Embed Size (px)
Citation preview
Copyright 1997 byThe Cerontological Society of America
The GerontologistVol. 37, No. 2,157-167
Data from 252 female primary caregivers, their husbands, and children living inmultigenerational households were used to create family typologies based on the extent of
similarity among reports of elder behaviors. Analysis of variance indicates that familiescharacterized by high agreement and those characterized by low agreement were significantly
different from one another on a number of dimensions. When the relationship betweencaregiver-reported stressors and mental health was examined as a function of family typology,
results indicate that for high agreement families there were significant correlations betweenthe caregiver's report of the elder's behaviors and her burden; satisfaction with caregiving;
relationships with her husband, child, and elder; and depression. Similar relationshipscharacterize data reported by husbands and children in high agreement families. For families
characterized by low agreement, the majority of these relationships were not significant.Key Words: Family caregivers, Family typologies, Caregiver well-being
Typologies of Caregiving Families: FamilyCongruence and Individual Well-Being1
Rachel A. Pruchno, PhD,2 Christopher J. Burant, MA,3
and Norah D. Peters, PhD2
One of the most well studied issues within caregiv-ing research concerns the effect that stressors, gen-erally operationalized as characteristics or behaviorsof the care recipient, have on the well-being of theprimary caregiver. The relationship between stres-sors and outcomes among caregivers of elderly peo-ple, however, has been reported by some research-ers as positive (Deimling & Bass, 1986; Fengler &Goodrich, 1979; Grad & Sainsbury, 1968; Montgom-ery, Gonyea, & Hooyman, 1985; Pearson, Verma, &Nellett, 1988), whereas others report that the rela-tionship is either weak or nonexistent (George &Gwyther, 1986; Gilhooly, 1984; Haley, Brown, &Levine, 1987; Morycz, 1985; Ory et al., 1985; Zarit,Reever, & Bach-Peterson, 1980; Zarit, Todd, & Zarit,1986). The theoretical models upon which much ofthis work is based assume that stressors are objectiveand outcomes such as depression and burden aresubjective, because reports of stressors and reportsof well-being are generally made by the same individ-ual. It is difficult to understand whether they repre-sent separate constructs or multiple indicators of thesame construct. For example, when positive relation-ships are found between stressors and outcomes,they are interpreted as providing evidence that themore severe the condition of the elder, the bur-
1This research was supported by Grant PO1 MH43371 (Caregiving andMental Health: A Multifaceted Approach) to the Philadelphia GeriatricCenter (with a subcontract to the Myers Research Institute of Menorah ParkCenter for the Aging) from the National Institute of Mental Health.
Philadelphia Geriatric Center. Dr. Peters is currently Acting Director ofthe Departments of Sociology and Anthropology, Beaver College, Glen-side, PA. Address correspondence to Dr. Rachel Pruchno, Director, Centeron Aging, Bradley University, Peoria, IL 61625.
3Myers Research Institute of Menorah Park Center for the Aging.
dened, upset, or depressed is the caregiver. It isequally plausible, however, to posit that positiverelationships between stressors and outcomes arefound because those caregivers who are more upsetor burdened or depressed are likely to report morestressors than those caregivers who are not upset,burdened, or depressed.
In this article, we will use a rough estimation ofobjectivity of reports, that is, the extent of similarity ofreports about an elder's behavior made by multiplefamily members, in an effort to separate reports ofstressors from reports of well-being. It will develop atypology of families based on the extent to whichreports of elder behavior made by family members aresimilar to one another, examine characteristics of fam-ily members and families in these groups, and explorewhether the relationship between the caregiver's re-port of elder's behaviors and outcome variables differas a function of family typology.
Caregiving from the Perspective of MultipleFamily Members: Empirical Findings
Caregiver researchers only occasionally have stud-ied two members of the intergenerational dyad, usu-ally the daughter and her widowed mother (Brody,1985; Walker & Thompson, 1983). Less often, data arecollected from the siblings of the primary caregiver(Brody, 1985; Townsend & Poulshock, 1986). Theextent to which primary caregivers and other familymembers agree on the stressors that characterize thecare receiver has received little empirical attention.In a qualitative analysis of a single three-generationfamily, Pruchno (1994) described how reports madeby the primary caregiver, her husband, and the elder
Vol. 37, No. 2,1997 157
Dow
nloaded from https://academ
ic.oup.com/gerontologist/article/37/2/157/617002 by guest on 04 February 2022
about the health status of the elder differed from oneanother. Using a standard health checklist, the threeinformants agreed on the existence of only threehealth conditions (emphysema, pneumonia, andnervousness). In addition, the primary caregiver re-ported that her father suffered from hearing prob-lems, chronic bronchitis, heart trouble, troublesleeping, Parkinson's disease, and Alzheimer's dis-ease. This caregiver's husband reported that hisfather-in-law had hearing problems, a stomach ulcer,headaches, circulation, and liver problems, while theelder indicated that he suffered from back problems.
In their study that collected data from a very oldparent and two of her or his adult children, Mat-thews, Adamek, and Dunkle (1993) found significantdifferences between the adult children's and par-ent's evaluation of the parent's ability to performactivities of daily living tasks, but no significant dif-ferences between the reports made by the siblings.The adult children agreed with one another, but notwith their parent, about the parent's functional abili-ties. Furthermore, the adult children agreed thattheir parent was less able than the parent consideredhimself or herself to be. On the other hand, whenBrody, Hoffman, Kleban, and Schoonover (1989)compared reports provided by the primary care-givers of widowed mothers about their mother'shealth conditions and functional abilities with thosemade by local siblings, they found that the reportswere virtually identical.
Theoretical UnderpinningsThe dominant model guiding much of caregiving
research during the past 30 years is one in which thedemands associated with caregiving are conceptual-ized as being external to the caregiver. From withinthe context of both gerontological research and fam-ily research, caregiving demands or stressors fallunder the domain of "press" as described by Murray(1938) and are generally characterized as being ob-jective rather than subjective in nature. Within thesemodels, caregiving is not prejudged as stressful;rather the demands associated with caregiving havethe potential to become stressful when there is in-congruence between the strength of the demandand the competence of the caregiver to deal with thedemand (e.g., Lawton & Nahemow, 1973). This viewis eloquently expressed within the gerontologicalliterature by Pearlin, Mullan, Semple, and Skaff(1990). They stated that "daily dependencies, prob-lematic behaviors, and cognitive status (of the olderperson) are objective indicators of stressors in thesense that they are based on the health, behavior,and functional capabilities of the impaired relative"(p. 587). They contended that these "objective assess-ments of the patient's behaviors and capabilities"serve as indicators of the current demands of care-giving and as benchmarks of transformations thathave already occurred and those that are expected tooccur. This view of objective indicators of stressors isconsistent with that which has been dominant in thefamily literature. For example, the ABCX model of
family stress originally described by Hill (1949) holdsthat the event and related hardships (the A compo-nent of the model) lie outside the family per se, andincludes attributes of the event itself. As events oc-curring outside the family, stressors are generallydescribed as objective rather than subjective.
The assumption that stressors such as problematicbehaviors are objective is not one that can easily betested. Philosophers of science have long debatedthe topic of objectivity in measurement, and mostscholars have agreed that objectivity can only beapproximated. Although examining data collectedfrom multiple family members is a way of checkingthe extent to which reports from a single individualare characteristic of those provided by other familymembers, there is a question as to whether reportsfrom multiple family members tell us anything aboutthe "objective" characteristics of the household. Jes-sop (1981) has suggested that the degree to whichmultiple family members see things the same waytells us little about the objective content of familylife, for there is still no objective criterion againstwhich the validity of multiple reports can bechecked. Similarly, Larsen and Olson (1990) havewarned, "just as it is dangerous to assume that onemember can adequately represent the family's real-ity, it is equally problematic to conclude that theacquisition of several members' data can provide amore valid reality" (p. 22).
Despite these caveats, Singer (1973) contendedthat when reports are corroborated by another fam-ily member we may intuitively have greater confi-dence in the reality of the reports. Using Singer's(1973) contention, it is postulated that when reportsof stressors are corroborated by multiple familymembers, the reports are more likely to be objectivethan when reports are not corroborated. When threefamily members, for example, all report that theirelderly family member is restless, greater evidenceexists that, in reality, the older person is restless thanwhen only one family member reports that the olderrelative is restless. Furthermore, it is suggested thatwhen the reports of family members are similar, andthe stressors reported by any one individual repre-sent stressors that are objective, the principles ofstress theory and family stress theory should be con-firmed. That is, more problematic behaviors shouldbe associated with greater burden and depressionand less satisfaction.
