Embed Size (px)
Citation preview

Eur Arch Otorhinolaryngol (2010) 267:593–600
DOI 10.1007/s00405-009-1087-4HEAD & NECK
Social withdrawal after laryngectomy
Helge Danker · Dorit Wollbrück · Susanne Singer · Michael Fuchs · Elmar Brähler · Alexandra Meyer
Received: 14 January 2009 / Accepted: 26 August 2009 / Published online: 16 September 2009© Springer-Verlag 2009
Abstract This investigation focuses on the psychosocialconcomitants of a laryngectomy. Semistructured interviewswere conducted with 218 laryngectomized patients. Stand-ardised questionnaires were used to assess patients’ socialactivity (FPAL, EORTC QLQ-C30), intelligibility ofspeech (PLTT, FPAL), mental well-being (HADS), andperceived stigmatisation (FPAL). More than 40% of thepatients withdrew from conversation. Only one-third of allpatients regularly took part in social activities. About 87%perceived stigmatisation because of their changed voiceand more than 50% felt embarrassed because of their tra-cheostoma. Almost one-third of the patients had increasedanxiety and depression scores. Moderate objective speechintelligibility was found, though patients were not particu-larly satisWed with their voice. Social activity emerged to beindependent from age, gender, treatment variables, andstage of disease. Multivariate analysis resulted in two inde-pendent factors representing two patterns of social with-drawal. On the one hand, there was withdrawal fromconversation accompanied by increased depression andpoor speech intelligibility. On the other hand, there werereduced social activities accompanied by increased anxietyand perceived stigmatisation.
Keywords Cancer · Oncology · Social withdrawal · Laryngectomy · Stigmatisation · Depression
Introduction
Total laryngectomy still remains to be an essential treat-ment for individuals diagnosed with advanced laryngealcancer despite the fact that chemotherapy and radiationhave been increasingly used for organ preservation. Treat-ment options have been thoroughly discussed and primarilydepend on tumour stage, tumour site, patient factors, andlocal expertise [1, 2]. If laryngectomy was considered to bethe treatment of choice, individuals have to cope with sev-eral negative physical and psychosocial consequences. Thesurgical procedure results in altered phonation, respiration,swallowing, and not least general health [3–6].
In consequence, patients have to learn new forms of ala-ryngeal communication such as oesophageal or tracheoe-sophageal speech. Laryngectomees who fail to acquirefunctional substitute voice are obliged to use electronicdevices for communication. But yet today, some individu-als remain aphonic [7–10]. Although oesophageal speechand electrolaryngeal methods are still common, the use ofprosthetic voice is increasing [11]. It provides a highly sat-isfactory and immediate vocalisation and a superior voicequality [9, 12, 13]. Furthermore, it appears that the qualityof normal speech is nearly approximated by prostheticspeech [14, 15].
However, diVerent authors report that voice qualityapproaches at best that of patients with partial laryngec-tomy [16] and substitute speech by itself has still lowerintelligibility [17]. Listeners clearly identify even tra-cheoesophageal speakers as being perceptually “diVerent”from normal laryngeal speakers [18]. ScientiWc analyses of
H. Danker (&) · D. Wollbrück · S. Singer · E. Brähler · A. MeyerIndependent Department of Medical Psychology and Medical Sociology, University of Leipzig, Philipp-Rosenthal-Straße 55, 04103 Leipzig, Germanye-mail: [email protected]
M. FuchsDepartment of Otorhinolaryngology, Section of Phoniatrics and Audiology, University of Leipzig, Leipzig, Germany
123
594 Eur Arch Otorhinolaryngol (2010) 267:593–600
the objective voice parameters bear out that the quality oftracheoesophageal speech is inferior to that of normalspeech [19]. Correlations between the objective and percep-tual parameters that had been rated by trained listeners weremoderate. Beyond this, there is evidence suggesting thattracheoesophageal speakers were rated worse in voice qual-ity and less acceptable than normal speakers [20]. Eadieand Doyle [21] found that especially women were identi-Wed from independent listeners as having less acceptableand less pleasant voices.
DiVerent authors report associations between voice-impairment and diYculties in interacting with family andfriends, and with participation in public events [22–24].Dysfunctional voice may contribute to social complica-tions and limited social activity, sometimes for the factthat patients have great problems, to make them under-stood in a noisy environment [5]. Voice problems, partic-ularly patients’ perception of voice handicap, might haveconsiderable implications on social interaction andadjustment. Some studies have indicated that patientswho perceive their own voice quality as less acceptableconWrm a lower level of social activity [25, 26]. Otherstudies revealed a trend for patients to experience diY-culties with social functioning due to a broad variety ofother reasons (for example dysphagia, radiation therapy,anxiety, depression, and quality of life) [6, 27–30].Another explanation for social withdrawal arises fromthe case that some patients who have had a laryngectomyfelt bothered by their appearance and their changed voice[31–34].
In summary, we state a growing availability of studiesthat provide for a better understanding the impact of a lar-yngectomy on patients’ physical and functional well-being.What is less clear is how especially social withdrawal isinXuenced by the patients’ perceptions of voice handicap,physical disWgurement, and mental well-being.
