Embed Size (px)
Citation preview
IIFT: Crithidia luciliae (anti-dsDNA) Instructions for the indirect immunofluorescence test
ORDER NO. ANTIBODIES AGAINST SUBSTRATE SPECIES FORMAT
SLIDES x FIELDSFA 1572-1003 FA 1572-1005 FA 1572-1010 FA 1572-2003 FA 1572-2005 FA 1572-2010
dsDNA (nDNA) flagellates Crithidia luciliae
10 x 03 (030) 10 x 05 (050) 10 x 10 (100) 20 x 03 (060) 20 x 05 (100) 20 x 10 (200)
Indication: This test kit is designed for the qualitative or semiquantitative in vitro determination of human antibodies of immunoglobulin class IgG against dsDNA in patient samples for the diagnosis of systemic lupus erythematosus (SLE). Application: Indirect immunofluorescence using Crithidia luciliae is the gold standard for the specific detection of antibodies against double-stranded deoxyribonucleic acid (dsDNA). Test principle: Crithidia luciliae flagellates are incubated with a diluted patient sample. If a positive reaction is obtained, specific antibodies of classes IgA, IgG and IgM attach to the antigens. In a second step, the attached antibodies are stained with fluorescein-labelled anti-human antibodies and made visible with a fluorescence microscope. Contents of a test system for 50 determinations (e.g. FA 1572-1005): Description Format Symbol1. Slides, each containing BIOCHIPs coated with a smear of
Crithidia luciliae 10 slides .SLIDE.
2. Fluorescein-labelled anti-human IgG (goat), ready for use 1 x 1.5 ml .CONJUGATE.
3. Positive control: autoantibody against dsDNA, serum with titer information, human, ready for use
1 x 0.1 ml .POS CONTROL.
4. Negative control: autoantibody negative, human, ready for use 1 x 0.1 ml .NEG CONTROL.
5. Salt for PBS pH 7.2 2 packs .PBS.
6. Tween 20 2 x 2.0 ml .TWEEN 20.
7. Mounting medium, ready for use 1 x 3.0 ml .GLYCEROL.
8. Cover glasses (62 mm x 23 mm) 12 pieces .COVERGLASS.
9. Instruction booklet 1 booklet ---
.LOT. Lot description
Storage temperature .IVD. In vitro diagnostic medical device Unopened usable until
Single slides (e.g., EUROIMMUN order no. FB 1572-1005) are provided together with cover glasses. Additional positive control (e.g., order no. CA 1572-0101-3) and negative control (e.g., order no. CA 1000-0101) can be ordered. Performance of the test requires reagent trays TRAY, which are not provided in the test kits. They are available from EUROIMMUN under the following order no.: - ZZ 9999-0110 Reagent trays for slides containing up to 10 fields Storage and stability: The slides and the reagents should be stored at a temperature between +2°C and +8°C. Unopened, all test kit components are stable until the indicated expiry date. Waste disposal: Patient samples, controls and slides are to be handled as potentially infectious materials. All reagents are to be disposed of in accordance with official disposal regulations.
FA_1572_A_UK_C13.doc
Version: 10/01/2017
2
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
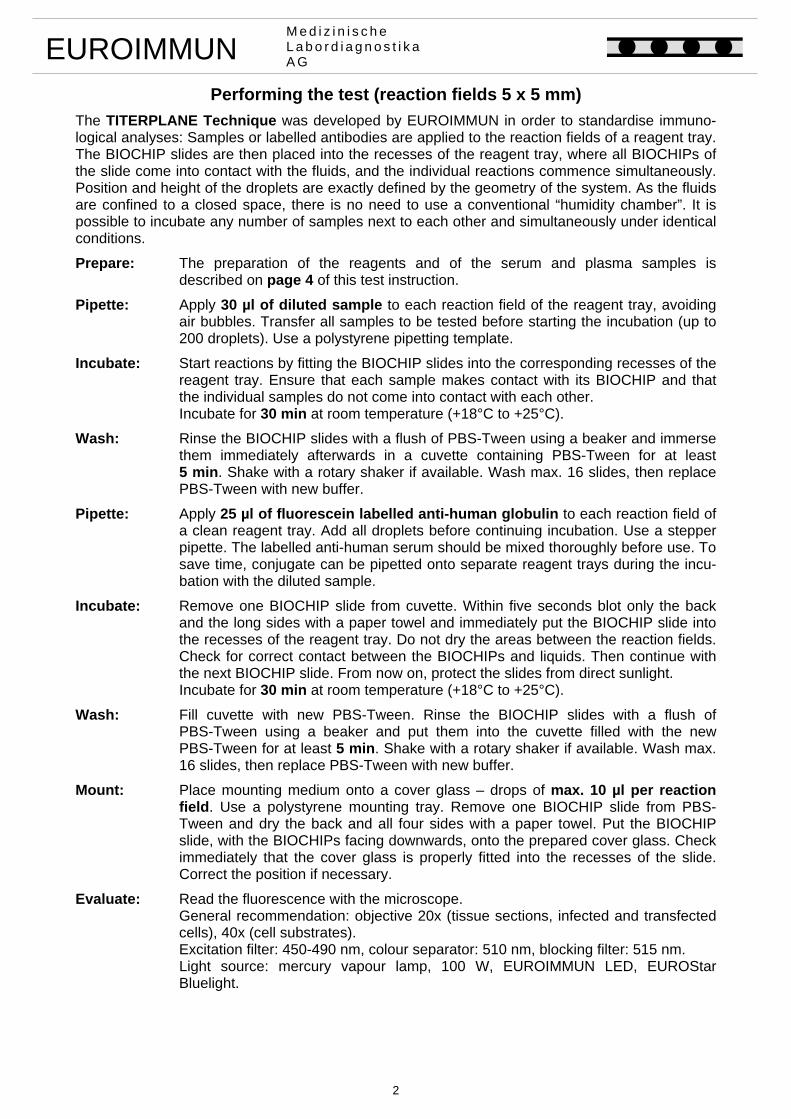
Performing the test (reaction fields 5 x 5 mm)
The TITERPLANE Technique was developed by EUROIMMUN in order to standardise immuno-logical analyses: Samples or labelled antibodies are applied to the reaction fields of a reagent tray. The BIOCHIP slides are then placed into the recesses of the reagent tray, where all BIOCHIPs of the slide come into contact with the fluids, and the individual reactions commence simultaneously. Position and height of the droplets are exactly defined by the geometry of the system. As the fluids are confined to a closed space, there is no need to use a conventional “humidity chamber”. It is possible to incubate any number of samples next to each other and simultaneously under identical conditions.
