Embed Size (px)
Citation preview
Author Pro
of
Review
10.1586/14737175.8.6.XXX © 2008 Expert Reviews Ltd ISSN 1473-7175 1www.expert-reviews.com
Brain tumors and epilepsy
Expert Rev. Neurother. 8(6), xxx–xxx (2008)
Christian Brogna, Santiago Gil Robles and Hugues Duffau†
†Author for correspondenceDepartment of Neurosurgery, CNRS UMR 8189 and INSERM U678, Hôpital Gui de Chauliac, CHU de Montpellier, 80 Avenue Augustin Fliche, 34295 Montpellier Cedex 5, FranceTel.: +33 467 33 6612Fax: +33 467 33 [email protected]
When treating patients harboring a brain tumor, it is mandatory to integrate the dogmas ofepilepsy into a neuro–oncological viewpoint. The frequency of seizures differ widely betweenlow- and high-grade tumors because of different mechanisms of epileptogenesis. The moderntheories of pathological neural networks, especially in low-grade gliomas, can provide the keyfor an in-depth understanding of the principles of connectionism that underline both seizures,cognitive impairment and plasticity. It is a consuetude that principles of general managementof patients with nontumor-related epilepsy are applied to neuro-oncology. Nevertheless, sincetumors are complex evolving lesions requiring a multidisciplinary treatment approach (surgery,radiotherapy and chemotherapy), it is mandatory to have a comprehensive view of the naturalhistory of each lesion when choosing the best antiepileptic drug. More than two thirds ofpatients with brain tumors and medically intractable epilepsy benefit from (sub)total surgicalresection. Therefore, these patients are good surgical candidates both for oncological andepileptological considerations, in order to change the natural history of the lesion and toimprove the quality of life at the same time. However, 15% of patients still have intractablemedical seizures after surgery. Moreover, the insula may participate more often than usuallyconsidered in (intractable) seizures. Therefore, in these patients, invasive EEG recordings andeventually a second epilepsy surgery might be proposed.
KEYWORDS: brain tumor • connectivity • epilepsy • glioma • insula • network • plasticity
Approximately 10–15% of adult-onset and0.2–6.0% of childhood-onset cases of epilepsy arecaused by CNS neoplasms [1–3]. Conversely, sei-zure can be the presenting symptom, leading todiagnosis of the underlying brain tumor in 38% ofprimary and 20% of secondary CNS tumors [4].
It is noteworthy that the frequency of seizuresas the first symptom of pathology differs widelybetween different histologies, and, as a conse-quence, between tumors with different naturalhistories and growth patterns. In fact, whileslow-growing tumors are much more relatedwith epilepsy [5–7], high-grade tumors are lessrelated [8–10], probably owing to different mech-anisms of epileptogenesis involved in each type.In particular, dysembryoplastic neuroepithelialtumors can be associated with seizures in up to100% of patients [3,11–16], and 60–85% ofpatients harboring a low-grade glioma, such asoligodendrogliomas, oligoastrocytomas, mixedoligoastrocytomas and gangliogliomas, will haveseizures during the course of their disease [17–19].
Instead, the incidence of epilepsy decreasesdramatically in high-grade tumors: only 30–50%
of patients harboring glioblastoma multiforme[20–22] and 20–35% with brain metastases [23] willhave seizures during their life. Moreover, focalneurological deficits instead of seizures are morelikely to be the presenting symptoms of patientswith high-grade tumors [8].
All the data mentioned above are confirmedby a recent retrospective study [4], that under-lines the inverse relationship between incidenceof epilepsy as a presenting symptom and histo-logical grade of the tumor, with the incidence ofseizures in WHO grade II oligodendendrogli-oma, grade II astrocytoma, and WHO grade IIIand IV astrocytoma being 100, 60, 50 and25%, respectively. These differences reflect thedifferent mechanisms of epileptogenesisbetween low- and high-grade tumors.
Mechanisms of epileptogenesisRole of microenvironmentThe effects of a mass lesion on the surroundingbrain parenchyma include mechanical compres-sion, increased pressure, ischemia and specific

Author Pro
of
2 Expert Rev. Neurother. 8(6), (2008)
Review Brogna, Gil Robles & Duffau
trophic factors [24]. Although voltage-gated ion channels con-trolling cell excitability are involved in epilepsy [25–27], it is notknown whether this is also true for tumor-related epilepsy,since there is no correlation between the presence of voltage-gated sodium channels and epileptogenic discharges usingmagnetoencephalography (MEG) and EEG [28].
Nevertheless, morphological changes in peritumoral tissuethat may affect epileptogenesis include: aberrant neuronalmigration [15,29], changes in synaptic vesicles [30,31], enhancedintercellular communication through increased expression ofgap junction channels [32], or an imbalance between inhibitoryand excitatory mechanisms through changes in local concentra-tions of GABA [33,34], glutamate and lactate [35,36].
The tumor microenvironment may also affect gene expres-sion. The occurrence of hypoxic brain regions, as usually occursin the core of brain tumors, are associated with changes in geneexpression with negative effects on the stability of DNA repairmechanisms and on the likelihood of mutations. Under theseconditions, the astrocytic cell membrane becomes prone toinward sodium currents, leading to risk of epilepsy [37].
The tumor-suppressor gene LGI1 [38], apart from playing arole in glioma progression probably participating to cell inva-sion and migration, is also responsible for the rare syndromeautosomal dominant lateral temporal lobe epilepsy, whichshows Mendelian inheritance. Moreover, LGI1 is not expressedin glioblastoma multiforme cell lines and other high-gradetumors. Since these considerations support the existence of arelationship between low-grade gliomas and epilepsy,Brodtkorb and colleagues have suggested that LGI1 plays a rolein epileptogenesis in patients with brain tumors [39]. Conversly,a recent study has suggested that it is necessary to reconsider itsrole as a tumor suppressor in gliomas [40].
Tumor-associated epilepsy as a deviation of the functional network topology from the optimal small-world patternThe modern theories of pathological neural networks [41–47]
give the tools for a new in-depth understanding of tumor-related epilepsy. These theories can be well applied to slow-growing lesions, which, more than high-grade lesions that arerelated to an abrupt change of the microenvironment, deter-mine a continuous middle- and long-term remodeling of neu-ronal–synaptic organization [48]. Low-grade gliomas are alsoresponsible for a functional imbalance of the white matter fib-ers connecting different cortical networks, since they have atendency to spread to adjacent brain structures, migratingalong the main white matter pathways both within the lesionalhemisphere or even contralaterally essentially via the corpuscallosum [49,50].
Traditionally, neurology has considered the brain cortex to bedivided into specific segregated functional areas, specifically ded-icated to one function. From this assumption derives the consue-tude to correlate through a basic neurological examination a spe-cific clinical deficit to a specific anatomical location of the lesionwithin the brain. However, especially since neuropsychological
assessment before, during and after surgery is more and moregiven to the patients in a clinical setting [51–56], it is clear thatthose patients harboring a brain tumor often suffer from diffusealterations of cognitive functions (attentional deficits, workingmemory problems, reduced psychomotor speed and problemswith executive functions [57]) that cannot be explained by thefocal theory.
Conversely, the modern theory of brain networks, which isderived from the graph theory [58], can explain why a braintumor interferes with widespread functional networks in thebrain rather than only the site of the lesion itself [42]. In fact,cognitive functions in the brain require the functional interac-tions between multiple distinct neural networks [41,59,60]. Inorder to explore the consequences of a lesion on the brain it ismandatory to evaluate its impact on the functional connectivitytaking place between different brain regions [61–63]. MEGrecordings and functional MRI seem to be valuable ways ofanalyzing the functional connectivity between different brainregions [64,65], measuring statistical interdependencies betweensignals of brain activity and analyzing them with the graph the-ory approach [66–68]. In this setting, Bartolomei et al. concludedthat brain tumors determine changes in network architecture offunctional connectivity [41,42]. In particular, frontoparietal con-nections are the most involved in a network’s disarrangement;in normal subjects working memory or direct attentional tasksinvolve the transient synchronization between these tworegions [42,69,70].
In accordance with the small-world network theory, synchro-nization of neurons in networks is mandatory for normal func-tioning and information processing [45,46], but may also reflectabnormal dynamics related to epilepsy. Excessive synchroniza-tion owing to compensatory mechanisms after network imbal-ance from a lesion may be the cause of epilepsy [46,71]. Networkrandomization can be a result of general brain damage, causedby tumors or even surgery. Random networks caused by tumorinfiltration of white matter fibers, and not only infiltration ofthe cortex, might have a lower threshold for seizures than small-world networks [41,71].
Neural networks may develop towards a critical regimenbetween local and global synchronization. Seizures would resultif pathology pushes the system beyond this critical state [44,45,72].
In summary, brain tumors probably convert a healthy globalfunctional network into a pathological network with randomstructure, which may be associated with both cognitive prob-lems and a lower threshold for seizures [73,74]. It not a coinci-dence if cognitive impairment and seizures are both the mainissues of low-grade gliomas. This hypothesis has to be exploredin further studies.
In favor of the potential modifications of cerebral networksare all the studies on brain plasticity, namely the continuousprocessing allowing short-, middle- and long-term remodelingof the neuronal-synaptic organization [48]. Several hypothesesabout the pathophysiological mechanisms underlying brainplasticity and, as a consequence, the modifications of cerebral

Author Pro
of
Brain tumors & epilepsy Review
www.expert-reviews.com 3
networks, can be considered. At a microscopic scale, these mech-anisms seem to be essentially represented by: synaptic efficacymodulations [75], unmasking of latent connections [76], pheno-typic modifications [77] and neurogenesis [78]. At a microscopicscale, diaschisis [79], functional redundancies [80], cross-modalplasticity with sensory substitution [81] and morphologicalchanges [82] are implicated.
All these studies support the idea that we deal with extremelycomplex networks, with a dynamic and not static architecture,when trying to understand the mechanisms underlying brainfunctions. Tumors and probably surgery can modify the naturalbalance and synchronization of these networks leading to abenefit in terms of plasticity with preservation of functionsand/or to the randomization of networks causing seizure onset.
Nowadays, since it is demonstrated that mechanisms of epilep-togenesis involve not only the microenvironment, but also theglobal scale networks and connectivity, in clinical setting bothaspects must be take into account. A global individually basedstrategy, including antiepileptic drugs, surgery, radiotherapyand chemotherapy, is mandatory when treating brain tumor-related epilepsy, both from an oncological and epileptologicalviewpoint.
Clinical settingIt is a consuetude that principles of general management ofpatients with nontumor-related epilepsy are applied to neuro-oncology. Nevertheless, since tumors are complex evolvinglesions dealing with a multidisciplinary treatment approach(surgery, radiotherapy and chemotherapy), it is mandatory tohave a comprehensive view of the natural history of each lesionin order to incorporate in this scenario the dogmas of generalepilepsy treatment.
In addition, there are several theoretical and practical issuesto be considered when giving antiepileptic drugs to patientswith brain tumors, including pharmacokinetics, pharmaco-dynamics, and the potential for drug interactions and sideeffects [11].
Clinical manifestations of tumor-related seizuresComplex partial seizures and complex partial seizures with sec-ondary generalization are relatively frequent in patients withchronic seizures (seizure duration >1 year), whereas simple par-tial seizures and simple partial seizures with secondary generali-zation are relatively common in patients with acute seizures(seizure duration <1 year) [83]. Moreover, secondary generaliza-tion may occur so quickly that, in certain patients, the focalphase passes unnoticed [84,85].
