Embed Size (px)
Citation preview

DOI: 10.1016/j.athoracsur.2006.03.067 2006;82:637-644 Ann Thorac Surg
Drazner, Clyde W. Yancy, Jr, W. Steves Ring and J. Michael DiMaio C. Paul, Patricia A. Kaiser, Paul A. Pappas, Dan M. Meyer, Michael A. Wait, Mark H.
David H. Rosenbaum, Brian C. Adams, Joshua D. Mitchell, Michael E. Jessen, Michelle Effects of Early Steroid Withdrawal After Heart Transplantation
http://ats.ctsnetjournals.org/cgi/content/full/82/2/637located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2006 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on May 30, 2013 ats.ctsnetjournals.orgDownloaded from

ETDMPCDTD
nowdpt
cwwpgtTei
AtaslohtenotsAscr
A
PS
AT
©P
CA
RD
IOV
ASC
ULA
R
ffects of Early Steroid Withdrawal After Heartransplantation
avid H. Rosenbaum, MD, Brian C. Adams, BS, Joshua D. Mitchell, BS,ichael E. Jessen, MD, Michelle C. Paul, BS, Patricia A. Kaiser, RN,
aul A. Pappas, MS, Dan M. Meyer, MD, Michael A. Wait, MD, Mark H. Drazner, MD,lyde W. Yancy, Jr, MD, W. Steves Ring, MD, and J. Michael DiMaio, MD
epartment of Cardiovascular and Thoracic Surgery, and Division of Cardiology, Department of Internal Medicine, University ofexas Southwestern Medical Center, Dallas, Texas, and Duke Clinical Research Institute, Duke University Medical Center,
urham, North Carolinassaatdte0t
padit
Background. Managing immunosuppression is a sig-ificant aspect of posttransplantation patient care. Previ-usly, our institution reported that prednisone could beithdrawn in cardiac allograft recipients without jeopar-izing midterm survival. We returned to this group ofatients to investigate the long-term effects of our steroid
aper protocol.Methods. We reviewed the records of 162 consecutive
ardiac transplant recipients from our institution. Patientsho underwent transplantation between 1988 and 1990ere treated with traditional triple-therapy immunosup-ression (cyclosporine, azathioprine, and prednisone). Be-inning June 1990, we instituted a protocol of early steroidaper with discontinuation by 6 months after transplant.he two groups were comparable with respect to age, sex,thnicity, cause of heart failure, ischemic time, body massndex, and creatinine at the time of transplantation.
Results. Fifty-seven percent of the patients in the early
couedtwh
P
TSfrarw
ddress correspondence to Dr DiMaio, 5323 Harry Hines Blvd, Dallas,X 75390-8879; e-mail: [email protected].
2006 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
teroid taper group were successfully withdrawn fromteroids at 6 months after transplantation. This group had
decreased freedom from and increased frequency ofcute rejection (p < 0.01 for each) when compared withhe traditional therapy group. There was, however, noifference in freedom from posttransplant coronary ar-
ery disease (p � 0.53). The early steroid taper groupnjoyed an increased freedom from malignancy (p �.01) and trended toward a decreased frequency of infec-ion (p � 0.10) and improved survival (p � 0.06).
Conclusions. Steroid withdrawal is possible in 57% ofatients at 6 months after transplantation. The institution ofn early steroid taper protocol improves the overall free-om from malignancies and may decrease the frequency of
nfection and prolong overall survival without increasinghe risk of posttransplant coronary artery disease.
(Ann Thorac Surg 2006;82:637–44)
© 2006 by The Society of Thoracic Surgeonsdvances in immunosuppressive therapy are a signifi-cant factor behind the success of heart transplanta-
ion. Successful immunosuppression, however, must bal-nce the prevention of rejection with the well-documentedide effects of immunosuppressive drugs, including those ofong-term steroid therapy. To decrease the negative effectsf prolonged steroid treatment, many transplant programsave investigated steroid-free or withdrawal protocols. In
he mid 1980s, Yacoub and colleagues [1] demonstratedncouraging results with a steroid-free regimen. This pio-eering work was quickly followed with several variationsf this theme by other investigators. These included at-empts at complete avoidance of steroids and early or lateteroid taper after initial treatment with prednisone [2–17].lthough these protocols demonstrated the feasibility of
teroid withdrawal with varying effects on rejection, steroidomplications, and survival, 75% of today’s heart transplantecipients are still treated with chronic steroid therapy [18].
ccepted for publication March 22, 2006.
resented at the Fifty-second Annual Meeting of the Southern Thoracicurgical Association, Orlando, FL, Nov 10–12, 2005.
Previously our institution reported that prednisoneould be withdrawn in heart transplant recipients with-ut jeopardizing survival and graft function. [11] Follow-p, however, was insufficient to assess the full impact ofarly withdrawal on long-term graft function, the inci-ence of coronary artery disease, and other complica-
ions. This report provides a reanalysis of this steroidithdrawal protocol to explore its long-term effects ineart transplant recipients.