Methods
Participants
Using information that was provided by the Leipzig tumorregistry and six collaborating ENT-clinics in EasternGermany (the Universities of Halle and Leipzig, the Com-munity Hospitals St. Georg Leipzig, Chemnitz, Dresden-Friedrichstadt, and Martha-Maria Halle-Dölau), we recorded418 persons who had undergone a total laryngectomy since1986. There were 153 patients who had died at the timewhen contact was made, 35 patients refused participa-tion, and Wnally, there were 12 persons whose currentwhereabouts could not be determined. In total, 218 laryn-gectomees were interviewed in a cross-sectional study.
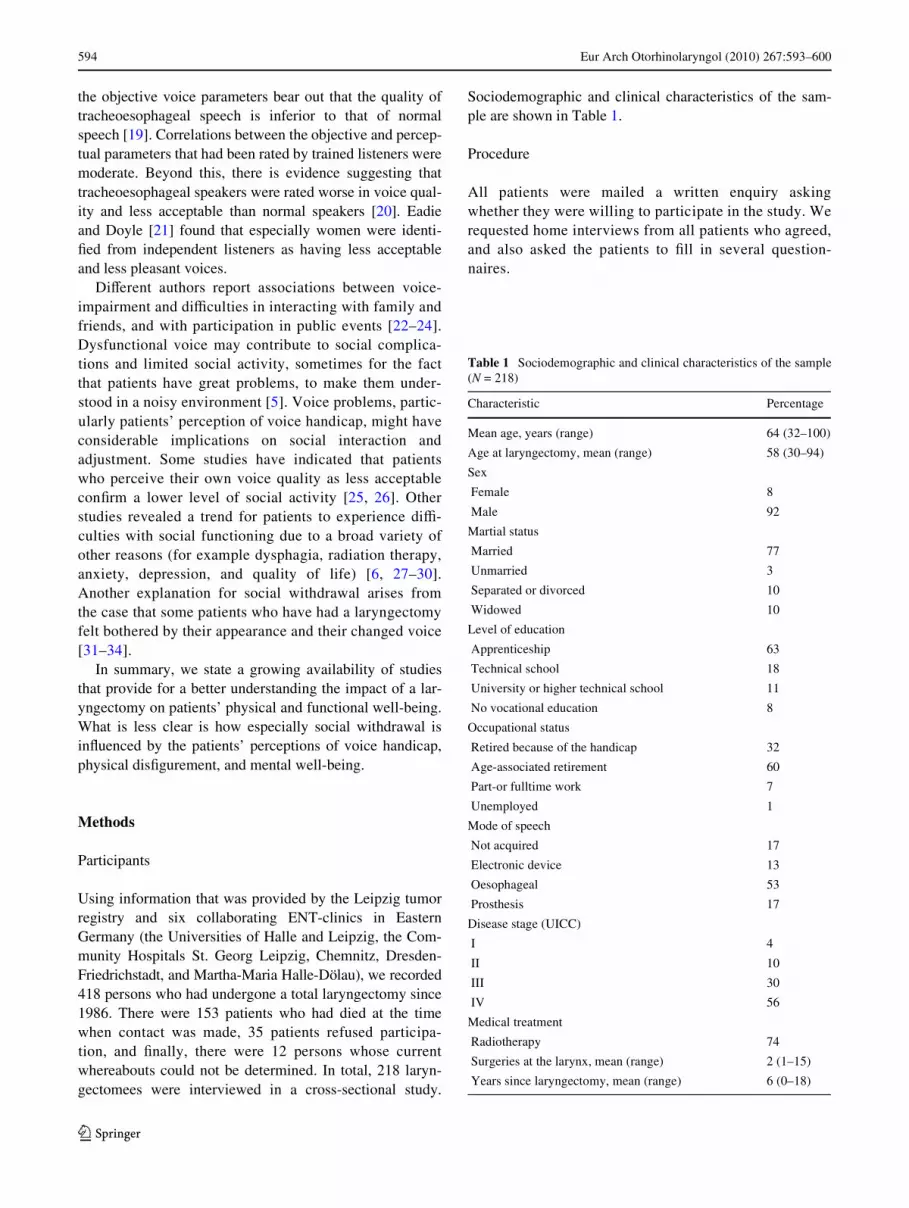
Sociodemographic and clinical characteristics of the sam-ple are shown in Table 1.
Procedure
All patients were mailed a written enquiry askingwhether they were willing to participate in the study. Werequested home interviews from all patients who agreed,and also asked the patients to Wll in several question-naires.