This hypothesis is consistent with Durkheim's(1933) explanation for why some families appear tobe less affected by stressors than others and withHill's (1949) explanation of successful adjustment tothe stressors associated with war-induced separa-tion, adaptation, and reunion. Both Hill andDurkheim highlighted the salience of similarityamong family members. A salient component ofDurkheim's work was the extent to which the familywas characterized by a "common conscience." Simi-larly, one of the major factors identified by Hill (1949)to explain successful adjustment of individuals wasfamily integration, which he defined as pride in fam-ily traditions and high participation as a family in joint
158 The Gerontologist
Dow
nloaded from https://academ
ic.oup.com/gerontologist/article/37/2/157/617002 by guest on 04 February 2022

activities. Deutsch (1968) also found that consensusamong group members related to group functioning.Given the importance of this sense of family solidar-ity, common conscience, and family integration inexplaining family functioning, it is postulated that asalient dimension underlying family solidarity amongcaregiving families is the extent to which familymembers agree on the existence of stressors associ-ated with the care receiver. When family membersagree on the presence of stressors, there is evidencefor greater solidarity among the family than whenfamily members do not agree. When family membershave a common conscience, it is expected that theywill experience less stress than when they do nothave a common conscience. Furthermore, whenthere is a common conscience, it is expected that thepredicted relationships between stressors and out-comes (e.g., more stressors, more negative out-comes) should be confirmed.
It should be noted, however, that the interpreta-tion of similarity of reports as representative ofgreater objectivity has several caveats associatedwith it. First, the extent of similarity may be attributedto the extent to which family members have access tothe older person. Second, the extent of similarity ofreports may be influenced by the sensitivity of differ-ent family members to the behavior in question. Forexample, a family member's report that the olderperson was restless may be associated with that fam-ily member's tolerance for the behavior as well as tothe existence of the behavior itself.
Goals and Hypotheses
In this article, we have three goals. First, the extentof similarity in reports of characteristics describingelderly household members made by caregivers andtheir family members will be examined by comparingcaregiver reports with those made by their co-resident husbands and children. Second, a typologyof families will be developed based on the extent ofsimilarity between these reports as made by care-givers and their husbands and children, and differ-ences in the groups of families will be investigated inan exploratory fashion. Third, the relationship be-tween caregiver-reported stressors and the care-giver's mental health will be examined for groups offamilies in which the caregiver's report of stressors issimilar to those made by other family members, forfamilies in which the caregiver's report of stressors ismoderately similar to those made by other familymembers, and for families in which the caregiver'sreport of stressors differs from that of other familymembers. The following hypotheses will be tested:
1. The greater the similarity of the perceptions re-garding the elder that family members have, theless the burden and depressive symptoms, thegreater the caregiving satisfaction and mastery,and the better the relationships among familymembers will be.
2. When family members agree with one anotherabout the elder's behaviors, models predictingthat more aberrant behaviors produce greater tur-
moil will be supported. When family members donot agree with one another, the relationships be-tween elder behaviors and outcomes will not besignificant. These relationships will exist aftercontrolling for elder's health and amount of timespent helping the elder by family members.
Methods
Sample
Personal interviews were conducted with threemembers of 252 three-generation families who livedin the same household: a caregiving woman, herhusband, and a selected child. Each household in-cluded an elderly relative (mother's parent or parent-in-law). Primary caregivers lived in the Philadelphiaarea and were recruited through newspaper an-nouncements and community organizations, thusrepresenting a sample of convenience. Criteria forinclusion in the study, in addition to living in ahousehold that included an elderly parent or parent-in-law, were that the caregiver be married, have achild living in the household, and all three individ-uals (the woman, her husband, and a child of theirs)would agree to participate in the study. When therewas more than one child living at home, the primarycaregiver was asked to nominate the child they felthad been most affected by the multigenerationalliving situation.
The sample was primarily White (93.9%). Care-givers in the study had a mean age of 48.3 years(range from 33 to 67 years), their husbands had amean age of 50.5 years (range from 32 to 75 years),and their children who participated in the study had amean age of 19 years (range of 11 to 31). The elderlyrelative was an average age of 80.2 years old (range64-103). The majority of older relatives had movedinto the homes of their younger family members(80.6%), although 11.5% of the elders had youngerfamily members move in with them, 4.8% had alwayslived together, and 3.2% had both generations movetogether into a new home. The primary reason citedfor the elder joining the multigenerational house-holds was a decline in his or her physical or mentalhealth. Family members had been living together fora mean of 8.16 years (range 1 month to 59 years).Fifty-four percent of the families were Catholic,35.9% were Protestant, and 7.6% were Jewish. Familyincome ranged from under $10,000 to more than$70,000 (mean of $52,500).
Measures
The caregivers, their husbands, and their childrenwere asked to report on the frequency with which 19behaviors characterized the elder with whom theywere living. Behaviors included trouble breathing,yelling, pain, choking, hearing things that were notthere, and exhibiting embarrassing behavior. Re-spondents indicated the frequency with which eachbehavior characterized their elder during the pastmonth. Responses included: (1) never, (2) once or
Vol. 37, No. 2,1997 159
Dow
nloaded from https://academ
ic.oup.com/gerontologist/article/37/2/157/617002 by guest on 04 February 2022
twice during the month, (3) 3-4 times during themonth, (4) 2-5 times a week, and (5) almost everyday. Table 1 displays mean scores on each behaviorreported by the three respondents for each behav-ior. Individual reports of elders' behaviors were cre-ated for each respondent by summing across the 19behaviors. Caregivers' scores had a mean of 39.09(range 19-81). Their husbands had a mean score of36.18 (range 19-73), whereas the children had a meanscore of 39.22 (range 19-73).
Each family member reported on the number ofhours he or she spent helping the elder; the qualityof relationship with each family member; caregivingburden, satisfaction, and mastery; health; and de-pressive symptoms. Physical health of the elder wasreported by the caregiver and her husband. Addi-tionally, information was gathered about family in-come and about the length of time the family mem-bers had been living together, as reported by thecaregiver.
The number of hours each family member spenthelping the elder was elicited using the followingquestion: "On the average, about how many hours aweek during the past month did you spend actuallyhelping your (elder) with the tasks we talked about?"(These tasks included 7 activities of daily living and 8instrumental activities of daily living.) The caregiversindicated that they spent an average of 18.55 hourshelping (range 0-168 hours), their husbands said thatthey spent an average of 7.45 hours (range 0-60hours) and their children reported spending an aver-age of 7.14 hours (range 0-50 hours).
Physical health of the elder was independentlyassessed by the caregiver and her husband using the24-item index of physical health conditions devel-oped for the National Long-Term Care Survey. Thecount of physical health problems reported by care-givers ranged from 0 to 17 (mean = 5.5). The count ofphysical health problems reported by husbandsranged from 0 to 15 (mean = 4.6).
Quality of relationship among family members wasmeasured by asking each of the three respondentsthe following four questions: "Overall, what wouldyou say is the quality of your current relationship to
?" (excellent [4]; good [3]; fair [2]; poor [1]),"Taking everything into consideration, how close doyou feel the relationship is between you and ?"(extremely close [4]; very close [3]; somewhat close[2]; not close at all [1]), Generally would you say thatyou and get along: (extremely well [4]; verywell [3]; somewhat well [2]; not well at all [1])?", and"How easy is it for you and to talk about thingsthat really concern you?" (extremely easy [4]; veryeasy [3]; somewhat easy [2]; or not easy at all [1]).Caregivers and their husbands reported on theirrelationships with one another, with their child par-ticipating in the study, and with the elder with whomthey were living. Children reported on their relation-ships with their mother, father, and elder. Each rela-tionship score ranged from 4 to 16, with higherscores indicating better relationships. Cronbach al-phas for the scales ranged from .82 to .89. Caregiversreporting on their relationships with their husband,
child, and elder had mean scores of 13.04,13.07, and11.17. Husbands, reporting on relationships withtheir wife, child, and elder had mean scores of 13.26,12.13, and 10.78. Children had mean relationshipscores of 12.39 with their mother, 11.67 with theirfather, and 10.60 with their elder.
