Embed Size (px)
Citation preview

w w w w.
w w w.dentalnewsweek .com
DENTOPHOBIA
DENTAL NEWSWEEK
PLUSmore updated topics and dental materilas
page 11
OZONE THERAPY IN PEDIATRIC >>> page 16
A SMILE MAKEOVER CASE REPORT >>> page 19
IS THE STATE OF ART IN DENTAL AND ORAL SCIENCES
ISSUE July 2016
RESILAN AND GUTTA-PERCHA >>> page 6
Issue August 2016

P U B L I S H I N G D I R E C TO R
Dr.H icham Nuaimi
dr.h ichamnuaimi@
gmai l .com
D E S I G N / P R O D U C T I O N
Ahmet S Aga
Elena Stanica
CO N T R I B U T I N G
W R I T E R S
Jennifer Sta infor th
R ana Al jabaj i
Dra Mar ia chairez
Sura Salem
K r ist ina Dani l i shin
Sai f A Abdl R azaq
P R I N T I N G
Onl ine and Digita l
Vers ion
(w w w.dentalnews-
week .com)
Publ ished three t imes
a year by by Dental
United spz .o.o
, Atensk a, 03-798
Warsaw, Poland
D R H I C H A M N UA I M I Associate
Editor & Scientif ic Manager of
D ental Newsweek . our a im is
to capture h igh- qual i t y wor k
t h a t d o e s n’ t o t h e r j o u r n a l s
focusing on dental research.
D R B A R B A R A P O D O B A S -
M Ü D E R R I S O Ğ L U A d v i s o r y
B o a r d C h a i r m a n o f D e n t a l
N e ws we k . O u r M a g a z i n e w i l l
publish more than cl inical and
academic research.
D R M U S TA FA K A M I L Pu b l i c
relation & International Affairs
( I r a q R e gi o n ) . Th i s m a g a z i n e
l a u n c h e s a n o p e n - m i n d e d
s t a n c e t o w a r d s t h e s c o p i n g
in dental sc iences.
2
D E N T A L N E W S W E E K M A G A Z I N E | A U G U S T 2 0 1 6
MEE T THE TEAMINFORMATION

DR.BURHAN KOMBARJI Chief Editor of Dental Newsweek
is a new broad-scope publ ica-
t i o n a i m i n g to p u b l i s h h i g h -
q u a l i t y r e s e a r c h a n d e x p e r t
k n o w l e d g e o n d e n t a l t o p i c s
that guarantee the refreshing
and bui ld ing modern k nowl-
ege that enhance dental care
T h e M a g a z i n e h a s a s t r o n g
emphasis on interdisc ipl inar y
issues as we’re conscious that
c h a l l e n g i n g c a s e s w h i c h a re
in c lose contac t with dent is t
s a n d d e nt a l te c h n i s i o n s w h o
are deals with update solution
for previous impossible cured.
U l t i m a t e l y , t h e M a g a z i n e
wants to cover a l l aspec ts of
o r a l s c i e n c e a n d t e c h n o l o g y
c o n c e r n e d w i t h t h e d e n t a l
f ie ld.
We look for ward to welcoming
your submiss ions.
3
D E N T A L N E W S W E E K M A G A Z I N E | A U G U S T 2 0 1 6
MESSAGE FROM EDITOR

» p.11 » p.22 » p.23
11 3D ANATOMICAL Z I R C O N I A IMPLANTS
22 D E N T A L E V E N T S A N D CONFERENCES
23 SPOT ON POLAND
4
D E N T A L N E W S W E E K M A G A Z I N E | A U G U S T 2 0 1 6
CONTENTS

5
D E N T A L N E W S W E E K M A G A Z I N E | A U G U S T 2 0 1 6
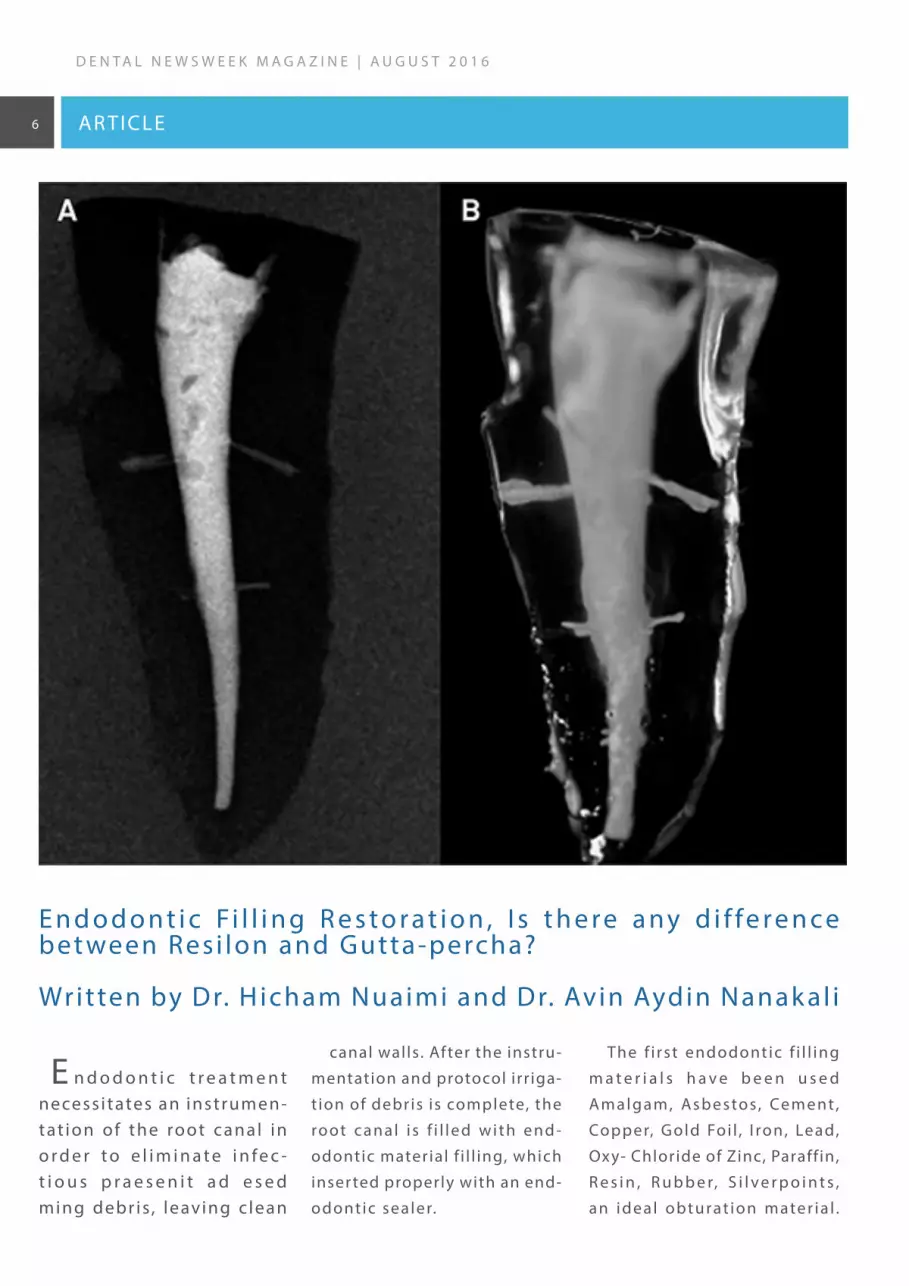
E n d o d o n t i c t r e a t m e n t necess i tates an instrumen-tat ion of the root canal in o r d e r t o e l i m i n a t e i n f e c -t i o u s p r a e s e n i t a d e s e d ming debr is , leaving c lean
canal walls. After the instru-
mentation and protocol irr iga-
t ion of debris is complete, the
root canal i s f i l led with end -
odontic material f i l l ing, which
inser ted properly with an end-
odontic sealer.
The f i rst endodontic f i l l ing
m a t e r i a l s h a v e b e e n u s e d
Amalg am, As be s tos, Cement ,
Copper, Gold Foi l , I ron, Lead,
Oxy- Chloride of Zinc, Paraffin,
R e s i n , R u b b e r, S i l v e r p o i n t s ,
an ideal obturat ion mater ia l .
E n d o d o n t i c Fi l l i n g R e s t o r a t i o n , I s t h e r e a ny d i f fe r e n c e bet ween Resi lon and Gutta-percha?
Written by Dr. H icham Nuaimi and Dr. Avin Aydin Nanak al i
6
D E N T A L N E W S W E E K M A G A Z I N E | A U G U S T 2 0 1 6
D E N T A L N E W S W E E K M A G -A Z I N E | A U G U S T 2 0 1 6
AR TICLE