Prepare: The preparation of the reagents and of the serum and plasma samples is described on page 4 of this test instruction.
Pipette: Apply 30 µl of diluted sample to each reaction field of the reagent tray, avoiding air bubbles. Transfer all samples to be tested before starting the incubation (up to 200 droplets). Use a polystyrene pipetting template.
Incubate: Start reactions by fitting the BIOCHIP slides into the corresponding recesses of the reagent tray. Ensure that each sample makes contact with its BIOCHIP and that the individual samples do not come into contact with each other.
Incubate for 30 min at room temperature (+18°C to +25°C).
Wash: Rinse the BIOCHIP slides with a flush of PBS-Tween using a beaker and immerse them immediately afterwards in a cuvette containing PBS-Tween for at least 5 min. Shake with a rotary shaker if available. Wash max. 16 slides, then replace PBS-Tween with new buffer.
Pipette: Apply 25 µl of fluorescein labelled anti-human globulin to each reaction field of a clean reagent tray. Add all droplets before continuing incubation. Use a stepper pipette. The labelled anti-human serum should be mixed thoroughly before use. To save time, conjugate can be pipetted onto separate reagent trays during the incu-bation with the diluted sample.
Incubate: Remove one BIOCHIP slide from cuvette. Within five seconds blot only the back and the long sides with a paper towel and immediately put the BIOCHIP slide into the recesses of the reagent tray. Do not dry the areas between the reaction fields. Check for correct contact between the BIOCHIPs and liquids. Then continue with the next BIOCHIP slide. From now on, protect the slides from direct sunlight.
Incubate for 30 min at room temperature (+18°C to +25°C).
Wash: Fill cuvette with new PBS-Tween. Rinse the BIOCHIP slides with a flush of PBS-Tween using a beaker and put them into the cuvette filled with the new PBS-Tween for at least 5 min. Shake with a rotary shaker if available. Wash max. 16 slides, then replace PBS-Tween with new buffer.
Mount: Place mounting medium onto a cover glass – drops of max. 10 µl per reaction field. Use a polystyrene mounting tray. Remove one BIOCHIP slide from PBS-Tween and dry the back and all four sides with a paper towel. Put the BIOCHIP slide, with the BIOCHIPs facing downwards, onto the prepared cover glass. Check immediately that the cover glass is properly fitted into the recesses of the slide. Correct the position if necessary.
Evaluate: Read the fluorescence with the microscope. General recommendation: objective 20x (tissue sections, infected and transfected
cells), 40x (cell substrates). Excitation filter: 450-490 nm, colour separator: 510 nm, blocking filter: 515 nm.
Light source: mercury vapour lamp, 100 W, EUROIMMUN LED, EUROStar Bluelight.
3
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
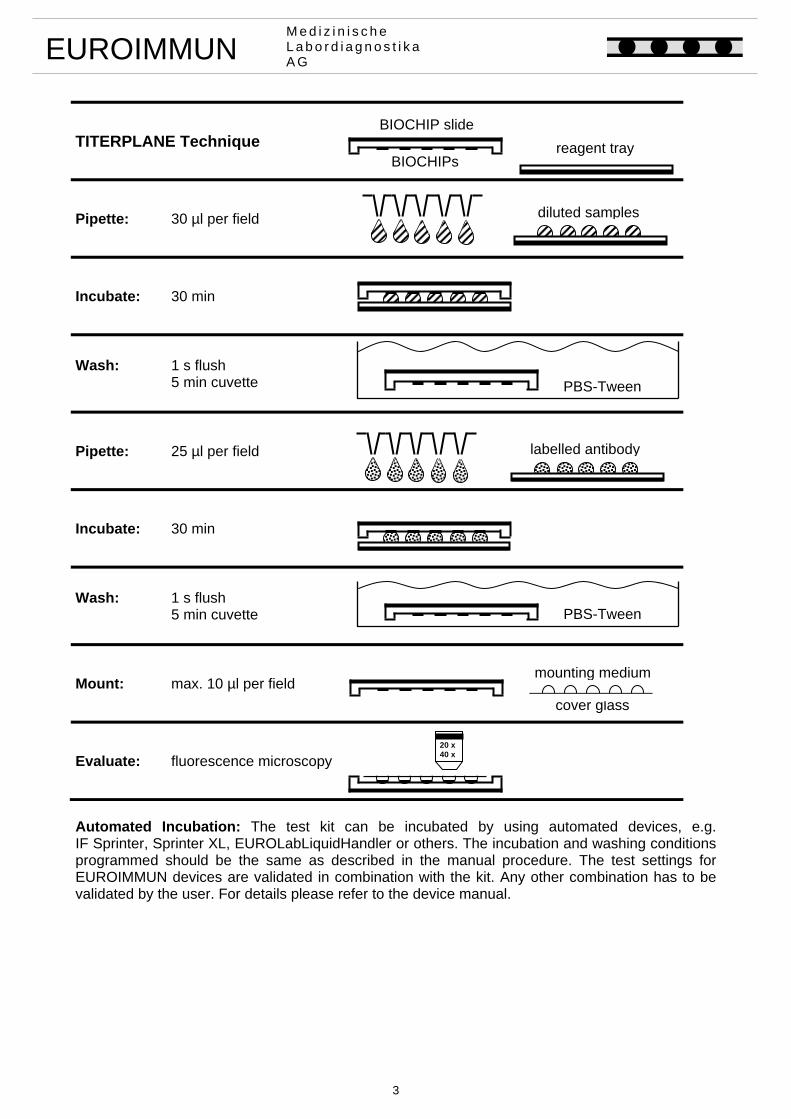
TITERPLANE Technique
Pipette: 30 µl per field
Incubate: 30 min
Wash: 1 s flush 5 min cuvette
Pipette: 25 µl per field
Incubate: 30 min
Wash: 1 s flush 5 min cuvette
Mount: max. 10 µl per field
Evaluate: fluorescence microscopy
Automated Incubation: The test kit can be incubated by using automated devices, e.g. IF Sprinter, Sprinter XL, EUROLabLiquidHandler or others. The incubation and washing conditions programmed should be the same as described in the manual procedure. The test settings for EUROIMMUN devices are validated in combination with the kit. Any other combination has to be validated by the user. For details please refer to the device manual.
