Embed Size (px)
Citation preview

Immunosuppressive therapy in adults with aplasticanaemia: single-institution experience from IndiaVelu Nair, Ajay Sharma, Satyaranjan Das, Vishal Sondhi, Sanjeevan Sharma
Department of Hematology andBone Marrow Transplantation,Army Hospital (Research andReferral Centre), New Delhi,India
Correspondence toDr Velu Nair, Department ofMedicine, Armed ForcesMedical College, Pune,Maharashtra 411040, India;[email protected],[email protected]
Received 14 November 2011Revised 26 March 2013Accepted 16 April 2013
To cite: Nair V, Sharma A,Das S, et al. Postgrad Med JPublished Online First:[please include Day MonthYear] doi:10.1136/postgradmedj-2011-130605
ABSTRACTObjective To determine overall survival and factorspredicting survival after immunosuppressive therapy inpatients with acquired aplastic anaemia.Design Retrospective.Setting Tertiary care hospital.Patients 120 adults diagnosed as having acquiredaplastic anaemia between 1 January 1996 and31 December 2009.Interventions Anti-thymocyte globulin (ATG) followedby ciclosporin was administered to all patients for15–18 months as the initial treatment. Haematologicalresponse was assessed 6 months after ATGadministration and 6-monthly thereafter. Platelets weretransfused if levels were <10 ! 103/l and forsymptomatic bleeding. Transfusions of red blood cellswere given for haemoglobin levels <70 g/l orsymptomatic anaemia. Febrile neutropenia was managedwith antibiotics, with the addition of antifungal agentsafter 3–4 days of unresponsive fever. Granulocytecolony-stimulating factor was administered at a dose of5 mg/kg/day (maximum 300 mg/day) subcutaneously forinfective episodes.Main outcome measures Primary outcome: overallsurvival. Secondary outcome: response toimmunosuppressive therapy, failure-free survival, relapseand clonal evolutions. The response and relapse criteriawere defined in accordance with the British Council forStandards in Haematology guidelines.Results Overall response at 6 months after initiation oftreatment was 85.8% (103/120). Overall survival at76 months was 83.4%. Overall survival correlated withpresence of response (complete response or partialresponse) at 6 months after ATG administration(HR=0.021, 95% CI 0.006 to 0.079, p<0.001). Theoccurrence of infectious complications adversely affectedthe overall survival (HR=5.71, 95% CI 1.22 to 26.77,p=0.027). Six patients relapsed. There were no deaths oradverse events 12 months after treatment amongresponders.Conclusions In our study, overall survival was 83.4%at a median follow-up of 76 months. The two variablesthat significantly affected overall survival were responseto therapy at 6 months and occurrence of infectiouscomplications.
INTRODUCTIONAplastic anaemia (AA) is an immune mediated dis-order characterised by peripheral blood pancyto-penia with a hypocellular bone marrow.1 This bonemarrow failure mostly results from T-cell mediateddestruction of bone marrow haematopoietic stemcells.2 3 Allogeneic haematopoietic stem cell trans-plantation (allo-HSCT) replaces these stem cells.The current techniques for allo-HSCT produce a
high cure rate.4 However, only a minority ofpatients have a matched related donor for thismodality of treatment, and matched unrelateddonor HSCT is still associated with high morbidityand mortality.5
The observation of recovery after failed bonemarrow transplant led to the treatment of AA withimmunosuppressive therapy (IST) alone.6 Improvedsurvival was noted with the use of combination ISTintegrating anti-thymocyte globulin (ATG), whichlyses the lymphocytes, and ciclosporin A (CsA),which blocks the T-cell function.6–8 However, ISThas been labelled ‘an imperfect treatment’ whichonly ‘postpones the inevitable’.6 9 About one-thirdof patients have failed to respond 3 months afterinitiation of IST, and even those who respond areat a risk of relapse and secondary clonal disordersover the next 5–10 years.6
Most of the work investigating the use of IST hasbeen carried out in developed nations. There is apaucity of data from developing countries in thiscontext, and the limited literature suggests an inferiorresult to that in developed countries.10 This may bepartly due to a different healthcare set up withlimited resources and possibly to genetic heterogen-eity across different ethnic groups. In addition, theadministration of granulocyte colony-stimulatingfactor (G-CSF) in AA is debatable. While manycentres continue to use G-CSF, others tend to avoid ituntil the position becomes clearer.11 12
The delivery of healthcare in the public andprivate sector in India is extremely heterogeneous.This heterogeneity leads to different levels ofhealthcare related to cost. In addition, the standardof supportive care affects the outcome, especially inthe first 6 months after IST, which is by no meansuniform in India and is often dictated by the costand affordability by the patient.In view of the sparse and heterogeneous data from
the sub-continent, this study was undertaken toevaluate the overall survival (OS) of adult patientsdiagnosed with acquired AA and treated with IST,from 1 January 1996 to 31 December 2009. It wasconducted at a tertiary care armed forces hospital inIndia where the treatment was provided free of costand in accordance with standard guidelines across allsocioeconomic groups. The patients were adminis-tered IST in accordance with the British Council forStandards in Haematology guidelines after theirconsent had been obtained.1 The study was approvedby the institutional ethics committee. Patients wereassessed at 6 months after ATG administration forhaematological response. Thereafter, they wereassessed 6 monthly with a complete blood count.Medical records were scrutinised, and data on IST(ATG and CsA) and supportive therapy (antibiotics,
Nair V, et al. Postgrad Med J 2013;0:1–8. doi:10.1136/postgradmedj-2011-130605 1
Original article PGMJ Online First, published on May 18, 2013 as 10.1136/postgradmedj-2011-130605
Copyright Article author (or their employer) 2013. Produced by BMJ Publishing Group Ltd under licence.
group.bmj.com on May 24, 2013 - Published by pmj.bmj.comDownloaded from

transfusions and G-CSF) were reviewed. All courses of ATG andCsA were documented, and response to therapy at 6, 12 and18 months and the last follow-up was chronicled.