7
D E N T A L N E W S W E E K M A G A Z I N E | A U G U S T 2 0 1 6
D E N T A L N E W S W E E K M A G -A Z I N E | A U G U S T 2 0 1 6
but none of them seen to be
re q u i re d a s a n i d e a l o b t u r a -
t ion mater ia l .
A c c o r d i n g t o G r o s s m a n ,
R o o t c a n a l f i l l i n g m a t e r i a l
s h o u l d h a v e t h e f o l l o w i n g
charac ter ist ics , (1) :
(1) i t should be easi ly intro -
duced into a root canal
(2) i t should be preferably a
semisol id upon inser t ion and
b e co m e s o l i d a f te r wa rd s ; ( 3 )
i t should seal the canal later-
a l ly as wel l as apical ly
(4) it should not shrink after
being inser ted
(5) i t should be imper vious
to moisture
( 6 ) i t s h o u l d b e b a c t e r i o -
stat ic , or at least not encour-
age bac ter ia l growth
(7) i t should be radiopaque
(8) i t should not sta in tooth
struc ture
( 9 ) i t s h o u l d n o t i r r i t a t e
per iapical t i ssue
(10) i t should be ster i le, or
e a s i l y a n d q u i c k l y s t e r i l i z e d
immediately before inser t ion
canal i f necessar y
b ( 1 1 ) i t s h o u l d b e e a s i l y
removable from the root canal
i f necessar y
Subsequent, scientists discov-
ered (Gutta-percha) as a suit-
able root canal f i l l ing material.
Gutta-percha name is der ived
f rom (GE TAH) that mean gum,
whi le (PER TJA) f rom the name
of the tree in that used it mate -
r ia l . Dr. Wi l l iam Montogmerie,
who was a medica l of f icer in
Indian ser vice. He was the f irst
t o a p p r e c i a t e t h e p o t e n t i a l
of th is mater ia l in London in
1843, (1) .
H o w e v e r , t h e n e e d f o r
improve me nt and g e t t ing an
ideal root canal f i l l ing mate -
r ial propagates during sophis-
t icat ion endodontic therapy.
W h i l e c u r r e n t l y u s e d f i l l i n g
m ate r i a l s s e e m to a f fo rd t h e
p r a c t i t i o n e r s a h i g h l e ve l o f
s u c c e s s a n d l o n g d u r a b i l i t y.
Updating in endodontic f i l l ing
m a te r i a l s , e n d o d o n t i c s e a l e r
a n d t e c h n i q u e s a re c o n t i n u -
ing over this centur y.
R e s i l o n f i l l i n g m a t e r i a l i s a
thermoplastic, polyester poly-
m e r - b a s e d r o o t c a n a l f i l l i n g
mater ia l . Resi lon is composed
o f b i o a c t i v e g l a s s a n d r a d i -
opaque f i l lers .
I ts implementation is similar
to gutta-percha in function, in
addit ion to the same handling
proper t ies (2) .
H o w e v e r, s e v e r a l s t u d i e s
have shown that , whi le us ing
gutta-percha as a f i l l ing resto-
ration, the canal walls may not
b e co m p l e te l y f re e o f d e b r i s
( 2 , 3 ) . S e ve ra l p ro ce d u re s a re
used to remove gutta-percha
by using either hand or rotar y
i n s t r u m e n t s w i t h o r w i t h o u t
heat appl icat ion. I n addit ion,
chemical solvents materials as
chloroform is one of the most
effec t ive procedure for gutta-
p e r c h a r e m o v a l ( 4 ) . c h l o r o -
f o r m s o l v e n t m a t e r i a l h a s
a l s o b e e n r e c o m m e n d e d fo r
the removal of Res i lon f i l l ing
mater ia l .
I n o r d e r t o o b t a i n g o o d
o b t u rat i o n , p ra c t i o n e r s h ave
t o u s e p r o p e r e n d o d o n t i c
sealers l ike :

Resin obturat ion can strengthen the remaining tooth st ruc ture, improv-ing the long-term prognosis for teeth obturated with Res i lon
8
D E N T A L N E W S W E E K M A G A Z I N E | A U G U S T 2 0 1 6
Calc ium hydroxides
Zinc- Oxide Eugenol cements
Glass Ionomer Cements.
Once Resi lon f i l l ing mater ia ls
w e r e i n t r o d u c e d d u r i n g t h e
recent decay, a lot of concern
w a s s t a t e d f o r t h e p r o p e r
o b t u r a t i o n m a t e r i a l t o f i l l
c a n a l s r i v a l e d t o g u t t a - p e r -
c h a . Fo r g u t t a - p e r c h a , p r a c -
t ioners could provide ZOE or
epox y res in root canal sealer.
T h e p r o p e r s e a l e r u s e d f o r
Resi lon is a methacr ylate resin
sealer l ike :
Epiphany, RealSeal , EndoRez
Studies have shown the prop -
e r t i e s o f R e s i l o n e n d o d o n t i c
mater ia l in compare to gutta-
percha restorat ion.
Biocompatibi l i t y
ADA has focused on the c yto -
toxic i t y for se lec t ing a dental
mater ial due to direc t contac t
w i t h h u m a n i t y . S o t h a t i t
s h o u l d n o t n e g a t i ve l y a f fe c t
t h e h o s t s c e l l s fo u n d i n t h e
PDL.
S t u d i e s h a v e s h o w n t h a t
affected the host cel ls. Key J
et .a l , 2006 showed that ef fec t
of R es i lon and g ut t a -pe rcha
o n t h e f i b r o b l a s t c e l l s w e r e
t h e s a m e . W h i l e t h e s e a l e r s
t h a t u s e d m a y p o t e n t i a l l y
h a v e a c y t o t o x i c p o t e n t i a l
w h e n s e t t i n g re a c t i o n s we re
n o t c o m p l e t e . E p i p h a ny w a s
f o u n d t o b e l e s s c y t o t o x i c
than Grossman’s sealer (ZOE-
b a s e d ) . O n t h e o t h e r h a n d
E p i p h a n y w a s f o u n d t o b e
more c ytotoxic than Sealapex,
w h i c h i s c a l c i u m hy d r ox i d e -
b a s e d ( 5 ) . S o u s a e t . a l , 2 0 0 6
s h o w e d t h a t E n d o R E Z p r o -
d u c e d h i g h i n f l a m m a t o r y
r e a c t i o n i n t r a o s s e o u s b o n e
w h e n c o m p a r e d w i t h t h e
o t h e r s e a l e r, w h i l e E p i p h a ny
showed the lowest inf lamma-
t o r y e f fe c t a n d h i g h b i c o m -
patibi lty when compared with
others (6) .
O n e o f t h e m a j o r i d e n t i t y
for success or fa i lure of end -
odontic restorat ion is coronal
l e a k a g e d u e t o i n v a s i v e o f
bac ter ia .
Leak age
M i c ro l e a k a g e re m a i n s o n e
o f t h e m a i n r e a s o n f o r t h e
fa i lure of root canal therapy,
w h e r e v e r t h e c h a l l e n g e h a s
been to achieve a proper seal
b e t we e n e n d o d o nt i c o b t u ra-
t ion mater ia l and interdental
dent ine sur faces.
B a c t e r i a m i g r a t e a p i c a l l y
t h r o u g h c o r o n a l m i c r o l e a k -
age. Khayate et .al , 1993 found
t h a t w h e n r o o t c a n a l f i l l i n g
e x p o s e d t o a r t i f i c i a l a n d
natural sal iva, leak age appear
a n d t h e n b a c t e r i a c o n t a m i -
nate to the root apex (7) . Br ito
et .a l , 2003 demonstrated that
u s i n g o f a n a d h e s i v e s e a l e r
s h owe d s i gn i f i c a nt l y s l ow o r
s top coronal -apica l bac ter ia l
m i g r a t i o n , i n s p i t e o f u s i n g
Gutta-percha (8) .
Te i x e i r a e t . a l , 2 0 0 4 d e m -
o n s t r a t e d t h a t e n d o d o n t i c
s e a l e r s f o r m a c l o s e a d h e -
sion to the intra dentinal wall ,
b u t n o n e i s a b l e t o b o n d t o
t h e g u t t a - p e rc h a co re m a te -
r ia l . Dur ing sett ing of sealer,
s h r i n k a g e a d m i t s t h e s e a l e r
to p u l l away f ro m t h e g u t t a -
p e r c h a m a t e r i a l t h a t l e a d
t o c re a t e a m i c ro g a p, w h i c h
p e r m i t s b a c t e r i a p a s s a p i -
c a l l y ( 9 ) . S h i p p e r e t . a l , 2 0 0 5
f o u n d t h a t u s i n g g u t t a - p e r -
c h a a n d A H - 2 6 s e a l e r h a v e
m o re i n f l a m m ato r y re s p o n s e
AR TICLE

