Embed Size (px)
Citation preview

Available online at www.sciencedirect.com
South African Journal of Botany 82 (2012) 60–66www.elsevier.com/locate/sajb
Review
Ensuring quality in herbal medicines: Toxic phthalates in plastic-packagedcommercial herbal products
A.R. Ndhlala, B. Ncube, J. Van Staden ⁎
Research Centre for Plant Growth and Development, School of Life Sciences, University of KwaZulu-Natal Pietermaritzburg, Private Bag X01, Scottsville 3209,South Africa
Available online
5 September 2012Abstract
There is a proliferation in the use of commercial herbal preparations, most notably liquid preparations of plant material packaged in plasticcontainers. The quality of these herbal preparations has always and still remains questionable. A number of research institutes and research groupsin tertiary institutions throughout South Africa have embarked on the development of quality control programmes to test herbal medicines forsafety and efficacy. However, very few of these groups have placed any emphasis on commercial herbal mixtures. This paper describes someeffects of toxic phthalates such as bis(2-ethylhexyl) phthalates, (a common plasticiser) used in cheap soft plastics and its metabolites. Analyticalmethods for the determination, quantification and monitoring of DEHP in herbal remedies to ensure safety are also highlighted.© 2012 SAAB. Published by Elsevier B.V. All rights reserved.
Keywords: Bis(2-ethylhexyl) phthalates; Herbal products; Phthalates; Quality control
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 602. Phthalate contaminants in herbal products . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 613. DEHP biomarkers of exposure and effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
3.1. Phthalates and the reproductive development in human infants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 623.2. Phthalates and respiratory function, asthma, and allergy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
4. The fate of DEHP: Its metabolites and their effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 625. Tolerable daily intake and minimal risk level . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 636. Analytical methods for determining DEHP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 637. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
1. Introduction
Despite its negative consequence on plant biodiversity anddestabilisation of most ecosystems, the inter-relationship between
⁎ Corresponding author. Tel.: +27 33 2605130; fax: +27 33 2605897.E-mail address: [email protected] (J. Van Staden).
0254-6299/$ -see front matter © 2012 SAAB. Published by Elsevier B.V. All rightdoi:10.1016/j.sajb.2012.07.004
society and nature, and the importance of herbal medicine tohuman health, continues to dominate most medical traditions.Plants form an integral part of virtually every medicinalsystem in both modern and less civilised societies. SouthAfrica is one of the countries that are richly bestowed withboth floral and cultural diversity, and for this reason thepopulation exploits phytomedicines as part of their medical
s reserved.

61A.R. Ndhlala et al. / South African Journal of Botany 82 (2012) 60–66
tradition. A large number of medicinal plants are regularly sold aseither crude, unprocessed material, semi-processed or processedas commercial herbal preparations (CHP) on various traditionalmarkets across the country (Mander, 1998; Ndhlala et al., 2011b;Williams et al., 2000). As a result of urbanisation and theconsequent commercialisation of traditional health care, thedemand for herbal medicine has increased significantly in mostSouth African cities. There exists an insatiable market for theseproducts from most urban dwellers, on which traders capitalise.Among the herbal products sold in urban areas, CHPs dominatethis market (Ndhlala et al., 2011b). This has become a modernavenue for traditional plant-derived therapeutics in South Africa.
Although herbal medicines are widely used for the prevention,diagnosis, treatment and management of disease, quality controlremains the biggest challenge. The widely held perception, byherbal medicinal users, that natural plant-derived products aresafe, effective and non-toxic, has often left unsuspecting con-sumers exposed to a multitude of risks associated with the useand/or overuse of these products. It is important that the generalpublic be warned of the range of possible dangers that emanatefrom using these plant-derived products. CHPs present somecomplications to herbal medicine with regard to efficacy, safetyand quality. Chemical interactions between and among theconstituents of the component plant species in each preparationcould be diverse and result in synergism, antagonism, or toxicity(Ncube et al., 2012; Ndhlala et al., 2009) within the human body.Herbal preparations are produced and packaged by privateentrepreneurs (Ndhlala et al., 2009), and their quality, efficacyand safety are determined by the manufacturing conditions,condition and quality of material used for packaging, quantityand type of component plant species used, as well as their storageand handling, all of which remain solely under the control of themanufacturer and distributor. Production and marketing of theseproducts have become a lucrative business in most cities of SouthAfrica, to such an extent that their quality and safety has oftenbeen overlooked in an effort to make a profit. As a result,consumers are offered products that are sub-standard andpackaged using cheap recycled plastic materials (Nair et al.,2012). Could such herbal products deliver health benefits or arethey a potential health hazard to consumers? Logically, onewould be compelled to view such products as weapons of death.Herbal preparations in general, are probably characterised withimpure, contaminated and sometimes lethally toxic componentsthat pose risks to humankind. A solution to this lies in intensivescreening of these products and the subsequent enacting of, andstrict adherence to, quality and safety regulations. Consideringthe large number of people relying on these products on a day today basis and the associated health concerns, an interest wasaroused in their pharmacological and toxicological screening(Nair et al., 2012; Ndhlala et al., 2010a,b, 2011a), in which bothpositive and negative effects have been reported.