Caregiving burden, satisfaction, and mastery weremeasured using scales based on those developed atthe Philadelphia Geriatric Center. As described byLawton, Moss, Kleban, Glicksman, and Rovine(1991), caregiving burden is "the perception of psy-chological distress, anxiety, depression, demoraliza-tion, and generalized loss of personal freedom at-tributed directly to caregiving" (p. P182). Caregivingsatisfaction represents the gains from desirable as-pects of, or positive affective returns from, caregiv-ing. It is the extent to which what one does or feels asa caregiver represents a source of personal satisfac-tion. Caregiving mastery represents a positive viewof one's ability and ongoing behavior during thecaregiving process. A pool of 29 items, includingitems developed by Lawton, Brody, and Saperstein(1989) to assess caregiving burden, satisfaction, andcaregiving mastery, as well as additional items devel-oped in the spirit of these constructs were includedin the study. A 5-point Likert-scale was used, withresponses for each question ranging from nearlyalways (5) to never (1). Principal components analysisconducted on a sample of 517 primary caregiversparticipating in the Philadelphia Geriatric Center Pro-gram Project (of which the sample described is oneof three components) produced a 3-factor solution.
The first two factors, caregiver burden and caregiv-ing satisfaction, approximated the original factorsdescribed by Lawton et al. (1989). Caregiving burdenconsisted of 9 items, with factor loadings rangingfrom .46 to .85. It tapped the respondent's subjectiveexperience of caregiving stress and included theextent to which individuals felt: (a) they could fit inmost of the things they need to do in spite of the timetaken by caring for a family member; (b) trapped; (c)that their health had suffered because of their care-giving experience; (d) that because of the time theyspend with their elder they do not have enough timefor themselves; (e) that their social life had sufferedbecause of caregiving; (f) that they will be unable tocare for their elder for much longer; (g) isolated andalone as a result of caring for their elder; (h) verytired as a result of caring for their elder; and (i) thatthey have lost control of their lives because of caringfor their elder. Cronbach alpha reliabilities for thescales ranged from .81 (children) to .90 (caregivers).Scores on the burden index ranged from 9 to 45, withhigher scores indicating greater burden. Burdenscores reported by caregivers had a mean of 20.89, bytheir husbands, 16.6, and by their children, 14.4.
Caregiving satisfaction, the second factor, con-tained 6 items with factor loadings ranging from .69to .84. This factor tapped positive feelings associatedwith caregiving, such as enjoyment or enhanced self-esteem. Items included the extent to which individ-uals: (a) get a sense of satisfaction from helping theirelder; (b) feel that helping their elder made them feel
160 The Gerontologist
Dow
nloaded from https://academ
ic.oup.com/gerontologist/article/37/2/157/617002 by guest on 04 February 2022
closer to him or her; (c) enjoy being with their elder;(d) feel that taking responsibility for their elder givestheir self-esteem a boost, report that their elder'spleasure over some little thing gives them pleasure;and (f) feel that caring for their elder gives moremeaning to their lives. Scores on the scale rangedfrom 6 to 30, with higher scores indicating greatersatisfaction from the caregiving role. Coefficient al-phas ranged from .87 (children) to .89 (caregivers).The mean scores reported by the caregivers was20.09, by their husbands, 19.23, and by their chil-dren, 20.91.
Caregiving mastery included items with factorloadings ranging from .46 to .90. The 6-item scaleincluded reports about the extent to which the re-spondent felt: (a) able to handle most problems inthe care of their elder; (b) able to figure out whattheir elder needs; (c) reassured knowing that as longas they are helping their elder she or he is gettingproper care; (d) uncertain about what to do abouttheir elder; (e) that they should be doing more fortheir elder; and (f) that they could do a better job incaring for their elder. Scores on the scale rangedfrom 6 to 30, with higher scores indicating less mas-tery. Coefficient alphas ranged from .58 (children) to.70 (caregivers). The mean scores reported by thecaregivers was 11.57, by their husbands, 12.55, andby their children, 14.61.
Depressive symptoms were measured using the 20-item Center for Epidemiological Studies DepressionIndex (CES-D; Radloff, 1977). Scores on the scale rangefrom 0 to 60, with higher scores indicating greaterdepressive symptomatology. Coefficient alphas rangedfrom .87 (husbands) to .93 (caregivers). The mean scorereported by primary caregivers was 10.66, by theirhusbands, 6.74, and by their children, 12.05.
Analysis
Although studies that collect data from multiplefamily members have successfully advanced ourknowledge base, most have not gone beyond basicdescriptive information regarding the similaritiesand differences that characterize individual reports.Moving from the individual as the unit of analysis bycombining data from multiple family members toconstruct variables that describe families has beensuggested by family sociologists (Mangen & McChes-ney, 1988; Thompson & Walker, 1982). The ways inwhich these variables are created, however, are asdiverse as the questions the data seek to address.Fisher, Kokes, Ransom, Phillips, and Rudd (1985),Draper and Marcos (1990), and Pruchno (1989,1994)provided guidelines for the creation of family varia-bles. Strategies for combining scores include crea-tion of a mean score, summative score, discrepancyscore, maximized couple score, couple ratio score,percent agreement score, and creation of typologiesbased on multiple reports. With respect to the crea-tion of typologies, strategies include those that aretheoretically based and those that are atheoretical.Probably the most well-recognized methodology forcreating typologies is cluster or factor analysis. Thesetechniques, however, are atheoretical and based on
an empirical model with the data alone dictating theoutcome (Fisher et al., 1985).
Because the goal of these analyses was to create atypology reflective of the degree to which caregiversand their family members agree on the extent towhich behaviors characterize the elder, the follow-ing procedures were used to develop a family typol-ogy. Using the caregiver's rating as a base, absolutedifference scores were created for each behaviorbetween the caregiver's rating and the rating madeby her husband. Unlike difference scores, whichreveal information about which reporter had higherscores, absolute difference scores focus only on themagnitude of the differences and represent the con-struct of interest. Absolute difference scores result inpositive scores. Similar procedures were used tocreate absolute difference scores between the care-giver and her child. These absolute difference scoreswere then added across behaviors for each family.Absolute difference scores for families ranged from 1to 62, with a mean of 25.8. Higher absolute differencescores reflect families in which greater disagreementcharacterized reports about their elderly relative'sbehavior, whereas lower absolute difference scoresreflect families in which greater agreement charac-terize their reports.
A typology was created from these absolute differ-ence scores so that differences between familieswhere agreement was high and where agreementwas low could be examined. Although there arenumerous ways for dividing a sample into threegroups, the chosen procedure divided the sampleinto three groups using one standard deviation fromthe mean to create the two breakpoints. This proce-dure was selected because it affords the opportunityto examine differences between the two extremegroups. This procedure resulted in 40 families beingcharacterized by high agreement (difference scoresranging from 1 to 12), 152 families being character-ized as having moderate agreement (differencescores ranging from 13 to 39), and 38 families beingcharacterized as low agreement (difference scoresranging from 40-62).
Family composite scores were created to reflectreports made by husbands and their wives of theelder's physical health conditions, and by husbands,wives, and children of the number of hours of helpthe elder received from these three family members.The first composite was created by counting thenumber of independent health problems that eitherthe husband or wife reported. Described as a "maxi-mized couple" score by Draper and Marcos (1990),this type of composite score was selected becausethe goal was to capture every possible physicalhealth condition characterizing the elder. This scoreis based on the systems theory idea that if a conditionis important enough to be reported by one person, itmost likely affects the entire system. If either thehusband or the wife indicated that the elder sufferedfrom a physical health problem, it was scored. If bothidentified the physical health problem, it was stillcounted only once. Scores on the composite variable(total illnesses) ranged from 0 to 18 (mean 6.7). The
Vol. 37, No. 2,1997 161
Dow
nloaded from https://academ
ic.oup.com/gerontologist/article/37/2/157/617002 by guest on 04 February 2022
second composite (total help hours) was created as acount of the total number of hours of help per weekthe elder received from the three reporters. Scoresranged from 1 to 175 (mean 33.15).