atients and Methods
he Institutional Review Board at the University of Texasouthwestern Medical Center waived the requirement
or obtaining patient consent for participation in thisetrospective study. After Institutional Review Boardpproval was granted, we retrospectively reviewed theecords of 162 consecutive cardiac transplantations thatere performed at our institution between the years 1988
Dr Ring discloses a financial relationship with
Novartis.0003-4975/06/$32.00doi:10.1016/j.athoracsur.2006.03.067
by on May 30, 2013 als.org

apTpaipith6arbecoiwt1tpt
geiampsoqtmCrraoa
bw
aTlft
oilpgSwufaisaAIsd
R
OsCtyt
wTm(4tws
RF
T
C rine,
638 ROSENBAUM ET AL Ann Thorac SurgSTEROID TAPER AFTER HEART TRANSPLANTATION 2006;82:637–44
CA
RD
IOV
ASC
ULA
R
nd 1996. During this time, 9 patients suffered posttrans-lant in-hospital mortality and 3 were lost to follow-up.hese 12 patients were excluded from the study. Theatients who underwent transplantation between 1988nd 1990 were treated with traditional triple-therapymmunosuppression (cyclosporine, azathioprine, andrednisone [CAP; n � 46]). Beginning June 1990, we
nstituted a protocol of early steroid taper with discon-inuation of steroids at 6 months after transplant. Oneundred four patients were transplanted during this-year period. Seven patients who either lived too farway from the transplant center or for various financialeasons were unable to partake in the more extensiveiopsy protocol necessary for early steroid taper werexcluded from the study. Another 4 patients were ex-luded from this study for the following reasons: sarcoid-sis (requiring steroid treatment), single kidney (lower-
ng cyclosporine levels if renal function deterioratedould lead to underimmunosuppression), retransplanta-
ion, and age younger than 18 years. Therefore, 93 of the04 patients who underwent cardiac transplantation be-ween the years 1990 and 1996 were treated with arotocol of cyclosporine, azathioprine, and prednisone
aper (CAPT group).The immunosuppressive protocol used by our pro-
ram during this study period is outlined in detaillsewhere [11]. Briefly; both groups received cyclospor-ne and azathioprine during the entire study periodccording to an identical protocol. All patients receivedethylprednisolone on initiation of cardiopulmonary by-
ass and during the first postoperative day. On theecond postoperative day, both groups were started onral prednisone at a dose of 1 mg/kg per day. Subse-uently, the steroid dose was tapered at different rates in
he two groups and was completely withdrawn at 6onths after transplant in the CAPT group (Table 1). TheAPT patients were returned to the standard triple-drug
egimen if they experienced two episodes of acute graftejection, any hemodynamically compromised rejection,cute vascular rejection, leukopenia, renal insufficiency,r any other indication for steroid treatment. Data werenalyzed according to intention-to-treat.Table 1 describes our surveillance endomyocardial
iopsy protocol. The diagnosis of acute graft rejection
able 1. Steroid Taper and Biopsy Protocols
Condition CAP
Prednisone taper ● 1 mg/kg per day � 2● 0.25 mg/kg per day �
● 0.15 mg/kg per day �
● 0.1 mg/kg per day theBiopsy protocol ● every 2 wk � 3 mont
● every 1 month � 3 m● every 3 months � 1.5● annually thereafter
AP � cyclosporine, azathioprine, and prednisone; CAPT � cyclospo
as made according to Billingham’s criteria before 1990 d
ats.ctsnetjournDownloaded from
nd the classification of the International Society of Heartransplantation after 1990. A coronary angiogram and
eft ventriculogram were obtained within 6 to 12 weeksrom transplantation and used as a baseline with whicho compare yearly follow-up studies.
Follow-up was concluded on December 31, 2004. Seri-us infection was defined as any case that necessitated
ntravenous therapy or hospital admission. A solid ma-ignancy was defined as any malignancy in which therimary lesion was not in the skin, including oropharyn-eal cancers. Continuous variables were compared withtudent’s t tests, and categorical variables were analyzedith the �2 statistic. Two-by-two tables were analyzedsing Fisher’s exact test. Patient survival and freedom
rom events were analyzed with Kaplan–Meier curvesnd compared with the log-rank statistic. The impact ofmmunosuppressive therapy on body mass index anderum creatinine values between the two groups wasnalyzed using a repeated-measure analysis of variance.ll statistics were computed using SAS Version 9.1 (SAS
nstitute, Cary, NC), and p less than 0.05 determinedignificance. Data are expressed as mean � standardeviation.
esults
ne hundred thirty-nine patients were included in thistudy. The CAP group included 46 patients, and theAPT group included 93 patients. The mean follow-up
ime was 10.8 � 4.5 years in the CAP group and 10.0 � 3.7ears in the CAPT group. Demographic information forhe two groups is provided in Table 2.
Of the 93 patients eligible for steroid taper, 53 (57%)ere successfully withdrawn from steroids at 6 months.hirty-five patients continued to require steroids forultiple episodes of rejection (n � 19), renal insufficiency
n � 7), acute vascular rejection (n � 4), leukopenia (n �), and reactive airway disease (n � 1). Table 3 compareshe characteristics of the patients in the CAPT group whoere successfully weaned with those who failed the
teroid taper.
ejection and Posttransplant Graft Vasculopathyive cases of acute rejection occurred in the CAP group
CAPT
ths ● 1 mg/kg per day � 1 monthonths ● 0.25 mg/kg per day � 1 monthonths ● 0.15 mg/kg per day � 4 monthster ● off prednisone thereafter
● every 2 wk � 8 monthss ● every 1 month � 4 monthss ● every 3 months � 1 year
● annually thereafter
azathioprine, and prednisone taper.
