Embed Size (px)
Citation preview
Biliary Sequelae following Radioembolizationwith Yttrium-90 Microspheres
Bassel Atassi, MD, Affaan K. Bangash, DO, Robert J. Lewandowski, MD, Saad Ibrahim, MD, Laura Kulik, MD,Mary F. Mulcahy, MD, Ravi Murthy, MD, Robert K. Ryu, MD, Kent T. Sato, MD, Frank H. Miller, MD,Reed A. Omary, MD, and Riad Salem, MD, MBA
PURPOSE: Yttrium-90 (90Y) radioembolization has emerged as a promising and safe therapeutic modality for patientswith hepatocellular carcinoma (HCC) or metastatic liver cancer. The present report describes biliary sequelaefollowing intraarterial 90Y therapy in patients with HCC or liver metastases.
MATERIALS AND METHODS: All patients were treated with 90Y therapy according to standard lobar treatmentprotocol. Pre- and posttreatment imaging, liver function tests, and serum total bilirubin measurements were per-formed. Three to 6 months after treatment, biliary sequelae were evaluated with computed tomography and magneticresonance imaging, and any liver-related laboratory adverse events were noted.
RESULTS: A total of 327 patients (HCC, n � 190; liver metastases, n � 137) received 569 infusions of 90Y. At follow-upimaging, 33 patients (10.1%; liver metastases, n � 26; HCC, n � 7) had 40 imaging findings related to the biliary tree,including biliary necrosis (n � 17), biloma (n � 3), cholecystitis (n � 2), gallbladder wall enhancement (n � 6),gallbladder wall rent (n � 3), abscess (n � 1), and stricture (n � 8). A total of 31 patients exhibited grade 3/4 bilirubintoxicities (13 [6.8%] with HCC, 18 [13.1%] with liver metastases). Unplanned interventions prompted by biliarysequelae were necessary in six of 327 patients (1.8%).
CONCLUSIONS: 90Y therapy in patients with HCC or metastatic disease to the liver is associated with an acceptablerate of biliary toxicities. Further studies assessing long-term biliary sequelae are warranted.
J Vasc Interv Radiol 2008; 19:691–697
Abbreviations: HCC � hepatocellular carcinoma, RF � radiofrequency, TACE � transcatheter arterial chemoembolization
THE debate on minimally invasiveliver-directed therapies for primaryand/or metastatic disease continues toexpand. In the past decade, nonsurgi-cal percutaneous locoregional thera-pies have included radiofrequency(RF) ablation, cryoablation, and percu-
From the Department of Radiology, Section of Inter-ventional Radiology (B.A., A.K.B., R.J.L., R.K.R.,K.T.S., F.H.M., R.A.O., R.S.), and Department ofMedicine, Division of Hematology and Oncology(M.K.M., R.S.), Robert H. Lurie Comprehensive Can-cer Center, Northwestern Memorial Hospital; andDepartment of Hepatology (L.K.), NorthwesternMemorial Hospital, 676 North St. Clair Street, Suite800, Chicago, Illinois 60611; and Division of Diag-nostic Imaging, Interventional Radiology Section
(R.M.), The University of Texas M. D. AndersonCancer Center, Houston, Texas. Received August 27,taneous ethanol ablation in the effec-tive treatment of small liver tumors(1), whereas transcatheter arterial che-moembolization (TACE) and trans-catheter arterial embolization haveshown to be effective in larger liverlesions given appropriate selection cri-
2007; final revision received and accepted January 2,2008. Address correspondence to R.S.; E-mail:[email protected]
From the SIR 2007 Annual Meeting.
R.S. is a consultant for MDS Nordion, Ottawa, ON,Canada. None of the other authors have identified aconflict of interest.
© SIR, 2008
DOI: 10.1016/j.jvir.2008.01.003
teria (2). Recently, yttrium-90 (90Y) ra-dioembolization has gained further ac-ceptance for the treatment ofhepatocellular carcinoma (HCC) andmetastatic liver disease (3). Despitepromising clinical results, radioembo-lization may result in early and latecomplications (3,4).
Although complications involvingthe biliary tree have been reportedwith other locoregional therapies,studies outlining the biliary sequelaeof radioembolization have been lim-ited. General complications of radio-embolization have been described (3),but specific biliary sequelae after 90Ymicrosphere treatment in patientswith HCC and/or liver metastases arescarce. Herein we describe biliary se-
quelae after 90Y therapy diagnosed on691
692 • Biliary Sequelae after Radioembolization with 90Y Microspheres May 2008 JVIR
the basis of radiographic imaging andlaboratory values.
MATERIALS AND METHODS
Patient Population
Between 2001 and 2006, 327 pa-tients were treated with 90Y radioem-bolization therapy at two institutions.The institutional review boards at bothinstitutions approved the study proto-col and all patients signed informedconsent allowing the use of their data.This study was compliant with theHealth Insurance Portability and Ac-countability Act. All patients were re-ferred to the interventional radiologydepartment for treatment by medical,surgical, or transplant oncology. Pa-tient selection criteria for treatmentwith radioembolization included (i)confirmed diagnosis of HCC or meta-static cancer to the liver on computedtomography (CT); (ii) unresectableliver tumor; (iii) Eastern CooperationOncology Group performance statusof 0–3; (iv) adequate pulmonary func-tion test findings; (v) adequate hema-tologic parameters (granulocyte count�1.5 � 109/L, platelet count �50 �109/L), renal function (creatinine level�2.0 mg/dL), and liver function; and(vi) ability to undergo angiographyand selective visceral catheterization.Exclusion criteria included (i) anyother liver therapy planned for cancertreatment, (ii) life expectancy less than3 months, (iii) uncorrectable flow tothe gastrointestinal tract, and (iv) esti-mated radiation doses to the lungsgreater than 30 Gy in a single admin-istration or 50 Gy in multiple admin-istrations (5). Patients with metastaticdisease had failed standard-of-carepolychemotherapy.