Among the negative reports on the CHP, the most recent andpotentially worrying discovery, is the isolation of a commercialplasticiser di(2-ethylhexyl) phthalate (DEHP) from one of themost popular preparations (Nair et al., 2012). This adds anotherdimension to the safety and quality concerns of CHPs sold inSouth African medicinal markets. An assessment of the possible
risks of phthalate contaminants and its metabolites in herbalproducts, as well as the minimum daily tolerable levels, areoutlined in this review. Analytical methods for the determination,quantification and monitoring of DEHP in herbal remedies toensure safety are also highlighted.
2. Phthalate contaminants in herbal products
An increasing social concern has been aroused by the adverseeffects on public health caused by phthalates. Phthalates havebeen shown to have endocrine disrupting properties resulting incarcinogenic effects, metabolic disorders, and developmental andreproductive defects (Hauser et al., 2006; Mahood et al., 2007;Willhite, 2001). DEHP is used as a plasticiser in polyvinylchloride (PVC) plastics, rubber, cellulose and styrene productionto impart flexibility, strength, broad-range temperature tolerance,and optical clarity (Chen et al., 2004). Phthalates are used in awide variety of consumer products and applications, that includegelling agents, medical devices, cosmetics, adhesives, lubricants,dispersants, food wrappings, nail polish, plastic goods, kitchenplastic ware and emulsifying agents (Chen et al., 2004; Wormuthet al., 2006). Since phthalates are not chemically bound to theseproducts, leaching and migration of these substances result insignificant environmental contamination and human exposure isa common phenomenon (Clewell et al., 2008; Mahood et al.,2007; Wormuth et al., 2006).
CHPs are, particularly those that are packed using cheaprecycled plastic materials, no exception to this contamination.These contaminants could reach alarming levels in these productsin South Africa, owing to the fact that there are no effectivequality regulation mechanisms and/or policies with regard to themanufacturing and handling of these products (Ndhlala et al.,2011b). The highly toxic phthalate compound (DEHP) isolatedfrom one of the popular herbal preparations (‘Sejeso’ herbalmixture) in South Africa, was found to be 43.3 mg/L (Nair et al.,2012). An important concern about DEHP relates to its potentialto act as a non-genotoxic hepatocarcinogen, a reproductive anddevelopmentally toxic substance and its neurodegenerativeeffects (Hauser et al., 2006; Koch et al., 2006; Willhite, 2001;Wittassek and Angerer, 2008). Due to its widespread use in avariety of consumer products and its associated health risks tohumans, the World Health Organisation (WHO) have im-plemented strict guidelines with regard to the tolerable dailyintake levels of DEHP (WHO, 2003). The recommended dose forpatients using ‘Sejeso’ herbal mixture would translate to eachindividual consuming on average 7.8 mg DEHP per day.Compared to the daily tolerable levels of 8 μg/L and 1.5 mg/kgfor drinking water and food consumed respectively, this figure(7.8 mg) is higher than the recommended values. These resultsindicate how exposed consumers of these herbal products are. Inmany cases, one patient might be using more than one CHP atany given time per day, resulting in the accumulation of thesetoxic contaminants to alarming levels. The risks could even be farmore, considering the fact that consumers rarely stick to therecommended doses on the container labels, but tend to takehigher doses, with the belief that the healing effects will be fasterand more effective.
62 A.R. Ndhlala et al. / South African Journal of Botany 82 (2012) 60–66
It could be hypothesised that these contaminants are not onlyconfined to one herbal mixture but could be a common char-acteristic of some plastic-packaged CHPs since most of them arepackaged in similar plastic containers. Phthalate contaminants inherbal products could either be emanating from the plasticcontainers in which they are packaged (to a larger extent) and/orduring the manufacturing process. The levels of these chemicalsubstances could have far reaching effects on the health of currentand future generations of the population relying on these herbalproducts. Against a background of widespread use, ubiquitousexposure and concerns about the ability of phthalates to causeadverse health effects in humans, quality assurance of botanicalsand herbal preparations should be a prerequisite if these healthconcerns are to be addressed. Very little research has been doneregarding the safety and quality of CHPs used in South Africaand hence the need for further studies in this regard, particularlyon phthalates. The literature to this aspect (phthalates in CHPsused in South Africa) is indeed scarce and hence this review is tobring this to the fore to stimulate further research work on CHPsand other food products.
3. DEHP biomarkers of exposure and effects
Through experimental and epidemiological studies, evidencehas accumulated for the association of other detrimental healtheffects associated with phthalate exposure. Phthalates are rapidlyhydrolyzed followed by oxidation and are mainly excreted viaurine (Wittassek andAngerer, 2008). Thus, the content of phthalatemetabolites in human urine acts as an indicator of recent internalexposure to the respective parent phthalate. Several studies haveassessed phthalate exposure of the general population by mea-suring phthalate metabolites in human urine samples.