Several patients with temporal lobe tumors also report onlyisolated auras [86]. Somatosensory signs, experimental phenom-ena with mnemonic components, language disturbances, vis-ceromotor and/or viscerosensitive manifestations, olfactory orgustatory hallucinations, and oroalimentary automatisms canbe related both to temporal and insular lesions.
Classification of epilepsy outcomeClinically, there are two main frequency-based classifications ofthe outcome of patients with seizures that are widely used inthe literature. The Engel’s classification is based on four classes[87,88]: class I: free of disabling seizures; class II: rare disablingseizures (almost seizure-free); class III: worthwhile improve-ment; and class IV: no worthwhile improvement. Recently pro-posed, the International League Against Epilepsy classification(ILAE) [89] is based on six classes: class 1: completely seizurefree, no auras; class 2: only auras, no other seizures; class 3: 1–3seizure days per year ± auras; class 4: At least 4 seizure days peryear to 50% reduction of baseline seizure days ± auras; class 5:less than 50% reduction of baseline seizure days to 100%increase of baseline seizure days ± auras; class 6: more than100% increase of baseline seizure days ± auras.
MonotherapyFor partial seizures, the anticonvulsants carbamazepine orlamotrigine are recommended as first-line treatments [90]. Valp-roic acid [91–93] and levetiracetam [94–96] are broad-spectrumanticonvulsants both for partial and generalized seizures.
It is interesting that side effects associated with levetiracetam[97], gabapentin [98,99], tiagabine [100] and topiramate [101] areinfrequent. Nevertheless, it is of importance to make someconsiderations.
Although carbamazepine alone is one of the most effectiveantiepileptic drugs for treatment of partial epilepsy, inpatients with cancer it has the drawback of being an enzyme-inducer and thus might compromise the effectiveness of con-comitantly administered chemotherapy [11,102]. Further-more, carbamazepine is associated with a small risk of bone-marrow depression, which needs careful consideration inpatients receiving chemotherapy [103]. Although the use oflamotrigine is well established for the treatment of sympto-matic localization-related epilepsy, it has a somewhat pro-tracted prescription formulation (i.e., it can take severalweeks to achieve a therapeutic dose) [104]. Although topiram-ate is a nonenzyme-inducer and can be chosen as immuno-therapy, it might have lower tolerability compared withnewer antiepileptic drugs [105,106].
Valproic acid has a sound reputation as a broad-spectrumanticonvulsant for the treatment of generalized and partial epi-lepsy; it has mild toxic effects and has the advantage that it canbe started at therapeutic dosages immediately [93,95,107]. How-ever, combined with chemotherapy, the enzyme-inhibitingeffects of valproic acid might increase the risk of bone-marrowtoxicity [92,108]. Nevertheless, findings on this drug further cor-roborate its use in patients with brain tumors [109]. In fact, val-proic acid was suggested to have also inherent antitumoreffects through inhibition of histone deacetylase, which leadsto cell differentiation, growth arrest, and apoptosis of cancercells [110–112]. Moreover, valproic acid might also suppress for-mation of MDR-1, which possibly diminishes the chances ofrefractoriness [113].
Author Pro
of
4 Expert Rev. Neurother. 8(6), (2008)
Review Brogna, Gil Robles & Duffau
A double-blind, randomized trial showed that levetiracetamas immunotherapy was as effective as carbamazepine for thetreatment of de novo partial epilepsy, and was associated withfewer or about the same amount of side effects [114]. Moreover,a retrospective study showed that phenytoin was the most com-mon anticonvulsant medication to be discontinued in favor oflevetiracetam [4,97].
PolytherapyUnfortunately, 70% of patients with low-grade gliomas whotake carbamazepin, 51% who take phenytoin and 44% whoreceive valproic acid still have recurrent seizures. Thus, if a first-line agent is insufficient, levetiracetam or gabapentin can beadded, both of which do not interact with other agents[95,107,115]. Studies suggest levetiracetam has greater efficacythan gabapentin [105,106]. Add-on levetiracetam can lead tosome patients becoming seizure-free or having fewer seizurethan before the treatment [4,97,105,115,116]. In a retrospectivestudy of 147 patients harboring brain tumors treated at oneinstitution [4], levetiracetam was the most common additionalmedication used when polytherapy was required: 95% ofpatients on polytherapy were seizure free or had only occasionalbreakthrough seizures.
These results suggest that add-on treatment with levetira-cetam seems to be well tolerated, and that further assessment ofthese drugs in patients with brain tumors is warranted [3].
Interactions between antiepileptic & chemotherapeutic agentsOnce again, it is mandatory to have a global viewpoint on themanagement of brain tumors when choosing the most appro-priate antiepileptic drug for one patient, according to the spe-cific phase of the natural history of the tumor, and in particularto the concomitant administration of chemotherapeutic agentsas adjuvant or neoadjuvant therapies both in high- and low-grade gliomas [105,117,118]. In fact, interactions between antiepi-leptic drugs and antineoplastic agents may lead to insufficientcontrol of the tumor or epilepsy, or to toxic effects of one orboth of the agents.
Low levels of antiepileptic drugs have been reported in60–70% of patients [21]. In patients with brain tumors, thera-peutic antiepileptic drug levels are difficult to maintain becauseof frequent pharmacodynamic and pharmacokinetic interac-tions [11] with concomitant medications, as changes in plasmaprotein (especially albumin) levels. In particular, pharmacoki-netic interactions can affect drug uptake, metabolism in theliver or elimination of the drug. Furthermore, drug–drug inter-actions can change the volume of drug distribution and affectprotein binding. Several antiepileptic drugs (e.g., phenobarbi-tal, primidone, carbamazepine, and phenytoin) induce cyto-chrome P450 coenzymes, such as 3A4, 2C9 or 2C19, whichleads to faster metabolism and lower plasma concentrations ofagents given concomitantly that share the same metabolicisoenzyme [119].
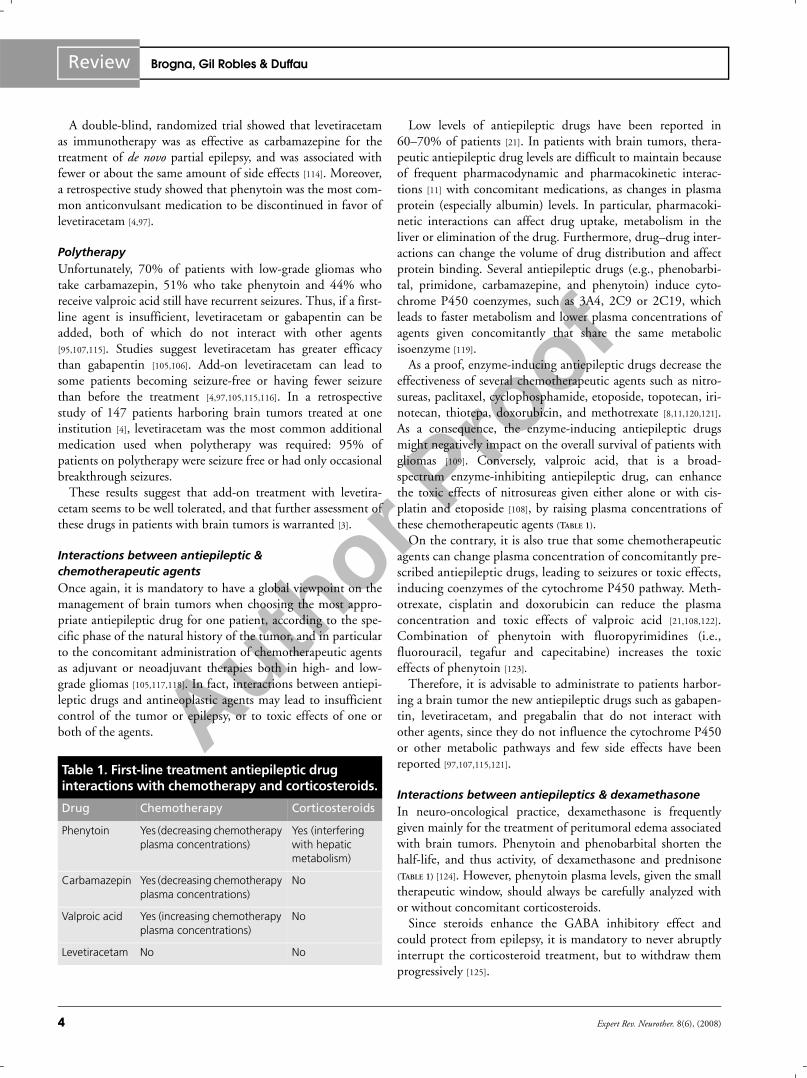
As a proof, enzyme-inducing antiepileptic drugs decrease theeffectiveness of several chemotherapeutic agents such as nitro-sureas, paclitaxel, cyclophosphamide, etoposide, topotecan, iri-notecan, thiotepa, doxorubicin, and methotrexate [8,11,120,121].As a consequence, the enzyme-inducing antiepileptic drugsmight negatively impact on the overall survival of patients withgliomas [109]. Conversely, valproic acid, that is a broad-spectrum enzyme-inhibiting antiepileptic drug, can enhancethe toxic effects of nitrosureas given either alone or with cis-platin and etoposide [108], by raising plasma concentrations ofthese chemotherapeutic agents (TABLE 1).
On the contrary, it is also true that some chemotherapeuticagents can change plasma concentration of concomitantly pre-scribed antiepileptic drugs, leading to seizures or toxic effects,inducing coenzymes of the cytochrome P450 pathway. Meth-otrexate, cisplatin and doxorubicin can reduce the plasmaconcentration and toxic effects of valproic acid [21,108,122].Combination of phenytoin with fluoropyrimidines (i.e.,fluorouracil, tegafur and capecitabine) increases the toxiceffects of phenytoin [123].
Therefore, it is advisable to administrate to patients harbor-ing a brain tumor the new antiepileptic drugs such as gabapen-tin, levetiracetam, and pregabalin that do not interact withother agents, since they do not influence the cytochrome P450or other metabolic pathways and few side effects have beenreported [97,107,115,121].
Interactions between antiepileptics & dexamethasoneIn neuro-oncological practice, dexamethasone is frequentlygiven mainly for the treatment of peritumoral edema associatedwith brain tumors. Phenytoin and phenobarbital shorten thehalf-life, and thus activity, of dexamethasone and prednisone(TABLE 1) [124]. However, phenytoin plasma levels, given the smalltherapeutic window, should always be carefully analyzed withor without concomitant corticosteroids.
Since steroids enhance the GABA inhibitory effect andcould protect from epilepsy, it is mandatory to never abruptlyinterrupt the corticosteroid treatment, but to withdraw themprogressively [125].
Table 1. First-line treatment antiepileptic drug interactions with chemotherapy and corticosteroids.
Drug Chemotherapy Corticosteroids
Phenytoin Yes (decreasing chemotherapy plasma concentrations)
Yes (interfering with hepatic metabolism)
Carbamazepin Yes (decreasing chemotherapy plasma concentrations)
No
Valproic acid Yes (increasing chemotherapy plasma concentrations)
No
Levetiracetam No No

Author Pro
of
Brain tumors & epilepsy Review
www.expert-reviews.com 5
Epilepsy prophylaxis in neuro-oncologyWhile initiation of an antiepileptic treatment is generally justi-fied after a first single seizure in patients harboring a braintumor, it not clear whether an antiepileptic drug should beprescribed to patients who have never had a seizure.