mon4 m6 mreaf
hsonthyear
uring the first 6 months after transplant, whereas 41
by on May 30, 2013 als.org

cgc3lrcfice
MTfcodnrtiHssr
IOsfgc2
MCfssdtasa�
SFp4p
T
V
PAS
E
E
ICB
a
B nison
639Ann Thorac Surg ROSENBAUM ET AL2006;82:637–44 STEROID TAPER AFTER HEART TRANSPLANTATION
CA
RD
IOV
ASC
ULA
R
ases occurred during the same period in the CAPTroup. During the remainder of the follow-up period, 11ases of acute rejection occurred in the CAP group, and2 occurred in the CAPT group. During the entire fol-ow-up period, there were 0.35 � 0.77 cases of acuteejection per patient in the CAP group versus 0.78 � 0.87ases per patient in the taper group (p � 0.01). Freedomrom acute rejection was greater in the CAP group thann the CAPT group (Fig 1). Interestingly, freedom fromoronary artery disease was not significantly altered byarly withdrawal of steroids (Fig 2).
alignancyhe CAPT patients had an increased overall freedom
rom malignancy (Fig 3). When examining different can-er types, there was no difference in freedom from solidrgan malignancy or posttransplant lymphoproliferativeisorder. The 10-year freedom from solid organ malig-ancy was 75.1 and 83.1 in the CAP and CAPT groupsespectively (p � 0.26). The 10-year freedom from post-ransplant lymphoproliferative disorder was 94.7 and 98.7n the CAP and CAPT groups, respectively (p � 0.27).
owever, there was significantly increased freedom fromkin cancer in the taper group (10-year freedom fromkin cancer of 36.3 and 53.9 in the CAP and CAPT groups,
able 2. Demographics of Heart Transplant Patients
ariableEntireStudy
atients 139ge (years) 53.1 � 9.9exMale 112Female 27
thnicityWhite 123Black 14Hispanic 1American Indian 1
tiologyIschemic 81Idiopathic 46Other 12
Acquired valvular 3Congenital 2Alcoholic 3Hypertrophic 1Postpartum 1Other 2
schemic time (min) 165.7 � 48.6reatinine at transplantation (mg/dL) 1.3 � 0.4MI at transplantation 23.9 � 4.1
p value represents Caucasian versus non-Caucasian ethnicity because o
MI � body mass index; CAP � cyclosporine, azathioprine, and pred
espectively; p � 0.03). t
ats.ctsnetjournDownloaded from
nfectionverall, there were 91 versus 124 serious infective epi-
odes in the CAP and CAPT groups, respectively. Overallreedom from infection did not differ between the tworoups (Fig 4); however, there was a trend toward in-reased episodes of infection in the CAP group (1.96 �.72 per patient versus 1.24 � 2.19 per patient; p � 0.10).
orbidityommon posttransplant morbidities such as renal dys-
unction, obesity, and diabetes were not altered by earlyteroid withdrawal. The freedom from diabetes, as mea-ured by the need for insulin or oral medication, did notiffer between the two groups (p � 0.38). Renal dysfunc-
ion, as measured by serum creatinine level, and obesity,s measured by the patient’s body mass index, were notignificantly different at the time of transplantation andt 1, 5, and 10 years after transplantation (p � 0.28 and p
0.22, respectively).
urvivalive patients died during the first 6 months after trans-lantation in the CAPT group. One died of infection, andpatients died of sudden cardiac death. Of those 4, 1
atient had been leukopenic from cytomegalovirus infec-
CAP CAPT p Value
46 9353.5 � 8.9 52.9 � 10.5 0.74
0.1141 715 22
0.58a
42 814 100 10 1
0.6829 5214 323 90 31 10 30 10 12 0
176.9 � 51.6 160.2 � 46.3 0.061.3 � 0.3 1.3 � 0.4 0.77
23.3 � 3.1 24.2 � 4.5 0.20
number of Hispanic and American Indian patients.
e; CAPT � cyclosporine, azathioprine, and prednisone taper.
f low
ion, and azathioprine had been held for almost a month.
by on May 30, 2013 als.org

Awphrtda
anvfsTgc
T
V
PAS
E
E
IC
a
n
C
Ft(
Ft
640 ROSENBAUM ET AL Ann Thorac SurgSTEROID TAPER AFTER HEART TRANSPLANTATION 2006;82:637–44
CA
RD
IOV
ASC
ULA
R
second patient, who was known to be noncompliantith medications, was found deceased at home. A thirdatient suffered a cardiac arrest while in the hospital afteris cyclosporine dosing had been decreased secondary toenal insufficiency. The fourth patient was also beingreated with decreased dosing of cyclosporine when heied. All 4 patients’ causes of death were classified ascute rejection; however, in each case the patient was on
able 3. Demographics of Steroid-Taper Group
ariable CAPT
atients 93a
ge (years) 52.9 � 10.5exMale 71Female 22
thnicityWhite 81Black 10Other 2
Hispanic 1American Indian 1
tiologyIdiopathic 52Ischemic 32Other 9
Acquired valvular 3Congenital 1Alcoholic 3Hypertrophic 1Postpartum 1
schemic time (min) 160.2 � 46.3reatinine at transplantation (mg/dL) 1.3 � 0.4
Five patients died before being tapered off steroids. b p value represumber of American Indian and Hispanic patients.