9
D E N T A L N E W S W E E K M A G A Z I N E | A U G U S T 2 0 1 6
compared with Res i lon and
E p i p h a n y . T h e y c o n c l u d e d
t h i s r e s u l t d u e t o t h e s u p e -
r i o r r e s i s t a n c e o f R e s i l o n t o
c o r o n a l m i c r o l e a k a g e ( 1 0 ) .
K u r t z m a n e t . a l , 2 0 0 6 f o u n d
t h a t t e e t h t h a t w e r e o b t u -
r a t e d u s i n g R e s i l o n s h o w e d
s i g n i f i c a n t l e s s s h r i n k a g e i n
c o m p a r e w i t h c o n v e n t i o n a l
Gutta-percha. (11)
Ac c o rd i n g t o t h e p re v i o u s
s t u d i e s , R e s i l o n - E p i p h a n y
s y s t e m w a s r e c o m m e n d f o r
improvement in leak age resis-
tance compared to gutta-per-
cha techniques.
Obturat ion
C a l c i u m h y d r o x i d e h a s
b e e n a d vo c a t e d a s a n i n t r a -
canal medicament whi le end-
o d o n t i c p r o c e d u r e r e q u i r e d
a n e x t r a v i s i t . I t i s r e c o m -
m e n d e d t h a t i r r i g a t i o n w i t h
1 7 % e t h y l e n e d i a m i n e t e t r a -
c i t ic ac id (EDTA) , When obtu-
rat ion is not occurred dur ing
single visit to remove any rem-
nants of the ca lc ium hydrox-
ide. When this technique was
a c h i e v e d i t w a s d i s c o v e r e d
t h a t c a l c i u m h y d r o x i d e d i d
n o t b a d l y a f f e c t t h e s e a l o f
t h e r o o t - c a n a l s y s t e m w i t h
Resi lon(12) . Moreover, dur ing
o b t u r a t i o n p r o c e d u r e s , i t i s
required to use a dis infec t ion
mater ia l as sodium hypochol-
or ite (NaOCl) or chlorhexidine
before obturat ion. I sc i S et .a l ,
2 0 0 6 f o u n d t h a t a 1 - m i n u t e
i m m e r s i o n i n e i t h e r s o l u -
t i o n d i d n o t s h o w a n y s i g -
n i f icant deter iorat ion on the
Resi lon cone’s sur face (13)
N ie lsen et .a l , 2006 showed
t h a t R e s i l o n s e a l e r s e t i n 3 0
minutes in anaerobic environ-
ments (normal ly found in the
canal ) , whi le in a i r i t required
1 week to set , they concluded
that the key of sett ing t ime is
l i m i t i n g ox yg e n i n t h e c a n a l
system(14) .
U s i n g r e s i n o b t u r a t i o n
m a t e r i a l s a re n o t p re fe r a b l e
in most cases due to concern
of retreatment procedure that
m a y o c c u r a f t e r o b t u r a t i o n .
Resi lon obturat ion consists of
a sof t core mater ia l (Res i lon)
with a methacr yl ic resin sealer
( E p i p h a ny ) . d e O l i ve i ra e t . a l ,
2006 showed that the abil ity of
progress ion of a f i le through
t h e R e s i l o n - o b t u r a te d c a n a l .
Essent ia l ly, Resi lon was faster
to remove than gutta-percha
and resulted in c leaner canal
wal ls in the apical third of the
teeth obturated with R es i lon
when compared to gutta-per-
c h a ( 1 5 ) . M a l te zo s e t . a l , 2 0 0 6
found that mineral t r ioxalate
(MTA) does not show a s igni f -
i c a n c e i n b a c t e r i a l l e a k a g e
i n t h e a p i c a l p o r t i o n o f ro o t
when compared with R es i lon
sealer, but Resi lon leaked s ig-
nif icantly less than Super-EBA
(16) So that Res i lon may be a
v iable option as a retrograde -
i l l i n g m a t e r i a l w i t h g o o d
s u r g i c a l i s o l a t i o n a n d m o i s -
ture control .
Physical Proper t ies
E n d o d o n t i c a l l y t r e a t e d
t e e t h h a v e b e e n s t a t e d t o
b e m o re s u b j e c t to f ra c t u re /
cracked because of reduc tion
i n d e n t i n a l t o u g h n e s s , l e s s
w a t e r c o n t e n t , a n d d e e p e r
cavit ies(17) .
S o t h a t d u r a b i l i t y o f e n d -
o d o n t i c a l l y t r e a t e d t e e t h
d u r i n g f u n c t i o n m a k e t h e
t o o t h w i t h d r a w w e a k n e s s ,
w h i c h m a y l e a d t o f r a c t u r e
( 1 8 ) . M i c r o f r a c t u r e s c u r r e n t
p r i o r t o e n d o d o n t i c t h e r a p y
m a y p r o p a g a t e u n d e r l o a d ,
l e a d i n g t o c l i n i c a l l y s i g n i f i -
c a n t c r a c k s t h a t c a n f i n a l l y
lead to the loss of the tooth.
instrumentat ion process lead
t o w e a k e n t h e t o o t h a s t h e
canals by enlarged and dis in-
fect the root canal system(17).
F u r t h e r m o r e , t h e w e a k e s t
por tion of endodontic tooth is
the cer vical aspect due to s ig-
ni f icant compress ive, tensi le,
a n d t o r s i o n a l f o r c e s d u r i n g
f u n c t i o n a n d b r u x i s m t h a t
may lead to the fat igue then
f r a c t u r e . T h e r e f o r e , t h e k e y
element is obturation to assist
i n re i n fo rc i n g t h e re m a i n i n g
tooth struc ture (18) .

10
D E N T A L N E W S W E E K M A G A Z I N E | A U G U S T 2 0 1 6
Refrences
1- Grossman L(1970) : Endodontic Prac t ice, 7th ed, Phi ladelphia : Lea & Febiger Co. , pp. 329-33. 2-Shipper G, Orstavik D, Teixeira F, Trope M
(2004) An evaluation of microbial leak age in roots f i l led with a thermoplast ic synthetic polymer-based root canal f i l l ing mater ial (Resi lon) .
J Endod 30, 342- 347. 3-Fr iedman S , Rotstein I , Shar-Lev S (1989) Bypass ing gutta-percha root f i l l ings with an automated device. J Endod
15, 432-437. 4- Cunha R , De Mar t in A, Barros P, da S i lva F, de Cast i lho Jacinto R , da S i lvei ra Bueno CE (2007) I n v i t ro evaluat ion of the
c leansing work ing t ime and analys is of the amount of gutta-percha or Res i lon remnants in the root canal wal ls af ter instrumentat ion for
endodontic retreatment. J Endod 33, 1426-1428 5-Sousa C, Montes C , Pascon E (2006) Compar ison of the intraosseous biocompatibi l i t y
of AH Plus, EndoREZ, and Epiphany root canal sealers . J Endod;32(7) :656-662. 6-K hayat A, Lee S , Torabinejad M (1993) Human sal iva pen-
etrat ion of coronal ly unsealed obturated root canals . J Endod;19(9) :458-461. 7-Br i t to L , Gr imaudo N, Ver tucci F (2003) Coronal micro -
leak age assessed by polymicrobia l markers. J Contemp Dent Prac t . 2003;4(3) : 1-10. 8-Teixeira F, Teixeira E , Thompson J (2004) Dent inal
bonding reaches the root canal system. J Esthet Restor Dent ;16(6) :348-354. 9-Shipper G, Orstavik D, Teixeira F (2004) An evaluat ion of
microbia l leak age in roots f i l led with a thermoplast ic synthet ic polymer-based root canal f i l l ing mater ia l (Res i lon) . J Endod;30(5) :342-
347. 10-Kur tzman G, von Fraunhofer J , Ol ivei ra D (2006) Endodontic Leak age Resistance of Fiber Obturators. Poster presentat ion AADR,
Or lando, FL , #1443. 11-Wang C, Debel ian G, Teixeira F (2006) Ef fec t of intracanal medicament on the seal ing abi l i t y of root canals f i l led
with Res i lon. J Endod ;32(6) :532-536. Epub 2006. I2- sc i S , Yoldas O, Dumani A (2006) Ef fec ts of sodium hypochlor i te and chlorhexidine
solutions on Resi lon (synthetic polymer based root canal f i l l ing material) cones: an atomic force microscopy study. J Endod;32(10) :967-969.
13-N ielsen B, Beeler W, Vy C , (2006) Sett ing t imes of Res i lon and other sealers in aerobic and anaerobic environments. J Endod;32(2) :130-
132. 14- de Ol iveira D, Barbizam J, Trope M (2006) Compar ison bet ween gutta-percha and res i lon removal us ing t wo di f ferent techniques
in endodontic retreatment. J Endod;32(4) :362-364. 15-Maltezos C , Gl ick man G, Ezzo P (2006) Compar ison of the seal ing of Res i lon, Pro
Root MTA, and Super-EBA as root- end f i l l ing mater ia ls : a bac ter ia l leak age study. J Endod;32(4) :324-327. 16-Madison S , Wi lcox L (1988) An
evaluat ion of coronal microleak age in endodontical ly t reated teeth. Par t I I I . I n v ivo study. J Endod;14(9) :455-458. 17- Gutmann J (1992)
The dent in-root complex : Anatomic and biologic considerat ions in restor ing endodont ica l ly t reated teeth. J Prosthet D ent ;67(4) :458-
467.18-Teixeira F, Teixeira E , Thompson J (2004) Frac ture res istance of roots endodontical ly t reated with a new res in f i l l ing mater ia l . J
Am Dent Assoc;135(5) :646-652.
AR TICLE