20 x40 x
diluted samples
labelled antibody
PBS-Tween
cover glass
PBS-Tween
BIOCHIP slide
BIOCHIPsreagent tray
mounting medium
4
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
Preparation and stability of reagents Note: After initial opening, the reagents are stable until the expiry date when stored between +2°C and +8°C and protected from contamination, unless stated otherwise below. - Slides: Ready for use. Remove the protective cover only when the slides have reached room
temperature (+18°C up to +25°C; condensed water can damage the substrate). Do not touch the BIOCHIPs. If the protective cover is damaged, the slide must not be used for diagnostics.
- Fluorescein-labelled secondary antibody (FITC): Ready for use. Before using for the first
time, mix thoroughly. The conjugate is sensitive to light. Protect from sunlight . - Positive and negative controls: Ready for use. Before using for the first time, mix thoroughly.
Positive control with titer information: The label contains the target value and the substrate used to determine the target value. The lower tolerance limit is one titer level below the target value, the upper tolerance limit lies two titer levels above the target value. The control is to be diluted with PBS-Tween. Diluted controls must be incubated within one working day.
- PBS-Tween: 1 pack of “Salt for PBS” should be dissolved in 1 liter of distilled water (optimal:
aqua pro infusione, aqua ad injectabilia) and mixed with 2 ml of Tween 20 (stir for 20 min until homogeneous). The prepared PBS-Tween can be stored at +2°C to +8°C, generally for 1 week. PBS-Tween should not be used if the solution becomes cloudy or contamination appears.
- Mounting medium: Ready for use. - Reagent trays: Reaction fields of the reagent tray must be hydrophilic and surrounding area
hydrophobic. If necessary, leave in 2% Deconex 11 universal (EUROIMMUN order number: ZZ 9912-0101) for 12 hours. Afterwards rinse generously with water and dry. Cleaning: Rub reagent trays with 5% Extran MA 01 (EUROIMMUN order number: ZZ 9911-0130) and rinse with plenty of water. To disinfect: Spray reagent trays generously with Mikrozid (EUROIMMUN order number: ZZ 9921-0125), turn over and leave for 5 minutes. Afterwards, rinse generously with water and dry.
Warning: The BIOCHIPs coated with antigen substrates have been treated with a disinfecting fixing agent. Neither HBsAg nor antibodies against HIV-1, HIV-2, and HCV could be detected in the control sera using appropriate ELISA or indirect immunofluorescence tests. Nevertheless, all test system components should be handled as potentially infectious materials. Some of the reagents also contain the agent sodium azide in a non-declarable concentration. Avoid skin contact.
Preparation and stability of serum and plasma samples Samples: Human sera or EDTA, heparin or citrate plasma. Stability: The patient samples to be investigated can generally be stored up to 14 days at a temperature between +2°C and +8°C. Diluted samples must be incubated within one working day. Recommended sample dilution for qualitative evaluation: The sample to be investigated is diluted 1:10 in PBS-Tween. For example, dilute 11.1 µl sample in 100 µl PBS-Tween and mix thoroughly, e.g., vortex for 4 seconds. Recommended sample dilution for semiquantitative evaluation: The dilution of samples to be investigated is performed using PBS-Tween. Add 100 µl of PBS-Tween to each tube and mix with 11.1 µl of the next highest concentration, e.g. vortex for 2 seconds. EUROIMMUN recommends incubating samples from a dilution of 1:10.
5
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
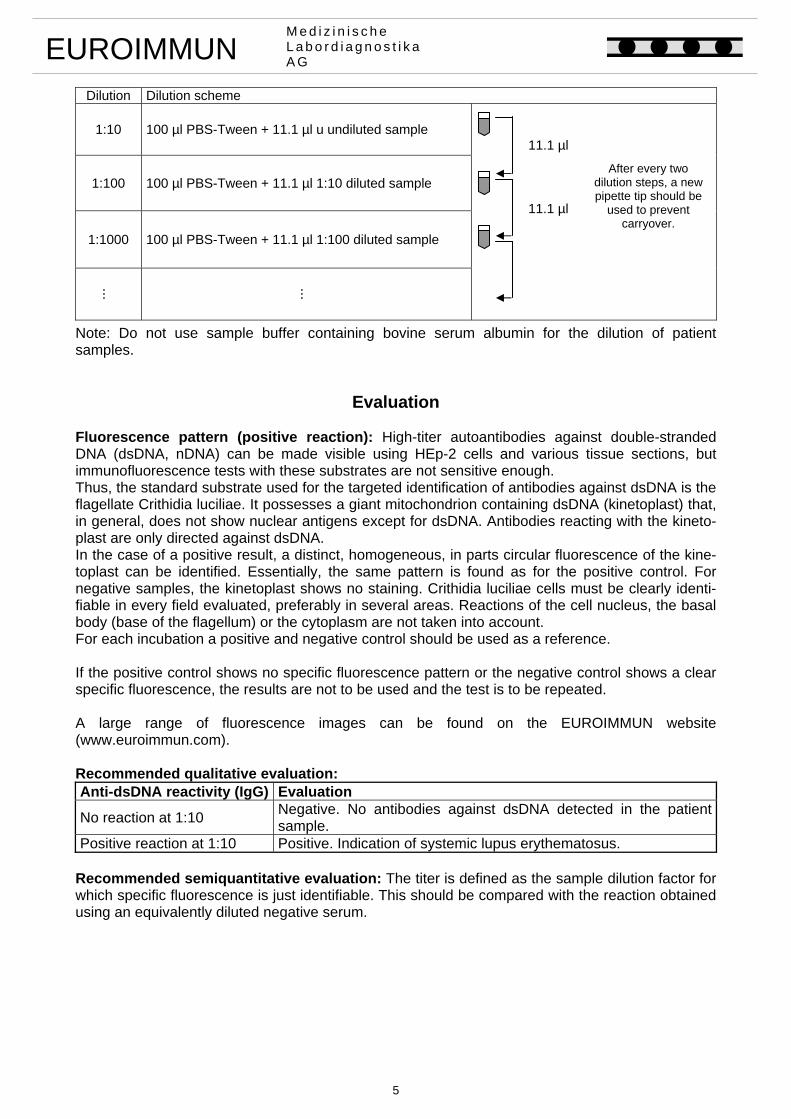
Dilution Dilution scheme
1:10
100 µl PBS-Tween + 11.1 µl u undiluted sample
1:100
100 µl PBS-Tween + 11.1 µl 1:10 diluted sample
1:1000
100 µl PBS-Tween + 11.1 µl 1:100 diluted sample
...
...
Note: Do not use sample buffer containing bovine serum albumin for the dilution of patient samples.