Yttrium-90 Treatment
TheraSphere (90Y microspheres;
Table 1National Cancer Institute Common Toxi
Toxicity G
Aminotransferases/alkalinephosphatase
�2.
Bilirubin �1.
Note.—ULN � upper limit of normal.
MDS Nordion, Ottawa, ON, Canada)
is approved under a HumanitarianDevice Exemption for the treatment ofunresectable HCC with or withoutportal vein thrombosis. Investigatorsare directed to published Food andDrug Administration guidelines onthe use of this device in conditions thatdeviate from the approved indication.It is comprised of nonbiodegradableglass microspheres with 90Y as an es-sential constituent. The microspheresare supplied in 0.5 mL of sterile pyo-gen-free water contained in a 0.3-mLV-bottom vial secured within a 12-mmclear acrylic vial shield. Ninety-fivepercent of microspheres range in di-ameter between 15 �m and 35 �m.Yttrium-90 is a pure �-emitter that de-cays to stable zirconium Zr 90 with ahalf-life of 64.1 days. The average en-ergy of �-emission is 0.9367 MeV, witha mean tissue penetration of 2.5 mmand a maximum penetration of 10mm. One gigabecquerel (27 mCi) of90Y per kilogram of tissue provides adose of 50 Gy (6,7). The method forcalculating the required activity for in-jection and the dose delivered to targettissue with and without lung shuntfraction calculations have been previ-ously published (7).
Before treatment, baseline CT ormagnetic resonance (MR) images andlaboratory test results, including liverfunction tests, complete blood count,and coagulation profile, were obtainedon the day of first 90Y treatment for allpatients. A baseline angiogram wasobtained to determine proper hepaticvasculature for placement of the cath-eter and identification of any aberrantor collateral vessels. As described byprevious authors (8), prophylactic em-bolization of extrahepatic vessels wasundertaken (eg, right gastric, gas-troduodenal). Estimated lung shunt-ing was calculated with a technetiumTc 99m macroaggregated albuminscan, and the estimated dose of 90Y to
Criteria Version 3.0
de 1 Grade 2
ULN �2.5–5.0 � ULN
ULN �1.5–3.0 � ULN
the lungs was calculated. Microsphere
treatment was administered in a lobartreatment fashion, wherein one lobewas treated per treatment session. Theother lobe was treated 30–90 dayslater. After each treatment, patientswere observed for 6 hours and dis-charged home the same day.
Data Collection and Definition ofOutcome Measures
All data were collected prospec-tively. Patient reevaluation was per-formed at standard follow-up exami-nations scheduled initially at 1 monthand every 3 months thereafter. At eachfollow-up visit, patients were assessedclinically for signs and symptoms oftumor response and/or treatment tox-icity hematologically with liver func-tion tests and radiographically withCT or MR imaging. Findings related tothe biliary tree were identified by fourradiologists. Specifically, images werereviewed for the presence of biliarysequelae including biliary strictures,bilomas, biliary necrosis, and chole-cystitis. Because pathologic proof wasunobtainable for most of these find-ings, the following evidence was usedif not present before radioemboliza-tion: (i) biliary stricture in the form ofperipheral or biliary ductal dilation;(ii) bilomas, ie, large fluid-filled collec-tion usually requiring drainage; (iii)biliary necrosis in the form of multiplesmall, cystic-appearing structures notusually requiring drainage; (iv) chole-cystitis, ie, gallbladder wall enhance-ment and/or disruption and/or peri-cholecystic fluid on CT/MR imaging.
For the purposes of this analysis, abiliary sequela was defined as any bil-iary imaging finding and/or liverfunction–based adverse event ofgrade 3/4 severity based on the Com-mon Toxicity Criteria of the NationalCancer Institute (version 3.0; Table 1)occurring any time in the process dur-
Grade 3 Grade 4
5.0–20 � ULN �20 � ULN
3.0–10.0 � ULN �10.0 � ULN
city
ra
5 � �
5 � �
ing the entire follow-up period (9). No
l de sta
Atassi et al • 693Volume 19 Number 5
time cut-off point was applied. Also,given the significant clinical differ-ences between HCC and metastases,separate analyses were performed foreach patient group.
