Embed Size (px)
Citation preview

DOI 101212WNL593327200259327-334 Neurology
Douglas J LanskaAnthrax meningoencephalitis
This information is current as of August 13 2002
httpwwwneurologyorgcontent593327fullhtmlthe World Wide Web at
The online version of this article along with updated information and services is located on
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
CME Anthrax meningoencephalitisDouglas J Lanska MD MS MSPH
AbstractmdashObjective To review reported cases of anthrax meningoencephalitis and describe the clinical findings diagnos-tic test results treatment and outcome over the past 50 years Methods Retrospective review of English language articlespublished since Haightrsquos (1952) review Results Thirty-four core articles were identified describing 70 patients withcutaneous (29) gastrointestinal (17) inhalational (39) and unknown (16) sources of infection Clinical signs onpresentation included fever malaise meningeal signs hyperreflexia and delirium stupor or coma CSF analyses demon-strated hemorrhagic meningitis with positive Gramrsquos stains and CSF cultures Many patients presented in extremisfollowing a prodromal period of 1 to 6 days and 75 died within 24 hours of presentation Despite aggressive treatment inmany cases only 6 (4 of 70) survived none of whom had pulmonary anthrax Surviving patients generally had acutaneous portal of entry were younger and had less severely abnormal initial CSF results than patients who died Mostof the survivors recovered fully Pathologic findings included hemorrhagic meningitis multifocal subarachnoid andintraparenchymal hemorrhages vasculitis and cerebral edema Conclusions Anthrax meningoencephalitis has a highcase-fatality rate even with aggressive antibiotic treatment and supportive therapy Hemorrhagic meningitis should raisesuspicion of anthrax infection particularly if gram-positive rods are demonstrated on Gramrsquos stain Anthrax meningoen-cephalitis can develop from any primary focus but survival appears to be most likely if meningoencephalitis develops fromcutaneous anthrax Treatment of surviving patients was generally begun before signs and symptoms of meningoencepha-litis were present
NEUROLOGY 200259327ndash334
In 1952 Haight reviewed the world literature onanthrax meningoencephalitis and added two cases ofhis own1 Several excellent recent reviews on clinicalaspects of human anthrax infection have beenpublished2-6 The purpose of this report is to reviewreported cases of anthrax meningoencephalitis sinceHaightrsquos report to describe the clinical findings di-agnostic test results treatment and outcome overthe past 50 years and to compare these results withthose in Haightrsquos report
Methods English language articles on anthrax menin-goencephalitis published since Haightrsquos (1952) review1
were identified by searching the Entrez-PubMed electronicdatabase for articles published between January 1966 andJanuary 2002 and by hand search of bibliographies ofretrieved articles previous reviews monographs and text-books Reports were selected if they provided patient-specific clinical information with confirmation ofmeningoencephalitis and either microbiological or patho-logic confirmation of anthrax infection In outbreaks with asingle-source exposure (eg ingestion of contaminatedmeat) a case was considered confirmed if the clinical datasupported anthrax infection and at least one of the affected
individuals had microbiological or pathologic confirmationData were abstracted using a standardized instrument
The core articles in this series do not include reports7-10
without case-specific clinical information (17 cases) a re-port11 without microbiological or pathologic confirmation(one case) a case12 without lumbar puncture postmortemor other confirmation of leptomeningitis (one case) laterreports of a case713 that had been reported earlier1415 andcited by Haight1 (one case) and reports16-26 written in lan-guages other than English (ie French German Hungar-ian Romanian Spanish Russian [eight additional cases])Haight1 omitted from his tallies the two new cases that hereported and a separate case with survival reported in194827 for purposes of comparison with later cases re-viewed here these three cases were added to Haightrsquos se-ries of 70 cases
Statistical comparisons of count data between Haightrsquosseries and the present one were made using 2 or Fisherrsquosexact test (two-tailed) The nonparametric MannndashWhitneyU test was used for comparison of age and CSF resultsbetween patients who survived and those who died Mi-crosoft Excel 2000 V90 for Windows spreadsheet programwas used for data management and descriptive statisticsSPSS (Chicago IL) PC V50 was used for analyticstatistics
Results Seventy cases were identified from 34 re-ports1228-59 these reports form the core of this review Anumber of cases or outbreaks were described in multiple
Additional material related to this article can be found on the NeurologyWeb site Go to wwwneurologyorg and scroll down the Table of Con-tents for the August 13 issue to find the title link for this article
See also page 300
From the Veterans Affairs Medical Center Great Lakes VA Healthcare System Tomah and Department of Neurology University of Wisconsin MadisonReceived February 18 2002 Accepted in final form June 3 2002Address correspondence and reprint requests to Dr Douglas J Lanska Chief of Staff VA Medical Center 500 E Veterans Street Tomah WI 54660 e-mailDouglasLanskamedvagov
Copyright copy 2002 by AAN Enterprises Inc 327
reports sometimes by several different authors An out-break of inhalational and cutaneous anthrax at a textilemill in Manchester New Hampshire in 1957 was describedin several reports by different authors29306061 A clinicalreview in 198032 included seven case reports of inhala-tional anthrax and all three of the cases with anthraxmeningoencephalitis had been previously reported313440 Anumber of reports in the American4462-64 and Russian24-26
medical literature have described aspects of the anthraxoutbreak that resulted from accidental release of anthraxspores in April 1979 from a military bioweapons factory(Military Compound 19) in Sverdlovsk in the former SovietUnion (now Ekaterinburg Russia) This outbreak resultedin at least 66 human deaths (among the 77 patients iden-tified) in a narrow zone up to 4 kilometers downwind fromthe facility as well as outbreaks of anthrax in livestock upto 50 kilometers downwind62 Other reports and subse-quent analyses indicate that the numbers of cases anddeaths may have been significantly higher665 Forty-two ofthese cases were autopsied and 21 of the autopsied caseshad anthrax meningoencephalitis44 In 1992 Russian Pres-ident Boris Yeltsin confirmed that this outbreak was aresult of ldquomilitary developmentsrdquo62 and subsequent clini-cal and epidemiologic studies documented inhalational an-thrax from a mixture of different Bacillus anthracisstrains as the cause4462-64 Only one case of anthrax menin-goencephalitis59 has been identified among the 11 cases ofinhalational anthrax in the September 2001 bioterroristanthrax outbreak in the United States
Of the 70 cases in this series 54 (77) were malegiving a malefemale ratio of approximately 31 which wasthe ratio reported by Haight1 The age of cases ranged from2 to 72 years (median 41) similar to the range of newbornto 71 years reported by Haight1 A probable source of expo-sure was reported in 49 cases (70) of which 22 (31)were exposed to weaponized anthrax spores as a resultof the Sverdlovsk Russia bioweapons release in 1979 (21cases)44 or the US outbreak of bioterrorism anthrax in2001 (1 case)59 13 (19) had direct exposure to livestock(usually occupational)12363941434546495056 10 (14) ingestedcontaminated meat51-5358 and four (6) had exposure tolivestock products (2 wool mill workers 1 boy who skinneda goat and 1 butcher)12293037 Additional possible sourcesof anthrax exposure included ritual head shaving48 andinsect bite45 previous studies have suggested that shaving(with either contaminated animal hair brushes or instru-ments)66 and blood-feeding insects67 can be sources of an-thrax transmission A recent experimental study hasestablished that blood-feeding insects can in fact transmitanthrax68
Portal of entry Meningoencephalitis may develop withany type of anthrax including cutaneous18123335-373942
4548525456-58 gastrointestinal2851-535558 and inhalational29-32
34404459 but in some cases the portal of entry was not iden-tified (table 1)135383943465069 Excluding the single case of inutero anthrax in Haightrsquos series1 the distribution of portalof entry in the present series differed from that reported byHaight (p 002) with a higher proportion of gastrointes-tinal and inhalational cases and a lower proportion of cu-taneous cases in the present series (see table 1)
Clinical features Anthrax meningoencephalitis pre-sents with fever headache nausea vomiting and alteredmentation (ie confusion or agitation) in association with
symptoms related to the source of infection (eg cutane-ous gastrointestinal or inhalational) Clinical signs in-clude fever (383 degC to 41 degC) malaise meningeal signs(ie nuchal rigidity Kernig and Brudzinski signs) hyper-reflexia (often with unilateral or bilateral Babinski signs)and confusion delirium stupor or coma (table 2) Otherless frequent findings include papilledema cranial neurop-athies focal or generalized seizures myoclonus fascicula-
Table 1 Primary focus of anthrax in reported cases ofanthrax meningoencephalitis
Primary focusHaight 1952
(n 73)Lanska 2002
(n 70)Total
(n 143)
Cutaneous 39 (53) 20 (29) 59 (41)
Gastrointestinal 7 (10) 12 (17)dagger 19 (13)Dagger
Inhalational 17 (23) 27 (39) 44 (31)
Maternal sepsis 1 (1) 0 (0) 1 (1)
None identified 9 (12) 11 (16) 20 (14)
Values are expressed as n ()
Includes one case mixed cutaneousdagger Includes four cases mixed cutaneousDagger Includes five cases mixed cutaneous
Table 2 Reported symptoms and signs during course ofanthrax meningoencephalitis
Symptom or sign Value
Stupor or coma 38 (78)
Fever 35 (71)
Skin lesions 24 (49)
Headache 22 (45)
Nauseavomiting 21 (43)
Seizures 20 (41)
Nuchal rigidity 18 (37)
Focal neurologic deficit 15 (31)
Confusion or agitation 13 (27)
Cranial neuropathies 13 (27)
Kernig or Brudzinski sign 11 (22)
Lateralizing long-tract signs 11 (22)
Malaise 7 (14)
Hyperreflexia 7 (14)
Respiratory symptoms 6 (12)
Decerebrate rigidity 4 (8)
Diaphoresis 3 (6)
Papilledema 3 (6)
Dizziness 2 (4)
Values are expressed as n ()
Because of variable and incomplete reporting of clinical fea-tures at onset presentation and over the course of the illnessthe frequencies may be underestimates of the frequency withwhich these symptoms and signs occurred in these patientsThese results are based on 49 cases and exclude the autopsycases from the Sverdlovsk Russia bioweapons anthrax out-break from 1979
328 NEUROLOGY 59 August (1 of 2) 2002
tions generalized rigidity lateralizing long-tract signsand decerebrate posturing
CSF Results of analyses of CSF were reported insome detail for 43 patients (table 3) eight of whom hadserial lumbar punctures113143335364048 with up to six lum-bar punctures in a single patient1314 Serial lumbar punc-tures were performed to monitor response to therapy andin some cases to administer intrathecal penicillin113142733
In some cases initial suspicion of anthrax meningoenceph-alitis was the result of CSF abnormalities In the indexcase in the 2001 US bioterrorist outbreak a diagnosis ofanthrax was considered on the basis of CSF Gramrsquos stainand ultimately confirmed by CSF culture59
CSF studies typically showed findings of hemorrhagicmeningitis (see table 3) CSF in anthrax meningoencepha-litis may appear cloudy with yellowish or pinkish colora-tion or may be grossly bloody evolution across thisspectrum has been reported in serial lumbar punctures inan individual patient1 The supernatant was frequentlyxanthochromic Opening pressure was frequently elevatedwith a range of 130 to 700 mm H2O45 Hypoglycorrhachiawas common with CSF glucose in the range of 20 to 40
mgdL but occasionally less than 20 mgdL CSF proteinconcentration was generally elevated with a range of 10 to2800 mgdL CSF was frequently hemorrhagic but early inthe illness there may be no red blood cells13273545 Therewas generally a CSF pleocytosis with from 0 to 10000white cellsmm3 with a predominance of polymorphonu-clear leukocytes There were many large gram-positiverods on Gramrsquos stain either singly or in short or longchains CSF cultures from the initial lumbar puncturewere always positive when tested although some caseswere confirmed instead by culture of swabs or fluid fromskin lesions other body fluids or postmortem tissuesamples28-3032344445 CSF may be sterile after several daysof antibiotics136 Serial lumbar punctures may documentan evolution from cloudy to grossly bloody CSF with in-creasing protein concentration increasing numbers of redcells and polymorphonuclear leukocytes and increasingpredominance of polymorphonuclear leukocytes11314 Simi-lar collective findings were reported in a recent series of 12cases that did not provide case-specific results9
Other diagnostic studies Patients with anthrax me-ningoencephalitis generally have elevated white blood cell
Table 3 CSF analyses in anthrax meningoencephalitis
Variablevalue n () Variablevalue n ()
Appearance White cells per mm3
Cloudy 15 (35) 100 4 (9)
Bloody 12 (28) 100ndash999 3 (7)
Mixed 6 (14) 1000ndash9999 15 (35)
Clear 3 (7) 10000 3 (7)
Unknown 7 (16) Unknown 18 (42)
Glucose mddL Neutrophils
20 3 (7) 50 0 (0)
20ndash40 13 (30) 50ndash79 3 (7)
40 13 (30) 80 10 (23)
Unknown 14 (33) Unknown 30 (70)
Protein mgdL Gram-stain positive
45 2 (5) Yes 33 (77)
46ndash199 4 (9) No 3 (7)
200ndash999 18 (42) Unknown 7 (16)
1000 8 (19) CSF culture positive
Unknown 11 (26) Yes 35 (81)
Red cells per mm3 No 0 (0)
100 4 (9) Unknown 8 (19)
100ndash999 5 (12)
1000ndash9999 5 (12)
10000 2 (5)
Bloody count not reported 12 (28)
Unknown 15 (35)
These results are from the initial spinal taps for 43 cases with reported CSF results Haight1 did not summarize CSF results for hisseries although he reported fairly detailed results from serial lumbar punctures in the two cases he reported For the purpose of sum-marizing CSF results in anthrax meningitis Haightrsquos two cases from 19521 and two cases with survival from the late 1940s131427 wereincluded For CSF glucose two patients with normal values were coded as 40 mgdL and one patient with a low CSFblood ratio ofglucose concentration (017) was coded as 20ndash40 mgdL Three patients had negative CSF Gram stains and CSF cultures were notdone diagnostic confirmation in these cases was based on antemortem or postmortem cultures of other tissues histology or in onecase immunohistochemistry Because of rounding percentages for each variable may not sum to 100
August (1 of 2) 2002 NEUROLOGY 59 329
counts with a left shift The range of white cell counts inthe current series was from 5400 to 27700 somewhatlower than the range of 10000 to 80000 reported byHaight1 Blood cultures were positive in 71 (ie 1521) ofcases for whom these were reported nearly identical to thevalue of 70 reported by Haight1 Chest x-rays were oftenabnormal in patients with inhalational anthrax32344059
and occasionally in patients with gastrointestinal51 or cuta-neous disease3554 Chest x-ray findings included pleuraleffusion3234405159 hilar adenopathy3240 widened mediasti-num59 infiltrates35 and soft tissue edema54
EEG results have rarely been reported even thoughseizures are fairly common In part this reflects the mori-bund state of most of these patients In one patient withreported myoclonus and fasciculations EEG showed disor-ganized low-amplitude slow waves (1 to 7 Hz)39
CT or MRI of the head in patients with anthrax menin-goencephalitis may demonstrate focal intracerebral hemor-rhage subarachnoid hemorrhage intraventricularhemorrhage diffuse cerebral edema and prominent lepto-meningeal enhancement5458 Parenchymal cerebral en-hancement has not been reported58 but its absence maysimply reflect the paucity of neuroimaging studies in thesepatients Abnormalities may progress rapidly on serialbrain imaging studies54
Differential diagnosis Hemorrhagic meningitis shouldraise suspicion of anthrax infection36 particularly if gram-positive rods are demonstrated on Gramrsquos stain Listeriamonocytogenes the only common gram-positive rod caus-ing meningitis does not produce a hemorrhagic meningitisand is rarely seen on Gramrsquos stain Based on initial clinicaldiagnoses in reported cases the differential diagnosis ofanthrax meningoencephalitis may include subarachnoidand intracerebral hemorrhage ischemic stroke nonan-thrax bacterial meningoencephalitis herpes simplex virusencephalitis and other viral encephalitides eclampsia andcerebral malaria
Treatment Antianthrax treatment was reported in 39patients1228-3840424345-5255-59 Of these 19 (49) receivedpenicillin only28-32353842454849525658 (administered parenter-ally in all but one case)2930 19 (49) received penicillin (orin one case ampicillin)55 in combination with other antibi-otic therapy12293032-343637404345-475051555759 and one (3) re-ceived antianthrax serum only33 Antibiotics used inconjunction with penicillin therapy included chloramphen-icol (11 cases)33364345-475057 streptomycin (7 cas-es)1229303233374051 sulfonamides (4 cases)122930364557
cefotaxime (2 cases)5559 tetracyclines (1 case)33 vancomy-cin (1 case)59 and antianthrax serum (1 case)33 Corticoste-roids were administered in conjunction with antibiotics inten cases (26)3336424345485257 In the Sverdlovsk inhala-tional anthrax outbreak in 1979 hospitalized patientswere treated variously with penicillin cephalosporinchloramphenicol antianthrax globulin and corticoste-roids62 but case-specific treatments and outcomes were notreported in the English language literature either in gen-eral or for the 21 patients autopsied after dying with an-thrax meningoencephalitis446263
Prognosis Septicemia toxic shock and death rapidlyfollow development of anthrax meningoencephalitis inmost cases Many patients presented in extremis followinga prodromal period of 1 to 6 days and 75 died within 24hours of presentation (ie 4155 of cases for whom such
information was available)28-3538394144-4749-5269 Four pa-tients (6) in the present series survived36374851 comparedwith three (4) in the previous world literature a differ-ence that was not significant (p 071) (table 4) Exclud-ing the 21 cases of inhalational anthrax from theSverdlovsk autopsy series44 estimated survival in the cur-rent series is four of 49 (8) and in all reported cases todate is seven of 122 (6) the difference in survival be-tween this restricted group of deceased patients and thesurviving patients was also not significant (p 044) Re-ported additional cases of survival had no clinical informa-tion (two cases)7 or were not established microbiologicallyor pathologically as cases of anthrax (one case)11 An addi-tional recent series of 12 cases with no survivals did notreport case-specific information9
Survival appears to be most likely if meningoencephali-tis develops as part of the course of cutaneous an-thrax363748 but a single case with survival has beenreported with gastrointestinal anthrax51 In the currentseries 15 of cutaneous cases survived compared with 8among gastrointestinal cases none among inhalationalcases and none among unknown or unspecified cases (seetable 3) The difference in survival of the cutaneous casesin the current series (15) and Haightrsquos series (5) wasnot significant (p 032) To date in the world literaturethere are no reported cases of survival following anthraxmeningoencephalitis associated with inhalational anthrax
The seven surviving patients reported to date are sum-marized in table 513-15273637485170 Surviving patients wereyounger as a group than those in the present series whodied (median age of surviving cases 24 years n7 me-dian age of cases who died 45 years n 66 p 004) Ifthe comparison is restricted to cases in the current seriesonly the difference in age is greater (median age of surviv-ing cases 1025 years n 4 p 0003) In generalinitial CSF results from the surviving patients were eithernormal or were less severely abnormal compared to de-ceased patients However because of the small samplesizes for different CSF studies in the survival group noneof the individual contrasts was significant (glucose p 041 protein p 012 red cells p 024 white cellsp 008)
Many reports and reviews failed to identify all of thepreviously reported cases with survival or misreported as-pects of the cases they did review resulting in incorrectconclusions about the agents that are potentially effective
Table 4 Survival with anthrax meningoencephalitis inreported cases
Primary focus Haight 1952 Lanska 2002 Total
Cutaneous 239 (5) 320 (15) 559 (8)
Gastrointestinal 07 (0) 112 (8) 119 (5)
Inhalational 017 (0) 027 (0) 044 (0)
Maternal sepsis 01 (0) 01 (0)
None identified 19 (11) 011 (0) 120 (5)
Total 373 (4) 470 (6) 7143 (5)
Values are expressed as n ()
Excluding the 21 inhalational cases from the Sverdlovsk autopsyseries estimated survival in the current series is 449 (8) andin reported cases to date is 7122 (6)
330 NEUROLOGY 59 August (1 of 2) 2002
treatments The treatments administered to surviving pa-tients were in fact similar to those chosen in the entiregroup of patients in the current series All of the patientsreceived penicillin except the first case (Patient 1) whoreportedly received no treatment (Bernd Remler MD per-sonal communication February 2002)70 Only two of thepatients received corticosteroids in addition to antibiotics(Patients 4 and 6)3648 The only case with gastrointestinalanthrax (Patient 7) received the same treatment as hissister (aged 2 years) who died51 Treatment of survivingpatients was generally begun before the disease was clini-cally advanced Three of the patients who survived (Pa-tients 2 through 4) were receiving treatment for cutaneousanthrax (that included penicillin) before development ofsymptoms of meningoencephalitis13-152736 There is limitedinformation on long-term outcomes among the survivorsbut most were reported to have fully recovered13-1527363751
although two patients had residual focal weakness4870
Autopsy findings Autopsies were obtained in 40 of the66 deceased patients (61)28-32343538-4043-454755-5759 Thissummary is restricted to pathologic findings in the centralnervous system Gross findings typically included cloudyand congested leptomeninges with occasional obvious pu-rulent exudate13034354447 and with variable degrees of sub-arachnoid hemorrhage128293135394044455557 In many casessubarachnoid hemorrhage was the dominant gross patho-logic feature1282931353940444555 The vascular congestionand extensive subarachnoid hemorrhage of the leptome-ninges gave a dark red appearance on gross examination ofthe brain a finding sometimes referred to as a ldquocardinalrsquoscaprdquo2 Other common findings included intraventricularhemorrhage2939 intracerebral hematoma13956 multifocalsmall intraparenchymal cortical hemorrhages394047 or nu-merous petechial hemorrhages in cerebral parenchyma2864
zones of infarction in arterial venous or watershed distri-butions3964 and cerebral edema35454757 with tonsillar35 oruncal herniation47
Microscopic findings included hemorrhagic leptomen-ingitis2930343538-404447555764 and associated necrotizing vas-
culitis164 multifocal subarachnoid128-313538-404445555764 andintracerebral hemorrhage128-3038394756 multifocal cerebralinfarction3964 and leptomeningeal and cerebral ede-ma35394445475764 The hemorrhagic leptomeningitis was as-sociated with polymorphonuclear leukocytic inflammatoryexudates3538444755-5764 severe congestion of meningealblood vessels3538404756 hemorrhagic infiltration3544455664 orfrank subarachnoid hemorrhage128-313538-404445555764 aggre-gations of neutrophils and mononuclear phagocytes in andaround meningeal vessels3538404764 and tracking of bloodand inflammatory infiltrates along the VirchowndashRobin(perivascular) spaces into the parenchyma47 The superfi-cial cerebral cortex showed diffuse perineuronal andperivascular infiltration by neutrophils353947 severe vascu-lar congestion3540 necrosis of blood vessel walls3539475664
recent thromboses353964 zones of ischemia3964 areas ofhemorrhage47 and edema35394445475764 Numerous largegram-positive rods in short chains were present in theleptomeninges and the subarachnoid and VirchowndashRobinspaces29-31344756 within and around meningeal and superfi-cial cortical vessels and vessels in regions of hemor-rhage313235394064 and within hemorrhagic lesions313247
Discussion Meningoencephalitis develops in atmost 5 of cases of cutaneous anthrax1428 howevermost cases of anthrax meningoencephalitis to datehave developed from cutaneous anthrax because thevast majority of naturally acquired cases of anthraxare cutaneous28 Meningoencephalitis may occur inup to half of the cases in industrial or bioweaponsoutbreaks of inhalational anthrax829303244 howeverin the recent bioterrorist outbreak of anthrax in theUnited States only the index case had meningitisamong the 11 cases of confirmed or suspected inhala-tional anthrax identified5971-73 The relatively low fre-quency of meningitis among anthrax cases in the USbioterrorism outbreak may be misleading though aslumbar punctures were done in few cases and the
Table 5 Patients with anthrax meningoencephalitis who survived
Variable
Patient no
1 2 3 4 5 6 7
Reference no 70 14 27 36 37 48 51
Year 1916 1947 1948 1972 1973 1989 1993
Age y 24 57 51 85 12 25 6
Sex F M M F M M M
Clinical type Unknown Cutaneous Cutaneous Cutaneous Cutaneous Cutaneous Gastrointestinal
Treatment None
Antianthrax serum X
Penicillin X X X X X X
Chloramphenicol I
Streptomycin X X
Sulfonamide X I
Corticosteroid X X
Residual L hemiparesis None None None None RUE weakness None
X main therapy I initial therapy only RUE right upper extremity
August (1 of 2) 2002 NEUROLOGY 59 331
brain was not examined in some autopsies Based onprevious experience44 the potential exists for largenumbers of cases of anthrax meningoencephalitiswith further bioterrorist outbreaks or bioweaponsdispersals Meningoencephalitis may also occur withgastrointestinal anthrax or without a clinically ap-parent primary focus
Current guidelines from the Centers for DiseaseControl indicate that ciprofloxacin or doxycyclineshould be included as essential components of initialtherapy for anthrax infections of any portal of en-try7274 It is important to treat anthrax meningoen-cephalitis with a polydrug antibiotic regimen usingantimicrobial agents that have good CSF penetrationin meningitis and that provide good antibacterialcoverage for B anthracis All six patients who sur-vived after antibiotic treatment for anthrax menin-goencephalitis were treated with penicillinHowever because of the presence of constitutive orinducible beta-lactamases in B anthracis isolatesfrom the recent US bioterrorist outbreak and expec-tations that beta-lactamase activity may be likelywith bioengineered bioweapons agents ampicillin orpenicillin G alone are not recommended for initialtherapy for anthrax meningoencephalitis prior to an-tibiotic sensitivity results from culture7274 Rifampinplus vancomycin would be a reasonable choice foraddition to ciprofloxacin or doxycycline in the initialtreatment of anthrax meningoencephalitis Some in-fectious disease authorities recommend ciprofloxacinin preference to doxycycline plus augmentation withchloramphenicol rifampin or penicillin for estab-lished or suspected anthrax meningoencephalitis6
Aztreonam trimethoprim-sulfamethoxazole orthird-generation cephalosporins should not be usedbecause of natural resistance of B anthracis strainsto these antibiotics
Bacterial toxins have long been felt to play a ma-jor role in anthrax meningoencephalitis becausemany effects of B anthracis cannot be attributed tomicroscopically evident tissue changes1075 Virulenceof B anthracis requires an antiphagocytic capsuleand two exotoxins The two toxins are binary pro-teins composed of a binding protein and an enzymat-ically active protein2476 Among other actions thesetoxins collectively produce local edema impair neu-trophil function depress cerebral cortical electricalactivity depress central respiratory center activitycause bleeding and destruction of the brain and vitalorgans in the chest and induce cardiovascular col-lapse and shock244476-79