Two meta-analyses of antiepileptic drugs in patients with braintumors who did not have seizures suggested no efficacy as proph-ylaxis [21,126]. A consensus statement from the Quality StandardsSubcommittee of the American Academy of Neurology recom-mends not to use antiepileptic drugs routinely as prophylaxis inpatients with brain tumors, and to withdraw these drugs in thefirst week after surgery if patients have never had seizures [21].
Nevertheless, it is mandatory to integrate these recommenda-tions into a neuro-oncological setting for the following reasons.First, even if epilepsy is not the presenting symptom of thetumor, 20–45% of these patients have a risk of developing sei-zures later on, depending on tumor type, location, patient ageand previous cancer treatment [21]. Second, since the naturalhistory of low-grade gliomas differs dramatically from high-grade tumors [127–129], we must take into consideration the dif-ference in prognosis, treatment modalities and the adjunct riskof epilepsy between them.
Thus, in patients harboring a low-grade glioma with at leastsubtotal resection and no decision of adjuvant oncologicaltreatment modalities (until a recurrence or anaplastic transfor-mation), when no seizures occur after surgery as happens inmore than 85% of cases [18,84], it is reasonable to follow theavailable guidelines [21] and to try to withdraw antiepilepticdrugs if possible. However, as physicians, we have to respect thewill of patients who wish to continue to take their daily antiepi-leptic drugs. In fact, some patients find a good psychologicalbalance between the assumption of antiepileptic drugs, theircertainty that “everything is going on well” and their self-confi-dence. A good psychological balance has a great impact on thepatient’s quality of life.
Conversly, in patients harboring a high-grade glioma, consid-ering the poor prognosis and the certainty of a recurrence in afew months [130], it is reasonable to withdraw antiepilepticdrugs only in a subset of patients after radiotherapy, with grosstotal resection, good performance status, absence of seizures, orin case of intolerance. Once again, as physicians we have to takeinto account the will and the psychology of our patients.
Multidrug resistance-related proteins in refractory epilepsyA clinically useful definition of medical refractory epilepsy is thepresence of seizures so frequent or severe that they limit dailylife, despite the use of antiepileptic drugs at adequate serumconcentrations [131]. Patients with refractory epilepsy are com-monly resistant to many antiepileptic drugs despite differentmechanisms of action, which suggests nonspecific mechanismsof resistance [132].
In fact, MDR in brain tumor proteins is a major cause ofrefractoriness [90,132–135]. While in healthy brains MDR1(ABCB1, P-glycoprotein) and multidrug resistance-related
protein (MRP, ABCC1) contribute to the function of the BBBand blood–cerebrospinal fluid barrier [115,132,136,137], braintumors can diminish antiepileptic drugs’ transport into thebrain parenchyma [138].
Therefore, insufficient concentration of antiepileptic drugs inthe blood can be the result of an active defense mechanism byMDR1, which restricts the penetration of lipophilic substancesinto the brain. To support this hypothesis, overexpression ofMDR1 was founded in samples of brain tissue from patientswith focal cortical dysplasia and ganglioglioma [16,139].
Valproic acid, carbamazepin, phenytoin, phenobarbital andlamotrigine are substrates for this gene product [132,137], butrecent data do not support the hypothesis that MRP1 or MRP2are involved in the efflux of valproic acid from the brain [140]. Inpreclinical studies it has been demonstrated that levetiracetamis not a substrate for MRPs [141]. Theoretically, blockers ofMDR might overcome drug resistance [97,105,142].
Tumor locationTumor location affects the risk of medically intractable epilepsy.A tumor invading the cortex is the main predictive factor fordevelopment of epilepsy [3,143], and lesions in the frontal, tem-poral and parietal lobes are more commonly associated with sei-zures than are occipital lesions [4,126]. Moreover, low-grade glio-mas are situated more frequently in eloquent corticosubcorticalareas compared with de novo glioblastoma multiforme [143]. It isof importance that low-grade gliomas, which are highly associ-ated with medically refractory seizures, are also located signifi-cantly more often within the supplementary motor area (SMA)and insula regions [143], both of which have been demonstratedto have a functional role in epilepsy [88,144]. In fact, the insulaand SMA share similar transitional structural and functionalprofiles [145–149]. Therefore, it can be hypothesized that particu-lar interactions may exist between neurons and glial cells inthese regions [143] due to the fact that glial cells play a role inneuronal migration [150]. It may explain the existence of migra-tion disorders in some cortical epilepsies [151], including theextratemporal epilepsy that often originates from the SMA [152]
and insula [153] in the regulation of synaptic transmission [154],
and in the energy metabolism of the neuron, explaining theneurovascular and metabolic decoupling in gliomas [155].
In the temporal lobe region, mass lesions might induce sec-ondary epileptogenicity in the mesiotemporal structures lead-ing to refractory epilepsy after surgery with lesionectomy alone[156]. The relation between epilepsy and tumors might bestronger than we think. In neuropathological series of en bloctemporal resections for surgically treated temporal lobe epi-lepsy, focal lesions other than hippocampal sclerosis have beenreported in a substantial number of specimens, ranging from30 to 71% [157,158]. In a recent series of en bloc temporal loberesections for temporal lobe epilepsy, neoplasms were seen in25.6% of the patients [156]. Two comparable publications of anIndian group reported only 8.3 and 13.8% of neoplasmsaccounting for temporal lobe epilepsy [159].

Author Pro
of
6 Expert Rev. Neurother. 8(6), (2008)
Review Brogna, Gil Robles & Duffau
Brain tumor surgery & epilepsyFunctional brain mappingAn essential advance in surgery of intrinsic brain tumors is theuse of intraoperative direct corticosubcortical stimulation(DCS), under general or local anesthesia due to the frequentlocation of these tumors, in particular low-grade gliomas, in elo-quent areas and their infiltrative feature [51,143,59,160–163]. DCSallows the mapping of motor function (possibly under generalanesthesia, by inducing involuntary motor response if stimula-tion at the level of an eloquent site), somatosensory function (byeliciting dysesthesia described by the patient intraoperatively),and also the mapping of cognitive functions such as language(e.g., spontaneous speech, object naming and comprehension),calculation, memory, and reading or writing, performed in thesecases on awake patients, by generating transient disturbances ifthe electrical stimulation is applied at the level of a functionalepicenter. Thus, DCS is able to identify in real-time the corticalsites and subcortical white matter fibers essential for functionthat must be imperatively preserved.
Intraoperative mapping also allows a better understanding ofbrain functioning [160,164–166] and, above all, the study ofanatomo–functional connectivity, through the detection ofbundles for subcortical, motor, somatosensory and languagepathways, and those for other cognitive functions [59,167–169],
namely the principles of connectionism underlying both sei-zures, and cognitive impairment and plasticity. Moreover, grad-ual repetition of electrical stimulation during resection allowsthe existence of reorganization phenomena of the functionalcortical maps to be documented over the short and long term,making it possible to consider a second surgical interventionwith the addition of resecting lesions located in the eloquentzones that could not be removed during the first intervention[80,166,167,170–172].
The integration of a systematic functional mapping, of theonline study of the effective connectivity and of the individualplastic potential during each surgical procedure has enabledan extension of the indications for surgery of gliomas, espe-cially low grade, to maximize the quality of the resection andto minimize the risk of inducing permanent postoperativeneurological deficit.
Impact of brain tumor surgery on epilepsySeveral authors have studied the surgical and epileptologicaloutcome of tumor-associated epilepsy [86,173–175]. Favorableresults have been reported for complete lesionectomies, withthe percentage of seizure-free patients ranging from 65 to 80%[86,159,173,175,176]. In these cases, the cortex surrounding thetumor probably loses the ability to independently initiate andpropagate seizures once the tumor itself has been removed [174].
In low-grade gliomas, the extent of surgery favorably influ-ences the immediate functional outcome in terms of seizure fre-quency [177], not solely when it allows the alleviation of signs ofraised intracranial pressure or focal deficits (rarely) due to a
compressive mechanism. After surgical resection of low-gradegliomas in the right and even in the left insula, seizure controlwith the patient being in Engel class I is achieved in 80% ofcases [84].
Epilepsy benefits from surgery in the majority of cases, evenwithout the use of specialized approaches/techniques of corti-cectomy (with improvement of quality of life), even in eloquentareas and more so with subtotal or total resections [84].
However, there is evidence to support the concept of separateseizure foci surrounding a tumor. After resection of temporallobe tumors, residual spikes can be observed with intraoperativeelectrocorticography monitoring over the hippocampus andamygdala in 86.4 and 63.6% of cases, respectively [28,178]. Inthe surgical series of Sugano et al., seizure control was better ifthe zone of seizure origin and the zone of maximal interictalspiking were completely excised [178]. In a comparative study ofanterior temporal lobectomy incorporating the lesion andlesionectomy, 90% of lobectomy patients compared twith 50%of lesionectomies patients were seizure free [179].
Therefore, there are circumstances where electrophysiologicalchanges presumably do not reach the stage of independent sec-ondary epileptogenicity, and effective seizure control is possiblewith lesionectomy alone, while in other cases residual spikescan be true independent secondary foci of epileptogenicity andthe surgical treatment of independent secondary epilepticspikes can improve seizure outcome [178].
It has been suggested that intraoperative electrocorticographyunder local anesthesia could be a sensible tool to enable theneurosurgeon to decide whether or not to continue to resectpotential epileptic foci originating in the amygdala and/or hip-pocampus, while the posterior limit of surgical resection in thetemporal lobe, especially within the dominate hemisphere, isfound according to functional boundaries (for instance, untillanguage disturbances are induced by cortical and subcorticalmapping in awake patients) [160,167,178,180–182].
Early surgical intervention showed a strong tendency to pre-dict better seizure outcome [175]. Seizure free rate after surgeryof gliomas is 82.9% in patients with acute onset of seizures(mostly high-grade tumors) and 62.5% in patients withchronic seizures (mostly low-grade gliomas). This supportsearly operation not only regarding oncological considerations,but also to avoid the risk of chronic epilepsy and optimize thepatient’s quality of life [84,86,178]. This can be hypothesized alsoin gangliogliomas, which are associated with intractable seizuresin up to 100% of cases. However, even in glioneuronal tumors,which represent and indication for a true epilepsy surgery [183],oncological considerations are important, since gangliogliomasmight progress to high-grade tumors [184].
Brain tumor surgery & refractory epilepsyDespite the fact that more than 80% of brain tumor-relatedepilepsies benefit from surgery, 15–20% of patients still sufferfrom medically intractable seizures, even after (sub)total tumorresection [84,86,159,173,175,176].

Author Pro
of
Brain tumors & epilepsy Review
www.expert-reviews.com 7
It is reasonable that chronic preoperative epileptic patientsmight develop aberrant networks, even far from the location ofthe lesion. In fact, the possible coexistence of multiple epilep-tic foci and dual pathology is well demonstrated [185], evencontralaterally, in patients with a long history of epilepsy.