RESULTS
Imaging Biliary Complications
A total of 327 patients (HCC, n �190; liver metastases; n � 137) re-ceived 569 90Y infusions with a targetdose of 120 Gy � 10%. Mean imagingfollow-up time was 270 days. Risk fac-tors for biliary sequelae were as fol-lows: in the HCC group, 14 had pre-
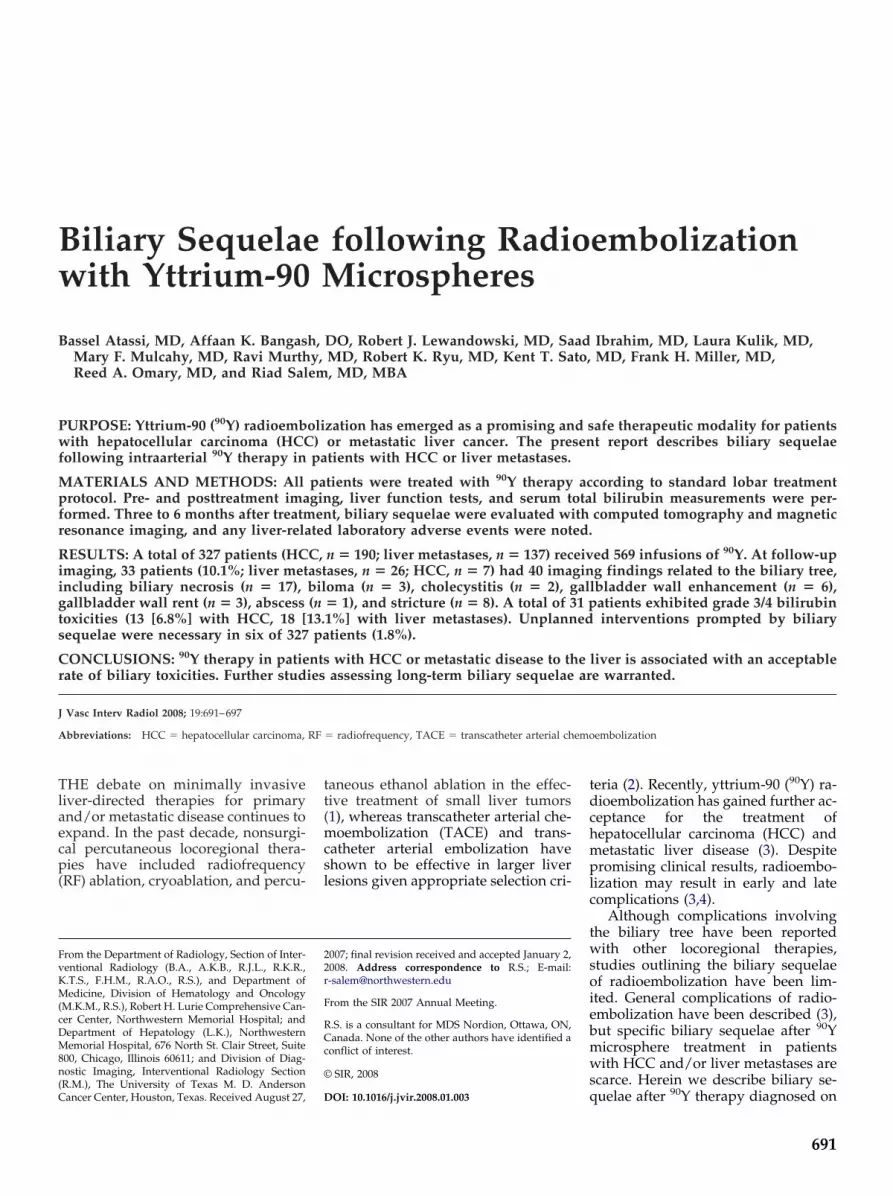
Figure 1. Images from a 59-year-old manwith 90Y microspheres. (a) Axial T1-weightehepatic lobe shows small, hypoenhancingenhancement in the right lobe, consistent wbiliary tree. (c) CT demonstrates successfu
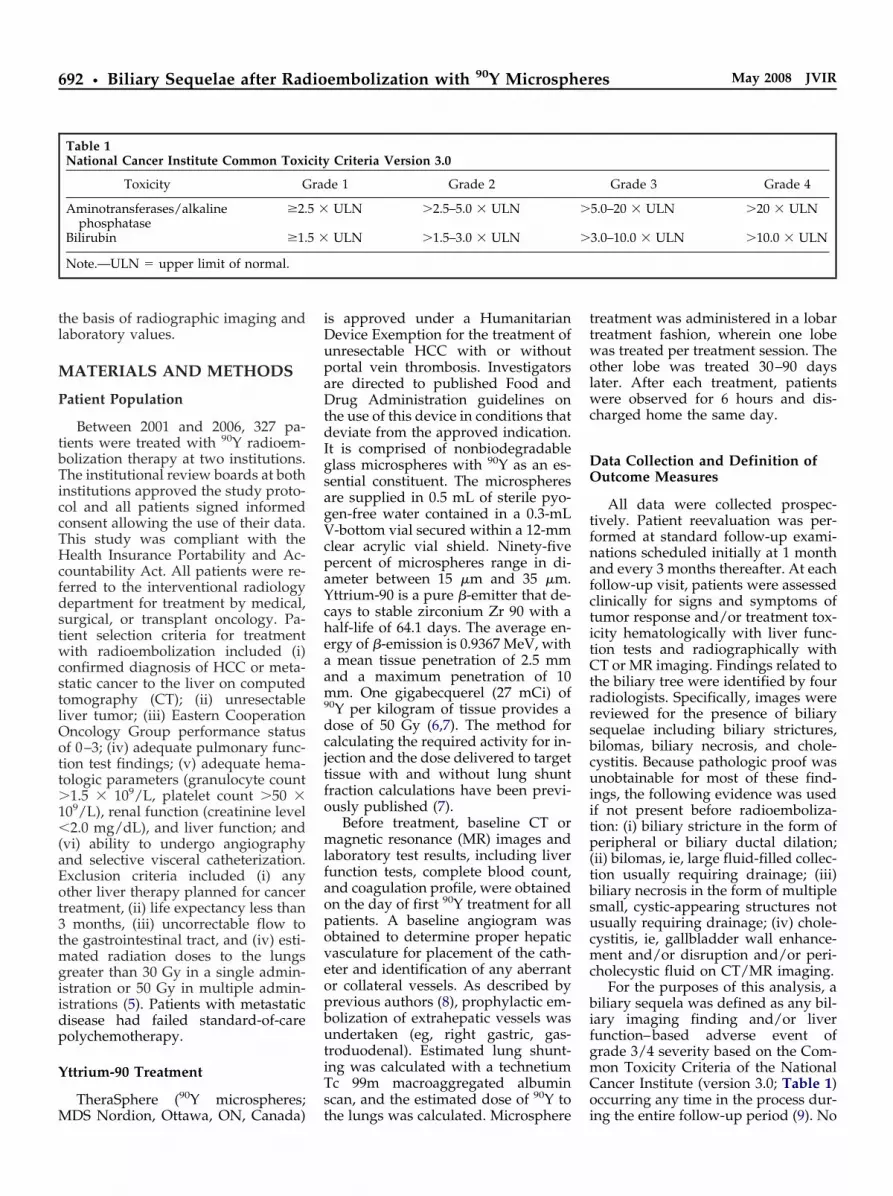
Figure 2. Axial CT images in a patient wi4 weeks earlier demonstrates disruption o(arrow). Hematoxylin and eosin stain shcholecystectomy.