APT � cyclosporine, azathioprine, and prednisone taper.
ig 1. Freedom from acute rejection in traditional triple-therapy pa-ients (CAP; solid line) and early steroid withdrawal patients
CAPT; dashed line). wats.ctsnetjournDownloaded from
nonstandard immunosuppression protocol owing tooncompliance or decreased dosing for the various pre-iously stated reasons. Overall, the CAPT patients wereound to have a very strong trend toward improvedurvival when compared with the CAP patients (Fig 5).here was no significant difference between the tworoups in frequency of death because of acute rejection,hronic rejection, or malignancy (Table 4). The CAP
Tapered Failed Taper p Value
53 3553.5 � 11.7 52.2 � 8.7 0.57
0.0844 239 12
0.03b
50 282 71 00 01 0
0.3819 1231 18
3 51 20 12 10 00 1
155.0 � 40.5 170.7 � 52.4 0.121.3 � 0.4 1.3 � 0.5 0.63
frican American versus non–African American ethnicity because of low
ig 2. Freedom from posttransplant coronary artery disease in tradi-ional triple-therapy patients (CAP; solid line) and early steroid
ents A
ithdrawal patients (CAPT; dashed line).
by on May 30, 2013 als.org
gt
C
SsyHtmapptsto
tortrsmt
freadtwtp
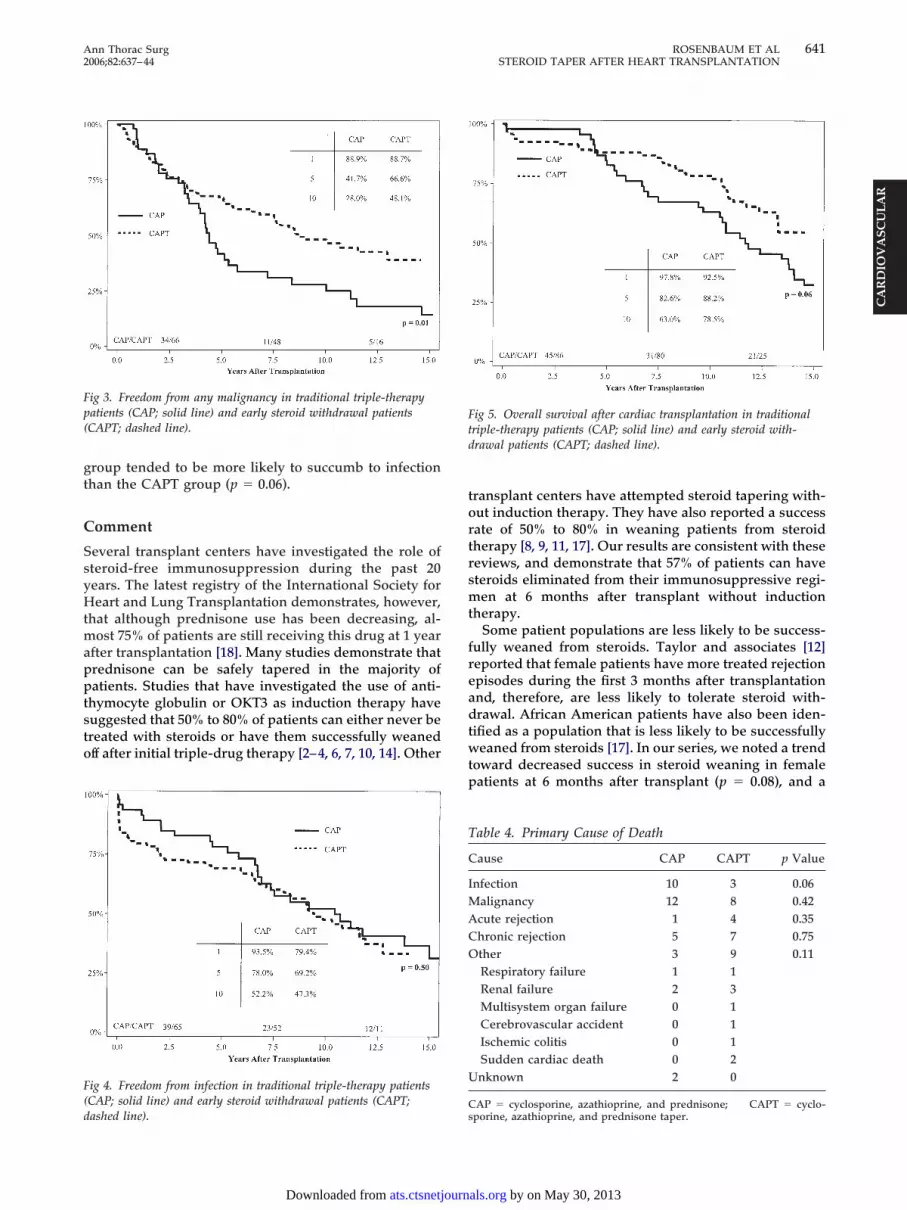
Fp(
F(d
Ftd
T
C
IMACO
U
641Ann Thorac Surg ROSENBAUM ET AL2006;82:637–44 STEROID TAPER AFTER HEART TRANSPLANTATION
CA
RD
IOV
ASC
ULA
R
roup tended to be more likely to succumb to infectionhan the CAPT group (p � 0.06).