METHODSPatientsAll patients >18 years diagnosed as having AA between 1 January1996 and 31 December 2009 at a tertiary care armed forces hos-pital in New Delhi, India were included for retrospective analysis.Patients were excluded if they had congenital AA, paroxysmal noc-turnal haemoglobinuria (PNH) or a clonal cytogenetic abnormal-ity (myelodysplastic syndrome (MDS) or leukaemia). In addition,patients who had previously undergone HSCT or died within6 months of ATG administration were excluded. Congenital AAcould be excluded with reasonable certainty in all patients!40 years based on medical history, family history, physical exam-ination, and bone marrow cytogenetic and chromosomal fragilitystudies with diepoxybutane. PNH screening was performed usingHam’s test, sucrose lysis and urinary haemosiderin until 2004 andby flow cytometric determination of CD55/59 from January 2005onwards. Additional tests, including liver and renal function testsand serology for hepatitis B and C and HIV, were performed in allcases. Tests for Epstein–Barr virus, cytomegalovirus (CMV) andparvovirus B-19 were performed depending on the clinical setting.The seroprevalence of CMV varies in different geographic areas,ranging from 30% to 100%.13–15 Hence, active CMV disease wasdiagnosed on the basis of CMV IgM levels until 2004 and CMVDNA copies from January 2005 onwards.
Disease severityPatients were classified according to the established severity cri-teria.1 AA was considered severe (SAA) if marrow cellularity was<25% and at least two of the following criteria were met: abso-lute neutrophil count (ANC) <0.5! 109/l, platelet count<20! 109/l, reticulocytes <20! 109/l. AA was considered verysevere (VSAA) if the above criteria for SAA were fulfilled, andthe ANC was <0.2! 109/l. Non-severe AA (NSAA) was definedas hypocellular bone marrow with at least two of the following:ANC <1! 109/l, platelet count <50! 109/l, reticulocyte count<60! 109/l. Hepatitis-associated AA was defined as AA thatoccurred either concurrent with, or within 6 months of presen-tation with, an increase in serum alanine aminotransferase activ-ity of at least five times the upper reference limit.
Treatment protocolAll patients were treated with equine ATG (e-ATG; Atgam;Pfizer), which was administered intravenously at a dose of40 mg/kg/day on days 1–4. On day 1, the e-ATG administrationwas started at a slow rate for the initial 30 min to monitorimmediate hypersensitivity, and, if there was no reaction to infu-sion, it was infused at a regular rate over a period of 8–12 h.e-ATG administration was preceded, each day, by premedicationwith acetaminophen, chlorpheniramine and hydrocortisone. Ifinfusion-related toxicity was noted during e-ATG infusion, itwas stopped and restarted at a slower rate after administrationof antihistamines. Oral prednisolone (1 mg/kg/day) was adminis-tered for 7 days followed by tapering over 1–2 weeks to preventserum sickness. CsA was administered orally from day 21 ofATG treatment at a dose of 8–10 mg/kg/day in two divideddoses and adjusted to maintain serum levels at 150–200 ng/mlor for renal/hepatic toxicity. Serum CsA was measured once inthe first month of therapy to maintain appropriate levels.Thereafter, repeat measurements of serum CsA were performedonly if the patient developed gastrointestinal toxicity,
hypertension or hyperkalaemia, or showed features of renal/hepatic toxicity. CsA was continued for 12 months and there-after was tapered gradually over the next 3–6 months, so thateach patient received CsA for 15–18 months, with a median of16 months. A second course of e-ATG or rabbit ATG (r-ATG;thymoglobulin; Genzyme Corporation) was administered if thepatient had not responded after 6 months of the initial treat-ment or relapsed after the initial response.
Supportive care was provided as per the clinical setting.Platelets were transfused prophylactically for levels <10! 103/land at higher levels if there was symptomatic bleeding. Redblood cell transfusions were given for haemoglobin <70 g/l orsymptomatic anaemia. All blood products were irradiated. Mostpatients received group-specific units of single-donor platelets.However, if the latter were not available, random-donor plate-lets were also used. Febrile neutropenia was managed with intra-venous antibiotics, with the addition of antifungal agents after3–4 days of unresponsive fever in accordance with the institu-tional antimicrobial policy. No prophylactic oral antifungalagents or antibiotics were administered. G-CSF was adminis-tered at a dose of 5 mg/kg/day (maximum 300 mg/day) subcuta-neously at the discretion of the treating physician.
Response criteriaA complete response (CR) was defined as ANC>1.5! 109/l,platelets >100! 109/l, and haemoglobin >100 g/l. A partialresponse (PR) was defined as ANC>0.5! 109/l, platelets>20! 109/l, and haemoglobin >80 g/l in patients with SAA,and as ANC >1.0! 109/l, platelets >30! 109/l, and haemoglo-bin >80 g/l in patients with NSAA.1 The response was assessed6 months after ATG administration. Relapse was defined as adecline in peripheral blood cell count to levels meeting the def-inition of severe or moderate AA.
Statistical analysisOS was measured from the time of onset of treatment to thetime of last follow-up or death. For calculating overall response,the patient was considered responsive to IST if the criteria forPR were satisfied. Summary statistics, including means, mediansand range, were used to describe the patient’s baseline character-istics. Binary group analyses were performed using the Fisherexact test or !2 test.
Cumulative survival for time to death (OS) and time torelapse/death (failure-free survival (FFS)) were estimated by theKaplan–Meier method. The log-rank (Mantel–Cox) test wasused for univariate comparisons of survival curves betweengroups. The multivariate Cox regression model was used toanalyse risk factors for death. Variables with p<0.1 in univariateanalysis were entered into stepwise selection models, and HRwith 95% CIs were calculated.
