter- ruption of treatment is often associated with a worsening histology (and sometimes with a de- terioration of left ventricular function). (3) Im- munosuppressive treatment is associated, in a sub- group of patients, with an improvement of left ventricular function. (4) The improvement of left
ventricular function may appear late. (5) The rela- tionship between the treatment and the improve- ment in histology and in ventricular function and the possible deterioration after withdrawal (ob- served also by other authors) [9,12,26] suggest that immunosuppressive therapy may be useful at least in a subset of patients with active myocarditis.
References
Take M. Sekiguchi M, Hiroe M. Hirosawa K. Early clinical profiles of cases with histopathologically proven acute idio-
pathic myocarditis and a proposal for diagnostic criteria.
Jpn Circul J 1981:45:1415-1420.
Onouchi Z, Haba S, Kiyosawa N, Shimazu S, Hamaoka K.
Kusunoki T. Stokes-Adams attacks due to acute non-
specific myocarditis in childhood. Jpn Heart J 1980:21:
307-315.
Kitahura Y. Morita H. Virus myocarditis and cardiomyo- pathy. Jpn Circul J 1979;43:1017-1031.
Hauser AM. Gordon S, Cieszkowski J, Timmis GC. Severe
transient left ventricular “ hypertrophy” occurring during acute myocarditis. Chest 1983;83:275-277.
O’Connell JB. Henkin RE, Fowles RE. Modes of detection
337
to detect coxsackie B virus specific RNA in myocardial tissue of patients with myocarditis even in their late, healed stage and this may imply continuing virus replication in the myocardial cells. Should this observation be confirmed, the ration- ale for the use of an immunosuppressive treatment in human myocarditis should be redefined.
Finally, it has to be mentioned that, although the traditional measures of treatment were main- tained constant during the period of study, beta- blockers were added in seven patients. This form of therapy may have a potential beneficial effect in patients with depressed ventricular function secondary to dilated cardiomyopathy [34,35]. We cannot define whether the complex effects induced by beta-blockade [36-381 benefitted also our group of patients with myocarditis.

338
6
I
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
of inflammation in the cardiomyopathic heart. In: Robin-
son JA. O’Connell JB. eds. Myocarditis: precursor of
cardiomyopathy. Toronto: Collamore Press, 1983;109%127.
Yasuda T. Palacios IF. Dee GW, et al. lndium lll-mono-
clonal antimyosin antibody imaging in the diagnosis of
acute myocarditis. Circulation 1987:76:306311.
Chandraratna PAN, Nimalasuriya A, Reid CR, Cohn S,
Rahimtoola SH. Left ventricular asynergy in acute
myocarditis: simulation of acute myocardial infarction. J
Am Med Assoc 1983;250:1428-1430.
Sakakibara S. Konno S. Endomyocardial biopsy. Jpn Heart
J 1962;3:537-543.
Mason JW, Billingham ME. Ricci DR. Treatment of acute
inflammatory myocarditis assisted by endomyocardial
biopsy. Am J Cardiol 1980:45:1037-1044.
Zee-Cheng C-S, Tsai CC, Palmer DC, Codd JE. Pennington
DG, Williams GA. High incidence of myocarditis by endo-
myocardial biopsy in patients with idiopathic congestive
cardiomyopathy. J Am Co11 Cardiol 1984;3:63-70.
Edwards WD. Holmes DR, Reeder GS. Diagnosis of active
lymphocytic myocarditis by endomyocardial biopsy:
quantitative criteria for light microscopy. Mayo Clin Proc
1982:57:419-425.
Daly K. Richardson PJ. Olsen EGJ, et al. Acute myocardi-
tis: role of histological and virological examination in the
diagnosis and assessment of immunosuppressive treatment.
Br Heart J 1984;51:30-35.
Hosenpud JD, McAnulty JH, Niles NR. Lack of objective
improvement in ventricular systolic function in patients with myocarditis treated with azathioprine and prednisone.
J Am Co11 Cardiol 1985:6:797-801.
Richardson PJ. King’s endomyocardial bioptome. Lancet
1974: i:660-661.
Richardson PJ. Endomyocardial biopsy: technique and
evaluation of a new disposable forceps and catheter sheath
system. In: Bolte HD. ed. Viral heart disease. Berlin:
Springer, 1984:173-176.
Aretz HT, Billingham ME, Edwards WD, et al. Myocardi-
tis: a histopathologic definition and classification. Am J
Cardiovasc Path01 1986;1:3-14.
Grist NR, Bell EJ. A six year study of Coxsackievirus B
infections in heart disease. J Hyg 1974:73:165-172.
Richardson PJ. Immunosuppressive therapy in the manage-
ment of biopsy proven acute myocarditis. Hera 1985;lO:
36-43.