Interestingly, the majority of reports studied seizures associ-ated with gliomas involving the limbic system (essentially themesiotemporal structures) and/or neocortex [176], but very fewdescribed the epilepsy outcome after surgery of glial tumorsinvading the insular mesocortex [186–189]. Moreover, none ofthese rare series except one [186] report of two cases detailed theresults concerning medically intractable epilepsy [84].
Conversly, recent studies demonstrated that insular epilepsymay share many clinical and EEG features with temporomesialand opercular seizures [153,190,191], probably owing to the richconnections between the insular cortex and the limbic/neocor-tical regions via the uncinate fasciculus [145,192]. Thus, it is pos-sible that the insula may participate more often than usuallyconsidered in (intractable) seizures [153,190].
Penfield noted the similarity between many of the symptomsof medial temporal lobe epilepsy and those he found with insu-lar stimulations, indicating that, in theory, insula seizures couldbe confused with medial temporal lobe epilepsy seizures (citedfrom [88]).
Ictal symptoms related to insula onset are: somatosensorysigns, experimental phenomena with mnemonic component,language disturbances, visceromotor and/or viscerosensitivemanifestations, olfactory or gustatory hallucinations, and oro-alimentary automatisms [84], and sensations of unreality ofbody movement [88]. If seizures spread to the insula from themesial temporal lobe, patients’ reports of their symptoms areinconsistent and unreliable because their consciousness isaffected [88]. Thus, only patients with seizures arising in theinsula (10%) can provide such information. A fully consciouspatient with laryngeal discomfort, unpleasant perioral orsomatic paresthesias, and dysarthric speech, following hemi-sensory paresthesias, is quite specific for insular involvement.Thus, the participation of insular cortex in refractory epilepsyremains poorly understood [84,88].
First, the difficulty in studying this complex structureaccounted for the incomplete knowledge of its precise func-tionality for many decades. The new developments in noninva-sive functional neuroimaging methods have recently allowed abetter analysis of the physiopathology of this entity, whichseems to constitute an interface between the limbic system andthe neocortex.
Second, the insular lobe lesions were consequently poorlystudied, particularly concerning insular gliomas and/or seizures,with few series in several decades [153,170,191,193,194]. Indeed, forepileptological investigations, due to its location deep within thesylvian fissure, scalp EEG is relatively insensitive to electricalactivity in the insula, and chronic invasive electrographic studiesof the region have not been reported for a long time takingaccount of a dense wall of arteries running on the insular surface.
Third, because of the technical complexity in approachingand dissecting this region, very few neurosurgeons attemptedsurgery of the insula structure [170,188,193,194].
Independent epileptogenicity of the insula cortex was diffi-cult to prove. It has been extremely challenging to differentiateseizures arising from the mesial temporal lobe and rapidlyspread to the insula versus those that originate in the insula andconsequently spread to the temporal lobe. Although the formermight still be cured with a temporal lobectomy, the latter likelyrequires insular resection for successful outcome.
Owing to recent technological improvements of stereo-EEG,in particular the smaller size of the electrode diameter and thegreater accuracy of localization of the cortical targets using MRI,chronic recording of the insular cortex with transopercular elec-trodes is now possible [88]. Indeed, only two observations in theliterature were reported before these developments: a chronicallyimplanted depth EEG strip electrode in the Sylvian fissure, in acase of surgical resection of insular glioma, with recording of theseizures in the insular cortex [186]; and a study in 1985 on stereo-EEG activity recording in 11 patients with low-grade gliomasand severe partial epilepsy, which demonstrated that while back-ground activity is never found in the core of the tumor, it couldbe found in the infiltrating white matter fibers [195]. Interest-ingly, using the new technical progress of stereo-EEG, Isnardet al. showed that all the recorded spontaneous seizures in aseries of 21 patients with intractable temporal lobe epilepsy werefound to invade the insula, most often after a relay in the ipsilat-eral hippocampus (19 of 21 cases), but for two patients, withseizures directly originating in the insular cortex itself [153,196].
All these new data suggest that the insula may play an impor-tant role in the genesis of ictal symptoms, maybe sometimeswrongly attributed to the temporal lobe [84]. In fact, the insulahas long been implicated in the 30% failure rate after temporalresections for medial temporal lobe epilepsy [88]. Moreover, 15%of patients harboring a low-grade glioma within the insula, evenafter (sub)total surgical resection, still have intractable medicalseizures that deeply affect the quality of life [84]. In these cases,the invasion by the tumor into functional areas, as frequentlyoccurs in low-grade gliomas [143,197], probably leads to a struc-tural remodeling of the optimal small-world network and toaberrant axonal sprouting [41,42,71,71,198–200].
For all these reasons, the authors suggest invasive recordingswith stereo-EEG in patients with total resection of tumorswithin the temporal or insula lobes, who still have intractablemedical seizures. Second epilepsy surgery may be proposed tothese patients, depending on the pathways involved in currentspreading (surgical interruption of these pathways), with theaim of improving the patient’s quality of life.
Impact of radiotherapy & chemotherapy on epilepsyCranial radiotherapy might have a long-term positive effect onepilepsy in brain tumors [201,202]. It can induce a reduction inseizure frequency of more than 75% with a median follow-up

Author Pro
of
8 Expert Rev. Neurother. 8(6), (2008)
Review Brogna, Gil Robles & Duffau
of 12 months or more after this procedure [203]. Interstitial radio-surgery might lower the incidence of seizures by increasing ben-zodiazepine receptor density [204]. Gamma-knife radiosurgery formesiotemporal tumor-related epilepsy, with the aim to also irra-diate the presumed epileptic foci surrounding the tumor volume,might determine an improvement in seizure outcome [205].
Nevertheless, seizure frequency increases occasionally aftersurgery or radiotherapy, secondary to complications such asedema, bleeding or radiation necrosis [206].
The alkylating chemotherapeutic agent temozolomidereduces seizure frequency in 50–60% of patients with glioma,and 20–40% of patients become seizure free [207,208]. Therefore,in patients with partially resected WHO grade II gliomas andrefractory epilepsy, the administration of temozolomide foroncological reasons might also positively influence the seizureactivity, leading to an improvement in the quality of life.
Expert commentaryWhen treating patients harboring a brain tumor, it is mandatoryto integrate the dogmas of epilepsy into a neuro-oncologicalviewpoint, according to the natural history of the tumor and themultiple oncological treatments given to these patients. It has tobe noted that frequency of seizures, as the first symptom ofpathology, differs widely between low- and high-grade tumors.
Thus, in patients harboring a low-grade glioma with at leastsubtotal resection and no decision of adjuvant oncologicaltreatment modalities (until a recurrence or anaplastic transfor-mation), when no seizures occur after surgery, as happens inmore than 85% of cases [18,84], it is reasonable to follow theguidelines available [21] and to try to withdraw antiepilepticdrugs if possible.
Conversly, in patients harboring a high-grade glioma, consid-ering the necessity, after surgical resection, to maintain a goodperformance status in order to receive radiotherapy and chemo-therapy, and considering the poor prognosis and the certainty ofa recurrence in a few months, it seems reasonable to maintainthe antiepileptic coverage through the patient’s lifetime.
The ideal antiepileptic drug should be effective in avoidingboth partial and generalized seizures and should not interferewith other treatments. New antiepileptic drugs, such as leveti-racetam, are of interest in neuro–oncology, since they have abroad-spectrum efficacy, poor side effects, are not substrates forMDR proteins and are not enzyme inducers.
Mechanisms of epileptogenesis act at different levels: on geneexpression; on the microenvironment of the surrounding brainparenchyma; and on global scale networks.
Nowadays, we know that the brain’s functions are shadowedin highly complex, time based, well balanced small-world net-works. The modern theories of pathological neural networksexplain that brain tumors determine an imbalance in networkarchitecture of functional connectivity [41,42]. Therefore, exces-sive synchronization owing to compensatory mechanisms afternetwork imbalance may be the cause of epilepsy [43,46,71].
Low-grade gliomas seem to be highly involved in networkrandomization, since they not only infiltrate the cortex, butalso spread along the white matter fibers (cables) that connectdifferent cortices.
More than two thirds of patients with brain tumors and med-ically intractable epilepsy benefit from (sub)total surgical resec-tion. Therefore, these patients are good surgical candidates,both for oncological (impact on time to progression disease andoverall survival) and epileptological considerations. Moreover,early surgical intervention shows a strong tendency to predictbetter seizure outcome
Nevertheless, in approximately 20% of patients, surgery failsthe goal to reduce seizures and they are still intractable after theresection of the tumor. The more we wait to operate patientswith brain tumors and medically intractable seizures, the morethe risk of developing aberrant networks even far from the loca-tion of the lesion.
We can also speculate about which treatment to propose tothese patients after the first surgery has failed in terms of seizurereduction. Invasive EEG recordings could answer the question:where are the epileptic foci far beyond the surgical cavity, andhow does the current spread along white matter pathways? Ifthe distribution of the epileptic foci is clear, we could proposeto these patients a second epilepsy surgery, aiming to improvetheir quality of life.
Five-year viewIn 5 years, several developments could be predicted in the treat-ment of tumor-related epilepsy.
• First, in patients with brain tumors, large prospective studiesare mandatory to understand whether new antiepilepticdrugs are effective, free of side effects and free of interactionswith other drugs.
• Second, the great interest about new theories of pathologicalbrain networks will translate in a new in-depth understandingof global neural network imbalance leading to epilepsy.
• Third, the modern theories of neural networks will be a uniquemathematical model to correlate at the same time epilepsy,cognitive impairment and plasticity in brain tumors.
• Fourth, using preoperative diffusion tensor MRI (subcorticalanatomical information), MEG (temporal data), functionalMRI (functional data) and stereo-EEG (electrophysiologicaldata) will enable elaboration of the individual and predictivemodels of the functioning of neuronal-synaptic circuits, andthen to tailor the surgical strategy in term of oncological,functional and seizure results.
• Fifth, invasive EEG recordings will help to localize seizurefoci far from the lesion, in patients with sub(total) surgicalresection, but still medically refractory epilepsy, especially incases where the insula seems to be involved, and to eventuallypropose to the patients a second epilepsy surgery in order toimprove their quality of life.

Author Pro
of
Brain tumors & epilepsy Review
www.expert-reviews.com 9
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement withany organization or entity with a financial interest in or financial conflict
with the subject matter or materials discussed in the manuscript. Thisincludes employment, consultancies, honoraria, stock ownership or options,expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Key issues
• Slow-growing brain tumors, such as dysembryoplastic neuroepithelial tumors, gangliogliomas and WHO grade II gliomas, are highly associated with seizures (and no neurological deficit), while high-grade brain tumors are less associated with seizures.
• Different mechanisms of epileptogenesis are involved in low- and high-grade tumors. Epileptogenesis in brain tumors can be explained at different levels: gene expression, changes in microenvironment, and imbalance and/or hypersynchronization of complex brain networks underlying higher order functions.
• The ideal antiepileptic drug, given to patients harboring a brain tumor, should be effective both in partial and generalized seizures, should not interfere with neurocognitive status, with other chemotherapeutic agents administered during the natural history of disease or with radiotherapy. In patients with no history of seizures, withdrawal of antiepileptic drugs is possible in low-grade gliomas, while it is not recommended in high-grade tumors because of the immediate adjuvant treatments and the certainty of recurrence within months to years. Moreover, despite the guidelines, we must consider the psychological balance of those patients who do not wish to withdraw antiepileptic drugs and respect them.