Table 1 Sociodemographic and clinical characteristics of the sample(N = 218)
Characteristic Percentage
Mean age, years (range) 64 (32–100)
Age at laryngectomy, mean (range) 58 (30–94)
Sex
Female 8
Male 92
Martial status
Married 77
Unmarried 3
Separated or divorced 10
Widowed 10
Level of education
Apprenticeship 63
Technical school 18
University or higher technical school 11
No vocational education 8
Occupational status
Retired because of the handicap 32
Age-associated retirement 60
Part-or fulltime work 7
Unemployed 1
Mode of speech
Not acquired 17
Electronic device 13
Oesophageal 53
Prosthesis 17
Disease stage (UICC)
I 4
II 10
III 30
IV 56
Medical treatment
Radiotherapy 74
Surgeries at the larynx, mean (range) 2 (1–15)
Years since laryngectomy, mean (range) 6 (0–18)
123

Eur Arch Otorhinolaryngol (2010) 267:593–600 595
Assessment instruments
Questionnaire for psychosocial adjustment after laryngectomy
The questionnaire for psychosocial adjustment after laryn-gectomy (FPAL) was developed to assess social and mentalwell-being especially among laryngectomized individuals.It consists of 124 items. In the current study, we chose Wvescales out of 12: “social activity”, and “withdrawal fromtalking” to assess social withdrawal; “stigmatisationbecause of tracheostoma”, and “stigmatisation because ofvoice” to assess perceived stigmatisation, and “intelligibil-ity towards signiWcant others” to assess perceived speechintelligibility. The total score for each subscale was com-puted by summation of the referring single items (range 0–100). Internal consistency is declared by the authors being0.69–0.89 [31, 35].
Postlaryngectomy telephone test
The postlaryngectomy telephone test (PLTT) was devel-oped by Zenner and Pfrang [36] to assess the objectiveintelligibility of speech. It is based on a pool of 400 phonet-ically balanced monosyllables and 100 sentences. In eachtrial, an interviewer randomly selects 20 words and Wvesentences written on cards. The laryngectomee wasrequested to read all words and sentences one by one viatelephone or via walkie-talkie. The listener noted the num-ber of correctly understood words and sentences. Finally,total speech intelligibility was computed with its maximumvalue of 100%. The test has an internal consistency rangingfrom 0.88 to 0.90 for diVerent listeners and diVerent condi-tions. Validity is given by correlations between perceivedintelligibility of laryngectomees and listeners’ assessment(r = 0.24–0.39).
Hospital Anxiety and Depression Scale
The Hospital Anxiety and Depression Scale is a 14-itemself-report instrument, specially used for screening ofdepression and anxiety [37]. Each of two scales consistsof seven items with a Likert response scale. The two-factor structure has been conWrmed in several studies[38–41]. Increasing scores indicate increasing burden.Total scores were computed by summation. The cut-oVpoints for the identiWcation of psychological distress arestill controversial. DiVerent cut-oV scores are necessaryfor diVerent populations. The scores with the bestproportions of sensitivity (given the fact that sensitivityis as important as speciWcity) for laryngectomizedpatients were ¸7 for both, anxiety and depression scale[42].
EORTC QLQ-C30
The European Organisation for Research and Treatment ofCancer Core Questionnaire, the EORTC QLQ-C30, is awidely known and used instrument for assessing quality oflife in cancer patients. It is a 30-item self-administeredinstrument. The subscale ‘social functioning’ (EORTC-SF)consists of two Likert-scaled items. High scores indicate ahigh level of functioning [43, 44].
Statistical analysis
SPSS 15.0® for Windows was used for the statistical analy-sis. Spearman’s correlation coeYcient was employed toassess bivariate correlations between social withdrawal,stigmatisation, and quality of voice, because normal distri-bution was not given. Only values of � > 0.2 were deemedto be relevant. A multivariate canonical correlation analysiswas calculated, in order to verify bivariate correlations andto prevent alpha-error-cumulation in multiple testing.
Results
Descriptive analysis
Findings indicate social withdrawal that is posed bydecreased communication in more than 40% of the patients.A description of the most frequent problems experiencedby the patients indicates that 54% declared to talk consider-ably less than before treatment, and 57% thought that muchwas remaining unsaid. Another 51% exclusively talkedabout important things, followed by 42% who spoke as lit-tle as possible, and Wnally 40% who refused to go wherethey had to speak (Fig. 1).
More than 80% of the participants were aware of thestigma associated with their changed voice. In addition,half of those surveyed felt embarrassed because of their tra-cheostoma (Fig. 1).
The most frequent activity was small talk with neigh-bours (77%), followed by making errands (73%). Onlyaround one-third goes on trips, meetings, restaurants, orpublic events. Finally, another third of the surveyed personswas an active member in a support group (35%) (Fig. 2).
For each scale, seven items on the HADS questionnairemeasured the extent to which patients felt depressed or anx-ious. Following the recommended cut-oV value for laryngec-tomized patients [42], there are around one-third of thepatients who had increased anxiety scores and another third ofthe patients who had increased depression scores (Table 2).
As can be seen from the mean score in the PLTT, theobjective speech intelligibility was moderate. However, thehigh standard deviation for this score indicates that individual
123

596 Eur Arch Otorhinolaryngol (2010) 267:593–600
intelligibility commonly diVers to quite an extent frommean score. Consequently, there were both successful anddeWcient voice rehabilitation outcomes. In comparison tothe objective parameter, patients were not particularly satis-Wed with their perceived quality of speech (Table 2).