Although antitoxin was used early in the 20thcentury to treat anthrax alone or in combinationwith penicillin13-15 it has not been available in recentdecades to US civilian populations Conceptually an-tianthrax serum may augment the effect of antibiot-ics by helping to neutralize the anthrax toxinswhich are not inactivated by antibiotics Howeverthere are no documented cases of successful treat-ment of anthrax meningitis with antianthrax serumalone Haight incorrectly stated that a case reported
by Czyhlarz in 191670 had been cured by treatmentwith antianthrax serum when in fact a full transla-tion indicates that the patient received no treatment(Bernd Remler MD personal communication Feb-ruary 2002 see supplementary document) this er-ror has been promulgated by numerous subsequentauthors and has been a source of incorrect conclu-sions regarding potentially effective therapy for an-thrax meningoencephalitis in recent reviewsCzyhlarz70 also presented unpublished second-handinformation on another patient who purportedly re-covered from anthrax meningoencephalitis withouttreatment In light of subsequent experience withthis disease it is hard to interpret or credit either ofthese reports Available experimental data80 do notindicate a significant treatment effect of antianthraxserum beyond that of penicillin Nevertheless anti-anthrax immune globulin derived from the blood ofsoldiers who have received the anthrax vaccine isbeing added to the US bioterrorism treatment stock-pile and is being considered as a potential experi-mental anthrax treatment in the event of furtherbioterrorism anthrax cases681
Corticosteroids have been recommended as an ad-junctive agent in the treatment of meningitis in chil-dren82 Use of corticosteroids in adults withmeningitis is controversial but steroids have beenrecommended for consideration as adjunctive agentswithout any age restriction in anthrax meningitis72
If corticosteroids are used in conjunction with vanco-mycin therapy antibiotic dosing may need to bemodified because CSF vancomycin levels may be de-creased by corticosteroids contributing to treatmentfailure82-86
In addition to antibiotic management patientswith anthrax meningoencephalitis may require ag-gressive intensive care measures Seizures in-creased intracranial pressure subarachnoid andintracerebral hemorrhage electrolyte disturbanceshypotension shock and disseminated intravascularcoagulation may develop as complications of this in-fection Despite aggressive treatment the prognosisfor survival with anthrax meningoencephalitis isvery poor
AcknowledgmentThe author thanks Glen Salter MS of the Tomah VA MedicalCenter Library for assistance in locating references Pat Mennickeof the Tomah VA Medical Center for assistance with Excel spread-sheets Bernd Remler MD of the Medical College of WisconsinMilwaukee for translating the paper by Czyhlarz Larry DavisMD of the Albuquerque VA Medical Center for helpful correspon-dence regarding corticosteroids and vancomycin Jeffrey M JonesMD PhD of the William S Middleton VA Medical Center Madi-son for helpful discussions regarding antibiotic treatment of an-thrax meningoencephalitis and Mary Jo Lanska MD MS of theTomah VA Medical Center for helpful discussions and for criti-cally reviewing the manuscript
References1 Haight TH Anthrax meningitis review of literature and report
of two cases with autopsies Am J Med Sci 195222457ndash692 Dixon TC Meselson M Guillemin J Hanna PC Anthrax
N Engl J Med 1999341815ndash826
332 NEUROLOGY 59 August (1 of 2) 2002
3 Inglesby TV Henderson DA Bartlett JG et al Anthrax as abiological weapon medical and public health managementJAMA 19992811735ndash1745
4 Swartz MN Recognition and management of anthrax an up-date N Engl J Med 20013451621ndash1626
5 Jernigan JA Stephens DS Ashford DA et al Bioterrorism-related inhalational anthrax the first 10 cases reported in theUnited States Emerg Infect Dis 20017933ndash944
6 Inglesby TV OrsquoToole T Henderson DA et al Anthrax as abiological weapon 2002 updated recommendations for man-agement JAMA 20022872236ndash2252
7 Miller JK Human anthrax in New York State NY StateJ Med 1961612046ndash2053
8 Brachman PS Human anthrax in the United States Antimi-crob Agents Chemother 19655111ndash114
9 Kumar A Kanungo R Bhattacharya S Badrinath S DuttaTK Swaminathan RP Human anthrax in India urgent needfor effective prevention J Commun Dis 200032240ndash246
10 Dutz W Kohout E Anthrax Pathol Annu 197162009ndash224811 Trivedy JR Case of anthrax meningitis survival Cent Afr
J Med 19812716612 Roberts CJ Chambers PG An outbreak of anthrax in the
Mondoro Tribal Trust lands Cent Afr J Med 19752173ndash7613 Kindler D Recovery from anthrax meningitis Ind Med Surg
195221487ndash48814 Shanahan RH Griffin JR Von Auersperg AP Anthrax men-
ingitis report of a case of internal anthrax with recoveryAm J Clin Pathol 194717719ndash722
15 Griffin JR Shanahan RH DeAngelis CE Treatment of cuta-neous anthrax with penicillin NY State J Med 1948481718ndash1721
16 Boudin G Lauras A Vaillant C Etat de mal eacutepileptiquereacuteveacutelateur drsquoune meacuteningite charbonneuse etude anatamo-clinique Bull Mem Soc Med Hop Paris 1964115183ndash187
17 Rapun Pac JL Ull Laita M Meningitis carbuncosa Arch Neu-robiol (Madr) 197235143ndash148
18 Baltiev A Besleaga E Cuciureanu G Obreja E Meningo-encefalita carbunoasa la un copil cu pustula cutanata necarac-teristica Rev Med Chir Soc Med Nat Iasi 197377885ndash888
19 Beer K Milzbrandmeningitis Path Microbiol 19733912ndash1320 Bach I Simon L Baacuten E Toacuteth L Kovaacutecs M Haemorrhagiaacutes
meningitises apoplexia anthrax sepsisben Orv Hetil 19781191797ndash1799
21 Marandian MH Kamali A Meacuteningite charbonneuse un casen apparence primitif Nouv Presse Med 1981101747ndash1748
22 Duumlrst UN Bartenstein J Buumlhlmann H Wuumlst J Spiegel MVAnthraxmeningitis Schweiz Med Wochenschr 19861161222ndash1228
23 Gonzalez A Rodriguez E Castillo M Ortega I Ramirez EFajardo J Lesioacuten necroacutetica en mentoacuten en paciente con siacuten-drome meniacutengeo Enferm Infecc Mircobiol Clin 199715163ndash164
24 Abramova AA Grinberg LM [Pathology of anthrax sepsisaccording to materials of the infectious outbreak in 1979 inSverdlovsk (macroscopic changes)] Arkh Patol 19935512ndash17
25 Abramova AA Grinberg LM [Pathology of anthrax sepsisaccording to materials of infectious outbreak in 1979 in Sverd-lovsk (microscopic changes)] Arkh Patol 19935518ndash23
26 Grinberg LM Abramova AA [Pathology of anthrax sepsisaccording to materials of the infectious outbreak in 1979 inSverdlovsk (various aspects of morpho- patho- and thanato-genesis] Arkh Patol 19935523ndash26
27 Weinstein L Oliver CS The treatment of human anthraxwith penicillin Am Pract 19482533ndash538
28 Raper AB Anthrax meningo-encephalitis East Afr Med J195330399-401
29 Albrink WS Brooks SM Biron RE Kopel M Human inhala-tional anthrax a report of three fatal cases Am J Pathol196036457ndash468
30 Plotkin SA Brachman PS Utell M Bumford FH AtchisonMM An epidemic of inhalation anthrax the first in the twen-tieth century I Clinical features Am J Med 196029992ndash1001
31 Brachman PS Pagano JS Albrink WS Two cases of fatalinhalation anthrax one associated with sarcoidosis N EnglJ Med 1961265203ndash208
32 Brachman PS Inhalation anthrax Ann NY Acad Sci 198035383ndash93
33 Vita A Secu A Cuciureanu G Leibovici M Bejanariu C CujuG Considerations on 3 cases of meningo-encephalitis due toanthrax bacilli Rom Med Rev 1961536ndash39
34 LaForce FM Bumford FH Freely JC Stokes SL Snow DBEpidemiologic study of a fatal case of inhalation anthrax ArchEnviron Health 196918798ndash805
35 Rangel RA Gonzaacutelez DA Bacillus anthracis meningitis Neu-rology 197525525ndash530
36 Tahernia AC Hashemi G Survival in anthrax meningitisPediatrics 197250329ndash333
37 Tengio FU Anthrax meningitis report of two cases East AfrMed J 197350337ndash339
38 Viratchai C Anthrax gastro-enteritis and meningitis J MedAssoc Thai 197457147ndash150
39 Pluot M Vital C Aubertin J Croix JC Pire JC Poisot DAnthrax meningitis report of two cases with autopsies ActaNeuropathol (Berl) 197636339ndash345
40 Suffin SC Carnes WH Kaufman AF Inhalation anthrax in ahome craftsman Hum Pathol 19789594ndash597
41 Al-Dulaimy SB Al-Allaf GA Anthrax meningitis Trans R SocTrop Med Hyg 197872315
42 Manios S Kavaliotis I Anthrax in children a long forgottenpotentially fatal condition Scand J Infect Dis 197911203ndash206
43 Koshi G Lalitha MK Daniel J Chacko A Pulimood BMAnthrax meningitis a rare clinical entity J Assoc PhysiciansIndia 19812959ndash62
44 Abramova FA Grinberg LM Tampolskaya OV Walker DHPathology of inhalational anthrax in 42 cases from the Sverd-lovsk outbreak of 1979 Proc Natl Acad Sci USA 1993902291ndash2294
45 Levy L Baker N Meyer MP Crosland P Hampton J Anthraxmeningitis in Zimbabwe Cent Afr J Med 198127101ndash104
46 Bhat P Pereira P Mohan N Primary anthrax meningitis acase report Neurol India 19833171ndash73
47 Chandramukhi A Shankar P Rao TV Sundararajan SSwamy HS Acute leptomeningitis due to Bacillus anthracis acase report Trop Geogr Med 19833579ndash82
48 Khanna N Gokul BN Ravikumar R et al Successfullytreated primary anthrax meningitis Indian J Pathol Micro-biol 198932315ndash317
49 Kanungo R Sujatha S Das AK Rao RS Anthrax meningitisa clinical enigma Indian J Med Microbiol 19906149ndash151
50 Bharathmoorthy Chakravarthy I Swaminathan RP et alHaemorrhagic meningitis due to Bacillus anthrax J AssocPhysicians India 199240134ndash135
51 Tabatabaie P Syadati A Bacillus anthracis as a cause ofbacterial meningitis Pediatr Infect Dis 1993121035ndash1037
52 George S Mathai D Balraj V Lalitha MK John TJ An out-break of anthrax meningoencephalitis Trans R Soc Trop MedHyg 199488206ndash207
53 Berthier M Fauchegravere J-L Perrin J Grignon B Oriot D Ful-minant meningitis due to Bacillus anthracis in 11-year-oldgirl during Ramadan Lancet 1996347828
54 Domiacutenguez E Bustos C Garcia M Recio S Anthrax meningo-encephalitis radiologic findings AJR Am J Roentgenol 1997169317
55 Kwong KL Que TL Wong SN So KT Fatal meningoenceph-alitis due to Bacillus anthracis J Paediatr Child Health 199733539ndash541
56 Garcia AG Jiminez RR Bacillus anthracis meningitis N EnglJ Med 1999341814
57 Ringertz SH Hoiby EA Jensenius M et al Injectional an-thrax in a heroin skin-popper Lancet 20003461574ndash1575
58 Kim HJ Jun WB Lee SH Rho MH CT and MR findings ofanthrax meningoencephalitis report of two cases and reviewof the literature AJNR Am J Neuroradiol 2001221303ndash1305
59 Bush LM Abrams BH Heall A Johnson CC Index case offatal inhalational anthrax due to bioterrorism in the UnitedStates N Engl J Med 20013451607ndash1610
60 Brachman PS Plotkin SA Bumford FH Atchison MM Anepidemic of inhalation anthrax the first in the twentieth cen-tury II Epidemiology Am J Hygiene 1960726ndash23
61 Belluck P Anthrax outbreak of rsquo57 felled a mill but yieldedanswers New York Times October 27 2001B8
62 Meselson M Guillemin J Hugh-Jones M et al The Sverd-lovsk anthrax outbreak of 1979 Science 19942661202ndash1208
August (1 of 2) 2002 NEUROLOGY 59 333
63 Jackson PJ Hugh-Jones ME Adair DM et al PCR analysis oftissue samples from the 1979 Sverdlovsk anthrax victims thepresence of multiple Bacillus anthracis strains in differentvictims Proc Natl Acad Sci USA 1998951224ndash1229
64 Grinberg LM Abramova FA Yampolskaya OV Walker DHSmith JH Quantitative pathology of inhalational anthrax IQuantitative microscopic findings Mod Pathol 200114482ndash495
65 Brookmeyer R Blades N Hugh-Jones M Henderson D Thestatistical analysis of truncated data application to the Sverd-lovsk anthrax outbreak Biostatistics 20012233ndash247
66 Knott FA A note on anthrax infection by shaving brushesLancet 19231227ndash228
67 Bradaric N Punda-Polic V Cutaneous anthrax due topenicillin-resistant Bacillus anthracis transmitted by an in-sect bite Lancet 1992340306ndash307
68 Turell MJ Knudson GB Mechanical transmission of Bacillusanthracis by stable flies (Stomoxys calcitrans) and mosquitoes(Aedes aegypti and Aedes taeniorhynchus) Infect Immun1987551859ndash1861
69 Drake DJ Meningitic anthrax Cent Afr J Med 19711797ndash9870 Czyhlarz EV Beitrag zur Lehre von der Milzbrandmeningitis
Wein Klin Wochenscr 191629768ndash76971 Centers for Disease Control Investigation of anthrax associ-
ated with intentional exposure and interim public healthguidelines October 2001 MMWR Morb Mortal Wkly Rep200150889ndash893
72 Centers for Disease Control Update investigation ofbioterrorism-related anthrax and interim guidelines for expo-sure management and antimicrobial therapy October 2001MMWR Morb Mortal Wkly Rep 200150909ndash919
73 Centers for Disease Control Investigation of bioterrorism-related anthrax and interim guidelines for clinical evaluationof persons with possible anthrax MMWR Morb Mortal WklyRep 200150941ndash948
74 Centers for Disease Control Updated recommendations forantimicrobial prophylaxis among asymptomatic pregnantwomen after exposure to Bacillus anthracis MMWR MorbMortal Wkly Rep 200150960
75 Bonventure PF Sueoka W True CW Klein F Lincoln RAttempts to implicate the central nervous system as a pri-
mary site of action for Bacillus anthracis lethal toxin FedProc 1967261549ndash1553
76 Friedlander AM Anthrax In Sidell FR Takafuji ET FranzDR eds Textbook of military medicine medical aspects ofchemical and biological warfare Washington DC Office ofthe Surgeon General 1997467ndash478
77 Vick JA Lincoln RE Klein F Mahlandt BG Walker JS FishDC Neurological and physiological responses of the primateto anthrax toxin J Infect Dis 196811885ndash96
78 Klein F Lincoln RE Dobbs JP Mahlandt BG Remmele NSWalker JS Neurological and physiological responses of theprimate to anthrax infection J Infect Dis 196811897ndash103
79 Remmele NS Klein F Vick JA Walker JS Mahlandt BGLincoln RE Anthrax toxin primary site of action J Infect Dis1968118104ndash113
80 Doganay M Hanagasi R Zora A [Evaluation of penicillinalone and penicillin combined with anti-anthrax serum in ex-perimental anthrax in mice] Mikrobiyol Bul 19851957ndash64
81 Associated Press Government may offer anthrax treatmentNew York Times January 7 2002
82 Davis LE Acute bacterial meningitis In Johnson RT GriffinJW eds Current therapy in neurologic disease 5th ed StLouis Mosby 1997120ndash127
83 Viladrich PF Gudiol F Lintildeares J et al Evaluation of vanco-mycin for therapy of adult pneumococcal meningitis Antimi-crob Agents Chemother 1991352467ndash2472
84 Pariacutes M Hickey SM Uscher MI Shelton S Olsen KD Mc-Cracken GH Jr Effect of dexamethasone on therapy of exper-imental penicillin- and cephalosporin-resistant pneumococcalmeningitis Antimicrob Agents Chemother 1994381320ndash1324
85 Cabellos C Martinez-Lacasa J Martos A et al Influence ofdexamethasone on efficacy of ceftriaxone and vancomycintherapy in experimental pneumococcal meningitis AntimicrobAgents Chemother 1995392158ndash2160
86 Ahmed A Jafri H Lutsar I et al Pharmacodynamics of van-comycin for the treatment of experimental penicillin- andcephalosporin-resistant pneumococcal meningitis AntimicrobAgents Chemother 199943876ndash881
334 NEUROLOGY 59 August (1 of 2) 2002
DOI 101212WNL593327200259327-334 Neurology
Douglas J LanskaAnthrax meningoencephalitis
This information is current as of August 13 2002
ServicesUpdated Information amp
httpwwwneurologyorgcontent593327fullhtmlincluding high resolution figures can be found at
Supplementary Material
htmlhttpwwwneurologyorgneurologysuppl20020716593327DC2
htmlhttpwwwneurologyorgneurologysuppl20020716593327DC1Supplementary material can be found at
References httpwwwneurologyorgcontent593327fullhtmlref-list-1
This article cites 73 articles 15 of which you can access for free at
Citations httpwwwneurologyorgcontent593327fullhtmlotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpwwwneurologyorgcgicollectionmeningitisMeningitis
httpwwwneurologyorgcgicollectionencephalitisEncephalitis
httpwwwneurologyorgcgicollectionbacterial_infectionsBacterial infections
httpwwwneurologyorgcgicollectionall_infectionsAll Infectionsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsin its entirety can be found online atInformation about reproducing this article in parts (figurestables) or
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

CME Anthrax meningoencephalitisDouglas J Lanska MD MS MSPH
AbstractmdashObjective To review reported cases of anthrax meningoencephalitis and describe the clinical findings diagnos-tic test results treatment and outcome over the past 50 years Methods Retrospective review of English language articlespublished since Haightrsquos (1952) review Results Thirty-four core articles were identified describing 70 patients withcutaneous (29) gastrointestinal (17) inhalational (39) and unknown (16) sources of infection Clinical signs onpresentation included fever malaise meningeal signs hyperreflexia and delirium stupor or coma CSF analyses demon-strated hemorrhagic meningitis with positive Gramrsquos stains and CSF cultures Many patients presented in extremisfollowing a prodromal period of 1 to 6 days and 75 died within 24 hours of presentation Despite aggressive treatment inmany cases only 6 (4 of 70) survived none of whom had pulmonary anthrax Surviving patients generally had acutaneous portal of entry were younger and had less severely abnormal initial CSF results than patients who died Mostof the survivors recovered fully Pathologic findings included hemorrhagic meningitis multifocal subarachnoid andintraparenchymal hemorrhages vasculitis and cerebral edema Conclusions Anthrax meningoencephalitis has a highcase-fatality rate even with aggressive antibiotic treatment and supportive therapy Hemorrhagic meningitis should raisesuspicion of anthrax infection particularly if gram-positive rods are demonstrated on Gramrsquos stain Anthrax meningoen-cephalitis can develop from any primary focus but survival appears to be most likely if meningoencephalitis develops fromcutaneous anthrax Treatment of surviving patients was generally begun before signs and symptoms of meningoencepha-litis were present
NEUROLOGY 200259327ndash334
In 1952 Haight reviewed the world literature onanthrax meningoencephalitis and added two cases ofhis own1 Several excellent recent reviews on clinicalaspects of human anthrax infection have beenpublished2-6 The purpose of this report is to reviewreported cases of anthrax meningoencephalitis sinceHaightrsquos report to describe the clinical findings di-agnostic test results treatment and outcome overthe past 50 years and to compare these results withthose in Haightrsquos report
Methods English language articles on anthrax menin-goencephalitis published since Haightrsquos (1952) review1
were identified by searching the Entrez-PubMed electronicdatabase for articles published between January 1966 andJanuary 2002 and by hand search of bibliographies ofretrieved articles previous reviews monographs and text-books Reports were selected if they provided patient-specific clinical information with confirmation ofmeningoencephalitis and either microbiological or patho-logic confirmation of anthrax infection In outbreaks with asingle-source exposure (eg ingestion of contaminatedmeat) a case was considered confirmed if the clinical datasupported anthrax infection and at least one of the affected
individuals had microbiological or pathologic confirmationData were abstracted using a standardized instrument
The core articles in this series do not include reports7-10
without case-specific clinical information (17 cases) a re-port11 without microbiological or pathologic confirmation(one case) a case12 without lumbar puncture postmortemor other confirmation of leptomeningitis (one case) laterreports of a case713 that had been reported earlier1415 andcited by Haight1 (one case) and reports16-26 written in lan-guages other than English (ie French German Hungar-ian Romanian Spanish Russian [eight additional cases])Haight1 omitted from his tallies the two new cases that hereported and a separate case with survival reported in194827 for purposes of comparison with later cases re-viewed here these three cases were added to Haightrsquos se-ries of 70 cases
Statistical comparisons of count data between Haightrsquosseries and the present one were made using 2 or Fisherrsquosexact test (two-tailed) The nonparametric MannndashWhitneyU test was used for comparison of age and CSF resultsbetween patients who survived and those who died Mi-crosoft Excel 2000 V90 for Windows spreadsheet programwas used for data management and descriptive statisticsSPSS (Chicago IL) PC V50 was used for analyticstatistics
Results Seventy cases were identified from 34 re-ports1228-59 these reports form the core of this review Anumber of cases or outbreaks were described in multiple
Additional material related to this article can be found on the NeurologyWeb site Go to wwwneurologyorg and scroll down the Table of Con-tents for the August 13 issue to find the title link for this article
See also page 300
From the Veterans Affairs Medical Center Great Lakes VA Healthcare System Tomah and Department of Neurology University of Wisconsin MadisonReceived February 18 2002 Accepted in final form June 3 2002Address correspondence and reprint requests to Dr Douglas J Lanska Chief of Staff VA Medical Center 500 E Veterans Street Tomah WI 54660 e-mailDouglasLanskamedvagov
Copyright copy 2002 by AAN Enterprises Inc 327
reports sometimes by several different authors An out-break of inhalational and cutaneous anthrax at a textilemill in Manchester New Hampshire in 1957 was describedin several reports by different authors29306061 A clinicalreview in 198032 included seven case reports of inhala-tional anthrax and all three of the cases with anthraxmeningoencephalitis had been previously reported313440 Anumber of reports in the American4462-64 and Russian24-26
medical literature have described aspects of the anthraxoutbreak that resulted from accidental release of anthraxspores in April 1979 from a military bioweapons factory(Military Compound 19) in Sverdlovsk in the former SovietUnion (now Ekaterinburg Russia) This outbreak resultedin at least 66 human deaths (among the 77 patients iden-tified) in a narrow zone up to 4 kilometers downwind fromthe facility as well as outbreaks of anthrax in livestock upto 50 kilometers downwind62 Other reports and subse-quent analyses indicate that the numbers of cases anddeaths may have been significantly higher665 Forty-two ofthese cases were autopsied and 21 of the autopsied caseshad anthrax meningoencephalitis44 In 1992 Russian Pres-ident Boris Yeltsin confirmed that this outbreak was aresult of ldquomilitary developmentsrdquo62 and subsequent clini-cal and epidemiologic studies documented inhalational an-thrax from a mixture of different Bacillus anthracisstrains as the cause4462-64 Only one case of anthrax menin-goencephalitis59 has been identified among the 11 cases ofinhalational anthrax in the September 2001 bioterroristanthrax outbreak in the United States
Of the 70 cases in this series 54 (77) were malegiving a malefemale ratio of approximately 31 which wasthe ratio reported by Haight1 The age of cases ranged from2 to 72 years (median 41) similar to the range of newbornto 71 years reported by Haight1 A probable source of expo-sure was reported in 49 cases (70) of which 22 (31)were exposed to weaponized anthrax spores as a resultof the Sverdlovsk Russia bioweapons release in 1979 (21cases)44 or the US outbreak of bioterrorism anthrax in2001 (1 case)59 13 (19) had direct exposure to livestock(usually occupational)12363941434546495056 10 (14) ingestedcontaminated meat51-5358 and four (6) had exposure tolivestock products (2 wool mill workers 1 boy who skinneda goat and 1 butcher)12293037 Additional possible sourcesof anthrax exposure included ritual head shaving48 andinsect bite45 previous studies have suggested that shaving(with either contaminated animal hair brushes or instru-ments)66 and blood-feeding insects67 can be sources of an-thrax transmission A recent experimental study hasestablished that blood-feeding insects can in fact transmitanthrax68
Portal of entry Meningoencephalitis may develop withany type of anthrax including cutaneous18123335-373942
4548525456-58 gastrointestinal2851-535558 and inhalational29-32
34404459 but in some cases the portal of entry was not iden-tified (table 1)135383943465069 Excluding the single case of inutero anthrax in Haightrsquos series1 the distribution of portalof entry in the present series differed from that reported byHaight (p 002) with a higher proportion of gastrointes-tinal and inhalational cases and a lower proportion of cu-taneous cases in the present series (see table 1)
Clinical features Anthrax meningoencephalitis pre-sents with fever headache nausea vomiting and alteredmentation (ie confusion or agitation) in association with
symptoms related to the source of infection (eg cutane-ous gastrointestinal or inhalational) Clinical signs in-clude fever (383 degC to 41 degC) malaise meningeal signs(ie nuchal rigidity Kernig and Brudzinski signs) hyper-reflexia (often with unilateral or bilateral Babinski signs)and confusion delirium stupor or coma (table 2) Otherless frequent findings include papilledema cranial neurop-athies focal or generalized seizures myoclonus fascicula-
Table 1 Primary focus of anthrax in reported cases ofanthrax meningoencephalitis
Primary focusHaight 1952
(n 73)Lanska 2002
(n 70)Total
(n 143)
Cutaneous 39 (53) 20 (29) 59 (41)
Gastrointestinal 7 (10) 12 (17)dagger 19 (13)Dagger
Inhalational 17 (23) 27 (39) 44 (31)
Maternal sepsis 1 (1) 0 (0) 1 (1)
None identified 9 (12) 11 (16) 20 (14)
Values are expressed as n ()
Includes one case mixed cutaneousdagger Includes four cases mixed cutaneousDagger Includes five cases mixed cutaneous
Table 2 Reported symptoms and signs during course ofanthrax meningoencephalitis
Symptom or sign Value
Stupor or coma 38 (78)
Fever 35 (71)
Skin lesions 24 (49)
Headache 22 (45)
Nauseavomiting 21 (43)
Seizures 20 (41)
Nuchal rigidity 18 (37)
Focal neurologic deficit 15 (31)
Confusion or agitation 13 (27)
Cranial neuropathies 13 (27)
Kernig or Brudzinski sign 11 (22)
Lateralizing long-tract signs 11 (22)
Malaise 7 (14)
Hyperreflexia 7 (14)
Respiratory symptoms 6 (12)
Decerebrate rigidity 4 (8)
Diaphoresis 3 (6)
Papilledema 3 (6)
Dizziness 2 (4)
Values are expressed as n ()
Because of variable and incomplete reporting of clinical fea-tures at onset presentation and over the course of the illnessthe frequencies may be underestimates of the frequency withwhich these symptoms and signs occurred in these patientsThese results are based on 49 cases and exclude the autopsycases from the Sverdlovsk Russia bioweapons anthrax out-break from 1979
328 NEUROLOGY 59 August (1 of 2) 2002
tions generalized rigidity lateralizing long-tract signsand decerebrate posturing
CSF Results of analyses of CSF were reported insome detail for 43 patients (table 3) eight of whom hadserial lumbar punctures113143335364048 with up to six lum-bar punctures in a single patient1314 Serial lumbar punc-tures were performed to monitor response to therapy andin some cases to administer intrathecal penicillin113142733
In some cases initial suspicion of anthrax meningoenceph-alitis was the result of CSF abnormalities In the indexcase in the 2001 US bioterrorist outbreak a diagnosis ofanthrax was considered on the basis of CSF Gramrsquos stainand ultimately confirmed by CSF culture59
CSF studies typically showed findings of hemorrhagicmeningitis (see table 3) CSF in anthrax meningoencepha-litis may appear cloudy with yellowish or pinkish colora-tion or may be grossly bloody evolution across thisspectrum has been reported in serial lumbar punctures inan individual patient1 The supernatant was frequentlyxanthochromic Opening pressure was frequently elevatedwith a range of 130 to 700 mm H2O45 Hypoglycorrhachiawas common with CSF glucose in the range of 20 to 40