vious TACE and none had biliary-
enteric anastomosis; and amongpatients with liver metastases, ninehad previous TACE and one had bili-ary-enteric anastomosis.
At follow-up imaging, 33 patients(10.1%; liver metastases, n � 26; HCC,n � 7) showed 40 imaging findingsrelated to the biliary tree. Seventeenpatients (3.9%) exhibited demon-strated biliary necrosis on follow-upimaging (14 patients with metastaticliver cancer and three with HCC). Ofthese, three cases (1%) of biliary necro-sis developed, leading to a largebiloma formation requiring percutane-ous drainage (Fig 1). There were two
th liver metastases from rectal melanomaat-suppressed gadolinium-enhanced MR imetastatic lesions in the left lobe and nonbiloma. (b) A drainage catheter has been
compression of the biliary tree. New meta
etastatic disease to the liver from a primare gallbladder wall (arrow, a). (b) Microsps hemorrhage and inflammation in the
cases (0.6%) of radiation-induced cho-
lecystitis requiring surgery (Fig 2).There were six cases (1.8%) of in-creased gallbladder enhancement andthree cases (0.9%) of asymptomaticgallbladder wall disruption (Fig 3).One patient (0.3%) developed hepaticabscess (Fig 4) and eight (2.4%) pre-sented with biliary stricture after 90Ytherapy (Fig 5). None of the patientswith strictures exhibited clinicalsymptoms or laboratory toxicities.Overall, unplanned interventions as aresult of biliary sequelae after 90Y werenecessary in six of 327 patients (1.8%;three biloma drainages, one abscessdrainage, two cholecystectomies).
h infected hepatic bilomas after treatmente obtained 25 weeks after treatment of rightancing lesions with peripheral thick rimced and confirms communication with thetic lesions have appeared.
reast tumor treated with 90Y microspheresre is identified in the gallbladder mucosallbladder wall in the same patient after
wi witd f agm enhith pla
th m y bf th heow ga
In the two patients who underwent

694 • Biliary Sequelae after Radioembolization with 90Y Microspheres May 2008 JVIR
cholecystectomy, the decision to per-form surgery was based on one ormore of the following clinical findings:persistent right upper quadrant painand/or tenderness after treatment,nausea/vomiting, narcotic require-ment for pain management, clinical di-agnosis of surgical cholecystitis byphysical examination, and CT/MR/ultrasound imaging findings of chole-cystitis.
Biochemical Toxicities
Mean laboratory follow-up timewas greater than 300 days (range, 140–1,533 d). Seventy-six and 90% of pa-tients with HCC and metastases, re-spectively, presented with normalbaseline bilirubin levels before treat-ment (�1.3 mg/dL). After treatment,grade 3/4 toxicities involved alkalinephosphatase (HCC; n � 3; metastases,n � 11), aspartate/alanine amino-transferase (n � 13; metastases, n �15), and total bilirubin (n � 13; metas-tases, n � 18). Overall, symptomatic orasymptomatic toxicities were seen in29 patients with HCC (15.2%) and 44patients with metastases. Overall totalbilirubin toxicity was seen in 31 pa-tients (9.5%) among the entire cohortduring the entire follow-up period.
Figure 3. In a patient with metastatic dispancreatic primary tumor, an apparent rent(arrow) is noted after treatment. The patiand did not require any intervention.
Table 2 lists the complications as de-
fined by the standards established bythe Society of Interventional Radiol-ogy (10,11).
DISCUSSION
Previously, the most commonly re-ported complications of radioemboli-zation have included nontarget radia-tion effects such as gastrointestinalulceration, pancreatitis, radiationpneumonitis, and radiation hepatitis(3,12,13). Although studies have re-ported treatment-related biliarycomplications associated with exter-nal-beam radiation (14,15), livertransplantation (16,17), TACE (18–21),RF ablation (4,22–24), and intraarterialchemotherapy (25–30), few studieshave reported on specific biliary find-ings after 90Y radioembolization.Among others, biloma formation aftertherapy, bile duct strictures and/or di-lations, biliary cysts, cholangitis, cho-lecystitis, and gallbladder infarctionhave been some of the most commonlyreported biliary complications (4,16–18,20–23,25–31). Of the 327 patients inthis report, 33 (10.1%) exhibited 40 im-aging complications related to the bil-iary tree.