3.1. Phthalates and the reproductive development in humaninfants
Exposure to environmental chemicals with antiandrogenicactivity, such as phthalates, is considered one of the causes forthe increased incidence of testicular dysgenesis syndrome(TDS). The foetus is considered to be the most sensitive stageof life to the potential developmental and reproductive toxicityof phthalates (Wittassek et al., 2009). Some phthalates havebeen found to be developmental and reproductive toxicants inrats, with pronounced effect on the male reproductive system(Borch et al., 2006; Foster, 2005; Gray et al., 2006). Recentresearch has focused on the effects of certain phthalate esters onreproduction, commonly on male reproductive development inexperimental animals. There are indications that phthalates maybe associated with abnormal sexual development and birth defectsin humans (McKee et al., 2004; Sharpe, 2008; Swan, 2008). Thepathways of androgen action are similar in both experimentalanimals and humans, suggesting that phthalates may causecomparable adverse effects on reproduction and development inhumans compared to experimental animals. Several epidemiolog-ical studies suggest that environmental exposure to a number ofphthalates may be associated with adverse reproductive outcomes,like alterations in semen parameters, DNA damage in sperm,
reduced reproductive hormone levels in adult men and decreasedanogenital distance in male infants (Duty et al., 2003; Swan,2008). The relationship between phthalate exposure and adverseeffects in human reproduction impacts negatively on theiroffspring.
3.2. Phthalates and respiratory function, asthma, and allergy
The term allergy describes adverse health effects that mightresult from the stimulation of a specific immune response(Kimber and Dearman, 2010). One important aspect of allergicsensitisation is that some chemicals may have qualitative, as wellas quantitative, effects on specific immune responses. Thepossibility that phthalates may present a risk factor for the de-velopment of allergies and asthma has been described in severalcase studies (Bornehag et al., 2004; Bornehag and Nanberg, 2009;Jaakkola et al., 2004; Kimber and Dearman, 2010). This has led tothe conclusion that some cleaning products used in domesticenvironments are associated with an increased risk of asthma(Bornehag et al., 2004; Rumchev et al., 2004). In addition,occupational exposure to high concentrations of phthalate fumeshas been linked to asthma and other respiratory symptoms(Andrasch et al., 1976; Markowitz, 1989; Nielsen et al., 1989). Avariety of respiratory symptoms such as cough, work-relatedshortness of breath, wheezing and rhinitis, as well as a decline inforced expiratory volume (FEV1) were found to be increased inexposed workers compared to control groups (Kimber andDearman, 2010).
Persuasive as these investigations are to an association betweenhousehold cleaning and clinical diseases such as respiratoryreactions, they do not necessarily implicate cleaning materials asbeing responsible for an increase in the incidence of allergicsensitisation. The implication is that certain phthalates may act asadjuvants and thereby predispose to, and/or otherwise enhance,acquisition of allergic sensitisation (Kimber and Dearman, 2010).It is appropriate, therefore, in advance of reviewing published dataon the association between phthalates and allergy, to consider thenature of phthalates and their function as adjuvants. In this regard,two independent studies were conducted in Sweden (Bornehag etal., 2004) and Bulgaria (Kolarik et al., 2008) in which theassociation between the phthalate content of house dust andallergic symptoms in children was investigated. Both studiesreported a significant association between the concentration ofDEHP in house dust and allergic symptoms (asthma or wheezing)in children. The implication that phthalates might play a role in thedevelopment of respiratory disorders, asthma and allergy cantherefore not be overlooked.
4. The fate of DEHP: Its metabolites and their effects
Humans can be exposed to phthalates through ingestion,inhalation and dermal contact when using phthalate-containingconsumer products (Silva et al., 2007). Human exposure tophthalates is facilitated by nutrition, medical devices and personalcare products. After absorption, phthalates are readily metabolisedto hydrolytic monoesters which can be further metabolised toother oxidative products before excretion in urine or faeces either

Table 1The effect of three DEHP metabolites used as markers of human exposure.