mgdL but occasionally less than 20 mgdL CSF proteinconcentration was generally elevated with a range of 10 to2800 mgdL CSF was frequently hemorrhagic but early inthe illness there may be no red blood cells13273545 Therewas generally a CSF pleocytosis with from 0 to 10000white cellsmm3 with a predominance of polymorphonu-clear leukocytes There were many large gram-positiverods on Gramrsquos stain either singly or in short or longchains CSF cultures from the initial lumbar puncturewere always positive when tested although some caseswere confirmed instead by culture of swabs or fluid fromskin lesions other body fluids or postmortem tissuesamples28-3032344445 CSF may be sterile after several daysof antibiotics136 Serial lumbar punctures may documentan evolution from cloudy to grossly bloody CSF with in-creasing protein concentration increasing numbers of redcells and polymorphonuclear leukocytes and increasingpredominance of polymorphonuclear leukocytes11314 Simi-lar collective findings were reported in a recent series of 12cases that did not provide case-specific results9
Other diagnostic studies Patients with anthrax me-ningoencephalitis generally have elevated white blood cell
Table 3 CSF analyses in anthrax meningoencephalitis
Variablevalue n () Variablevalue n ()
Appearance White cells per mm3
Cloudy 15 (35) 100 4 (9)
Bloody 12 (28) 100ndash999 3 (7)
Mixed 6 (14) 1000ndash9999 15 (35)
Clear 3 (7) 10000 3 (7)
Unknown 7 (16) Unknown 18 (42)
Glucose mddL Neutrophils
20 3 (7) 50 0 (0)
20ndash40 13 (30) 50ndash79 3 (7)
40 13 (30) 80 10 (23)
Unknown 14 (33) Unknown 30 (70)
Protein mgdL Gram-stain positive
45 2 (5) Yes 33 (77)
46ndash199 4 (9) No 3 (7)
200ndash999 18 (42) Unknown 7 (16)
1000 8 (19) CSF culture positive
Unknown 11 (26) Yes 35 (81)
Red cells per mm3 No 0 (0)
100 4 (9) Unknown 8 (19)
100ndash999 5 (12)
1000ndash9999 5 (12)
10000 2 (5)
Bloody count not reported 12 (28)
Unknown 15 (35)
These results are from the initial spinal taps for 43 cases with reported CSF results Haight1 did not summarize CSF results for hisseries although he reported fairly detailed results from serial lumbar punctures in the two cases he reported For the purpose of sum-marizing CSF results in anthrax meningitis Haightrsquos two cases from 19521 and two cases with survival from the late 1940s131427 wereincluded For CSF glucose two patients with normal values were coded as 40 mgdL and one patient with a low CSFblood ratio ofglucose concentration (017) was coded as 20ndash40 mgdL Three patients had negative CSF Gram stains and CSF cultures were notdone diagnostic confirmation in these cases was based on antemortem or postmortem cultures of other tissues histology or in onecase immunohistochemistry Because of rounding percentages for each variable may not sum to 100
August (1 of 2) 2002 NEUROLOGY 59 329
counts with a left shift The range of white cell counts inthe current series was from 5400 to 27700 somewhatlower than the range of 10000 to 80000 reported byHaight1 Blood cultures were positive in 71 (ie 1521) ofcases for whom these were reported nearly identical to thevalue of 70 reported by Haight1 Chest x-rays were oftenabnormal in patients with inhalational anthrax32344059
and occasionally in patients with gastrointestinal51 or cuta-neous disease3554 Chest x-ray findings included pleuraleffusion3234405159 hilar adenopathy3240 widened mediasti-num59 infiltrates35 and soft tissue edema54
EEG results have rarely been reported even thoughseizures are fairly common In part this reflects the mori-bund state of most of these patients In one patient withreported myoclonus and fasciculations EEG showed disor-ganized low-amplitude slow waves (1 to 7 Hz)39
CT or MRI of the head in patients with anthrax menin-goencephalitis may demonstrate focal intracerebral hemor-rhage subarachnoid hemorrhage intraventricularhemorrhage diffuse cerebral edema and prominent lepto-meningeal enhancement5458 Parenchymal cerebral en-hancement has not been reported58 but its absence maysimply reflect the paucity of neuroimaging studies in thesepatients Abnormalities may progress rapidly on serialbrain imaging studies54
Differential diagnosis Hemorrhagic meningitis shouldraise suspicion of anthrax infection36 particularly if gram-positive rods are demonstrated on Gramrsquos stain Listeriamonocytogenes the only common gram-positive rod caus-ing meningitis does not produce a hemorrhagic meningitisand is rarely seen on Gramrsquos stain Based on initial clinicaldiagnoses in reported cases the differential diagnosis ofanthrax meningoencephalitis may include subarachnoidand intracerebral hemorrhage ischemic stroke nonan-thrax bacterial meningoencephalitis herpes simplex virusencephalitis and other viral encephalitides eclampsia andcerebral malaria
Treatment Antianthrax treatment was reported in 39patients1228-3840424345-5255-59 Of these 19 (49) receivedpenicillin only28-32353842454849525658 (administered parenter-ally in all but one case)2930 19 (49) received penicillin (orin one case ampicillin)55 in combination with other antibi-otic therapy12293032-343637404345-475051555759 and one (3) re-ceived antianthrax serum only33 Antibiotics used inconjunction with penicillin therapy included chloramphen-icol (11 cases)33364345-475057 streptomycin (7 cas-es)1229303233374051 sulfonamides (4 cases)122930364557
cefotaxime (2 cases)5559 tetracyclines (1 case)33 vancomy-cin (1 case)59 and antianthrax serum (1 case)33 Corticoste-roids were administered in conjunction with antibiotics inten cases (26)3336424345485257 In the Sverdlovsk inhala-tional anthrax outbreak in 1979 hospitalized patientswere treated variously with penicillin cephalosporinchloramphenicol antianthrax globulin and corticoste-roids62 but case-specific treatments and outcomes were notreported in the English language literature either in gen-eral or for the 21 patients autopsied after dying with an-thrax meningoencephalitis446263
Prognosis Septicemia toxic shock and death rapidlyfollow development of anthrax meningoencephalitis inmost cases Many patients presented in extremis followinga prodromal period of 1 to 6 days and 75 died within 24hours of presentation (ie 4155 of cases for whom such
information was available)28-3538394144-4749-5269 Four pa-tients (6) in the present series survived36374851 comparedwith three (4) in the previous world literature a differ-ence that was not significant (p 071) (table 4) Exclud-ing the 21 cases of inhalational anthrax from theSverdlovsk autopsy series44 estimated survival in the cur-rent series is four of 49 (8) and in all reported cases todate is seven of 122 (6) the difference in survival be-tween this restricted group of deceased patients and thesurviving patients was also not significant (p 044) Re-ported additional cases of survival had no clinical informa-tion (two cases)7 or were not established microbiologicallyor pathologically as cases of anthrax (one case)11 An addi-tional recent series of 12 cases with no survivals did notreport case-specific information9
Survival appears to be most likely if meningoencephali-tis develops as part of the course of cutaneous an-thrax363748 but a single case with survival has beenreported with gastrointestinal anthrax51 In the currentseries 15 of cutaneous cases survived compared with 8among gastrointestinal cases none among inhalationalcases and none among unknown or unspecified cases (seetable 3) The difference in survival of the cutaneous casesin the current series (15) and Haightrsquos series (5) wasnot significant (p 032) To date in the world literaturethere are no reported cases of survival following anthraxmeningoencephalitis associated with inhalational anthrax
The seven surviving patients reported to date are sum-marized in table 513-15273637485170 Surviving patients wereyounger as a group than those in the present series whodied (median age of surviving cases 24 years n7 me-dian age of cases who died 45 years n 66 p 004) Ifthe comparison is restricted to cases in the current seriesonly the difference in age is greater (median age of surviv-ing cases 1025 years n 4 p 0003) In generalinitial CSF results from the surviving patients were eithernormal or were less severely abnormal compared to de-ceased patients However because of the small samplesizes for different CSF studies in the survival group noneof the individual contrasts was significant (glucose p 041 protein p 012 red cells p 024 white cellsp 008)
Many reports and reviews failed to identify all of thepreviously reported cases with survival or misreported as-pects of the cases they did review resulting in incorrectconclusions about the agents that are potentially effective
Table 4 Survival with anthrax meningoencephalitis inreported cases
Primary focus Haight 1952 Lanska 2002 Total
Cutaneous 239 (5) 320 (15) 559 (8)
Gastrointestinal 07 (0) 112 (8) 119 (5)
Inhalational 017 (0) 027 (0) 044 (0)
Maternal sepsis 01 (0) 01 (0)
None identified 19 (11) 011 (0) 120 (5)
Total 373 (4) 470 (6) 7143 (5)
Values are expressed as n ()
Excluding the 21 inhalational cases from the Sverdlovsk autopsyseries estimated survival in the current series is 449 (8) andin reported cases to date is 7122 (6)
330 NEUROLOGY 59 August (1 of 2) 2002
treatments The treatments administered to surviving pa-tients were in fact similar to those chosen in the entiregroup of patients in the current series All of the patientsreceived penicillin except the first case (Patient 1) whoreportedly received no treatment (Bernd Remler MD per-sonal communication February 2002)70 Only two of thepatients received corticosteroids in addition to antibiotics(Patients 4 and 6)3648 The only case with gastrointestinalanthrax (Patient 7) received the same treatment as hissister (aged 2 years) who died51 Treatment of survivingpatients was generally begun before the disease was clini-cally advanced Three of the patients who survived (Pa-tients 2 through 4) were receiving treatment for cutaneousanthrax (that included penicillin) before development ofsymptoms of meningoencephalitis13-152736 There is limitedinformation on long-term outcomes among the survivorsbut most were reported to have fully recovered13-1527363751
although two patients had residual focal weakness4870
Autopsy findings Autopsies were obtained in 40 of the66 deceased patients (61)28-32343538-4043-454755-5759 Thissummary is restricted to pathologic findings in the centralnervous system Gross findings typically included cloudyand congested leptomeninges with occasional obvious pu-rulent exudate13034354447 and with variable degrees of sub-arachnoid hemorrhage128293135394044455557 In many casessubarachnoid hemorrhage was the dominant gross patho-logic feature1282931353940444555 The vascular congestionand extensive subarachnoid hemorrhage of the leptome-ninges gave a dark red appearance on gross examination ofthe brain a finding sometimes referred to as a ldquocardinalrsquoscaprdquo2 Other common findings included intraventricularhemorrhage2939 intracerebral hematoma13956 multifocalsmall intraparenchymal cortical hemorrhages394047 or nu-merous petechial hemorrhages in cerebral parenchyma2864
zones of infarction in arterial venous or watershed distri-butions3964 and cerebral edema35454757 with tonsillar35 oruncal herniation47
Microscopic findings included hemorrhagic leptomen-ingitis2930343538-404447555764 and associated necrotizing vas-
culitis164 multifocal subarachnoid128-313538-404445555764 andintracerebral hemorrhage128-3038394756 multifocal cerebralinfarction3964 and leptomeningeal and cerebral ede-ma35394445475764 The hemorrhagic leptomeningitis was as-sociated with polymorphonuclear leukocytic inflammatoryexudates3538444755-5764 severe congestion of meningealblood vessels3538404756 hemorrhagic infiltration3544455664 orfrank subarachnoid hemorrhage128-313538-404445555764 aggre-gations of neutrophils and mononuclear phagocytes in andaround meningeal vessels3538404764 and tracking of bloodand inflammatory infiltrates along the VirchowndashRobin(perivascular) spaces into the parenchyma47 The superfi-cial cerebral cortex showed diffuse perineuronal andperivascular infiltration by neutrophils353947 severe vascu-lar congestion3540 necrosis of blood vessel walls3539475664
recent thromboses353964 zones of ischemia3964 areas ofhemorrhage47 and edema35394445475764 Numerous largegram-positive rods in short chains were present in theleptomeninges and the subarachnoid and VirchowndashRobinspaces29-31344756 within and around meningeal and superfi-cial cortical vessels and vessels in regions of hemor-rhage313235394064 and within hemorrhagic lesions313247
Discussion Meningoencephalitis develops in atmost 5 of cases of cutaneous anthrax1428 howevermost cases of anthrax meningoencephalitis to datehave developed from cutaneous anthrax because thevast majority of naturally acquired cases of anthraxare cutaneous28 Meningoencephalitis may occur inup to half of the cases in industrial or bioweaponsoutbreaks of inhalational anthrax829303244 howeverin the recent bioterrorist outbreak of anthrax in theUnited States only the index case had meningitisamong the 11 cases of confirmed or suspected inhala-tional anthrax identified5971-73 The relatively low fre-quency of meningitis among anthrax cases in the USbioterrorism outbreak may be misleading though aslumbar punctures were done in few cases and the
Table 5 Patients with anthrax meningoencephalitis who survived
Variable
Patient no
1 2 3 4 5 6 7
Reference no 70 14 27 36 37 48 51
Year 1916 1947 1948 1972 1973 1989 1993
Age y 24 57 51 85 12 25 6
Sex F M M F M M M
Clinical type Unknown Cutaneous Cutaneous Cutaneous Cutaneous Cutaneous Gastrointestinal
Treatment None
Antianthrax serum X
Penicillin X X X X X X
Chloramphenicol I
Streptomycin X X
Sulfonamide X I
Corticosteroid X X
Residual L hemiparesis None None None None RUE weakness None
X main therapy I initial therapy only RUE right upper extremity
August (1 of 2) 2002 NEUROLOGY 59 331
brain was not examined in some autopsies Based onprevious experience44 the potential exists for largenumbers of cases of anthrax meningoencephalitiswith further bioterrorist outbreaks or bioweaponsdispersals Meningoencephalitis may also occur withgastrointestinal anthrax or without a clinically ap-parent primary focus
Current guidelines from the Centers for DiseaseControl indicate that ciprofloxacin or doxycyclineshould be included as essential components of initialtherapy for anthrax infections of any portal of en-try7274 It is important to treat anthrax meningoen-cephalitis with a polydrug antibiotic regimen usingantimicrobial agents that have good CSF penetrationin meningitis and that provide good antibacterialcoverage for B anthracis All six patients who sur-vived after antibiotic treatment for anthrax menin-goencephalitis were treated with penicillinHowever because of the presence of constitutive orinducible beta-lactamases in B anthracis isolatesfrom the recent US bioterrorist outbreak and expec-tations that beta-lactamase activity may be likelywith bioengineered bioweapons agents ampicillin orpenicillin G alone are not recommended for initialtherapy for anthrax meningoencephalitis prior to an-tibiotic sensitivity results from culture7274 Rifampinplus vancomycin would be a reasonable choice foraddition to ciprofloxacin or doxycycline in the initialtreatment of anthrax meningoencephalitis Some in-fectious disease authorities recommend ciprofloxacinin preference to doxycycline plus augmentation withchloramphenicol rifampin or penicillin for estab-lished or suspected anthrax meningoencephalitis6
Aztreonam trimethoprim-sulfamethoxazole orthird-generation cephalosporins should not be usedbecause of natural resistance of B anthracis strainsto these antibiotics
Bacterial toxins have long been felt to play a ma-jor role in anthrax meningoencephalitis becausemany effects of B anthracis cannot be attributed tomicroscopically evident tissue changes1075 Virulenceof B anthracis requires an antiphagocytic capsuleand two exotoxins The two toxins are binary pro-teins composed of a binding protein and an enzymat-ically active protein2476 Among other actions thesetoxins collectively produce local edema impair neu-trophil function depress cerebral cortical electricalactivity depress central respiratory center activitycause bleeding and destruction of the brain and vitalorgans in the chest and induce cardiovascular col-lapse and shock244476-79
Although antitoxin was used early in the 20thcentury to treat anthrax alone or in combinationwith penicillin13-15 it has not been available in recentdecades to US civilian populations Conceptually an-tianthrax serum may augment the effect of antibiot-ics by helping to neutralize the anthrax toxinswhich are not inactivated by antibiotics Howeverthere are no documented cases of successful treat-ment of anthrax meningitis with antianthrax serumalone Haight incorrectly stated that a case reported
by Czyhlarz in 191670 had been cured by treatmentwith antianthrax serum when in fact a full transla-tion indicates that the patient received no treatment(Bernd Remler MD personal communication Feb-ruary 2002 see supplementary document) this er-ror has been promulgated by numerous subsequentauthors and has been a source of incorrect conclu-sions regarding potentially effective therapy for an-thrax meningoencephalitis in recent reviewsCzyhlarz70 also presented unpublished second-handinformation on another patient who purportedly re-covered from anthrax meningoencephalitis withouttreatment In light of subsequent experience withthis disease it is hard to interpret or credit either ofthese reports Available experimental data80 do notindicate a significant treatment effect of antianthraxserum beyond that of penicillin Nevertheless anti-anthrax immune globulin derived from the blood ofsoldiers who have received the anthrax vaccine isbeing added to the US bioterrorism treatment stock-pile and is being considered as a potential experi-mental anthrax treatment in the event of furtherbioterrorism anthrax cases681
Corticosteroids have been recommended as an ad-junctive agent in the treatment of meningitis in chil-dren82 Use of corticosteroids in adults withmeningitis is controversial but steroids have beenrecommended for consideration as adjunctive agentswithout any age restriction in anthrax meningitis72
If corticosteroids are used in conjunction with vanco-mycin therapy antibiotic dosing may need to bemodified because CSF vancomycin levels may be de-creased by corticosteroids contributing to treatmentfailure82-86
In addition to antibiotic management patientswith anthrax meningoencephalitis may require ag-gressive intensive care measures Seizures in-creased intracranial pressure subarachnoid andintracerebral hemorrhage electrolyte disturbanceshypotension shock and disseminated intravascularcoagulation may develop as complications of this in-fection Despite aggressive treatment the prognosisfor survival with anthrax meningoencephalitis isvery poor
AcknowledgmentThe author thanks Glen Salter MS of the Tomah VA MedicalCenter Library for assistance in locating references Pat Mennickeof the Tomah VA Medical Center for assistance with Excel spread-sheets Bernd Remler MD of the Medical College of WisconsinMilwaukee for translating the paper by Czyhlarz Larry DavisMD of the Albuquerque VA Medical Center for helpful correspon-dence regarding corticosteroids and vancomycin Jeffrey M JonesMD PhD of the William S Middleton VA Medical Center Madi-son for helpful discussions regarding antibiotic treatment of an-thrax meningoencephalitis and Mary Jo Lanska MD MS of theTomah VA Medical Center for helpful discussions and for criti-cally reviewing the manuscript
References1 Haight TH Anthrax meningitis review of literature and report
of two cases with autopsies Am J Med Sci 195222457ndash692 Dixon TC Meselson M Guillemin J Hanna PC Anthrax
N Engl J Med 1999341815ndash826
332 NEUROLOGY 59 August (1 of 2) 2002
3 Inglesby TV Henderson DA Bartlett JG et al Anthrax as abiological weapon medical and public health managementJAMA 19992811735ndash1745
4 Swartz MN Recognition and management of anthrax an up-date N Engl J Med 20013451621ndash1626
5 Jernigan JA Stephens DS Ashford DA et al Bioterrorism-related inhalational anthrax the first 10 cases reported in theUnited States Emerg Infect Dis 20017933ndash944
6 Inglesby TV OrsquoToole T Henderson DA et al Anthrax as abiological weapon 2002 updated recommendations for man-agement JAMA 20022872236ndash2252
7 Miller JK Human anthrax in New York State NY StateJ Med 1961612046ndash2053
8 Brachman PS Human anthrax in the United States Antimi-crob Agents Chemother 19655111ndash114
9 Kumar A Kanungo R Bhattacharya S Badrinath S DuttaTK Swaminathan RP Human anthrax in India urgent needfor effective prevention J Commun Dis 200032240ndash246
10 Dutz W Kohout E Anthrax Pathol Annu 197162009ndash224811 Trivedy JR Case of anthrax meningitis survival Cent Afr
J Med 19812716612 Roberts CJ Chambers PG An outbreak of anthrax in the
Mondoro Tribal Trust lands Cent Afr J Med 19752173ndash7613 Kindler D Recovery from anthrax meningitis Ind Med Surg
195221487ndash48814 Shanahan RH Griffin JR Von Auersperg AP Anthrax men-
ingitis report of a case of internal anthrax with recoveryAm J Clin Pathol 194717719ndash722
15 Griffin JR Shanahan RH DeAngelis CE Treatment of cuta-neous anthrax with penicillin NY State J Med 1948481718ndash1721
16 Boudin G Lauras A Vaillant C Etat de mal eacutepileptiquereacuteveacutelateur drsquoune meacuteningite charbonneuse etude anatamo-clinique Bull Mem Soc Med Hop Paris 1964115183ndash187
17 Rapun Pac JL Ull Laita M Meningitis carbuncosa Arch Neu-robiol (Madr) 197235143ndash148
18 Baltiev A Besleaga E Cuciureanu G Obreja E Meningo-encefalita carbunoasa la un copil cu pustula cutanata necarac-teristica Rev Med Chir Soc Med Nat Iasi 197377885ndash888
19 Beer K Milzbrandmeningitis Path Microbiol 19733912ndash1320 Bach I Simon L Baacuten E Toacuteth L Kovaacutecs M Haemorrhagiaacutes
meningitises apoplexia anthrax sepsisben Orv Hetil 19781191797ndash1799
21 Marandian MH Kamali A Meacuteningite charbonneuse un casen apparence primitif Nouv Presse Med 1981101747ndash1748
22 Duumlrst UN Bartenstein J Buumlhlmann H Wuumlst J Spiegel MVAnthraxmeningitis Schweiz Med Wochenschr 19861161222ndash1228
23 Gonzalez A Rodriguez E Castillo M Ortega I Ramirez EFajardo J Lesioacuten necroacutetica en mentoacuten en paciente con siacuten-drome meniacutengeo Enferm Infecc Mircobiol Clin 199715163ndash164
24 Abramova AA Grinberg LM [Pathology of anthrax sepsisaccording to materials of the infectious outbreak in 1979 inSverdlovsk (macroscopic changes)] Arkh Patol 19935512ndash17
25 Abramova AA Grinberg LM [Pathology of anthrax sepsisaccording to materials of infectious outbreak in 1979 in Sverd-lovsk (microscopic changes)] Arkh Patol 19935518ndash23
26 Grinberg LM Abramova AA [Pathology of anthrax sepsisaccording to materials of the infectious outbreak in 1979 inSverdlovsk (various aspects of morpho- patho- and thanato-genesis] Arkh Patol 19935523ndash26
27 Weinstein L Oliver CS The treatment of human anthraxwith penicillin Am Pract 19482533ndash538
28 Raper AB Anthrax meningo-encephalitis East Afr Med J195330399-401
29 Albrink WS Brooks SM Biron RE Kopel M Human inhala-tional anthrax a report of three fatal cases Am J Pathol196036457ndash468
30 Plotkin SA Brachman PS Utell M Bumford FH AtchisonMM An epidemic of inhalation anthrax the first in the twen-tieth century I Clinical features Am J Med 196029992ndash1001
31 Brachman PS Pagano JS Albrink WS Two cases of fatalinhalation anthrax one associated with sarcoidosis N EnglJ Med 1961265203ndash208
32 Brachman PS Inhalation anthrax Ann NY Acad Sci 198035383ndash93
33 Vita A Secu A Cuciureanu G Leibovici M Bejanariu C CujuG Considerations on 3 cases of meningo-encephalitis due toanthrax bacilli Rom Med Rev 1961536ndash39
34 LaForce FM Bumford FH Freely JC Stokes SL Snow DBEpidemiologic study of a fatal case of inhalation anthrax ArchEnviron Health 196918798ndash805
35 Rangel RA Gonzaacutelez DA Bacillus anthracis meningitis Neu-rology 197525525ndash530
36 Tahernia AC Hashemi G Survival in anthrax meningitisPediatrics 197250329ndash333
37 Tengio FU Anthrax meningitis report of two cases East AfrMed J 197350337ndash339
38 Viratchai C Anthrax gastro-enteritis and meningitis J MedAssoc Thai 197457147ndash150
39 Pluot M Vital C Aubertin J Croix JC Pire JC Poisot DAnthrax meningitis report of two cases with autopsies ActaNeuropathol (Berl) 197636339ndash345
40 Suffin SC Carnes WH Kaufman AF Inhalation anthrax in ahome craftsman Hum Pathol 19789594ndash597
41 Al-Dulaimy SB Al-Allaf GA Anthrax meningitis Trans R SocTrop Med Hyg 197872315
42 Manios S Kavaliotis I Anthrax in children a long forgottenpotentially fatal condition Scand J Infect Dis 197911203ndash206
43 Koshi G Lalitha MK Daniel J Chacko A Pulimood BMAnthrax meningitis a rare clinical entity J Assoc PhysiciansIndia 19812959ndash62
44 Abramova FA Grinberg LM Tampolskaya OV Walker DHPathology of inhalational anthrax in 42 cases from the Sverd-lovsk outbreak of 1979 Proc Natl Acad Sci USA 1993902291ndash2294
45 Levy L Baker N Meyer MP Crosland P Hampton J Anthraxmeningitis in Zimbabwe Cent Afr J Med 198127101ndash104
46 Bhat P Pereira P Mohan N Primary anthrax meningitis acase report Neurol India 19833171ndash73
47 Chandramukhi A Shankar P Rao TV Sundararajan SSwamy HS Acute leptomeningitis due to Bacillus anthracis acase report Trop Geogr Med 19833579ndash82
48 Khanna N Gokul BN Ravikumar R et al Successfullytreated primary anthrax meningitis Indian J Pathol Micro-biol 198932315ndash317
49 Kanungo R Sujatha S Das AK Rao RS Anthrax meningitisa clinical enigma Indian J Med Microbiol 19906149ndash151
50 Bharathmoorthy Chakravarthy I Swaminathan RP et alHaemorrhagic meningitis due to Bacillus anthrax J AssocPhysicians India 199240134ndash135
51 Tabatabaie P Syadati A Bacillus anthracis as a cause ofbacterial meningitis Pediatr Infect Dis 1993121035ndash1037
52 George S Mathai D Balraj V Lalitha MK John TJ An out-break of anthrax meningoencephalitis Trans R Soc Trop MedHyg 199488206ndash207
53 Berthier M Fauchegravere J-L Perrin J Grignon B Oriot D Ful-minant meningitis due to Bacillus anthracis in 11-year-oldgirl during Ramadan Lancet 1996347828
54 Domiacutenguez E Bustos C Garcia M Recio S Anthrax meningo-encephalitis radiologic findings AJR Am J Roentgenol 1997169317
55 Kwong KL Que TL Wong SN So KT Fatal meningoenceph-alitis due to Bacillus anthracis J Paediatr Child Health 199733539ndash541
56 Garcia AG Jiminez RR Bacillus anthracis meningitis N EnglJ Med 1999341814
57 Ringertz SH Hoiby EA Jensenius M et al Injectional an-thrax in a heroin skin-popper Lancet 20003461574ndash1575
58 Kim HJ Jun WB Lee SH Rho MH CT and MR findings ofanthrax meningoencephalitis report of two cases and reviewof the literature AJNR Am J Neuroradiol 2001221303ndash1305
59 Bush LM Abrams BH Heall A Johnson CC Index case offatal inhalational anthrax due to bioterrorism in the UnitedStates N Engl J Med 20013451607ndash1610
60 Brachman PS Plotkin SA Bumford FH Atchison MM Anepidemic of inhalation anthrax the first in the twentieth cen-tury II Epidemiology Am J Hygiene 1960726ndash23
61 Belluck P Anthrax outbreak of rsquo57 felled a mill but yieldedanswers New York Times October 27 2001B8
62 Meselson M Guillemin J Hugh-Jones M et al The Sverd-lovsk anthrax outbreak of 1979 Science 19942661202ndash1208
August (1 of 2) 2002 NEUROLOGY 59 333
63 Jackson PJ Hugh-Jones ME Adair DM et al PCR analysis oftissue samples from the 1979 Sverdlovsk anthrax victims thepresence of multiple Bacillus anthracis strains in differentvictims Proc Natl Acad Sci USA 1998951224ndash1229
64 Grinberg LM Abramova FA Yampolskaya OV Walker DHSmith JH Quantitative pathology of inhalational anthrax IQuantitative microscopic findings Mod Pathol 200114482ndash495
65 Brookmeyer R Blades N Hugh-Jones M Henderson D Thestatistical analysis of truncated data application to the Sverd-lovsk anthrax outbreak Biostatistics 20012233ndash247
66 Knott FA A note on anthrax infection by shaving brushesLancet 19231227ndash228
67 Bradaric N Punda-Polic V Cutaneous anthrax due topenicillin-resistant Bacillus anthracis transmitted by an in-sect bite Lancet 1992340306ndash307
68 Turell MJ Knudson GB Mechanical transmission of Bacillusanthracis by stable flies (Stomoxys calcitrans) and mosquitoes(Aedes aegypti and Aedes taeniorhynchus) Infect Immun1987551859ndash1861
69 Drake DJ Meningitic anthrax Cent Afr J Med 19711797ndash9870 Czyhlarz EV Beitrag zur Lehre von der Milzbrandmeningitis
