Embed Size (px)
Citation preview

Full Terms & Conditions of access and use can be found athttp://www.tandfonline.com/action/journalInformation?journalCode=ycra20
Download by: [Deborah Wardly] Date: 01 July 2016, At: 23:25
CRANIO®The Journal of Craniomandibular & Sleep Practice
ISSN: 0886-9634 (Print) 2151-0903 (Online) Journal homepage: http://www.tandfonline.com/loi/ycra20
Idiopathic intracranial hypertension eliminatedby counterclockwise maxillomandibularadvancement: a case report
Deborah Wardly , Larry M. Wolford & Venkat Veerappan
To cite this article: Deborah Wardly , Larry M. Wolford & Venkat Veerappan (2016): Idiopathicintracranial hypertension eliminated by counterclockwise maxillomandibular advancement: acase report, CRANIO®, DOI: 10.1080/08869634.2016.1201634
To link to this article: http://dx.doi.org/10.1080/08869634.2016.1201634
Published online: 01 Jul 2016.
Submit your article to this journal
View related articles
View Crossmark data

1
Case Report
Idiopathic intracranial hypertension eliminated by counterclockwise maxillomandibular advancement: a case reportDeborah Wardly MD, FAAP1 , Larry M. Wolford DMD2,3,4 , Venkat Veerappan, MD5,6
1Independent, Department of Pediatrics, Las Vegas, NV, USA, 2Departments of Oral and Maxillofacial Surgery and Orthodontics, Texas A & M University Health Science Center, Baylor College of Dentistry, Dallas, TX, USA, 3Departments of Oral and Maxillofacial Surgery and Orthodontics, Baylor University Medical Center, Dallas, TX, USA, 4Private Practice, Dallas, TX, USA, 5Department of Neurology, Southern Hills Hospital, Las Vegas, NV, USA, 6Department of Neurology, Touro University, Las Vegas, NV, USA
Introduction: Obstructive sleep apnea (OSA) is a secondary cause of intracranial hypertension (IH). Decreased jugular venous drainage has been seen in patients with idiopathic IH.Clinical Presentation: A complex case of a 48-year-old female whose idiopathic IH was put into remission after counterclockwise maxillomandibular advancement (CC-MMA), despite persistence of her OSA.Conclusion: This case highlights the relationship between OSA and IH and points to the significant morbidity that can result from mild OSA and from what are considered borderline intracranial pressures. This indicates the need for a high index of suspicion for actual underlying pathology that can be surgically corrected when patients manifest symptoms of a somatic syndrome. This is the first report in the medical literature of clinical elimination of IH by CC-MMA. The authors propose that this positive outcome was effected via mandibular advancement producing a decrease in jugular venous resistance, allowing improved absorption of cerebrospinal fluid.
Keywords: Obstructive sleep apnea, Idiopathic intracranial hypertension, Maxillomandibular advancement, Multiple chemical sensitivity, Upper airway resistance syndrome, IIHWOP, Pseudotumor cerebri, Environmental intolerance
IntroductionIdiopathic intracranial hypertension (IIH) is a neurological disorder characterized by increased intracranial pressure (ICP) without the presence of a tumor or other diseases. The main signs and symptoms are headache, pulsatile tinnitus, diplopia, transient visual obscurations, and visual loss.1 Other symptoms seen are fatigue, memory and con-centration problems, dizziness, joint pains, and depres-sion,2 as well as nausea, neck, shoulder or back pain, photophobia, and phonophobia.3 It most commonly occurs in women of childbearing age, particularly with obesity.4 Common secondary etiologies of intracranial hyperten-sion include cerebral venous abnormalities, medications such as tetracyclines and retinoids, some endocrine disor-ders, obstructive sleep apnea, and renal failure.3
The modified Dandy Criteria are the standardized criteria by which idiopathic intracranial hypertension is classically diagnosed. They are: (1) signs and symptoms
of increased intracranial pressure; (2) no localizing signs except abducens nerve palsy; (3) CSF opening pres-sure ≥25 cm H2O with normal CSF composition; and (4) normal neuroimaging (ruling out venous sinus throm-bosis).5 The International Headache Society-2 criteria (ICHD-2 criteria) for a headache to be determined to be caused by IIH, are that the ICP must be greater than 20 cm H2O in the non-obese, and the headache must improve upon reduction of ICP by removal of CSF.2 The newly published ICHD-3 criteria state that the opening pressure must be greater than 25 cm H2O.6 However, a recent study by Higgins, et al.2 suggests that disorders of raised intrac-ranial pressure may begin at CSF pressures much lower than previously recognized, as will be discussed later.
Obstructive sleep apnea (OSA) is known to be asso-ciated with idiopathic intracranial hypertension (IIH) as well as to be a cause of papilledema, and it is known that apneas cause spikes in intracranial pressure (ICP).7–9 However, in practice, this does not seem to be widely recognized, and more attention needs to be brought to Correspondence to: Deborah Wardly, 7901 Autumn Gate Ave., Las
Vegas, NV 89131. Email: [email protected]
© 2016 Informa UK Limited, trading as Taylor & Francis GroupDOI 10.1080/08869634.2016.1201634 CRANIO®: The Journal of Craniomandibular & Sleep Practice 2016
Dow
nloa
ded
by [
Deb
orah
War
dly]
at 2
3:25
01
July
201
6

CRANIO®: The Journal of Craniomandibular & Sleep Practice 2016 2
Wardly et al. Idiopathic intracranial hypertension eliminated by counterclockwise maxillomandibular advancement
the relationship. Therefore, the authors are presenting this case report as an opportunity to discuss the issues involved in the relationship between OSA and IIH/ICP and to point out the need to increase awareness of these conditions. The authors also contend that counterclockwise maxillo-mandibular advancement surgery may be a novel surgical cure for the condition of idiopathic intracranial hyperten-sion, independent of its effect on OSA.