Compound Toxic effects References
MEHP • Anti-androgenic (disruption of testosterone action) Grasso et al. (1993), Fan et al. (2010) and Piché et al. (2012)• Inhibition of LH-stimulated steroid formation
MEOHP • May be toxic to the reproductive system Apostolidis et al. (2002), OSPAR (2002) and Bornehag et al. (2004)• Confirmed animal carcinogen with unknown relevanceto humans• Priority water pollutant• Probable endocrine disruptor• Prohibited in EU cosmetics• Gastrointestinal or liver toxicity hazards
MEHHP • Immune system toxicity Apostolidis et al. (2002), OSPAR (2002), and Bornehag et al. (2004)• Respiratory system toxicity• Respiratory toxicity hazards• Persistent, bioaccumulative toxicant• Prohibited in EU cosmetics
63A.R. Ndhlala et al. / South African Journal of Botany 82 (2012) 60–66
as free or conjugated species with elimination half-lives of lessthan 24 h (Herr et al., 2009). In the liver, phthalates are oxidisedby xenobiotic metabolising enzymes such as cytochrome P450(Dirven et al., 1993). There are however, differences in theexcretion pattern of urinary DEHP metabolites between species.Rats, for example, excrete more of the oxidised urinarymetabolitesthan humans and monkeys which excrete (glucuronide) conjugat-ed metabolites (Albro, 1986). The toxic effects of phthalate me-tabolites are outlined in Table 1.
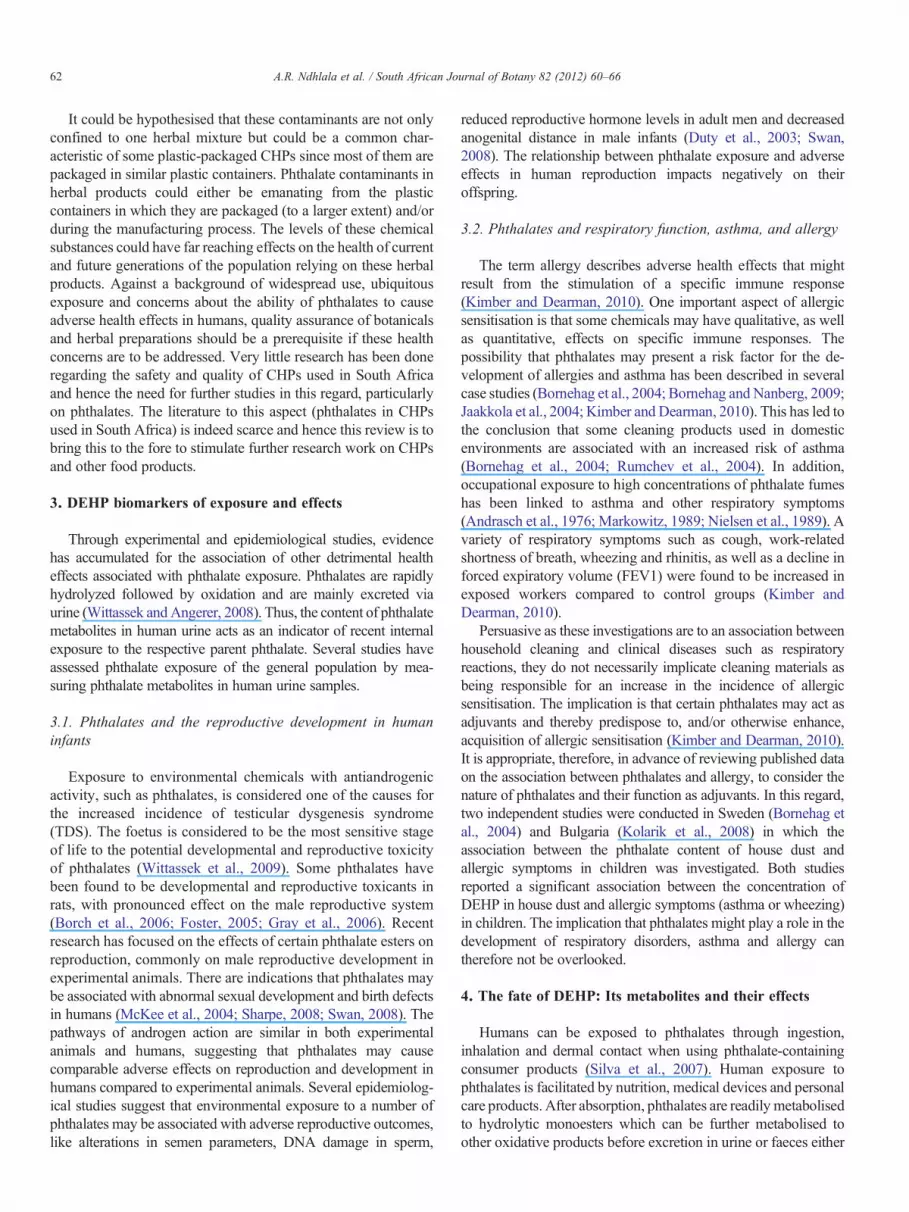
The main known DEHP metabolites excreted by humansare mono (2-ethylhexyl) phthalate (MEHP), mono (5-carboxy-2-ethylpentyl) phthalate, mono (2-ethyl-5-oxohexyl) phthalate(MEOHP), and mono (2-ethyl-5-hydroxyhexyl) phthalate(MEHHP) (Dirven et al., 1993) represented in Fig. 1 andTable 1. The other equally important phthalate metabolitesinclude phthalic acid (PA), monomethyl phthalate (MMP),monoethyl phthalate (MEP), mono-3-carboxypropyl phthalate(MCPP), mono-n-butyl phthalate (MBP), mono-isobutyl phthalate(MiBP), monocyclohexyl phthalate (MCHP), monobenzyl phthal-ate (MBzP), mono-n-octyl phthalate (MOP), mono-isononylphthalate (MNP), mono-isodecyl phthalate (MDP), mono-n-hexylphthalate (MHxP), mono-n-heptyl phthalate (MHpP), mono-2-ethyl-5-carboxypentyl phthalate (MECPP), mono-carboxy-n-heptyl phthalate (MCHpP), monocarboxy-isooctyl phthalate(MCOP), mono-hydroxyisononyl phthalate (MHNP), mono-oxoisononyl phthalate (MONP), and mono-carboxyisononylphthalate (MCNP) (Silva et al., 2007). These metabolites areexcreted in urine predominantly as glucuronide conjugates (Katoet al., 2004). The differences in the rate of metabolism amongphthalates could result in urinary excretion of higher levels of themonoester metabolites (MEHP, MEOHP and MEHHP) of thephthalates with short alkyl chains than for DEHP, making thesemetabolites suitable biomarkers for DEHP exposure (Kato et al.,2004). The metabolism of DEHP involves the hydrolysis of oneester bond, giving rise to MEHP, followed by oxidation toMEOHP and MEHHP.