Wein Klin Wochenscr 191629768ndash76971 Centers for Disease Control Investigation of anthrax associ-
ated with intentional exposure and interim public healthguidelines October 2001 MMWR Morb Mortal Wkly Rep200150889ndash893
72 Centers for Disease Control Update investigation ofbioterrorism-related anthrax and interim guidelines for expo-sure management and antimicrobial therapy October 2001MMWR Morb Mortal Wkly Rep 200150909ndash919
73 Centers for Disease Control Investigation of bioterrorism-related anthrax and interim guidelines for clinical evaluationof persons with possible anthrax MMWR Morb Mortal WklyRep 200150941ndash948
74 Centers for Disease Control Updated recommendations forantimicrobial prophylaxis among asymptomatic pregnantwomen after exposure to Bacillus anthracis MMWR MorbMortal Wkly Rep 200150960
75 Bonventure PF Sueoka W True CW Klein F Lincoln RAttempts to implicate the central nervous system as a pri-
mary site of action for Bacillus anthracis lethal toxin FedProc 1967261549ndash1553
76 Friedlander AM Anthrax In Sidell FR Takafuji ET FranzDR eds Textbook of military medicine medical aspects ofchemical and biological warfare Washington DC Office ofthe Surgeon General 1997467ndash478
77 Vick JA Lincoln RE Klein F Mahlandt BG Walker JS FishDC Neurological and physiological responses of the primateto anthrax toxin J Infect Dis 196811885ndash96
78 Klein F Lincoln RE Dobbs JP Mahlandt BG Remmele NSWalker JS Neurological and physiological responses of theprimate to anthrax infection J Infect Dis 196811897ndash103
79 Remmele NS Klein F Vick JA Walker JS Mahlandt BGLincoln RE Anthrax toxin primary site of action J Infect Dis1968118104ndash113
80 Doganay M Hanagasi R Zora A [Evaluation of penicillinalone and penicillin combined with anti-anthrax serum in ex-perimental anthrax in mice] Mikrobiyol Bul 19851957ndash64
81 Associated Press Government may offer anthrax treatmentNew York Times January 7 2002
82 Davis LE Acute bacterial meningitis In Johnson RT GriffinJW eds Current therapy in neurologic disease 5th ed StLouis Mosby 1997120ndash127
83 Viladrich PF Gudiol F Lintildeares J et al Evaluation of vanco-mycin for therapy of adult pneumococcal meningitis Antimi-crob Agents Chemother 1991352467ndash2472
84 Pariacutes M Hickey SM Uscher MI Shelton S Olsen KD Mc-Cracken GH Jr Effect of dexamethasone on therapy of exper-imental penicillin- and cephalosporin-resistant pneumococcalmeningitis Antimicrob Agents Chemother 1994381320ndash1324
85 Cabellos C Martinez-Lacasa J Martos A et al Influence ofdexamethasone on efficacy of ceftriaxone and vancomycintherapy in experimental pneumococcal meningitis AntimicrobAgents Chemother 1995392158ndash2160
86 Ahmed A Jafri H Lutsar I et al Pharmacodynamics of van-comycin for the treatment of experimental penicillin- andcephalosporin-resistant pneumococcal meningitis AntimicrobAgents Chemother 199943876ndash881
334 NEUROLOGY 59 August (1 of 2) 2002
DOI 101212WNL593327200259327-334 Neurology
Douglas J LanskaAnthrax meningoencephalitis
This information is current as of August 13 2002
ServicesUpdated Information amp
httpwwwneurologyorgcontent593327fullhtmlincluding high resolution figures can be found at
Supplementary Material
htmlhttpwwwneurologyorgneurologysuppl20020716593327DC2
htmlhttpwwwneurologyorgneurologysuppl20020716593327DC1Supplementary material can be found at
References httpwwwneurologyorgcontent593327fullhtmlref-list-1
This article cites 73 articles 15 of which you can access for free at
Citations httpwwwneurologyorgcontent593327fullhtmlotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpwwwneurologyorgcgicollectionmeningitisMeningitis
httpwwwneurologyorgcgicollectionencephalitisEncephalitis
httpwwwneurologyorgcgicollectionbacterial_infectionsBacterial infections
httpwwwneurologyorgcgicollectionall_infectionsAll Infectionsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsin its entirety can be found online atInformation about reproducing this article in parts (figurestables) or
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
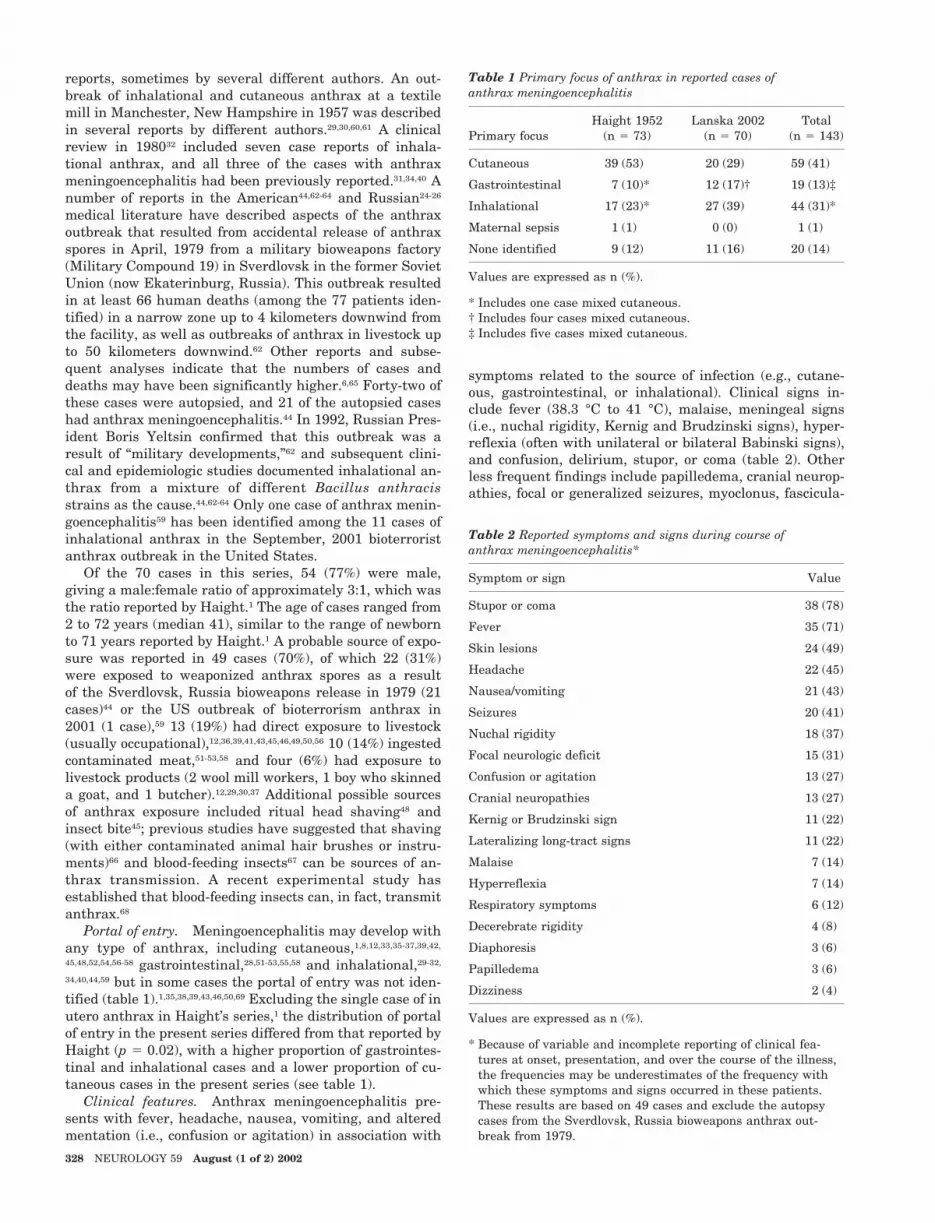
reports sometimes by several different authors An out-break of inhalational and cutaneous anthrax at a textilemill in Manchester New Hampshire in 1957 was describedin several reports by different authors29306061 A clinicalreview in 198032 included seven case reports of inhala-tional anthrax and all three of the cases with anthraxmeningoencephalitis had been previously reported313440 Anumber of reports in the American4462-64 and Russian24-26
medical literature have described aspects of the anthraxoutbreak that resulted from accidental release of anthraxspores in April 1979 from a military bioweapons factory(Military Compound 19) in Sverdlovsk in the former SovietUnion (now Ekaterinburg Russia) This outbreak resultedin at least 66 human deaths (among the 77 patients iden-tified) in a narrow zone up to 4 kilometers downwind fromthe facility as well as outbreaks of anthrax in livestock upto 50 kilometers downwind62 Other reports and subse-quent analyses indicate that the numbers of cases anddeaths may have been significantly higher665 Forty-two ofthese cases were autopsied and 21 of the autopsied caseshad anthrax meningoencephalitis44 In 1992 Russian Pres-ident Boris Yeltsin confirmed that this outbreak was aresult of ldquomilitary developmentsrdquo62 and subsequent clini-cal and epidemiologic studies documented inhalational an-thrax from a mixture of different Bacillus anthracisstrains as the cause4462-64 Only one case of anthrax menin-goencephalitis59 has been identified among the 11 cases ofinhalational anthrax in the September 2001 bioterroristanthrax outbreak in the United States
Of the 70 cases in this series 54 (77) were malegiving a malefemale ratio of approximately 31 which wasthe ratio reported by Haight1 The age of cases ranged from2 to 72 years (median 41) similar to the range of newbornto 71 years reported by Haight1 A probable source of expo-sure was reported in 49 cases (70) of which 22 (31)were exposed to weaponized anthrax spores as a resultof the Sverdlovsk Russia bioweapons release in 1979 (21cases)44 or the US outbreak of bioterrorism anthrax in2001 (1 case)59 13 (19) had direct exposure to livestock(usually occupational)12363941434546495056 10 (14) ingestedcontaminated meat51-5358 and four (6) had exposure tolivestock products (2 wool mill workers 1 boy who skinneda goat and 1 butcher)12293037 Additional possible sourcesof anthrax exposure included ritual head shaving48 andinsect bite45 previous studies have suggested that shaving(with either contaminated animal hair brushes or instru-ments)66 and blood-feeding insects67 can be sources of an-thrax transmission A recent experimental study hasestablished that blood-feeding insects can in fact transmitanthrax68
Portal of entry Meningoencephalitis may develop withany type of anthrax including cutaneous18123335-373942
4548525456-58 gastrointestinal2851-535558 and inhalational29-32
34404459 but in some cases the portal of entry was not iden-tified (table 1)135383943465069 Excluding the single case of inutero anthrax in Haightrsquos series1 the distribution of portalof entry in the present series differed from that reported byHaight (p 002) with a higher proportion of gastrointes-tinal and inhalational cases and a lower proportion of cu-taneous cases in the present series (see table 1)
Clinical features Anthrax meningoencephalitis pre-sents with fever headache nausea vomiting and alteredmentation (ie confusion or agitation) in association with
symptoms related to the source of infection (eg cutane-ous gastrointestinal or inhalational) Clinical signs in-clude fever (383 degC to 41 degC) malaise meningeal signs(ie nuchal rigidity Kernig and Brudzinski signs) hyper-reflexia (often with unilateral or bilateral Babinski signs)and confusion delirium stupor or coma (table 2) Otherless frequent findings include papilledema cranial neurop-athies focal or generalized seizures myoclonus fascicula-
Table 1 Primary focus of anthrax in reported cases ofanthrax meningoencephalitis
Primary focusHaight 1952
(n 73)Lanska 2002
(n 70)Total
(n 143)
Cutaneous 39 (53) 20 (29) 59 (41)
Gastrointestinal 7 (10) 12 (17)dagger 19 (13)Dagger
Inhalational 17 (23) 27 (39) 44 (31)
Maternal sepsis 1 (1) 0 (0) 1 (1)
None identified 9 (12) 11 (16) 20 (14)
Values are expressed as n ()
Includes one case mixed cutaneousdagger Includes four cases mixed cutaneousDagger Includes five cases mixed cutaneous
Table 2 Reported symptoms and signs during course ofanthrax meningoencephalitis
Symptom or sign Value
Stupor or coma 38 (78)
Fever 35 (71)
Skin lesions 24 (49)
Headache 22 (45)
Nauseavomiting 21 (43)
Seizures 20 (41)
Nuchal rigidity 18 (37)
Focal neurologic deficit 15 (31)
Confusion or agitation 13 (27)
Cranial neuropathies 13 (27)
Kernig or Brudzinski sign 11 (22)
Lateralizing long-tract signs 11 (22)
Malaise 7 (14)
Hyperreflexia 7 (14)
Respiratory symptoms 6 (12)
Decerebrate rigidity 4 (8)
Diaphoresis 3 (6)
Papilledema 3 (6)
Dizziness 2 (4)
Values are expressed as n ()
Because of variable and incomplete reporting of clinical fea-tures at onset presentation and over the course of the illnessthe frequencies may be underestimates of the frequency withwhich these symptoms and signs occurred in these patientsThese results are based on 49 cases and exclude the autopsycases from the Sverdlovsk Russia bioweapons anthrax out-break from 1979
328 NEUROLOGY 59 August (1 of 2) 2002
tions generalized rigidity lateralizing long-tract signsand decerebrate posturing
CSF Results of analyses of CSF were reported insome detail for 43 patients (table 3) eight of whom hadserial lumbar punctures113143335364048 with up to six lum-bar punctures in a single patient1314 Serial lumbar punc-tures were performed to monitor response to therapy andin some cases to administer intrathecal penicillin113142733
In some cases initial suspicion of anthrax meningoenceph-alitis was the result of CSF abnormalities In the indexcase in the 2001 US bioterrorist outbreak a diagnosis ofanthrax was considered on the basis of CSF Gramrsquos stainand ultimately confirmed by CSF culture59
CSF studies typically showed findings of hemorrhagicmeningitis (see table 3) CSF in anthrax meningoencepha-litis may appear cloudy with yellowish or pinkish colora-tion or may be grossly bloody evolution across thisspectrum has been reported in serial lumbar punctures inan individual patient1 The supernatant was frequentlyxanthochromic Opening pressure was frequently elevatedwith a range of 130 to 700 mm H2O45 Hypoglycorrhachiawas common with CSF glucose in the range of 20 to 40
mgdL but occasionally less than 20 mgdL CSF proteinconcentration was generally elevated with a range of 10 to2800 mgdL CSF was frequently hemorrhagic but early inthe illness there may be no red blood cells13273545 Therewas generally a CSF pleocytosis with from 0 to 10000white cellsmm3 with a predominance of polymorphonu-clear leukocytes There were many large gram-positiverods on Gramrsquos stain either singly or in short or longchains CSF cultures from the initial lumbar puncturewere always positive when tested although some caseswere confirmed instead by culture of swabs or fluid fromskin lesions other body fluids or postmortem tissuesamples28-3032344445 CSF may be sterile after several daysof antibiotics136 Serial lumbar punctures may documentan evolution from cloudy to grossly bloody CSF with in-creasing protein concentration increasing numbers of redcells and polymorphonuclear leukocytes and increasingpredominance of polymorphonuclear leukocytes11314 Simi-lar collective findings were reported in a recent series of 12cases that did not provide case-specific results9
Other diagnostic studies Patients with anthrax me-ningoencephalitis generally have elevated white blood cell
Table 3 CSF analyses in anthrax meningoencephalitis
Variablevalue n () Variablevalue n ()
Appearance White cells per mm3
Cloudy 15 (35) 100 4 (9)
Bloody 12 (28) 100ndash999 3 (7)
Mixed 6 (14) 1000ndash9999 15 (35)
Clear 3 (7) 10000 3 (7)
Unknown 7 (16) Unknown 18 (42)
Glucose mddL Neutrophils
20 3 (7) 50 0 (0)
20ndash40 13 (30) 50ndash79 3 (7)
40 13 (30) 80 10 (23)
Unknown 14 (33) Unknown 30 (70)
Protein mgdL Gram-stain positive
45 2 (5) Yes 33 (77)
46ndash199 4 (9) No 3 (7)
200ndash999 18 (42) Unknown 7 (16)
1000 8 (19) CSF culture positive
Unknown 11 (26) Yes 35 (81)
Red cells per mm3 No 0 (0)
100 4 (9) Unknown 8 (19)
100ndash999 5 (12)
1000ndash9999 5 (12)
10000 2 (5)
Bloody count not reported 12 (28)
Unknown 15 (35)
These results are from the initial spinal taps for 43 cases with reported CSF results Haight1 did not summarize CSF results for hisseries although he reported fairly detailed results from serial lumbar punctures in the two cases he reported For the purpose of sum-marizing CSF results in anthrax meningitis Haightrsquos two cases from 19521 and two cases with survival from the late 1940s131427 wereincluded For CSF glucose two patients with normal values were coded as 40 mgdL and one patient with a low CSFblood ratio ofglucose concentration (017) was coded as 20ndash40 mgdL Three patients had negative CSF Gram stains and CSF cultures were notdone diagnostic confirmation in these cases was based on antemortem or postmortem cultures of other tissues histology or in onecase immunohistochemistry Because of rounding percentages for each variable may not sum to 100
August (1 of 2) 2002 NEUROLOGY 59 329
counts with a left shift The range of white cell counts inthe current series was from 5400 to 27700 somewhatlower than the range of 10000 to 80000 reported byHaight1 Blood cultures were positive in 71 (ie 1521) ofcases for whom these were reported nearly identical to thevalue of 70 reported by Haight1 Chest x-rays were oftenabnormal in patients with inhalational anthrax32344059
and occasionally in patients with gastrointestinal51 or cuta-neous disease3554 Chest x-ray findings included pleuraleffusion3234405159 hilar adenopathy3240 widened mediasti-num59 infiltrates35 and soft tissue edema54
EEG results have rarely been reported even thoughseizures are fairly common In part this reflects the mori-bund state of most of these patients In one patient withreported myoclonus and fasciculations EEG showed disor-ganized low-amplitude slow waves (1 to 7 Hz)39
CT or MRI of the head in patients with anthrax menin-goencephalitis may demonstrate focal intracerebral hemor-rhage subarachnoid hemorrhage intraventricularhemorrhage diffuse cerebral edema and prominent lepto-meningeal enhancement5458 Parenchymal cerebral en-hancement has not been reported58 but its absence maysimply reflect the paucity of neuroimaging studies in thesepatients Abnormalities may progress rapidly on serialbrain imaging studies54
Differential diagnosis Hemorrhagic meningitis shouldraise suspicion of anthrax infection36 particularly if gram-positive rods are demonstrated on Gramrsquos stain Listeriamonocytogenes the only common gram-positive rod caus-ing meningitis does not produce a hemorrhagic meningitisand is rarely seen on Gramrsquos stain Based on initial clinicaldiagnoses in reported cases the differential diagnosis ofanthrax meningoencephalitis may include subarachnoidand intracerebral hemorrhage ischemic stroke nonan-thrax bacterial meningoencephalitis herpes simplex virusencephalitis and other viral encephalitides eclampsia andcerebral malaria
Treatment Antianthrax treatment was reported in 39patients1228-3840424345-5255-59 Of these 19 (49) receivedpenicillin only28-32353842454849525658 (administered parenter-ally in all but one case)2930 19 (49) received penicillin (orin one case ampicillin)55 in combination with other antibi-otic therapy12293032-343637404345-475051555759 and one (3) re-ceived antianthrax serum only33 Antibiotics used inconjunction with penicillin therapy included chloramphen-icol (11 cases)33364345-475057 streptomycin (7 cas-es)1229303233374051 sulfonamides (4 cases)122930364557
cefotaxime (2 cases)5559 tetracyclines (1 case)33 vancomy-cin (1 case)59 and antianthrax serum (1 case)33 Corticoste-roids were administered in conjunction with antibiotics inten cases (26)3336424345485257 In the Sverdlovsk inhala-tional anthrax outbreak in 1979 hospitalized patientswere treated variously with penicillin cephalosporinchloramphenicol antianthrax globulin and corticoste-roids62 but case-specific treatments and outcomes were notreported in the English language literature either in gen-eral or for the 21 patients autopsied after dying with an-thrax meningoencephalitis446263
Prognosis Septicemia toxic shock and death rapidlyfollow development of anthrax meningoencephalitis inmost cases Many patients presented in extremis followinga prodromal period of 1 to 6 days and 75 died within 24hours of presentation (ie 4155 of cases for whom such
information was available)28-3538394144-4749-5269 Four pa-tients (6) in the present series survived36374851 comparedwith three (4) in the previous world literature a differ-ence that was not significant (p 071) (table 4) Exclud-ing the 21 cases of inhalational anthrax from theSverdlovsk autopsy series44 estimated survival in the cur-rent series is four of 49 (8) and in all reported cases todate is seven of 122 (6) the difference in survival be-tween this restricted group of deceased patients and thesurviving patients was also not significant (p 044) Re-ported additional cases of survival had no clinical informa-tion (two cases)7 or were not established microbiologicallyor pathologically as cases of anthrax (one case)11 An addi-tional recent series of 12 cases with no survivals did notreport case-specific information9
Survival appears to be most likely if meningoencephali-tis develops as part of the course of cutaneous an-thrax363748 but a single case with survival has beenreported with gastrointestinal anthrax51 In the currentseries 15 of cutaneous cases survived compared with 8among gastrointestinal cases none among inhalationalcases and none among unknown or unspecified cases (seetable 3) The difference in survival of the cutaneous casesin the current series (15) and Haightrsquos series (5) wasnot significant (p 032) To date in the world literaturethere are no reported cases of survival following anthraxmeningoencephalitis associated with inhalational anthrax
The seven surviving patients reported to date are sum-marized in table 513-15273637485170 Surviving patients wereyounger as a group than those in the present series whodied (median age of surviving cases 24 years n7 me-dian age of cases who died 45 years n 66 p 004) Ifthe comparison is restricted to cases in the current seriesonly the difference in age is greater (median age of surviv-ing cases 1025 years n 4 p 0003) In generalinitial CSF results from the surviving patients were eithernormal or were less severely abnormal compared to de-ceased patients However because of the small samplesizes for different CSF studies in the survival group noneof the individual contrasts was significant (glucose p 041 protein p 012 red cells p 024 white cellsp 008)
Many reports and reviews failed to identify all of thepreviously reported cases with survival or misreported as-pects of the cases they did review resulting in incorrectconclusions about the agents that are potentially effective
Table 4 Survival with anthrax meningoencephalitis inreported cases
Primary focus Haight 1952 Lanska 2002 Total
Cutaneous 239 (5) 320 (15) 559 (8)
Gastrointestinal 07 (0) 112 (8) 119 (5)
Inhalational 017 (0) 027 (0) 044 (0)
Maternal sepsis 01 (0) 01 (0)
None identified 19 (11) 011 (0) 120 (5)
Total 373 (4) 470 (6) 7143 (5)
Values are expressed as n ()
Excluding the 21 inhalational cases from the Sverdlovsk autopsyseries estimated survival in the current series is 449 (8) andin reported cases to date is 7122 (6)
330 NEUROLOGY 59 August (1 of 2) 2002
treatments The treatments administered to surviving pa-tients were in fact similar to those chosen in the entiregroup of patients in the current series All of the patientsreceived penicillin except the first case (Patient 1) whoreportedly received no treatment (Bernd Remler MD per-sonal communication February 2002)70 Only two of thepatients received corticosteroids in addition to antibiotics(Patients 4 and 6)3648 The only case with gastrointestinalanthrax (Patient 7) received the same treatment as hissister (aged 2 years) who died51 Treatment of survivingpatients was generally begun before the disease was clini-cally advanced Three of the patients who survived (Pa-tients 2 through 4) were receiving treatment for cutaneousanthrax (that included penicillin) before development ofsymptoms of meningoencephalitis13-152736 There is limitedinformation on long-term outcomes among the survivorsbut most were reported to have fully recovered13-1527363751
although two patients had residual focal weakness4870
Autopsy findings Autopsies were obtained in 40 of the66 deceased patients (61)28-32343538-4043-454755-5759 Thissummary is restricted to pathologic findings in the centralnervous system Gross findings typically included cloudyand congested leptomeninges with occasional obvious pu-rulent exudate13034354447 and with variable degrees of sub-arachnoid hemorrhage128293135394044455557 In many casessubarachnoid hemorrhage was the dominant gross patho-logic feature1282931353940444555 The vascular congestionand extensive subarachnoid hemorrhage of the leptome-ninges gave a dark red appearance on gross examination ofthe brain a finding sometimes referred to as a ldquocardinalrsquoscaprdquo2 Other common findings included intraventricularhemorrhage2939 intracerebral hematoma13956 multifocalsmall intraparenchymal cortical hemorrhages394047 or nu-merous petechial hemorrhages in cerebral parenchyma2864
zones of infarction in arterial venous or watershed distri-butions3964 and cerebral edema35454757 with tonsillar35 oruncal herniation47
Microscopic findings included hemorrhagic leptomen-ingitis2930343538-404447555764 and associated necrotizing vas-
culitis164 multifocal subarachnoid128-313538-404445555764 andintracerebral hemorrhage128-3038394756 multifocal cerebralinfarction3964 and leptomeningeal and cerebral ede-ma35394445475764 The hemorrhagic leptomeningitis was as-sociated with polymorphonuclear leukocytic inflammatoryexudates3538444755-5764 severe congestion of meningealblood vessels3538404756 hemorrhagic infiltration3544455664 orfrank subarachnoid hemorrhage128-313538-404445555764 aggre-gations of neutrophils and mononuclear phagocytes in andaround meningeal vessels3538404764 and tracking of bloodand inflammatory infiltrates along the VirchowndashRobin(perivascular) spaces into the parenchyma47 The superfi-cial cerebral cortex showed diffuse perineuronal andperivascular infiltration by neutrophils353947 severe vascu-lar congestion3540 necrosis of blood vessel walls3539475664
recent thromboses353964 zones of ischemia3964 areas ofhemorrhage47 and edema35394445475764 Numerous largegram-positive rods in short chains were present in theleptomeninges and the subarachnoid and VirchowndashRobinspaces29-31344756 within and around meningeal and superfi-cial cortical vessels and vessels in regions of hemor-rhage313235394064 and within hemorrhagic lesions313247
Discussion Meningoencephalitis develops in atmost 5 of cases of cutaneous anthrax1428 howevermost cases of anthrax meningoencephalitis to datehave developed from cutaneous anthrax because thevast majority of naturally acquired cases of anthraxare cutaneous28 Meningoencephalitis may occur inup to half of the cases in industrial or bioweaponsoutbreaks of inhalational anthrax829303244 howeverin the recent bioterrorist outbreak of anthrax in theUnited States only the index case had meningitisamong the 11 cases of confirmed or suspected inhala-tional anthrax identified5971-73 The relatively low fre-quency of meningitis among anthrax cases in the USbioterrorism outbreak may be misleading though aslumbar punctures were done in few cases and the
Table 5 Patients with anthrax meningoencephalitis who survived
Variable
Patient no
1 2 3 4 5 6 7
Reference no 70 14 27 36 37 48 51
Year 1916 1947 1948 1972 1973 1989 1993
Age y 24 57 51 85 12 25 6
Sex F M M F M M M
Clinical type Unknown Cutaneous Cutaneous Cutaneous Cutaneous Cutaneous Gastrointestinal
Treatment None
Antianthrax serum X
Penicillin X X X X X X
Chloramphenicol I
Streptomycin X X
Sulfonamide X I
Corticosteroid X X
Residual L hemiparesis None None None None RUE weakness None
X main therapy I initial therapy only RUE right upper extremity
August (1 of 2) 2002 NEUROLOGY 59 331
brain was not examined in some autopsies Based onprevious experience44 the potential exists for largenumbers of cases of anthrax meningoencephalitiswith further bioterrorist outbreaks or bioweaponsdispersals Meningoencephalitis may also occur withgastrointestinal anthrax or without a clinically ap-parent primary focus
Current guidelines from the Centers for DiseaseControl indicate that ciprofloxacin or doxycyclineshould be included as essential components of initialtherapy for anthrax infections of any portal of en-try7274 It is important to treat anthrax meningoen-cephalitis with a polydrug antibiotic regimen usingantimicrobial agents that have good CSF penetrationin meningitis and that provide good antibacterialcoverage for B anthracis All six patients who sur-vived after antibiotic treatment for anthrax menin-goencephalitis were treated with penicillinHowever because of the presence of constitutive orinducible beta-lactamases in B anthracis isolatesfrom the recent US bioterrorist outbreak and expec-tations that beta-lactamase activity may be likelywith bioengineered bioweapons agents ampicillin orpenicillin G alone are not recommended for initialtherapy for anthrax meningoencephalitis prior to an-tibiotic sensitivity results from culture7274 Rifampinplus vancomycin would be a reasonable choice foraddition to ciprofloxacin or doxycycline in the initialtreatment of anthrax meningoencephalitis Some in-fectious disease authorities recommend ciprofloxacinin preference to doxycycline plus augmentation withchloramphenicol rifampin or penicillin for estab-lished or suspected anthrax meningoencephalitis6
Aztreonam trimethoprim-sulfamethoxazole orthird-generation cephalosporins should not be usedbecause of natural resistance of B anthracis strainsto these antibiotics
Bacterial toxins have long been felt to play a ma-jor role in anthrax meningoencephalitis becausemany effects of B anthracis cannot be attributed tomicroscopically evident tissue changes1075 Virulenceof B anthracis requires an antiphagocytic capsuleand two exotoxins The two toxins are binary pro-teins composed of a binding protein and an enzymat-ically active protein2476 Among other actions thesetoxins collectively produce local edema impair neu-trophil function depress cerebral cortical electricalactivity depress central respiratory center activitycause bleeding and destruction of the brain and vitalorgans in the chest and induce cardiovascular col-lapse and shock244476-79
Although antitoxin was used early in the 20thcentury to treat anthrax alone or in combinationwith penicillin13-15 it has not been available in recentdecades to US civilian populations Conceptually an-tianthrax serum may augment the effect of antibiot-ics by helping to neutralize the anthrax toxinswhich are not inactivated by antibiotics Howeverthere are no documented cases of successful treat-ment of anthrax meningitis with antianthrax serumalone Haight incorrectly stated that a case reported
by Czyhlarz in 191670 had been cured by treatmentwith antianthrax serum when in fact a full transla-tion indicates that the patient received no treatment(Bernd Remler MD personal communication Feb-ruary 2002 see supplementary document) this er-ror has been promulgated by numerous subsequentauthors and has been a source of incorrect conclu-sions regarding potentially effective therapy for an-thrax meningoencephalitis in recent reviewsCzyhlarz70 also presented unpublished second-handinformation on another patient who purportedly re-covered from anthrax meningoencephalitis withouttreatment In light of subsequent experience withthis disease it is hard to interpret or credit either ofthese reports Available experimental data80 do notindicate a significant treatment effect of antianthraxserum beyond that of penicillin Nevertheless anti-anthrax immune globulin derived from the blood ofsoldiers who have received the anthrax vaccine isbeing added to the US bioterrorism treatment stock-pile and is being considered as a potential experi-mental anthrax treatment in the event of furtherbioterrorism anthrax cases681