Vignola PA, Aonuma K. Swaye PS. et al. Lymphocytic
myocarditis presenting as unexplained ventricular arrhyth-
mias: diagnosis with endomyocardial biopsy and response to immunosuppression. J Am Co11 Cardiol 1984;4:812-819.
Salvi A, Della Grazia E, Silvestri F, Camerini F. Acute
rickettsial myocarditis and advanced atrioventricular block: diagnosis and treatment aided by endomyocardial biopsy.
Int J Cardiol 1985;7:405-409.
Costanzo-Nordin MR. O’Connell JB. Subramanian R.
Robinson JA, Scanlon PJ. Myocarditis confirmed by biop-
sy presenting as acute myocardial infarction. Br Heart J
1985;53:25529.
Lowry PJ. Edwards CW. Nagle RE. Herpes-like virus par-
ticles in myocardium of patient progressing to congestive
cardiomyopathy. Br Heart J 1982;48:501-503.
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
Engblom E, Ekfors TO, Meurman OH. Toivanen A.
Nikoskelainen J. Fatal influenza A myocarditis with isola-
tion of virus from the myocardium. Acta Med Stand
1983;213:75-78.
Wilson FM. Miranda QR. Chason JL. Lerner AM. Resid-
ual pathologic changes following murine coxsackie A and B
myocarditis. Am J Path01 1969:55:253-265.
Woodruff JF. Woodruff JJ. Involvement of T lymphocytes in the pathogenesis of coxsackie virus B heart disease. J
lmmunol 1974;113:1726-1734. Dee GW. Palacios IF. Fallon JT. et al. Active myocarditis
in the spectrum of acute dilated cardiomyopathies: clinical
features. histologic correlates. and clinical outcome. N Engl
J Med 1985:312:8X5-890.
Fenoglio JJ, Ursell PC, Kellogg CF. Drusin RE, Weiss MB.
Diagnosis and classification of myocarditis by endomyocar-
dial biopsy. New Engl J Med 1983;308:12-18.
Mason JW. Endomyocardial biopsy: the balance of success
and failure. Circulation 1985;71:185-188.
Salvi A, Hrovatin E, Dreas L, Silvestri F. Camerini F.
Changes in histology and left ventricular ejection fraction
during immunosuppressive treatment in active myocarditis.
Eur Heart J 1987~8 (suppl):267-269.
Anderson JL. Fowles RE. Unverferth DV. Mason JW
Immunosuppressive therapy of myocardial inflammatory disease. Initial experience and future trials to define indica-
tion for therapy. Em Heart J 1987:8(suppl):263-266.
Hahn BH. Systemic lupus erythematosus. In: Braunwald E,
Isselbacher KJ. Petersdorf RG, Wilson JD, Martin JB.
Fauci AS. eds. Harrison’s principles of internal medicine.
New York: McGraw-Hill. 1987:1418-1423.
Kawamura K. Kitaura Y. Morita H, Deguchi H, Kotaka
M. Viral and idiopathic myocarditis in Japan: a question-
naire survey. In: Sekiguchi M, Olsen EGJ, Goodwin JF.
eds. Myocarditis and related disorders. Tokyo: Springer-
Verlag. 1985:18%22.
Bowles NE, Olsen EGJ. Richardson PJ. Archard LC. De-
tection of Coxsackie-B-virus specific RNA sequences in
myocardial biopsy samples from patients with myocarditis
and dilated cardiomyopathy. Lancet 1986: i: 1120-l 122.
Waagstein F, Hjalmarson A. Swedberg K. Wallentin I.
Beta-blockers in dilated cardiomyopathies: they work. Eur
Heart J. 1983;4 (suppl. A):173-178.
Engelmaier RS, O’Connel JB, Walsh R. Rad N. Scanlon PJ.
Gunnar RM. Improvement in symptoms and exercise toler-
ance by metoprolol in patients with dilated cardiomyopa-
thy: a double blind randomized, placebo controlled trial.
Circulation 1985:72:536-546. Fowler MB. Bristow MR. Laser JA, Ginsburg R, Scott LB.
Schroeder JS. Beta blocker therapy in severe heart failure:
improvement related to beta I-adrenergic receptor up-regu- lation? Circulation 1984;70: II-1 12.
Waagstein F. Hjalmarson A, Varnauskas E. Wallentin I.
Effect of chronic beta-adrenergic receptor blockade in con
gestive cardiomyopathy. Br Heart J 1975;37:1022-1036.
Alderman J. Grossman W. Are beta-adrenergic blocking
drugs useful in the treatment of dilated cardiomyopathy?
Circulation 1985;71:854-857.





