5. Tolerable daily intake and minimal risk level
Based on the experimental data derived from animal studies,the Scientific Committee on Toxicity, Ecotoxicity and theEnvironment obtained tolerable daily intakes (TDI) andminimal risk level (MRL) values for phthalates (Yen et al.,2011). The WHO has set the TDI for DEHP at 8 μg/L fordrinking water and 1.5 mg/kg for food (WHO, 1996, 2003). Itis therefore important to carry out quality checks on the levelsof DEHP and its metabolites in commonly consumed productslike CHPs. As mentioned before, Nair et al. (2012) calculatedexposure levels of 7.8 mg DEHP per day in a commercialherbal mixture (Sejeso herbal mixture, Ingwe brand). Theauthors warned that the levels were alarming and reflected alack of effective quality control in the traditional medicinesector in South Africa.
6. Analytical methods for determining DEHP
Several analytical methods have been reported for thedetermination of DEHP in foods, biological fluids, and tissuesamples. These include high performance liquid chromatogra-phy (HPLC), gas chromatography (GC), mass spectroscopy(MS) and nuclear magnetic resonance techniques (NMR)(Aignasse et al., 1995; Dirven et al., 1993; Faouzi et al.,1999; Herr et al., 2009; Nair et al., 2012). These methods oftendiffer in extraction and sample preparation proceduresinvolved. Nevertheless, all the techniques are tedious andtime consuming (Aignasse et al., 1995). The idea is however, touse a sensitive and specific analytical method to determineDEHP and its metabolites in any matrix. HPLC has been themost useful and sensitive method to determine concentrationsof DEHP and its metabolites in food and liquid matrices(Kambia et al., 2001). However, as revealed by Torto et al.(2007), Africa as a continent has its unique challenges foranalytical chemists in sample preparation for chromatographic
bis (2-ethylhexyl) phthalates (DEHP)
mono (2-ethylhexyl) phthalate (MEHP)
mono (2-ethyl-5-hydroxyhexyl) phthalate (MEHHP)
mono (2-ethyl-5-oxohexyl) phthalate (MEOHP)
O
O
O
CH3
CH3
O
CH3
CH3
OH
O
O
CH3
CH3
O
OH
O
O
CH3
CH3
O
OH
OH
O
O
CH3
CH3
O
O
Fig. 1. DEHP and its metabolites as biomarkers in human exposure.
64 A.R. Ndhlala et al. / South African Journal of Botany 82 (2012) 60–66
analyses. This has led to the development of a protocol for thedetermination of phthalate esters and polycyclic aromatic hy-drocarbons in both aquatic samples and sediments (Torto et al.,2007).
In the investigation of simple methods for extraction ofphthalates, two approaches were employed either using liquid–liquid extraction or solid-phase extraction. For liquid–liquidextraction, extraction efficiencies for chloroform, dichloromethane(DCM) and ethyl acetate were investigated for the determination ofphthalates in recovery experiments (Torto et al., 2007). The authorsconcluded that DCM was the best extracting solvent forphthalates as the other solvents formed emulsions, which weredifficult to separate from the aqueous medium and consequentlygave low recovery. Dichloromethane was cited as suitablebecause of its low cost, availability in highly purified form,inertness and easy separation from water because of its higherdensity. Alumina was cited as the better suitable sorbent material
for clean-up as compared to silica gel adsorbents (Fatoki andOgunfowokan, 1993).