Experience with TACE has identi-fied various biliary complications in-
e to the liver from athe gallbladder wallwas asymptomatic
Figure 4. Contrast mastatic pancreatic cana history of Whippllesion containing fluipatient was successfantibiotics.
cluding biloma formation (18–21), fo-
cal strictures of bile ducts (20), diffusedilation of intrahepatic bile ducts (20),gallbladder infarction/necrosis (19,30),bile duct necrosis (29), and cystic arteryocclusion (29). Biloma formation as acomplication of intrahepatic chemoem-bolic agents can result in cholangitis orabscess formation secondary to biliarystasis (19). In one of the largest studies toanalyze the occurrence of biloma, Saka-moto et al (19) treated 972 patients withchemoembolization with gelatin spongeand anticancer drugs and reported that3.6% of all patients treated developedintrahepatic biloma. In patients withHCC (n � 920) and those with meta-static liver disease (n � 52), 3.3% and9.6% of patients developed intrahepaticbiloma, respectively. Follow-up CT wasperformed at scheduled intervals, andbiloma appeared as a round solitary ormultiple cystic areas. Among patientswith HCC and those with metastases,the risk of bile duct injury was greater inpatients with intrahepatic biliary ductdilation, those with tumors smaller than5 cm, and those without portal veinthrombosis (19). Similar to our experi-ence, the incidence of biliary necrosiswas higher in metastatic disease versusprimary HCC, which is possibly relatedto the well known protective effect ofhypertrophied peribiliary plexus in
ium–enhanced CT after treatment of met-to the right hepatic lobe in a patient withrgery shows focal, peripheral enhancing
nd air, suspicious for hepatic abscess. Thetreated with percutaneous drainage and
easin
ent
edcer
e sud aully
cases of cirrhosis and the significant che-

atio
Atassi et al • 695Volume 19 Number 5
motherapy history in patients with me-tastases (32).
Makuuchi et al (29) reported bileduct necrosis in two of 29 patients(7%) treated with gelatin powder viathe common hepatic artery, in addi-tion to gallbladder necrosis in 12 of 29patients. Similarly, another study (30)reported gallbladder infarction in sixof eight patients and cystic arteryocclusion in all patients treated withgelatin sponge powder via the righthepatic artery. Infarction of the gall-bladder was noted despite distalplacement of the catheter tip to thecystic artery during embolization. Thiswas based on reflux of embolic mate-rials into the cystic artery. A study of807 patients treated via the commonhepatic artery with gelatin sponge par-ticles and iodized oil (20) reported bil-iary complications in only 2% of pa-tients. Of all complications, 71% weresubcapsular bilomas, 17% were focalstrictures of the common hepatic orcommon bile duct, and 12% showeddiffuse mild dilation of the intrahe-patic bile duct. The authors suggested
Figure 5. Pretreatment MR image showslateral aspect of the right lobe of the livresolution of the mass. However, biliary dil
Table 2Incidence of Biliary ComplicationsAccording to Society of InterventionalRadiology Standards
Type Minor Major
HCC 13 (6.8) 0Liver metastases 18 (13.1) 6 (4.4)
Note.—Increased aminotransferase andalkaline phosphatase levels are notconsidered complications. Values inparentheses are percentages.
an association of biloma formation
with iodized oil rather than gelatinsponge. Although a wide range of the-ories draw attention to the variouscauses of biliary complications in se-lect patients treated with TACE, simi-lar complications are seen with othertherapeutic modalities. The 3.9% inci-dence of biliary necrosis in this studyis comparable to other reports ofTACE.
Biliary complications have been re-ported with intraarterial chemother-apy. Botet et al (28) reported cholangi-tis in approximately 7% of patients (n� 87) treated with intraarterial chemo-therapy infused via an implantableport for metastatic colorectal carci-noma to the liver. Patterns of segmen-tal narrowing similar to cholangitiswere demonstrated on cholangio-grams in these patients. Cholangitiswas seen in patients with less meta-static disease (25%) compared with pa-tients with a higher metastatic burden(42%). Similarly, Shea et al (26) re-ported radiologic biliary abnormalitiessimilar to those encountered in scle-rosing biliary cholangitis in 15% of pa-tients (17 of 110) treated with intraar-terial chemotherapy for colorectalcarcinoma metastatic to the liver. Nofactors were identified to predictwhich patients were most susceptibleto biliary sclerosis and strictures, andthe incidence of biliary strictures wasreported to range from 8% to 26% withintraarterial chemotherapy (26). Theincidence of biliary strictures waslower in our cohort (2.4%).
A large multicenter study (4) re-ported two major complications in-volving the biliary tree after percuta-neous internally cooled RF ablation of
oral mass with low signal intensity in theAfter treatment, there is near-complete
n secondary to focal stricture is identified.
liver lesions in 2,320 patients with pri-
mary HCC and/or metastatic liverdisease. In addition to other minor bil-iary complications, the investigatorsreported a large biloma requiringdrainage in one case and biliary stric-ture requiring stent placement in an-other. Complications such as biliarystrictures have also been reported inoperative RF ablation (23). Additionalstudies have reported a range of prev-alence of biliary complications, includ-ing biliary strictures (0.07%) (4) andbiloma formation (0.2%) (4), after RFablation (24). Notwithstanding thereported therapeutic effects of RF ab-lation, biliary complications are com-mon and require strategic pretreat-ment planning and early detection (4).