Corticosteroids have been recommended as an ad-junctive agent in the treatment of meningitis in chil-dren82 Use of corticosteroids in adults withmeningitis is controversial but steroids have beenrecommended for consideration as adjunctive agentswithout any age restriction in anthrax meningitis72
If corticosteroids are used in conjunction with vanco-mycin therapy antibiotic dosing may need to bemodified because CSF vancomycin levels may be de-creased by corticosteroids contributing to treatmentfailure82-86
In addition to antibiotic management patientswith anthrax meningoencephalitis may require ag-gressive intensive care measures Seizures in-creased intracranial pressure subarachnoid andintracerebral hemorrhage electrolyte disturbanceshypotension shock and disseminated intravascularcoagulation may develop as complications of this in-fection Despite aggressive treatment the prognosisfor survival with anthrax meningoencephalitis isvery poor
AcknowledgmentThe author thanks Glen Salter MS of the Tomah VA MedicalCenter Library for assistance in locating references Pat Mennickeof the Tomah VA Medical Center for assistance with Excel spread-sheets Bernd Remler MD of the Medical College of WisconsinMilwaukee for translating the paper by Czyhlarz Larry DavisMD of the Albuquerque VA Medical Center for helpful correspon-dence regarding corticosteroids and vancomycin Jeffrey M JonesMD PhD of the William S Middleton VA Medical Center Madi-son for helpful discussions regarding antibiotic treatment of an-thrax meningoencephalitis and Mary Jo Lanska MD MS of theTomah VA Medical Center for helpful discussions and for criti-cally reviewing the manuscript
References1 Haight TH Anthrax meningitis review of literature and report
of two cases with autopsies Am J Med Sci 195222457ndash692 Dixon TC Meselson M Guillemin J Hanna PC Anthrax
N Engl J Med 1999341815ndash826
332 NEUROLOGY 59 August (1 of 2) 2002
3 Inglesby TV Henderson DA Bartlett JG et al Anthrax as abiological weapon medical and public health managementJAMA 19992811735ndash1745
4 Swartz MN Recognition and management of anthrax an up-date N Engl J Med 20013451621ndash1626
5 Jernigan JA Stephens DS Ashford DA et al Bioterrorism-related inhalational anthrax the first 10 cases reported in theUnited States Emerg Infect Dis 20017933ndash944
6 Inglesby TV OrsquoToole T Henderson DA et al Anthrax as abiological weapon 2002 updated recommendations for man-agement JAMA 20022872236ndash2252
7 Miller JK Human anthrax in New York State NY StateJ Med 1961612046ndash2053
8 Brachman PS Human anthrax in the United States Antimi-crob Agents Chemother 19655111ndash114
9 Kumar A Kanungo R Bhattacharya S Badrinath S DuttaTK Swaminathan RP Human anthrax in India urgent needfor effective prevention J Commun Dis 200032240ndash246
10 Dutz W Kohout E Anthrax Pathol Annu 197162009ndash224811 Trivedy JR Case of anthrax meningitis survival Cent Afr
J Med 19812716612 Roberts CJ Chambers PG An outbreak of anthrax in the
Mondoro Tribal Trust lands Cent Afr J Med 19752173ndash7613 Kindler D Recovery from anthrax meningitis Ind Med Surg
195221487ndash48814 Shanahan RH Griffin JR Von Auersperg AP Anthrax men-
ingitis report of a case of internal anthrax with recoveryAm J Clin Pathol 194717719ndash722
15 Griffin JR Shanahan RH DeAngelis CE Treatment of cuta-neous anthrax with penicillin NY State J Med 1948481718ndash1721
16 Boudin G Lauras A Vaillant C Etat de mal eacutepileptiquereacuteveacutelateur drsquoune meacuteningite charbonneuse etude anatamo-clinique Bull Mem Soc Med Hop Paris 1964115183ndash187
17 Rapun Pac JL Ull Laita M Meningitis carbuncosa Arch Neu-robiol (Madr) 197235143ndash148
18 Baltiev A Besleaga E Cuciureanu G Obreja E Meningo-encefalita carbunoasa la un copil cu pustula cutanata necarac-teristica Rev Med Chir Soc Med Nat Iasi 197377885ndash888
19 Beer K Milzbrandmeningitis Path Microbiol 19733912ndash1320 Bach I Simon L Baacuten E Toacuteth L Kovaacutecs M Haemorrhagiaacutes
meningitises apoplexia anthrax sepsisben Orv Hetil 19781191797ndash1799
21 Marandian MH Kamali A Meacuteningite charbonneuse un casen apparence primitif Nouv Presse Med 1981101747ndash1748
22 Duumlrst UN Bartenstein J Buumlhlmann H Wuumlst J Spiegel MVAnthraxmeningitis Schweiz Med Wochenschr 19861161222ndash1228
23 Gonzalez A Rodriguez E Castillo M Ortega I Ramirez EFajardo J Lesioacuten necroacutetica en mentoacuten en paciente con siacuten-drome meniacutengeo Enferm Infecc Mircobiol Clin 199715163ndash164
24 Abramova AA Grinberg LM [Pathology of anthrax sepsisaccording to materials of the infectious outbreak in 1979 inSverdlovsk (macroscopic changes)] Arkh Patol 19935512ndash17
25 Abramova AA Grinberg LM [Pathology of anthrax sepsisaccording to materials of infectious outbreak in 1979 in Sverd-lovsk (microscopic changes)] Arkh Patol 19935518ndash23
26 Grinberg LM Abramova AA [Pathology of anthrax sepsisaccording to materials of the infectious outbreak in 1979 inSverdlovsk (various aspects of morpho- patho- and thanato-genesis] Arkh Patol 19935523ndash26
27 Weinstein L Oliver CS The treatment of human anthraxwith penicillin Am Pract 19482533ndash538
28 Raper AB Anthrax meningo-encephalitis East Afr Med J195330399-401
29 Albrink WS Brooks SM Biron RE Kopel M Human inhala-tional anthrax a report of three fatal cases Am J Pathol196036457ndash468
30 Plotkin SA Brachman PS Utell M Bumford FH AtchisonMM An epidemic of inhalation anthrax the first in the twen-tieth century I Clinical features Am J Med 196029992ndash1001
31 Brachman PS Pagano JS Albrink WS Two cases of fatalinhalation anthrax one associated with sarcoidosis N EnglJ Med 1961265203ndash208
32 Brachman PS Inhalation anthrax Ann NY Acad Sci 198035383ndash93
33 Vita A Secu A Cuciureanu G Leibovici M Bejanariu C CujuG Considerations on 3 cases of meningo-encephalitis due toanthrax bacilli Rom Med Rev 1961536ndash39
34 LaForce FM Bumford FH Freely JC Stokes SL Snow DBEpidemiologic study of a fatal case of inhalation anthrax ArchEnviron Health 196918798ndash805
35 Rangel RA Gonzaacutelez DA Bacillus anthracis meningitis Neu-rology 197525525ndash530
36 Tahernia AC Hashemi G Survival in anthrax meningitisPediatrics 197250329ndash333
37 Tengio FU Anthrax meningitis report of two cases East AfrMed J 197350337ndash339
38 Viratchai C Anthrax gastro-enteritis and meningitis J MedAssoc Thai 197457147ndash150
39 Pluot M Vital C Aubertin J Croix JC Pire JC Poisot DAnthrax meningitis report of two cases with autopsies ActaNeuropathol (Berl) 197636339ndash345
40 Suffin SC Carnes WH Kaufman AF Inhalation anthrax in ahome craftsman Hum Pathol 19789594ndash597
41 Al-Dulaimy SB Al-Allaf GA Anthrax meningitis Trans R SocTrop Med Hyg 197872315
42 Manios S Kavaliotis I Anthrax in children a long forgottenpotentially fatal condition Scand J Infect Dis 197911203ndash206
43 Koshi G Lalitha MK Daniel J Chacko A Pulimood BMAnthrax meningitis a rare clinical entity J Assoc PhysiciansIndia 19812959ndash62
44 Abramova FA Grinberg LM Tampolskaya OV Walker DHPathology of inhalational anthrax in 42 cases from the Sverd-lovsk outbreak of 1979 Proc Natl Acad Sci USA 1993902291ndash2294
45 Levy L Baker N Meyer MP Crosland P Hampton J Anthraxmeningitis in Zimbabwe Cent Afr J Med 198127101ndash104
46 Bhat P Pereira P Mohan N Primary anthrax meningitis acase report Neurol India 19833171ndash73
47 Chandramukhi A Shankar P Rao TV Sundararajan SSwamy HS Acute leptomeningitis due to Bacillus anthracis acase report Trop Geogr Med 19833579ndash82
48 Khanna N Gokul BN Ravikumar R et al Successfullytreated primary anthrax meningitis Indian J Pathol Micro-biol 198932315ndash317
49 Kanungo R Sujatha S Das AK Rao RS Anthrax meningitisa clinical enigma Indian J Med Microbiol 19906149ndash151
50 Bharathmoorthy Chakravarthy I Swaminathan RP et alHaemorrhagic meningitis due to Bacillus anthrax J AssocPhysicians India 199240134ndash135
51 Tabatabaie P Syadati A Bacillus anthracis as a cause ofbacterial meningitis Pediatr Infect Dis 1993121035ndash1037
52 George S Mathai D Balraj V Lalitha MK John TJ An out-break of anthrax meningoencephalitis Trans R Soc Trop MedHyg 199488206ndash207
53 Berthier M Fauchegravere J-L Perrin J Grignon B Oriot D Ful-minant meningitis due to Bacillus anthracis in 11-year-oldgirl during Ramadan Lancet 1996347828
54 Domiacutenguez E Bustos C Garcia M Recio S Anthrax meningo-encephalitis radiologic findings AJR Am J Roentgenol 1997169317
55 Kwong KL Que TL Wong SN So KT Fatal meningoenceph-alitis due to Bacillus anthracis J Paediatr Child Health 199733539ndash541
56 Garcia AG Jiminez RR Bacillus anthracis meningitis N EnglJ Med 1999341814
57 Ringertz SH Hoiby EA Jensenius M et al Injectional an-thrax in a heroin skin-popper Lancet 20003461574ndash1575
58 Kim HJ Jun WB Lee SH Rho MH CT and MR findings ofanthrax meningoencephalitis report of two cases and reviewof the literature AJNR Am J Neuroradiol 2001221303ndash1305
59 Bush LM Abrams BH Heall A Johnson CC Index case offatal inhalational anthrax due to bioterrorism in the UnitedStates N Engl J Med 20013451607ndash1610
60 Brachman PS Plotkin SA Bumford FH Atchison MM Anepidemic of inhalation anthrax the first in the twentieth cen-tury II Epidemiology Am J Hygiene 1960726ndash23
61 Belluck P Anthrax outbreak of rsquo57 felled a mill but yieldedanswers New York Times October 27 2001B8
62 Meselson M Guillemin J Hugh-Jones M et al The Sverd-lovsk anthrax outbreak of 1979 Science 19942661202ndash1208
August (1 of 2) 2002 NEUROLOGY 59 333
63 Jackson PJ Hugh-Jones ME Adair DM et al PCR analysis oftissue samples from the 1979 Sverdlovsk anthrax victims thepresence of multiple Bacillus anthracis strains in differentvictims Proc Natl Acad Sci USA 1998951224ndash1229
64 Grinberg LM Abramova FA Yampolskaya OV Walker DHSmith JH Quantitative pathology of inhalational anthrax IQuantitative microscopic findings Mod Pathol 200114482ndash495
65 Brookmeyer R Blades N Hugh-Jones M Henderson D Thestatistical analysis of truncated data application to the Sverd-lovsk anthrax outbreak Biostatistics 20012233ndash247
66 Knott FA A note on anthrax infection by shaving brushesLancet 19231227ndash228
67 Bradaric N Punda-Polic V Cutaneous anthrax due topenicillin-resistant Bacillus anthracis transmitted by an in-sect bite Lancet 1992340306ndash307
68 Turell MJ Knudson GB Mechanical transmission of Bacillusanthracis by stable flies (Stomoxys calcitrans) and mosquitoes(Aedes aegypti and Aedes taeniorhynchus) Infect Immun1987551859ndash1861
69 Drake DJ Meningitic anthrax Cent Afr J Med 19711797ndash9870 Czyhlarz EV Beitrag zur Lehre von der Milzbrandmeningitis
Wein Klin Wochenscr 191629768ndash76971 Centers for Disease Control Investigation of anthrax associ-
ated with intentional exposure and interim public healthguidelines October 2001 MMWR Morb Mortal Wkly Rep200150889ndash893
72 Centers for Disease Control Update investigation ofbioterrorism-related anthrax and interim guidelines for expo-sure management and antimicrobial therapy October 2001MMWR Morb Mortal Wkly Rep 200150909ndash919
73 Centers for Disease Control Investigation of bioterrorism-related anthrax and interim guidelines for clinical evaluationof persons with possible anthrax MMWR Morb Mortal WklyRep 200150941ndash948
74 Centers for Disease Control Updated recommendations forantimicrobial prophylaxis among asymptomatic pregnantwomen after exposure to Bacillus anthracis MMWR MorbMortal Wkly Rep 200150960
75 Bonventure PF Sueoka W True CW Klein F Lincoln RAttempts to implicate the central nervous system as a pri-
mary site of action for Bacillus anthracis lethal toxin FedProc 1967261549ndash1553
76 Friedlander AM Anthrax In Sidell FR Takafuji ET FranzDR eds Textbook of military medicine medical aspects ofchemical and biological warfare Washington DC Office ofthe Surgeon General 1997467ndash478
77 Vick JA Lincoln RE Klein F Mahlandt BG Walker JS FishDC Neurological and physiological responses of the primateto anthrax toxin J Infect Dis 196811885ndash96
78 Klein F Lincoln RE Dobbs JP Mahlandt BG Remmele NSWalker JS Neurological and physiological responses of theprimate to anthrax infection J Infect Dis 196811897ndash103
79 Remmele NS Klein F Vick JA Walker JS Mahlandt BGLincoln RE Anthrax toxin primary site of action J Infect Dis1968118104ndash113
80 Doganay M Hanagasi R Zora A [Evaluation of penicillinalone and penicillin combined with anti-anthrax serum in ex-perimental anthrax in mice] Mikrobiyol Bul 19851957ndash64
81 Associated Press Government may offer anthrax treatmentNew York Times January 7 2002
82 Davis LE Acute bacterial meningitis In Johnson RT GriffinJW eds Current therapy in neurologic disease 5th ed StLouis Mosby 1997120ndash127
83 Viladrich PF Gudiol F Lintildeares J et al Evaluation of vanco-mycin for therapy of adult pneumococcal meningitis Antimi-crob Agents Chemother 1991352467ndash2472
84 Pariacutes M Hickey SM Uscher MI Shelton S Olsen KD Mc-Cracken GH Jr Effect of dexamethasone on therapy of exper-imental penicillin- and cephalosporin-resistant pneumococcalmeningitis Antimicrob Agents Chemother 1994381320ndash1324
85 Cabellos C Martinez-Lacasa J Martos A et al Influence ofdexamethasone on efficacy of ceftriaxone and vancomycintherapy in experimental pneumococcal meningitis AntimicrobAgents Chemother 1995392158ndash2160
86 Ahmed A Jafri H Lutsar I et al Pharmacodynamics of van-comycin for the treatment of experimental penicillin- andcephalosporin-resistant pneumococcal meningitis AntimicrobAgents Chemother 199943876ndash881
334 NEUROLOGY 59 August (1 of 2) 2002
DOI 101212WNL593327200259327-334 Neurology
Douglas J LanskaAnthrax meningoencephalitis
This information is current as of August 13 2002
ServicesUpdated Information amp
httpwwwneurologyorgcontent593327fullhtmlincluding high resolution figures can be found at
Supplementary Material
htmlhttpwwwneurologyorgneurologysuppl20020716593327DC2
htmlhttpwwwneurologyorgneurologysuppl20020716593327DC1Supplementary material can be found at
References httpwwwneurologyorgcontent593327fullhtmlref-list-1
This article cites 73 articles 15 of which you can access for free at
Citations httpwwwneurologyorgcontent593327fullhtmlotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpwwwneurologyorgcgicollectionmeningitisMeningitis
httpwwwneurologyorgcgicollectionencephalitisEncephalitis
httpwwwneurologyorgcgicollectionbacterial_infectionsBacterial infections
httpwwwneurologyorgcgicollectionall_infectionsAll Infectionsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsin its entirety can be found online atInformation about reproducing this article in parts (figurestables) or
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

tions generalized rigidity lateralizing long-tract signsand decerebrate posturing
CSF Results of analyses of CSF were reported insome detail for 43 patients (table 3) eight of whom hadserial lumbar punctures113143335364048 with up to six lum-bar punctures in a single patient1314 Serial lumbar punc-tures were performed to monitor response to therapy andin some cases to administer intrathecal penicillin113142733
In some cases initial suspicion of anthrax meningoenceph-alitis was the result of CSF abnormalities In the indexcase in the 2001 US bioterrorist outbreak a diagnosis ofanthrax was considered on the basis of CSF Gramrsquos stainand ultimately confirmed by CSF culture59
CSF studies typically showed findings of hemorrhagicmeningitis (see table 3) CSF in anthrax meningoencepha-litis may appear cloudy with yellowish or pinkish colora-tion or may be grossly bloody evolution across thisspectrum has been reported in serial lumbar punctures inan individual patient1 The supernatant was frequentlyxanthochromic Opening pressure was frequently elevatedwith a range of 130 to 700 mm H2O45 Hypoglycorrhachiawas common with CSF glucose in the range of 20 to 40
mgdL but occasionally less than 20 mgdL CSF proteinconcentration was generally elevated with a range of 10 to2800 mgdL CSF was frequently hemorrhagic but early inthe illness there may be no red blood cells13273545 Therewas generally a CSF pleocytosis with from 0 to 10000white cellsmm3 with a predominance of polymorphonu-clear leukocytes There were many large gram-positiverods on Gramrsquos stain either singly or in short or longchains CSF cultures from the initial lumbar puncturewere always positive when tested although some caseswere confirmed instead by culture of swabs or fluid fromskin lesions other body fluids or postmortem tissuesamples28-3032344445 CSF may be sterile after several daysof antibiotics136 Serial lumbar punctures may documentan evolution from cloudy to grossly bloody CSF with in-creasing protein concentration increasing numbers of redcells and polymorphonuclear leukocytes and increasingpredominance of polymorphonuclear leukocytes11314 Simi-lar collective findings were reported in a recent series of 12cases that did not provide case-specific results9
Other diagnostic studies Patients with anthrax me-ningoencephalitis generally have elevated white blood cell
Table 3 CSF analyses in anthrax meningoencephalitis
Variablevalue n () Variablevalue n ()
Appearance White cells per mm3
Cloudy 15 (35) 100 4 (9)
Bloody 12 (28) 100ndash999 3 (7)
Mixed 6 (14) 1000ndash9999 15 (35)
Clear 3 (7) 10000 3 (7)
Unknown 7 (16) Unknown 18 (42)
Glucose mddL Neutrophils
20 3 (7) 50 0 (0)
20ndash40 13 (30) 50ndash79 3 (7)
40 13 (30) 80 10 (23)
Unknown 14 (33) Unknown 30 (70)
Protein mgdL Gram-stain positive
45 2 (5) Yes 33 (77)
46ndash199 4 (9) No 3 (7)
200ndash999 18 (42) Unknown 7 (16)
1000 8 (19) CSF culture positive
Unknown 11 (26) Yes 35 (81)
Red cells per mm3 No 0 (0)
100 4 (9) Unknown 8 (19)
100ndash999 5 (12)
1000ndash9999 5 (12)
10000 2 (5)
Bloody count not reported 12 (28)
Unknown 15 (35)
These results are from the initial spinal taps for 43 cases with reported CSF results Haight1 did not summarize CSF results for hisseries although he reported fairly detailed results from serial lumbar punctures in the two cases he reported For the purpose of sum-marizing CSF results in anthrax meningitis Haightrsquos two cases from 19521 and two cases with survival from the late 1940s131427 wereincluded For CSF glucose two patients with normal values were coded as 40 mgdL and one patient with a low CSFblood ratio ofglucose concentration (017) was coded as 20ndash40 mgdL Three patients had negative CSF Gram stains and CSF cultures were notdone diagnostic confirmation in these cases was based on antemortem or postmortem cultures of other tissues histology or in onecase immunohistochemistry Because of rounding percentages for each variable may not sum to 100
August (1 of 2) 2002 NEUROLOGY 59 329
counts with a left shift The range of white cell counts inthe current series was from 5400 to 27700 somewhatlower than the range of 10000 to 80000 reported byHaight1 Blood cultures were positive in 71 (ie 1521) ofcases for whom these were reported nearly identical to thevalue of 70 reported by Haight1 Chest x-rays were oftenabnormal in patients with inhalational anthrax32344059
and occasionally in patients with gastrointestinal51 or cuta-neous disease3554 Chest x-ray findings included pleuraleffusion3234405159 hilar adenopathy3240 widened mediasti-num59 infiltrates35 and soft tissue edema54
EEG results have rarely been reported even thoughseizures are fairly common In part this reflects the mori-bund state of most of these patients In one patient withreported myoclonus and fasciculations EEG showed disor-ganized low-amplitude slow waves (1 to 7 Hz)39
CT or MRI of the head in patients with anthrax menin-goencephalitis may demonstrate focal intracerebral hemor-rhage subarachnoid hemorrhage intraventricularhemorrhage diffuse cerebral edema and prominent lepto-meningeal enhancement5458 Parenchymal cerebral en-hancement has not been reported58 but its absence maysimply reflect the paucity of neuroimaging studies in thesepatients Abnormalities may progress rapidly on serialbrain imaging studies54
Differential diagnosis Hemorrhagic meningitis shouldraise suspicion of anthrax infection36 particularly if gram-positive rods are demonstrated on Gramrsquos stain Listeriamonocytogenes the only common gram-positive rod caus-ing meningitis does not produce a hemorrhagic meningitisand is rarely seen on Gramrsquos stain Based on initial clinicaldiagnoses in reported cases the differential diagnosis ofanthrax meningoencephalitis may include subarachnoidand intracerebral hemorrhage ischemic stroke nonan-thrax bacterial meningoencephalitis herpes simplex virusencephalitis and other viral encephalitides eclampsia andcerebral malaria
Treatment Antianthrax treatment was reported in 39patients1228-3840424345-5255-59 Of these 19 (49) receivedpenicillin only28-32353842454849525658 (administered parenter-ally in all but one case)2930 19 (49) received penicillin (orin one case ampicillin)55 in combination with other antibi-otic therapy12293032-343637404345-475051555759 and one (3) re-ceived antianthrax serum only33 Antibiotics used inconjunction with penicillin therapy included chloramphen-icol (11 cases)33364345-475057 streptomycin (7 cas-es)1229303233374051 sulfonamides (4 cases)122930364557
cefotaxime (2 cases)5559 tetracyclines (1 case)33 vancomy-cin (1 case)59 and antianthrax serum (1 case)33 Corticoste-roids were administered in conjunction with antibiotics inten cases (26)3336424345485257 In the Sverdlovsk inhala-tional anthrax outbreak in 1979 hospitalized patientswere treated variously with penicillin cephalosporinchloramphenicol antianthrax globulin and corticoste-roids62 but case-specific treatments and outcomes were notreported in the English language literature either in gen-eral or for the 21 patients autopsied after dying with an-thrax meningoencephalitis446263
Prognosis Septicemia toxic shock and death rapidlyfollow development of anthrax meningoencephalitis inmost cases Many patients presented in extremis followinga prodromal period of 1 to 6 days and 75 died within 24hours of presentation (ie 4155 of cases for whom such
information was available)28-3538394144-4749-5269 Four pa-tients (6) in the present series survived36374851 comparedwith three (4) in the previous world literature a differ-ence that was not significant (p 071) (table 4) Exclud-ing the 21 cases of inhalational anthrax from theSverdlovsk autopsy series44 estimated survival in the cur-rent series is four of 49 (8) and in all reported cases todate is seven of 122 (6) the difference in survival be-tween this restricted group of deceased patients and thesurviving patients was also not significant (p 044) Re-ported additional cases of survival had no clinical informa-tion (two cases)7 or were not established microbiologicallyor pathologically as cases of anthrax (one case)11 An addi-tional recent series of 12 cases with no survivals did notreport case-specific information9
Survival appears to be most likely if meningoencephali-tis develops as part of the course of cutaneous an-thrax363748 but a single case with survival has beenreported with gastrointestinal anthrax51 In the currentseries 15 of cutaneous cases survived compared with 8among gastrointestinal cases none among inhalationalcases and none among unknown or unspecified cases (seetable 3) The difference in survival of the cutaneous casesin the current series (15) and Haightrsquos series (5) wasnot significant (p 032) To date in the world literaturethere are no reported cases of survival following anthraxmeningoencephalitis associated with inhalational anthrax
The seven surviving patients reported to date are sum-marized in table 513-15273637485170 Surviving patients wereyounger as a group than those in the present series whodied (median age of surviving cases 24 years n7 me-dian age of cases who died 45 years n 66 p 004) Ifthe comparison is restricted to cases in the current seriesonly the difference in age is greater (median age of surviv-ing cases 1025 years n 4 p 0003) In generalinitial CSF results from the surviving patients were eithernormal or were less severely abnormal compared to de-ceased patients However because of the small samplesizes for different CSF studies in the survival group noneof the individual contrasts was significant (glucose p 041 protein p 012 red cells p 024 white cellsp 008)
Many reports and reviews failed to identify all of thepreviously reported cases with survival or misreported as-pects of the cases they did review resulting in incorrectconclusions about the agents that are potentially effective
Table 4 Survival with anthrax meningoencephalitis inreported cases
Primary focus Haight 1952 Lanska 2002 Total
Cutaneous 239 (5) 320 (15) 559 (8)
Gastrointestinal 07 (0) 112 (8) 119 (5)
Inhalational 017 (0) 027 (0) 044 (0)
Maternal sepsis 01 (0) 01 (0)
None identified 19 (11) 011 (0) 120 (5)
Total 373 (4) 470 (6) 7143 (5)
Values are expressed as n ()
Excluding the 21 inhalational cases from the Sverdlovsk autopsyseries estimated survival in the current series is 449 (8) andin reported cases to date is 7122 (6)
330 NEUROLOGY 59 August (1 of 2) 2002
treatments The treatments administered to surviving pa-tients were in fact similar to those chosen in the entiregroup of patients in the current series All of the patientsreceived penicillin except the first case (Patient 1) whoreportedly received no treatment (Bernd Remler MD per-sonal communication February 2002)70 Only two of thepatients received corticosteroids in addition to antibiotics(Patients 4 and 6)3648 The only case with gastrointestinalanthrax (Patient 7) received the same treatment as hissister (aged 2 years) who died51 Treatment of survivingpatients was generally begun before the disease was clini-cally advanced Three of the patients who survived (Pa-tients 2 through 4) were receiving treatment for cutaneousanthrax (that included penicillin) before development ofsymptoms of meningoencephalitis13-152736 There is limitedinformation on long-term outcomes among the survivorsbut most were reported to have fully recovered13-1527363751
although two patients had residual focal weakness4870
Autopsy findings Autopsies were obtained in 40 of the66 deceased patients (61)28-32343538-4043-454755-5759 Thissummary is restricted to pathologic findings in the centralnervous system Gross findings typically included cloudyand congested leptomeninges with occasional obvious pu-rulent exudate13034354447 and with variable degrees of sub-arachnoid hemorrhage128293135394044455557 In many casessubarachnoid hemorrhage was the dominant gross patho-logic feature1282931353940444555 The vascular congestionand extensive subarachnoid hemorrhage of the leptome-ninges gave a dark red appearance on gross examination ofthe brain a finding sometimes referred to as a ldquocardinalrsquoscaprdquo2 Other common findings included intraventricularhemorrhage2939 intracerebral hematoma13956 multifocalsmall intraparenchymal cortical hemorrhages394047 or nu-merous petechial hemorrhages in cerebral parenchyma2864
zones of infarction in arterial venous or watershed distri-butions3964 and cerebral edema35454757 with tonsillar35 oruncal herniation47
Microscopic findings included hemorrhagic leptomen-ingitis2930343538-404447555764 and associated necrotizing vas-
culitis164 multifocal subarachnoid128-313538-404445555764 andintracerebral hemorrhage128-3038394756 multifocal cerebralinfarction3964 and leptomeningeal and cerebral ede-ma35394445475764 The hemorrhagic leptomeningitis was as-sociated with polymorphonuclear leukocytic inflammatoryexudates3538444755-5764 severe congestion of meningealblood vessels3538404756 hemorrhagic infiltration3544455664 orfrank subarachnoid hemorrhage128-313538-404445555764 aggre-gations of neutrophils and mononuclear phagocytes in andaround meningeal vessels3538404764 and tracking of bloodand inflammatory infiltrates along the VirchowndashRobin(perivascular) spaces into the parenchyma47 The superfi-cial cerebral cortex showed diffuse perineuronal andperivascular infiltration by neutrophils353947 severe vascu-lar congestion3540 necrosis of blood vessel walls3539475664