Intracranial hypertension and obstructive sleep apneaThe underlying cause of IIH is still largely unknown. There is evidence that obesity, delayed CSF absorption, and venous outflow abnormality with increased cerebral venous pressure are involved in the elevation of intracra-nial pressure in IIH.4 Increased central venous pressure in obesity is one hypothesis to explain the association of obesity with IIH.10 A pressure gradient from the ventricles to ultimately the right atrium of the heart is required for normal CSF absorption.11 Alperin et al.12 has shown that in a group of obese women with IIH, they manifested both increased interstitial fluid volume in the gray matter of the brain, and decreased jugular venous drainage. IIH has been demonstrated to be caused in some people by internal jugular venous compression in part by an elon-gated styloid process.13
Jennum and Børgeson7 first described the relation-ship between OSA and ICP. They showed that individual apneas might acutely elevate ICP as well as arterial pres-sure. In their patients with OSA, they demonstrated that more than half of them had elevated ICP while awake in the morning, and that the ICP in the morning was higher than it was in the evening. Their OSA patients’ ICP was higher during REM sleep, when more apneas occur. Hypercapnia and hypoxia may play a role in cerebral vasodilation to effect this increase in ICP via an increase in cerebral blood flow. An increase in arterial pressure and an increase in central venous pressure during apneas may also be contributing to the increase in ICP; however increased intrathoracic pressure at the termination of the apnea may also be involved.7 OSA has been associated with idiopathic intracranial hypertension (also called pseudotumor cerebri) as well as with papilledema. It has been shown that individuals with papilledema and IIH can improve with treatment of their OSA with continuous positive airway pressure (CPAP),8,9,14 and there is a recent case study demonstrating resolution of IIH in a child after adenotonsillectomy.15 However, there is very little in the literature documenting this. It has also been demonstrated that papilledema can occur in OSA even when ICP is nor-mal on lumbar punctures (LP) performed while the patient is awake. Purvin et al.16 showed that nocturnal monitoring
in one patient with papilledema indicated marked ICP elevation during apneas.
In this case study, the authors describe a 48-year-old woman who was diagnosed with both OSA and IIH. She underwent a surgical counterclockwise maxillomandibu-lar advancement procedure, achieved rapid clinical reso-lution of the majority of her symptoms of IIH following surgery, and was confirmed on LP performed 14 months after surgery to be in remission from her IIH.
Case reportA 44-year-old female developed sudden onset of near constant ‘brain fog.’ It was disabling, and described as beyond fatigue, but a feeling like one is deep underwater, like having the flu or a hangover. This alteration in her sensorium would come and go and was aggravated by chemical exposure. While she did have odor hypersen-sitivity, her symptoms could occur from chemical expo-sures in the absence of odor perception, and neurological changes from chemical exposure below odor threshold were confirmed on functional MRI testing. Hence, she was initially diagnosed with multiple chemical sensitivity (MCS). She had a long history of headaches diagnosed as migraines. The headaches were accompanied by brain fog and occasionally nausea, but no increase in photophobia or phonophobia. (Phonophobia developed slowly after age 45, became disabling, and was ultimately diagnosed as Meniere’s disease; however this auditory hypersen-sitivity did not fluctuate. Photophobia developed at age 36 concurrent with Graves’ ophthalmopathy and did not fluctuate.) The headaches were moderate and occasion-ally severe, and could be triggered by altitude changes, food sensitivities, and inhaled chemicals, as well as severe stress. By age 45, she had a very strong Valsalva trigger for the headaches: just starting to cry could trigger an ice pick-like headache that would leave her ill for 24 h. Shortly after the onset of the near constant brain fog, she developed chronic nausea that lasted six months, and sus-tained a 40 lb weight loss. Despite being thin, she con-tinued to have severe symptoms, which were ultimately diagnosed at age 47 as intracranial hypertension.
At age 45, she was diagnosed with OSA at Stanford University. Her AHI was 10.2 with a minimum oxygen desaturation to 91%. This was after two prior sleep studies in her home city failed to detect the OSA. An ophthal-mology exam was normal. At this point, she was having daytime airway symptoms that at times led her to gasp for air and become lightheaded, triggered by eating, only to resolve these symptoms with a tongue thrust out of the mouth. She was diagnosed with tongue collapse. At age 46, these daytime airway symptoms resolved completely after a midline glossectomy; however, her AHI on another
Dow
nloa
ded
by [
Deb
orah
War
dly]
at 2
3:25
01
July
201
6

CRANIO®: The Journal of Craniomandibular & Sleep Practice 2016 3
Wardly et al. Idiopathic intracranial hypertension eliminated by counterclockwise maxillomandibular advancement
sleep study at Stanford was 17 after the tongue surgery. She tried multiple different methods to treat the OSA, including auto-CPAP, CPAP, a tongue-retaining device, and a mandibular advancement device. The tongue- retaining device, when it stayed on without fail, worked well to prevent the brain fog and headaches, leading to the conclusion that the OSA was causing these symptoms. Auto-CPAP was poorly tolerated, and a CPAP of 8 helped somewhat but not completely; however it was more reli-able than the tongue-retaining device. The mandibular advancement device (MAD) did not resolve the apnea; her AHI was 6.7 using it, and while using it she had a near syncopal episode that required TIA (transient ischemic attack) workup. This episode was triggered by a Valsalva maneuver, and in the aftermath it was determined that a lumbar puncture (LP) should be performed.
The first lumbar puncture, done at age 47 (she was using a CPAP at night set at 8), showed a CSF opening pressure (OP) of 22 cm H2O, which was considered bor-derline but positive because she noted improvement in brain fog symptoms after removal of CSF. A repeat LP was performed after the patient stopped CPAP for several days, and the OP was 23 cm H2O. MRI studies showed that the patient had a doubling of CSF flow velocity when she did not use CPAP, compared to when she did. The brain MRI was otherwise normal. The neuroradiologist who performed the LPs noted that the patient’s speech became more rapid immediately after her LPs. The patient realized that she had intermittent situational pulsatile tin-nitus going back to the age of 36, which was around the time that her headaches worsened considerably and that she first noted symptoms upon chemical exposure. These symptoms did not become disabling until age 44, how-ever. (There were persistent symptoms at age 36 which were similar to the illness at age 44, but this appeared to go into remission immediately after a total thyroidectomy for Graves’ disease, leaving her with only intermittent symp-toms.) She attempted unsuccessfully to use acetazolamide for the IIH but did not tolerate more than 125 mg twice a day due to sedation, and therefore, was unable to attain a therapeutic level.