11
D E N T A L N E W S W E E K M A G A Z I N E | A U G U S T 2 0 1 6
Replacement of lost teeth
u s i n g o r a l i m p l a n t s i s a n
accepted treatment modality
with wel l documented, h igh
long-term success rates of up
to 90 % at 10-year fo l low up.
Conventional dental implant
strategies that work success-
f u l l y i n d e l a y e d i m p l a n t o l -
ogy have ser ious l imitat ions
re g a rd i n g f u n c t i o n a l i t y a n d
esthetic outcome in immedi-
ate implantology. Although,
I m p l a n t i n d i c a t i o n e x p a n d s
nowadays. The major advan-
tages of immediate implant
p l a c e m e n t a r e t h e r e d u c -
t i o n i n t re at m e nt t i m e w i t h
f e w e r s u r g i c a l i n t e r v e n -
t ions leading to an improved
quality of l i fe and overall cost
re d u c t i o n , a n d m o s t i m p o r-
tant socket preser vat ion due
to ear ly func t ional load.
The main reasons for these
s h o r t c o m i n g s a r e b a s e d o n
t h e f a c t t h at c u r re nt l y ava i l -
able dental implants are cyl in-
d r i c a l a n d m a d e o f t i t a n i u m .
A c t u a l l y, t h e y r e s e m b l e t h e
n a t u r a l ro o t n e i t h e r i n fo r m
n o r i n c o l o r. T h e l a c k o f t h e
c o r re c t f i t i n m o s t i n s t a n c e s
h a s t o b e c o m p e n s a t e d b y
m u l t i p l e c o m p l e x a d d i t i o n a l
t reatments such as bone aug-
m e n t a t i o n , g u i d e d t i s s u e
re g e n e r a t i o n a s we l l a s g u m
p a s t y. S o t h a t , t h e s e p r o c e -
d u r e s a r e t i m e c o n s u m i n g ,
c o s t l y a n d n o t f u l l y p re d i c t -
a b l e . T h e n a t u r a l e x t r a c t i o n
s o c k e t r e p r e s e n t s t h e i d e a l
a n a t o m y a n d s t a r t i n g p o i n t
f o r a r o o t f o r m e d i m p l a n t .
The anato mic bone s i t uat ion
is ideal for the absorpt ion of
the load of a root analogue
i m p l a n t . I n a d d i t i o n , t h e
c y l i n d r i c a l i m p l a n t s d o n o t
f i t at a l l , that leads to a hor-
i zo n t a l a n d ve r t i c a l a t ro p hy.
I n m a ny c a s e s t h e a t ro p h i e d
b o n e e s p e c i a l l y i n t h e p re s -
e nce of t h in s of t t i s s ue does
n o t s h o w e s t h e t i c a p p r o a c h
because of the grayish gingiva
or even vis ible implant shoul -
d e r s . T h e s e c o m p l i c a t i o n s
m a y o c c u r w i t h i n d a y s a f t e r
implantat ion or af ter years in
t h e co n te x t o f o l d a g e i nvo -
l u t i o n . A c o r r e c t i o n o f t h i s
f a i l u re re q u i re s a n u m b e r o f
invasive procedures as Guided
t issue regeneration, which are
quest ionable outcome, there -
fore i t i s advisable to use root
c o l o re d i m p l a n t s . D i s p l a y o f
different dental implant forms
c l e a r l y i n d i c a t e s t h a t O s s e o
i nte grat i o n d o e s n o t p r i m a r-
i l y d e p e n d o n t h e f o r m o f
t h e i m p l a n t . I n a d d i t i o n t o
sur face t reatment of implant ,
i t i s i m p o r t a n t t o p r e p a r e
t h e i m p l a n t s i te i n a n a t ra u-
matic way in order to achieve
a p e r f e c t b o n e t o i m p l a n t
contac t .
T h e r e i s a b s o l u t e l y n o
l o g i c a l r e a s o n a t a l l n o t t o
use the already exist ing intact
t o o t h s o c k e t a s i m p l a n t s i t e
a n d t o a d a p t t h e i m p l a n t t o
the tooth socket instead of the
vice versa approach including
d r i l l i n g , b o n e t r a u m a , b o n e
loss and adit ional bond
3 D A N ATO M I C A L Z I R CO N I A I M P L A N T wr i t ten by Prof Al f red Kocher and Dr. Pi rker

12
D E N T A L N E W S W E E K M A G A Z I N E | A U G U S T 2 0 1 6
A n o t h e r r e a s o n f o r t h e
h i g h r e g e n e r a t i v e p o t e n -
t i a l o f s p o n g y b o n e l i e s i n
i ts ex tens ive vascular izat ion.
Retent ions in the area of the
thin cor t ica l bone leads i r re -
v o c a b l e t o f r a c t u r e s , s o m e -
t i m e s a t r e m o t e s i t e s , w i t h
s u b s e q u e n t b o n e r e c e s s i o n .
I n o r d e r t o b e o n t h e s a f e
s i d e a n d a v o i d f r a c t u r e o f
the th in cor t ica l bone at any
c o s t , t h e i m p l a n t i s re d u c e d
at the buccal and l ingual face
by approximately 0 .1–0.2mm.
T h e p r i n c i p l e o f d i f f e r e n t i -
ated Osseo integrat ion there -
fo r e d i c t a t e s t h e i n n o v a t i v e
i m p l a n t d e s i g n . I n a r e a s
w i t h o u t m a c r o r e t e n t i o n s
n o f r a c t u r e o r i m p r e s s i o n
i n d u c e d r e s o r p t i o n t a k e s
place and pr imar y Osseo inte -
grat ion occurs without delay.
What are the advantages of
the novel implant?
No bone dr i l l ing equals no
o p e r a t i v e t r a u m a , n o b o n e
l o s s , n o d a m a g e t o n e i g h -
b o r i n g s t r u c t u r e s i n c l u d i n g
dental roots, mandible ner ve,
o r m a x i l l a r y s i n u s. Th e ex a c t
f i t o f t h e i m p l a n t l e a d s t o
a n o p t i m i z e d i m p l a n t - b o n e
contac t sur face with maximal
pr imar y stabi l i t y.
A l l a t t e m p t s i n t h e l o n g
h i s t o r y o f d e n t a l s c i e n c e t o
f ix homologue, heterologous
o r a l l o g e n e i c r o o t a n a l o g u e
i m p l a nt s i nto a f re s h e x t ra c -
t ion socket fa i led due to the
c o n i c a l r o o t f o r m , r e j e c t i o n
a n d l a c k o f p r e c i s e n e s s a n d
w e r e t h e r e f o r e n o t e s t a b -
l ished. With the implementa-
t ion of the modern CAD/CAM
t e c h n o l o g y i t b e c a m e e a s i l y
p o s s i b l e t o m a n u f a c t u r e a n
exac t copy of the dental root .
I s t h e r e a n y d i f f e r e n c e i n
Osseo integrat ion?
I t i s not only to reconstruc t
t h e a n a t o my o f t h e i n d i v i d -
ual tooth, but i t i s poss ible to
consider the under ly ing bone
quantity and qual ity. This way
t h e s u r f a c e o f t h e i m p l a n t
c a n b e m o d i f i e d a c c o r d -
ingly. M acro -retent ions (pro -
t r u s i o n s ) a re a c o n d i t i o n fo r
t h e s a f e f i x a t i o n o f a r o o t -
formed and therefore conical
i m p l a n t i n t h e b o n e. M a c ro -
re t e n t i o n s h ave t o b e f i r m l y
l imited to spongy bone, s ince
only spongy bone can absorb
p re s s u re w i t h o u t f r a c t u re a t
a remote s i te. M icro f rac tures
cannot be avoided, but in con-
t r a s t t o f r a c t u re s o f c o r t i c a l
bone fractures in spongy bone
re m a i n l i m i te d w i t h re d u ce d
d a m a g e a n d q u i c k r e g e n e r -
a t i o n d u e t o t h e e x c e l l e n t
b l o o d s u p p l y a l ways p re s e nt
in spongy bone.
AR TICLE