recent thromboses353964 zones of ischemia3964 areas ofhemorrhage47 and edema35394445475764 Numerous largegram-positive rods in short chains were present in theleptomeninges and the subarachnoid and VirchowndashRobinspaces29-31344756 within and around meningeal and superfi-cial cortical vessels and vessels in regions of hemor-rhage313235394064 and within hemorrhagic lesions313247
Discussion Meningoencephalitis develops in atmost 5 of cases of cutaneous anthrax1428 howevermost cases of anthrax meningoencephalitis to datehave developed from cutaneous anthrax because thevast majority of naturally acquired cases of anthraxare cutaneous28 Meningoencephalitis may occur inup to half of the cases in industrial or bioweaponsoutbreaks of inhalational anthrax829303244 howeverin the recent bioterrorist outbreak of anthrax in theUnited States only the index case had meningitisamong the 11 cases of confirmed or suspected inhala-tional anthrax identified5971-73 The relatively low fre-quency of meningitis among anthrax cases in the USbioterrorism outbreak may be misleading though aslumbar punctures were done in few cases and the
Table 5 Patients with anthrax meningoencephalitis who survived
Variable
Patient no
1 2 3 4 5 6 7
Reference no 70 14 27 36 37 48 51
Year 1916 1947 1948 1972 1973 1989 1993
Age y 24 57 51 85 12 25 6
Sex F M M F M M M
Clinical type Unknown Cutaneous Cutaneous Cutaneous Cutaneous Cutaneous Gastrointestinal
Treatment None
Antianthrax serum X
Penicillin X X X X X X
Chloramphenicol I
Streptomycin X X
Sulfonamide X I
Corticosteroid X X
Residual L hemiparesis None None None None RUE weakness None
X main therapy I initial therapy only RUE right upper extremity
August (1 of 2) 2002 NEUROLOGY 59 331
brain was not examined in some autopsies Based onprevious experience44 the potential exists for largenumbers of cases of anthrax meningoencephalitiswith further bioterrorist outbreaks or bioweaponsdispersals Meningoencephalitis may also occur withgastrointestinal anthrax or without a clinically ap-parent primary focus
Current guidelines from the Centers for DiseaseControl indicate that ciprofloxacin or doxycyclineshould be included as essential components of initialtherapy for anthrax infections of any portal of en-try7274 It is important to treat anthrax meningoen-cephalitis with a polydrug antibiotic regimen usingantimicrobial agents that have good CSF penetrationin meningitis and that provide good antibacterialcoverage for B anthracis All six patients who sur-vived after antibiotic treatment for anthrax menin-goencephalitis were treated with penicillinHowever because of the presence of constitutive orinducible beta-lactamases in B anthracis isolatesfrom the recent US bioterrorist outbreak and expec-tations that beta-lactamase activity may be likelywith bioengineered bioweapons agents ampicillin orpenicillin G alone are not recommended for initialtherapy for anthrax meningoencephalitis prior to an-tibiotic sensitivity results from culture7274 Rifampinplus vancomycin would be a reasonable choice foraddition to ciprofloxacin or doxycycline in the initialtreatment of anthrax meningoencephalitis Some in-fectious disease authorities recommend ciprofloxacinin preference to doxycycline plus augmentation withchloramphenicol rifampin or penicillin for estab-lished or suspected anthrax meningoencephalitis6
Aztreonam trimethoprim-sulfamethoxazole orthird-generation cephalosporins should not be usedbecause of natural resistance of B anthracis strainsto these antibiotics
Bacterial toxins have long been felt to play a ma-jor role in anthrax meningoencephalitis becausemany effects of B anthracis cannot be attributed tomicroscopically evident tissue changes1075 Virulenceof B anthracis requires an antiphagocytic capsuleand two exotoxins The two toxins are binary pro-teins composed of a binding protein and an enzymat-ically active protein2476 Among other actions thesetoxins collectively produce local edema impair neu-trophil function depress cerebral cortical electricalactivity depress central respiratory center activitycause bleeding and destruction of the brain and vitalorgans in the chest and induce cardiovascular col-lapse and shock244476-79
Although antitoxin was used early in the 20thcentury to treat anthrax alone or in combinationwith penicillin13-15 it has not been available in recentdecades to US civilian populations Conceptually an-tianthrax serum may augment the effect of antibiot-ics by helping to neutralize the anthrax toxinswhich are not inactivated by antibiotics Howeverthere are no documented cases of successful treat-ment of anthrax meningitis with antianthrax serumalone Haight incorrectly stated that a case reported
by Czyhlarz in 191670 had been cured by treatmentwith antianthrax serum when in fact a full transla-tion indicates that the patient received no treatment(Bernd Remler MD personal communication Feb-ruary 2002 see supplementary document) this er-ror has been promulgated by numerous subsequentauthors and has been a source of incorrect conclu-sions regarding potentially effective therapy for an-thrax meningoencephalitis in recent reviewsCzyhlarz70 also presented unpublished second-handinformation on another patient who purportedly re-covered from anthrax meningoencephalitis withouttreatment In light of subsequent experience withthis disease it is hard to interpret or credit either ofthese reports Available experimental data80 do notindicate a significant treatment effect of antianthraxserum beyond that of penicillin Nevertheless anti-anthrax immune globulin derived from the blood ofsoldiers who have received the anthrax vaccine isbeing added to the US bioterrorism treatment stock-pile and is being considered as a potential experi-mental anthrax treatment in the event of furtherbioterrorism anthrax cases681
Corticosteroids have been recommended as an ad-junctive agent in the treatment of meningitis in chil-dren82 Use of corticosteroids in adults withmeningitis is controversial but steroids have beenrecommended for consideration as adjunctive agentswithout any age restriction in anthrax meningitis72
If corticosteroids are used in conjunction with vanco-mycin therapy antibiotic dosing may need to bemodified because CSF vancomycin levels may be de-creased by corticosteroids contributing to treatmentfailure82-86
In addition to antibiotic management patientswith anthrax meningoencephalitis may require ag-gressive intensive care measures Seizures in-creased intracranial pressure subarachnoid andintracerebral hemorrhage electrolyte disturbanceshypotension shock and disseminated intravascularcoagulation may develop as complications of this in-fection Despite aggressive treatment the prognosisfor survival with anthrax meningoencephalitis isvery poor
AcknowledgmentThe author thanks Glen Salter MS of the Tomah VA MedicalCenter Library for assistance in locating references Pat Mennickeof the Tomah VA Medical Center for assistance with Excel spread-sheets Bernd Remler MD of the Medical College of WisconsinMilwaukee for translating the paper by Czyhlarz Larry DavisMD of the Albuquerque VA Medical Center for helpful correspon-dence regarding corticosteroids and vancomycin Jeffrey M JonesMD PhD of the William S Middleton VA Medical Center Madi-son for helpful discussions regarding antibiotic treatment of an-thrax meningoencephalitis and Mary Jo Lanska MD MS of theTomah VA Medical Center for helpful discussions and for criti-cally reviewing the manuscript
References1 Haight TH Anthrax meningitis review of literature and report
of two cases with autopsies Am J Med Sci 195222457ndash692 Dixon TC Meselson M Guillemin J Hanna PC Anthrax
N Engl J Med 1999341815ndash826
332 NEUROLOGY 59 August (1 of 2) 2002
3 Inglesby TV Henderson DA Bartlett JG et al Anthrax as abiological weapon medical and public health managementJAMA 19992811735ndash1745
4 Swartz MN Recognition and management of anthrax an up-date N Engl J Med 20013451621ndash1626
5 Jernigan JA Stephens DS Ashford DA et al Bioterrorism-related inhalational anthrax the first 10 cases reported in theUnited States Emerg Infect Dis 20017933ndash944
6 Inglesby TV OrsquoToole T Henderson DA et al Anthrax as abiological weapon 2002 updated recommendations for man-agement JAMA 20022872236ndash2252
7 Miller JK Human anthrax in New York State NY StateJ Med 1961612046ndash2053
8 Brachman PS Human anthrax in the United States Antimi-crob Agents Chemother 19655111ndash114
9 Kumar A Kanungo R Bhattacharya S Badrinath S DuttaTK Swaminathan RP Human anthrax in India urgent needfor effective prevention J Commun Dis 200032240ndash246
10 Dutz W Kohout E Anthrax Pathol Annu 197162009ndash224811 Trivedy JR Case of anthrax meningitis survival Cent Afr
J Med 19812716612 Roberts CJ Chambers PG An outbreak of anthrax in the
Mondoro Tribal Trust lands Cent Afr J Med 19752173ndash7613 Kindler D Recovery from anthrax meningitis Ind Med Surg
195221487ndash48814 Shanahan RH Griffin JR Von Auersperg AP Anthrax men-
ingitis report of a case of internal anthrax with recoveryAm J Clin Pathol 194717719ndash722
15 Griffin JR Shanahan RH DeAngelis CE Treatment of cuta-neous anthrax with penicillin NY State J Med 1948481718ndash1721
16 Boudin G Lauras A Vaillant C Etat de mal eacutepileptiquereacuteveacutelateur drsquoune meacuteningite charbonneuse etude anatamo-clinique Bull Mem Soc Med Hop Paris 1964115183ndash187
17 Rapun Pac JL Ull Laita M Meningitis carbuncosa Arch Neu-robiol (Madr) 197235143ndash148
18 Baltiev A Besleaga E Cuciureanu G Obreja E Meningo-encefalita carbunoasa la un copil cu pustula cutanata necarac-teristica Rev Med Chir Soc Med Nat Iasi 197377885ndash888
19 Beer K Milzbrandmeningitis Path Microbiol 19733912ndash1320 Bach I Simon L Baacuten E Toacuteth L Kovaacutecs M Haemorrhagiaacutes
meningitises apoplexia anthrax sepsisben Orv Hetil 19781191797ndash1799
21 Marandian MH Kamali A Meacuteningite charbonneuse un casen apparence primitif Nouv Presse Med 1981101747ndash1748
22 Duumlrst UN Bartenstein J Buumlhlmann H Wuumlst J Spiegel MVAnthraxmeningitis Schweiz Med Wochenschr 19861161222ndash1228
23 Gonzalez A Rodriguez E Castillo M Ortega I Ramirez EFajardo J Lesioacuten necroacutetica en mentoacuten en paciente con siacuten-drome meniacutengeo Enferm Infecc Mircobiol Clin 199715163ndash164
24 Abramova AA Grinberg LM [Pathology of anthrax sepsisaccording to materials of the infectious outbreak in 1979 inSverdlovsk (macroscopic changes)] Arkh Patol 19935512ndash17
25 Abramova AA Grinberg LM [Pathology of anthrax sepsisaccording to materials of infectious outbreak in 1979 in Sverd-lovsk (microscopic changes)] Arkh Patol 19935518ndash23
26 Grinberg LM Abramova AA [Pathology of anthrax sepsisaccording to materials of the infectious outbreak in 1979 inSverdlovsk (various aspects of morpho- patho- and thanato-genesis] Arkh Patol 19935523ndash26
27 Weinstein L Oliver CS The treatment of human anthraxwith penicillin Am Pract 19482533ndash538
28 Raper AB Anthrax meningo-encephalitis East Afr Med J195330399-401
29 Albrink WS Brooks SM Biron RE Kopel M Human inhala-tional anthrax a report of three fatal cases Am J Pathol196036457ndash468
30 Plotkin SA Brachman PS Utell M Bumford FH AtchisonMM An epidemic of inhalation anthrax the first in the twen-tieth century I Clinical features Am J Med 196029992ndash1001
31 Brachman PS Pagano JS Albrink WS Two cases of fatalinhalation anthrax one associated with sarcoidosis N EnglJ Med 1961265203ndash208
32 Brachman PS Inhalation anthrax Ann NY Acad Sci 198035383ndash93
33 Vita A Secu A Cuciureanu G Leibovici M Bejanariu C CujuG Considerations on 3 cases of meningo-encephalitis due toanthrax bacilli Rom Med Rev 1961536ndash39
34 LaForce FM Bumford FH Freely JC Stokes SL Snow DBEpidemiologic study of a fatal case of inhalation anthrax ArchEnviron Health 196918798ndash805
35 Rangel RA Gonzaacutelez DA Bacillus anthracis meningitis Neu-rology 197525525ndash530
36 Tahernia AC Hashemi G Survival in anthrax meningitisPediatrics 197250329ndash333
37 Tengio FU Anthrax meningitis report of two cases East AfrMed J 197350337ndash339
38 Viratchai C Anthrax gastro-enteritis and meningitis J MedAssoc Thai 197457147ndash150
39 Pluot M Vital C Aubertin J Croix JC Pire JC Poisot DAnthrax meningitis report of two cases with autopsies ActaNeuropathol (Berl) 197636339ndash345
40 Suffin SC Carnes WH Kaufman AF Inhalation anthrax in ahome craftsman Hum Pathol 19789594ndash597
41 Al-Dulaimy SB Al-Allaf GA Anthrax meningitis Trans R SocTrop Med Hyg 197872315
42 Manios S Kavaliotis I Anthrax in children a long forgottenpotentially fatal condition Scand J Infect Dis 197911203ndash206
43 Koshi G Lalitha MK Daniel J Chacko A Pulimood BMAnthrax meningitis a rare clinical entity J Assoc PhysiciansIndia 19812959ndash62
44 Abramova FA Grinberg LM Tampolskaya OV Walker DHPathology of inhalational anthrax in 42 cases from the Sverd-lovsk outbreak of 1979 Proc Natl Acad Sci USA 1993902291ndash2294
45 Levy L Baker N Meyer MP Crosland P Hampton J Anthraxmeningitis in Zimbabwe Cent Afr J Med 198127101ndash104
46 Bhat P Pereira P Mohan N Primary anthrax meningitis acase report Neurol India 19833171ndash73
47 Chandramukhi A Shankar P Rao TV Sundararajan SSwamy HS Acute leptomeningitis due to Bacillus anthracis acase report Trop Geogr Med 19833579ndash82
48 Khanna N Gokul BN Ravikumar R et al Successfullytreated primary anthrax meningitis Indian J Pathol Micro-biol 198932315ndash317
49 Kanungo R Sujatha S Das AK Rao RS Anthrax meningitisa clinical enigma Indian J Med Microbiol 19906149ndash151
50 Bharathmoorthy Chakravarthy I Swaminathan RP et alHaemorrhagic meningitis due to Bacillus anthrax J AssocPhysicians India 199240134ndash135
51 Tabatabaie P Syadati A Bacillus anthracis as a cause ofbacterial meningitis Pediatr Infect Dis 1993121035ndash1037
52 George S Mathai D Balraj V Lalitha MK John TJ An out-break of anthrax meningoencephalitis Trans R Soc Trop MedHyg 199488206ndash207
53 Berthier M Fauchegravere J-L Perrin J Grignon B Oriot D Ful-minant meningitis due to Bacillus anthracis in 11-year-oldgirl during Ramadan Lancet 1996347828
54 Domiacutenguez E Bustos C Garcia M Recio S Anthrax meningo-encephalitis radiologic findings AJR Am J Roentgenol 1997169317
55 Kwong KL Que TL Wong SN So KT Fatal meningoenceph-alitis due to Bacillus anthracis J Paediatr Child Health 199733539ndash541
56 Garcia AG Jiminez RR Bacillus anthracis meningitis N EnglJ Med 1999341814
57 Ringertz SH Hoiby EA Jensenius M et al Injectional an-thrax in a heroin skin-popper Lancet 20003461574ndash1575
58 Kim HJ Jun WB Lee SH Rho MH CT and MR findings ofanthrax meningoencephalitis report of two cases and reviewof the literature AJNR Am J Neuroradiol 2001221303ndash1305
59 Bush LM Abrams BH Heall A Johnson CC Index case offatal inhalational anthrax due to bioterrorism in the UnitedStates N Engl J Med 20013451607ndash1610
60 Brachman PS Plotkin SA Bumford FH Atchison MM Anepidemic of inhalation anthrax the first in the twentieth cen-tury II Epidemiology Am J Hygiene 1960726ndash23
61 Belluck P Anthrax outbreak of rsquo57 felled a mill but yieldedanswers New York Times October 27 2001B8
62 Meselson M Guillemin J Hugh-Jones M et al The Sverd-lovsk anthrax outbreak of 1979 Science 19942661202ndash1208
August (1 of 2) 2002 NEUROLOGY 59 333
63 Jackson PJ Hugh-Jones ME Adair DM et al PCR analysis oftissue samples from the 1979 Sverdlovsk anthrax victims thepresence of multiple Bacillus anthracis strains in differentvictims Proc Natl Acad Sci USA 1998951224ndash1229
64 Grinberg LM Abramova FA Yampolskaya OV Walker DHSmith JH Quantitative pathology of inhalational anthrax IQuantitative microscopic findings Mod Pathol 200114482ndash495
65 Brookmeyer R Blades N Hugh-Jones M Henderson D Thestatistical analysis of truncated data application to the Sverd-lovsk anthrax outbreak Biostatistics 20012233ndash247
66 Knott FA A note on anthrax infection by shaving brushesLancet 19231227ndash228
67 Bradaric N Punda-Polic V Cutaneous anthrax due topenicillin-resistant Bacillus anthracis transmitted by an in-sect bite Lancet 1992340306ndash307
68 Turell MJ Knudson GB Mechanical transmission of Bacillusanthracis by stable flies (Stomoxys calcitrans) and mosquitoes(Aedes aegypti and Aedes taeniorhynchus) Infect Immun1987551859ndash1861
69 Drake DJ Meningitic anthrax Cent Afr J Med 19711797ndash9870 Czyhlarz EV Beitrag zur Lehre von der Milzbrandmeningitis
Wein Klin Wochenscr 191629768ndash76971 Centers for Disease Control Investigation of anthrax associ-
ated with intentional exposure and interim public healthguidelines October 2001 MMWR Morb Mortal Wkly Rep200150889ndash893
72 Centers for Disease Control Update investigation ofbioterrorism-related anthrax and interim guidelines for expo-sure management and antimicrobial therapy October 2001MMWR Morb Mortal Wkly Rep 200150909ndash919
73 Centers for Disease Control Investigation of bioterrorism-related anthrax and interim guidelines for clinical evaluationof persons with possible anthrax MMWR Morb Mortal WklyRep 200150941ndash948
74 Centers for Disease Control Updated recommendations forantimicrobial prophylaxis among asymptomatic pregnantwomen after exposure to Bacillus anthracis MMWR MorbMortal Wkly Rep 200150960
75 Bonventure PF Sueoka W True CW Klein F Lincoln RAttempts to implicate the central nervous system as a pri-
mary site of action for Bacillus anthracis lethal toxin FedProc 1967261549ndash1553
76 Friedlander AM Anthrax In Sidell FR Takafuji ET FranzDR eds Textbook of military medicine medical aspects ofchemical and biological warfare Washington DC Office ofthe Surgeon General 1997467ndash478
77 Vick JA Lincoln RE Klein F Mahlandt BG Walker JS FishDC Neurological and physiological responses of the primateto anthrax toxin J Infect Dis 196811885ndash96
78 Klein F Lincoln RE Dobbs JP Mahlandt BG Remmele NSWalker JS Neurological and physiological responses of theprimate to anthrax infection J Infect Dis 196811897ndash103
79 Remmele NS Klein F Vick JA Walker JS Mahlandt BGLincoln RE Anthrax toxin primary site of action J Infect Dis1968118104ndash113
80 Doganay M Hanagasi R Zora A [Evaluation of penicillinalone and penicillin combined with anti-anthrax serum in ex-perimental anthrax in mice] Mikrobiyol Bul 19851957ndash64
81 Associated Press Government may offer anthrax treatmentNew York Times January 7 2002
82 Davis LE Acute bacterial meningitis In Johnson RT GriffinJW eds Current therapy in neurologic disease 5th ed StLouis Mosby 1997120ndash127
83 Viladrich PF Gudiol F Lintildeares J et al Evaluation of vanco-mycin for therapy of adult pneumococcal meningitis Antimi-crob Agents Chemother 1991352467ndash2472
84 Pariacutes M Hickey SM Uscher MI Shelton S Olsen KD Mc-Cracken GH Jr Effect of dexamethasone on therapy of exper-imental penicillin- and cephalosporin-resistant pneumococcalmeningitis Antimicrob Agents Chemother 1994381320ndash1324
85 Cabellos C Martinez-Lacasa J Martos A et al Influence ofdexamethasone on efficacy of ceftriaxone and vancomycintherapy in experimental pneumococcal meningitis AntimicrobAgents Chemother 1995392158ndash2160
86 Ahmed A Jafri H Lutsar I et al Pharmacodynamics of van-comycin for the treatment of experimental penicillin- andcephalosporin-resistant pneumococcal meningitis AntimicrobAgents Chemother 199943876ndash881
334 NEUROLOGY 59 August (1 of 2) 2002
DOI 101212WNL593327200259327-334 Neurology
Douglas J LanskaAnthrax meningoencephalitis
This information is current as of August 13 2002
ServicesUpdated Information amp
httpwwwneurologyorgcontent593327fullhtmlincluding high resolution figures can be found at
Supplementary Material
htmlhttpwwwneurologyorgneurologysuppl20020716593327DC2
htmlhttpwwwneurologyorgneurologysuppl20020716593327DC1Supplementary material can be found at
References httpwwwneurologyorgcontent593327fullhtmlref-list-1
This article cites 73 articles 15 of which you can access for free at
Citations httpwwwneurologyorgcontent593327fullhtmlotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpwwwneurologyorgcgicollectionmeningitisMeningitis
httpwwwneurologyorgcgicollectionencephalitisEncephalitis
httpwwwneurologyorgcgicollectionbacterial_infectionsBacterial infections
httpwwwneurologyorgcgicollectionall_infectionsAll Infectionsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsin its entirety can be found online atInformation about reproducing this article in parts (figurestables) or
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

counts with a left shift The range of white cell counts inthe current series was from 5400 to 27700 somewhatlower than the range of 10000 to 80000 reported byHaight1 Blood cultures were positive in 71 (ie 1521) ofcases for whom these were reported nearly identical to thevalue of 70 reported by Haight1 Chest x-rays were oftenabnormal in patients with inhalational anthrax32344059
and occasionally in patients with gastrointestinal51 or cuta-neous disease3554 Chest x-ray findings included pleuraleffusion3234405159 hilar adenopathy3240 widened mediasti-num59 infiltrates35 and soft tissue edema54
EEG results have rarely been reported even thoughseizures are fairly common In part this reflects the mori-bund state of most of these patients In one patient withreported myoclonus and fasciculations EEG showed disor-ganized low-amplitude slow waves (1 to 7 Hz)39
CT or MRI of the head in patients with anthrax menin-goencephalitis may demonstrate focal intracerebral hemor-rhage subarachnoid hemorrhage intraventricularhemorrhage diffuse cerebral edema and prominent lepto-meningeal enhancement5458 Parenchymal cerebral en-hancement has not been reported58 but its absence maysimply reflect the paucity of neuroimaging studies in thesepatients Abnormalities may progress rapidly on serialbrain imaging studies54
Differential diagnosis Hemorrhagic meningitis shouldraise suspicion of anthrax infection36 particularly if gram-positive rods are demonstrated on Gramrsquos stain Listeriamonocytogenes the only common gram-positive rod caus-ing meningitis does not produce a hemorrhagic meningitisand is rarely seen on Gramrsquos stain Based on initial clinicaldiagnoses in reported cases the differential diagnosis ofanthrax meningoencephalitis may include subarachnoidand intracerebral hemorrhage ischemic stroke nonan-thrax bacterial meningoencephalitis herpes simplex virusencephalitis and other viral encephalitides eclampsia andcerebral malaria
Treatment Antianthrax treatment was reported in 39patients1228-3840424345-5255-59 Of these 19 (49) receivedpenicillin only28-32353842454849525658 (administered parenter-ally in all but one case)2930 19 (49) received penicillin (orin one case ampicillin)55 in combination with other antibi-otic therapy12293032-343637404345-475051555759 and one (3) re-ceived antianthrax serum only33 Antibiotics used inconjunction with penicillin therapy included chloramphen-icol (11 cases)33364345-475057 streptomycin (7 cas-es)1229303233374051 sulfonamides (4 cases)122930364557
cefotaxime (2 cases)5559 tetracyclines (1 case)33 vancomy-cin (1 case)59 and antianthrax serum (1 case)33 Corticoste-roids were administered in conjunction with antibiotics inten cases (26)3336424345485257 In the Sverdlovsk inhala-tional anthrax outbreak in 1979 hospitalized patientswere treated variously with penicillin cephalosporinchloramphenicol antianthrax globulin and corticoste-roids62 but case-specific treatments and outcomes were notreported in the English language literature either in gen-eral or for the 21 patients autopsied after dying with an-thrax meningoencephalitis446263
Prognosis Septicemia toxic shock and death rapidlyfollow development of anthrax meningoencephalitis inmost cases Many patients presented in extremis followinga prodromal period of 1 to 6 days and 75 died within 24hours of presentation (ie 4155 of cases for whom such
information was available)28-3538394144-4749-5269 Four pa-tients (6) in the present series survived36374851 comparedwith three (4) in the previous world literature a differ-ence that was not significant (p 071) (table 4) Exclud-ing the 21 cases of inhalational anthrax from theSverdlovsk autopsy series44 estimated survival in the cur-rent series is four of 49 (8) and in all reported cases todate is seven of 122 (6) the difference in survival be-tween this restricted group of deceased patients and thesurviving patients was also not significant (p 044) Re-ported additional cases of survival had no clinical informa-tion (two cases)7 or were not established microbiologicallyor pathologically as cases of anthrax (one case)11 An addi-tional recent series of 12 cases with no survivals did notreport case-specific information9
Survival appears to be most likely if meningoencephali-tis develops as part of the course of cutaneous an-thrax363748 but a single case with survival has beenreported with gastrointestinal anthrax51 In the currentseries 15 of cutaneous cases survived compared with 8among gastrointestinal cases none among inhalationalcases and none among unknown or unspecified cases (seetable 3) The difference in survival of the cutaneous casesin the current series (15) and Haightrsquos series (5) wasnot significant (p 032) To date in the world literaturethere are no reported cases of survival following anthraxmeningoencephalitis associated with inhalational anthrax
The seven surviving patients reported to date are sum-marized in table 513-15273637485170 Surviving patients wereyounger as a group than those in the present series whodied (median age of surviving cases 24 years n7 me-dian age of cases who died 45 years n 66 p 004) Ifthe comparison is restricted to cases in the current seriesonly the difference in age is greater (median age of surviv-ing cases 1025 years n 4 p 0003) In generalinitial CSF results from the surviving patients were eithernormal or were less severely abnormal compared to de-ceased patients However because of the small samplesizes for different CSF studies in the survival group noneof the individual contrasts was significant (glucose p 041 protein p 012 red cells p 024 white cellsp 008)
Many reports and reviews failed to identify all of thepreviously reported cases with survival or misreported as-pects of the cases they did review resulting in incorrectconclusions about the agents that are potentially effective
Table 4 Survival with anthrax meningoencephalitis inreported cases
Primary focus Haight 1952 Lanska 2002 Total
Cutaneous 239 (5) 320 (15) 559 (8)
Gastrointestinal 07 (0) 112 (8) 119 (5)
Inhalational 017 (0) 027 (0) 044 (0)
Maternal sepsis 01 (0) 01 (0)
None identified 19 (11) 011 (0) 120 (5)
Total 373 (4) 470 (6) 7143 (5)
Values are expressed as n ()
Excluding the 21 inhalational cases from the Sverdlovsk autopsyseries estimated survival in the current series is 449 (8) andin reported cases to date is 7122 (6)
330 NEUROLOGY 59 August (1 of 2) 2002
treatments The treatments administered to surviving pa-tients were in fact similar to those chosen in the entiregroup of patients in the current series All of the patientsreceived penicillin except the first case (Patient 1) whoreportedly received no treatment (Bernd Remler MD per-sonal communication February 2002)70 Only two of thepatients received corticosteroids in addition to antibiotics(Patients 4 and 6)3648 The only case with gastrointestinalanthrax (Patient 7) received the same treatment as hissister (aged 2 years) who died51 Treatment of survivingpatients was generally begun before the disease was clini-cally advanced Three of the patients who survived (Pa-tients 2 through 4) were receiving treatment for cutaneousanthrax (that included penicillin) before development ofsymptoms of meningoencephalitis13-152736 There is limitedinformation on long-term outcomes among the survivorsbut most were reported to have fully recovered13-1527363751
although two patients had residual focal weakness4870