In the present study, we report bil-iary sequelae assessed on imaging in327 patients treated with 90Y radioem-bolization with TheraSphere. These in-clude (i) biliary insult including necro-sis, focal obstruction, and strictureformation; (ii) biloma formation; (iii)radiation-induced cholecystitis; (iv)hepatic abscess; and (v) serum biliru-bin and/or aminotransferase toxicity.Because a few studies have reportedthe biliary findings of 90Y radioembo-lization of liver lesions, some compar-ison versus the reported complicationsof TACE, RF ablation, and radiationtherapy can be made. Perhaps the clos-est comparisons can be made with thereported biliary complications ofTACE and radiation therapy (18–21,33,34). In addition to biliary stricturereported as a short-term biliary com-plications of TACE, other biliary com-plications were seen with 90Y therapy.Microscopic injury to the biliary treehas been postulated as the cause ofmany of these complications.
Bilomas result from bile duct leakcaused by insult to the biliary tree andcan be solitary or multiple. They mayoccur after biliary surgery or livertransplantation or as a result of non-surgical iatrogenic causes such as per-cutaneous cholangiography, liver bi-opsy, or biliary drainage (35,36). Morerecently, biloma has been reported af-ter TACE, intraarterial chemotherapy,and RF ablation (18–21,24–30). Bilomaformation secondary to regional dam-age to the peribiliary plexus and/orcholestasis may resolve spontane-ously, whereas some may require per-cutaneous drainage. Given the similar-ity in size of the peribiliary vascular
tumer.
plexus and the 20–60-�m 90Y spheres

696 • Biliary Sequelae after Radioembolization with 90Y Microspheres May 2008 JVIR
injected, the possibility of local micro-vascular injury with 90Y microsphereshas been theorized (3). Seventeen pa-tients developed biliary necrosis onimaging follow-up. Three developedlarge biloma that required interven-tion, likely as a result of irradiation ofthe biliary tree.
Strictures of the intrahepatic bileducts mainly result from sclerosingcholangitis or recurrent pyogeniccholangitis (ie, “oriental cholangio-hepatitis”), whereas benign stricturesof the extrahepatic ducts result mainlyfrom surgical trauma during routinebiliary surgery (36). In addition, focalstrictures may form from ischemia sec-ondary to chronic inflammation andsubsequent fibrosis seen with RF abla-tion (23) and repeated embolization(20). Microscopic injury to the 30-�mperibiliary plexus from microemboli-zation with 90Y microspheres (20–60�m) has been proposed (3). Most bili-ary complications we encounteredwere incidentally noted on routine fol-low-up imaging in asymptomatic pa-tients after 90Y radioembolization ther-apy. In fact, most patients initiallypresented with biliary obstruction sec-ondary to tumoral mass effect, whichsubsequently resolved after 90Y ther-apy. In addition, it is difficult to assesswhether the bilomas seen in our pa-tient population were secondary to tu-mor compression or radiation injuryfrom 90Y therapy. Overall, we notedmore biliary imaging sequelae in pa-tients with metastatic disease com-pared with primary HCC, similar toexperiences with TACE (19). In the pa-tients with metastatic liver disease,previous systemic chemotherapy mayhave increased susceptibility to biliaryinjury by disrupting the usual hepaticvasculature (and occasionally the bili-ary vasculature) to some degree. Inthis cohort of 327 patients, the incidenceof biliary sequelae was comparable tothose reported with other liver-directedtherapies.
It is well known that the peribiliaryvascular plexus is supplied in part bythe cystic artery, commonly arisingfrom the right hepatic artery (3,37).This plexus drains into the portal ve-nous system or directly into the he-patic sinusoids. However, variation oforigin of the cystic artery may includethe left hepatic artery, proper hepaticartery, gastroduodenal artery, celiac
trunk, and many others (37). Althoughcare is taken to avoid occlusion of thecystic or accessory cystic arteries byplacement of the microcatheter distalto the origin of the cystic artery if pos-sible, gallbladder necrosis may resultfrom occlusion of its blood supply.Complications of cholecystitis, gall-bladder necrosis, and bile duct necro-sis have been reported with TACE(19,29,30,38). In some patients, symp-toms of biliary dyskinesia after 90Ymay include right upper quadrantpain and recurrent pain after meals. Inmore serious cases of gallbladder in-jury and cholecystitis, the patient mayexhibit fever, nausea, and vomiting.Radiation-induced cholecystitis hasbeen reported with 90Y microspheretherapy (39). In addition, there doesnot appear to be a correlation betweenimaging findings and clinical symp-toms of cholecystitis after 90Y therapy.Treatment for radiation-induced cho-lecystitis is dependent on the severityof the disease and the patient’s medi-cal history. Treatment options includeantibiotics or cholecystectomy, de-pending on the clinical scenario (40).In the present study, only two patientswith radiation-induced cholecystitisrequired surgical management.
Microorganisms access the hepaticparenchyma via ascending cholangi-tis, chronic biliary colonization, orportal pyemia (36). Several hepatic in-terventions may result in hepatic ab-scess, such as RF ablation, bland em-bolization, and TACE (18–21,24–30).Yttrium-90 therapy can also result inhepatic abscess, particularly in pa-tients with an incompetent ampulla ofVater (eg, hepaticoenterostomy). Clin-ical presentation of a suspected liverabscess includes pain, nausea, vomit-ing, fever, and chills. In our patientcohort, one patient did present withthese symptoms and was found tohave developed a hepatic abscess. Thispatient had undergone a Whipple pro-cedure for pancreatic cancer.