Bivariate testing
Correlations were tested between the diVerent measures ofspeech intelligibility and variables representing social with-drawal and perceived stigmatisation (Table 3).
The data show positive moderate correlations betweensocial withdrawal and perceived speech intelligibility,which were stronger than those observed with objectivequality of speech. Similarly, slight correlations were foundbetween perceived stigmatisation and subjective speechintelligibility. Social withdrawal was also found to be asso-ciated with increased anxiety and depression. As shown inthe table, patients who experienced higher levels of distressmore often reported problems in social contacts.
Furthermore, a slight correlation between time sincetreatment and social activity was observed. Data reveal
Fig. 1 FPAL-scale “withdrawal from talking”
0% 20% 40% 60% 80% 100%
much remains unsaid
conversations are muchless common today
speak almost exclusivelyabout important things
speak as little as possible
prefer not to go where haveto talk
speak only if there is notany other way
yes partly no
Fig. 2 Two items from FPAL stigmatisation-scales and FPAL scale “social activity”
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
much remains unsaid
conversations are muchless common today
speak almost exclusivelyabout important things
speak as little as possible
prefer not to go where haveto talk
speak only if there is notany other way
feel stigmatised because ofvoice
feel stigmatised because oftracheostoma
yes partly no
Table 2 HADS anxiety scale, HADS depression scale, objective speech intelligibility (PLTT), and subjective speech intelligibility (FPAL scale“intelligibility towards signiWcant others”)
N Minimum Maximum Mean SD N increased score ¸7 (%)
HADS anxiety 193 0 14 5.4 3.3 64 (33.3)
HADS depression 192 0 17 5.3 3.9 62 (32.5)
Objective speech intelligibility 153 0 100 53.2 34.6
Subjective speech intelligibility 192 0 100 31.5 22.3
123

Eur Arch Otorhinolaryngol (2010) 267:593–600 597
that the longer the time since treatment, the fewerpatients withdrew from social situations. What is inter-esting in this data is that social activity was regardless ofage (Table 3).
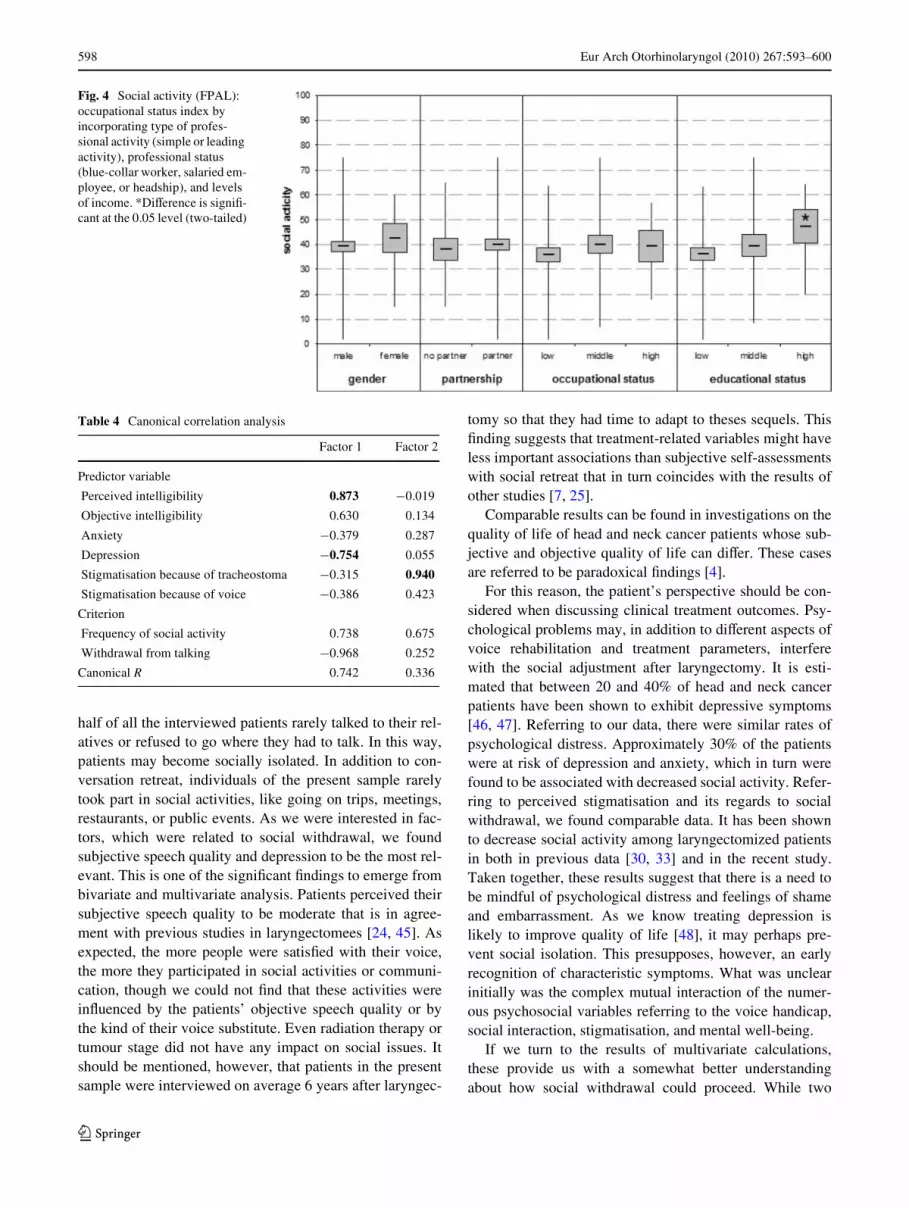
There were no signiWcant diVerences in social activitybetween sociodemographic or treatment variables, exceptfor education. Those people who have higher education lev-els also report signiWcantly more social activity in theFPAL-scale (Figs. 3, 4).