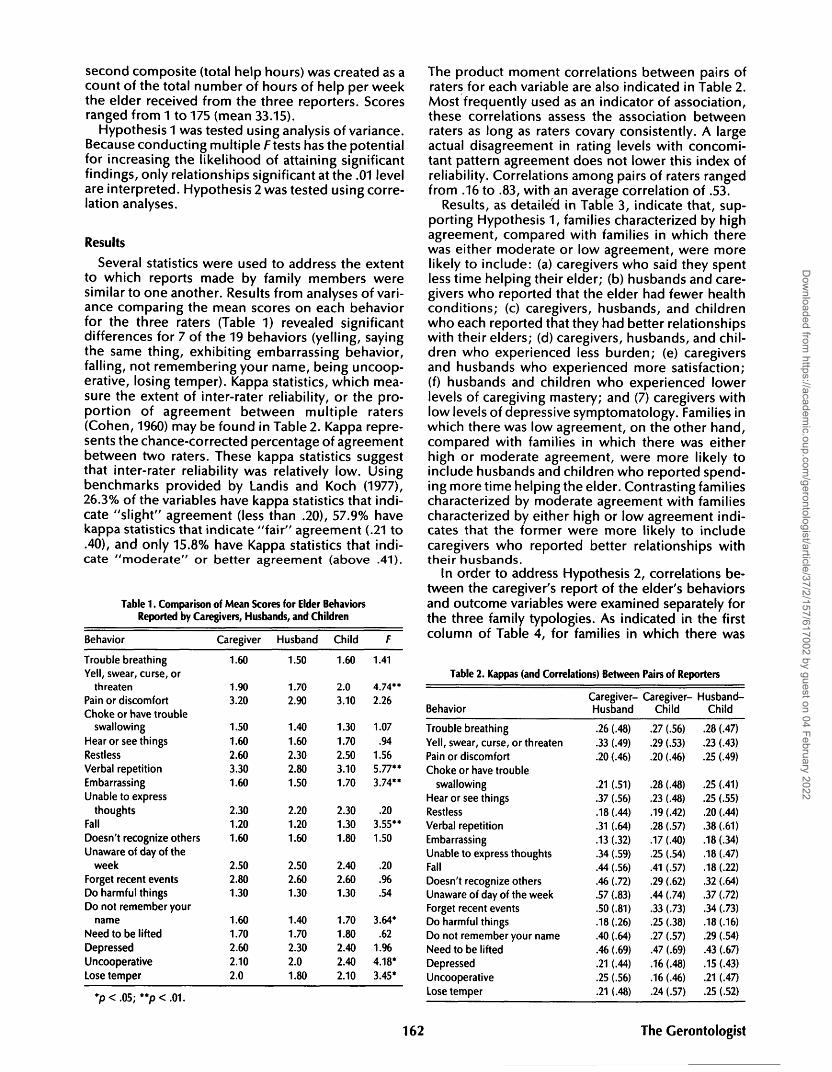
Hypothesis 1 was tested using analysis of variance.Because conducting multiple F tests has the potentialfor increasing the likelihood of attaining significantfindings, only relationships significant at the .01 levelare interpreted. Hypothesis 2 was tested using corre-lation analyses.
Results
Several statistics were used to address the extentto which reports made by family members weresimilar to one another. Results from analyses of vari-ance comparing the mean scores on each behaviorfor the three raters (Table 1) revealed significantdifferences for 7 of the 19 behaviors (yelling, sayingthe same thing, exhibiting embarrassing behavior,falling, not remembering your name, being uncoop-erative, losing temper). Kappa statistics, which mea-sure the extent of inter-rater reliability, or the pro-portion of agreement between multiple raters(Cohen, 1960) may be found in Table 2. Kappa repre-sents the chance-corrected percentage of agreementbetween two raters. These kappa statistics suggestthat inter-rater reliability was relatively low. Usingbenchmarks provided by Landis and Koch (1977),26.3% of the variables have kappa statistics that indi-cate "slight" agreement (less than .20), 57.9% havekappa statistics that indicate "fair" agreement (.21 to.40), and only 15.8% have Kappa statistics that indi-cate "moderate" or better agreement (above .41).
Table 1. Comparison of Mean Scores for Elder BehaviorsReported by Caregivers, Husbands, and Children
Behavior Caregiver Husband Child
The product moment correlations between pairs ofraters for each variable are also indicated in Table 2.Most frequently used as an indicator of association,these correlations assess the association betweenraters as long as raters covary consistently. A largeactual disagreement in rating levels with concomi-tant pattern agreement does not lower this index ofreliability. Correlations among pairs of raters rangedfrom .16 to .83, with an average correlation of .53.
Results, as detailed in Table 3, indicate that, sup-porting Hypothesis 1, families characterized by highagreement, compared with families in which therewas either moderate or low agreement, were morelikely to include: (a) caregivers who said they spentless time helping their elder; (b) husbands and care-givers who reported that the elder had fewer healthconditions; (c) caregivers, husbands, and childrenwho each reported that they had better relationshipswith their elders; (d) caregivers, husbands, and chil-dren who experienced less burden; (e) caregiversand husbands who experienced more satisfaction;(f) husbands and children who experienced lowerlevels of caregiving mastery; and (7) caregivers withlow levels of depressive symptomatology. Families inwhich there was low agreement, on the other hand,compared with families in which there was eitherhigh or moderate agreement, were more likely toinclude husbands and children who reported spend-ing more time helping the elder. Contrasting familiescharacterized by moderate agreement with familiescharacterized by either high or low agreement indi-cates that the former were more likely to includecaregivers who reported better relationships withtheir husbands.
In order to address Hypothesis 2, correlations be-tween the caregiver's report of the elder's behaviorsand outcome variables were examined separately forthe three family typologies. As indicated in the firstcolumn of Table 4, for families in which there was
Trouble breathing
Yell, swear, curse, or
threaten
Pain or discomfortChoke or have trouble
swallowing
Hear or see things
Restless
Verbal repetition
Embarrassing
Unable to express
thoughtsFall
Doesn't recognize others
Unaware of day of the
week
Forget recent events
Do harmful thingsDo not remember your
name
Need to be lifted
DepressedUncooperativeLose temper
*p<.05; **p<.01.1 ' 9
1.60
I.W3.20
1.50
1.60
2.60
3.30
1.60
2.30
1.20
1.60
2.50
2.80
1.30
1.60
1.70
2.60
2.10
2.0
1.50
I./U2.90
1.40
1.60
2.30
2.80
1.50
2.20
1.20
1.60
2.50
2.60
1.30
1.40
1.70
2.30
2.01.80
1.60