Statistical analysis was performed using GraphPad PrismV.5.00 for MacOsX and SPSS V.16.0.
RESULTSPatient characteristicsFrom January 1996 to December 2009, 184 patients were diag-nosed as having AA, of which 120 were eligible for final analysis(figure 1). Patient characteristics are shown in table 1.
Three patients had hepatitis-associated AA. No cause for sec-ondary AA was found in any other patient. The serological testfor hepatitis C was positive in one patient.
Ninety-six (80%) patients had SAA (94 idiopathic, twohepatitis-associated), 17 (14.2%) had VSAA (16 idiopathic, onehepatitis-associated), and seven (5.8%) patients had NSAA.
2 Nair V, et al. Postgrad Med J 2013;0:1–8. doi:10.1136/postgradmedj-2011-130605
Original article
group.bmj.com on May 24, 2013 - Published by pmj.bmj.comDownloaded from

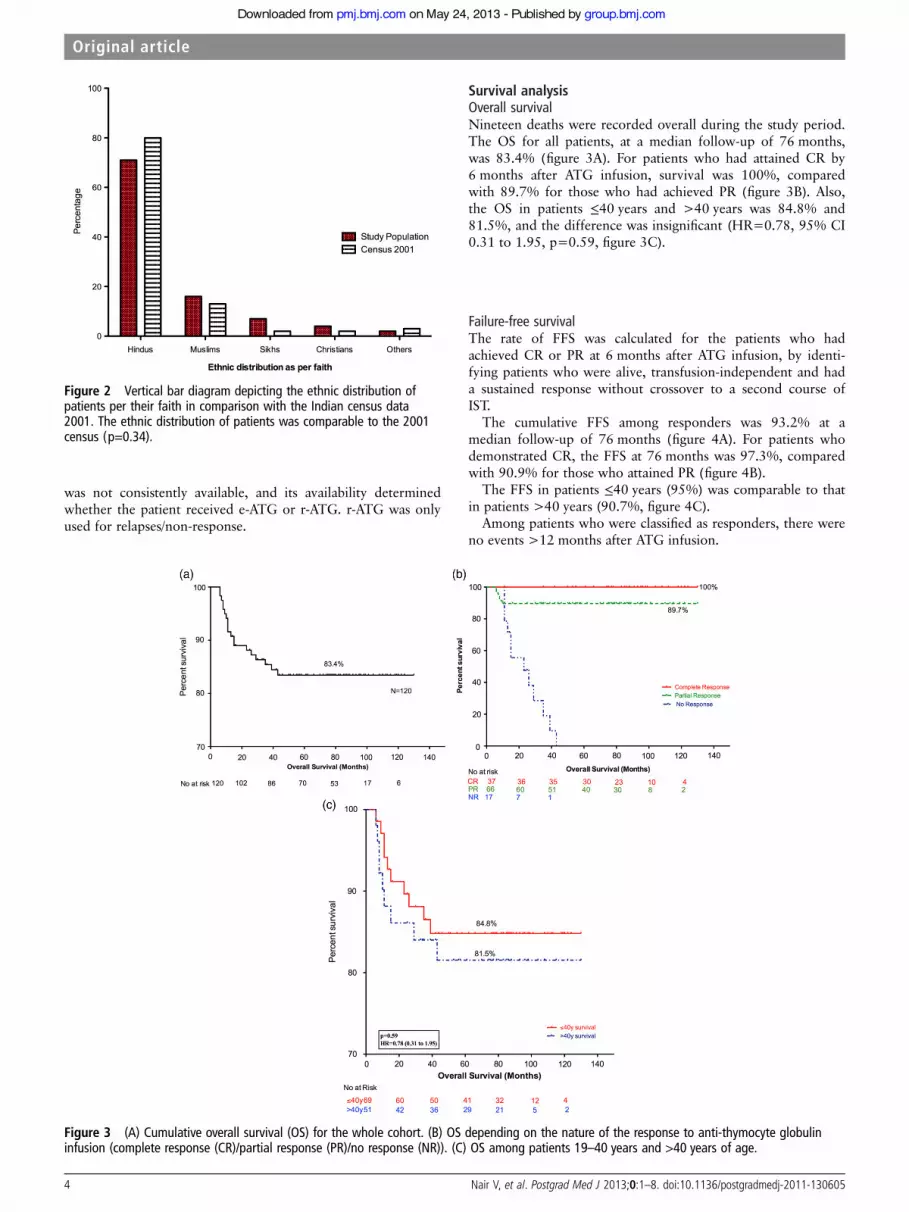
The ethnic distribution of patients with respect to their faithwas found to be comparable to that in the Indian nationalcensus of 2001 (p=0.34, figure 2).
Response to ISTOverall response (response "PR) to IST was observed in103/120 (85.8%) patients at 6 months; 17 patients did notrespond to IST. Six months after ATG administration, 11/120(9.2%) had achieved CR, and 92/120 (76.7%) demonstratedPR. The number of patients attaining CR increased to 37(30.8%) at 18 months, with the median time to attain CR being9.5 months (range 4.5–16). At the last clinical visit, 37 patients
had achieved CR, and 61 continued to show a partial haemato-logical response.