No signiWcant diVerences were found in the social func-tioning scale (EORTC QLQ-C30).
Canonical correlation analysis
Relationships with multiple correlation and most importantcomponents were pointed out in a canonical correlationanalysis. We established one set of predictors (perceivedintelligibility, objective intelligibility, anxiety, depression,and stigmatisation) and one set of criterion variables (fre-quency of social activity and withdrawal from talking).Those predictor and criterion variables with a maximumcorrelation were extracted as independent factors.
Finally, we found a signiWcant total correlation (Pillai’sF = 10.02; P = 0.000). Two independent factors represent-ing two forms of social withdrawal could be extracted outof six predictor variables and two criterion variables(CR1 = 0.742; CR2 = 0.336; see Table 4). On the one hand,there is withdrawal from conversation accompanied withincreased depression, poor objective speech intelligibility,and poor perceived speech intelligibility. On the otherhand, there are social activities accompanied with increasedanxiety and perceived stigmatisation.
Discussion
This study set out to determine the importance of socialwithdrawal in individuals treated by total laryngectomy. Inreviewing the literature, we found references, which led tothe assumption that social activity could be severelyimpaired by the treatment and its consequences, especiallyby the voice handicap. In the present sample, wherepatients were treated on average 6 years ago, we also foundconsiderable evidence for social withdrawal. The presentWndings seem to be consistent with other research, whichfound a tendency for respondents to reduce conversationwith others [7, 30]. For example, we found that more than
Table 3 Bivariate correlation and Spearman rho for non-normal dis-tributed data
*Correlation is signiWcant at the 0.05 level (two-tailed)
**Correlation is signiWcant at the 0.01 level (two-tailed)
Withdrawal from talking (�)
Social activity (�)
Objective intelligibility ¡0.367** 0.366**
Perceived intelligibility ¡0.634** 0.497**
Stigmatisation because of voice 0.280** 0.040
Stigmatisation because of tracheostoma
0.315** ¡0.137
Anxiety 0.322** ¡0.150*
Depression 0.544** ¡0.404**
Age 0.105 ¡0.061
Time since treatment 0.119 0.233**
Stigmatisation because of voice (�)
Stigmatisation because of tracheostoma (�)
Objective intelligibility ¡0.152 ¡0.131
Perceived intelligibility ¡0.252** ¡0.295**
Fig. 3 FPAL-scale “social activity”, N = 191, disease stage (UICC I–IV)
123
598 Eur Arch Otorhinolaryngol (2010) 267:593–600
half of all the interviewed patients rarely talked to their rel-atives or refused to go where they had to talk. In this way,patients may become socially isolated. In addition to con-versation retreat, individuals of the present sample rarelytook part in social activities, like going on trips, meetings,restaurants, or public events. As we were interested in fac-tors, which were related to social withdrawal, we foundsubjective speech quality and depression to be the most rel-evant. This is one of the signiWcant Wndings to emerge frombivariate and multivariate analysis. Patients perceived theirsubjective speech quality to be moderate that is in agree-ment with previous studies in laryngectomees [24, 45]. Asexpected, the more people were satisWed with their voice,the more they participated in social activities or communi-cation, though we could not Wnd that these activities wereinXuenced by the patients’ objective speech quality or bythe kind of their voice substitute. Even radiation therapy ortumour stage did not have any impact on social issues. Itshould be mentioned, however, that patients in the presentsample were interviewed on average 6 years after laryngec-
tomy so that they had time to adapt to theses sequels. ThisWnding suggests that treatment-related variables might haveless important associations than subjective self-assessmentswith social retreat that in turn coincides with the results ofother studies [7, 25].
Comparable results can be found in investigations on thequality of life of head and neck cancer patients whose sub-jective and objective quality of life can diVer. These casesare referred to be paradoxical Wndings [4].