A CPAP titration was performed at Stanford, and she was titrated to a pressure of 12–13. However, at that pres-sure she experienced the expiratory pressure as a Valsalva, and after one night, she developed an episode of severe ICP symptoms including sudden weakness and inability to stand or walk. She changed to a Bi-level machine that allowed her to increase the inspiratory pressure without developing severe ICP symptoms but still did not feel normal. She concluded that she was failing all OSA treat-ments despite having only mild OSA that was triggering her IIH, and that she had failed medical management of the IIH, as she was unable to tolerate acetazolamide or
topiramate, and found furosemide inadequate. Prednisone worked to abort the symptoms triggered by OSA; however this is not acceptable as a long-term solution.
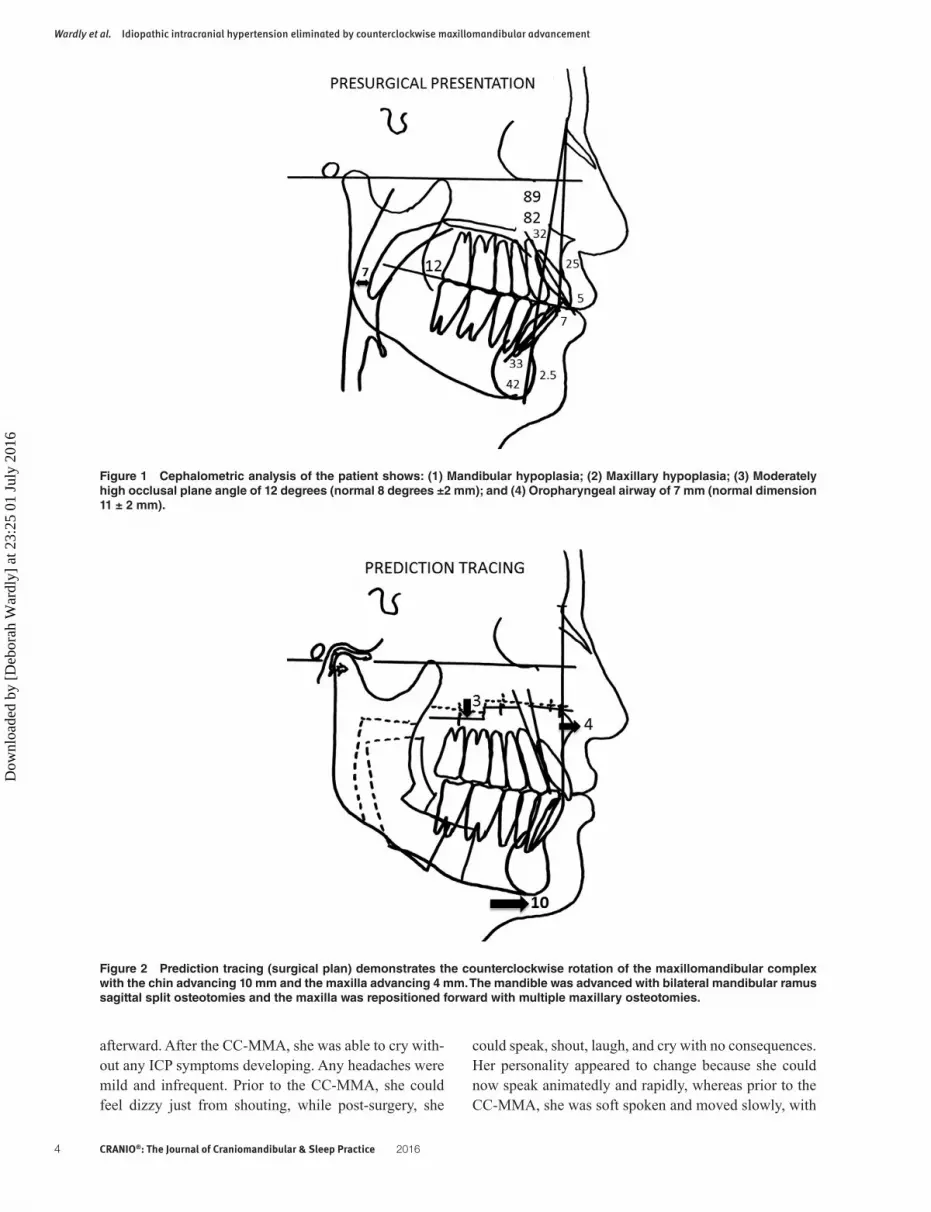
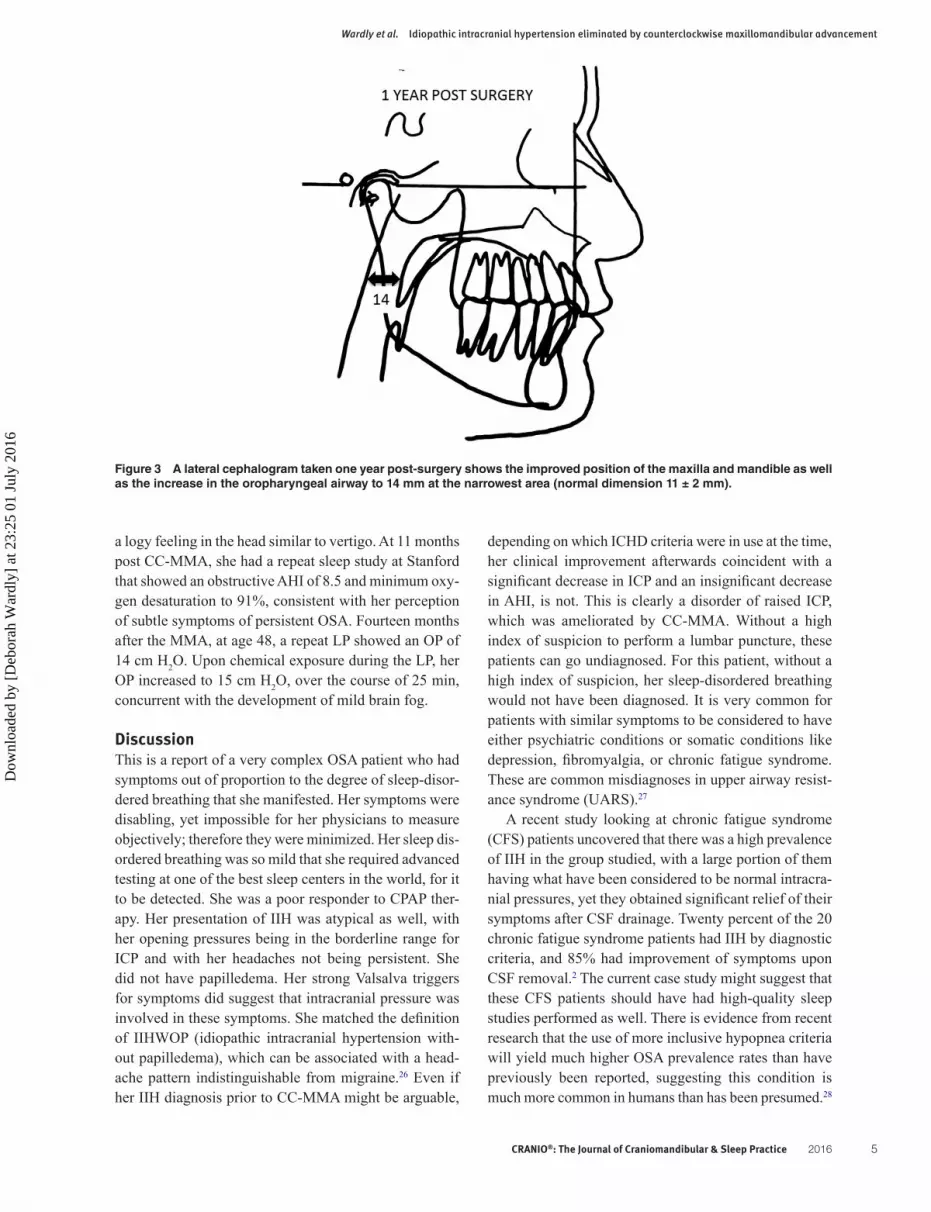
She decided to investigate a surgical solution and travelled to Dallas, TX to see an oral and maxillofacial jaw surgeon, on the advice of her orthodontist. After evaluation and consultation, it was determined that she had the following diagnosis: (1) Mandibular hypoplasia; (2) Maxillary hypoplasia; (3) Bilateral temporomandibu-lar joint (TMJ) articular disc dislocation (the TMJ pathol-ogy could be contributory to the chronic headaches); and (4) Moderately decreased oropharyngeal airway (Figure 1). It was recommended that she undergo surgery for counterclockwise rotation of the maxillomandibular complex (CC-MMA) for advancement to increase the size of the oropharyngeal airway and improve facial bal-ance. The CC-MMA surgical philosophy, protocol, and evidence-based outcome studies were developed and researched by Wolford.17–23 For this patient, the surgical protocol consisted of the following: (1) Bilateral TMJ articular disc repositioning with a Mitek anchor tech-nique24,25; (2) Bilateral mandibular ramus osteotomies with bone plate stabilization for mandibular advance-ment in a counterclockwise direction; and (3) Multiple maxillary osteotomies with bone plate stabilization to advance the maxilla in a counterclockwise direction (Figure 2). With this approach, the chin advanced 10 mm while the maxilla at the osteotomy level advanced 4 mm, creating a significant