Given the recent surge and popularity of plastic packagedcommercial herbal remedies, the South African governmentshould provide adequate support for analytical studies andcontrol of levels of DEHP in formulated products. WHO hasalready published several technical guidelines for appropriateapproaches to assessing chemical toxins in herbal medicines(WHO, 1996, 2003). Despite the fact that a lot of research hasbeen conducted on the effects of DEHP, its replacement withsafer chemicals still remains a challenge. Providing adequateresearch facilities and experienced personnel, as well as settingup common accepted analytical standards through bilateralrecognition and through international and regional regulatorycooperation for herbal medicines should be considered.
7. Conclusions
In conclusion, DEHP is a liquid widely used to make plasticsmore flexible. A potential exists for DEHP contamination of foodand CHPs during processing, handling, transportation and pack-aging. Most cases of exposure occur from the leaching of DEHPfrom plasticised products during their use. The level of exposuresis affected by the thickness of the plastic item, the tempera-ture, storage conditions and the specific nature of the product.Mandatory quality control mechanisms should therefore beimplemented for the manufacturing and packaging of productsin plastic containers intended for human consumption.
Acknowledgements
This work was supported by the Claude Leon Foundation,the University of KwaZulu-Natal (UKZN) College of Scienceand Agriculture and the UKZN Research Office.
References
Aignasse, M.F., Prognon, P., Stachowicz, M., Gheyouche, R., Pradeau, D., 1995.A new simple and rapid HPLC method for determination of DEHP in PVCpackaging and releasing studies. International Journal of Pharmaceutics 113,241–246.
Albro, P.W., 1986. The biochemical toxicology of di-(2-ethylhexyl) and relatedphthalates: testicular atrophy and hepatocarcinogenesis. Review of Biochemistryand Toxicology 8, 73–119.
Andrasch, R.H., Bardana Jr., E.J., Koster, F., Pirofsky, B., 1976. Clinical andbronchial provocation studies in patients with meatwrappers' asthma. TheJournal of Allergy and Clinical Immunology 58, 291–298.
Apostolidis, S., Chandra, T., Demirhan, I., Cinatl, J., Doerr, H.W., Chandra, A.,2002. Evaluation of carcinogenic potential of two nitro-musk derivatives,musk xylene and musk tibetene in a host-mediated in vivo/in vitro assaysystem. Anticancer Research 22, 2657–2662.
Borch, J., Axelstad, M., Vinggaard, A.M., Dalgaard, M., 2006. Diisobutylphthalate has comparable anti-androgenic effects to di-n-butyl phthalate infoetal rat testis. Toxicology Letters 163, 183–190.
Bornehag, C.G., Nanberg, E., 2009. Phthalate exposure and asthma in children.International Journal of Andrology 33, 1–13.
Bornehag, C.G., Sundell, J., Weschler, C.J., Sigsgaard, T., Lundgren, B.,Hasselgren,M., Hägerhed-Engman, L., 2004. The association between asthmaand allergic symptoms in children and phthalates in house dust: a nested case–control study. Environmental Health Perspectives 112, 1393–1397.

65A.R. Ndhlala et al. / South African Journal of Botany 82 (2012) 60–66
Chen, C.Y., Ghule, A.V., Chen, W.Y., Wang, C.C., Chiang, Y.S., Ling, Y.C.,2004. Rapid identification of phthalates in blood bags and food packagingusing ToF-SIMS. Applied Surface Science 231–232, 447–451.
Clewell, R.A., Kremer, J.J., Williams, C.C., Campbell Jr., J.L., Andersen, M.E.,Borghoff, S.J., 2008. Tissue exposures to free and glucuronidatedmonobutylyphthalate in the pregnant and fetal rat following exposure todi-n-butylphthalate: evaluation with a PBPK model. Toxicological Sciences103, 241–259.
Dirven, H.A.A.M., Van den Broek, P.H.H., Jongeneelen, F.J., 1993. Determina-tion of four metabolites of the plasticizer di(2-ethylhexyl)phthalate in humanurine samples. International Archives of Occupational and EnvironmentalHealth 64, 555–560.
Duty, S.M., Singh, N.P., Silva, M.J., Barr, D.B., Brock, J.W., Ryan, L., Herrick,R.F., Christiani, D.C., Hauser, R., 2003. The relationship between environ-mental exposure to phthalates and DNA damage in human sperm using theneutral comet assay. Environmental Health Perspectives 111, 1164–1169.
Fan, J., Traore, K., Li, W., Amri, H., Huang, H., Wu, C., Chen, H., Zirkin, B.,Papadopoulos, V., 2010. Molecular mechanisms mediating the effect ofmono-(2-ethylhexyl) phthalate on hormone-stimulated steroidogenesis inMA-10 mouse tumor leydig cells. Endocrinology 151, 3348–3362.