13
D E N T A L N E W S W E E K M A G A Z I N E | A U G U S T 2 0 1 6
In the past thir ty-f ive years,
I have encountered hundreds
o f p a t i e n t s w h o w e r e p e t -
r i f i e d o f s i t t i n g i n a d e n t a l
c h a i r. W h e n I re f l e c t o n t h i s
population of fear ful patients,
they a l l seem to have a fa i r ly
c o n s i s t e n t p r o f i l e . T h e y a r e
most ly above the age of f i f t y
y e a r s o l d , t h e y o f t e n h a v e
ser ious dental needs and they
a l m o s t u n i ve r s a l l y c a n re c a l l
o n e o r m u l t i p l e t r a u m a t i c
v is i ts to the dentist as a chi ld.
The memor y of the t rauma or
t r a u m a s h a s / h a v e , i t w o u l d
seem, left an indelible imprint
which is diff icult , i f not impos-
s i b l e t o e n t i r e l y e x p u n g e .
Fi f t y years ago, dentists of ten
t r e a t e d y o u n g p a t i e n t s l i k e
s m a l l a d u l t s . A n d , w h e n t h e
child’s response to unpleasant
o r u n u s u a l e x p e r i e n c e s
was fear or poor control , the
d e n t i s t o f t e n b e c a m e f r u s -
trated, or impatient , or, in the
e x t r e m e , b r u t a l . T h a n k f u l l y,
t h i s c l i n i c a l a p p r o a c h h a s
become increasingly rare. The
specialty of pediatric dentistr y
has produced a group of den-
t ists who have been taught to
ef fec t ively and appropr iately
t r e a t c h i l d r e n . T h e r e s u l t i s
a m o d e r n d e n t a l p o p u l a t i o n
which v iews denta l care as a
st ress- f ree ac t iv i t y. The chi ld
w i t h m e m o r i e s o f t r a u m a t i c
dental care becomes an adult
w h o b e c o m e s , u n d e r s t a n d -
a b l y, o n e w h o avo i d s d e n t a l
t reatment. This avoidance, in
many cases, leads to increas-
i n g l y g r e a t e r d e n t a l n e e d s .
Through the years, I have seen
a n u m b e r o f p a t i e n t s w h o
have not had a rout ine dental
v i s i t i n ove r t we n t y ye a r s . I f
i t were not for ex treme pain ,
or an inabi l i t y to chew ef fec-
t i v e l y, o r a s e r i o u s e s t h e t i c
p r o b l e m , t h e y w o u l d n e v e r
h a v e a r r i v e d a t my o f f i c e a t
al l . So how does one begin the
conve r s ion of t he de ntopho -
b i c i nto o n e w h o vo l u nt a r i l y
s e e k s a n d i s a b l e t o s u s t a i n
d e n t a l c a re ? We l l , a l l fe a r f u l
dental pat ients seem to have
a c o n c e r n t h a t t h e y w i l l b e
hur t in the chair and that they
have l imited abi l i t y to stop i t .
S o, the f i rst step is to demon-
strate to a pat ient that dental
care can be del ivered without
d i s c o m f o r t . I n o r d e r t o d o
th is , moder n dent ist r y of fers
a n u m b e r o f p a i n c o n t r o l
s t r a t e g i e s . Lo c a l a n e s t h e t i c s
(Novocain) have been around
s i n c e t h e 1 9 5 0 ’s . I n t h e p a s t
s i x d e c a d e s , t h o s e s e n s at i o n
blockers, and the techniques
of deliver y, have become more
ef fec t ive. N itrous oxide anal -
gesic (sweet air, laughing gas)
i s a useful adjunc t for dental
c a r e f o r t h e f e a r f u l p a t i e n t .
N i t r o u s o x i d e g a s i s m i x e d
w i t h o x y g e n a n d d e l i v e r e d
t h r o u g h a n o s e p i e c e . T h e
precise way this gas works is
n o t e nt i re l y u n d e r s to o d, b u t
when i t i s breathed, i t causes
re l a x at i o n a n d a te m p o ra r i l y
altered perception of unpleas-
ant st imul i .
D E N TO P H O B I A “ T H E O N LY T H I N G W E HAVE TO FEAR IS FEAR ITSELF.” BY ROBERT A. HERSH, DDS
14
D E N T A L N E W S W E E K M A G A Z I N E | A U G U S T 2 0 1 6
I h a ve fo u n d t h a t s t a r t i n g
t reatment wit h s hor t , s imple
procedures is helpful. As trust
i s d e v e l o p e d , l o n g e r, m o r e
complex procedures are more
e a s i l y t o l e r a t e d . T h e f e a r f u l
p a t i e n t s l o w l y u n d e r g o e s a
convers ion into a pat ient tol -
erant of dental care. S o why,
one must wonder, am I preach-
i n g t o t h e c h o i r ? A f t e r a l l ,
p a t i e n t s r e a d i n g t h i s n e w s -
letter have demonstrated an
O n c e t h e n i t r o u s o x i d e i s
f l u s h e d o u t , b y b r e a t h i n g
s t r a i g h t ox yg e n , t h e a l t e re d
state i s quick ly reversed and
t h e p a t i e n t c a n d r i v e a w a y
without res idual ef fec ts.
Sedation techniques such as
tak ing Valium prior to a dental
vis it is another effective strat-
egy for some. Val ium seems to
produce a calming effect prior
to a dental visit . Unlike nitrous
oxide however, Val ium, whi le
rather shor t ac t ing, cannot be
r e v e r s e d . Pa t i e n t s w h o t a k e
Val ium pr ior to a dental v is i t
should be dr iven to and f rom
the dental of f ice. I n the past
f e w y e a r s , a n e w t e c h n i q u e
c a l l e d “ S e d a t i o n D e n t i s t r y ”
h a s r e c e i v e d a l o t o f p u b -
l i c i t y . S e d a t i o n d e n t i s t r y
i n v o l v e s t a k i n g a s e d a t i o n
drug cal led Tr iazolan pr ior to
the dental v is i t . This drug has
a number of ef fec ts inc luding
a c h e m i c a l l y i n d u c e d s l e e p -
l i k e p e r i o d w h i l e t h e d e n -
t istr y is per formed. Whi le this
drug has a fa i r ly good safet y
record, patients must be mon-
itored dur ing and af ter tak ing
t h e d r u g b e c a u s e o f d o c u -
m e n t e d i n s t a n c e s o f s l e e p
w a l k i n g , s l e e p d r i v i n g a n d
trance - l ike behavior. Perhaps
the most effective mechanism
for helping the fear ful patient
is to establ ish t rust .
a b i l i t y t o r o u t i n e l y p a r t i c -
i p a t e i n d e n t a l c a r e . We l l ,
m a n y p a t i e n t s p r o b a b l y
k now fr iends or re lat ives who
n e e d c a re, b u t w h o s e d e nt a l
p h o b i a s p r e v e n t t h e m f r o m
gett ing help. This may be an
oppor tunit y to ass ist them in
el iminating pain or improving
their abi l i t y to eat or to help
t h e m t o l o o k b e t t e r. W h a t a
k ind gesture!
a
AR TICLE

15
D E N T A L N E W S W E E K M A G A Z I N E | A U G U S T 2 0 1 6

OZONE THERAPY – AN ALTERNATIVE TO CONVENTIONAL THERAPY IN PEDIATRIC DENTISTRY BY Dr. Sushma Gojanur.
T h e w o r d o z o n e i s d e r i v e d
f r o m t h e G r e e k “ o z e i n ”
meaning odorant . Ozone is a
t r i a t o m i c m o l e c u l e c o n s i s t -
i n g o f t h r e e o x y g e n a t o m s
w i t h a m o l e c u l a r w e i g h t o f
4 7 , 9 8 g / m o l 1 . Ozo n e i s t h e r-
modynamical ly h ighly unsta-
b l e c o m p o u n d w h i c h d i s s o -
c iates readi ly back to ox ygen
and s inglet ox ygen which is a
strong oxidizing agent quick ly
re n d e r i n g v a r i o u s b e n e f i c i a l
e f fe c t s . I t i s a b l u e g a s, w i t h
a s t r o n g o d o r a n d a b s o r b s
t h e h a r m f u l u l t r a v i o l e t r a y s
present in the l ight spec trum
from the sun and protec ts the
l iving creatures from the ultra-
violet rays. Ozone therapy can
be def ined as a versat i le bio -
o x i d a t i v e t h e r a p y i n w h i c h
oxygen/ozone is administered
v ia gas or d issolved in water
or oi l base to obtain therapeu-
t ic benef its . I nterest of Ozone
use in medic ine and dent istr y
i s d u e t o i t s a n t i - m i c r o b i a l ,
d i s i n f e c t a n t , b i o c o m p a t i b i l -
i t y and heal ing proper t ies.
Mechanism of ac t ion:
T h e r e a r e s e v e r a l a c t i o n s
h e a l i n g , i m p r o v e d o x y g e n
o f ozo n e s u c h a s a nt i - m i c ro -
bia l , ant i - inf lammator y, anal -
g e s i c , i m m u n e s t i m u l a t -
i n g, a n t i - hy p ox i c , d e t ox i c a t -
i n g , b i o - e n e r g e t i c a n d b i o -
s y n t h e t i c ( a c t i v a t i o n o f t h e
metabol ism of carbohydrates,
proteins & l ip ids) ac t ions2.
Mode of ac t ion: Ozone gas :
T h e r e a r e t h r e e d i f f e r e n t
systems for generat ing ozone
i . Ultraviolet system i i . Corona
D i s c h a r g e s y s t e m i i i . C o l d
p l a s m a s y s t e m . S o m e o f t h e
commercial ly avai lable Ozone
U n i t s a r e : H e a l O z o n eT E C 3
( C u r o z o n e , U S A ) , P r o z o n e
( W&H) , oz icure ozone device.
Ozone aqueous solut ion: The
fol lowing proper t ies of ozone
a r e u s e d : d i s i n f e c t a n t a n d
ster i l iz ing effec t , haemostatic
e f fe c t , e s p e c i a l l y i n c a s e s o f
h e m o r r h a g e s a c c e l e r a t e d
16
D E N T A L N E W S W E E K M A G A Z I N E | A U G U S T 2 0 1 6
AR TICLE