omment
everal transplant centers have investigated the role ofteroid-free immunosuppression during the past 20ears. The latest registry of the International Society foreart and Lung Transplantation demonstrates, however,
hat although prednisone use has been decreasing, al-ost 75% of patients are still receiving this drug at 1 year
fter transplantation [18]. Many studies demonstrate thatrednisone can be safely tapered in the majority ofatients. Studies that have investigated the use of anti-
hymocyte globulin or OKT3 as induction therapy haveuggested that 50% to 80% of patients can either never bereated with steroids or have them successfully weanedff after initial triple-drug therapy [2–4, 6, 7, 10, 14]. Other
ig 3. Freedom from any malignancy in traditional triple-therapyatients (CAP; solid line) and early steroid withdrawal patientsCAPT; dashed line).
ig 4. Freedom from infection in traditional triple-therapy patientsCAP; solid line) and early steroid withdrawal patients (CAPT;
ashed line).Cs
ats.ctsnetjournDownloaded from
ransplant centers have attempted steroid tapering with-ut induction therapy. They have also reported a successate of 50% to 80% in weaning patients from steroidherapy [8, 9, 11, 17]. Our results are consistent with theseeviews, and demonstrate that 57% of patients can haveteroids eliminated from their immunosuppressive regi-en at 6 months after transplant without induction
herapy.Some patient populations are less likely to be success-
ully weaned from steroids. Taylor and associates [12]eported that female patients have more treated rejectionpisodes during the first 3 months after transplantationnd, therefore, are less likely to tolerate steroid with-rawal. African American patients have also been iden-
ified as a population that is less likely to be successfullyeaned from steroids [17]. In our series, we noted a trend
oward decreased success in steroid weaning in femaleatients at 6 months after transplant (p � 0.08), and a
ig 5. Overall survival after cardiac transplantation in traditionalriple-therapy patients (CAP; solid line) and early steroid with-rawal patients (CAPT; dashed line).
able 4. Primary Cause of Death
ause CAP CAPT p Value
nfection 10 3 0.06alignancy 12 8 0.42cute rejection 1 4 0.35hronic rejection 5 7 0.75ther 3 9 0.11Respiratory failure 1 1Renal failure 2 3Multisystem organ failure 0 1Cerebrovascular accident 0 1Ischemic colitis 0 1Sudden cardiac death 0 2nknown 2 0
AP � cyclosporine, azathioprine, and prednisone; CAPT � cyclo-porine, azathioprine, and prednisone taper.
by on May 30, 2013 als.org

sA
wristgrswd3itagw
swattlpari
csiiataawmra6
mmtpipcncmclfer
spls
whtattupcssfnts
1s[bspsCtgcwosgdm
TcdfTcmeisocCswsp
pi
642 ROSENBAUM ET AL Ann Thorac SurgSTEROID TAPER AFTER HEART TRANSPLANTATION 2006;82:637–44
CA
RD
IOV
ASC
ULA
R
ignificant reduction in successful steroid weaning infrican American patients (p � 0.03).There is some debate as to whether or not steroidithdrawal leads to an increased incidence of acute
ejection. Some studies demonstrate that acute rejections lower in patients who are successfully tapered fromteroids. These studies usually exclude patients who failhe steroid taper or place them in the steroid-requiringroup for analysis. Price and coworkers [6] found thatejection was lower in patients who were tapered offteroids by four months and noted that successful steroidithdrawal may select for a group of patients with aecreased propensity for rejection during the following2 months. Pritzker and associates [7] reported a similarncidence of acute rejection in both double-therapy andriple-therapy groups. Arnold and colleagues [15] foundhigher incidence of acute rejection in the triple-therapyroup, but this was after risk-stratifying patients whoere at higher risk of rejection into the triple-drug group.In contrast to the above studies, several reports de-
cribe an increased incidence of acute rejection afterithdrawal of steroids. Keogh and coworkers [4] reportedhigher incidence of rejection in a group of patients
reated without steroids through the initial 3 months afterransplantation. Previous data from our institution ana-yzed patients on an intent-to-treat basis (leaving thoseatients who failed steroid taper in the taper group fornalysis) and found an increased incidence of acuteejection in the early withdrawal group [11]. Not surpris-ngly, our current results mirror this data.
This increased frequency of acute rejection may in-rease posttransplant coronary artery disease in ourteroid withdrawal patients if immunologically mediatednjury to the endothelium during acute rejection is anmportant etiologic factor in chronic rejection. Olivarind colleagues [19], however, reported that triple-drugherapy with cyclosporine, azathioprine, and prednisone,lthough effective in preventing acute rejection, does notlter the incidence of coronary lesions when comparedith earlier and less effective immunosuppressive regi-ens [19]. In the current study, the frequency of acute
ejection did not correlate with posttransplant coronaryrtery disease, a finding consistent with other reports [2,, 12].Cardiac transplant recipients are at risk for developingalignancies, especially cutaneous neoplasms [20]. Im-unosuppression is considered a possible etiologic fac-
or in the increased incidence of cancer in this patientopulation. Our results suggest that steroid withdrawal
mproves the overall freedom from malignancy in ouratient population. When individual types of malignan-ies were considered, however, only cutaneous malig-ancies were affected. These findings mirror other re-ently published data, which demonstrate that afterultivariate analysis, immunosuppressive load (for cy-
losporine, azathioprine, steroids, antithymocyte globu-in, and OKT3) failed to emerge as independent riskactors for noncutaneous malignancy [21]. When consid-ring cutaneous malignancies, however, the risk may be
elated to cumulative immunosuppressive dosage, and rats.ctsnetjournDownloaded from
unlight exposure may exert an additive immunosup-ressive effect in these patients [22]. Certainly, the etio-
ogic factors of cancer are multifactorial, and furthertudy is needed.