For this reason, the patient’s perspective should be con-sidered when discussing clinical treatment outcomes. Psy-chological problems may, in addition to diVerent aspects ofvoice rehabilitation and treatment parameters, interferewith the social adjustment after laryngectomy. It is esti-mated that between 20 and 40% of head and neck cancerpatients have been shown to exhibit depressive symptoms[46, 47]. Referring to our data, there were similar rates ofpsychological distress. Approximately 30% of the patientswere at risk of depression and anxiety, which in turn werefound to be associated with decreased social activity. Refer-ring to perceived stigmatisation and its regards to socialwithdrawal, we found comparable data. It has been shownto decrease social activity among laryngectomized patientsin both in previous data [30, 33] and in the recent study.Taken together, these results suggest that there is a need tobe mindful of psychological distress and feelings of shameand embarrassment. As we know treating depression islikely to improve quality of life [48], it may perhaps pre-vent social isolation. This presupposes, however, an earlyrecognition of characteristic symptoms. What was unclearinitially was the complex mutual interaction of the numer-ous psychosocial variables referring to the voice handicap,social interaction, stigmatisation, and mental well-being.
If we turn to the results of multivariate calculations,these provide us with a somewhat better understandingabout how social withdrawal could proceed. While two
Table 4 Canonical correlation analysis
Factor 1 Factor 2
Predictor variable
Perceived intelligibility 0.873 ¡0.019
Objective intelligibility 0.630 0.134
Anxiety ¡0.379 0.287
Depression ¡0.754 0.055
Stigmatisation because of tracheostoma ¡0.315 0.940
Stigmatisation because of voice ¡0.386 0.423
Criterion
Frequency of social activity 0.738 0.675
Withdrawal from talking ¡0.968 0.252
Canonical R 0.742 0.336
Fig. 4 Social activity (FPAL): occupational status index by incorporating type of profes-sional activity (simple or leading activity), professional status (blue-collar worker, salaried em-ployee, or headship), and levels of income. *DiVerence is signiW-cant at the 0.05 level (two-tailed)
123

Eur Arch Otorhinolaryngol (2010) 267:593–600 599
independent factors were obtained from the canonical cor-relation analysis, we could assume analogously two diVer-ent kinds of social withdrawal. On the one hand, there areindividuals who withdraw from conversation, suVer fromdepression and experience poor speech intelligibility. Onthe other hand, there are laryngectomees who participate insocial activities that are unfortunately accompanied byincreased feelings of anxiety and stigmatisation. These twoforms of withdrawal may represent diVerent behaviours ofadjustment to the postoperative situation, which in turncould help to enable professionals and relatives to a morespeciWc support.
Nevertheless, longitudinal investigations should providethe understanding of an underlying process that is likely tocontribute to social isolation.
Implications
It is suggested to pay attention to patients who showdepressive symptoms and who tend to withdraw from com-munication. If necessary, adequate psychosocial supportshould be oVered. Beyond this, self-help groups could helpto overcome social isolation. Therein patients need to begiven information about available resources for psychoso-cial support. The data from the study show that the integra-tion in self-help groups is still relatively low.
Acknowledgment The project was Wnanced with a grant from theGerman Federal Ministry for Education and Research (# 7DZAIQTX).
ConXict of interest statement The authors declare that they have noconXict of interest.
References
1. PWster DG, Laurie SA, Weinstein GS, Mendenhall WM, AdelsteinDJ, Ang KK, Clayman GL, Fisher SG, Forastiere AA, HarrisonLB, Lefebvre JL, Leupold N, List MA, O’Malley BO, Patel S,Posner MR, Schwartz MA, Wolf GT (2006) American Society ofClinical Oncology clinical practice guideline for the use of larynx-preservation strategies in the treatment of laryngeal cancer. J ClinOncol 24:3693–3704
2. Genden EM, Ferlito A, Rinaldo A, Silver CE, Fagan JJ, Suarez C,Langendijk JA, Lefebvre JL, Bradley PJ, Leemans R, Chen AY,Jose J, Wolf GT (2008) Recent changes in the treatment of patientswith advanced laryngeal cancer. Head Neck J Sci Spec Head Neck30:103–110
3. Bohnenkamp TA (2008) The eVects of a total laryngectomy onspeech breathing. Curr Opin Otolaryngol Head Neck Surg 16:200–204