improvement in the facial balance and profile, as well as maximizing the dimension of the oropharyngeal airway. Pre-surgery, the narrowest anter-oposterior area of the oropharyngeal airway measured 7 mm (normal = 11 ± 2 mm) and at one-year post surgery, the airway was 14 mm, doubling the presurgery dimen-sion, a significant improvement (Figure 3).
Six to eight weeks after the operation, the patient began to feel much better and was able to exercise again after years of feeling lightheaded and weak with exercise. She was no longer using anything for sleep apnea other than a nasal decongestant at bedtime, and while she continued to have symptoms of sleep apnea such as waking with a sore throat, her IIH symptoms were markedly improved. Prior to the MMA, sleeping without airway support led to awak-ening in a deep fog, while post-surgery, this was gone. She would only occasionally awake with mild brain fog. The brain fog could still result from chemical exposure. Prior to CC-MMA, this was disabling and long-lasting; how-ever post-surgery, the use of Lasix, exercise, or even just waiting an hour in addition to removal of the chemical, would lead to clearing of the fog. As noted above, prior to the CC-MMA, she had a very prominent Valsalva trigger for ICP, such that just starting to cry could precipitate an ice pick-type headache with persistent symptoms for 24 h
Dow
nloa
ded
by [
Deb
orah
War
dly]
at 2
3:25
01
July
201
6
CRANIO®: The Journal of Craniomandibular & Sleep Practice 2016 4
Wardly et al. Idiopathic intracranial hypertension eliminated by counterclockwise maxillomandibular advancement
could speak, shout, laugh, and cry with no consequences. Her personality appeared to change because she could now speak animatedly and rapidly, whereas prior to the CC-MMA, she was soft spoken and moved slowly, with
afterward. After the CC-MMA, she was able to cry with-out any ICP symptoms developing. Any headaches were mild and infrequent. Prior to the CC-MMA, she could feel dizzy just from shouting, while post-surgery, she
Figure 1 Cephalometric analysis of the patient shows: (1) Mandibular hypoplasia; (2) Maxillary hypoplasia; (3) Moderately high occlusal plane angle of 12 degrees (normal 8 degrees ±2 mm); and (4) Oropharyngeal airway of 7 mm (normal dimension 11 ± 2 mm).