One course of ATG was received by 103 patients, twocourses by 16 patients, and three courses by one patient. Of the16 patients who were administered two courses of ATG (sixwho had relapsed after the first course of ATG and 10 non-responders), nine received e-ATG and seven were administeredr-ATG. Among the patients receiving e-ATG as the secondcourse, 1/9 (11.1%) achieved PR. For those who received r-ATGas the second course, 5/7 (71.4%) attained PR. One patient, anon-responder, received three courses of ATG (e-ATG as thefirst and second course and r-ATG as the third course), andattained PR after the administration of r-ATG. However, r-ATG
Figure 1 Flow chart depictingselection of patient cohort. ATG,anti-thymocyte globulin; HSCT,haematopoietic stem celltransplantation; PNH, paroxysmalnocturnal haemoglobinuria
Table 1 Pretreatment characteristics of patients
Subset characteristics
Variable All patients !40 years >40 years
N 120 69 51Age (years), median (range) 36.5 (19–77) 28 (19–40) 55 (41–77)Male 63 35 28Female 57 34 23M : F 1.11 : 1 1.03 : 1 1.22 : 1Duration of symptoms before initiation of therapy (months), median (range) 4.5 (2–19) 4.2 (2–17) 4.9 (4–19)Haemoglobin (g/l), median (range) 58 (22–99) 59 (26–99) 58 (22–98)Absolute reticulocyte count (!109/l), median (range) 16 (7–24) 16 (7–24) 15 (8–21)WBC count (!109/l), median (range) 1.1 (0.4–4.7) 0.9 (0.4–4.0) 1.2 (0.6–4.7)ANC (!109/l), median (range) 0.36 (0.10–0.90) 0.36 (0.10–0.70) 0.36 (0.10–0.90)Platelets (!109/l), median (range) 22 (2–50) 21 (2–50) 24 (3–45)
ANC, absolute neutrophil count; WBC, white blood cell.
Nair V, et al. Postgrad Med J 2013;0:1–8. doi:10.1136/postgradmedj-2011-130605 3
Original article
group.bmj.com on May 24, 2013 - Published by pmj.bmj.comDownloaded from
was not consistently available, and its availability determinedwhether the patient received e-ATG or r-ATG. r-ATG was onlyused for relapses/non-response.
Survival analysisOverall survivalNineteen deaths were recorded overall during the study period.The OS for all patients, at a median follow-up of 76 months,was 83.4% (figure 3A). For patients who had attained CR by6 months after ATG infusion, survival was 100%, comparedwith 89.7% for those who had achieved PR (figure 3B). Also,the OS in patients !40 years and >40 years was 84.8% and81.5%, and the difference was insignificant (HR=0.78, 95% CI0.31 to 1.95, p=0.59, figure 3C).
Failure-free survivalThe rate of FFS was calculated for the patients who hadachieved CR or PR at 6 months after ATG infusion, by identi-fying patients who were alive, transfusion-independent and hada sustained response without crossover to a second course ofIST.
The cumulative FFS among responders was 93.2% at amedian follow-up of 76 months (figure 4A). For patients whodemonstrated CR, the FFS at 76 months was 97.3%, comparedwith 90.9% for those who attained PR (figure 4B).
The FFS in patients !40 years (95%) was comparable to thatin patients >40 years (90.7%, figure 4C).
Among patients who were classified as responders, there wereno events >12 months after ATG infusion.
Figure 3 (A) Cumulative overall survival (OS) for the whole cohort. (B) OS depending on the nature of the response to anti-thymocyte globulininfusion (complete response (CR)/partial response (PR)/no response (NR)). (C) OS among patients 19–40 years and >40 years of age.
Figure 2 Vertical bar diagram depicting the ethnic distribution ofpatients per their faith in comparison with the Indian census data2001. The ethnic distribution of patients was comparable to the 2001census (p=0.34).
4 Nair V, et al. Postgrad Med J 2013;0:1–8. doi:10.1136/postgradmedj-2011-130605
Original article
group.bmj.com on May 24, 2013 - Published by pmj.bmj.comDownloaded from

Ethnicity and survivalNeither OS (p=0.82; HR=0.84, 95% CI 0.19 to 3.81) norFFS (p=0.50; HR=0.72, 95% CI 0.30 to 1.76) were influencedby the ethnic distribution of the patients.
Response to salvage therapyNon-responderSeventeen patients who did not respond to IST were treatedwith alternative therapies including retreatment with e-ATG,r-ATG, fludarabine and mycophenolate mofetil, danazol andHSCT (table 2). A sustained haematological response wasobserved only after administration of r-ATG (2/4 achieved PR)or HSCT (1/1 achieved CR). However, a PR was observed in3/5 patients who were administered fludarabine and mycophe-nolate mofetil, but this response was short-lived and all of thepatients relapsed within 6–12 months. One of six patients whowere retreated with e-ATG attained PR.
RelapseRelapse of AA occurred in 6/103 (5.8%) patients at a mediantime of 9 months (range 6–11). All six patients who relapsedafter an initial response to IST received some form of salvagetherapy (table 3). PR was observed in 3/3 (100%) patients whowere administered r-ATG. No response was noted in threepatients who received a second course of e-ATG.
ComplicationsThere were 19 deaths (12 non-responders, seven partial respon-ders). Thirteen patients died from sepsis, one from intracranial
Table 2 Treatment of patients who did not respond to IST
Patient No Therapy Response Outcome
2 e-ATG+CsAr-ATG+CsA
NRPR
Sustained response (Survived)
10 Danazol NR Died18 Danazol NR Died34 Danazol NR Died35 Danazol NR Died43 Fludarabine+MMF PR Relapsed and died48 e-ATG+CsA NR Died51 e-ATG+CsA NR Relapsed and died
Fludarabine+MMF PR82 r-ATG+CsA NR Died85 e-ATG+CsA
Fludarabine+MMFDanazol
NRNRNR
Died
92 e-ATG+CsA NR Died93 r-ATG+CsA PR Sustained response (survived)110 e-ATG+CsA
Fludarabine+MMFNRPR
Relapsed and died
124 e-ATG+CsA PR Sustained response (survived)150 r-ATG+CsA
Fludarabine+MMFNR Died
147 r-ATG+CsA PR Sustained response (survived)170 HSCT Engraftment Survived
CsA, ciclosporin A; e-ATG, equine anti-thymocyte globulin; HSCT, haematopoieticstem cell transplantation; IST, immunosuppressive therapy; MMF, mycophenolatemofetil; NR, no response; PR, partial response; r-ATG, rabbit ATG.