Evaluation Fluorescence pattern (positive reaction): High-titer autoantibodies against double-stranded DNA (dsDNA, nDNA) can be made visible using HEp-2 cells and various tissue sections, but immunofluorescence tests with these substrates are not sensitive enough. Thus, the standard substrate used for the targeted identification of antibodies against dsDNA is the flagellate Crithidia luciliae. It possesses a giant mitochondrion containing dsDNA (kinetoplast) that, in general, does not show nuclear antigens except for dsDNA. Antibodies reacting with the kineto-plast are only directed against dsDNA. In the case of a positive result, a distinct, homogeneous, in parts circular fluorescence of the kine-toplast can be identified. Essentially, the same pattern is found as for the positive control. For negative samples, the kinetoplast shows no staining. Crithidia luciliae cells must be clearly identi-fiable in every field evaluated, preferably in several areas. Reactions of the cell nucleus, the basal body (base of the flagellum) or the cytoplasm are not taken into account. For each incubation a positive and negative control should be used as a reference. If the positive control shows no specific fluorescence pattern or the negative control shows a clear specific fluorescence, the results are not to be used and the test is to be repeated. A large range of fluorescence images can be found on the EUROIMMUN website (www.euroimmun.com). Recommended qualitative evaluation: Anti-dsDNA reactivity (IgG) Evaluation
No reaction at 1:10 Negative. No antibodies against dsDNA detected in the patient sample.
Positive reaction at 1:10 Positive. Indication of systemic lupus erythematosus. Recommended semiquantitative evaluation: The titer is defined as the sample dilution factor for which specific fluorescence is just identifiable. This should be compared with the reaction obtained using an equivalently diluted negative serum.
After every two
dilution steps, a new pipette tip should be
used to prevent carryover.
11.1 µl
11.1 µl
6
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
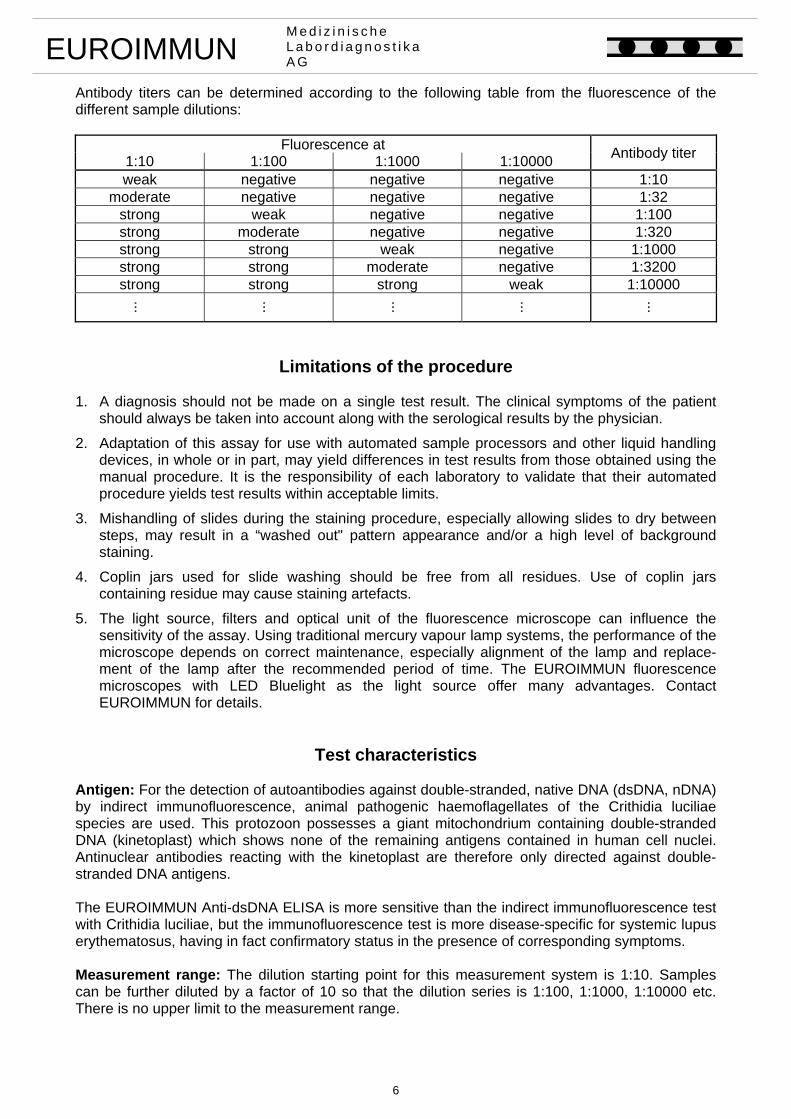
Antibody titers can be determined according to the following table from the fluorescence of the different sample dilutions:
Fluorescence at Antibody titer
1:10 1:100 1:1000 1:10000 weak negative negative negative 1:10
moderate negative negative negative 1:32 strong weak negative negative 1:100 strong moderate negative negative 1:320 strong strong weak negative 1:1000 strong strong moderate negative 1:3200 strong strong strong weak 1:10000
...
...
...
...
...
Limitations of the procedure 1. A diagnosis should not be made on a single test result. The clinical symptoms of the patient
should always be taken into account along with the serological results by the physician.
2. Adaptation of this assay for use with automated sample processors and other liquid handling devices, in whole or in part, may yield differences in test results from those obtained using the manual procedure. It is the responsibility of each laboratory to validate that their automated procedure yields test results within acceptable limits.
3. Mishandling of slides during the staining procedure, especially allowing slides to dry between steps, may result in a “washed out" pattern appearance and/or a high level of background staining.
4. Coplin jars used for slide washing should be free from all residues. Use of coplin jars containing residue may cause staining artefacts.
5. The light source, filters and optical unit of the fluorescence microscope can influence the sensitivity of the assay. Using traditional mercury vapour lamp systems, the performance of the microscope depends on correct maintenance, especially alignment of the lamp and replace-ment of the lamp after the recommended period of time. The EUROIMMUN fluorescence microscopes with LED Bluelight as the light source offer many advantages. Contact EUROIMMUN for details.