Figure 2 Prediction tracing (surgical plan) demonstrates the counterclockwise rotation of the maxillomandibular complex with the chin advancing 10 mm and the maxilla advancing 4 mm. The mandible was advanced with bilateral mandibular ramus sagittal split osteotomies and the maxilla was repositioned forward with multiple maxillary osteotomies.
Dow
nloa
ded
by [
Deb
orah
War
dly]
at 2
3:25
01
July
201
6
CRANIO®: The Journal of Craniomandibular & Sleep Practice 2016 5
Wardly et al. Idiopathic intracranial hypertension eliminated by counterclockwise maxillomandibular advancement
depending on which ICHD criteria were in use at the time, her clinical improvement afterwards coincident with a significant decrease in ICP and an insignificant decrease in AHI, is not. This is clearly a disorder of raised ICP, which was ameliorated by CC-MMA. Without a high index of suspicion to perform a lumbar puncture, these patients can go undiagnosed. For this patient, without a high index of suspicion, her sleep-disordered breathing would not have been diagnosed. It is very common for patients with similar symptoms to be considered to have either psychiatric conditions or somatic conditions like depression, fibromyalgia, or chronic fatigue syndrome. These are common misdiagnoses in upper airway resist-ance syndrome (UARS).27
A recent study looking at chronic fatigue syndrome (CFS) patients uncovered that there was a high prevalence of IIH in the group studied, with a large portion of them having what have been considered to be normal intracra-nial pressures, yet they obtained significant relief of their symptoms after CSF drainage. Twenty percent of the 20 chronic fatigue syndrome patients had IIH by diagnostic criteria, and 85% had improvement of symptoms upon CSF removal.2 The current case study might suggest that these CFS patients should have had high-quality sleep studies performed as well. There is evidence from recent research that the use of more inclusive hypopnea criteria will yield much higher OSA prevalence rates than have previously been reported, suggesting this condition is much more common in humans than has been presumed.28
a logy feeling in the head similar to vertigo. At 11 months post CC-MMA, she had a repeat sleep study at Stanford that showed an obstructive AHI of 8.5 and minimum oxy-gen desaturation to 91%, consistent with her perception of subtle symptoms of persistent OSA. Fourteen months after the MMA, at age 48, a repeat LP showed an OP of 14 cm H2O. Upon chemical exposure during the LP, her OP increased to 15 cm H2O, over the course of 25 min, concurrent with the development of mild brain fog.
DiscussionThis is a report of a very complex OSA patient who had symptoms out of proportion to the degree of sleep-disor-dered breathing that she manifested. Her symptoms were disabling, yet impossible for her physicians to measure objectively; therefore they were minimized. Her sleep dis-ordered breathing was so mild that she required advanced testing at one of the best sleep centers in the world, for it to be detected. She was a poor responder to CPAP ther-apy. Her presentation of IIH was atypical as well, with her opening pressures being in the borderline range for ICP and with her headaches not being persistent. She did not have papilledema. Her strong Valsalva triggers for symptoms did suggest that intracranial pressure was involved in these symptoms. She matched the definition of IIHWOP (idiopathic intracranial hypertension with-out papilledema), which can be associated with a head-ache pattern indistinguishable from migraine.26 Even if her IIH diagnosis prior to CC-MMA might be arguable,
Figure 3 A lateral cephalogram taken one year post-surgery shows the improved position of the maxilla and mandible as well as the increase in the oropharyngeal airway to 14 mm at the narrowest area (normal dimension 11 ± 2 mm).
Dow
nloa
ded
by [
Deb
orah
War
dly]
at 2
3:25
01
July
201
6

CRANIO®: The Journal of Craniomandibular & Sleep Practice 2016 6
Wardly et al. Idiopathic intracranial hypertension eliminated by counterclockwise maxillomandibular advancement
condylar resorption, resulting in the mandible becoming retruded again and a malocclusion redeveloping.38 The importance of the counterclockwise rotation in conjunc-tion with correcting co-existing TMJ pathology cannot be over emphasized.
It is known that treating OSA can improve IIH. However, this is the first report in the literature to doc-ument the use of CC-MMA to improve IIH via treating OSA. A second point would be that the OSA in this patient has NOT been completely cured by CC-MMA. An assess-ment of her oropharyngeal airway before and one year after surgery shows that the airway has doubled in size, corresponding to a decrease in airway resistance by a fac-tor of 30 (Figure 3). However, her AHI at presentation was measured at 10.2, and after CC-MMA it was 8.5. There were improvements in her sleep stages that imply that her sleep, and therefore, sleep-disordered breathing, has improved perhaps more than her AHI reflects, but she still desaturates to 91%, just as before surgery. This patient still exhibits mild obstructive sleep apnea symptoms and has persistent OSA on her sleep study. Radiographic and clin-ical evaluations demonstrate that the nasal and oropharyn-geal airways have greater airway space dimensions than considered normal. Residual problems may be related to constricture at the vocal cords, tracheal obstruction, tracheomalacia, or pulmonary factors. In addition, there may be hypotonia or tissue laxity of the upper airway, or a central nervous system component. Therefore, the authors contend that the improvement in OSA was not significant enough to account for the elimination of IIH and its symptoms in this patient (headaches, brain fog, Valsalva triggers), but that it was the mandibular advance-ment itself that effected this result.
The authors propose that this patient’s mandibular retraction and airway compression was impacting upon her jugular veins and increasing jugular venous resist-ance. If there is increased resistance in the internal jugular veins, this will decrease the pressure gradient required for CSF absorption to occur. This patient had already experi-enced the significant narrowing of her airway, which sits just medial and anterior to the internal jugular veins in the neck with only soft tissue in between.39 The venous system is very low pressure and could be affected by an alteration in anatomy that compressed the airway in this patient and could also have compressed the space the internal jugular veins occupy.