Figure 4 (A) Failure-free survival (FFS) among responders (complete response (CR) and partial response (PR)) to anti-thymocyte globulin infusion.(B) FFS: comparison between type of response. NR, no response. (C) FFS: comparison between patients 19–40 years and >40 years.
Nair V, et al. Postgrad Med J 2013;0:1–8. doi:10.1136/postgradmedj-2011-130605 5
Original article
group.bmj.com on May 24, 2013 - Published by pmj.bmj.comDownloaded from
bleeding and one from acute pancreatitis. Four patients with PRdied from non-disease-related causes.
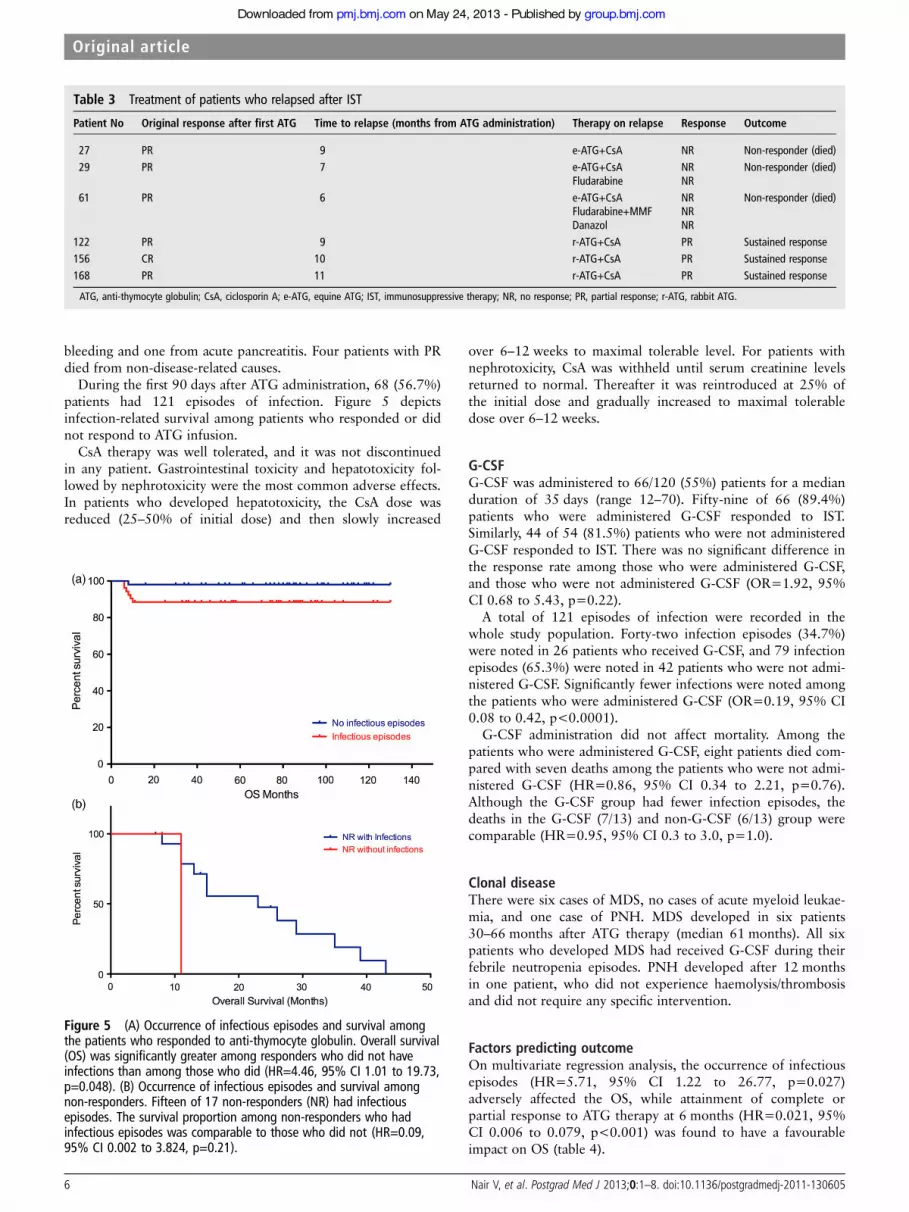
During the first 90 days after ATG administration, 68 (56.7%)patients had 121 episodes of infection. Figure 5 depictsinfection-related survival among patients who responded or didnot respond to ATG infusion.
CsA therapy was well tolerated, and it was not discontinuedin any patient. Gastrointestinal toxicity and hepatotoxicity fol-lowed by nephrotoxicity were the most common adverse effects.In patients who developed hepatotoxicity, the CsA dose wasreduced (25–50% of initial dose) and then slowly increased
over 6–12 weeks to maximal tolerable level. For patients withnephrotoxicity, CsA was withheld until serum creatinine levelsreturned to normal. Thereafter it was reintroduced at 25% ofthe initial dose and gradually increased to maximal tolerabledose over 6–12 weeks.
G-CSFG-CSF was administered to 66/120 (55%) patients for a medianduration of 35 days (range 12–70). Fifty-nine of 66 (89.4%)patients who were administered G-CSF responded to IST.Similarly, 44 of 54 (81.5%) patients who were not administeredG-CSF responded to IST. There was no significant difference inthe response rate among those who were administered G-CSF,and those who were not administered G-CSF (OR=1.92, 95%CI 0.68 to 5.43, p=0.22).