Test characteristics Antigen: For the detection of autoantibodies against double-stranded, native DNA (dsDNA, nDNA) by indirect immunofluorescence, animal pathogenic haemoflagellates of the Crithidia luciliae species are used. This protozoon possesses a giant mitochondrium containing double-stranded DNA (kinetoplast) which shows none of the remaining antigens contained in human cell nuclei. Antinuclear antibodies reacting with the kinetoplast are therefore only directed against double-stranded DNA antigens. The EUROIMMUN Anti-dsDNA ELISA is more sensitive than the indirect immunofluorescence test with Crithidia luciliae, but the immunofluorescence test is more disease-specific for systemic lupus erythematosus, having in fact confirmatory status in the presence of corresponding symptoms. Measurement range: The dilution starting point for this measurement system is 1:10. Samples can be further diluted by a factor of 10 so that the dilution series is 1:100, 1:1000, 1:10000 etc. There is no upper limit to the measurement range.
7
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
Reproducibility: The intensity of the specific fluorescence as a numeric value is called fluorescence intensity level by EUROIMMUN. These values can reach from “0” (no specific fluorescence) to “5” (extremely strong specific fluorescence).
Reproducibility Inter-lot Intra-assay Inter-assay
Minimum requirement
3 lots x 3 samples x 1 run x single determination:
max. ± 1 intensity level
1 lot x 3 samples x 1 run x tenfold determination:
max. ± 1 intensity level
1 lot x 3 samples x 2 runs x double
determination: max. ± 1 intensity level
Crithidia luciliae: Maximum deviation ± 1 intensity level
Maximum deviation ± 1 intensity level
Maximum deviation ± 1 intensity level.
Cross reactivity: Cross reactivities were investigated with two panels (anti-ssDNA positive sera n = 28, and anti-histone IgG positive sera n = 20). In both panels, no cross reactivities with Crithidia luciliae were found. Interference: Haemolytic, lipaemic and icteric samples showed no influences on analysis results. Reference range: Titer 1: < 10 The following antibody prevalences were determined using a panel of samples from healthy blood donors (origin: Germany):
Substrate Antibodies
against Conjugate Prevalence Cut-off
Number of samples
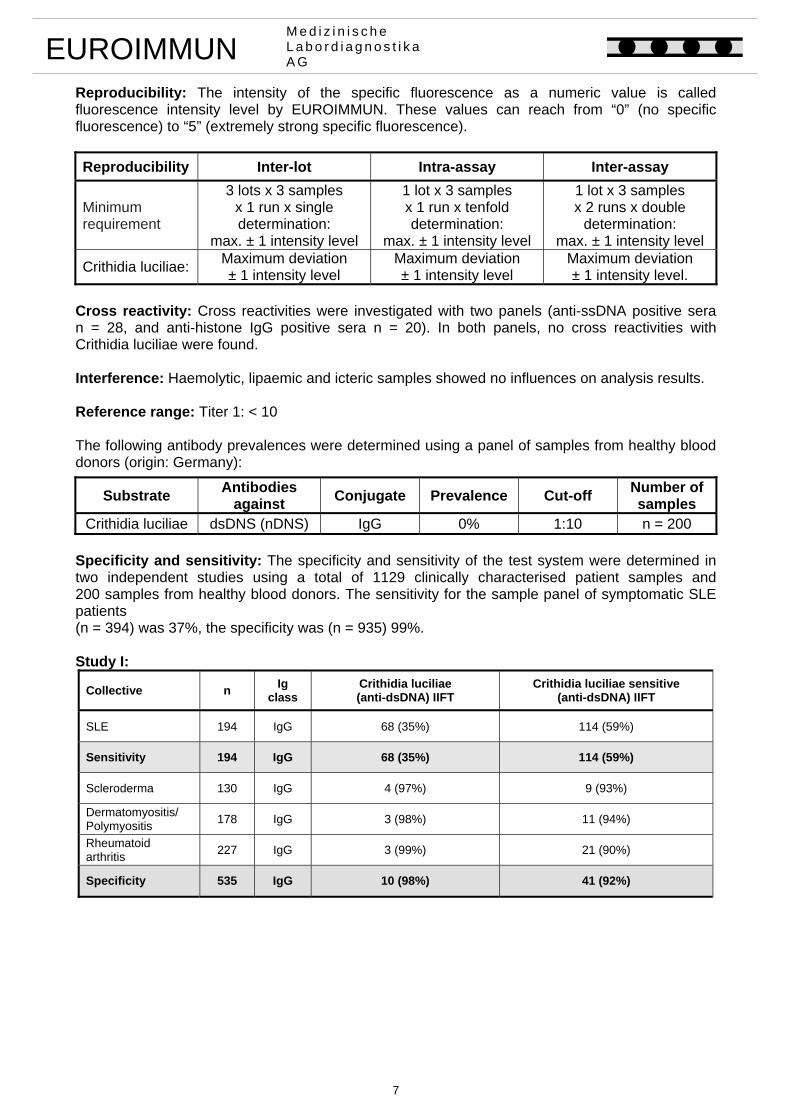
Crithidia luciliae dsDNS (nDNS) IgG 0% 1:10 n = 200 Specificity and sensitivity: The specificity and sensitivity of the test system were determined in two independent studies using a total of 1129 clinically characterised patient samples and 200 samples from healthy blood donors. The sensitivity for the sample panel of symptomatic SLE patients (n = 394) was 37%, the specificity was (n = 935) 99%. Study I:
Collective n Ig
class Crithidia luciliae (anti-dsDNA) IIFT
Crithidia luciliae sensitive (anti-dsDNA) IIFT
SLE 194 IgG 68 (35%) 114 (59%)
Sensitivity 194 IgG 68 (35%) 114 (59%)
Scleroderma 130 IgG 4 (97%) 9 (93%)
Dermatomyositis/ Polymyositis
178 IgG 3 (98%) 11 (94%)
Rheumatoid arthritis
227 IgG 3 (99%) 21 (90%)
Specificity 535 IgG 10 (98%) 41 (92%)
8
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
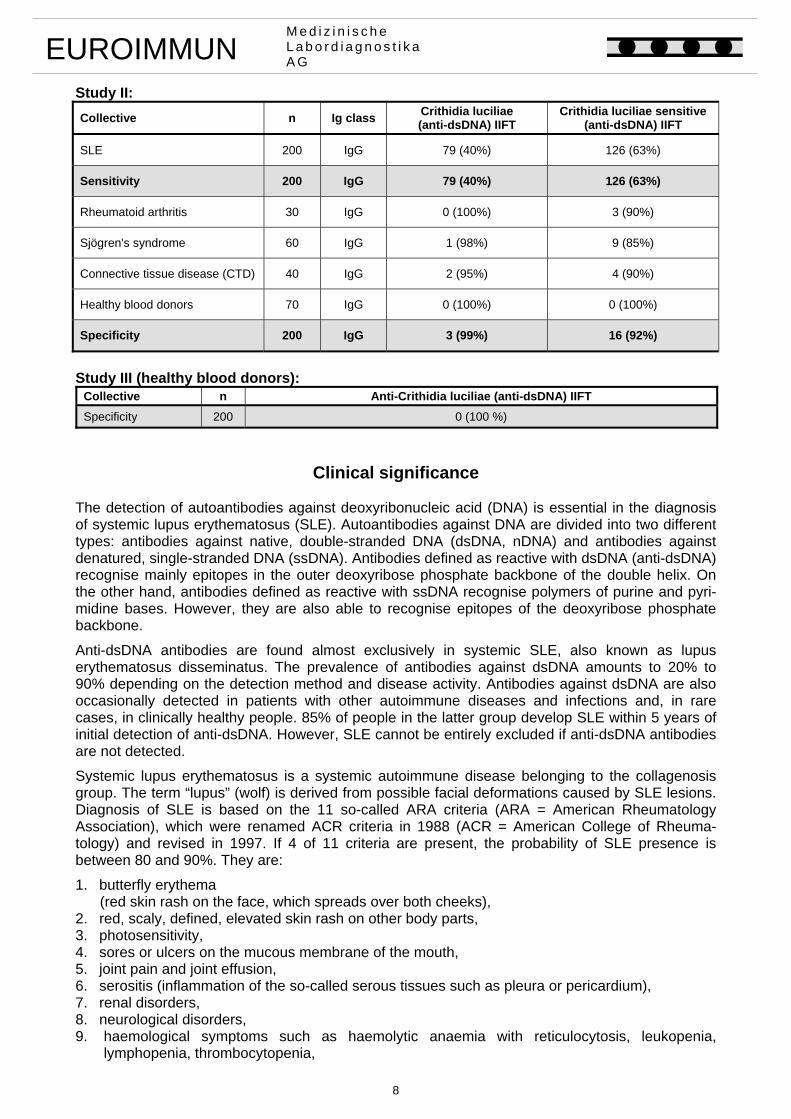
Study II:
Collective n Ig class Crithidia luciliae (anti-dsDNA) IIFT
Crithidia luciliae sensitive(anti-dsDNA) IIFT
SLE 200 IgG 79 (40%) 126 (63%)
Sensitivity 200 IgG 79 (40%) 126 (63%)
Rheumatoid arthritis 30 IgG 0 (100%) 3 (90%)
Sjögren's syndrome 60 IgG 1 (98%) 9 (85%)
Connective tissue disease (CTD) 40 IgG 2 (95%) 4 (90%)
Healthy blood donors 70 IgG 0 (100%) 0 (100%)
Specificity 200 IgG 3 (99%) 16 (92%)
Study III (healthy blood donors):
Collective n Anti-Crithidia luciliae (anti-dsDNA) IIFT
Specificity 200 0 (100 %)