4. Bindewald J, Herrmann E, Dietz A, Wulke C, Meister EF, Woll-bruck D, Singer S (2007) Quality of life and voice intelligibility inlaryngeal cancer patients. Relevance of the “Satisfaction paradox”.Laryngorhinootologie 86:426–430
5. Op de Coul BMR, AckerstaV AH, Van As CJ, van den HoogenFJA, Meeuwis CA, Manni JJ, Hilgers FJM (2005) Quality of life
assessment in laryngectomized individuals: do we need additionsto standard questionnaires in speciWc clinical research projects?Clin Otolaryngol 30:169–175
6. Boscolo-Rizzo P, Maronato F, Marchiori C, Gava A, Da MostoMC (2008) Long-term quality of life after total laryngectomy andpostoperative radiotherapy versus concurrent chemoradiotherapyfor laryngeal preservation. Laryngoscope 118:300–306
7. AckerstaV AH, Hilgers FJ, Aaronson NK, Balm AJ (1994)Communication, functional disorders and lifestyle changes aftertotal laryngectomy. Clin Otolaryngol 19:295–300
8. Mendenhall WM, Morris CG, Stringer SP, Amdur RJ, HinermanRW, Villaret DB, Robbins KT (2002) Voice rehabilitation aftertotal laryngectomy and postoperative radiation therapy. J ClinOncol 20:2500–2505
9. Ferrer Ramirez M, Guallart Domenech F, Brotons Durban S,Carrasco Llatas M, Estelles Ferriol E, Lopez Martinez R (2001)Surgical voice restoration after total laryngectomy: long-termresults. Eur Arch Otorhinolaryngol 258:463–466
10. Jassar P, England RJ, StaVord ND (1999) Restoration of voiceafter laryngectomy. J R Soc Med 92:299–302
11. Brown DH, Hilgers FJM, Irish JC, Balm AJM (2003) Postlaryng-ectomy voice rehabilitation: state of the art at the millennium.World J Surg 27:824–831
12. Op de Coul BMR, Hilgers FJM, Balm AJM, Tan IB, van denHoogen FJA, van Tinteren H (2000) A decade of postlaryngecto-my vocal rehabilitation in 318 patients: a single institution’s expe-rience with consistent application of provox indwelling voiceprostheses. Arch Otolaryngol Head Neck Surg 126:1320–1328
13. Debruyne F, Delaere P, Wouters J, Uwents P (1994) Acousticanalysis of tracheo-oesophageal versus oesophageal speech.J Laryngol Otol 108:325–328
14. Hilgers FJ, AckerstaV AH (2000) Comprehensive rehabilitationafter total laryngectomy is more than voice alone. Folia PhoniatrLogop 52:65–73
15. Hillman RE, Walsh MJ, Wolf GT, Fisher SG, Hong WK (1998)Functional outcomes following treatment for advanced laryngealcancer. Part I—voice preservation in advanced laryngeal cancer.Part II—laryngectomy rehabilitation: the state of the art in the VAsystem. Ann Otol Rhinol Laryngol Suppl 172:1–27
16. OlthoV A, Steuer-Vogt MK, Licht K, Sauer-Goenen M, Werner C,Ambrosch P (2006) Quality of life after treatment for laryngealcarcinomas. ORL 68:191–196
17. Schuster M, Haderlein T, Nöth E, Lohscheller J, Eysholdt U,Rosanowski F (2006) Intelligibility of laryngectomees substitutespeech: automatic speech recognition and subjective rating. EurArch Otorhinolaryngol 263:188–193
18. Tardymitzell S, Andrews ML, Bowman SA (1985) Acceptabilityand intelligibility of tracheoesophageal speech. Arch OtolaryngolHead Neck Surg 111:213–215
19. Moerman M, Martens JP, Dejonckere P (2004) Application of theVoice Handicap Index in 45 patients with substitution voicingafter total laryngectomy. Eur Arch Otorhinolaryngol 261:423–428
20. Finizia C, Dotevall H, Lundstrom E, Lindstrom J (1999) Acousticand perceptual evaluation of voice and speech quality—a study ofpatients with laryngeal cancer treated with laryngectomy vs irradi-ation. Arch Otolaryngol Head Neck Surg 125:157–163
21. Eadie TL, Doyle PC (2004) Auditory-perceptual scaling and qualityof life in tracheoesophageal speakers. Laryngoscope 114:753–759
22. Lundström E, Hammarberg B, Munck-Wikland E (2009) Voicehandicap and health-related quality of life in laryngectomees:assessments with the use of VHI and EORTC Questionnaires.Folia Phoniatrica et Logopaedica 61:83–92
23. Terrell JE, Ronis DL, Fowler KE, Bradford CR, Chepeha DB,Prince ME, Teknos TN, Wolf GT, DuVy SA (2004) Clinicalpredictors of quality of life in patients with head and neck cancer.Arch Otolaryngol Head Neck Surg 130:401–408
123

600 Eur Arch Otorhinolaryngol (2010) 267:593–600
24. Kazi R, Singh A, De Cordova J, Al Mutairy A, O’Leary L, NuttingCM, Clarke P, Rhys-Evans P, Harrington KJ (2007) Postlaryngec-tomy vocal rehabilitation: assessment using a validated question-naire in 51 patients. ORL 69:289–294
25. Hilgers FJ, AckerstaV AH, Aaronson NK, Schouwenburg PF,Van Zandwijk N (1990) Physical and psychosocial consequencesof total laryngectomy. Clin Otolaryngol 15:421–425
26. Pfrang H (1986) Social and psychosocial aspects of vocal rehabil-itation in laryngectomized patients—preliminary results. In:Herrmann IF (ed) Speech restoration via voice prothesis. Springer,Berlin, pp 162–164