Z.\)3.10
1.30
1.70
2.50
3.10
1.70
2.30
1.30
1.80
2.40
2.60
1.30
1.70
1.80
2.40
2.40
2.10
1.41
A 7/ !••4./42.26
1.07
.941.56
5.77**
3.74**
.203.55**
1.50
.20
.%
.54
3.64*
.621.96
4.18*
3.45*
162
Table 2. Kappas (and Correlations) Between Pairs of Reporters
Behavior
Trouble breathingYell, swear, curse, or threaten
Pain or discomfort
Choke or have troubleswallowing
Hear or see things
Restless
Verbal repetition
Embarrassing
Unable to express thoughtsFall
Doesn't recognize others
Unaware of day of the week
Forget recent eventsDo harmful things
Do not remember your name
Need to be lifted
Depressed
Uncooperative
Lose temper
Caregiver-Husband
.26 (.48)
.33 (.49)
.20 (.46)
.21 (.51)
.37 (.56)
.18 (.44)
.31 (.64)
.13 (.32)
.34 (.59)
.44 (.56)
.46 (.72)
.57 (.83)
.50 (.81)
.18 (.26)
.40 (.64)
.46 (.69)
.21 (.44)
.25 (.56)
.21 (.48)
Caregiver-Child
.27 (.56)
.29 (.53)
.20 (.46)
.28 (.48)
.23 (.48)
.19 (.42)
.28 (.57)
.17 (.40)
.25 (.54)
.41 (.57)
.29 (.62)
.44 (.74)
.33 (.73)
.25 (.38)
.27 (.57)
.47 (.69)
.16 (.48)
.16 (.46)
.24 (.57)
Husband-Child
.28 (.47)
.23 (.43)
.25 (.49)
.25 (.41)
.25 (.55)
.20 (.44)
.38 (.61)
.18 (.34)
.18 (.47)
.18 (.22)
.32 (.64)
.37 (.72)
.34 (.73)
.18 (.16)
.29 (.54)
.43 (.67)
.15 (.43)
.21 (.47)
.25 (.52)
The Gerontologist
Dow
nloaded from https://academ
ic.oup.com/gerontologist/article/37/2/157/617002 by guest on 04 February 2022
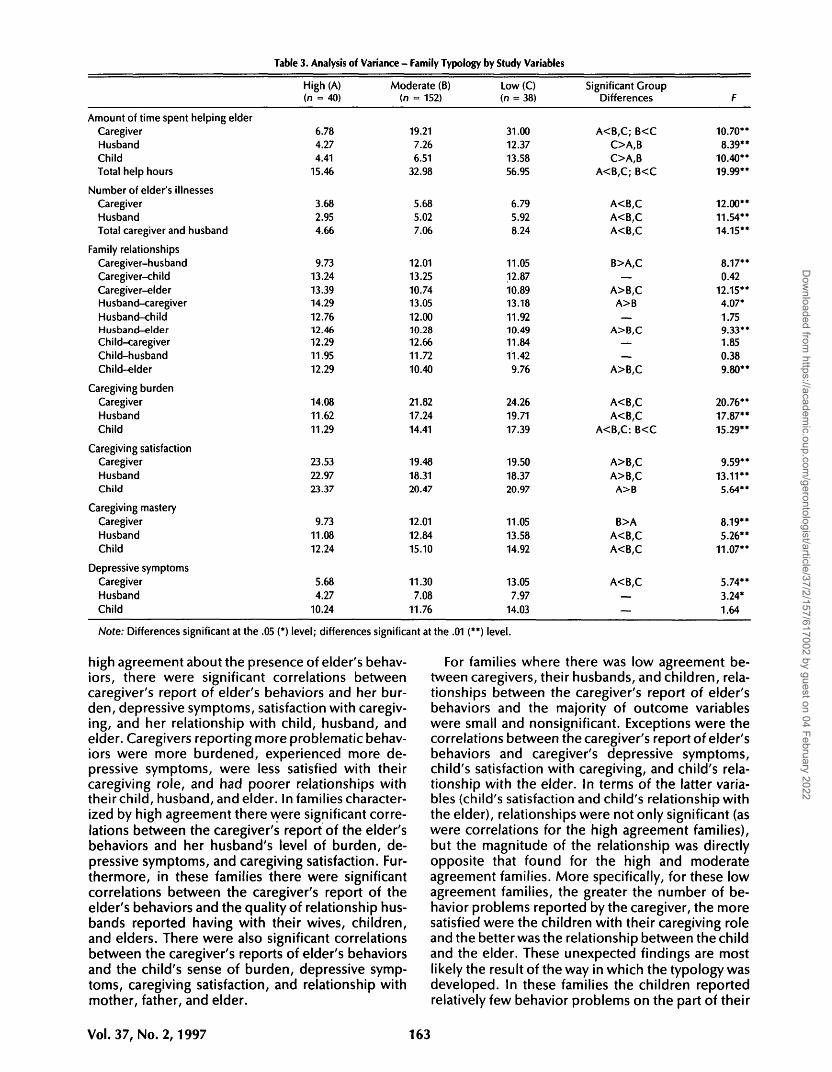
Table 3. Analysis of Variance - Family Typology by Study Variables
Amount of time spent helping elderCaregiverHusbandChildTotal help hours
Number of elder's illnessesCaregiverHusbandTotal caregiver and husband
Family relationshipsCaregiver-husbandCaregiver-childCaregiver-elderHusband-caregiverHusband-childHusband-elderChild-caregiverChild-husbandChild-elder
Caregiving burdenCaregiverHusbandChild
Caregiving satisfactionCaregiverHusbandChild
Caregiving masteryCaregiverHusbandChild
Depressive symptomsCaregiverHusbandChild
High (A)(n = 40)
6.784.274.41
15.46
3.68
2.954.66
9.7313.24
13.3914.29
12.7612.4612.29
11.95
12.29
14.0811.62
11.29
23.53
22.9723.37
9.73
11.0812.24
5.68
4.27
10.24
Moderate (B)(n = 152)
19.21
7.266.51
32.98
5.685.027.06
12.01
13.2510.7413.05
12.0010.2812.66
11.72
10.40
21.8217.24
14.41
19.48
18.3120.47
12.0112.84
15.10
11.30
7.08
11.76
Low (C)(n = 38)
31.0012.3713.5856.95
6.795.928.24
11.0512.87
10.8913.18
11.9210.4911.84
11.42
9.76
24.2619.71
17.39
19.50
18.3720.97
11.0513.5814.92
13.057.97
14.03
Significant GroupDifferences
A<B,C; B<CO A , BO A , B
A<B,C; B<C
A<B,CA<B,CA<B,C
B>A,C—
A>B,CA>B—
A>B,C—
—
A>B,C
A<B,CA<B,C
A<B,C: B<C
A>B,CA>B,C
A>B
B>AA<B,CA<B,C
A<B,C—
—
F
10.70**8.39**
10.40**19.99**
12.00**11.54**14.15**
8.17**0.42
12.15**4.07*
1.759.33**1.850.38
9.80**
20.76**17.87**
15.29**
9.59**
13.11**5.64**
8.19**5.26**
11.07**
5.74**3.24*1.64
Note: Differences significant at the .05 (*) level; differences significant at the .01 (**) level.
high agreement about the presence of elder's behav-iors, there were significant correlations betweencaregiver's report of elder's behaviors and her bur-den, depressive symptoms, satisfaction with caregiv-ing, and her relationship with child, husband, andelder. Caregivers reporting more problematic behav-iors were more burdened, experienced more de-pressive symptoms, were less satisfied with theircaregiving role, and had poorer relationships withtheir child, husband, and elder. In families character-ized by high agreement there were significant corre-lations between the caregiver's report of the elder'sbehaviors and her husband's level of burden, de-pressive symptoms, and caregiving satisfaction. Fur-thermore, in these families there were significantcorrelations between the caregiver's report of theelder's behaviors and the quality of relationship hus-bands reported having with their wives, children,and elders. There were also significant correlationsbetween the caregiver's reports of elder's behaviorsand the child's sense of burden, depressive symp-toms, caregiving satisfaction, and relationship withmother, father, and elder.