• More than two thirds of patients with brain tumors and medically intractable epilepsy benefit from (sub)total surgical resection. Therefore, in these patients, indications for surgery are both the impact on the oncological natural history of the lesion and the improvement of tumor-related seizure outcome. Nevertheless, approximately 15% of patients still have medically refractory epilepsy after surgery.
• Invasive EEG recordings have demonstrated that the insula cortex plays an important role, not only in seizure spreading, due to its multiple connections especially with the temporal lobe, but also in the initiation of seizures.
• Invasive EEG recording might be a valuable tool for studying patients with (sub)total resections and still medically refractory epilepsy.
• As now widely recommended in oncological surgery, namely to extend the quality of tumor removal while preserving the functions by performing resection according to individual functional boundaries using brain mapping, we suggest to also tailor the resection on the basis of functional mapping when performing a second surgery in patients with a brain tumor, not only for oncological but even for epileptological reasons.
References
Papers of special note have been highlighted as:
• of interest
•• of considerable interest
1 Ibrahim K, Appleton R. Seizures as the presenting symptom of brain tumours in children. Seizure 13(2), 108–112 (2004).
2 Bromfield EB. Epilepsy in patients with brain tumors and other cancers. Rev. Neurol. Dis. 1(Suppl. 1), S27–S33 (2004).
3 van Breemen MS, Wilms EB, Vecht CJ. Epilepsy in patients with brain tumours: epidemiology, mechanisms, and management. Lancet Neurol. 6(5), 421–430 (2007).
4 Lynam LM, Lyons MK, Drazkowski JF et al. Frequency of seizures in patients with newly diagnosed brain tumors: a retrospective review. Clin. Neurol. Neurosurg. 109(7), 634–638 (2007).
5 Klein M, Engelberts NH, van der Ploeg HM et al. Epilepsy in low-grade gliomas: the impact on cognitive function and quality of life. Ann. Neurol. 54(4), 514–520 (2003).
6 Stieber VW. Low-grade gliomas. Curr. Treat. Options Oncol. 2(6), 495–506 (2001).
7 Gunnarsson T, Olafsson E, Sighvatsson V, Hannesson B. Surgical treatment of patients with low-grade astrocytomas and medically intractable seizures. Acta Neurol. Scand. 105(4), 289–292 (2002).
8 Riva M, Salmaggi A, Marchioni E et al. Tumour-associated epilepsy: clinical impact and the role of referring centres in a cohort of glioblastoma patients. A multicentre study from the Lombardia Neurooncology Group. Neurol. Sci. 27(5), 345–351 (2006).
9 Hwang SL, Lieu AS, Kuo TH et al. Preoperative and postoperative seizures in patients with astrocytic tumours: analysis of incidence and influencing factors. J. Clin. Neurosci. 8(5), 426–429 (2001).
10 Pace A, Bove L, Innocenti P et al. Epilepsy and gliomas: incidence and treatment in 119 patients. J. Exp. Clin. Cancer Res. 17(4), 479–482 (1998).
11 Vecht CJ, Wagner GL, Wilms EB. Treating seizures in patients with brain tumors: drug interactions between
antiepileptic and chemotherapeutic agents. Semin. Oncol. 30(6 Suppl. 19), 49–52 (2003).
• Good overview on interactions between antiepileptic drugs and chemotherapy.
12 Nishida N, Hayase Y, Mikuni N et al. A nonspecific form of dysembryoplastic neuroepithelial tumor presenting with intractable epilepsy. Brain Tumor Pathol. 22(1), 35–40 (2005).
13 Duggal N, Taylor R, Zou GY, Hammond RR. Dysembryoplastic neuroepithelial tumours: clinical, proliferative and apoptotic features. J. Clin. Pathol. 61(1), 127–131 (2008).
14 Kwon KH, Lee JI, Hong SC, Seo DW, Hong SB. Gamma knife radiosurgery for epilepsy related to dysembryoplastic neuroepithelial tumor. Stereotact. Funct. Neurosurg. 84(5–6), 243–247 (2006).
15 Lee MC, Kang JY, Seol MB et al. Clinical features and epileptogenesis of dysembryoplastic neuroepithelial tumor. Childs Nerv. Syst. 22(12), 1611–1618 (2006).
Author Pro
of
10 Expert Rev. Neurother. 8(6), (2008)
Review Brogna, Gil Robles & Duffau
16 Aronica E, Gorter JA, Redeker S et al. Distribution, characterization and clinical significance of microglia in glioneuronal tumours from patients with chronic intractable epilepsy. Neuropathol. Appl. Neurobiol. 31(3), 280–291 (2005).
17 Van den Bent MJ, Reni M, Gatta G, Vecht C. Oligodendroglioma. Crit. Rev. Oncol. Hematol. (2008) (Epub ahead of print).
18 Chang EF, Potts MB, Keles GE et al. Seizure characteristics and control following resection in 332 patients with low-grade gliomas. J. Neurosurg. 108(2), 227–235 (2008).
19 van Breemen MS, Vecht CJ. Optimal seizure management in brain tumor patients. Curr. Neurol. Neurosci. Rep. 5(3), 207–213 (2005).
20 Herman ST. Clinical trials for prevention of epileptogenesis. Epilepsy Res. 68(1), 35–38 (2006).
21 Glantz MJ, Cole BF, Forsyth PA et al. Practice parameter: anticonvulsant prophylaxis in patients with newly diagnosed brain tumors. Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 54(10), 1886–1893 (2000).
22 Pasquier B, Peoc’H M, Fabre-Bocquentin B et al. Surgical pathology of drug-resistant partial epilepsy. A 10-year-experience with a series of 327 consecutive resections. Epileptic Disord. 4(2), 99–119 (2002).
23 Herman ST. Epilepsy after brain insult: targeting epileptogenesis. Neurology 59(9 Suppl. 5), S21–S26 (2002).
24 Blumcke I, Pauli E, Clusmann H et al. A new clinico-pathological classification system for mesial temporal sclerosis. Acta Neuropathol. 113(3), 235–244 (2007).
25 Wuttke TV, Lerche H. Novel anticonvulsant drugs targeting voltage-dependent ion channels. Expert Opin. Investig. Drugs 15(10), 1167–1177 (2006).
26 Tang B, Sander T, Craven KB, Hempelmann A, Escayg A. Mutation analysis of the hyperpolarization-activated cyclic nucleotide-gated channels HCN1 and HCN2 in idiopathic generalized epilepsy. Neurobiol. Dis. 29(1), 59–70 (2008).
27 Rusconi R, Scalmani P, Cassulini RR et al. Modulatory proteins can rescue a trafficking defective epileptogenic Nav1.1 Na+ channel mutant. J. Neurosci. 27(41), 11037–11046 (2007).
28 Patt S, Steenbeck J, Hochstetter A et al. Source localization and possible causes of interictal epileptic activity in tumor-associated epilepsy. Neurobiol. Dis. 7(4), 260–269 (2000).
29 Lee MC, Kim GM, Woo YJ et al. Pathogenic significance of neuronal migration disorders in temporal lobe epilepsy. Hum. Pathol. 32(6), 643–648 (2001).
30 Perego C, Vanoni C, Bossi M et al. The GLT-1 and GLAST glutamate transporters are expressed on morphologically distinct astrocytes and regulated by neuronal activity in primary hippocampal cocultures. J. Neurochem. 75(3), 1076–1084 (2000).
31 Alonso-Nanclares L, De Felipe J. Vesicular glutamate transporter 1 immunostaining in the normal and epileptic human cerebral cortex. Neuroscience 134(1), 59–68 (2005).
32 Aronica E, Gorter JA, Jansen GH, Leenstra S, Yankaya B, Troost D. Expression of connexin 43 and connexin 32 gap-junction proteins in epilepsy-associated brain tumors and in the perilesional epileptic cortex. Acta Neuropathol. 101(5), 449–459 (2001).
33 Richardson MP, Hammers A, Brooks DJ, Duncan JS. Benzodiazepine-GABAA receptor binding is very low in dysembryoplastic neuroepithelial tumor: a PET study. Epilepsia 42(10), 1327–1334 (2001).
34 di Michele F, Verdecchia M, Dorofeeva M et al. GABA(A) receptor active steroids are altered in epilepsy patients with tuberous sclerosis. J. Neurol. Neurosurg. Psychiatry 74(5), 667–670 (2003).
35 Stefan H, Lopes da Silva FH, Loscher W et al. Epileptogenesis and rational therapeutic strategies. Acta Neurol. Scand. 113(3), 139–155 (2006).
36 Aronica E, Yankaya B, Jansen GH et al. Ionotropic and metabotropic glutamate receptor protein expression in glioneuronal tumours from patients with intractable epilepsy. Neuropathol. Appl. Neurobiol. 27(3), 223–237 (2001).
37 Schaller B. Influences of brain tumor-associated pH changes and hypoxia on epileptogenesis. Acta Neurol. Scand. 111(2), 75–83 (2005).
38 Gu W, Brodtkorb E, Piepoli T, Finocchiaro G, Steinlein OK. LGI1: a gene involved in epileptogenesis and glioma progression? Neurogenetics 6(2), 59–66 (2005).
39 Brodtkorb E, Nakken KO, Steinlein OK. No evidence for a seriously increased malignancy risk in LGI1-caused epilepsy. Epilepsy Res. 56(2–3), 205–208 (2003).
40 Piepoli T, Jakupoglu C, Gu W et al. Expression studies in gliomas and glial cells do not support a tumor suppressor role for LGI1. Neuro Oncol. 8(2), 96–108 (2006).
41 Bartolomei F, Bosma I, Klein M et al. Disturbed functional connectivity in brain tumour patients: evaluation by graph analysis of synchronization matrices. Clin. Neurophysiol. 117(9), 2039–2049 (2006).
•• The first study showing how brain tumors interfere with global brain networks.
42 Bartolomei F, Bosma I, Klein M et al. How do brain tumors alter functional connectivity? A magnetoencephalography study. Ann. Neurol. 59(1), 128–138 (2006).
43 Bartolomei F, Wendling F, Regis J, Gavaret M, Guye M, Chauvel P. Pre-ictal synchronicity in limbic networks of mesial temporal lobe epilepsy. Epilepsy Res. 61(1–3), 89–104 (2004).
44 Bartolomei F, Chauvel P, Wendling F. [Spatio-temporal dynamics of neuronal networks in partial epilepsy]. Rev. Neurol. (Paris) 161(8–9), 767–780 (2005).
45 Stam CJ, Reijneveld JC. Graph theoretical analysis of complex networks in the brain. Nonlinear Biomed. Phys. 1(1), 3 (2007).
46 Bartolomei F, Wendling F, Bellanger JJ, Regis J, Chauvel P. Neural networks involving the medial temporal structures in temporal lobe epilepsy. Clin. Neurophysiol. 112(9), 1746–1760 (2001).
•• Demonstrates how an imbalance in global brain neural networks might induce medically intractable seizures.
47 Stam CJ, Jones BF, Nolte G, Breakspear M, Scheltens P. Small-world networks and functional connectivity in Alzheimer’s disease. Cereb. Cortex 17(1), 92–99 (2007).