27. Birkhaug E, Aarstad H, Olofsson J (2002) Relation between mood,social support and the quality of life in patients with laryngecto-mies. Eur Arch Otorhinolaryngol 259:197–204
28. Hanna E, Sherman AC, Adams DC, Vural E, Fan C-Y, Suen JY(2004) Quality of life for patients following total laryngectomy vschemoradiation for laryngeal preservation. Arch OtolaryngolHead Neck Surg 130:875–879
29. Maclean J, Cotton S, Perry A (2009) Dysphagia following a totallaryngectomy: the eVect on quality of life, functioning, and psy-chological well-being. Dysphagia 24(3):314–321
30. de Maddalena H, Pfrang H, Zenner HP (1992) Erklärungsmodelledes sozialen Rückzugs bei Krebspatienten. Ergebnisse einer pros-pektiven Verlaufsuntersuchung bei Patienten nach Kehlkopfoper-ation, pp 74–114
31. de Maddalena H (2002) The inXuence of early speech rehabilita-tion with voice prostheses on the psychological state of laryngec-tomized patients. Eur Arch Otorhinolaryngol 259:48–52
32. Nalbadian M, Nikolaou A, Nikolaidis V, Petridis D, Themelis C,Daniilidis I (2001) Factors inXuencing quality of life in laryngec-tomized patients. Eur Arch Otorhinolaryngol 258:336–340
33. Devins GM, Stam HJ, Koopmans JP (1994) Psychosocial impactof laryngectomy mediated by perceived stigma and illnessintrusiveness. Can J Psychiatry 39:608–616
34. de Boer MF, Pruyn JF, van den Borne B, Knegt PP, Ryckman RM,Verwoerd CD (1995) Rehabilitation outcomes of long-termsurvivors treated for head and neck cancer. Head Neck 17:503–515
35. de Maddalena H, Pfrang H, Schohe R, Zenner HP (1991)Sprachverständlichkeit und psychosoziale Anpassung bei verschi-edenen Stimmrehabilitationsmethoden nach Laryngektomie.Laryngorhinootologie 70:562–567
36. de Maddalena H, Zenner HP (1996) Evaluation of speech intelli-gibility after prosthetic voice restoration by a standardizedtelephone test. In: Algaba J (ed) Surgery and prosthetic voicerestoration after total and subtotal laryngectomy. Elsevier,Amsterdam, pp 183–187
37. Zigmond AS, Snaith RP (1983) The Hospital Anxiety and Depres-sion Scale. Acta Psychiatr Scand 67:361–370
38. Hinz A, Schwarz R (2001) Angst und Depression in der All-gemeinbevölkerung: eine Normierungsstudie zur Hospital Anxi-ety and Depression Scale. Psychother Psychosom Med Psychol51:193–200
39. Herrmann C, Buss U, Snaith RP (1995) HADS-D: Hospital Anxi-ety and Depression Scale. Deutsche Version. Ein Fragebogen zurErfassung von Angst und Depressivität in der somatischen Medi-zin
40. Mykletun A, Stordal E, Dahl AA (2001) Hospital Anxiety andDepression (HAD) scale: factor structure, item analyses and inter-nal consistency in a large population. Br J Psychiatry 179:540–544
41. Smith AB, Selby PJ, Velikova G, Stark D, Wright EP, Gould A,Cull A (2002) Factor analysis of the Hospital Anxiety and Depres-sion Scale from a large cancer population. Psychol Psychother75:165–176
42. Singer S, Danker H, Dietz A, Homemann B, Koscielny S, OekenJ, Matthaus C, Vogel HJ, Krauss O (2008) Screening for mentaldisorders in laryngeal cancer patients: a comparison of 6 methods.Psycho-Oncology 17:280–286
43. Aaronson N, Ahmedzai S, Bergmann B, Bullinger M, Cull A,Duez NJ, Filiberti A, Flechtner H, de Haes JCJM, Kaasa S, KleeM, Osoba D, Razavi D, Rofe PB, Schraub S, Sneeuw K, SullivanM, Takeda F, for the EORTC Study Group on Quality of Life(1993) The European Organization for Research and Treatment ofCancer QLQ-C30: a quality-of-life instrument for use in interna-tional clinical trials in oncology. J Nat Cancer Inst 85:365–376
44. Björdal K, de GraeV A (2000) A 12 country Weld study of theEORTC QLQ-C30 (version 3.0) and the head and neck cancer spe-ciWc module (EORTC QLQ-H&N35) in head and neck patients.Eur J Cancer 36:1796–1807
45. Stewart MG, Chen AY, Stach CB (1998) Outcomes analysis ofvoice and quality of life in patients with laryngeal cancer. ArchOtolaryngol Head Neck Surg 124:143–148
46. DuVy SA, Terrell JE, Valenstein M, Ronis DL, Copeland LA,Connors M (2002) EVect of smoking, alcohol, and depression onthe quality of life of head and neck cancer patients. Gen HospPsychiatry 24:140–147
47. Singer S, Herrmann E, Welzel C, Klemm E, Heim M, Schwarz R(2005) Comorbid mental disorders in laryngectomees. Onkologie28:631–636
48. DuVy SA, Ronis DL, Valenstein M, Fowler KE, Lambert MT,Bishop C, Terrell JE, University of Michigan Head and NeckCancer (2007) Depressive symptoms, smoking, drinking, andquality of life among head and neck cancer patients. Psychosomat-ics 48:142–148
123





