Faouzi, M.A., Khalfi, F., Dine, T., Luyck, M., Brunet, C., Gressier, B., Goudaliez,F., Cazin, M., Kablan, J., Belabed, A., Cazin, J.C., 1999. Stability, compatibilityand plasticizer extraction of quinine injection added to infusion solutions andstored in polyvinyl chloride (PVC) containers. Journal of Pharmaceutical andBiomedical Analysis 21, 923–930.
Fatoki, O.S., Ogunfowokan, A.O., 1993. Procedure cleanup technique fordetermination of phthalate esters in an aquatic environment. InternationalJournal of Environmental Studies 44, 237–243.
Foster, P.M., 2005. Mode of action: impaired foetal leydig cell function —effects on male reproductive development produced by certain phthalateesters. Critical Reviews in Toxicology 35, 713–719.
Grasso, P., Heindel, J.J., Powell, C.J., Reichert Jr., L.E., 1993. Effects of mono(2-ethylhexyl) phthalate, a testicular toxicant, on follicle-stimulatinghormone binding to membranes from cultured rat Sertoli cells. Biology ofReproduction 48, 454–459.
Gray Jr., L.E., Wilson, V.S., Stoker, T., Lambright, C., Furr, J., Noriega, N.,Howdeshell, K., Ankley, G.T., Guillette, L., 2006. Adverse effects ofenvironmental antiandrogens and androgens on reproductive development inmammals. International Journal of Andrology 29, 96–104.
Hauser, R., Meeker, J.D., Duty, S., Silva, M.J., Calafat, A.M., 2006. Alteredsemen quality in relation to urinary concentrations of phthalate monoesterand oxidative metabolites. Epidemiology 17, 682–691.
Herr, C., Nieden, A., Koch, H.M., Schuppe, H.-C., Fieber, C., Angerer, J.,Eikmann, T., Stilianakis, N.I., 2009. Urinary di(2-ethylhexyl)phthalate(DEHP) metabolites and male human markers of reproductive function.International Journal of Hygiene and Environmental Health 212, 648–653.
Jaakkola, J.J., Parise, H., Kislitsin, V., Lebedeva, N.I., Spengler, J.D., 2004.Asthma, wheezing, and allergies in Russian schoolchildren in relation tonew surface materials in the home. American Journal of Public Health 94,560–562.
Kambia, K., Dine, T., Gressier, B., Germe, A.-F., Luyckx, M., Bruneta, C.,Michaud, L., Gottrand, F., 2001. High-performance liquid chromatographicmethod for the determination of di(2-ethylhexyl) phthalate in totalparenteral nutrition and in plasma. Journal of Chromatography B 755,297–303.
Kato, K., Silva, M.J., Reidy, J.A., Hurtz, D., Malek, N.A., Needham, L.L.,Nakazawa, H., Barr, D.B., Calafat, A.M., 2004. Mono(2-ethyl-5-hydroxyhexyl)phthalate and mono-(2-ethyl-5-oxohexyl) phthalate as biomarkers for humanexposure assessment to di-(2-ethylhexyl) phthalate. Environmental HealthPerspectives 112, 327–330.
Kimber, I., Dearman, R.J., 2010. An assessment of the ability of phthalates toinfluence immune and allergic responses. Toxicology 271, 73–82.
Koch, H.M., Preuss, R., Angerer, J., 2006. Di(2-ethylhexyl) phthalate (DEHP):human metabolism and internal exposure-an update and latest results.International Journal of Andrology 29, 155–165.
Kolarik, B., Naydenov, K., Larrson, M., Borenhag, C.G., Sundell, J., 2008. Theassociation between phthalates in dust and allergic diseases amongBulgarian children. Environmental Health Perspectives 116, 98–103.
Mahood, I.K., Scott, H.M., Brown, R., Hallmark, N., Walker, M., Sharpe, R.M.,2007. In utero exposure to di(n-butyl) phthalate and testicular dysgenesis:comparison of fetal and adult end points and their dose sensitivity.Environmental Health Perspectives 115 (Suppl. 1), 55–61.
Mander, M., 1998. The Marketing of Indigenous Medicinal Plants in SouthernAfrica: A Case Study in KwaZulu-Natal. FAO, Rome.
Markowitz, J.S., 1989. Self-reported short- and long-term respiratory effects amongPVC-exposed firefighters. Archives of Environmental Health 44, 30–33.
McKee, R.H., Butala, J.H., David, R.M., Gans, G., 2004. NTP center for theevaluation of risks to human reproduction reports on phthalates: addressingthe data gaps. Reproduction Toxicology 18, 1–22.
Nair, J.J., Ndhlala, A.R., Chukwujekwu, J.C., Van Staden, J., 2012. Isolation ofdi(2-ethylhexyl) phthalate from a commercial South African cognate herbalmixture. South African Journal of Botany 80, 21–24.
Ncube, B., Finnie, J.F., Van Staden, J., 2012. In vitro antimicrobial synergismwithin plant extract combinations from three South African medicinal bulbs.South African Journal of Botany 139, 81–89.