48 Duffau H. Brain plasticity: from pathophysiological mechanisms to therapeutic applications. J. Clin. Neurosci. 13(9), 885–897 (2006).
49 Giese A. Glioma invasion – pattern of dissemination by mechanisms of invasion and surgical intervention, pattern of gene expression and its regulatory control by tumorsuppressor p53 and proto-oncogene ETS-1. Acta Neurochir. Suppl. 88, 153–162 (2003).
50 Duffau H, Khalil I, Gatignol P, Denvil D, Capelle L. Surgical removal of corpus callosum infiltrated by low-grade glioma: functional outcome and oncological considerations. J. Neurosurg. 100(3), 431–437 (2004).
Author Pro
of
Brain tumors & epilepsy Review
www.expert-reviews.com 11
51 Duffau H. New concepts in surgery of WHO grade II gliomas: functional brain mapping, connectionism and plasticity – a review. J. Neurooncol. 79(1), 77–115 (2006).
52 Gil Robles S, Gatignol P, Capelle L, Mitchell MC, Duffau H. The role of dominant striatum in language: a study using intraoperative electrical stimulations. J. Neurol. Neurosurg. Psychiatry 76(7), 940–946 (2005).
53 Teixidor P, Gatignol P, Leroy M, Masuet-Aumatell C, Capelle L, Duffau H. Assessment of verbal working memory before and after surgery for low-grade glioma. J. Neurooncol. 81(3), 305–313 (2007).
54 Jourdan MS, Schneider J, Lutschg J, Weber P. Fast improvement of verbal memory function after left temporal tumour resection. Acta Paediatr. 95(10), 1306–1309 (2006).
55 Correa DD, DeAngelis LM, Shi W, Thaler HT, Lin M, Abrey LE. Cognitive functions in low-grade gliomas: disease and treatment effects. J. Neurooncol. 81(2), 175–184 (2007).
56 Tucha O, Smely C, Preier M, Lange KW. Cognitive deficits before treatment among patients with brain tumors. Neurosurgery 47(2), 324–333 (2000).
57 Taphoorn MJ, Klein M. Cognitive deficits in adult patients with brain tumours. Lancet Neurol. 3(3), 159–168 (2004).
•• Good overview of the impact of brain tumors and their treatments on cognitive functions and quality of life.
58 Amaral LA, az-Guilera A, Moreira AA, Goldberger AL, Lipsitz LA. Emergence of complex dynamics in a simple model of signaling networks. Proc. Natl Acad. Sci. USA 101(44), 15551–15555 (2004).
59 Duffau H. The anatomo-functional connectivity of language revisited. New insights provided by electrostimulation and tractography. Neuropsychologia 46, 927–934 (2008).
• Extensive review of the anatomo-functional language connectivity.
60 Liang H, Bressler SL, Ding M, Truccolo WA, Nakamura R. Synchronized activity in prefrontal cortex during anticipation of visuomotor processing. Neuroreport 13(16), 2011–2015 (2002).
61 Lowe MJ, Mock BJ, Sorenson JA. Functional connectivity in single and multislice echoplanar imaging using resting-state fluctuations. Neuroimage 7(2), 119–132 (1998).
62 Salvador R, Suckling J, Schwarzbauer C, Bullmore E. Undirected graphs of frequency-dependent functional connectivity in whole brain networks. Philos. Trans. R. Soc. Lond. B. Biol. Sci. 360(1457), 937–946 (2005).
63 Stam CJ, van Cappellen van Walsum AM, Micheloyannis S. Variability of EEG synchronization during a working memory task in healthy subjects. Int. J. Psychophysiol. 46(1), 53–66 (2002).
64 Schnitzler A, Gross J. Functional connectivity analysis in magnetoencephalography. Int. Rev. Neurobiol. 68, 173–195 (2005).
65 Hadjipapas A, Hillebrand A, Holliday IE, Singh KD, Barnes GR. Assessing interactions of linear and nonlinear neuronal sources using MEG beamformers: a proof of concept. Clin. Neurophysiol. 116(6), 1300–1313 (2005).
66 Marrelec C, Bellec P, Krainik A et al. Regions, systems, and the brain: hierarchical measures of functional integration in fMRI. Med. Image Anal. (2008 ) (In press).
•• A study of connectionism and brain networks with functional MRI.
67 Sporns O, Chialvo DR, Kaiser M, Hilgetag CC. Organization, development and function of complex brain networks. Trends Cogn. Sci. 8(9), 418–425 (2004).
68 Strogatz SH. Exploring complex networks. Nature 410(6825), 268–276 (2001).
69 Halgren E, Boujon C, Clarke J, Wang C, Chauvel P. Rapid distributed fronto-parieto-occipital processing stages during working memory in humans. Cereb. Cortex 12(7), 710–728 (2002).
70 von Stein A, Sarnthein J. Different frequencies for different scales of cortical integration: from local gamma to long range α/θ synchronization. Int. J. Psychophysiol. 38(3), 301–313 (2000).
71 Ponten SC, Bartolomei F, Stam CJ. Small-world networks and epilepsy: graph theoretical analysis of intracerebrally recorded mesial temporal lobe seizures. Clin. Neurophysiol. 118(4), 918–927 (2007).
72 Harter D, Kozma R. Chaotic neurodynamics for autonomous agents. IEEE Trans. Neural. Netw. 16(3), 565–579 (2005).
73 Chavez M, Hwang DU, Amann A, Boccaletti S. Synchronizing weighted complex networks. Chaos 16(1), 015106 (2006).
74 Chavez M, Hwang DU, Amann A, Hentschel HG, Boccaletti S. Synchronization is enhanced in weighted complex networks. Phys. Rev. Lett. 94(21), 218701 (2005).
75 Zhang F, Endo S, Cleary LJ, Eskin A, Byrne JH. Role of transforming growth factor-β in long-term synaptic facilitation in Aplysia. Science 275(5304), 1318–1320 (1997).
76 Jacobs KM, Donoghue JP. Reshaping the cortical motor map by unmasking latent intracortical connections. Science 251(4996), 944–947 (1991).
77 Ivanco TL, Greenough WT. Physiological consequences of morphologically detectable synaptic plasticity: potential uses for examining recovery following damage. Neuropharmacology 39(5), 765–776 (2000).
78 Gross CG. Neurogenesis in the adult brain: death of a dogma. Nat. Rev. Neurosci. 1(1), 67–73 (2000).
79 Nguyen DK, Botez MI. Diaschisis and neurobehavior. Can. J. Neurol. Sci. 25(1), 5–12 (1998).
80 Duffau H. Acute functional reorganisation of the human motor cortex during resection of central lesions: a study using intraoperative brain mapping. J. Neurol. Neurosurg. Psychiatry 70(4), 506–513 (2001).
81 Bavelier D, Neville HJ. Cross-modal plasticity: where and how? Nat. Rev. Neurosci. 3(6), 443–452 (2002).
82 Draganski B, Gaser C, Busch V, Schuierer G, Bogdahn U, May A. Neuroplasticity: changes in grey matter induced by training. Nature 427(6972), 311–312 (2004).
83 Kim OJ, Yong AJ, Chung YS et al. Significance of chronic epilepsy in glial tumors and correlation with surgical strategies. J. Clin. Neurosci. 11(7), 702–705 (2004).
84 Duffau H, Capelle L, Lopes M, Bitar A, Sichez JP, Van ER. Medically intractable epilepsy from insular low-grade gliomas: improvement after an extended lesionectomy. Acta Neurochir. (Wien.) 144(6), 563–572 (2002).
• First study showing seizure outcome after resection of low-grade gliomas within the insula.
85 Riva M. Brain tumoral epilepsy: a review. Neurol. Sci. 26(Suppl. 1), S40–S42 (2005).
86 Bauer R, Dobesberger J, Unterhofer C et al. Outcome of adult patients with temporal lobe tumours and medically refractory focal epilepsy. Acta Neurochir. (Wien.) 149(12), 1211–1216 (2007).

Author Pro
of
12 Expert Rev. Neurother. 8(6), (2008)
Review Brogna, Gil Robles & Duffau
87 Engel J, Jr., Burchfiel J, Ebersole J et al. Long-term monitoring for epilepsy. Report of an IFCN committee. Electroencephalogr. Clin. Neurophysiol. 87(6), 437–458 (1993).
88 Isnard J, Guenot M, Sindou M, Mauguiere F. Clinical manifestations of insular lobe seizures: a stereo-electroencephalographic study. Epilepsia 45(9), 1079–1090 (2004).
•• Recent study demonstrating the role of the insula in refractory epilepsy using stereo-EEG.
89 Wieser HG, Blume WT, Fish D et al. ILAE Commission Report. Proposal for a new classification of outcome with respect to epileptic seizures following epilepsy surgery. Epilepsia 42(2), 282–286 (2001).
90 Karceski S, Morrell MJ, Carpenter D. Treatment of epilepsy in adults: expert opinion, 2005. Epilepsy Behav. 7(Suppl. 1), S1–64 (2005).
91 Wagner GL, Wilms EB, Vecht C. [Levetiracetam: an anti-epileptic drug with interesting pharmacokinetic properties]. Ned Tijdschr Geneeskd 146(26), 1218–1221 (2002).
92 Acharya S, Bussel JB. Hematologic toxicity of sodium valproate. J. Pediatr. Hematol. Oncol. 22(1), 62–65 (2000).
93 Marson AG, Williamson PR, Clough H, Hutton JL, Chadwick DW. Carbamazepine versus valproate monotherapy for epilepsy: a meta-analysis. Epilepsia 43(5), 505–513 (2002).
94 Carreno M. Levetiracetam. Drugs Today (Barc.) 43(11), 769–794 (2007).
95 Wick W, Menn O, Meisner C et al. Pharmacotherapy of epileptic seizures in glioma patients: who, when, why and how long? Onkologie 28(8–9), 391–396 (2005).
96 Berkovic SF, Knowlton RC, Leroy RF, Schiemann J, Falter U. Placebo-controlled study of levetiracetam in idiopathic generalized epilepsy. Neurology 69(18), 1751–1760 (2007).
97 Newton HB, Goldlust SA, Pearl D. Retrospective analysis of the efficacy and tolerability of levetiracetam in brain tumor patients. J. Neurooncol. 78(1), 99–102 (2006).
• Good overview on the new antiepileptic drug levetiracetam.
98 Perry JR, Sawka C. Add-on gabapentin for refractory seizures in patients with brain tumours. Can. J. Neurol. Sci. 23(2), 128–131 (1996).
99 Khan RB, Hunt DL, Thompson SJ. Gabapentin to control seizures in children undergoing cancer treatment. J. Child Neurol. 19(2), 97–101 (2004).
100 Sirven JI, Fife TD, Wingerchuk DM, Drazkowski JF. Second-generation antiepileptic drugs’ impact on balance: a meta-analysis. Mayo Clin. Proc. 82(1), 40–47 (2007).
101 Maschio M, Dinapoli L, Zarabla A et al. Outcome and tolerability of topiramate in brain tumor associated epilepsy. J. Neurooncol. 86(1), 61–70 (2008).
102 Patsalos PN, Perucca E. Clinically important drug interactions in epilepsy: interactions between antiepileptic drugs and other drugs. Lancet Neurol. 2(8), 473–481 (2003).
103 Vecht CJ, Wagner GL, Wilms EB. Interactions between antiepileptic and chemotherapeutic drugs. Lancet Neurol. 2(7), 404–409 (2003).