supply and suppor t of meta-
bol ic processes.
O zo n e o i l : O zo n a te d o i l s a re
p u re p l a n t e x t r a c t s , t h ro u g h
which pure ox ygen and ozone
are passed. The plant ex trac ts
u n d e rg o a c h e m i c a l re a c t i o n
t o fo r m a t h i c k , v i s c o u s o i l ,
or in some cases, a petroleum
j e l l y - l i k e p r o d u c t . T h e f i n a l
p r o d u c t s c o n t a i n o z o n i d e s .
This method of external appli-
cat ion is harmless.
Cl in ical appl icat ions :
Pre ve nt i o n a n d m a n a g e m e nt
of dental car ies : The appl ica-
t ion of Ozone therapy in the
management of dental car ies
i s widely studied. Most of the
c h i l d p a t i e n t s h ave fe a r a n d
anxiet y towards dental t reat-
ment. Dahnhar t JE et a l4 eval-
u a t e d t h e a n x i e t y l e v e l o f
c h i l d r e n ( a n d t h e i r p a r e n t s )
t reated with ozone and found
t h a t a l l c h i l d r e n & p a r e n t s
r e p o r t e d s i g n i f i c a n t a n x i e t y
p r i o r t o o z o n e t r e a t m e n t .
However, fo l lowing the t reat-
m e n t , t h e c h i l d r e n r e p o r t e d
t h e y w o u l d b e p l e a s e d t o
re t u r n fo r f u t u re t re at m e nt s .
Also, 80% of the parents sa id
they would be wi l l ing to pay
m o r e f o r t h i s t h e r a p y c o m -
p a r e d w i t h t r a d i t i o n a l d r i l l -
ing and f i l l ing. Huth et al5 ran
a spl i t mouth c l in ica l t r ia l to
assess the effect of a s ingle 40
second application of gaseous
o z o n e o n n o n c a v i t a t e d
f issure car ies in permanent
m o l a r s . Th e ozo n e - t re ate d
t e e t h s h o w e d r e d u c e d
c a r i e s p r o g r e s s i o n w h e n
compared to the untreated
c o n t r o l l e s i o n s i n t h e s e
s a m e p a t i e n t s . K r o n u s o v a
M6 found that Ozone treat-
ment e i ther a lone or com-
b i n e d w i t h a r e m i n e r a l i z -
i n g s o l u t i o n w a s fo u n d t o
b e e f f e c t i v e f o r r e m i n e r -
a l i z a t i o n o f i n i t i a l f i s s u r e
c a r i e s l e s i o n s . O z o n e h a s
b e e n s h o w n t o r e v e r s e
p i t a n d f i s s u r e s c a r i e s i n
deciduous teeth7. Ozone is
a l s o fo u n d to b e e f fe c t i ve
against the microflora asso -
c i a t e d w i t h p r i m a r y r o o t
car ies lesion8. I t a lso oxides
volati le sulphur compounds
precursor methionine to i ts
c o r re s p o n d i n g s u l p h ox i d e
and thus prevents malodor
associated with root car ies.
T h e m e c h a n i s m o f a c t i o n
i s d u e to i t s a n t i m i c ro b i a l
p r o p e r t i e s a n d i t s a b i l i t y
t o o x i d i z e t h e b a c t e r i a l
ce l l wal l . Pyruvic ac id that
is produced by bacteria and
i m p l i c ate d i n t h e p ro gre s -
s i o n o f c a r i e s i s o x i d i z e d
b y O z o n e t o a c e t a t e a n d
carbon dioxide. Ozone gen-
erating equipment conver ts
oxygen to ozone. The ozone
is thereaf ter led to a hand
piece f i t ted with a s i l icone
cup. sur faces. This ensures
c lose contac t bet ween
t h e s i l i c o n e c u p a n d t h e
c a r i o u s a r e a o f t h e t o o t h
s o t h a t t h e o z o n e d o e s
n o t e s c a p e . T h e o z o n e i s
l e d t h r o u g h t h e s i l i c o n e
c u p o v e r t h e t o o t h f o r a
m i n i m u m o f 1 0 s e c o n d s .
T h e o z o n e i n t h e s i l i c o n e
cup is col lec ted again and
re c o nve r t e d t o ox yg e n b y
the apparatus.
Management of Periodontal
diseases: Studies found that
o z o n a t e d w a t e r s t r o n g l y
i n h i b i t e d t h e f o r m a t i o n
o f d e n t a l p l a q u e a n d w a s
h i g h l y e f f e c t i v e i n k i l l i n g
o f b o t h gra m p o s i t i ve a n d
g r a m n e g a t i v e m i c r o o r -
g a n i s m s 9 . Ozo n ate d wate r
c a n b e u s e d i n t h e u l t r a -
s o n i c wate r re s e r vo i r, a l s o
a s a p r e t r e a t m e n t r i n s e
b e fo r e s c a l i n g, r o o t p l a n -
ning and the sulc i , pockets
are i r r igated us ing syr inge
a n d c a n u l a i n n o n s u r g i -
c a l p o c k e t c u re t t a g e. T h i s
p r o c e s s w i l l r e d u c e t h e
i n i t i a l p a t h o g e n i c l o a d o n
the pat ient local ly and sys-
temical ly. Af ter t reatment ,
e a c h p o c k e t & s u l c u s i s
insuff lated with ozone gas
w h i c h d i r e c t l y g o e s i n t o
t issues, ster i l iz ing the area.
The pat ients are a lso given
ozonated o i l to apply top -
i c a l l y t o t h e s o f t t i s s u e .
Huth et a l10 in their study
declared that the aqueous
form of ozone, as a potential
17
D E N T A L N E W S W E E K M A G A Z I N E | A U G U S T 2 0 1 6