For families where there was low agreement be-tween caregivers, their husbands, and children, rela-tionships between the caregiver's report of elder'sbehaviors and the majority of outcome variableswere small and nonsignificant. Exceptions were thecorrelations between the caregiver's report of elder'sbehaviors and caregiver's depressive symptoms,child's satisfaction with caregiving, and child's rela-tionship with the elder. In terms of the latter varia-bles (child's satisfaction and child's relationship withthe elder), relationships were not only significant (aswere correlations for the high agreement families),but the magnitude of the relationship was directlyopposite that found for the high and moderateagreement families. More specifically, for these lowagreement families, the greater the number of be-havior problems reported by the caregiver, the moresatisfied were the children with their caregiving roleand the better was the relationship between the childand the elder. These unexpected findings are mostlikely the result of the way in which the typology wasdeveloped. In these families the children reportedrelatively few behavior problems on the part of their
Vol. 37, No. 2,1997 163
Dow
nloaded from https://academ
ic.oup.com/gerontologist/article/37/2/157/617002 by guest on 04 February 2022
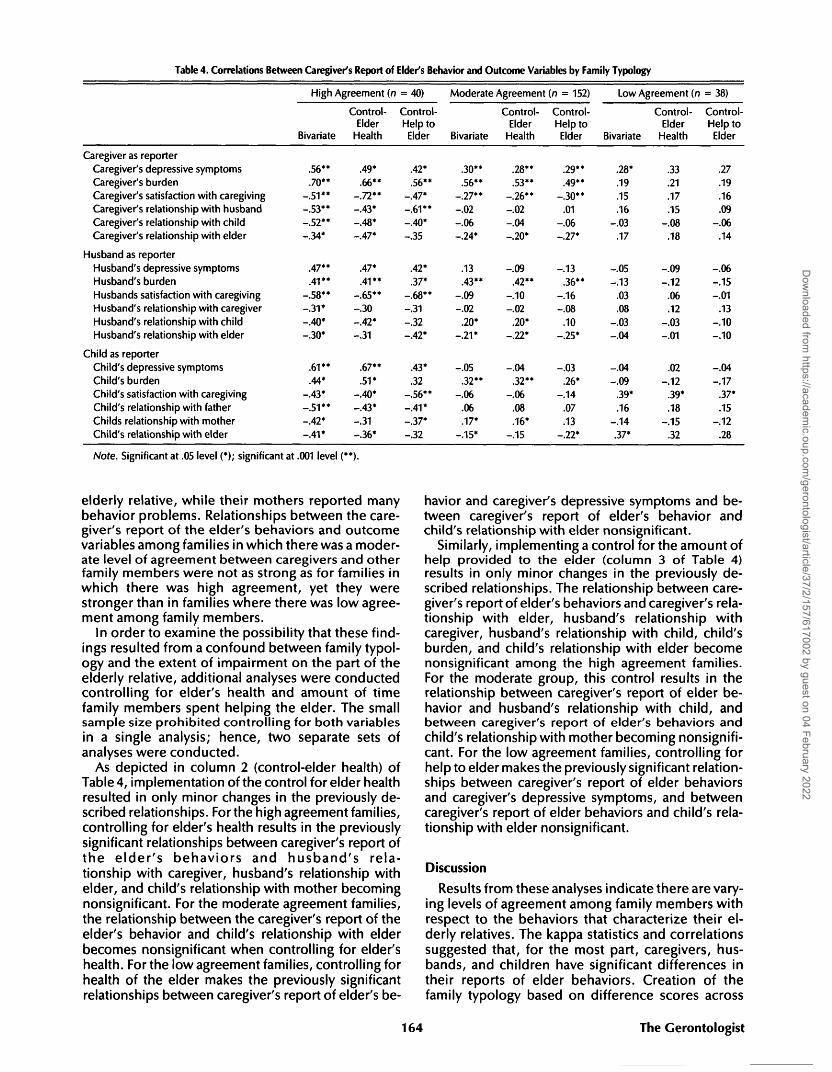
Table 4. Correlations Between Caregiver's Report of Elder's Behavior and Outcome Variables by Family Typology
High Agreement (n = 40) Moderate Agreement (n = 152) Low Agreement (n = 38)
Caregiver as reporterCaregiver's depressive symptomsCaregiver's burdenCaregiver's satisfaction with caregivingCaregiver's relationship with husbandCaregiver's relationship with childCaregiver's relationship with elder
Husband as reporterHusband's depressive symptomsHusband's burdenHusbands satisfaction with caregivingHusband's relationship with caregiverHusband's relationship with childHusband's relationship with elder
Child as reporterChild's depressive symptomsChild's burdenChild's satisfaction with caregivingChild's relationship with fatherChilds relationship with motherChild's relationship with elder
Bivariate
.56**
.70**-.51**-.53**-.52**-.34*
.47**
.41**-.58**-.31*-.40*-.30*
.61 **
.44*-.43*-.51**-.42*-.41*
Control-Elder
Health
.49*
.66**-.72**-.43*-.48*-.47*
.47*
.41**-.65**-.30-.42*-.31
.67**
.51*-.40*-.43*-.31-.36*
Control-Help toElder
.42*
.56**-.47*-.61**-.40*-.35
.42*
.37*-.68**-.31-.32-.42*
.43*
.32-.56**-.41*-.37*-.32
Bivariate
.30**
.56**-.27**-.02-.06-.24*
.13
.43**-.09-.02
.20*-.21*
-.05.32**
-.06.06.17*
-.15*
Control-Elder
Health
.28**
.53**-.26**-.02-.04-.20*
-.09.42**
-.10-.02
.20*-.22*
-.04.32**
-.06.08.16*
-.15
Control-Help toElder
.29**
.49**-.30**
.01-.06-.27*
-.13.36**
-.16-.08
.10-.25*
-.03.26*
-.14.07.13
-.22*
Bivariate
.28*
.19
.15
.16-.03
.17
-.05-.13
.03
.08-.03-.04
-.04-.09
.39*
.16-.14.37*
Control-Elder
Health
.33
.21
.17
.15-.08
.18
-.09-.12
.06
.12-.03-.01
.02-.12
.39*
.18-.15
.32
Control-Help toElder
27.19.16.09
-.06.14
-.06-.15-.01
.13-.10-.10
-.04-.17
.37*
.15-.12
.28
Note. Significant at .05 level (*); significant at .001 level (**).
elderly relative, while their mothers reported manybehavior problems. Relationships between the care-giver's report of the elder's behaviors and outcomevariables among families in which there was a moder-ate level of agreement between caregivers and otherfamily members were not as strong as for families inwhich there was high agreement, yet they werestronger than in families where there was low agree-ment among family members.
In order to examine the possibility that these find-ings resulted from a confound between family typol-ogy and the extent of impairment on the part of theelderly relative, additional analyses were conductedcontrolling for elder's health and amount of timefamily members spent helping the elder. The smallsample size prohibited controlling for both variablesin a single analysis; hence, two separate sets ofanalyses were conducted.
As depicted in column 2 (control-elder health) ofTable 4, implementation of the control for elder healthresulted in only minor changes in the previously de-scribed relationships. For the high agreement families,controlling for elder's health results in the previouslysignificant relationships between caregiver's report ofthe elder 's behaviors and husband's rela-tionship with caregiver, husband's relationship withelder, and child's relationship with mother becomingnonsignificant. For the moderate agreement families,the relationship between the caregiver's report of theelder's behavior and child's relationship with elderbecomes nonsignificant when controlling for elder'shealth. For the low agreement families, controlling forhealth of the elder makes the previously significantrelationships between caregiver's report of elder's be-
havior and caregiver's depressive symptoms and be-tween caregiver's report of elder's behavior andchild's relationship with elder nonsignificant.
Similarly, implementing a control for the amount ofhelp provided to the elder (column 3 of Table 4)results in only minor changes in the previously de-scribed relationships. The relationship between care-giver's report of elder's behaviors and caregiver's rela-tionship with elder, husband's relationship withcaregiver, husband's relationship with child, child'sburden, and child's relationship with elder becomenonsignificant among the high agreement families.For the moderate group, this control results in therelationship between caregiver's report of elder be-havior and husband's relationship with child, andbetween caregiver's report of elder's behaviors andchild's relationship with mother becoming nonsignifi-cant. For the low agreement families, controlling forhelp to elder makes the previously significant relation-ships between caregiver's report of elder behaviorsand caregiver's depressive symptoms, and betweencaregiver's report of elder behaviors and child's rela-tionship with elder nonsignificant.
Discussion
Results from these analyses indicate there are vary-ing levels of agreement among family members withrespect to the behaviors that characterize their el-derly relatives. The kappa statistics and correlationssuggested that, for the most part, caregivers, hus-bands, and children have significant differences intheir reports of elder behaviors. Creation of thefamily typology based on difference scores across
164 The Gerontologist
Dow
nloaded from https://academ
ic.oup.com/gerontologist/article/37/2/157/617002 by guest on 04 February 2022
behaviors revealed a somewhat different trend. To-gether, however, these different approaches tostudying multiple family members present a coher-ent picture. The data indicate that the majority offamilies are characterized by moderate levels ofagreement, whereas a subset of families have highlevels of agreement and a subset of families have lowlevels of agreement.
Several explanations may illustrate why familymembers disagree about the condition of the elder.Each explanation focuses on the interaction betweenthe person who is the reporter and the behavior. First,family members may disagree because individuals inthe family have differing levels of interaction or expe-rience with the elderly member. When a caregiver, forexample, reports higher levels of problematic behav-ior on the part of the elder and their husband andchildren report much lower levels of these behaviors,it may be because the caregiver is home all day withthe elder and has the opportunity to interact morewith the elder. An alternative explanation may be thatfamily members have different ranges of tolerance forbehaviors. As such, one family member may over-report a behavior in relationship to other family mem-bers because he or she is particularly sensitive to thebehavior. For an individual who is sensitive to yelling,for example, having an elder yell at him or her oncemay be over-reported because it is so troubling.Other family members, who may have a greater toler-ance for yelling, may report this behavior as occurringless frequently. Yet another explanation may be thatreport of current behaviors is influenced by the pre-vious relationship that the individual had with theelderly person. For people who previously had a veryclose relationship with the elderly person, problem-atic behaviors may be under-reported as they over-look the behaviors and remember the person whoonce was. For others whose previous relationship wascharacterized by strife, current behaviors may be evenmore troublesome.