Clinical significance The detection of autoantibodies against deoxyribonucleic acid (DNA) is essential in the diagnosis of systemic lupus erythematosus (SLE). Autoantibodies against DNA are divided into two different types: antibodies against native, double-stranded DNA (dsDNA, nDNA) and antibodies against denatured, single-stranded DNA (ssDNA). Antibodies defined as reactive with dsDNA (anti-dsDNA) recognise mainly epitopes in the outer deoxyribose phosphate backbone of the double helix. On the other hand, antibodies defined as reactive with ssDNA recognise polymers of purine and pyri-midine bases. However, they are also able to recognise epitopes of the deoxyribose phosphate backbone.
Anti-dsDNA antibodies are found almost exclusively in systemic SLE, also known as lupus erythematosus disseminatus. The prevalence of antibodies against dsDNA amounts to 20% to 90% depending on the detection method and disease activity. Antibodies against dsDNA are also occasionally detected in patients with other autoimmune diseases and infections and, in rare cases, in clinically healthy people. 85% of people in the latter group develop SLE within 5 years of initial detection of anti-dsDNA. However, SLE cannot be entirely excluded if anti-dsDNA antibodies are not detected.
Systemic lupus erythematosus is a systemic autoimmune disease belonging to the collagenosis group. The term “lupus” (wolf) is derived from possible facial deformations caused by SLE lesions. Diagnosis of SLE is based on the 11 so-called ARA criteria (ARA = American Rheumatology Association), which were renamed ACR criteria in 1988 (ACR = American College of Rheuma-tology) and revised in 1997. If 4 of 11 criteria are present, the probability of SLE presence is between 80 and 90%. They are:
1. butterfly erythema (red skin rash on the face, which spreads over both cheeks), 2. red, scaly, defined, elevated skin rash on other body parts, 3. photosensitivity, 4. sores or ulcers on the mucous membrane of the mouth, 5. joint pain and joint effusion, 6. serositis (inflammation of the so-called serous tissues such as pleura or pericardium), 7. renal disorders, 8. neurological disorders, 9. haemological symptoms such as haemolytic anaemia with reticulocytosis, leukopenia, lymphopenia, thrombocytopenia,
9
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
10. immunological finds such as dsDNA antibodies, Sm antibodies, anti-cardiolipin antibodies (ACA), 11. ANA in IIFT.
The disease was first described by P. L. A. Cazenave in 1851. According to estimations, approxi-mately 40,000 people, particularly young women of child-bearing age, suffer from SLE in Germany. The incidence of SLE in Europe amounts to 25 to 27 new cases per 100,000 persons a year; the number is higher in the US. The probability for SLE patients to survive for more than 5 years is 95% and 85% for 10 years.
It is known to a large extent that anti-DNA antibodies play a role in the pathogenesis of SLE. During the course of disease, immunocomplexes of double-stranded DNA and the corresponding autoantibodies are deposited in the capillaries of the subcutis, the kidneys and other organs. Here they cause organ damage via activation of the complement system. There is increasing evidence that the primary target antigen of the pathogenically relevant autoantibodies is not “naked” DNA, but DNA complexed with nucleosomes.
Serological testing is of particular significance within the frame of the ACR criteria. Antibodies against dsDNA are among the most important criteria for diagnosis of SLE due to their high specificity: 70% to 98% depending on the method of detection. Since the concentration of these antibodies correlates with the disease activity, particularly with the activity of lupus nephritis, titer determinations are suitable for monitoring therapy.