As expected with any therapy, lab-oratory toxicities were documented af-ter treatment. Clinically relevant toxic-ities (ie, total bilirubin) occurred in9.8% of the cohort. Weighing the risk/benefit ratio of this therapy, these tox-icities were deemed clinically accept-able. For patients with HCC, anincrease in bilirubin level represents adevelopment in the natural history ofcirrhosis. The 6.8% of patients with
HCC who developed increased biliru-bin levels likely represent a combina-tion of disease progression, naturalcourse of cirrhosis, and treatment-re-lated toxicity. Similarly, patients withend-stage liver disease with metasta-ses often develop lower-extremityedema, inanition, and overall failureto thrive. Hyperbilirubinemia is acomponent of this process. In this co-hort, bilirubin toxicity occurred in13.1% of patients. To eliminate anybias in attribution of toxicity, neither acut-off time nor the presence of dis-ease progression were incorporated inreporting toxicities. Hence, all toxicityfindings are reported herein.
The present study has several im-portant limitations. First, there is noattribution of laboratory toxicity todisease progression. This is the mostconservative approach to toxicity anal-ysis, as some toxicities were likelycaused by treatment failure and pro-gression. Second, long-term outcomesafter the 300-day mean follow-up ofbiliary changes are lacking. Also, thereis an element of subjectivity to the ra-diologic interpretation of biliary find-ings. Finally, no control group exists.Hence, comparing the results versusthose of other therapies can only beaccomplished by cohort comparisonfrom the peer-reviewed literature.
Although 90Y radioembolizationtherapy for primary and secondaryliver tumors is safe, several importantbiliary findings are of note, most ofwhich are clinically inconsequential.We present 90Y therapy–associated bil-iary sequelae that have been previ-ously noted with other locoregionaltherapeutic modalities. Although thisstudy shows an acceptable rate of bil-iary sequelae, timely diagnosis andrecognition of these findings with cor-relation to liver function will permitoptimal interpretation and follow-upof patients undergoing this treatment.
References1. Georgiades CS, Ramsey DE, Solomon
S, Geschwind JF. New nonsurgicaltherapies in the treatment of hepatocel-lular carcinoma. Tech Vasc Interv Ra-diol 2001; 4:193–199.
2. Llovet JM, Real MI, Montana X, et al.Arterial embolisation or chemoembo-lisation versus symptomatic treatmentin patients with unresectable hepato-cellular carcinoma: a randomised con-trolled trial. Lancet 2002; 359:1734–
1739.
Atassi et al • 697Volume 19 Number 5
3. Salem R, Thurston KG. Radio-embolization with 90yttrium micro-spheres: a state-of-the-art brachytherapytreatment for primary and secondaryliver malignancies. Part 2: special topics.J Vasc Interv Radiol 2006; 17:1425–1439.
4. Goldberg SN, Grassi CJ, Cardella JF, etal. Image-guided tumor ablation:standardization of terminology and re-porting criteria. J Vasc Interv Radiol2005; 16:765–778.
5. TheraSphere Yttrium-90 microspherespackage insert, MDS Nordion, Kanata,Canada. 2004.
6. Campbell AM, Bailey IH, Burton MA.Analysis of the distribution of intra-arterial microspheres in human liverfollowing hepatic yttrium-90 micro-sphere therapy. Phys Med Biol 2000;45:1023–1033.
7. Salem R, Lewandowski RJ, Atassi B, etal. Treatment of unresectable hepato-cellular carcinoma with use of 90Y mi-crospheres (TheraSphere): safety, tu-mor response, and survival. J VascInterv Radiol 2005; 16:1627–1639.
8. Lewandowski RJ, Sato KT, Atassi B, etal. Radioembolization with (90)y mi-crospheres: angiographic and technicalconsiderations. Cardiovasc InterventRadiol 2007; 30:571–592.
9. National Cancer Institute. CommonToxicity Criteria for Adverse Eventsv3.0. Available at: http://ctep.cancer.gov/forms/CTCAEv3.pdf. AccessedDecember 2007.
10. Brown DB, Gould JE, Gervais DA, et al.Transcatheter therapy for hepatic ma-lignancy: standardization of terminol-ogy and reporting criteria. J Vasc In-terv Radiol 2007; 18:1469–1478.
11. Omary RA, Bettmann MA, Cardella JF,et al. Quality improvement guide-lines for the reporting and archiving ofinterventional radiology procedures. JVasc Interv Radiol 2003; 14(suppl):S293–S295.
12. Yip D, Allen R, Ashton C, Jain S.Radiation-induced ulceration of thestomach secondary to hepatic emboli-zation with radioactive yttrium micro-spheres in the treatment of metastaticcolon cancer. J Gastroenterol Hepatol2004; 19:347–349.
13. Steel J, Baum A, Carr B. Quality oflife in patients diagnosed with primaryhepatocellular carcinoma: hepatic arte-rial infusion of cisplatin versus 90-yt-trium microspheres (Therasphere).Psychooncology 2004; 13:73–79.
14. Cherqui D, Palazzo L, Piedbois P, et al.Common bile duct stricture as a latecomplication of upper abdominal ra-diotherapy. J Hepatol 1994; 20:693–697.
15. Nakakubo Y, Kondo S, Katoh H,Shimizu M. Biliary stricture as a pos-
sible late complication of radiationtherapy. Hepatogastroenterology 2000;47:1531–1532.
16. Beltran MM, Marugan RB, Oton E,Blesa C, Nuno J. Accuracy of mag-netic resonance cholangiography in theevaluation of late biliary complicationsafter orthotopic liver transplantation.Transplant Proc 2005; 37:3924–3925.