Ndhlala, A.R., Stafford, G.I., Finnie, J.F., Van Staden, J., 2009. In vitropharmacological effects of manufactured herbal concoctions used inKwaZulu-Natal South Africa. Journal of Ethnopharmacology 122, 117–122.
Ndhlala, A.R., Anthonissen, R., Stafford, G.I., Finnie, J.F., Verschaeve, L., VanStaden, J., 2010a. In vitro cytotoxic and mutagenic evaluation of thirteencommercial herbal mixtures sold in KwaZulu-Natal, South Africa. SouthAfrican Journal of Botany 76, 132–138.
Ndhlala, A.R., Finnie, J.F., Van Staden, J., 2010b. In vitro antioxidantproperties, HIV-1 reverse transcriptase and acetylcholinesterase inhibitoryeffects of traditional herbal preparations sold in South Africa. Molecules 15,6888–6904.
Ndhlala, A.R., Finnie, J.F., Van Staden, J., 2011a. Plant composition, pharmaco-logical properties and mutagenic evaluation of a commercial Zulu herbalmixture: Imbiza ephuzwato. Journal of Ethnopharmacology 133, 663–674.
Ndhlala, A.R., Stafford, G.I., Finnie, J.F., Van Staden, J., 2011b. Unregisteredcommercial herbal preparations in KwaZulu-Natal: the urban face oftraditional medicine. South African Journal of Botany 77, 830–843.
Nielsen, J., Fahraeus, C., Bensryd, I., Akesson, B., Welinder, H., Linden, K.,Skerfving, S., 1989. Small airways function in workers processingpolyvinylchloride. International Archives of Occupational and Environ-mental Health 61, 427–430.
OSPAR, 2002. OSPAR List of Substances of Possible Concern. OSPARConvention for the Protection of theMarine Environment of North-east Atlantic.
Piché, C.D., Sauvageau, D., Vanlian, M., Erythropel, H.C., Robaire, B., Leask,R.L., 2012. Effects of di-(2-ethylhexyl) phthalate and four of its metaboliteson steroidogenesis in MA-10 cells. Ecotoxicology and EnvironmentalSafety 79, 108–115.
Rumchev, K., Spickett, J., Bulsara,M., Phillips,M., Stick, S., 2004. Association ofdomestic exposure to volatile organic compounds with asthma in youngchildren. Thorax 59, 746–751.
Sharpe, R.M., 2008. Additional effects of phthalate mixtures on fetaltestosterone production. Toxicological Science 105, 1–4.
Silva, M.J., Samandar, E., Preau Jr., J.L., Reidy, J.A., Needham, L.L., Calafat,A.M., 2007. Quantification of 22 phthalate metabolites in human urine.Journal of Chromatography B 860, 106–112.
Swan, S.H., 2008. Environmental phthalate exposure in relation to reproductiveoutcomes and other health endpoints in humans. Environmental Research108, 177–184.
Torto, N., Mmualefea, L.C., Mwatseteza, J.F., Nkoane, B., Chimuka, L., Nindi,M.M., Ogunfowokan, A.O., 2007. Sample preparation for chromatography:an African perspective. Journal of Chromatography. A 1153, 1–13.
WHO, 1996. Guidelines for Drinking Water Quality. WHO Press, Geneva,Switzerland.
WHO, 2003. Diethyl Phthalate. Concise International Chemical AssessmentDocument 52. WHO Press, Geneva, Switzerland.
Willhite, C.C., 2001. Weight-of-evidence versus strength-of-evidence in toxico-logic hazard identification: di(2-ethylhexyl)phthalate (DEHP). Toxicology160, 219–226.
Williams, V.L., Balkwill, K., Witkowski, E.T.F., 2000. Unraveling thecommercial market for medicinal plants and plant parts on the Witwaters-rand, South Africa. Economic Botany 54, 310–327.

66 A.R. Ndhlala et al. / South African Journal of Botany 82 (2012) 60–66
Wittassek, M., Angerer, J., 2008. Phthalates: metabolism and exposure.International Journal of Andrology 31, 131–138.
Wittassek, M., Angerer, J., Kolossa-Gehring, M., Schäfer, S.D., Klockenbusch,W., Dobler, L., Günsel, A.K., Müller, A., Wiesmüller, G.A., 2009. Fetalexposure to phthalates-a pilot study. International Journal of Hygiene andEnvironmental Health 212, 492–498.
Wormuth, M., Scheringer, M., Vollenweider, M., Hungerbuhler, K., 2006.What are the sources of exposure to eight frequently used phthalic acidesters in Europeans? Risk Analysis 26, 803–824.
Yen, T.-H., Lin-Tan, D.-T., Lin, J.-L., 2011. Food safety involving ingestion offoods and beverages prepared with phthalate-plasticizer containing cloudingagents. Journal of the Formosan Medical Association 110, 671–684.
Edited by AM Viljoen




