Multiple reviews have examined the effects of steroidithdrawal on posttransplant infection. Several authorsave reported that steroid withdrawal does not influence
he incidence of infection [2–4, 23]. In contrast, Pritzkernd colleagues [7] found an increased incidence of bac-erial infection in patients who underwent early steroidaper. That study involved a group of patients whonderwent induction therapy with OKT3. Previouslyublished data from our institution described a de-reased incidence of infection in patients who underwentteroid taper at 2-year follow-up [11]. Our current resultsuggest that this benefit may be lost during long-termollow-up (see Fig 4). Although freedom from infection isot different between our groups of patients, there is a
rend toward decreased frequency of infection in theteroid-taper group.
Previous data from our institution demonstrated that atyear after transplantation, the incidence of diabetes was
ignificantly higher in patients who remained on steroids11]. Other series found no effect on posttransplant dia-etes after steroid withdrawal [3, 17]. In the currenttudy, we find no difference in freedom from diabetes inatients who undergo steroid withdrawal and also noignificant difference in body mass index between theAP and CAPT groups. Only one series demonstrated
hat those patients who are treated with triple therapyain more weight [6]. Most authors have noted thatardiac transplant recipients regain their premorbideight after surgery and that there is no difference inbesity between those patients managed with or withoutteroids [7, 9, 11, 16, 17]. Lake and associates [24] sug-ested that posttransplant weight gain is more depen-ent on genetic factors than immunosuppressiveedications.Survival tended to be improved in our CAPT patients.
his is an interesting finding given the observed in-reased frequency of acute rejection and absence of anyifference in posttransplant coronary artery disease and
reedom from solid malignancy between the two groups.he improved survival could be attributed to the in-reased freedom from cutaneous malignancies, althoughalignancy as a cause of death is not significantly differ-
nt between the two groups. The trend toward increasedncidence of infective episodes may lead to decreasedurvival in the CAP group, a hypothesis supported by thebservation that infection tended to more often be aause of death in this group when compared with theAPT group. Taylor and colleagues [12] also demon-
trated improved survival in patients who could beeaned off of steroids. They suggested that those who are
uccessfully tapered off steroids are “immunologicallyrivileged” and have a low risk of long-term mortality.In addition to the increased survival of the CAPT
atients, there is evidence that these patients enjoy anmproved quality of life as well. Jones and associates [25]
eported that patients who are managed on doubleby on May 30, 2013 als.org

tpsttt
rtqpHtmuefioAstwmaaClI(teteehasli
6awmlwa
WtITv
R
1
1
1
1
1
1
1
1
1
1
2
2
643Ann Thorac Surg ROSENBAUM ET AL2006;82:637–44 STEROID TAPER AFTER HEART TRANSPLANTATION
CA
RD
IOV
ASC
ULA
R
herapy (ie, without steroids) have a better sense ofhysical well being, are less anxious, more sexuallyatisfied, and financially more secure than their triple-herapy counterparts. In addition, double-therapy pa-ients demonstrated a lower frequency of and less dis-ress from therapeutic side effects [25].
We acknowledge the limitations inherent in this non-andomized retrospective study. It is certainly possiblehat the decreased freedom from and increased fre-uency of acute rejection that is seen in the taperedatients is owing to the increased frequency of biopsies.owever, when the steroid taper protocol was first insti-
uted, it was thought that these patients must be closelyonitored with increased biopsy frequency, and we still
se this biopsy protocol today. It is difficult to assess theffects that a more frequent biopsy schedule during therst 2 years after transplant may have on long-termutcomes, but it is possible that it biases our results.dditionally, the improved survival that is seen in the
teroid-taper patients could be related to the era in whichhese patients received their transplant. Unfortunately,e can only analyze variables that are available in theedical records. Subtle changes in surgical technique
nd postoperative care that evolve with time cannotlways be captured. However, the years that define ourAP and CAPT patients (1988–1990 and 1990–1996) over-
ap three eras as defined by the latest registry of thenternational Society of Heart and Lung Transplantation1982–1988, 1989–1993, and 1994–1998) [18]. Therefore,he increased survival of the CAPT patients cannot bexplained exclusively by the era in which their transplan-ation was performed. Finally, it is difficult to assess theffects of steroid withdrawal on other important postop-rative morbidities such as hypercholesterolemia andypertension, when almost all heart transplant patientsre routinely placed on lipid-lowering and antihyperten-ive therapies. Our study is strengthened, however, by itsarge size, long follow-up, and statistical analysis byntention-to-treat.
In conclusion, steroid withdrawal is possible in almost0% of patients at 6 months after transplantation. Despiten increased frequency of acute rejection, early steroidithdrawal improves the freedom from malignancy anday decrease the frequency of infection and improve
ong-term survival in the cardiac transplant populationithout increasing the risk of posttransplant coronary
rtery disease.
e thank Jesse Williams for his support and insightful review ofhe manuscript. This work is supported in part by the Nationalnstitutes of Health (5T32GM08593) Training Program in Burns,rauma and Critical Care and the Donald W. Reynolds Cardio-ascular Research Center.
eferences
1. Yacoub M, Alivizatos P, Khaghani A, Mitchell A. The use ofcyclosporine, azathioprine, and antithymocyte globulin with
or without low-dose steroids for immunosuppression ofcardiac transplant patients. Transplant Proc 1985;17:221–2.ats.ctsnetjournDownloaded from
2. O’Connell JB, Bristow MR, Rasmussen LG, et al. Cardiacallograft function with corticosteroid-free maintenance im-munosuppression. Circulation 1990;82(Suppl):IV-318–21.