Regardless of the reason for different reports,these data support Hypothesis 1, with findings sug-gesting that when family members have similar per-ceptions regarding their elderly relative, levels ofcaregiving burden and depression experienced bycaregivers, their husbands, and children are lower,and levels of caregiving satisfaction and mastery aregreater. These results also indicate that there aresignificant differences among families in which thereare high as opposed to low levels of agreementregarding the elder's condition. Family relationships,for example, are better among families who agreeabout the behaviors characterizing the elder. Al-though data that directly address the processes in-volved in family interactions were not collected inthis study, it might be hypothesized that families inwhich members agree with one another are thosefamilies whose members work together with oneanother to cope with the demands made by theelder's situation. In these families, individuals agreewith one another because they interact with oneanother frequently, talk about problems that arise,and try to solve them as a team.
Results from these analyses are consistent withDurkheim's (1933) observation that families having acommon conscience appear to be less affected bystressors than families who lack a common con-science. Similarly, consistent with Hill's (1949) senseof family integration as central to successful adjust-ment of individuals, these analyses highlight the im-portance of similar perceptions for adjustment to thedemands of caregiving.
The analyses also support Hypothesis 2, with thecaregiver's report of stressors having a different rela-tionship with various outcome measures dependingon the extent to which her reports are consistent withothers in the family. When family members agreeabout the stressors in the household, the caregiver'sreport of stressors correlates significantly not onlywith her own caregiving burden, satisfaction, mas-tery, and overall level of depressive symptoms, butalso with that of the other family members. Addition-ally, relationships among family members are corre-lated with these reports. However, when the reportsmade by caregivers differ from those made by otherfamily members, the caregiver's report of stressors isnot associated with these variables.
It is tempting to interpret results regarding consist-ency of reports among family members in terms ofthe degree of objectivity of an individual's report. Assuggested earlier, greater consistency of report mayserve as an indicator of the extent to which an indi-vidual's report of the stressors is separate and apartfrom his or her response or reaction to the stressor.The positive relationship between stressors and out-comes among caregivers in high agreement familiesand the absence of these relationships among lowagreement families suggests that when the stressorsassociated with caregiving are truly external to thecaregiver, the predicted relationships between stres-sors and outcomes hold, with greater stressors beingassociated with more negative outcomes and lesspositive outcomes. When the reports of stressors areless objective, and the caregiver's report is not cor-roborated by other family members, stressors arenot related to outcomes. These findings suggest that,at least for families in which the caregiver's report ofelder behaviors is objective, positive relationshipsbetween stressors and outcomes can probably beinterpreted as providing evidence that caregiverswho have realistic perceptions of the demands ofcaregiving are upset by the stressors. On the otherhand, there is no parallel relationship among stres-sors and outcomes for caregivers who lack a realisticperception of the demands of caregiving. Althoughinteresting to ponder, this interpretation must betempered by Larsen and Olsen's (1990) caveat that itis problematic to conclude that multiple family mem-bers can provide a more valid reality than can a singlefamily member; hence, better understanding of thecausal relationship between stressors and outcomesawaits future study.
Generalization of results is limited for several rea-sons. First, the strategy used to define the familytypology, that is, developing groups based on cutoffsof one standard deviation from the mean is not one
Vol. 37, No. 2,1997 165
Dow
nloaded from https://academ
ic.oup.com/gerontologist/article/37/2/157/617002 by guest on 04 February 2022

that is frequently used. It was selected, however,because the goal of the analysis was to separate, asmuch as possible, those families where agreementwas high from those families where agreement waslow. It should be noted, however, that standarddeviations are dependent on the particular samplebeing analyzed, and consequently, the extent ofgeneralizability of findings awaits replication. A sec-ond limitation is that this methodology resulted insmall sample sizes characterizing the high and lowagreement families. As such, analyses were limitedto examination of correlations and univariate analy-ses. Nonetheless, the patterns characterizing thedata are intriguing and result in a host of questionsregarding the usefulness and meaning of individualreports. Additionally, although focusing on families,the data collected derived only from three membersof each family. Generalization from three membersof a family to the whole family is premature. Further-more, the strategy of identifying the third generationfor inclusion in the study (when more than one childmet study criteria) was somewhat random. Askingthe caregiver to nominate the child they felt hadbeen most affected by the multigeneration livingsituation most likely resulted in some children beingnominated because they provided a great deal ofcare to the elder, whereas others may have beennominated because their school grades had sufferedthe most. A shortfall of this project was failure toexamine why each child was nominated. Ideally,however, research focusing on the dynamics of thehousehold should include data collected from allhousehold members. Balancing the complex reali-ties of data collection with this goal is a significantchallenge for future research.
Despite these limitations, results from this studyprovide an interesting context in which to interpretfindings from existing caregiving research studies.For the majority of caregiving families in this study,reports about the elder's behaviors made by thecaregiver and those made by other household mem-bers are moderately similar. In these families, re-ports of stressors made by the caregiver relate inpredictable fashion to what existing theories sug-gest. When, however, reports made by the caregiverare different from those made by other family mem-bers, knowing the caregiver's report of the fre-quency with which these behaviors occur has littleassociation with the outcomes experienced by thecaregiver, her husband, or child.
The lack of relationship between the caregiver'sreport of stressors and the outcome variables in theabsence of family agreement is both fascinating andtroublesome. Questions that suggest themselves in-clude what, if anything, do these reports relate to,and what is it that does predict well-being for peopleliving in households where family members do notagree about the presence or absence of behaviorscharacterizing the elderly member?
Data collected from multiple members of a house-hold have the potential to be very rich. They can alsobe very puzzling. It is clear that in order to under-stand what goes on in caregiving families we need to
reach beyond the primary caregiver. Including multi-ple family members in research studies, however, ismerely the first step in increasing our understandingof the effects that caregiving has on families. Studiesthat limit themselves to comparison of reports frommultiple individuals provide little if any new informa-tion about what goes on within families. In order toincrease our knowledge about the functioning offamilies, analyses must maintain the integrity of thefamily. Family typologies, such as that developedhere, provide a useful beginning for understandingthe complexities that exist within families.
Data collected from multiple family members alsohave important practical implications. When infor-mation is provided from multiple family members, aricher, more complex picture of the caregiving situa-tion exists. Practitioners are advised to gather infor-mation about older people from multiple familymembers, listening carefully to where there are simi-larities and where there are differences in the re-ports. Such information can be invaluable for under-standing the dynamics that guide both familyinterventions and interventions targeted toward pri-mary caregivers. Furthermore, data provided by mul-tiple family members have the potential to makefamily members feel that they are integral to thegoals of any family intervention, thereby makingpractitioners more effective in their efforts to helpcaregiving families.
References
Brody, E. M. (1985). Parent care as a normative family stress. The Gerontolo-gist, 25,19-29.
Brody, E. M., Hoffman, C , Kleban, M. H., & Schoonover, C. B. (1989).Caregiving daughters and their local siblings: Perceptions, strains, andinteractions. The Cerontologist, 29(4), 529-538.
Cohen, J. (1960). A coefficient of agreement for nominal scales. EducationalPsychological Measurement, 20, 37-46.
Deimling, G. T., & Bass, D. M. (1986). Symptoms of mental impairmentamong elderly adults and their effects on family caregivers. Journal ofGerontology, 41, 778-784.
Deutsch, M. (1968). Field theory in social psychology. In C. Lindzey & E.Aronson (Eds.). The handbook of social psychology (pp. 412-487).Reading, MA: Addison-Wesley.
Draper, T. W., & Marcos, A. C. (1990). Family variables: Conceptualization,measurement, and use. Newbury Park, CA: Sage.
Durkheim, E. (1933). The division of labor in society (H. Simpson Trans.).New York: Free Press.
Fengler, A. P., & Goodrich, N. (1979). Wives of elderly disabled men: Thehidden patients. The Gerontologist, 19, 175-183.
Fisher, L, Kokes, R. F., Ransom, D. C , Phillips, S. L , & Rudd, P. (1985).Alternative strategies for creating "relational" family data. Family Pro-cess, 24, 213-224.
George, L, &Gwyther, L. (1986). Caregiver well-being: A multidimensionalexamination of family caregivers of demented adults. The Gerontolo-gist, 26, 253-259.
Gilhooly, M. L. M. (1984). The impact of caregiving on caregivers: Factorsassociated with the psychological well-being of people supporting ademeriting relative in the community. British journal of Medical Psy-chology, 57, 35-44.