a n t i s e p t i c a g e n t , s h o w e d
l e s s c y t o t o x i c i t y t h a n
g a s e o u s o z o n e o r e s t a b -
l ished antimicrobials under
m o s t c o n d i t i o n s . D h i n g r a
et a l11 proposed that sub -
g i n g i v a l o z o n e i r r i g a t i o n
c a n b e p e r f o r m e d d u r i n g
m o n t h l y v i s i t s o n o r t h -
odontic pat ients to reduce
s u b g i n g i v a l i n f l a m m a t i o n
because of plaque retentive
or thodontic appl iances.
Dis infection of the infected
r o o t c a n a l s : O z o n e w a s
f o u n d t o b e e f f e c t i v e
against endodontic patho -
g e n i c m i c ro o rg a n i s m s l i k e
E . Fa e c a l i s , C a n d i d a a l b i -
c a n s , Pe p t o s t r e p t o c o c c u s
m i c r o s a n d Ps e u d o m o n a s
a e r u g i n o s a d i s i n f e c t i n g
o f r o o t c a n a l s a n d d e n -
t inal tubules12. Ozone wi l l
a lso penetrate through the
a p i c a l fo r a m e n a n d e n te r -
i n t o t h e s u r r o u n d i n g a n d
s u p p o r t i v e b o n e t i s s u e
e n c o u r a g i n g h e a l i n g &
regenerat ion of bone.
B l e a c h i n g o f d i s c o l o r e d
teeth: Crown discolorat ion
i s o n e o f t h e m a j o r a e s -
thetic problem in root canal
t r e a t e d t e e t h . Te e t h w h i t -
e n i n g c a n b e d o n e u s i n g
ozone gas due to i ts st rong
oxidiz ing proper t ies.
Desensit ization of sensit ive
teeth:
Ozone removes smear layer,
o p e n s u p t h e d e n t i n a l
t u b u l e s , b r o a d e n s t h e i r
d iameter and then calc ium
and f luor ide ions f low into
t h e t u b u l e s e a s i l y, d e e p l y
a n d e f f e c t i v e l y t o p l u g
t h e d e n t i n a l t u b u l e s , p re -
vent ing the f lu id exchange
through these tubules fo l -
l o w e d e x p o s e d d e n t i n e
repet i t ive manner 15.
Wo u n d h e a l i n g : Th e i n f l u -
e n c e o f o z o n i z e d w a t e r
o n t h e e p i t h e l i a l w o u n d
heal ing process in the oral
c a v i t y w a s o b s e r v e d b y
Fi l i p p i 1 6 . O zo n e h a s b e e n
repor ted to accelerate the
healing of soft t issue condi-
t ions i .e . : aphthous ulcers ,
h e r p e s l a b i a l i s , A N U G a n d
o t h e r g i n g i v a l i n f e c t i o n s
because ozone encourages
p hy s i o l o g i c a l h e a l i n g r a t e
as wel l as control oppor tu-
nist ic infec t ions.
Contraindications: Ozone is
co n t r a i n d i c a te d i n ce r t a i n
m e d i c a l c o n d i t i o n s l i k e
pregnancy, glucose -6-phos-
p h a te d e hyd ro g e n a s e d e f i -
c i e n c y ( f a v i s m ) , r e c e n t
m y o c a r d i a l i n f a r c t i o n ,
h y p e r t h y r o i d i s m , s e v e r e
anemia, severe myasthenia,
hemorrhage, acute a lcohol
i n t o x i c a t i o n a n d o z o n e
a l lergy3
O z o n e To x i c i t y : O z o n e
w a s r e p o r t e d t o c a u s e
c e r t a i n s i d e e f f e c t s l i k e
e p i p h o r a , u p p e r r e s p i r a -
to r y t r a c t i r r i t a t i o n , r h i n i -
t is , cough, headache, occa-
s i o n a l n a u s e a , v o m i t i n g ,
shor tness of breath, b lood
vessel swel l ing, poor c i rcu-
lat ion, hear t problems and
at t imes stroke3. Because of
i ts ex treme oxidant capac-
i t y, good ozone hygiene is
required.
Conclus ions :Due to proven
t h e ra p e u t i c a d va nt a g e s o f
ozo n e i t i s u s e d i n a l m o s t
a l l a s p e c t s o f d e n t i s t r y .
Ozone therapy al lows a new
vision, which complies with
needs and demands of the
p u b l i c f o r n o n - i n v a s i v e ,
e f f e c t i v e d e n t a l c a r e a n d
i t i s t ru ly a paradigm shi f t
i n d e n t a l p r a c t i c e . O z o n e
t h e r a p y h a s o p e n e d n e w
vistas in t reatment modal -
i t i e s f o r d e n t a l p a t i e n t s
o f a l l a g e s a n d a p p l i c a b l e
t o a w i d e r a n g e o f c o n d i -
t ions of intra ora l hard and
sof t t i ssues. I t i s especia l ly
s u i t a b l e t o t h e p e d i a t r i c
pat ie nt s who f ind conven -
t ional t reatment unaccept-
a b l e . Fu r t h e r r e s e a r c h i s
needed to standardize indi-
cat ions and treatment pro -
c e d u r e s o f o z o n e t h e r a p y
which would br ing a revo -
lut ion in dental prac t ice in
near future.
18
D E N T A L N E W S W E E K M A G A Z I N E | A U G U S T 2 0 1 6
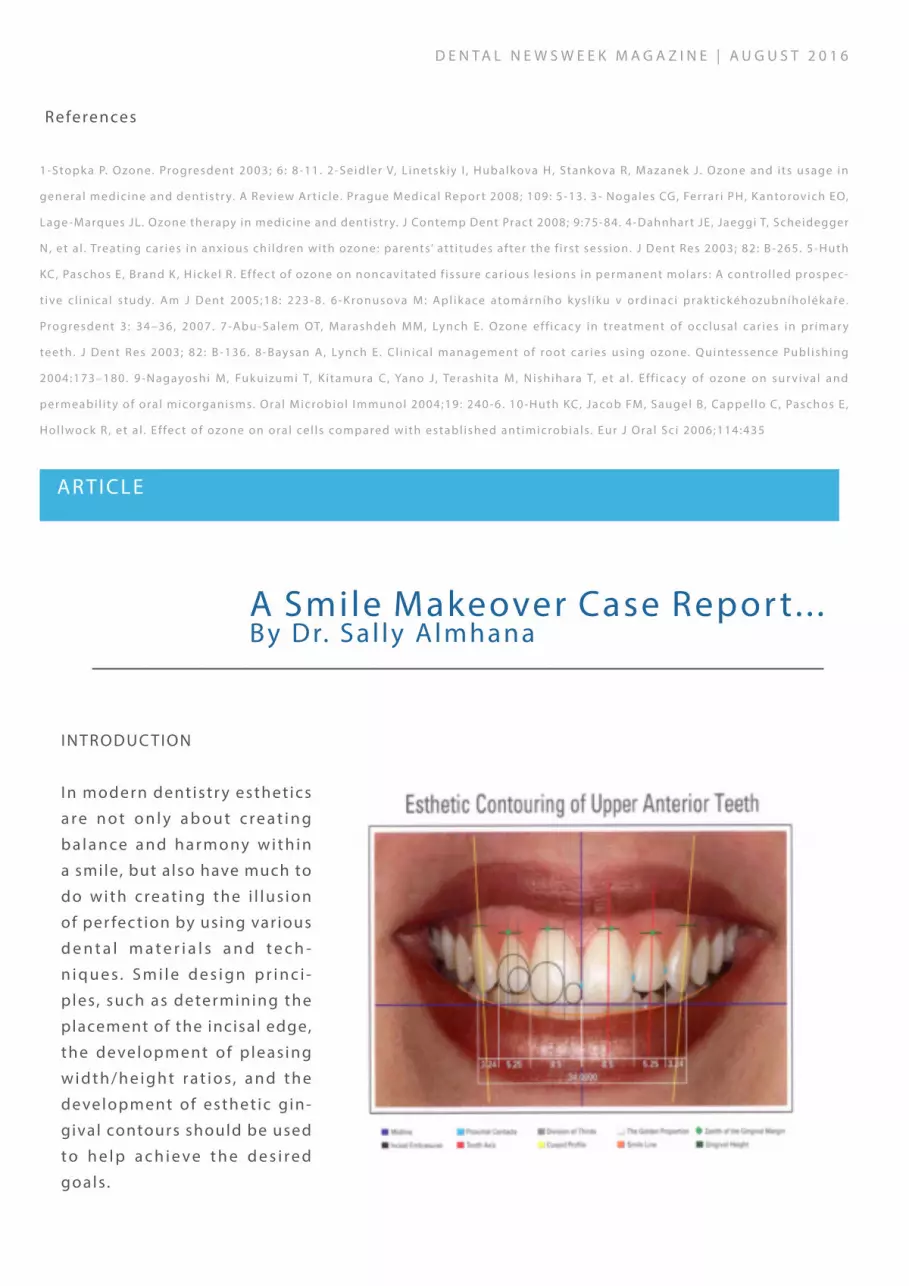
INTRODUC TION
I n modern dent istr y esthet ics
a r e n o t o n l y a b o u t c r e a t i n g
b a l a n ce a n d h a r m o ny w i t h i n
a smile, but also have much to
d o w i t h c re at i n g t h e i l l u s i o n
of per fection by using var ious
d e n t a l m a t e r i a l s a n d t e c h -
n i q u e s . S m i l e d e s i g n p r i n c i -
ples, such as determining the
placement of the incisal edge,
the development of p leas ing
w i d t h / h e i g h t r a t i o s , a n d t h e
development of esthet ic gin-
gival contours should be used
t o h e l p a c h i e v e t h e d e s i r e d
goals .
A Smile Makeover Case Repor t. . .By Dr. Sa l ly Almhana
References
1-Stopk a P. Ozone. Progresdent 2003; 6 : 8-11. 2-Seidler V, L inetsk iy I , Hubalkova H, Stankova R , Mazanek J . Ozone and i ts usage in
general medic ine and dentistr y. A Review Ar t ic le. Prague Medical Repor t 2008; 109: 5-13. 3- Nogales CG, Ferrar i PH, K antorovich EO,
Lage -Marques JL. Ozone therapy in medicine and dentistr y. J Contemp Dent Pract 2008; 9:75-84. 4-Dahnhar t JE, Jaeggi T, Scheidegger
N, et a l . Treat ing car ies in anxious chi ldren with ozone: parents’ att i tudes af ter the f i rst sess ion. J Dent Res 2003; 82 : B-265. 5-Huth
KC, Paschos E , Brand K , H ickel R . Ef fec t of ozone on noncavitated f issure car ious les ions in permanent molars : A control led prospec-
t ive c l in ica l s tudy. Am J Dent 2005;18: 223-8 . 6-K ronusova M: Apl ik ace atomárního k ys l íku v ordinaci prakt ickéhozubníholék aře.
Progresdent 3 : 34–36, 2007. 7-Abu-Salem OT, M arashdeh MM, Lynch E . Ozone ef f icac y in t reatment of occlusal car ies in pr imar y
teeth. J Dent Res 2003; 82 : B-136. 8-Baysan A, Lynch E . C l in ical management of root car ies us ing ozone. Quintessence Publ ishing
2004:173–180. 9-Nagayoshi M, Fukuizumi T, K i tamura C, Yano J , Terashita M, N ishihara T, et a l . E f f icac y of ozone on sur vival and
permeabi l i t y of ora l micorganisms. Oral M icrobiol I mmunol 2004;19: 240-6 . 10-Huth KC, Jacob FM, Saugel B, Cappel lo C , Paschos E ,
Hol lwock R , et a l . E f fec t of ozone on oral cel ls compared with establ ished ant imicrobia ls . Eur J Oral Sc i 2006;114:435
AR TICLE
D E N T A L N E W S W E E K M A G A Z I N E | A U G U S T 2 0 1 6
GOALS OF SMILE DESIGNING
Th e m a i n g o a l o f a n e s t h e t i c
m a k e o v e r i s t o d e v e l o p a
p e a ce f u l a n d s t a b l e m a s t i c a -
tor y system, where the teeth,
tissues, muscles, skeletal struc-
t u r e s a n d j o i n t s a l l f u n c t i o n
in harmony (Peter Dawson) . I t
i s v e r y i m p o r t a n t t h a t w h e n
planning treatment for esthet-
ics cases, smi le design cannot
b e i s o l a t e d f r o m a c o m p r e -
h e n s i v e a p p r o a c h t o p a t i e n t
c a re . Ac h i e v i n g a s u c c e s s f u l ,
heal thy and func t ional resul t
requires an understanding of
t h e i n t e r r e l a t i o n s h i p a m o n g
a l l the suppor t ing ora l s t ruc -
t u re s , i n c l u d i n g t h e m u s c l e s ,
bones, jo ints, gingival t i ssues
and occlus ion.
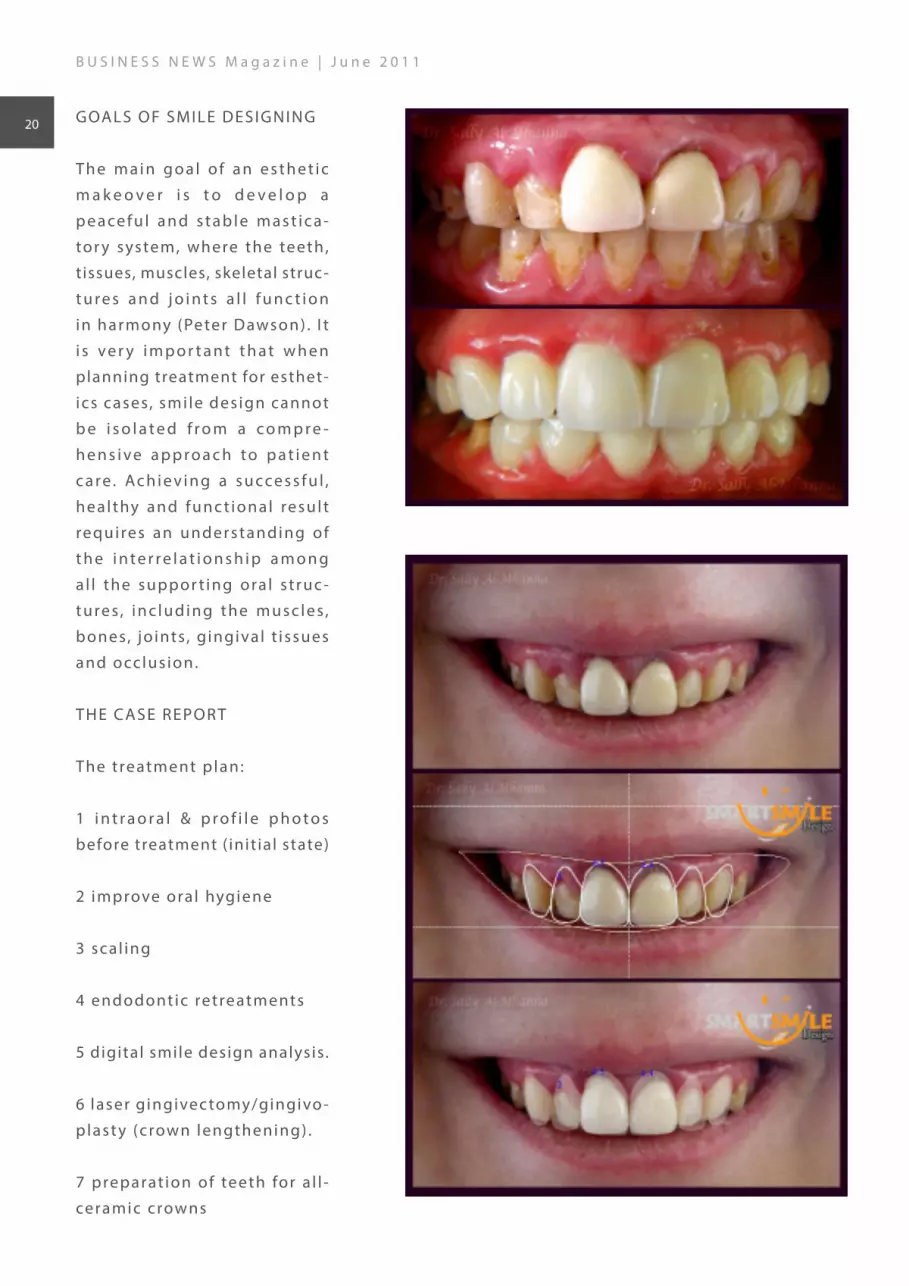
THE CASE REPOR T
The treatment plan:
1 i n t r a o r a l & p r o f i l e p h o t o s
before treatment ( init ial state)
2 improve oral hygiene
3 scal ing
4 endodontic retreatments
5 digital smile design analysis.
6 laser gingivec tomy/gingivo -
plast y (crown lengthening) .
7 preparat ion of teeth for a l l -
ceramic crowns
B U S I N E S S N E W S M a g a z i n e | J u n e 2 0 1 1
20