A total of 121 episodes of infection were recorded in thewhole study population. Forty-two infection episodes (34.7%)were noted in 26 patients who received G-CSF, and 79 infectionepisodes (65.3%) were noted in 42 patients who were not admi-nistered G-CSF. Significantly fewer infections were noted amongthe patients who were administered G-CSF (OR=0.19, 95% CI0.08 to 0.42, p<0.0001).
G-CSF administration did not affect mortality. Among thepatients who were administered G-CSF, eight patients died com-pared with seven deaths among the patients who were not admi-nistered G-CSF (HR=0.86, 95% CI 0.34 to 2.21, p=0.76).Although the G-CSF group had fewer infection episodes, thedeaths in the G-CSF (7/13) and non-G-CSF (6/13) group werecomparable (HR=0.95, 95% CI 0.3 to 3.0, p=1.0).
Clonal diseaseThere were six cases of MDS, no cases of acute myeloid leukae-mia, and one case of PNH. MDS developed in six patients30–66 months after ATG therapy (median 61 months). All sixpatients who developed MDS had received G-CSF during theirfebrile neutropenia episodes. PNH developed after 12 monthsin one patient, who did not experience haemolysis/thrombosisand did not require any specific intervention.
Factors predicting outcomeOn multivariate regression analysis, the occurrence of infectiousepisodes (HR=5.71, 95% CI 1.22 to 26.77, p=0.027)adversely affected the OS, while attainment of complete orpartial response to ATG therapy at 6 months (HR=0.021, 95%CI 0.006 to 0.079, p<0.001) was found to have a favourableimpact on OS (table 4).
Figure 5 (A) Occurrence of infectious episodes and survival amongthe patients who responded to anti-thymocyte globulin. Overall survival(OS) was significantly greater among responders who did not haveinfections than among those who did (HR=4.46, 95% CI 1.01 to 19.73,p=0.048). (B) Occurrence of infectious episodes and survival amongnon-responders. Fifteen of 17 non-responders (NR) had infectiousepisodes. The survival proportion among non-responders who hadinfectious episodes was comparable to those who did not (HR=0.09,95% CI 0.002 to 3.824, p=0.21).
Table 3 Treatment of patients who relapsed after IST
Patient No Original response after first ATG Time to relapse (months from ATG administration) Therapy on relapse Response Outcome
27 PR 9 e-ATG+CsA NR Non-responder (died)29 PR 7 e-ATG+CsA
FludarabineNRNR
Non-responder (died)
61 PR 6 e-ATG+CsAFludarabine+MMFDanazol
NRNRNR
Non-responder (died)
122 PR 9 r-ATG+CsA PR Sustained response156 CR 10 r-ATG+CsA PR Sustained response168 PR 11 r-ATG+CsA PR Sustained response
ATG, anti-thymocyte globulin; CsA, ciclosporin A; e-ATG, equine ATG; IST, immunosuppressive therapy; NR, no response; PR, partial response; r-ATG, rabbit ATG.
6 Nair V, et al. Postgrad Med J 2013;0:1–8. doi:10.1136/postgradmedj-2011-130605
Original article
group.bmj.com on May 24, 2013 - Published by pmj.bmj.comDownloaded from

DISCUSSIONIST is the treatment of choice for patients with AA who are ineli-gible for HSCT. We accomplished an OS of 83.4% at a medianfollow-up of 76 months. The overall response at 6 months afterATG administration was 85.8%. Seventeen patients did notrespond to IST, and six patients relapsed after an initial response.In addition, six patients developed MDS on follow-up. Previousdata, mostly from developed nations, show an overall response of60–85% with a 5-year survival rate of 75–85%.4 16–18 The limiteddata from developing countries reveals a response rate of <50%with an OS of 40–60%.10 Most of the earlier reports from theIndian sub-continent used heterogeneous protocols involving vari-able doses and duration of ATG and CsA.10 19 20 In addition, thequality of supportive care in the form of blood components andantimicrobials at many centres in India is dictated by the cost andaffordability status of the patient.21 We provided treatment free ofcost to all patients irrespective of their financial background, andhence could ensure a standard of care across the entire cohort.These differences in study protocol may partially explain the infer-ior results of earlier researchers from India.
The occurrence of infectious episodes and lack of response toATG therapy were associated with poor outcome. No otherpatient characteristics, including age and blood count, influ-enced survival in our cohort. We demonstrate that the use ofG-CSF reduces the number of infectious episodes in thesepatients but does not affect the outcome and survival. Infectiousepisodes, in turn, were found to adversely affect the survival ofthese patients. However, we failed to demonstrate any directeffect of G-CSF on survival/outcome. These results corroboratethose of Tichelli et al where they failed to demonstrate an effectof G-CSF on OS, event-free survival or remission.22 Theregional distribution of patients in our cohort closely mirroredthe regional distribution of the population as per the nationalcensus of India in 2001.23 Thus, our cohort had multiethnicrepresentation. Nevertheless, we failed to demonstrate anyeffect of ethnicity on response to ISTor long-term survival.
The cumulative incidence of relapse among the responders was5.8% (median time to relapse 9 months, range 6–11 months),which is significantly less than earlier reports of 9–35%.6 16 24
This is possibly due to the prolonged administration of CsA.1 25
Among the non-responders and the patients who relapsed aftere-ATG administration, the use of r-ATG was associated with aresponse in 5/7 patients (2/4 non-responders; 3/3 patients whorelapsed).