For routine detection of autoantibodies against dsDNA, three test methods are currently available: enzyme immunoassays (ELISA, EUROASSAY, EUROLINE), Farr RIA and Crithidia luciliae immunofluorescence test. Since these diagnostic methods, which detect different autoantibody fractions, vary in sensitivity and specificity, many laboratories prefer a combination of two or three tests for supplementation or confirmation of diagnostic results in SLE diagnosis.
In the Crithidia luciliae dsDNA IIFT animal pathogenic haemoflagellates of Crithidia luciliae are used for the detection of autoantibodies against double-stranded, native DNA (dsDNA, nDNA). These monocellular flagellates possess a giant mitochondrion containing dsDNA (kinetoplast) that, in general, does not show any of the other antigens present in the cell nuclei. For this reason, anti-bodies reacting with the kinetoplast are only directed against dsDNA antigens. A fluorescence of the entire Crithidia cell or the cell nucleus or basal body alone is to be evaluated as anti-dsDNA negative. A positive reaction produces a homogeneous fluorescence of the kinetoplast or of both the nucleus and kinetoplast. Cross reactions of other antibodies with the specific antigen structure are unknown. Due to its specificity for the disease, the present Crithidia luciliae dsDNA IIFT allows reliable diagnosis of SLE in patients showing the respective symptoms. For monitoring the disease activity of SLE the Anti-dsDNA ELISA is recommended.
A high concentration of autoantibodies against dsDNA in Farr RIA is considered a very reliable marker for the diagnosis of SLE. The changes in the concentration of antibodies against dsDNA correlate with the activity of SLE and are therefore a useful prognostic marker for the disease.
Another test for the serological diagnosis of SLE should also be mentioned. A new anti-dsDNA ELISA that exceeds the diagnostic quality criteria of the Farr assay (Anti-dsDNA RIA) has now been developed (Anti-dsDNA(NcX) ELISA) using an innovative biochemical preparation. The antigen substrate consists of dsDNA coupled with nucleosomes (NcX) to the solid phase. Highest SLE specificity is ensured through use of a wafer-thin layer of a highly purified nucleosome fraction, which is free of H1, Scl-70 and other non-histone proteins. In contrast to conventional anti-dsDNA ELISA the use of linker substances such as poly-L-lysine or protamine sulphate, which represent a potential source of unspecific reactions, is not necessary.
The Anti-dsDNA-NcX ELISA provides a semiquantitative or quantitative in vitro assay for human autoantibodies of the immunoglobulin class IgG against double-stranded, genomic DNA (dsDNA) from serum or plasma. The test is not only very useful as a prognostic marker for SLE but also as a means for monitoring the activity of the disease.
10
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
As can be seen from the variety of ACR criteria, the collagenosis SLE manifests itself in many different ways. It must be taken into consideration that other serologically detectable autoantibodies may be responsible for the individual picture of the disease in addition to anti-dsDNA. Therefore, antibodies against nucleosomes, Sm, nRNP/Sm (U1-nRNP), SS-A (Ro), SS-B (La), ribosomal P-proteins and against other antigens of the cell nucleus should also be investigated.
Literature references 1. Aarden LA, de Groot ER, Feltkamp TEW. Immunology of DNA. III. Crithidia luciliae, a
simple substrate for the determination of anti-dsDNA with the immunofluorescence technique. Annals New York Academy of Sciences 254 (1975) 505-515.
2. Bruns A, Blass S, Hausdorf G, Burmester GR, Hiepe F. Nucleosomes are major T and B cell autoantigens in systemic lupus erythematosus. Arthritis Rheum 43 (2000) 2307-2315.
3. Crowe W, Kushner I. An immunofluorescent method using Crithidia luciliae to detect antibodies to double-stranded DNA. Arthritis and Rheumatism 20 (1977) 811-814.
4. EUROIMMUN AG. Stöcker W, Schlumberger W, Krüger C. Alle Beiträge zum Thema Auto-immundiagnostik. In: Gressner A, Arndt T (Hrsg.) Lexikon der Medizinischen Laboratoriums-diagnostik. 2. Auflage. Springer Medizin Verlag, Heidelberg (2012).
5. EUROIMMUN AG. Suer W, Dähnrich C, Schlumberger W, Stöcker W. Autoantibodies in SLE but not in scleroderma react with protein-stripped nucleosomes. J Autoimmun 22 (2004) 325-334.
6. Haugbro K, Nossent JC, Winkler T, Figenschau Y, Rekvig OP. Anti-dsDNA antibodies and disease classification in antinuclear antibody positive patients: the role of analytical diversity. Ann Rheum Dis 63 (2004) 386-394.
7. Herrmann M, Voll R, Kalden VR. Etiopathogenesis of systemic lupus erythematosus. Immunol Today 21 (2000) 424-426.
8. Hoffman IE, Peene I, Meheus L, Huizinga TW, Cebecauer L, Isenberg D, De Bosschere K, Hulstaert F, Veys EM, De Keyser F. Specific antinuclear antibodies are associated with clinical features in systemic lupus erythematosus. Ann Rheum Dis 63 (2004) 1155-1158.
9. Linnik MD, Hu JZ, Heilbrunn KR, Strand V, Hurley FL, Joh T. Relationship between anti-double-stranded DNA antibodies and exacerbation of renal disease in patients with systemic lupus erythematosus. Arthritis Rheum 52 (2005) 1129-1137.
10. Makowski GS, Ramsby ML. Selective detection of autoimmune antibodies to single- and double-stranded DNA by enzyme immunoassay. Ann Clin Lab Sci 33 (2003) 142-148.
11. Nossent HC, Rekvig OP. Is closer linkage between systemic lupus erythematosus and anti-double-stranded DNA antibodies a desirable and attainable goal? Arthritis Res Ther 7 (2005) 85-87.
12. Sontheimer RD, Gilliam JN. An immunofluorescence assay for double-stranded DNA anti-bodies using the Crithidia luciliae kinetoplast as a double-stranded DNA substrate. J Lab Clin Med 91 (1978) 550-558.
13. Stinton LM, Barr SG, Tibbles LA, Yilmaz S, Sar A, Benedikttson H, Fritzler MJ. Autoantibodies in lupus nephritis patients requiring renal transplantation. Lupus 15 (2007) 394-400.