8 the impress ion
9 c h o o s e b l e a c h 3 a s a m a i n
color and give i t more natural
ef fec ts
1 0 c e m e n t a t i o n o f c r o w n s
using 3M opaque resin cement.
1 1 p i c t u r e s o f f i n a l r e s u l t -
af ter t reatment.
B U S I N E S S N E W S M a g a z i n e | J u n e 2 0 1 1
21
22
D E N T A L N E W S W E E K M A G A Z I N E | A U G U S T 2 0 1 6
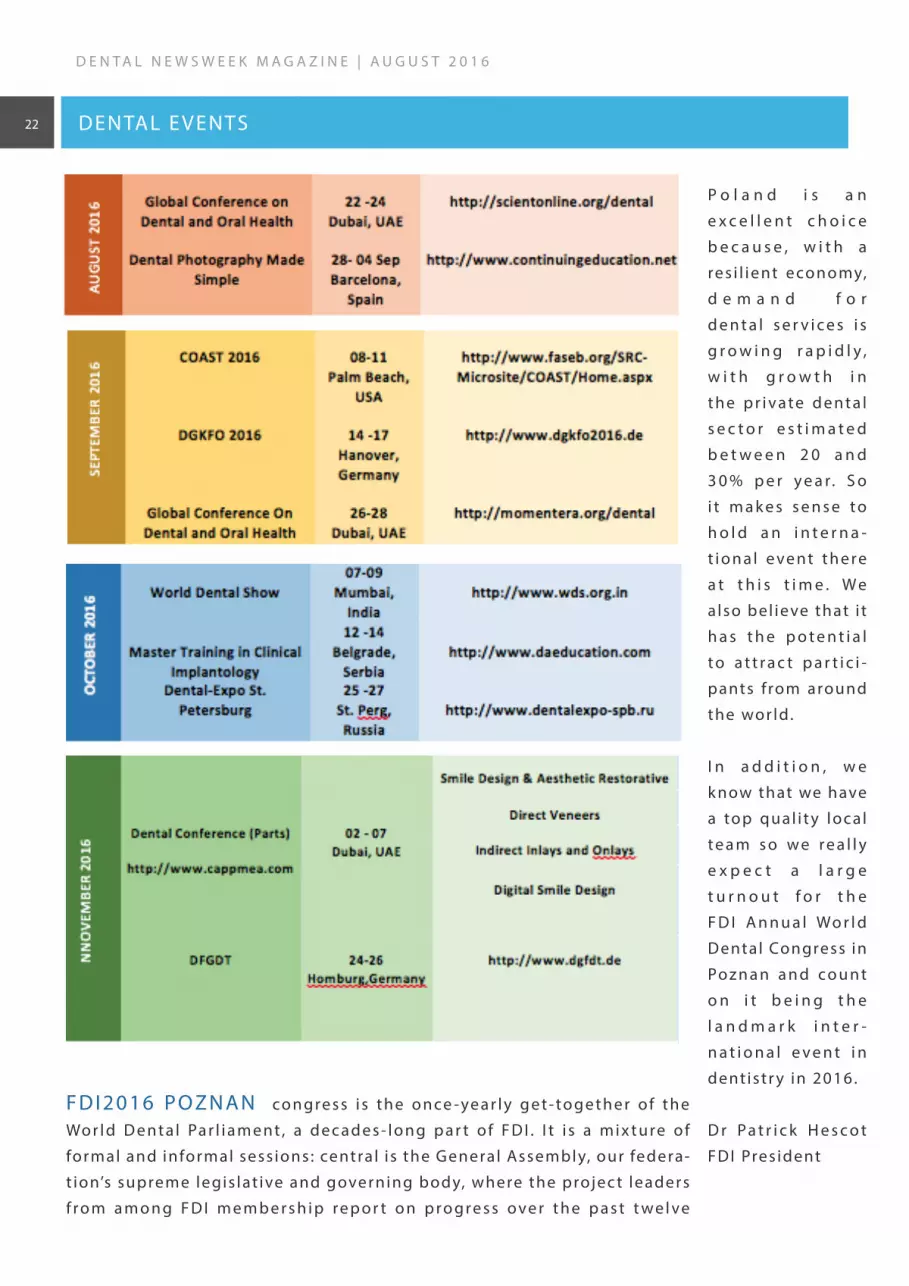
P o l a n d i s a n
e x c e l l e n t c h o i c e
b e c a u s e , w i t h a
re s i l i e nt e co n o my,
d e m a n d f o r
d e n t a l s e r v i c e s i s
g r o w i n g r a p i d l y ,
w i t h g r o w t h i n
t h e p r i v a te d e n t a l
s e c t o r e s t i m a t e d
b e t w e e n 2 0 a n d
3 0 % p e r y e a r. S o
i t m a k e s s e n s e t o
h o l d a n i n t e r n a -
t i o n a l e ve n t t h e re
a t t h i s t i m e . W e
a lso bel ieve that i t
h a s t h e p o t e n t i a l
t o a t t r a c t p a r t i c i -
pants f rom around
the wor ld.
I n a d d i t i o n , w e
k now that we have
a top qual i t y local
t e a m s o w e r e a l l y
e x p e c t a l a r g e
t u r n o u t f o r t h e
F D I A n n u a l Wo r l d
Dental Congress in
Po z n a n a n d c o u n t
o n i t b e i n g t h e
l a n d m a r k i n t e r -
n a t i o n a l e v e n t i n
dent istr y in 2016.
D r Pa t r i c k H e s c o t
FDI Pres ident
F D I 2 0 1 6 P O Z N A N co n gre s s i s t h e o n ce -ye a r l y g e t- to g e t h e r o f t h e
Wo r l d D e nt a l Pa r l i a m e nt , a d e c a d e s - l o n g p a r t o f F D I . I t i s a m i x t u re o f
formal and informal sess ions : centra l i s the General Assembly, our federa-
t ion’s su preme legis lat ive and governing body, where the projec t leaders
f ro m a m o n g F D I m e m b e r s h i p re p o r t o n p ro g re s s o ve r t h e p a s t t we l ve
DENTAL E VENTS

Po l i s h l a n g u a g e i s o n e o f
the most diff icult languages
to learn. I t has seven cases
and grammar that has actu-
a l l y m o r e e x c e p t i o n t h a n
rules.
Cusion
I f t h e r e ’s a t h i n g a b o u t
Poland we are real ly, real ly
proud of, the cuisine wil l be
probably number one. The
most popular Pol ish meals
a r e p i e r o g i ( d u m p l i n g s ) ,
k o t l e t s c h a b o w y ( t y p e o f
breaded cutlet), bigos (a mix
of cabbage, meat and mush-
r o o m s ) , g o ł ą b k i ( c a b b a g e
l e ave s s t u f fe d w i t h m e a t ) ,
ros ół ( ch ick e n s oup) , zupa
ogór kowa (cucumber soup
– i t ’s r e a l l y s o u r ! ! ! ) a n d
ż u re k ( s o u r s o u p w i t h e g g
and sausage) .
( 9 t h l a r g e s t c o u n t r y i n
Eu ro p e ) w i t h a p o p u l at i o n
of over 38.5 mil l ion people.
You should k now the name
of our capita l c i t y but just
to make sure you are wel l -
i n f o r m e d , w e w a n t y o u
t o k e e p i n m i n d t h a t i t ’s
Wa r s z a w a ( Wa r s a w ) – n o t
K rakow.
Faith
The great majority of Pol ish
p e o p l e a r e C h r i s t i a n s –
86.7% belong to the Roman
Cathol ic Church.
Language
T h e R e p u b l i c o f Po l a n d, a
p a r l i a m e n t a r y re p u b l i c , i s
s i tuated in Centra l Europe.
W e h a v e m a n y f r i e n d s
a r o u n d u s , f o l l o w i n g t h e
rule “the more, the merr ier ”
– Czech Republic, Germany,
S l ova k i a , B e l a r u s , U k ra i n e,
R u s s i a a n d L i t h u a n i a . O u r
c o u n t r y h a s a c c e s s t o t h e
Balt ic S ea in the nor th and
i s s u r r o u n d e d b y m o u n -
t a i n s ( Ta t r y , B i e s z c z a d y,
K a r p a t y ) i n t h e s o u t h . I t ’s
b e e n a w h i l e s i n c e o u r
countr y became a member
o f Eu ro p e a n U n i o n ( 2 0 0 4 ) .
The total area of Poland is
312,679 square k i lometers
23
D E N T A L N E W S W E E K M A G A Z I N E | A U G U S T 2 0 1 6
POLAND ON SPOT

AD





