3. Lee KF, Pierce JD, Hess ML, Hastillo AK, Wechsler AS,Guerraty AJ. Cardiac transplantation with corticosteroid-free immunosuppression: long-term results. Ann ThoracSurg 1991;52:211–8.
4. Keogh A, Macdonald P, Harvison A, Richens D, Mundy J,Spratt P. Initial steroid-free versus steroid-based mainte-nance therapy and steroid withdrawal after heart transplan-tation: two views of the steroid question. J Heart LungTransplant 1992;11:421–7.
5. Keogh A, Macdonald P, Mundy J, Chang V, Harvison A,Spratt P. Five-year follow-up of a randomized double-drugversus triple-drug therapy immunosuppressive trial afterheart transplantation. J Heart Lung Transplant 1992;11:550–6.
6. Price GD, Olsen SL, Taylor DO, O’Connell JB, Bristow MR,Renlund DG. Corticosteroid-free maintenance immunosup-pression after heart transplantation: feasibility and benefi-cial effects. J Heart Lung Transplant 1992;11:403–14.
7. Pritzker MR, Lake KD, Reutzel TJ, et al. Steroid-free main-tenance immunotherapy: Minneapolis Heart Institute expe-rience. J Heart Lung Transplant 1992;11:415–20.
8. Kobashigawa JA, Stevenson LW, Brownfield ED, et al. Initialsuccess of steroid weaning late after heart transplantation.J Heart Lung Transplant 1992;11:428–30.
9. Miller LW, Wolford T, McBride LR, Peigh P, Pennington DG.Successful withdrawal of corticosteroids in heart transplan-tation. J Heart Lung Transplant 1992;11:431–4.
0. Livi U, Luciani GB, Boffa GM, et al. Clinical results ofsteroid-free induction immunosuppression after heart trans-plantation. Ann Thorac Surg 1993;55:1160–5.
1. Olivari MT, Jessen ME, Baldwin BJ, et al. Triple-drug immu-nosuppression with steroid discontinuation by six monthsafter heart transplantation. J Heart Lung Transplant 1995;14:127–35.
2. Taylor DO, Bristow MR, O’Connell JB, et al. Improvedlong-term survival after heart transplantation predicted bysuccessful early withdrawal from maintenance corticoste-roid therapy. J Heart Lung Transplant 1996;15:1039–46.
3. Delgado D, Arazi HC, Sellanes M, et al. Study of earlycorticosteroid withdrawal in cardiac transplantation. Trans-plant Proc 1999;31:2524–5.
4. Oaks TE, Wannenberg T, Close SA, Tuttle LE, Kon ND.Steroid-free maintenance immunosuppression after hearttransplantation. Ann Thorac Surg 2001;72:102–6.
5. Arnold AN, Huffman M, Eich DM, et al. Risk-directedimmunosuppression in heart transplant recipients: mainte-nance prednisone can be avoided in selected patients.Transplant Proc 2002;34:1830–3.
6. Sanchez V, Delgado JE, Gomez MA, et al. Steroid with-drawal in nonimmunologically selected heart transplantrecipients. Transplant Proc 2002;34:164–5.
7. Felkel TO, Smith AL, Reichenspurner HC, et al. Survival andincidence of acute rejection in heart transplant recipientsundergoing successful withdrawal from steroid therapy.J Heart Lung Transplant 2002;21:530–9.
8. Taylor DO, Edwards LB, Boucek MM, et al. Registry of theInternational Society for Heart and Lung Transplantation:Twenty-Second Official Adult Heart Transplant Report—2005. J Heart Lung Transplant 2005;24:945–5.
9. Olivari MT, Homans DC, Wilson RF, Kubo SH, Ring WS.Coronary artery disease in cardiac transplant patients re-ceiving triple-drug immunosuppressive therapy. Circulation1989;80(Suppl):III-111–5.
0. Penn I. Tumors after renal and cardiac transplantation.Hematol Oncol Clin North Am 1993;7:431–45.
1. Caforio AL, Gambino A, Piaserico S, et al. De novo noncu-taneous malignancies in heart transplantation: a single-centre 15-year experience and risk factor analysis. Trans-
plant Proc 2001;33:3658–9.by on May 30, 2013 als.org

2
2
2
2
D
Daiattm
Dttmps
Dntytcti
DroaapciApim
DTcyssda
644 ROSENBAUM ET AL Ann Thorac SurgSTEROID TAPER AFTER HEART TRANSPLANTATION 2006;82:637–44
CA
RD
IOV
ASC
ULA
R
2. Caforio AL, Fortina AB, Piaserico S, et al. Skin cancer inheart transplant recipients: risk factor analysis and relevanceof immunosuppressive therapy. Circulation 2000;102(Suppl3):III-222–7.
3. Seydoux C, Berguer DG, Stumpe F, et al. Does early steroidwithdrawal influence rejection and infection episodes dur-ing the first 2 years after heart transplantation? Transplant
Proc 1997;29:620–4.t why the steroid patients are dying?
Dtonna
aieiwomtdpir
Dbvsdobyotwt
Dqtapactfwlp
ats.ctsnetjournDownloaded from
4. Lake KD, Reutzel TJ, Pritzker MR, Jorgensen CR, EmeryRW. The impact of steroid withdrawal on the de-velopment of lipid abnormalities and obesity in hearttransplant recipients. J Heart Lung Transplant 1993;12:580 –90.