Autopsy findings Autopsies were obtained in 40 of the66 deceased patients (61)28-32343538-4043-454755-5759 Thissummary is restricted to pathologic findings in the centralnervous system Gross findings typically included cloudyand congested leptomeninges with occasional obvious pu-rulent exudate13034354447 and with variable degrees of sub-arachnoid hemorrhage128293135394044455557 In many casessubarachnoid hemorrhage was the dominant gross patho-logic feature1282931353940444555 The vascular congestionand extensive subarachnoid hemorrhage of the leptome-ninges gave a dark red appearance on gross examination ofthe brain a finding sometimes referred to as a ldquocardinalrsquoscaprdquo2 Other common findings included intraventricularhemorrhage2939 intracerebral hematoma13956 multifocalsmall intraparenchymal cortical hemorrhages394047 or nu-merous petechial hemorrhages in cerebral parenchyma2864
zones of infarction in arterial venous or watershed distri-butions3964 and cerebral edema35454757 with tonsillar35 oruncal herniation47
Microscopic findings included hemorrhagic leptomen-ingitis2930343538-404447555764 and associated necrotizing vas-
culitis164 multifocal subarachnoid128-313538-404445555764 andintracerebral hemorrhage128-3038394756 multifocal cerebralinfarction3964 and leptomeningeal and cerebral ede-ma35394445475764 The hemorrhagic leptomeningitis was as-sociated with polymorphonuclear leukocytic inflammatoryexudates3538444755-5764 severe congestion of meningealblood vessels3538404756 hemorrhagic infiltration3544455664 orfrank subarachnoid hemorrhage128-313538-404445555764 aggre-gations of neutrophils and mononuclear phagocytes in andaround meningeal vessels3538404764 and tracking of bloodand inflammatory infiltrates along the VirchowndashRobin(perivascular) spaces into the parenchyma47 The superfi-cial cerebral cortex showed diffuse perineuronal andperivascular infiltration by neutrophils353947 severe vascu-lar congestion3540 necrosis of blood vessel walls3539475664
recent thromboses353964 zones of ischemia3964 areas ofhemorrhage47 and edema35394445475764 Numerous largegram-positive rods in short chains were present in theleptomeninges and the subarachnoid and VirchowndashRobinspaces29-31344756 within and around meningeal and superfi-cial cortical vessels and vessels in regions of hemor-rhage313235394064 and within hemorrhagic lesions313247
Discussion Meningoencephalitis develops in atmost 5 of cases of cutaneous anthrax1428 howevermost cases of anthrax meningoencephalitis to datehave developed from cutaneous anthrax because thevast majority of naturally acquired cases of anthraxare cutaneous28 Meningoencephalitis may occur inup to half of the cases in industrial or bioweaponsoutbreaks of inhalational anthrax829303244 howeverin the recent bioterrorist outbreak of anthrax in theUnited States only the index case had meningitisamong the 11 cases of confirmed or suspected inhala-tional anthrax identified5971-73 The relatively low fre-quency of meningitis among anthrax cases in the USbioterrorism outbreak may be misleading though aslumbar punctures were done in few cases and the
Table 5 Patients with anthrax meningoencephalitis who survived
Variable
Patient no
1 2 3 4 5 6 7
Reference no 70 14 27 36 37 48 51
Year 1916 1947 1948 1972 1973 1989 1993
Age y 24 57 51 85 12 25 6
Sex F M M F M M M
Clinical type Unknown Cutaneous Cutaneous Cutaneous Cutaneous Cutaneous Gastrointestinal
Treatment None
Antianthrax serum X
Penicillin X X X X X X
Chloramphenicol I
Streptomycin X X
Sulfonamide X I
Corticosteroid X X
Residual L hemiparesis None None None None RUE weakness None
X main therapy I initial therapy only RUE right upper extremity
August (1 of 2) 2002 NEUROLOGY 59 331
brain was not examined in some autopsies Based onprevious experience44 the potential exists for largenumbers of cases of anthrax meningoencephalitiswith further bioterrorist outbreaks or bioweaponsdispersals Meningoencephalitis may also occur withgastrointestinal anthrax or without a clinically ap-parent primary focus
Current guidelines from the Centers for DiseaseControl indicate that ciprofloxacin or doxycyclineshould be included as essential components of initialtherapy for anthrax infections of any portal of en-try7274 It is important to treat anthrax meningoen-cephalitis with a polydrug antibiotic regimen usingantimicrobial agents that have good CSF penetrationin meningitis and that provide good antibacterialcoverage for B anthracis All six patients who sur-vived after antibiotic treatment for anthrax menin-goencephalitis were treated with penicillinHowever because of the presence of constitutive orinducible beta-lactamases in B anthracis isolatesfrom the recent US bioterrorist outbreak and expec-tations that beta-lactamase activity may be likelywith bioengineered bioweapons agents ampicillin orpenicillin G alone are not recommended for initialtherapy for anthrax meningoencephalitis prior to an-tibiotic sensitivity results from culture7274 Rifampinplus vancomycin would be a reasonable choice foraddition to ciprofloxacin or doxycycline in the initialtreatment of anthrax meningoencephalitis Some in-fectious disease authorities recommend ciprofloxacinin preference to doxycycline plus augmentation withchloramphenicol rifampin or penicillin for estab-lished or suspected anthrax meningoencephalitis6
Aztreonam trimethoprim-sulfamethoxazole orthird-generation cephalosporins should not be usedbecause of natural resistance of B anthracis strainsto these antibiotics
Bacterial toxins have long been felt to play a ma-jor role in anthrax meningoencephalitis becausemany effects of B anthracis cannot be attributed tomicroscopically evident tissue changes1075 Virulenceof B anthracis requires an antiphagocytic capsuleand two exotoxins The two toxins are binary pro-teins composed of a binding protein and an enzymat-ically active protein2476 Among other actions thesetoxins collectively produce local edema impair neu-trophil function depress cerebral cortical electricalactivity depress central respiratory center activitycause bleeding and destruction of the brain and vitalorgans in the chest and induce cardiovascular col-lapse and shock244476-79
Although antitoxin was used early in the 20thcentury to treat anthrax alone or in combinationwith penicillin13-15 it has not been available in recentdecades to US civilian populations Conceptually an-tianthrax serum may augment the effect of antibiot-ics by helping to neutralize the anthrax toxinswhich are not inactivated by antibiotics Howeverthere are no documented cases of successful treat-ment of anthrax meningitis with antianthrax serumalone Haight incorrectly stated that a case reported
by Czyhlarz in 191670 had been cured by treatmentwith antianthrax serum when in fact a full transla-tion indicates that the patient received no treatment(Bernd Remler MD personal communication Feb-ruary 2002 see supplementary document) this er-ror has been promulgated by numerous subsequentauthors and has been a source of incorrect conclu-sions regarding potentially effective therapy for an-thrax meningoencephalitis in recent reviewsCzyhlarz70 also presented unpublished second-handinformation on another patient who purportedly re-covered from anthrax meningoencephalitis withouttreatment In light of subsequent experience withthis disease it is hard to interpret or credit either ofthese reports Available experimental data80 do notindicate a significant treatment effect of antianthraxserum beyond that of penicillin Nevertheless anti-anthrax immune globulin derived from the blood ofsoldiers who have received the anthrax vaccine isbeing added to the US bioterrorism treatment stock-pile and is being considered as a potential experi-mental anthrax treatment in the event of furtherbioterrorism anthrax cases681
Corticosteroids have been recommended as an ad-junctive agent in the treatment of meningitis in chil-dren82 Use of corticosteroids in adults withmeningitis is controversial but steroids have beenrecommended for consideration as adjunctive agentswithout any age restriction in anthrax meningitis72
If corticosteroids are used in conjunction with vanco-mycin therapy antibiotic dosing may need to bemodified because CSF vancomycin levels may be de-creased by corticosteroids contributing to treatmentfailure82-86
In addition to antibiotic management patientswith anthrax meningoencephalitis may require ag-gressive intensive care measures Seizures in-creased intracranial pressure subarachnoid andintracerebral hemorrhage electrolyte disturbanceshypotension shock and disseminated intravascularcoagulation may develop as complications of this in-fection Despite aggressive treatment the prognosisfor survival with anthrax meningoencephalitis isvery poor
AcknowledgmentThe author thanks Glen Salter MS of the Tomah VA MedicalCenter Library for assistance in locating references Pat Mennickeof the Tomah VA Medical Center for assistance with Excel spread-sheets Bernd Remler MD of the Medical College of WisconsinMilwaukee for translating the paper by Czyhlarz Larry DavisMD of the Albuquerque VA Medical Center for helpful correspon-dence regarding corticosteroids and vancomycin Jeffrey M JonesMD PhD of the William S Middleton VA Medical Center Madi-son for helpful discussions regarding antibiotic treatment of an-thrax meningoencephalitis and Mary Jo Lanska MD MS of theTomah VA Medical Center for helpful discussions and for criti-cally reviewing the manuscript
References1 Haight TH Anthrax meningitis review of literature and report
of two cases with autopsies Am J Med Sci 195222457ndash692 Dixon TC Meselson M Guillemin J Hanna PC Anthrax
N Engl J Med 1999341815ndash826
332 NEUROLOGY 59 August (1 of 2) 2002
3 Inglesby TV Henderson DA Bartlett JG et al Anthrax as abiological weapon medical and public health managementJAMA 19992811735ndash1745
4 Swartz MN Recognition and management of anthrax an up-date N Engl J Med 20013451621ndash1626
5 Jernigan JA Stephens DS Ashford DA et al Bioterrorism-related inhalational anthrax the first 10 cases reported in theUnited States Emerg Infect Dis 20017933ndash944
6 Inglesby TV OrsquoToole T Henderson DA et al Anthrax as abiological weapon 2002 updated recommendations for man-agement JAMA 20022872236ndash2252
7 Miller JK Human anthrax in New York State NY StateJ Med 1961612046ndash2053
8 Brachman PS Human anthrax in the United States Antimi-crob Agents Chemother 19655111ndash114
9 Kumar A Kanungo R Bhattacharya S Badrinath S DuttaTK Swaminathan RP Human anthrax in India urgent needfor effective prevention J Commun Dis 200032240ndash246
10 Dutz W Kohout E Anthrax Pathol Annu 197162009ndash224811 Trivedy JR Case of anthrax meningitis survival Cent Afr
J Med 19812716612 Roberts CJ Chambers PG An outbreak of anthrax in the
Mondoro Tribal Trust lands Cent Afr J Med 19752173ndash7613 Kindler D Recovery from anthrax meningitis Ind Med Surg
195221487ndash48814 Shanahan RH Griffin JR Von Auersperg AP Anthrax men-
ingitis report of a case of internal anthrax with recoveryAm J Clin Pathol 194717719ndash722
15 Griffin JR Shanahan RH DeAngelis CE Treatment of cuta-neous anthrax with penicillin NY State J Med 1948481718ndash1721
16 Boudin G Lauras A Vaillant C Etat de mal eacutepileptiquereacuteveacutelateur drsquoune meacuteningite charbonneuse etude anatamo-clinique Bull Mem Soc Med Hop Paris 1964115183ndash187
17 Rapun Pac JL Ull Laita M Meningitis carbuncosa Arch Neu-robiol (Madr) 197235143ndash148
18 Baltiev A Besleaga E Cuciureanu G Obreja E Meningo-encefalita carbunoasa la un copil cu pustula cutanata necarac-teristica Rev Med Chir Soc Med Nat Iasi 197377885ndash888
19 Beer K Milzbrandmeningitis Path Microbiol 19733912ndash1320 Bach I Simon L Baacuten E Toacuteth L Kovaacutecs M Haemorrhagiaacutes
meningitises apoplexia anthrax sepsisben Orv Hetil 19781191797ndash1799
21 Marandian MH Kamali A Meacuteningite charbonneuse un casen apparence primitif Nouv Presse Med 1981101747ndash1748
22 Duumlrst UN Bartenstein J Buumlhlmann H Wuumlst J Spiegel MVAnthraxmeningitis Schweiz Med Wochenschr 19861161222ndash1228
23 Gonzalez A Rodriguez E Castillo M Ortega I Ramirez EFajardo J Lesioacuten necroacutetica en mentoacuten en paciente con siacuten-drome meniacutengeo Enferm Infecc Mircobiol Clin 199715163ndash164
24 Abramova AA Grinberg LM [Pathology of anthrax sepsisaccording to materials of the infectious outbreak in 1979 inSverdlovsk (macroscopic changes)] Arkh Patol 19935512ndash17
25 Abramova AA Grinberg LM [Pathology of anthrax sepsisaccording to materials of infectious outbreak in 1979 in Sverd-lovsk (microscopic changes)] Arkh Patol 19935518ndash23
26 Grinberg LM Abramova AA [Pathology of anthrax sepsisaccording to materials of the infectious outbreak in 1979 inSverdlovsk (various aspects of morpho- patho- and thanato-genesis] Arkh Patol 19935523ndash26
27 Weinstein L Oliver CS The treatment of human anthraxwith penicillin Am Pract 19482533ndash538
28 Raper AB Anthrax meningo-encephalitis East Afr Med J195330399-401
29 Albrink WS Brooks SM Biron RE Kopel M Human inhala-tional anthrax a report of three fatal cases Am J Pathol196036457ndash468
30 Plotkin SA Brachman PS Utell M Bumford FH AtchisonMM An epidemic of inhalation anthrax the first in the twen-tieth century I Clinical features Am J Med 196029992ndash1001
31 Brachman PS Pagano JS Albrink WS Two cases of fatalinhalation anthrax one associated with sarcoidosis N EnglJ Med 1961265203ndash208
32 Brachman PS Inhalation anthrax Ann NY Acad Sci 198035383ndash93
33 Vita A Secu A Cuciureanu G Leibovici M Bejanariu C CujuG Considerations on 3 cases of meningo-encephalitis due toanthrax bacilli Rom Med Rev 1961536ndash39
34 LaForce FM Bumford FH Freely JC Stokes SL Snow DBEpidemiologic study of a fatal case of inhalation anthrax ArchEnviron Health 196918798ndash805
35 Rangel RA Gonzaacutelez DA Bacillus anthracis meningitis Neu-rology 197525525ndash530
36 Tahernia AC Hashemi G Survival in anthrax meningitisPediatrics 197250329ndash333
37 Tengio FU Anthrax meningitis report of two cases East AfrMed J 197350337ndash339
38 Viratchai C Anthrax gastro-enteritis and meningitis J MedAssoc Thai 197457147ndash150
39 Pluot M Vital C Aubertin J Croix JC Pire JC Poisot DAnthrax meningitis report of two cases with autopsies ActaNeuropathol (Berl) 197636339ndash345
40 Suffin SC Carnes WH Kaufman AF Inhalation anthrax in ahome craftsman Hum Pathol 19789594ndash597
41 Al-Dulaimy SB Al-Allaf GA Anthrax meningitis Trans R SocTrop Med Hyg 197872315
42 Manios S Kavaliotis I Anthrax in children a long forgottenpotentially fatal condition Scand J Infect Dis 197911203ndash206
43 Koshi G Lalitha MK Daniel J Chacko A Pulimood BMAnthrax meningitis a rare clinical entity J Assoc PhysiciansIndia 19812959ndash62
44 Abramova FA Grinberg LM Tampolskaya OV Walker DHPathology of inhalational anthrax in 42 cases from the Sverd-lovsk outbreak of 1979 Proc Natl Acad Sci USA 1993902291ndash2294
45 Levy L Baker N Meyer MP Crosland P Hampton J Anthraxmeningitis in Zimbabwe Cent Afr J Med 198127101ndash104
46 Bhat P Pereira P Mohan N Primary anthrax meningitis acase report Neurol India 19833171ndash73
47 Chandramukhi A Shankar P Rao TV Sundararajan SSwamy HS Acute leptomeningitis due to Bacillus anthracis acase report Trop Geogr Med 19833579ndash82
48 Khanna N Gokul BN Ravikumar R et al Successfullytreated primary anthrax meningitis Indian J Pathol Micro-biol 198932315ndash317
49 Kanungo R Sujatha S Das AK Rao RS Anthrax meningitisa clinical enigma Indian J Med Microbiol 19906149ndash151
50 Bharathmoorthy Chakravarthy I Swaminathan RP et alHaemorrhagic meningitis due to Bacillus anthrax J AssocPhysicians India 199240134ndash135
51 Tabatabaie P Syadati A Bacillus anthracis as a cause ofbacterial meningitis Pediatr Infect Dis 1993121035ndash1037
52 George S Mathai D Balraj V Lalitha MK John TJ An out-break of anthrax meningoencephalitis Trans R Soc Trop MedHyg 199488206ndash207
53 Berthier M Fauchegravere J-L Perrin J Grignon B Oriot D Ful-minant meningitis due to Bacillus anthracis in 11-year-oldgirl during Ramadan Lancet 1996347828
54 Domiacutenguez E Bustos C Garcia M Recio S Anthrax meningo-encephalitis radiologic findings AJR Am J Roentgenol 1997169317
55 Kwong KL Que TL Wong SN So KT Fatal meningoenceph-alitis due to Bacillus anthracis J Paediatr Child Health 199733539ndash541
56 Garcia AG Jiminez RR Bacillus anthracis meningitis N EnglJ Med 1999341814
57 Ringertz SH Hoiby EA Jensenius M et al Injectional an-thrax in a heroin skin-popper Lancet 20003461574ndash1575
58 Kim HJ Jun WB Lee SH Rho MH CT and MR findings ofanthrax meningoencephalitis report of two cases and reviewof the literature AJNR Am J Neuroradiol 2001221303ndash1305
59 Bush LM Abrams BH Heall A Johnson CC Index case offatal inhalational anthrax due to bioterrorism in the UnitedStates N Engl J Med 20013451607ndash1610
60 Brachman PS Plotkin SA Bumford FH Atchison MM Anepidemic of inhalation anthrax the first in the twentieth cen-tury II Epidemiology Am J Hygiene 1960726ndash23
61 Belluck P Anthrax outbreak of rsquo57 felled a mill but yieldedanswers New York Times October 27 2001B8
62 Meselson M Guillemin J Hugh-Jones M et al The Sverd-lovsk anthrax outbreak of 1979 Science 19942661202ndash1208
August (1 of 2) 2002 NEUROLOGY 59 333
63 Jackson PJ Hugh-Jones ME Adair DM et al PCR analysis oftissue samples from the 1979 Sverdlovsk anthrax victims thepresence of multiple Bacillus anthracis strains in differentvictims Proc Natl Acad Sci USA 1998951224ndash1229
64 Grinberg LM Abramova FA Yampolskaya OV Walker DHSmith JH Quantitative pathology of inhalational anthrax IQuantitative microscopic findings Mod Pathol 200114482ndash495
65 Brookmeyer R Blades N Hugh-Jones M Henderson D Thestatistical analysis of truncated data application to the Sverd-lovsk anthrax outbreak Biostatistics 20012233ndash247
66 Knott FA A note on anthrax infection by shaving brushesLancet 19231227ndash228
67 Bradaric N Punda-Polic V Cutaneous anthrax due topenicillin-resistant Bacillus anthracis transmitted by an in-sect bite Lancet 1992340306ndash307
68 Turell MJ Knudson GB Mechanical transmission of Bacillusanthracis by stable flies (Stomoxys calcitrans) and mosquitoes(Aedes aegypti and Aedes taeniorhynchus) Infect Immun1987551859ndash1861
69 Drake DJ Meningitic anthrax Cent Afr J Med 19711797ndash9870 Czyhlarz EV Beitrag zur Lehre von der Milzbrandmeningitis
Wein Klin Wochenscr 191629768ndash76971 Centers for Disease Control Investigation of anthrax associ-
ated with intentional exposure and interim public healthguidelines October 2001 MMWR Morb Mortal Wkly Rep200150889ndash893
72 Centers for Disease Control Update investigation ofbioterrorism-related anthrax and interim guidelines for expo-sure management and antimicrobial therapy October 2001MMWR Morb Mortal Wkly Rep 200150909ndash919
73 Centers for Disease Control Investigation of bioterrorism-related anthrax and interim guidelines for clinical evaluationof persons with possible anthrax MMWR Morb Mortal WklyRep 200150941ndash948
74 Centers for Disease Control Updated recommendations forantimicrobial prophylaxis among asymptomatic pregnantwomen after exposure to Bacillus anthracis MMWR MorbMortal Wkly Rep 200150960
75 Bonventure PF Sueoka W True CW Klein F Lincoln RAttempts to implicate the central nervous system as a pri-
mary site of action for Bacillus anthracis lethal toxin FedProc 1967261549ndash1553
76 Friedlander AM Anthrax In Sidell FR Takafuji ET FranzDR eds Textbook of military medicine medical aspects ofchemical and biological warfare Washington DC Office ofthe Surgeon General 1997467ndash478
77 Vick JA Lincoln RE Klein F Mahlandt BG Walker JS FishDC Neurological and physiological responses of the primateto anthrax toxin J Infect Dis 196811885ndash96
78 Klein F Lincoln RE Dobbs JP Mahlandt BG Remmele NSWalker JS Neurological and physiological responses of theprimate to anthrax infection J Infect Dis 196811897ndash103
79 Remmele NS Klein F Vick JA Walker JS Mahlandt BGLincoln RE Anthrax toxin primary site of action J Infect Dis1968118104ndash113
80 Doganay M Hanagasi R Zora A [Evaluation of penicillinalone and penicillin combined with anti-anthrax serum in ex-perimental anthrax in mice] Mikrobiyol Bul 19851957ndash64
81 Associated Press Government may offer anthrax treatmentNew York Times January 7 2002
82 Davis LE Acute bacterial meningitis In Johnson RT GriffinJW eds Current therapy in neurologic disease 5th ed StLouis Mosby 1997120ndash127
83 Viladrich PF Gudiol F Lintildeares J et al Evaluation of vanco-mycin for therapy of adult pneumococcal meningitis Antimi-crob Agents Chemother 1991352467ndash2472
84 Pariacutes M Hickey SM Uscher MI Shelton S Olsen KD Mc-Cracken GH Jr Effect of dexamethasone on therapy of exper-imental penicillin- and cephalosporin-resistant pneumococcalmeningitis Antimicrob Agents Chemother 1994381320ndash1324
85 Cabellos C Martinez-Lacasa J Martos A et al Influence ofdexamethasone on efficacy of ceftriaxone and vancomycintherapy in experimental pneumococcal meningitis AntimicrobAgents Chemother 1995392158ndash2160
86 Ahmed A Jafri H Lutsar I et al Pharmacodynamics of van-comycin for the treatment of experimental penicillin- andcephalosporin-resistant pneumococcal meningitis AntimicrobAgents Chemother 199943876ndash881
334 NEUROLOGY 59 August (1 of 2) 2002
DOI 101212WNL593327200259327-334 Neurology
Douglas J LanskaAnthrax meningoencephalitis
This information is current as of August 13 2002
ServicesUpdated Information amp
httpwwwneurologyorgcontent593327fullhtmlincluding high resolution figures can be found at
Supplementary Material
htmlhttpwwwneurologyorgneurologysuppl20020716593327DC2
htmlhttpwwwneurologyorgneurologysuppl20020716593327DC1Supplementary material can be found at
References httpwwwneurologyorgcontent593327fullhtmlref-list-1
This article cites 73 articles 15 of which you can access for free at
Citations httpwwwneurologyorgcontent593327fullhtmlotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpwwwneurologyorgcgicollectionmeningitisMeningitis
httpwwwneurologyorgcgicollectionencephalitisEncephalitis
httpwwwneurologyorgcgicollectionbacterial_infectionsBacterial infections
httpwwwneurologyorgcgicollectionall_infectionsAll Infectionsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsin its entirety can be found online atInformation about reproducing this article in parts (figurestables) or
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

treatments The treatments administered to surviving pa-tients were in fact similar to those chosen in the entiregroup of patients in the current series All of the patientsreceived penicillin except the first case (Patient 1) whoreportedly received no treatment (Bernd Remler MD per-sonal communication February 2002)70 Only two of thepatients received corticosteroids in addition to antibiotics(Patients 4 and 6)3648 The only case with gastrointestinalanthrax (Patient 7) received the same treatment as hissister (aged 2 years) who died51 Treatment of survivingpatients was generally begun before the disease was clini-cally advanced Three of the patients who survived (Pa-tients 2 through 4) were receiving treatment for cutaneousanthrax (that included penicillin) before development ofsymptoms of meningoencephalitis13-152736 There is limitedinformation on long-term outcomes among the survivorsbut most were reported to have fully recovered13-1527363751
although two patients had residual focal weakness4870
Autopsy findings Autopsies were obtained in 40 of the66 deceased patients (61)28-32343538-4043-454755-5759 Thissummary is restricted to pathologic findings in the centralnervous system Gross findings typically included cloudyand congested leptomeninges with occasional obvious pu-rulent exudate13034354447 and with variable degrees of sub-arachnoid hemorrhage128293135394044455557 In many casessubarachnoid hemorrhage was the dominant gross patho-logic feature1282931353940444555 The vascular congestionand extensive subarachnoid hemorrhage of the leptome-ninges gave a dark red appearance on gross examination ofthe brain a finding sometimes referred to as a ldquocardinalrsquoscaprdquo2 Other common findings included intraventricularhemorrhage2939 intracerebral hematoma13956 multifocalsmall intraparenchymal cortical hemorrhages394047 or nu-merous petechial hemorrhages in cerebral parenchyma2864
zones of infarction in arterial venous or watershed distri-butions3964 and cerebral edema35454757 with tonsillar35 oruncal herniation47
Microscopic findings included hemorrhagic leptomen-ingitis2930343538-404447555764 and associated necrotizing vas-
culitis164 multifocal subarachnoid128-313538-404445555764 andintracerebral hemorrhage128-3038394756 multifocal cerebralinfarction3964 and leptomeningeal and cerebral ede-ma35394445475764 The hemorrhagic leptomeningitis was as-sociated with polymorphonuclear leukocytic inflammatoryexudates3538444755-5764 severe congestion of meningealblood vessels3538404756 hemorrhagic infiltration3544455664 orfrank subarachnoid hemorrhage128-313538-404445555764 aggre-gations of neutrophils and mononuclear phagocytes in andaround meningeal vessels3538404764 and tracking of bloodand inflammatory infiltrates along the VirchowndashRobin(perivascular) spaces into the parenchyma47 The superfi-cial cerebral cortex showed diffuse perineuronal andperivascular infiltration by neutrophils353947 severe vascu-lar congestion3540 necrosis of blood vessel walls3539475664
recent thromboses353964 zones of ischemia3964 areas ofhemorrhage47 and edema35394445475764 Numerous largegram-positive rods in short chains were present in theleptomeninges and the subarachnoid and VirchowndashRobinspaces29-31344756 within and around meningeal and superfi-cial cortical vessels and vessels in regions of hemor-rhage313235394064 and within hemorrhagic lesions313247
Discussion Meningoencephalitis develops in atmost 5 of cases of cutaneous anthrax1428 howevermost cases of anthrax meningoencephalitis to datehave developed from cutaneous anthrax because thevast majority of naturally acquired cases of anthraxare cutaneous28 Meningoencephalitis may occur inup to half of the cases in industrial or bioweaponsoutbreaks of inhalational anthrax829303244 howeverin the recent bioterrorist outbreak of anthrax in theUnited States only the index case had meningitisamong the 11 cases of confirmed or suspected inhala-tional anthrax identified5971-73 The relatively low fre-quency of meningitis among anthrax cases in the USbioterrorism outbreak may be misleading though aslumbar punctures were done in few cases and the
Table 5 Patients with anthrax meningoencephalitis who survived
Variable
Patient no
1 2 3 4 5 6 7
Reference no 70 14 27 36 37 48 51
Year 1916 1947 1948 1972 1973 1989 1993
Age y 24 57 51 85 12 25 6
Sex F M M F M M M
Clinical type Unknown Cutaneous Cutaneous Cutaneous Cutaneous Cutaneous Gastrointestinal
Treatment None
Antianthrax serum X
Penicillin X X X X X X
Chloramphenicol I
Streptomycin X X
Sulfonamide X I
Corticosteroid X X
Residual L hemiparesis None None None None RUE weakness None
X main therapy I initial therapy only RUE right upper extremity
August (1 of 2) 2002 NEUROLOGY 59 331
brain was not examined in some autopsies Based onprevious experience44 the potential exists for largenumbers of cases of anthrax meningoencephalitiswith further bioterrorist outbreaks or bioweaponsdispersals Meningoencephalitis may also occur withgastrointestinal anthrax or without a clinically ap-parent primary focus
Current guidelines from the Centers for DiseaseControl indicate that ciprofloxacin or doxycyclineshould be included as essential components of initialtherapy for anthrax infections of any portal of en-try7274 It is important to treat anthrax meningoen-cephalitis with a polydrug antibiotic regimen usingantimicrobial agents that have good CSF penetrationin meningitis and that provide good antibacterialcoverage for B anthracis All six patients who sur-vived after antibiotic treatment for anthrax menin-goencephalitis were treated with penicillinHowever because of the presence of constitutive orinducible beta-lactamases in B anthracis isolatesfrom the recent US bioterrorist outbreak and expec-tations that beta-lactamase activity may be likelywith bioengineered bioweapons agents ampicillin orpenicillin G alone are not recommended for initialtherapy for anthrax meningoencephalitis prior to an-tibiotic sensitivity results from culture7274 Rifampinplus vancomycin would be a reasonable choice foraddition to ciprofloxacin or doxycycline in the initialtreatment of anthrax meningoencephalitis Some in-fectious disease authorities recommend ciprofloxacinin preference to doxycycline plus augmentation withchloramphenicol rifampin or penicillin for estab-lished or suspected anthrax meningoencephalitis6