During this CC-MMA procedure, the patient’s mandi-ble was advanced by 10 mm. The tongue is attached to the mandible and was advanced as well, opening the posterior airway space. This would decompress this space, and in a low pressure venous system, could lead to enough of a decrease in internal jugular venous resistance to allow
A 2011 study at Stanford University (Stanford, CA, USA) confirmed that more inclusive hypopnea criteria than that recommended by the American Academy of Sleep Medicine at that time, are also more accurate in detecting pediatric sleep disordered breathing.29 Therefore, lesson one from this case study is that a high index of suspicion should exist for detecting atypical cases of IIHWOP and also for detecting mild sleep-disordered breathing, given the high degree of morbidity that may occur as a result of these conditions. Part of the process of detecting atyp-ical cases of IIH is to consider that the accepted ranges for abnormal CSF pressure may not apply to all indi-viduals, and the response to CSF removal is important to consider. Just as papilledema may occur at what are considered normal ICPs,30 it is beginning to be apparent that other symptoms of IIH can occur at pressures that have been previously accepted as normal. Higgins et al.2 have pointed out that the development of these ‘normal’ ranges for ICP came from studies of patients who were not completely normal neurologically but were presumed to not have problems with elevated ICP. This was likely too great of an assumption to make, and it has significantly influenced policy and guidelines in diagnosis of disorders of raised ICP going forwards.
Lesson two from this case study would be in regard to the fact that the CC-MMA appeared to eliminate the IIH in this patient. This patient demonstrated some of the classic facial morphological characteristics of patients susceptible to sleep apnea symptoms; retruded mandible and maxilla, high occlusal plane angle, anterior dental open bite, and decreased oropharyngeal airway. This facial morphological type also commonly has TMJ pathology as well as nasal airway obstruction usually related to hyper-trophied inferior nasal turbinates and/or deviated nasal septum.31 (This patient had TMJ pathology but did not have nasal airway obstruction at presentation; however, eight years previously, she had nasal septoplasty and turbi-nate reduction.) Surgical counterclockwise rotation of the maxillomandibular complex compared to the traditional maxillomandibular advancement procedure has the advan-tage of maximizing the increase in oropharyngeal airway as well as the esthetic and functional outcomes.21,22,32,33 The traditional MMA procedure (no counterclockwise rotation) commonly creates an unpleasant esthetic out-come as well as less improvement in the oropharyngeal airway dimension. In addition, with Wolford’s treatment protocol,34–37 the TMJ pathology (common in this patient type) is addressed and corrected; whereas, those who use the traditional approach commonly ignore the TMJ pathology. When the TMJ pathology is ignored, there is a high risk for development of, or increase in TMJ pain and headaches (84% risk) and a 25% risk of subsequent TMJ
Dow
nloa
ded
by [
Deb
orah
War
dly]
at 2
3:25
01
July
201
6

CRANIO®: The Journal of Craniomandibular & Sleep Practice 2016 7
Wardly et al. Idiopathic intracranial hypertension eliminated by counterclockwise maxillomandibular advancement
mandible in the face43 and could therefore theoretically precipitate a change in CSF dynamics via an alteration in jugular venous flow.
An alternative explanation for how CC-MMA effected the positive results in this patient might be that it was in part a forward head posture, which may have narrowed the jugular foramen to increase resistance in the internal jugular veins. Forward head posture is directly correlated to disease severity in OSA as well as features of a nar-rowed airway, including large tongues, and is a reflection of an adaptation to a narrowed airway.44 Once the airway was opened, this patient may have been able to adopt a more normal head posture, which could have effected an improvement in venous flow, not just in the jugular veins but in the veins that pass through the thoracic outlet. Forward head posture is associated with thoracic outlet syndrome,45 which can be accompanied by compression of the veins of the neck and subclavian fossae.46
One way to confirm that the mechanism for elimina-tion of IIH by CC-MMA is correct would be to measure jugular venous pressure before and after surgery in future IIH patients who undergo this procedure. Alternatively, one could measure jugular venous pressure in IIH patients with and without full tongue thrust to determine if this makes a difference, before undergoing the full maxillo-mandibular advancement procedure.
The fact that the patient in the present case study also has chemical sensitivity in conjunction with her IIH symp-toms is of note. The reaction to chemicals increases her ICP symptoms, and even after what appears to be elimi-nation of her IIH, the chemical exposure still increases her ICP as measured on the LP, and produces mild brain fog. This has never before been reported in the literature and is an important link between IIH/ICP and MCS. This will be discussed in a separate report, in order not to detract from the important conclusions above regarding IIH and the value of CC-MMA for its treatment and possible cure.
ConclusionThis case highlights the relationship between OSA and IH and points to the significant morbidity that can result from mild OSA and from what are considered border-line intracranial pressures. This indicates the need for a high index of suspicion for actual underlying pathology that can be surgically corrected when patients manifest symptoms of a somatic syndrome. This is the first report in the medical literature of clinical elimination of IH by CC-MMA. The authors propose that this positive outcome was effected via mandibular advancement producing a decrease in jugular venous resistance, allowing improved absorption of cerebrospinal fluid.
normal CSF absorption after this procedure. It could also be argued that this concept explains why this patient did so well with a tongue-retaining device to effect the decom-pression of the posterior airway space and take pressure off the internal jugular veins. Jugular venous compression may explain her apparent ‘remission’ immediately after total thyroidectomy, if her goiter from Graves’ disease was compressing the jugular veins in the neck and affecting CSF absorption. This may have allowed the improvement until she developed tongue collapse. This concept might also explain why this patient never did as well with PAP therapy; the PAP itself may have led to higher internal jugular venous pressures by increasing the pressure in the posterior airway space. In 1994, Hormann et al.40 showed that a CPAP of 12 can increase ICP and central venous pressure. Even if this is not a significant increase in people with normal cranial compliance, in the presence of impaired CSF absorption, it may become clinically significant; this is something that requires further study. Certainly the Valsalva maneuver is known to increase ICP,41 and therefore the elevated expiratory pressures of CPAP will create a Valsalva, increasing ICP, which again may be more significant in IIH patients.