Our OS and response rates are comparable to the data fromthe West. The response rates may appear to be better because ofthis being a single-centre retrospective study with its inherentbias. The median age of the whole cohort was <40 years, andonly <10% of the patients were aged "60 years. Most Westerndata have a uniform distribution of patients across all ages, withthe best response among patients !40 years and worst for those"60 years.25 26 The relatively younger age of patients in ourcohort also might have skewed the response rates. Another limi-tation of our study is a median follow-up period of only76 months. In a condition such as AA where clonal disorderscan occur decades after treatment and other evolutionary fea-tures may take a long time, 76 months may be a shortfollow-up. In addition, we did not measure serial CsA levelsunless the patient developed signs of toxicity. Nonetheless,despite these limitations, the critical inference from our data is
Table 4 Factors predicting overall survival of patients in univariate and multivariate analysis
Univariate analysis Multivariate analysis
Variable HR (95% CI) p Value HR (95% CI) p Value
G-CSF use 0.69 (0.31 to 1.5) 0.37 Not testedInfectious episode occurrence 5.70 (2.31 to 14.07) <0.001 5.71 (1.22 to 26.77) 0.027Age !40 years 0.78 (0.31 to 1.95) 0.59 Not testedPresence of pallor 1.39 (0.56 to 3.44) 0.48 Not testedPresence of bleeding manifestations 0.79 (0.32 to 1.94) 0.61 Not testedPresence of fever 1.34 (0.55 to 3.46) 0.45 Not testedHaemoglobin <60 g/l 0.77 (0.31 to 1.93) 0.58 Not testedAbsolute reticulocyte count !10000!109/l 0.81 (0.21 to 3.10) 0.76 Not testedANC !0.25!109/l 1.29 (0.34 to 4.92) 0.71 Not testedPlatelet count !20!109/l 0.55 (0.22 to 1.36) 0.19 Not testedResponse present at 6 months (CR or PR) 0.0003 (5.841!10#5 to 0.0013) <0.0001 0.021 (0.006 to 0.079) <0.001
ANC, absolute neutrophil count; CR, complete response; G-CSF, granulocyte colony-stimulating factor; PR, partial response.
Main messages
▸ We found in our institution in a developing country thatimmunosuppressive therapy is a highly efficacious first-linetreatment for patients with aplastic anaemia, with 83.4%survival at 76 months. This is much better than previousreports from the Indian sub-continent.
▸ Response to anti-thymocyte globulin at 6 months is the bestpredictor of long-term survival.
▸ Granulocyte colony-stimulating factor (G-CSF) may reducethe episodes of infection but fails to offer any survivaladvantage or influence outcome.
▸ Ethnicity does not affect survival/outcome.
Current research questions
▸ Role of G-CSF and its cumulative dose in causation of clonaldisorders.
▸ Role of G-CSF in reducing cost of treatment by reducinghospital infection episodes.
▸ The aetiopathogenesis of non-responders and the patientswho relapsed.
Nair V, et al. Postgrad Med J 2013;0:1–8. doi:10.1136/postgradmedj-2011-130605 7
Original article
group.bmj.com on May 24, 2013 - Published by pmj.bmj.comDownloaded from
that, if standard-of-care IST and supportive care is administeredto patients from developing countries, outcomes comparable tothose in the West can be achieved. We demonstrate that morethan three out of four patients treated with IST will have FFSfor more than 6 years. The survival is predicted by the presenceof a response to ATG infusion at 6 months and absence of infec-tious complications.
Acknowledgements The study was carried out in the Army Hospital (Researchand Referral Centre, New Delhi), where the entire cost of the treatment was borneby the hospital. We acknowledge the support of the Commandant of the ArmyHospital (Research and Referral Centre) for this. We are also grateful to the office ofDGMS (Army) and the office of DGAFMS for supporting our endeavour. We alsoacknowledge the significant contribution of haematopathologists, Dr D K Mishra andDr J Kotwal, and microbiologists, Dr R M Gupta and Dr N Grover.
Contributors VN was the principal investigator and will act as guarantor of thestudy. VN, AS, SD and SS recruited the patients. VS participated in the statisticalanalysis. VN, AS and SD coordinated the research. VN and VS wrote the paper. Thefinal manuscript was approved by all authors. All authors had full access to all ofthe data (including statistical reports and tables) in the study and take responsibilityfor the integrity of the data and the accuracy of the data analysis.
Competing interests None.
Ethics approval Institutional ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.
REFERENCES1 Marsh JC, Ball SE, Cavenagh J, et al. Guidelines for the diagnosis and management
of aplastic anaemia. Br J Haematol 2009;147:43–70.2 Khamaganova E, Murashova L, Zaretskaya Y. HLA-DRB and DQB1 genes in
predisposition to aplastic anemia. Haematologica/ Hematology J 2007;92(Suppl 1):25.3 Young NS, Calado RT, Scheinberg P. Current concepts in the pathophysiology and
treatment of aplastic anemia. Blood 2006;108:2509–19.4 Locasciulli A, Oneto R, Bacigalupo A, et al. Outcome of patients with acquired
aplastic anemia given first line bone marrow transplantation or immunosuppressivetreatment in the last decade: a report from the European Group for Blood andMarrow Transplantation (EBMT). Haematologica 2007;92:11–18.
5 Horowitz MM. Current status of allogeneic bone marrow transplantation in acquiredaplastic anemia. Semin Hematol 2000;37:30–42.
6 Rosenfeld S, Follmann D, Nunez O, et al. Antithymocyte globulin and cyclosporinefor severe aplastic anemia: association between hematologic response andlong-term outcome. JAMA 2003;289:1130–5.
7 Frickhofen N, Kaltwasser JP, Schrezenmeier H, et al. Treatment of aplastic anemiawith antilymphocyte globulin and methylprednisolone with or without cyclosporine.The German Aplastic Anemia Study Group. N Engl J Med 1991;324:1297–304.
8 Rosenfeld SJ, Kimball J, Vining D, et al. Intensive immunosuppression withantithymocyte globulin and cyclosporine as treatment for severe acquired aplasticanemia. Blood 1995;85:3058–65.