104 Sondergaard KM, Nielsen KA, Dahl M, Wolf P. Lamotrigine therapeutic thresholds. Seizure (2008) (Epub ahead of print).
105 Maschio M, Albani F, Baruzzi A et al. Levetiracetam therapy in patients with brain tumour and epilepsy. J. Neurooncol. 80(1), 97–100 (2006).
106 Otoul C, Arrigo C, van RK, French JA. Meta-analysis and indirect comparisons of levetiracetam with other second-generation antiepileptic drugs in partial epilepsy. Clin. Neuropharmacol. 28(2), 72–78 (2005).
107 Wagner GL, Wilms EB, van Donselaar CA, Vecht C. Levetiracetam: preliminary experience in patients with primary brain tumours. Seizure 12(8), 585–586 (2003).
108 Bourg V, Lebrun C, Chichmanian RM, Thomas P, Frenay M. Nitroso-urea-cisplatin-based chemotherapy associated with valproate: increase of haematologic toxicity. Ann. Oncol. 12(2), 217–219 (2001).
109 Oberndorfer S, Piribauer M, Marosi C, Lahrmann H, Hitzenberger P, Grisold W. P450 enzyme inducing and non-enzyme inducing antiepileptics in glioblastoma patients treated with standard chemotherapy. J. Neurooncol. 72(3), 255–260 (2005).
110 Eyal S, Yagen B, Sobol E, Altschuler Y, Shmuel M, Bialer M. The activity of antiepileptic drugs as histone deacetylase inhibitors. Epilepsia 45(7), 737–744 (2004).
111 Chavez-Blanco A, Segura-Pacheco B, Perez-Cardenas E et al. Histone acetylation and histone deacetylase activity of magnesium
valproate in tumor and peripheral blood of patients with cervical cancer. A Phase I study. Mol. Cancer 4(1), 22 (2005).
112 Li XN, Shu Q, Su JM, Perlaky L, Blaney SM, Lau CC. Valproic acid induces growth arrest, apoptosis, and senescence in medulloblastomas by increasing histone hyperacetylation and regulating expression of p21Cip1, CDK4, and CMYC. Mol. Cancer Ther. 4(12), 1912–1922 (2005).
113 Tang K, Wong LP, Lee EJ, Chong SS, Lee CG. Genomic evidence for recent positive selection at the human MDR1 gene locus. Hum. Mol. Genet. 13(8), 783–797 (2004).
114 Ben-Menachem E. Levetiracetam: treatment in epilepsy. Expert Opin. Pharmacother. 4(11), 2079–2088 (2003).
115 Siddiqui TS. Febrile convulsions in children: relationship of family history to type of convulsions and age at presentation. J. Ayub. Med. Coll. Abbottabad. 14(4), 26–28 (2002).
116 van Rijckevorsel K, Boon PA. The ‘number needed to treat’ with Levetiracetam (LEV): comparison with the other new antiepileptic drugs (AEDs). Seizure 10(3), 235–236 (2001).
117 Stupp R, Pica A, Mirimanoff RO, Michielin O. [A practical guide for the management of gliomas]. Bull Cancer 94(9), 817–822 (2007).
118 Kaloshi G, ouaich-Amiel A, Diakite F et al. Temozolomide for low-grade gliomas: predictive impact of 1p/19q loss on response and outcome. Neurology 68(21), 1831–1836 (2007).
119 Turnheim K. [Drug interactions with antiepileptic agents]. Wien. Klin. Wochenschr. 116(4), 112–118 (2004).
120 Murry DJ, Cherrick I, Salama V et al. Influence of phenytoin on the disposition of irinotecan: a case report. J. Pediatr. Hematol. Oncol. 24(2), 130–133 (2002).
121 Maschio M, Dinapoli L, Zarabia A, Jandolo B. Issues related to the pharmacological management of patients with brain tumours and epilepsy. Funct. Neurol. 21(1), 15–19 (2006).
122 Stefan H, Wang Y, Pauli E, Schmidt B. A new approach in anti-epileptic drug evaluation. Eur. J. Neurol. 11(7), 467–473 (2004).
123 Gilbar PJ, Brodribb TR. Phenytoin and fluorouracil interaction. Ann. Pharmacother. 35(11), 1367–1370 (2001).
124 Ruegg S. Dexamethasone/phenytoin interactions: neurooncological concerns. Swiss Med. Wkly 132(29–30), 425–426 (2002).
Author Pro
of
Brain tumors & epilepsy Review
www.expert-reviews.com 13
125 Wiener P. Neuroactive steroids, relaxation, and seizure control. Int J. Neurosci. 113(5), 631–639 (2003).
126 Sirven JI, Wingerchuk DM, Drazkowski JF, Lyons MK, Zimmerman RS. Seizure prophylaxis in patients with brain tumors: a meta-analysis. Mayo Clin. Proc. 79(12), 1489–1494 (2004).
127 Soffietti R, Leoncini B, Ruda R. New developments in the treatment of malignant gliomas. Expert Rev. Neurother. 7(10), 1313–1326 (2007).
128 Claus EB, Black PM. Survival rates and patterns of care for patients diagnosed with supratentorial low-grade gliomas: data from the SEER program, 1973–2001. Cancer 106(6), 1358–1363 (2006).
129 Duffau H. [Management of low-grade gliomas]. Rev. Prat. 56(16), 1771–1777 (2006).
130 Boiardi A, Silvani A, Eoli M et al. Treatment of recurrent glioblastoma: can local delivery of mitoxantrone improve survival? J. Neurooncol. 88(1), 105–113 (2008).
131 Devinsky O. Patients with refractory seizures. N. Engl. J. Med. 340(20), 1565–1570 (1999).
132 Loscher W, Potschka H. Role of multidrug transporters in pharmacoresistance to antiepileptic drugs. J. Pharmacol. Exp. Ther. 301(1), 7–14 (2002).
133 Anderson GD, Shen DD. Where is the evidence that p-glycoprotein limits brain uptake of antiepileptic drug and contributes to drug resistance in epilepsy? Epilepsia 48(12), 2372–2374 (2007).
134 Tan NC, Berkovic SF. Prediction of drug resistance in epilepsy: not as easy as ABC. Lancet Neurol. 5(8), 641–642 (2006).
135 Van Vliet EA, van SR, Edelbroek PM, Redeker S et al. Inhibition of the multidrug transporter P-glycoprotein improves seizure control in phenytoin-treated chronic epileptic rats. Epilepsia 47(4), 672–680 (2006).
136 Hermann DM, Kilic E, Spudich A, Kramer SD, Wunderli-Allenspach H, Bassetti CL. Role of drug efflux carriers in the healthy and diseased brain. Ann. Neurol. 60(5), 489–498 (2006).
137 Rogawski MA. New evidence supporting a role for T-type Ca(2+) channels in absence epilepsy and in the action of ethosuximide. Epilepsy Curr. 2(2), 57 (2002).
138 Calatozzolo C, Gelati M, Ciusani E et al. Expression of drug resistance proteins Pgp, MRP1, MRP3, MRP5 and GST-pi in human glioma. J. Neurooncol. 74(2), 113–121 (2005).
139 Aronica E, Gorter JA, Van Vliet EA et al. Overexpression of the human major vault protein in gangliogliomas. Epilepsia 44(9), 1166–1175 (2003).
140 Baltes S, Fedrowitz M, Tortos CL, Potschka H, Loscher W. Valproic acid is not a substrate for P-glycoprotein or multidrug resistance proteins 1 and 2 in a number of in vitro and in vivo transport assays. J. Pharmacol. Exp. Ther. 320(1), 331–343 (2007).
141 Potschka H, Baltes S, Loscher W. Inhibition of multidrug transporters by verapamil or probenecid does not alter blood-brain barrier penetration of levetiracetam in rats. Epilepsy Res. 58(2–3), 85–91 (2004).
142 Goldman B. Multidrug resistance: can new drugs help chemotherapy score against cancer? J. Natl Cancer Inst. 95(4), 255–257 (2003).
143 Duffau H, Capelle L. Preferential brain locations of low-grade gliomas. Cancer 100(12), 2622–2626 (2004).
144 Labyt E, Houdayer E, Cassim F, Bourriez JL, Derambure P, Devanne H. Motor representation areas in epileptic patients with focal motor seizures: a TMS study. Epilepsy Res. 75(2–3), 197–205 (2007).
145 Augustine JR. Circuitry and functional aspects of the insular lobe in primates including humans. Brain Res. Brain Res. Rev. 22(3), 229–244 (1996).
146 Zilles K, Schlaug G, Geyer S et al. Anatomy and transmitter receptors of the supplementary motor areas in the human and nonhuman primate brain. Adv. Neurol. 70, 29–43 (1996).
147 Rivier F, Clarke S. Cytochrome oxidase, acetylcholinesterase, and NADPH-diaphorase staining in human supratemporal and insular cortex: evidence for multiple auditory areas. Neuroimage 6(4), 288–304 (1997).
148 Krainik A, Lehericy S, Duffau H et al. Role of the supplementary motor area in motor deficit following medial frontal lobe surgery. Neurology 57(5), 871–878 (2001).
149 Dronkers NF. A new brain region for coordinating speech articulation. Nature 384(6605), 159–161 (1996).
150 Hatten ME. New directions in neuronal migration. Science 297(5587), 1660–1663 (2002).
151 Rakic P. Molecular and cellular mechanisms of neuronal migration: relevance to cortical epilepsies. Adv. Neurol. 84, 1–14 (2000).
152 Barba C, Doglietto F, Policicchio D, Caulo M, Colicchio G. Unusual ipsilateral hyperkinetic automatisms in SMA seizures. Seizure 14(5), 354–361 (2005).
153 Isnard J, Guenot M, Ostrowsky K, Sindou M, Mauguiere F. The role of the insular cortex in temporal lobe epilepsy. Ann. Neurol. 48(4), 614–623 (2000).
154 Fields RD, Stevens-Graham B. New insights into neuron-glia communication. Science 298(5593), 556–562 (2002).
155 Aubert A, Costalat R, Duffau H, Benali H. Modeling of pathophysiological coupling between brain electrical activation, energy metabolism and hemodynamics: insights for the interpretation of intracerebral tumor imaging. Acta Biotheor. 50(4), 281–295 (2002).
156 Hennessy MJ, Elwes RD, Binnie CD, Polkey CE. Failed surgery for epilepsy. A study of persistence and recurrence of seizures following temporal resection. Brain 123(Pt 12), 2445–2466 (2000).
157 Wolf HK, Campos MG, Zentner J et al. Surgical pathology of temporal lobe epilepsy. Experience with 216 cases. J. Neuropathol. Exp. Neurol. 52(5), 499–506 (1993).
158 Plate KH, Wieser HG, Yasargil MG, Wiestler OD. Neuropathological findings in 224 patients with temporal lobe epilepsy. Acta Neuropathol. 86(5), 433–438 (1993).
159 Panda S, Radhakrishnan VV, Radhakrishnan K, Rao RM, Sarma SP. Electro-clinical characteristics and postoperative outcome of medically refractory tumoral temporal lobe epilepsy. Neurol. India 53(1), 66–71 (2005).
160 Duffau H. Contribution of cortical and subcortical electrostimulation in brain glioma surgery: methodological and functional considerations. Neurophysiol. Clin. 37(6), 373–382 (2007).