Grad, J., & Sainsbury, P. (1968). The effects that patients have on their familyin a community care and control psychiatric service—a two year follow-up. British Journal of Psychiatry, 114, 265-278.
Haley, W. E., Brown, S. L.,& Levine, E. G. (1987). Family caregiver appraisalsof patient behavioral disturbance in senile dementia. Clinical Gerontol-ogist, 6(4), 25-34.
Hill, R. (1949). Families under stress: Adjustment to the crises of warseparation and reunion. Westport, CT: Greenwood Press.
Jessop, D. J. (1981). Family relationships as viewed by parents and adoles-cents: A specification. Journal of Marriage and the Family, 95-107.
Landis, J. R., & Koch, G. G. (1977). The measurement of observer agreementfor categorical data. Biometrics, 33,159-174.
Larsen, A., & Olson, D. (1990). Capturing the complexity of family systems:Integrating family theory, family scores, and family analysis. In T. W.
166 The Gerontologist
Dow
nloaded from https://academ
ic.oup.com/gerontologist/article/37/2/157/617002 by guest on 04 February 2022
Draper & A. C. Marcos (Eds.), Family variables: Conception, measure-ment, and use (pp. 19-47). Newbury Park, CA: Sage.
Lawton, M. P., Brody, E. M., & Saperstein, A. R. (1989). A controlled study ofrespite service for caregivers of Alzheimer's patients. The Gerontolo-gist, 29, 8-16.
Lawton, M. P., Moss, M., Kleban, M. H., & Glicksman, A., & Rovine, M.(1991). A two-factor model of caregiving appraisal and psychologicalwell-being. Journal of Gerontology: Psychological Sciences, 46, P181-P189.
Lawton, M. P., & Nahemow, L. (1973). Ecology and the aging process. In C.Eisdorfer & M. P. Lawton (Eds.), Psychology of adult development andaging (pp. 619-674). Washington, DC: American Psychological Associa-tion.
Mangen, D., & McChesney, K. Y. (1988). Intergenerational cohesion: Acomparison of linear and nonlinear analytical approaches. In D. J.Mangen, V. L. Bengtson, & P. H. Landry (Eds.), Measurement of in-tergenerational relations (pp. 208-221). Newbury Park, CA: Sage.
Matthews, S. H., Adamek, M. E., & Dunkle, R. E. (1993). Research on olderfamilies when more than one member responds: Producing and inter-preting findings. Journal of Aging Studies, 7, 215-228.
Montgomery, R. J. V., Gonyea, J. G., & Hooyman, N. R. (1985). Caregivingand the experience of subjective and objective burden. Family Rela-tions, 34,19-26.
Morycz, R. K. (1985). Caregiving strain and the desire to institutionalizefamily members with Alzheimer's disease. Research on Aging, 2,329-361.
Murray, H. A. (1938). Explorations in personality. New York: Oxford.Ory, M. G., Williams, T. F., Emr, M., Lebowitz, B., Rabins, P., Salloway, J.,
Sluss-Radbaugh, T., Wolff, E., & Zarit, S. (1985). Families, informalsupports, and Alzheimer's disease. Research on Aging, 7, 623-644.
Pearlin, L. I., Mullan, J. T., Semple, S. J., & Skat, M. M. (1990). Caregivingand the stress process: An overview of concepts and their measures.The Gerontologist, 30, 583-591.
Pearson, J., Verma, S., & Nellett, C. (1988). Elderly psychiatric patient status
and caregiver perceptions and predictors of caregiver burden. TheGerontologist, 28, 79-83.
Pruchno, R. A. (1989). Alzheimer's disease and families: Methodologicaladvances. In E. Light & B. D. Lebowitz (Eds.), Alzheimer's diseasetreatment and family stress: Directions for research. Bethesda, MD:National Institute of Mental Health.
Pruchno, R. A. (1994). Studying caregiving families: Theoretical and meth-odological challenges. In E. Light, G. Niederhe, & B. D. Lebowitz (Eds.),Stress effects on family caregivers of Alzheimer's patients (pp. 333-350).New York: Springer.
Radloff, L. (1977). The CES-D Scale: A self-report depression scale forresearch in the general population. Applied Psychological Measure-ment, 1, 385-401.
Singer, E. (1973). Agreement between 'inaccessible' respondents and in-formants. Public Opinion Quarterly, 36, 603-611.
Thompson, L., & Walker, A. J. (1982). The dyad as the unit of analysis:Conceptual and methodological issues. Journal of Marriage and theFamily, 44, 889-900.
Townsend, A. L., & Poulshock, S. W. (1986). Intergenerational perspectiveson impaired elders' support networks. The Journals of Gerontology, 41,101-109.
Walker, A., & Thompson, L. (1983). Intimacy and intergenerational aid andcontact among mothers and daughters. Journal of Marriage and theFamily, 45, 841-849.
Zarit, S. H., Reever, K. E., & Bach-Peterson, J. (1980). Relatives of theimpaired aged: Correlates of feelings of burden. The Cerontologist, 20,649-655.
Zarit, S. H., Todd, P. A., & Zarit, J. M. (1986). Subjective burden of husbandsand wives as caregivers: A longitudinal study. The Gerontologist, 26,260-266.
Received July 17, 1995Accepted August 13, 1996
Two VacanciesDeputy Associate Chief of Staff for Geriatrics & Extended Care
andAcademic Geriatrician
The South Texas Veterans Health Care System (STVHCS), VA Hospital, San Antonio and the University of Texas Health Science Center at SanAntonio (UTHSCSA) are seeking qualified candidates for two positions: a Deputy Associate Chief of Staff for Extended Care at the Kerrviile Division, and anAcademic Geriatrician at the ALM Division in San Antonio. Applicants will be expected to participate in university and community activities requisite of aUTHSCSA faculty appointment.
The Deputy ACOS will assume primary responsibilities for academic and clinical activities in all geriatric programs at the Kerrviile Division. TheAcademic Geriatrician will be located at the ALM Division in San Antonio and the UTHSCSA. The Kerrviile Division is located approximately one houraway from San Antonio, in a scenic rural community nestled in the Texas Hill Country with a large retirement-age population.
A wide spectrum of Geriatrics and Extended Care Programs are functioning at the STVHCS and UTHSCSA, including: outpatient geriatric primary careclinics, acute geriatric inpatient care, in- and outpatient hospice, an inpatient Alzheimer's treatment unit, Adult Day Health Care (ADHC), Hospital-BasedPrimary Care (HBPC), two Nursing Home Care Units (NHCU), in- and outpatient rehabilitative care and community residential care program.
A full range of research, educational, and clinical collaborators are available for academic activities. The STVHCS and UTHSCSA jointly sponsoraccredited geriatric training programs, including: a geriatric medicine fellowship, a geropsychology postdoctoral fellowship, a geriatric dental fellowship, andclinical pharmacy residency training. Salary and benefits commensurate with training and experience.
Please send curriculum vitae to:Meghan B. Gerety, MD
ACOS for Geriatrics & Extended Care (18)STVHCS
7400 Merton Minter Blvd.San Antonio, TX 78284
(210)617-5237The STVHCS and UTHSCSA are Equal Opportunity Employers.
Vol.37, No. 2,1997 167
Dow
nloaded from https://academ
ic.oup.com/gerontologist/article/37/2/157/617002 by guest on 04 February 2022
Audiovisual Review EditorshipANNOUNCEMENT
After many years of dedicated and much appreciated service, Andrea Nevins has
stepped down as Audiovisual Review Editor for The Gerontologist. Members of the Society
with a strong critical interest in film, video, and related media who might be interested in
serving in the position are invited to apply. Please send a letter of interest, accompanied by
a resume and a one-page statement indicating what you would desire regarding the future
mission and format of the Audiovisual Review section, including what changes, if any, you
would make to its current form. Correspondence should be sent to me at the address
indicated on the inside back cover of this issue.
Vernon L. Greene, PhD
Editor in Chief
NOTICE TO AUTHORS
Beginning January 1,1997Manuscripts for
The GerontologistShould Be Sent to
Vernon L. Greene, PhDCenter for Policy Research
Maxwell School of Citizenship and Public AffairsEggers Hall, Syracuse University
Syracuse, NY 13244-1090
168 The Gerontologist
Dow
nloaded from https://academ
ic.oup.com/gerontologist/article/37/2/157/617002 by guest on 04 February 2022





