9 Moore MA, Castro-Malaspina H. Immunosuppression in aplastic anemia—postponing the inevitable? N Engl J Med 1991;324:1358–60.
10 George B, Mathews V, Viswabandya A, et al. Allogeneic hematopoietic stem celltransplantation is superior to immunosuppressive therapy in Indian children with
aplastic anemia—a single-center analysis of 100 patients. Pediatr Hematol Oncol2010;27:122–31.
11 Kojima S, Hibi S, Kosaka Y, et al. Immunosuppressive therapy using antithymocyteglobulin, cyclosporine, and danazol with or without human granulocytecolony-stimulating factor in children with acquired aplastic anemia. Blood2000;96:2049–54.
12 Shao Z, Chu Y, Zhang Y, et al. Treatment of severe aplastic anemia with animmunosuppressive agent plus recombinant human granulocyte-macrophagecolony-stimulating factor and erythropoietin. Am J Hematol 1998;59:185–91.
13 Crough T, Khanna R. Immunobiology of human cytomegalovirus: from bench tobedside. Clin Microbiol Rev 2009;22:76–98, Table of Contents.
14 Grundy JE. Virologic and pathogenetic aspects of cytomegalovirus infection. RevInfect Dis 1990;12(Suppl 7):S711–19.
15 Jain M, Duggal S, Chugh TD. Cytomegalovirus infection in non-immunosuppressedcritically ill patients. J Infect Dev Ctries 2011;5:571–9.
16 Bacigalupo A, Bruno B, Saracco P, et al. Antilymphocyte globulin, cyclosporine,prednisolone, and granulocyte colony-stimulating factor for severe aplastic anemia:an update of the GITMO/EBMT study on 100 patients. European Group for Bloodand Marrow Transplantation (EBMT) Working Party on Severe Aplastic Anemia andthe Gruppo Italiano Trapianti di Midolio Osseo (GITMO). Blood 2000;95:1931–4.
17 Bacigalupo A, Oneto R, Bruno B, et al. Current results of bone marrowtransplantation in patients with acquired severe aplastic anemia. Report of theEuropean Group for Blood and Marrow transplantation. On behalf of the WorkingParty on Severe Aplastic Anemia of the European Group for Blood and MarrowTransplantation. Acta Haematol 2000;103:19–25.
18 Fuhrer M, Rampf U, Baumann I, et al. Immunosuppressive therapy for aplasticanemia in children: a more severe disease predicts better survival. Blood2005;106:2102–4.
19 Choudhary DR, Kumar R, Dixit A, et al. Adverse effects and supportive therapyrequirements during administration of Anti-Thymocyte Globulin (ATG). Proceedingsof the 60th Annual Conference of the Association of Physicians of India (APICON).Mumbai, India, 2005.
20 Ganapule A, George B, Mathews V, et al. Immunosuppresive Therapy withAntilymphocyte (ALG)/Antithymocyte Globulin (ATG) for Aplastic Anemia: A SingleCentre Experience. Proceedings of the 51st National Conference of Indian Society ofHematology & Transfusion Medicine. Kolkata, India: Springer, 2010.
21 Kanwar VS. Immunotherapy for Childhood Aplastic Anemia in India: A Case forUniversal Healthcare? Indian Pediatrics 2012;49:354–5.
22 Tichelli A, Schrezenmeier H, Socie G, et al. A randomized controlled study innewly-diagnosed severe aplastic anemia patients receiving antithymocyte globulin(ATG), cyclosporine, with or without G-CSF: a study of the SAA Working Party ofthe EBMT. Blood 2011;117:4434–41.
23 Office of Registrar General I. Census data 2001, 2001.24 Schrezenmeier H, Marin P, Raghavachar A, et al. Relapse of aplastic anaemia after
immunosuppressive treatment: a report from the European Bone MarrowTransplantation Group SAA Working Party. Br J Haematol 1993;85:371–7.
25 Bacigalupo A, Passweg J. Diagnosis and treatment of acquired aplastic anemia.Hematol Oncol Clin North Am 2009;23:159–70.
26 Tichelli A, Socie G, Henry-Amar M, et al. Effectiveness of immunosuppressivetherapy in older patients with aplastic anemia. European Group for Blood andMarrow Transplantation Severe Aplastic Anaemia Working Party. Ann Intern Med1999;130:193–201.
8 Nair V, et al. Postgrad Med J 2013;0:1–8. doi:10.1136/postgradmedj-2011-130605
Original article
group.bmj.com on May 24, 2013 - Published by pmj.bmj.comDownloaded from

doi: 10.1136/postgradmedj-2011-130605 published online May 18, 2013Postgrad Med J
Velu Nair, Ajay Sharma, Satyaranjan Das, et al. experience from Indiaaplastic anaemia: single-institution Immunosuppressive therapy in adults with
http://pmj.bmj.com/content/early/2013/05/17/postgradmedj-2011-130605.full.htmlUpdated information and services can be found at:
These include:
References http://pmj.bmj.com/content/early/2013/05/17/postgradmedj-2011-130605.full.html#ref-list-1
This article cites 23 articles, 8 of which can be accessed free at:
P<P Published online May 18, 2013 in advance of the print journal.
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
CollectionsTopic
(178 articles)Drugs: infectious diseases (313 articles)Immunology (including allergy)
Articles on similar topics can be found in the following collections
Notes
(DOIs) and date of initial publication. publication. Citations to Advance online articles must include the digital object identifier citable and establish publication priority; they are indexed by PubMed from initialtypeset, but have not not yet appeared in the paper journal. Advance online articles are Advance online articles have been peer reviewed, accepted for publication, edited and
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on May 24, 2013 - Published by pmj.bmj.comDownloaded from





