161 Duffau H. Intraoperative cortico-subcortical stimulations in surgery of low-grade gliomas. Expert Rev. Neurother. 5(4), 473–485 (2005).
162 Sanai N, Mirzadeh Z, Berger MS. Functional outcome after language mapping for glioma resection. N. Engl. J. Med. 358(1), 18–27 (2008).
163 Ojemann G, Ojemann J, Lettich E, Berger M. Cortical language localization in left, dominant hemisphere. An electrical stimulation mapping investigation in 117 patients. 1989. J. Neurosurg. 108(2), 411–421 (2008).
Author Pro
of
14 Expert Rev. Neurother. 8(6), (2008)
Review Brogna, Gil Robles & Duffau
164 Duffau H, Denvil D, Lopes M et al. Intraoperative mapping of the cortical areas involved in multiplication and subtraction: an electrostimulation study in a patient with a left parietal glioma. J. Neurol. Neurosurg. Psychiatry 73(6), 733–738 (2002).
165 Duffau H, Capelle L, Denvil D et al. The role of dominant premotor cortex in language: a study using intraoperative functional mapping in awake patients. Neuroimage 20(4), 1903–1914 (2003).
166 Duffau H, Denvil D, Capelle L. Long term reshaping of language, sensory, and motor maps after glioma resection: a new parameter to integrate in the surgical strategy. J. Neurol. Neurosurg. Psychiatry 72(4), 511–516 (2002).
167 Duffau H, Gatignol P, Mandonnet E, Peruzzi P, Tzourio-Mazoyer N, Capelle L. New insights into the anatomo-functional connectivity of the semantic system: a study using cortico-subcortical electrostimulations. Brain 128(Pt 4), 797–810 (2005).
168 Duffau H, Gatignol P, Denvil D, Lopes M, Capelle L. The articulatory loop: study of the subcortical connectivity by electrostimulation. Neuroreport 14(15), 2005–2008 (2003).
169 Bartolomeo P, de Schotten MT, Duffau H. Mapping of visuospatial functions during brain surgery: a new tool to prevent unilateral spatial neglect. Neurosurgery 61(6), E1340 (2007).
170 Duffau H, Bauchet L, Lehericy S, Capelle L. Functional compensation of the left dominant insula for language. Neuroreport 12(10), 2159–2163 (2001).
171 Duffau H. Recovery from complete hemiplegia following resection of a retrocentral metastasis: the prognostic value of intraoperative cortical stimulation. J. Neurosurg. 95(6), 1050–1052 (2001).
172 Duffau H, Sichez JP, Lehericy S. Intraoperative unmasking of brain redundant motor sites during resection of a precentral angioma: evidence using direct cortical stimulation. Ann. Neurol. 47(1), 132–135 (2000).
173 Cataltepe O, Turanli G, Yalnizoglu D, Topcu M, Akalan N. Surgical management of temporal lobe tumor-related epilepsy in children. J. Neurosurg. 102(3 Suppl.), 280–287 (2005).
174 Jorge CL, Nagahashi-Marie SK, Pedreira CC et al. Clinical characteristics and surgical outcome of patients with temporal lobe tumors and epilepsy. Arq. Neuropsiquiatr. 58(4), 1002–1008 (2000).
175 Zaatreh MM, Firlik KS, Spencer DD, Spencer SS. Temporal lobe tumoral epilepsy: characteristics and predictors of surgical outcome. Neurology 61(5), 636–641 (2003).
176 Fried I, Kim JH, Spencer DD. Limbic and neocortical gliomas associated with intractable seizures: a distinct clinicopathological group. Neurosurgery 34(5), 815–823 (1994).
177 Peraud A, Meschede M, Eisner W, Ilmberger J, Reulen HJ. Surgical resection of grade II astrocytomas in the superior frontal gyrus. Neurosurgery 50(5), 966–975 (2002).
178 Sugano H, Shimizu H, Sunaga S. Efficacy of intraoperative electrocorticography for assessing seizure outcomes in intractable epilepsy patients with temporal-lobe-mass lesions. Seizure 16(2), 120–127 (2007).
179 Moore PM, Baker GA. The neuropsychological and emotional consequences of living with intractable temporal lobe epilepsy: implications for clinical management. Seizure 11(4), 224–230 (2002).
180 Duffau H, Velut S, Mitchell MC, Gatignol P, Capelle L. Intra-operative mapping of the subcortical visual pathways using direct electrical stimulations. Acta Neurochir. (Wien.) 146(3), 265–269 (2004).
181 Duffau H, Capelle L, Sichez N et al. Intraoperative mapping of the subcortical language pathways using direct stimulations. An anatomo-functional study. Brain 125(Pt 1), 199–214 (2002).
182 Mandonnet E, Nouet A, Gatignol P, Capelle L, Duffau H. Does the left inferior longitudinal fasciculus play a role in language? A brain stimulation study. Brain 130(Pt 3), 623–629 (2007).
183 Aronica E, Redeker S, Boer K et al. Inhibitory networks in epilepsy-associated gangliogliomas and in the perilesional epileptic cortex. Epilepsy Res. 74(1), 33–44 (2007).
184 Mittelbronn M, Schittenhelm J, Lemke D et al. Low grade ganglioglioma rapidly progressing to a WHO grade IV tumor showing malignant transformation in both astroglial and neuronal cell components. Neuropathology 27(5), 463–467 (2007).
185 Salanova V, Markand O, Worth R. Temporal lobe epilepsy: analysis of patients with dual pathology. Acta Neurol. Scand. 109(2), 126–131 (2004).
186 Roper SN, Levesque MF, Sutherling WW, Engel J Jr. Surgical treatment of partial epilepsy arising from the insular cortex.
Report of two cases. J. Neurosurg. 79(2), 266–269 (1993).
187 Ebeling U, Kothbauer K. Circumscribed low grade astrocytomas in the dominant opercular and insular region: a pilot study. Acta Neurochir. (Wien.) 132(1–3), 66–74 (1995).
188 Yasargil MG, Reeves JD. Tumours of the limbic and paralimbic system. Acta Neurochir. (Wien.) 116(2–4), 147–149 (1992).
189 Zentner J, Meyer B, Stangl A, Schramm J. Intrinsic tumors of the insula: a prospective surgical study of 30 patients. J. Neurosurg. 85(2), 263–271 (1996).
190 Isnard J, Mauguiere F. [The insula in partial epilepsy]. Rev. Neurol. (Paris) 161(1), 17–26 (2005).
191 Ostrowsky K, Isnard J, Ryvlin P, Guenot M, Fischer C, Mauguiere F. Functional mapping of the insular cortex: clinical implication in temporal lobe epilepsy. Epilepsia 41(6), 681–686 (2000).
192 Petrides M, Pandya DN. Efferent association pathways from the rostral prefrontal cortex in the macaque monkey. J. Neurosci. 27(43), 11573–11586 (2007).
193 Duffau H, Capelle L, Lopes M, Faillot T, Sichez JP, Fohanno D. The insular lobe: physiopathological and surgical considerations. Neurosurgery 47(4), 801–810 (2000).
194 Lang FF, Olansen NE, DeMonte F et al. Surgical resection of intrinsic insular tumors: complication avoidance. J. Neurosurg. 95(4), 638–650 (2001).
195 Munari C, Musolino A, umas-Duport C et al. Correlation between stereo-EEG, CT-scan and stereotactic biopsy data in epileptic patients with low-grade gliomas. Appl. Neurophysiol. 48(1–6), 448–453 (1985).
196 Gil Robles S, Tancu H, El Fertit H et al. Stereo EEG of insular cortex with occipito-insular electrodes in temporal plus or fronto-opercular epilepsy. Presented at: ESSFN 2006 (18th Congress). Montreaux, Switzerland 2006.
197 Schiffbauer H, Ferrari P, Rowley HA, Berger MS, Roberts TP. Functional activity within brain tumors: a magnetic source imaging study. Neurosurgery 49(6), 1313–1320 (2001).
198 Kozma R, Puljic M, Balister P, Bollobas B, Freeman WJ. Phase transitions in the neuropercolation model of neural populations with mixed local and non-local interactions. Biol. Cybern. 92(6), 367–379 (2005).
Author Pro
of
Brain tumors & epilepsy Review
www.expert-reviews.com 15
199 Micheloyannis S, Pachou E, Stam CJ et al. Small-world networks and disturbed functional connectivity in schizophrenia. Schizophr. Res. 87(1–3), 60–66 (2006).
200 Reijneveld JC, Ponten SC, Berendse HW, Stam CJ. The application of graph theoretical analysis to complex networks in the brain. Clin. Neurophysiol. 118(11), 2317–2331 (2007).
201 Khan RB, Onar A. Seizure recurrence and risk factors after antiepilepsy drug withdrawal in children with brain tumors. Epilepsia 47(2), 375–379 (2006).
202 Mathieu D, Kondziolka D, Niranjan A, Flickinger J, Lunsford LD. Gamma knife radiosurgery for refractory epilepsy caused by hypothalamic hamartomas. Stereotact. Funct. Neurosurg. 84(2–3), 82–87 (2006).
203 Chalifoux R, Elisevich K. Effect of ionizing radiation on partial seizures attributable to malignant cerebral tumors. Stereotact. Funct. Neurosurg. 67(3–4), 169–182 (1996).
204 Warnke PC, Berlis A, Weyerbrock A, Ostertag CB. Significant reduction of seizure incidence and increase of
benzodiazepine receptor density after interstitial radiosurgery in low-grade gliomas. Acta Neurochir. Suppl. 68, 90–92 (1997).
205 Schrottner O, Unger F, Eder HG, Feichtinger M, Pendl G. Gamma-knife radiosurgery of mesiotemporal tumour epilepsy observations and long-term results. Acta Neurochir. Suppl. 84, 49–55 (2002).
206 Hildebrand J. Management of epileptic seizures. Curr. Opin. Oncol. 16(4), 314–317 (2004).
207 Brada M, Viviers L, Abson C et al. Phase II study of primary temozolomide chemotherapy in patients with WHO grade II gliomas. Ann. Oncol. 14(12), 1715–1721 (2003).
208 Pace A, Vidiri A, Galie E et al. Temozolomide chemotherapy for progressive low-grade glioma: clinical benefits and radiological response. Ann. Oncol. 14(12), 1722–1726 (2003).
Affiliations
• Christian Brogna, MDDepartment of Neuroscience – Neurosurgery, “Sapienza” University of Rome, Viale del Policlinico, 155, 00185 Rome, ItalyTel.: +39 064 940 942Fax: +39 064 940 [email protected]
• Santiago Gil Robles, MDDepartment of Neurosurgery, Hôpital Gui de Chauliac, CHU de Montpellier, 80 Avenue Augustin Fliche, 34295 Montpellier Cedex 5, FranceTel.: +33 467 33 6612Fax: +33 467 33 [email protected]
• Hugues Duffau, MD, PhDDepartment of Neurosurgery, CNRS UMR 8189 and INSERM U678, Hôpital Gui de Chauliac, CHU de Montpellier, 80 Avenue Augustin Fliche, 34295 Montpellier Cedex 5, FranceTel.: +33 467 33 6612Fax: +33 467 33 [email protected]





