5. Jones BM, Taylor FJ, Wright OM, et al. Quality of life afterheart transplantation in patients assigned to double- or
triple-drug therapy. J Heart Transplant 1990;9:392– 6.ISCUSSION
R D. GLENN PENNINGTON (Johnson City, TN): I wanted tosk one question. Maybe you said it and I just missed it. Thencidence of rejection was higher in those who were weaned,nd so when they developed rejection episodes, were theyreated with steroids at that point? I know it was intention toreat, so they stayed in the same group, but how was that
anaged?
R ROSENBAUM: If they were diagnosed with acute rejection,hey were treated with 3 days of prednisone. If that resolved,hen they were put back on a steroid taper and tapered off at 6
onths. If they suffered another episode of rejection, they arelaced back on long-term steroid treatment and remained onteroids but were left in the tapered group for analysis.
R ANDREW J. LODGE (Durham, NC): Congratulations on aice presentation. Can you comment on the definition of infec-
ion that was used, and also on the types of malignancies thatou saw and what the breakdown of the different malignancyypes was? You also mentioned that none of these patients gotytolytic induction therapy. Are you currently using any induc-ion immunosuppression, and what is the current maintenancemmunosuppression regimen that you are using?
R ROSENBAUM: Definition of infection was any patient whoequired hospitalization or intravenous therapy. For breakdownf malignancies, I can actually show you a slide. I have one,nyway. When malignancies were broken down, there wasctually no difference in freedom from solid malignancies orosttransplant lymphoproliferative disorder. There was in-reased freedom from cutaneous malignancies, which probablys what led to the increased freedom from overall malignancy.s I said, we did not use induction therapy during this treatmenteriod. However, currently we are using induction with basilix-
mab on day 0 and 4, starting cyclosporine on day 5, and usingycophenolate mofetil and prednisone with a prednisone taper.
R THOMAS M. EGAN (Chapel Hill, NC): Nice presentation.wo questions. One is, with the data that you have, are youonsidering delaying the onset of your steroid taper, becauseou have a pretty significant number that needed to go back onteroids and you might improve that by waiting to a year? Theecond question is, although you have demonstrated a niceifference in survival, have you analyzed causes of death to look
R ROSENBAUM: Thank you for your comments. During thisreatment period we had a 62% success rate in getting patientsff steroids. With our current treatment protocol with mycophe-olate mofetil, basiliximab induction, cyclosporine, and pred-isone taper, we are actually getting people off at 6 months withn 85% success rate.(Slide) In terms of our cause of death, as you can see by this,
nd I am sorry, I just didn’t have time to include it in my talk, butnfection and other as causes of death were significantly differ-nt between the two groups. So although there was an increasen freedom from malignancy, malignancy as a cause of a deathas not significantly different, and that is probably, again, basedn the fact that the main cause of that increased freedom fromalignancy was cutaneous malignancies. Acute rejection, al-
hough increased in the tapered group, was not a cause of deathifference, coronary artery disease was not a difference. So theatients who were left on steroids increased risk of dying from
nfection and those who were tapered off die from events like theest of us.
R JOHN H. CALHOON (San Antonio, TX): Doctor Rosen-aum, I have a question, and congratulations on presenting thisery nicely and covering the data very nicely. To me, it almosteems as if you have defined two different groups and twoifferent immune matches: those who are able to be weaned offf steroids or those who have a better match and are going to doetter regardless of the steroids. Do you have any way or haveou figured out a way to define whether that plays a major roler whether it is the steroids themselves that you are weaning offhat are making them better? I can’t tell whether the steroids areeaned off or whether it is just the patients have a better match
hat you weaned the steroids off.
R ROSENBAUM: That is an interesting point and a gooduestion, and it has been suggested before by some investiga-
ors that the patients who are able to be weaned off of steroidsre inherently more immunologically adept at tolerating trans-lant and therefore are able to get off steroids and are thereforeble to survive longer, which is a reasonable point and aonsideration. However, we would expect that those patientsherefore would at least potentially have an increased freedomrom transplant coronary artery disease, and that was not seenith our patients. So we did not look at that specifically, but
ooking at transplant coronary vasculopathy as a potential end
oint difference in those types of patients, we did not see that.by on May 30, 2013 als.org

DOI: 10.1016/j.athoracsur.2006.03.067 2006;82:637-644 Ann Thorac Surg
Drazner, Clyde W. Yancy, Jr, W. Steves Ring and J. Michael DiMaio C. Paul, Patricia A. Kaiser, Paul A. Pappas, Dan M. Meyer, Michael A. Wait, Mark H.
David H. Rosenbaum, Brian C. Adams, Joshua D. Mitchell, Michael E. Jessen, Michelle Effects of Early Steroid Withdrawal After Heart Transplantation
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/82/2/637including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/82/2/637#BIBL
This article cites 25 articles, 3 of which you can access for free at:
Citations http://ats.ctsnetjournals.org/cgi/content/full/82/2/637#otherarticles
This article has been cited by 4 HighWire-hosted articles:
Subspecialty Collections
http://ats.ctsnetjournals.org/cgi/collection/transplantation_heart Transplantation - heart
following collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on May 30, 2013 ats.ctsnetjournals.orgDownloaded from





