If this explanation for why this patient improved is indeed accurate, it implies that PAP therapy is not appro-priate for patients with IIH. It actually implies that the CC-MMA might be the procedure of choice for a patient with IIH and OSA as long as other etiologies are ruled out, and even in the absence of diagnosable OSA. While it is an invasive procedure, so is CSF shunting. Once healed, the CC-MMA has a lower complication rate than a CSF shunting procedure and does not involve a foreign body in the brain, spinal canal, or abdominal cavity, which is prone to infection. Given the apparent pathophysiology thought to be involved in IIH, it seems that the CC-MMA may be more directly addressing the possible cause of this condition: the abnormal pressure gradient from the CSF compartment into the venous system. Ventriculoperitoneal (VP) shunting will actually impair this gradient further by draining the ventricles and decreasing ventricular pres-sure. In fact, CSF shunting is not a cure, because upon removal of the shunt, the cause of the IIH remains. IIH has been considered a rare illness that is largely incurable. This case report suggests that IIH may not be rare, just misdiagnosed, and that it may be curable.
If IIH is typically caused by a retracted mandible rather than this being something seen just in the present case study, this has wider implications, given the knowledge that mouth breathing in childhood can lead to this acquired malformation of the jaw.42 Also, retractive orthodontia may also lead to retraction of both the maxilla and the
Dow
nloa
ded
by [
Deb
orah
War
dly]
at 2
3:25
01
July
201
6

CRANIO®: The Journal of Craniomandibular & Sleep Practice 2016 8
Wardly et al. Idiopathic intracranial hypertension eliminated by counterclockwise maxillomandibular advancement
8 Larner A. Obstructive sleep apnoea-hypopnoea syndrome and idiopathic intracranial hypertension: coincident, comorbid, or causal relationship? Adv Clin Neurosci Rehabil. 2006 [cited 2014 Sep 19]. Available from http://www.acnr.co.uk/pdfs/Case%20reports/PapAJLcasestudy.pdf
9 Lee AG, Golnik K, Kardon R, Wall M, Eggenberger E, Yedavally S. Sleep apnea and intracranial hypertension in men. Ophthalmology. 2002;109(3):482–485.
10 Brazis PW, Lee AG. Elevated intracranial pressure and pseudotumor cerebri. Curr Opin Ophthalmol. 1998;9(6):27–32.
11 Pollay M. The function and structure of the cerebrospinal fluid outflow system. Cerebrospinal Fluid Res. 2010;7:9.
12 Alperin N, Ranganathan S, Bagci AM, Adams B, Ertl-Wagner E, Saraf-Lavi EM, et al. MRI evidence of impaired CSF homeostasis in obesity-associated idiopathic intracranial hypertension. Am J Neuroradiol. 2013;34:29–34.
13 Dashti SR, Nakaji P, Hu YC, Frei DF, Abla AA, Yao T, et al. Styloidogenic jugular venous compression syndrome: diagnosis and treatment: case report. Neurosurgery. 2012;70(3):E795–E799.
14 Javaheri S, Qureshi Z, Golnik K. Resolution of papilledema associated with OSA treatment. J Clin Sleep Med. 2011;7(4):399–400.
15 Kalyoussef E, Brooks NO, Quraishi H, Turbin R, Frohman L. Idiopathic intracranial hypertension in a child with obstructive sleep apnea cured by tonsillectomy/adenoidectomy. J Neuroopthalmol. 2013;33(4):413–414.
16 Purvin VA, Kawasaki A, Yee RD. Papilledema and obstructive sleep apnea syndrome. Arch Ophthalmol. 2000;118(12):1626–1630.
17 Wolford LM, Chemello PD, Hilliard FW. Occlusal plane alteration in orthognathic surgery. J Oral Maxillofac Surg. 1993;51:730–740.
18 Wolford LM, Chemello PD, Hilliard F. Occlusal plane alteration in orthognathic surgery–part I: effects on function and esthetics. Am J Orthod Dentofac Orthop. 1994;106:304–316.
19 Chemello PD, Wolford LM, Buschang MS. Occlusal plane alteration in orthognathic surgery – part II: long-term stability of results. Am J Orthod Dentofac Orthop. 1994;106:434–440.
20 Mehra P, Wolford LM. Surgical management of obstructive sleep apnea. Bayl Univ Med Cent Proc. 2000;13:338–342.
21 Mehra P, Downie M, Pita MC, Wolford LM. Pharyngeal airway space changes after counterclockwise rotation of the maxillomandibular complex. Am J Orthod Dentofac Orthop. 2001;120:154–159.
22 Goncalves JR, Buschang PH, Goncalves DG, Wolford LM. Postsurgical stability of oropharyngeal airway changes following counter-clockwise maxillo-mandibular advancement surgery. J Oral Maxillofac Surg. 2006;64:755–762.
23 Wolford LM. Surgical planning in orthognathic surgery (Chapter 60). In: Booth PW, Schendel SA, Hausamen JE, editors. Maxillofacial surgery. Vol. 2. St Louis, MO: Churchill Livingstone; 2007. p. 1155–1210.
24 Mehra P, Wolford LM. The Mitek mini anchor for TMJ disc repositioning: surgical technique and results. Int J Oral Maxillofac Surg. 2001;30:497–503.
25 Goncalves JR, Wolford LM, Cassano DS, da Porciuncula G, Paniagua B, Cevidanes LH. Temporomandibular joint condylar changes following maxillomandibular advancement and articular disc repositioning. J Oral Maxillofac Surg. 2013;71:1759.e1–1759.e15.
26 Bono F, Messina D, Giliberto C, Cristiano D, Broussard G, Fera F, et al. Bilateral transverse sinus stenosis predicts IIH without papilledema in patients with migraine. Neurology. 2006;67(3):419–423.
27 Guilleminault C, De Los Reyes, V. Upper-airway resistance syndrome. Handb Clin Neurol. 2011;98:401–409.
28 Tufik S, Santos-Silva R, Taddei J, Azeredo Bittencourt LR. Obstructive sleep apnea syndrome in the São Paulo epidemiologic sleep study. Sleep Med. 2010;11:441–446.