17. Ercolani G, Grazi GL, Ravaioli M, et al.The role of liver resections for noncolo-rectal, nonneuroendocrine metastases:experience with 142 observed cases.Ann Surg Oncol 2005; 12:459–466.
18. Touzios JG, Kiely JM, Pitt SC, et al.Neuroendocrine hepatic metastases:does aggressive management improvesurvival? Ann Surg 2005; 241:776–783.
19. Sakamoto I, Iwanaga S, Nagaoki K, etal. Intrahepatic biloma formation(bile duct necrosis) after transcatheterarterial chemoembolization. AJR Am JRoentgenol 2003; 181:79–87.
20. Kim HK, Chung YH, Song BC, et al.Ischemic bile duct injury as a seriouscomplication after transarterial chemo-embolization in patients with hepato-cellular carcinoma. J Clin Gastroenterol2001; 32:423–427.
21. Xia J, Ren Z, Ye S, et al. Study of severeand rare complications of transarterialchemoembolization (TACE) for livercancer. Eur J Radiol 2006; 59:407–412.
22. Giorgio A, Tarantino L, de Stefano G,et al. Percutaneous sonographicallyguided saline-enhanced radiofre-quency ablation of hepatocellular car-cinoma. AJR Am J Roentgenol 2003;181:479–484.
23. Wood TF, Rose DM, Chung M, AllegraDP, Foshag LJ, Bilchik AJ. Radio-frequency ablation of 231 unresectablehepatic tumors: indications, limitations,and complications. Ann Surg Oncol2000; 7:593–600.
24. Akahane M, Koga H, Kato N, et al.Complications of percutaneous radio-frequency ablation for hepato-cellularcarcinoma: imaging spectrum andmanagement. Radiographics 2005; 25(suppl 1):S57–S68.
25. Kemeny NE, Niedzwiecki D, HollisDR, et al. Hepatic arterial infusionversus systemic therapy for hepaticmetastases from colorectal cancer: arandomized trial of efficacy, quality oflife, and molecular markers (CALGB9481). J Clin Oncol 2006; 24:1395–1403.
26. Alazmi WM, McHenry L, Watkins JL,et al. Chemotherapy-induced scleros-ing cholangitis: long-term response toendoscopic therapy. J Clin Gastroen-terol 2006; 40:353–357.
27. Shea WJ, Jr., Demas BE, Goldberg HI,Hohn DC, Ferrell LD, Kerlan RK.Sclerosing cholangitis associated withhepatic arterial FUDR chemotherapy:radiographic-histologic correlation. AJR
Am J Roentgenol 1986; 146:717–721.28. Kemeny N, Daly J, Reichman B, GellerN, Botet J, Oderman P. Intrahepaticor systemic infusion of fluorodeoxyuri-dine in patients with liver metastasesfrom colorectal carcinoma: a random-ized trial. Ann Intern Med 1987; 107:459–465.
29. Minagawa M, Makuuchi M, Torzilli G,et al. Extension of the frontiers of sur-gical indications in the treatment ofliver metastases from colorectal cancer:long-term results. Ann Surg 2000; 231:487–499.
30. Kuroda C, Iwasaki M, Tanaka T, et al.Gallbladder infarction following he-patic transcatheter arterial emboliza-tion: angiographic study. Radiology1983; 149:85–89.
31. Murthy R, Nunez R, Szklaruk J, et al.Yttrium-90 microsphere therapy forhepatic malignancy: devices, indica-tions, technical considerations, and po-tential complications. Radiographics2005; 25(suppl 1):S41–S55.
32. Demachi H, Matsui O, Kawamori Y,Ueda K, Takashima T. The protectiveeffect of portoarterial shunts after ex-perimental hepatic artery embolizationin rats with liver cirrhosis. CardiovascIntervent Radiol 1995; 18:97–101.
33. Kamel IR, Bluemke DA, Ramsey D, etal. Role of diffusion-weighted imag-ing in estimating tumor necrosis afterchemoembolization of hepatocellularcarcinoma. AJR Am J Roentgenol 2003;181:708–710.
34. Capps GW, Fulcher AS, Szucs RA,Turner MA. Imaging features of radi-ation-induced changes in the abdomen.Radiographics 1997; 17:1455–1473.
35. Winick AB, Waybill PN, Venbrux AC.Complications of percutaneous tran-shepatic biliary interventions. TechVasc Interv Radiol 2001; 4:200–206.
36. Dondelinger RF, Kurdziel JC, Gathy C.Percutaneous treatment of pyogenicliver abscess: a critical analysis of re-sults. Cardiovasc Intervent Radiol1990; 13:174–182.
37. Nakanuma Y, Hoso M, Sanzen T, SasakiM. Microstructure and development ofthe normal and pathologic biliary tract inhumans, including blood supply. Mi-crosc Res Tech 1997; 38:552–570.
38. Kim W, Clark TW, Baum RA, SoulenMC. Risk factors for liver abscess for-mation after hepatic chemoembolization.J Vasc Interv Radiol 2001; 12:965–968.
39. Lewandowski R, Salem R. Incidenceof radiation cholecystitis in patients re-ceiving Y-90 treatment for unresectableliver malignancies. J Vasc Interv Radiol2004; 15:S162.
40. Xu Z, Wang L, Zhang N, Ling X, HouC, Zhou X. Chemical ablation of thegallbladder: clinical application andlong-term observations. Surg Endosc
2005; 19:693–696.




