11
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
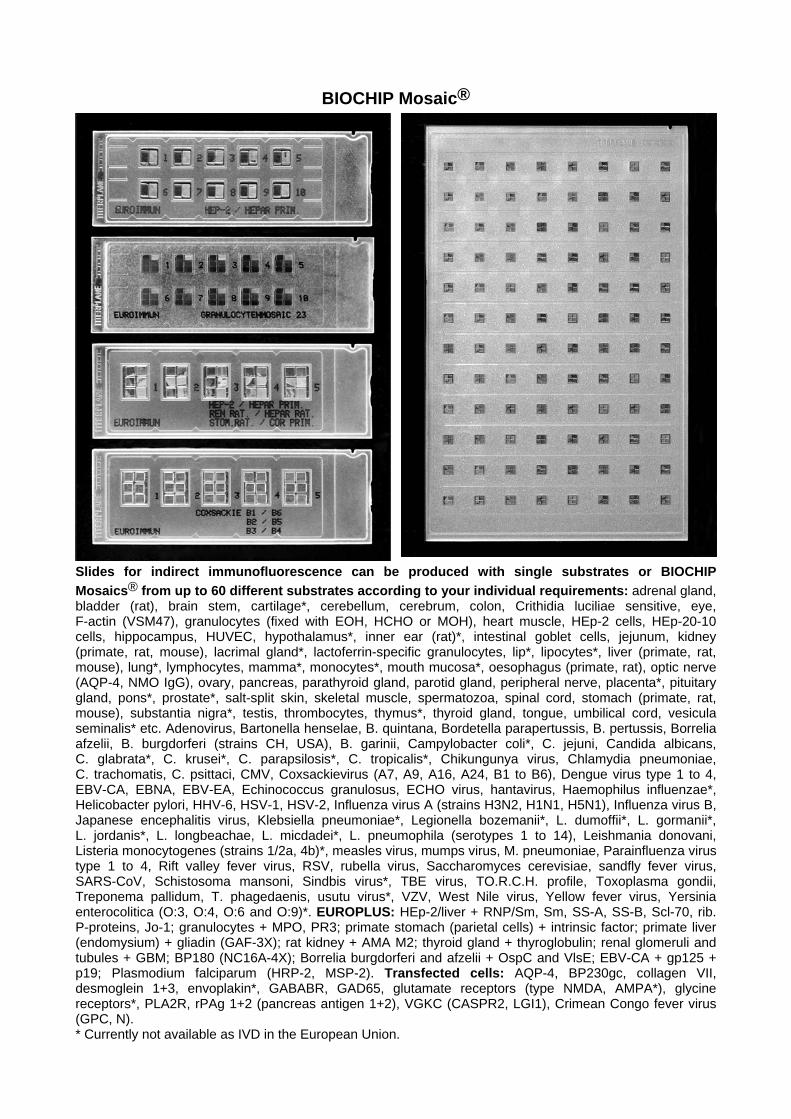
BIOCHIP Mosaic®
Slides for indirect immunofluorescence can be produced with single substrates or BIOCHIP
Mosaics® from up to 60 different substrates according to your individual requirements: adrenal gland, bladder (rat), brain stem, cartilage*, cerebellum, cerebrum, colon, Crithidia luciliae sensitive, eye, F-actin (VSM47), granulocytes (fixed with EOH, HCHO or MOH), heart muscle, HEp-2 cells, HEp-20-10 cells, hippocampus, HUVEC, hypothalamus*, inner ear (rat)*, intestinal goblet cells, jejunum, kidney (primate, rat, mouse), lacrimal gland*, lactoferrin-specific granulocytes, lip*, lipocytes*, liver (primate, rat, mouse), lung*, lymphocytes, mamma*, monocytes*, mouth mucosa*, oesophagus (primate, rat), optic nerve (AQP-4, NMO IgG), ovary, pancreas, parathyroid gland, parotid gland, peripheral nerve, placenta*, pituitary gland, pons*, prostate*, salt-split skin, skeletal muscle, spermatozoa, spinal cord, stomach (primate, rat, mouse), substantia nigra*, testis, thrombocytes, thymus*, thyroid gland, tongue, umbilical cord, vesicula seminalis* etc. Adenovirus, Bartonella henselae, B. quintana, Bordetella parapertussis, B. pertussis, Borrelia afzelii, B. burgdorferi (strains CH, USA), B. garinii, Campylobacter coli*, C. jejuni, Candida albicans, C. glabrata*, C. krusei*, C. parapsilosis*, C. tropicalis*, Chikungunya virus, Chlamydia pneumoniae, C. trachomatis, C. psittaci, CMV, Coxsackievirus (A7, A9, A16, A24, B1 to B6), Dengue virus type 1 to 4, EBV-CA, EBNA, EBV-EA, Echinococcus granulosus, ECHO virus, hantavirus, Haemophilus influenzae*, Helicobacter pylori, HHV-6, HSV-1, HSV-2, Influenza virus A (strains H3N2, H1N1, H5N1), Influenza virus B, Japanese encephalitis virus, Klebsiella pneumoniae*, Legionella bozemanii*, L. dumoffii*, L. gormanii*, L. jordanis*, L. longbeachae, L. micdadei*, L. pneumophila (serotypes 1 to 14), Leishmania donovani, Listeria monocytogenes (strains 1/2a, 4b)*, measles virus, mumps virus, M. pneumoniae, Parainfluenza virus type 1 to 4, Rift valley fever virus, RSV, rubella virus, Saccharomyces cerevisiae, sandfly fever virus, SARS-CoV, Schistosoma mansoni, Sindbis virus*, TBE virus, TO.R.C.H. profile, Toxoplasma gondii, Treponema pallidum, T. phagedaenis, usutu virus*, VZV, West Nile virus, Yellow fever virus, Yersinia enterocolitica (O:3, O:4, O:6 and O:9)*. EUROPLUS: HEp-2/liver + RNP/Sm, Sm, SS-A, SS-B, Scl-70, rib. P-proteins, Jo-1; granulocytes + MPO, PR3; primate stomach (parietal cells) + intrinsic factor; primate liver (endomysium) + gliadin (GAF-3X); rat kidney + AMA M2; thyroid gland + thyroglobulin; renal glomeruli and tubules + GBM; BP180 (NC16A-4X); Borrelia burgdorferi and afzelii + OspC and VlsE; EBV-CA + gp125 + p19; Plasmodium falciparum (HRP-2, MSP-2). Transfected cells: AQP-4, BP230gc, collagen VII, desmoglein 1+3, envoplakin*, GABABR, GAD65, glutamate receptors (type NMDA, AMPA*), glycine receptors*, PLA2R, rPAg 1+2 (pancreas antigen 1+2), VGKC (CASPR2, LGI1), Crimean Congo fever virus (GPC, N). * Currently not available as IVD in the European Union.





