29 Lin C, Guilleminault C. Current hypopnea scoring criteria underscore pediatric sleep disordered breathing. Sleep Med. 2011;12:720–729.
30 Suh SY, Kim SJ. IIH with normal CSF pressures? Ind J Ophthalmol. 2013;61(11):681–682.
31 Movahed R, Morales-Ryan C, Allen WR, Warren S, Wolford LM. Outcome assessment of 603 cases of concomitant inferior turbinectomy and lefort I osteotomy. Bayl Univ Med Cent Proc. 2013;26:376–381.
32 Goncalves J, Cassano DS, Wolford LM, Santos-Pinto A, Marquez IM. Postsurgical stability of counterclockwise maxillomandibular advancement surgery: affect of articular disc repositioning. J Oral Maxillofac Surg. 2008;66:724–738.
AbbreviationsAHI Apnea Hypopnea IndexCC-MMA counterclockwise maxillomandibular
advancementCFS chronic fatigue syndromeCPAP continuous positive airway pressureCSF cerebrospinal fluidICP intracranial pressureIIH idiopathic intracranial hypertensionIIHWOP idiopathic intracranial hypertension
without papilledemaLP lumbar punctureMAD mandibular advancement deviceMCS multiple chemical sensitivityOP opening pressureOSA obstructive sleep apneaREM rapid eye movementTIA transient ischemic attackTMJ temporomandibular jointUARS upper airway resistance syndrome
Declaration of interest and source of fundingThis project was completely self-funded by the authors. There is no financial conflict of interest. Deborah Wardly is the patient discussed in the case presentation.
AcknowledgmentParts of the patient details in the case report published here will be reproduced in a second article entitled: ‘Multiple chemical sensitivity as a variant of idiopathic intracranial hypertension: a case report,’ authored by Deborah Wardly, MD and Venkat Veerappan, MD.
ORCID
Deborah Wardly http://orcid.org/0000-0002-4275-4447Larry M. Wolford http://orcid.org/0000-0001-5699-4559
References 1 Wall M. Idiopathic intracranial hypertension. Neurol Clin.
2010;28(3):593–617. 2 Higgins N, Pickard J, Lever A. Lumbar puncture, chronic fatigue
syndrome and idiopathic intracranial hypertension: a cross-sectional study. J R Soc Med. 2013;4(12):1–7.
3 Friedman DI, Liu GT, Digre KB. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology. 2013;81:1159–1165.
4 Hoffman J, Goadsby PJ. Update on intracranial hypertension and hypotension. Curr Opin Neurol. 2013;26(3):240–247.
5 Fraser J, Bruce B, Rucker J, Fraser L, Atkins EJ, Newman NJ, et al. Risk factors for idiopathic intracranial hypertension in men: a case–control study. J Neurol Sci. 2010;290(1–2):86–89.
6 Headache Classification Committee of the International Headache Society. The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia. 2013;33(9):629–808.
7 Jennum P, Børgesen S. Intracranial pressure and obstructive sleep apnea. Chest. 1989;95:279–283.
Dow
nloa
ded
by [
Deb
orah
War
dly]
at 2
3:25
01
July
201
6

CRANIO®: The Journal of Craniomandibular & Sleep Practice 2016 9
Wardly et al. Idiopathic intracranial hypertension eliminated by counterclockwise maxillomandibular advancement
40 Hörmann C, Mohsenipour I, Gottardis M, Benzer A. Response of cerebrospinal fluid pressure to continuous positive airway pressure in volunteers. Anesth Analg. 1994;78:54–57.
41 Lazowick D, Meyer TJ, Pressman M, Peterson D. Orbital herniation associated with noninvasive positive pressure ventilation. Chest. 1998;113:841–843.
42 Jefferson Y. Mouth breathing: adverse effects on facial growth, health, academics, and behavior. Gen Dent. 2010;58(1):18–25.
43 Hang WM. How many years must a profession exist? Cranio. 2006;24(2):73–75.
44 Ozbek MM, Miyamoto K, Lowe AA, Fleetham JA. Natural head posture, upper airway morphology and obstructive sleep apnoea severity in adults. Eur J Orthodontics. 1998;20:133–143.
45 Robey JH, Boyle KL. Bilateral functional thoracic outlet syndrome in a collegiate football player. North Am J Sports Phys Ther. 2009;4(4):170–181.
46 Collins JD. A woman post scalenectomy and first-rib resection with dilated verterbral venous plexus and a facial rash. J Nat Med Assoc. 2012;104(5–6):306–310.
33 Mehra P, Wolford LM. Surgical management of obstructive sleep apnea. Bayl Univ Med Cent Proc. 2000;13:338–342.
34 Wolford LM. Concomitant temporomandibular joint and orthognathic surgery. J Oral Maxillofac Surg. 2003;61:1198–1204.
35 Wolford LM, Dhameja A. Planning for combined TMJ arthroplasty and orthognathic surgery. In: Ness GM, editor. Atlas of the oral and maxillofacial clinics of North America. Philadelphia, PA: WB Saunders; 2011. p. 243–270.
36 Wolford LM, Cassano DS, Goncalves JR. Common TMJ disorders: orthodontic and surgical management. In: McNamara JA, Kapila SD, editors. Temporomandibular disorders and orofacial pain: separating controversy from consensus. Vol. 46, Craniofacial growth series. Ann Arbor: The University of Michigan; 2009. p. 159–198.
37 Wolford LM, Karras S, Mehra P. Concomitant temporomandibular joint and orthognathic surgery: a preliminary report. J Oral Maxillofac Surg. 2002;60:356–362.
38 Wolford LM, Reische-Fischel O, Mehra P. Changes in temporomandibular joint dysfunction after orthognathic surgery. J Oral Maxillofac Surg. 2003;61:655–660.
39 Anderson JE. Grant’s atlas of anatomy. Baltimore, MD: Williams and Wilkins; 1983. Fig. 7–82.
Dow
nloa
ded
by [
Deb
orah
War
dly]
at 2
3:25
01
July
201
6





