Aztreonam trimethoprim-sulfamethoxazole orthird-generation cephalosporins should not be usedbecause of natural resistance of B anthracis strainsto these antibiotics
Bacterial toxins have long been felt to play a ma-jor role in anthrax meningoencephalitis becausemany effects of B anthracis cannot be attributed tomicroscopically evident tissue changes1075 Virulenceof B anthracis requires an antiphagocytic capsuleand two exotoxins The two toxins are binary pro-teins composed of a binding protein and an enzymat-ically active protein2476 Among other actions thesetoxins collectively produce local edema impair neu-trophil function depress cerebral cortical electricalactivity depress central respiratory center activitycause bleeding and destruction of the brain and vitalorgans in the chest and induce cardiovascular col-lapse and shock244476-79
Although antitoxin was used early in the 20thcentury to treat anthrax alone or in combinationwith penicillin13-15 it has not been available in recentdecades to US civilian populations Conceptually an-tianthrax serum may augment the effect of antibiot-ics by helping to neutralize the anthrax toxinswhich are not inactivated by antibiotics Howeverthere are no documented cases of successful treat-ment of anthrax meningitis with antianthrax serumalone Haight incorrectly stated that a case reported
by Czyhlarz in 191670 had been cured by treatmentwith antianthrax serum when in fact a full transla-tion indicates that the patient received no treatment(Bernd Remler MD personal communication Feb-ruary 2002 see supplementary document) this er-ror has been promulgated by numerous subsequentauthors and has been a source of incorrect conclu-sions regarding potentially effective therapy for an-thrax meningoencephalitis in recent reviewsCzyhlarz70 also presented unpublished second-handinformation on another patient who purportedly re-covered from anthrax meningoencephalitis withouttreatment In light of subsequent experience withthis disease it is hard to interpret or credit either ofthese reports Available experimental data80 do notindicate a significant treatment effect of antianthraxserum beyond that of penicillin Nevertheless anti-anthrax immune globulin derived from the blood ofsoldiers who have received the anthrax vaccine isbeing added to the US bioterrorism treatment stock-pile and is being considered as a potential experi-mental anthrax treatment in the event of furtherbioterrorism anthrax cases681
Corticosteroids have been recommended as an ad-junctive agent in the treatment of meningitis in chil-dren82 Use of corticosteroids in adults withmeningitis is controversial but steroids have beenrecommended for consideration as adjunctive agentswithout any age restriction in anthrax meningitis72
If corticosteroids are used in conjunction with vanco-mycin therapy antibiotic dosing may need to bemodified because CSF vancomycin levels may be de-creased by corticosteroids contributing to treatmentfailure82-86
In addition to antibiotic management patientswith anthrax meningoencephalitis may require ag-gressive intensive care measures Seizures in-creased intracranial pressure subarachnoid andintracerebral hemorrhage electrolyte disturbanceshypotension shock and disseminated intravascularcoagulation may develop as complications of this in-fection Despite aggressive treatment the prognosisfor survival with anthrax meningoencephalitis isvery poor
AcknowledgmentThe author thanks Glen Salter MS of the Tomah VA MedicalCenter Library for assistance in locating references Pat Mennickeof the Tomah VA Medical Center for assistance with Excel spread-sheets Bernd Remler MD of the Medical College of WisconsinMilwaukee for translating the paper by Czyhlarz Larry DavisMD of the Albuquerque VA Medical Center for helpful correspon-dence regarding corticosteroids and vancomycin Jeffrey M JonesMD PhD of the William S Middleton VA Medical Center Madi-son for helpful discussions regarding antibiotic treatment of an-thrax meningoencephalitis and Mary Jo Lanska MD MS of theTomah VA Medical Center for helpful discussions and for criti-cally reviewing the manuscript
References1 Haight TH Anthrax meningitis review of literature and report
of two cases with autopsies Am J Med Sci 195222457ndash692 Dixon TC Meselson M Guillemin J Hanna PC Anthrax
N Engl J Med 1999341815ndash826
332 NEUROLOGY 59 August (1 of 2) 2002
3 Inglesby TV Henderson DA Bartlett JG et al Anthrax as abiological weapon medical and public health managementJAMA 19992811735ndash1745
4 Swartz MN Recognition and management of anthrax an up-date N Engl J Med 20013451621ndash1626
5 Jernigan JA Stephens DS Ashford DA et al Bioterrorism-related inhalational anthrax the first 10 cases reported in theUnited States Emerg Infect Dis 20017933ndash944
6 Inglesby TV OrsquoToole T Henderson DA et al Anthrax as abiological weapon 2002 updated recommendations for man-agement JAMA 20022872236ndash2252
7 Miller JK Human anthrax in New York State NY StateJ Med 1961612046ndash2053
8 Brachman PS Human anthrax in the United States Antimi-crob Agents Chemother 19655111ndash114
9 Kumar A Kanungo R Bhattacharya S Badrinath S DuttaTK Swaminathan RP Human anthrax in India urgent needfor effective prevention J Commun Dis 200032240ndash246
10 Dutz W Kohout E Anthrax Pathol Annu 197162009ndash224811 Trivedy JR Case of anthrax meningitis survival Cent Afr
J Med 19812716612 Roberts CJ Chambers PG An outbreak of anthrax in the
Mondoro Tribal Trust lands Cent Afr J Med 19752173ndash7613 Kindler D Recovery from anthrax meningitis Ind Med Surg
195221487ndash48814 Shanahan RH Griffin JR Von Auersperg AP Anthrax men-
ingitis report of a case of internal anthrax with recoveryAm J Clin Pathol 194717719ndash722
15 Griffin JR Shanahan RH DeAngelis CE Treatment of cuta-neous anthrax with penicillin NY State J Med 1948481718ndash1721
16 Boudin G Lauras A Vaillant C Etat de mal eacutepileptiquereacuteveacutelateur drsquoune meacuteningite charbonneuse etude anatamo-clinique Bull Mem Soc Med Hop Paris 1964115183ndash187
17 Rapun Pac JL Ull Laita M Meningitis carbuncosa Arch Neu-robiol (Madr) 197235143ndash148
18 Baltiev A Besleaga E Cuciureanu G Obreja E Meningo-encefalita carbunoasa la un copil cu pustula cutanata necarac-teristica Rev Med Chir Soc Med Nat Iasi 197377885ndash888
19 Beer K Milzbrandmeningitis Path Microbiol 19733912ndash1320 Bach I Simon L Baacuten E Toacuteth L Kovaacutecs M Haemorrhagiaacutes
meningitises apoplexia anthrax sepsisben Orv Hetil 19781191797ndash1799
21 Marandian MH Kamali A Meacuteningite charbonneuse un casen apparence primitif Nouv Presse Med 1981101747ndash1748
22 Duumlrst UN Bartenstein J Buumlhlmann H Wuumlst J Spiegel MVAnthraxmeningitis Schweiz Med Wochenschr 19861161222ndash1228
23 Gonzalez A Rodriguez E Castillo M Ortega I Ramirez EFajardo J Lesioacuten necroacutetica en mentoacuten en paciente con siacuten-drome meniacutengeo Enferm Infecc Mircobiol Clin 199715163ndash164
24 Abramova AA Grinberg LM [Pathology of anthrax sepsisaccording to materials of the infectious outbreak in 1979 inSverdlovsk (macroscopic changes)] Arkh Patol 19935512ndash17
25 Abramova AA Grinberg LM [Pathology of anthrax sepsisaccording to materials of infectious outbreak in 1979 in Sverd-lovsk (microscopic changes)] Arkh Patol 19935518ndash23
26 Grinberg LM Abramova AA [Pathology of anthrax sepsisaccording to materials of the infectious outbreak in 1979 inSverdlovsk (various aspects of morpho- patho- and thanato-genesis] Arkh Patol 19935523ndash26
27 Weinstein L Oliver CS The treatment of human anthraxwith penicillin Am Pract 19482533ndash538
28 Raper AB Anthrax meningo-encephalitis East Afr Med J195330399-401
29 Albrink WS Brooks SM Biron RE Kopel M Human inhala-tional anthrax a report of three fatal cases Am J Pathol196036457ndash468
30 Plotkin SA Brachman PS Utell M Bumford FH AtchisonMM An epidemic of inhalation anthrax the first in the twen-tieth century I Clinical features Am J Med 196029992ndash1001
31 Brachman PS Pagano JS Albrink WS Two cases of fatalinhalation anthrax one associated with sarcoidosis N EnglJ Med 1961265203ndash208
32 Brachman PS Inhalation anthrax Ann NY Acad Sci 198035383ndash93
33 Vita A Secu A Cuciureanu G Leibovici M Bejanariu C CujuG Considerations on 3 cases of meningo-encephalitis due toanthrax bacilli Rom Med Rev 1961536ndash39
34 LaForce FM Bumford FH Freely JC Stokes SL Snow DBEpidemiologic study of a fatal case of inhalation anthrax ArchEnviron Health 196918798ndash805
35 Rangel RA Gonzaacutelez DA Bacillus anthracis meningitis Neu-rology 197525525ndash530
36 Tahernia AC Hashemi G Survival in anthrax meningitisPediatrics 197250329ndash333
37 Tengio FU Anthrax meningitis report of two cases East AfrMed J 197350337ndash339
38 Viratchai C Anthrax gastro-enteritis and meningitis J MedAssoc Thai 197457147ndash150
39 Pluot M Vital C Aubertin J Croix JC Pire JC Poisot DAnthrax meningitis report of two cases with autopsies ActaNeuropathol (Berl) 197636339ndash345
40 Suffin SC Carnes WH Kaufman AF Inhalation anthrax in ahome craftsman Hum Pathol 19789594ndash597
41 Al-Dulaimy SB Al-Allaf GA Anthrax meningitis Trans R SocTrop Med Hyg 197872315
42 Manios S Kavaliotis I Anthrax in children a long forgottenpotentially fatal condition Scand J Infect Dis 197911203ndash206
43 Koshi G Lalitha MK Daniel J Chacko A Pulimood BMAnthrax meningitis a rare clinical entity J Assoc PhysiciansIndia 19812959ndash62
44 Abramova FA Grinberg LM Tampolskaya OV Walker DHPathology of inhalational anthrax in 42 cases from the Sverd-lovsk outbreak of 1979 Proc Natl Acad Sci USA 1993902291ndash2294
45 Levy L Baker N Meyer MP Crosland P Hampton J Anthraxmeningitis in Zimbabwe Cent Afr J Med 198127101ndash104
46 Bhat P Pereira P Mohan N Primary anthrax meningitis acase report Neurol India 19833171ndash73
47 Chandramukhi A Shankar P Rao TV Sundararajan SSwamy HS Acute leptomeningitis due to Bacillus anthracis acase report Trop Geogr Med 19833579ndash82
48 Khanna N Gokul BN Ravikumar R et al Successfullytreated primary anthrax meningitis Indian J Pathol Micro-biol 198932315ndash317
49 Kanungo R Sujatha S Das AK Rao RS Anthrax meningitisa clinical enigma Indian J Med Microbiol 19906149ndash151
50 Bharathmoorthy Chakravarthy I Swaminathan RP et alHaemorrhagic meningitis due to Bacillus anthrax J AssocPhysicians India 199240134ndash135
51 Tabatabaie P Syadati A Bacillus anthracis as a cause ofbacterial meningitis Pediatr Infect Dis 1993121035ndash1037
52 George S Mathai D Balraj V Lalitha MK John TJ An out-break of anthrax meningoencephalitis Trans R Soc Trop MedHyg 199488206ndash207
53 Berthier M Fauchegravere J-L Perrin J Grignon B Oriot D Ful-minant meningitis due to Bacillus anthracis in 11-year-oldgirl during Ramadan Lancet 1996347828
54 Domiacutenguez E Bustos C Garcia M Recio S Anthrax meningo-encephalitis radiologic findings AJR Am J Roentgenol 1997169317
55 Kwong KL Que TL Wong SN So KT Fatal meningoenceph-alitis due to Bacillus anthracis J Paediatr Child Health 199733539ndash541
56 Garcia AG Jiminez RR Bacillus anthracis meningitis N EnglJ Med 1999341814
57 Ringertz SH Hoiby EA Jensenius M et al Injectional an-thrax in a heroin skin-popper Lancet 20003461574ndash1575
58 Kim HJ Jun WB Lee SH Rho MH CT and MR findings ofanthrax meningoencephalitis report of two cases and reviewof the literature AJNR Am J Neuroradiol 2001221303ndash1305
59 Bush LM Abrams BH Heall A Johnson CC Index case offatal inhalational anthrax due to bioterrorism in the UnitedStates N Engl J Med 20013451607ndash1610
60 Brachman PS Plotkin SA Bumford FH Atchison MM Anepidemic of inhalation anthrax the first in the twentieth cen-tury II Epidemiology Am J Hygiene 1960726ndash23
61 Belluck P Anthrax outbreak of rsquo57 felled a mill but yieldedanswers New York Times October 27 2001B8
62 Meselson M Guillemin J Hugh-Jones M et al The Sverd-lovsk anthrax outbreak of 1979 Science 19942661202ndash1208
August (1 of 2) 2002 NEUROLOGY 59 333
63 Jackson PJ Hugh-Jones ME Adair DM et al PCR analysis oftissue samples from the 1979 Sverdlovsk anthrax victims thepresence of multiple Bacillus anthracis strains in differentvictims Proc Natl Acad Sci USA 1998951224ndash1229
64 Grinberg LM Abramova FA Yampolskaya OV Walker DHSmith JH Quantitative pathology of inhalational anthrax IQuantitative microscopic findings Mod Pathol 200114482ndash495
65 Brookmeyer R Blades N Hugh-Jones M Henderson D Thestatistical analysis of truncated data application to the Sverd-lovsk anthrax outbreak Biostatistics 20012233ndash247
66 Knott FA A note on anthrax infection by shaving brushesLancet 19231227ndash228
67 Bradaric N Punda-Polic V Cutaneous anthrax due topenicillin-resistant Bacillus anthracis transmitted by an in-sect bite Lancet 1992340306ndash307
68 Turell MJ Knudson GB Mechanical transmission of Bacillusanthracis by stable flies (Stomoxys calcitrans) and mosquitoes(Aedes aegypti and Aedes taeniorhynchus) Infect Immun1987551859ndash1861
69 Drake DJ Meningitic anthrax Cent Afr J Med 19711797ndash9870 Czyhlarz EV Beitrag zur Lehre von der Milzbrandmeningitis
Wein Klin Wochenscr 191629768ndash76971 Centers for Disease Control Investigation of anthrax associ-
ated with intentional exposure and interim public healthguidelines October 2001 MMWR Morb Mortal Wkly Rep200150889ndash893
72 Centers for Disease Control Update investigation ofbioterrorism-related anthrax and interim guidelines for expo-sure management and antimicrobial therapy October 2001MMWR Morb Mortal Wkly Rep 200150909ndash919
73 Centers for Disease Control Investigation of bioterrorism-related anthrax and interim guidelines for clinical evaluationof persons with possible anthrax MMWR Morb Mortal WklyRep 200150941ndash948
74 Centers for Disease Control Updated recommendations forantimicrobial prophylaxis among asymptomatic pregnantwomen after exposure to Bacillus anthracis MMWR MorbMortal Wkly Rep 200150960
75 Bonventure PF Sueoka W True CW Klein F Lincoln RAttempts to implicate the central nervous system as a pri-
mary site of action for Bacillus anthracis lethal toxin FedProc 1967261549ndash1553
76 Friedlander AM Anthrax In Sidell FR Takafuji ET FranzDR eds Textbook of military medicine medical aspects ofchemical and biological warfare Washington DC Office ofthe Surgeon General 1997467ndash478
77 Vick JA Lincoln RE Klein F Mahlandt BG Walker JS FishDC Neurological and physiological responses of the primateto anthrax toxin J Infect Dis 196811885ndash96
78 Klein F Lincoln RE Dobbs JP Mahlandt BG Remmele NSWalker JS Neurological and physiological responses of theprimate to anthrax infection J Infect Dis 196811897ndash103
79 Remmele NS Klein F Vick JA Walker JS Mahlandt BGLincoln RE Anthrax toxin primary site of action J Infect Dis1968118104ndash113
80 Doganay M Hanagasi R Zora A [Evaluation of penicillinalone and penicillin combined with anti-anthrax serum in ex-perimental anthrax in mice] Mikrobiyol Bul 19851957ndash64
81 Associated Press Government may offer anthrax treatmentNew York Times January 7 2002
82 Davis LE Acute bacterial meningitis In Johnson RT GriffinJW eds Current therapy in neurologic disease 5th ed StLouis Mosby 1997120ndash127
83 Viladrich PF Gudiol F Lintildeares J et al Evaluation of vanco-mycin for therapy of adult pneumococcal meningitis Antimi-crob Agents Chemother 1991352467ndash2472
84 Pariacutes M Hickey SM Uscher MI Shelton S Olsen KD Mc-Cracken GH Jr Effect of dexamethasone on therapy of exper-imental penicillin- and cephalosporin-resistant pneumococcalmeningitis Antimicrob Agents Chemother 1994381320ndash1324
85 Cabellos C Martinez-Lacasa J Martos A et al Influence ofdexamethasone on efficacy of ceftriaxone and vancomycintherapy in experimental pneumococcal meningitis AntimicrobAgents Chemother 1995392158ndash2160
86 Ahmed A Jafri H Lutsar I et al Pharmacodynamics of van-comycin for the treatment of experimental penicillin- andcephalosporin-resistant pneumococcal meningitis AntimicrobAgents Chemother 199943876ndash881
334 NEUROLOGY 59 August (1 of 2) 2002
DOI 101212WNL593327200259327-334 Neurology
Douglas J LanskaAnthrax meningoencephalitis
This information is current as of August 13 2002
ServicesUpdated Information amp
httpwwwneurologyorgcontent593327fullhtmlincluding high resolution figures can be found at
Supplementary Material
htmlhttpwwwneurologyorgneurologysuppl20020716593327DC2
htmlhttpwwwneurologyorgneurologysuppl20020716593327DC1Supplementary material can be found at
References httpwwwneurologyorgcontent593327fullhtmlref-list-1
This article cites 73 articles 15 of which you can access for free at
Citations httpwwwneurologyorgcontent593327fullhtmlotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpwwwneurologyorgcgicollectionmeningitisMeningitis
httpwwwneurologyorgcgicollectionencephalitisEncephalitis
httpwwwneurologyorgcgicollectionbacterial_infectionsBacterial infections
httpwwwneurologyorgcgicollectionall_infectionsAll Infectionsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsin its entirety can be found online atInformation about reproducing this article in parts (figurestables) or
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

brain was not examined in some autopsies Based onprevious experience44 the potential exists for largenumbers of cases of anthrax meningoencephalitiswith further bioterrorist outbreaks or bioweaponsdispersals Meningoencephalitis may also occur withgastrointestinal anthrax or without a clinically ap-parent primary focus
Current guidelines from the Centers for DiseaseControl indicate that ciprofloxacin or doxycyclineshould be included as essential components of initialtherapy for anthrax infections of any portal of en-try7274 It is important to treat anthrax meningoen-cephalitis with a polydrug antibiotic regimen usingantimicrobial agents that have good CSF penetrationin meningitis and that provide good antibacterialcoverage for B anthracis All six patients who sur-vived after antibiotic treatment for anthrax menin-goencephalitis were treated with penicillinHowever because of the presence of constitutive orinducible beta-lactamases in B anthracis isolatesfrom the recent US bioterrorist outbreak and expec-tations that beta-lactamase activity may be likelywith bioengineered bioweapons agents ampicillin orpenicillin G alone are not recommended for initialtherapy for anthrax meningoencephalitis prior to an-tibiotic sensitivity results from culture7274 Rifampinplus vancomycin would be a reasonable choice foraddition to ciprofloxacin or doxycycline in the initialtreatment of anthrax meningoencephalitis Some in-fectious disease authorities recommend ciprofloxacinin preference to doxycycline plus augmentation withchloramphenicol rifampin or penicillin for estab-lished or suspected anthrax meningoencephalitis6
Aztreonam trimethoprim-sulfamethoxazole orthird-generation cephalosporins should not be usedbecause of natural resistance of B anthracis strainsto these antibiotics
Bacterial toxins have long been felt to play a ma-jor role in anthrax meningoencephalitis becausemany effects of B anthracis cannot be attributed tomicroscopically evident tissue changes1075 Virulenceof B anthracis requires an antiphagocytic capsuleand two exotoxins The two toxins are binary pro-teins composed of a binding protein and an enzymat-ically active protein2476 Among other actions thesetoxins collectively produce local edema impair neu-trophil function depress cerebral cortical electricalactivity depress central respiratory center activitycause bleeding and destruction of the brain and vitalorgans in the chest and induce cardiovascular col-lapse and shock244476-79
Although antitoxin was used early in the 20thcentury to treat anthrax alone or in combinationwith penicillin13-15 it has not been available in recentdecades to US civilian populations Conceptually an-tianthrax serum may augment the effect of antibiot-ics by helping to neutralize the anthrax toxinswhich are not inactivated by antibiotics Howeverthere are no documented cases of successful treat-ment of anthrax meningitis with antianthrax serumalone Haight incorrectly stated that a case reported
by Czyhlarz in 191670 had been cured by treatmentwith antianthrax serum when in fact a full transla-tion indicates that the patient received no treatment(Bernd Remler MD personal communication Feb-ruary 2002 see supplementary document) this er-ror has been promulgated by numerous subsequentauthors and has been a source of incorrect conclu-sions regarding potentially effective therapy for an-thrax meningoencephalitis in recent reviewsCzyhlarz70 also presented unpublished second-handinformation on another patient who purportedly re-covered from anthrax meningoencephalitis withouttreatment In light of subsequent experience withthis disease it is hard to interpret or credit either ofthese reports Available experimental data80 do notindicate a significant treatment effect of antianthraxserum beyond that of penicillin Nevertheless anti-anthrax immune globulin derived from the blood ofsoldiers who have received the anthrax vaccine isbeing added to the US bioterrorism treatment stock-pile and is being considered as a potential experi-mental anthrax treatment in the event of furtherbioterrorism anthrax cases681
Corticosteroids have been recommended as an ad-junctive agent in the treatment of meningitis in chil-dren82 Use of corticosteroids in adults withmeningitis is controversial but steroids have beenrecommended for consideration as adjunctive agentswithout any age restriction in anthrax meningitis72
If corticosteroids are used in conjunction with vanco-mycin therapy antibiotic dosing may need to bemodified because CSF vancomycin levels may be de-creased by corticosteroids contributing to treatmentfailure82-86
In addition to antibiotic management patientswith anthrax meningoencephalitis may require ag-gressive intensive care measures Seizures in-creased intracranial pressure subarachnoid andintracerebral hemorrhage electrolyte disturbanceshypotension shock and disseminated intravascularcoagulation may develop as complications of this in-fection Despite aggressive treatment the prognosisfor survival with anthrax meningoencephalitis isvery poor
AcknowledgmentThe author thanks Glen Salter MS of the Tomah VA MedicalCenter Library for assistance in locating references Pat Mennickeof the Tomah VA Medical Center for assistance with Excel spread-sheets Bernd Remler MD of the Medical College of WisconsinMilwaukee for translating the paper by Czyhlarz Larry DavisMD of the Albuquerque VA Medical Center for helpful correspon-dence regarding corticosteroids and vancomycin Jeffrey M JonesMD PhD of the William S Middleton VA Medical Center Madi-son for helpful discussions regarding antibiotic treatment of an-thrax meningoencephalitis and Mary Jo Lanska MD MS of theTomah VA Medical Center for helpful discussions and for criti-cally reviewing the manuscript
References1 Haight TH Anthrax meningitis review of literature and report
of two cases with autopsies Am J Med Sci 195222457ndash692 Dixon TC Meselson M Guillemin J Hanna PC Anthrax
N Engl J Med 1999341815ndash826
332 NEUROLOGY 59 August (1 of 2) 2002
3 Inglesby TV Henderson DA Bartlett JG et al Anthrax as abiological weapon medical and public health managementJAMA 19992811735ndash1745
4 Swartz MN Recognition and management of anthrax an up-date N Engl J Med 20013451621ndash1626
5 Jernigan JA Stephens DS Ashford DA et al Bioterrorism-related inhalational anthrax the first 10 cases reported in theUnited States Emerg Infect Dis 20017933ndash944
6 Inglesby TV OrsquoToole T Henderson DA et al Anthrax as abiological weapon 2002 updated recommendations for man-agement JAMA 20022872236ndash2252
7 Miller JK Human anthrax in New York State NY StateJ Med 1961612046ndash2053
8 Brachman PS Human anthrax in the United States Antimi-crob Agents Chemother 19655111ndash114
9 Kumar A Kanungo R Bhattacharya S Badrinath S DuttaTK Swaminathan RP Human anthrax in India urgent needfor effective prevention J Commun Dis 200032240ndash246
10 Dutz W Kohout E Anthrax Pathol Annu 197162009ndash224811 Trivedy JR Case of anthrax meningitis survival Cent Afr
J Med 19812716612 Roberts CJ Chambers PG An outbreak of anthrax in the
Mondoro Tribal Trust lands Cent Afr J Med 19752173ndash7613 Kindler D Recovery from anthrax meningitis Ind Med Surg
195221487ndash48814 Shanahan RH Griffin JR Von Auersperg AP Anthrax men-
ingitis report of a case of internal anthrax with recoveryAm J Clin Pathol 194717719ndash722
15 Griffin JR Shanahan RH DeAngelis CE Treatment of cuta-neous anthrax with penicillin NY State J Med 1948481718ndash1721
16 Boudin G Lauras A Vaillant C Etat de mal eacutepileptiquereacuteveacutelateur drsquoune meacuteningite charbonneuse etude anatamo-clinique Bull Mem Soc Med Hop Paris 1964115183ndash187
17 Rapun Pac JL Ull Laita M Meningitis carbuncosa Arch Neu-robiol (Madr) 197235143ndash148
18 Baltiev A Besleaga E Cuciureanu G Obreja E Meningo-encefalita carbunoasa la un copil cu pustula cutanata necarac-teristica Rev Med Chir Soc Med Nat Iasi 197377885ndash888
19 Beer K Milzbrandmeningitis Path Microbiol 19733912ndash1320 Bach I Simon L Baacuten E Toacuteth L Kovaacutecs M Haemorrhagiaacutes
meningitises apoplexia anthrax sepsisben Orv Hetil 19781191797ndash1799
21 Marandian MH Kamali A Meacuteningite charbonneuse un casen apparence primitif Nouv Presse Med 1981101747ndash1748
22 Duumlrst UN Bartenstein J Buumlhlmann H Wuumlst J Spiegel MVAnthraxmeningitis Schweiz Med Wochenschr 19861161222ndash1228
23 Gonzalez A Rodriguez E Castillo M Ortega I Ramirez EFajardo J Lesioacuten necroacutetica en mentoacuten en paciente con siacuten-drome meniacutengeo Enferm Infecc Mircobiol Clin 199715163ndash164
24 Abramova AA Grinberg LM [Pathology of anthrax sepsisaccording to materials of the infectious outbreak in 1979 inSverdlovsk (macroscopic changes)] Arkh Patol 19935512ndash17
25 Abramova AA Grinberg LM [Pathology of anthrax sepsisaccording to materials of infectious outbreak in 1979 in Sverd-lovsk (microscopic changes)] Arkh Patol 19935518ndash23
26 Grinberg LM Abramova AA [Pathology of anthrax sepsisaccording to materials of the infectious outbreak in 1979 inSverdlovsk (various aspects of morpho- patho- and thanato-genesis] Arkh Patol 19935523ndash26
27 Weinstein L Oliver CS The treatment of human anthraxwith penicillin Am Pract 19482533ndash538
28 Raper AB Anthrax meningo-encephalitis East Afr Med J195330399-401
29 Albrink WS Brooks SM Biron RE Kopel M Human inhala-tional anthrax a report of three fatal cases Am J Pathol196036457ndash468
30 Plotkin SA Brachman PS Utell M Bumford FH AtchisonMM An epidemic of inhalation anthrax the first in the twen-tieth century I Clinical features Am J Med 196029992ndash1001
31 Brachman PS Pagano JS Albrink WS Two cases of fatalinhalation anthrax one associated with sarcoidosis N EnglJ Med 1961265203ndash208
32 Brachman PS Inhalation anthrax Ann NY Acad Sci 198035383ndash93
33 Vita A Secu A Cuciureanu G Leibovici M Bejanariu C CujuG Considerations on 3 cases of meningo-encephalitis due toanthrax bacilli Rom Med Rev 1961536ndash39
34 LaForce FM Bumford FH Freely JC Stokes SL Snow DBEpidemiologic study of a fatal case of inhalation anthrax ArchEnviron Health 196918798ndash805
35 Rangel RA Gonzaacutelez DA Bacillus anthracis meningitis Neu-rology 197525525ndash530
36 Tahernia AC Hashemi G Survival in anthrax meningitisPediatrics 197250329ndash333
37 Tengio FU Anthrax meningitis report of two cases East AfrMed J 197350337ndash339
38 Viratchai C Anthrax gastro-enteritis and meningitis J MedAssoc Thai 197457147ndash150
39 Pluot M Vital C Aubertin J Croix JC Pire JC Poisot DAnthrax meningitis report of two cases with autopsies ActaNeuropathol (Berl) 197636339ndash345
40 Suffin SC Carnes WH Kaufman AF Inhalation anthrax in ahome craftsman Hum Pathol 19789594ndash597
41 Al-Dulaimy SB Al-Allaf GA Anthrax meningitis Trans R SocTrop Med Hyg 197872315
42 Manios S Kavaliotis I Anthrax in children a long forgottenpotentially fatal condition Scand J Infect Dis 197911203ndash206
43 Koshi G Lalitha MK Daniel J Chacko A Pulimood BMAnthrax meningitis a rare clinical entity J Assoc PhysiciansIndia 19812959ndash62
44 Abramova FA Grinberg LM Tampolskaya OV Walker DHPathology of inhalational anthrax in 42 cases from the Sverd-lovsk outbreak of 1979 Proc Natl Acad Sci USA 1993902291ndash2294
45 Levy L Baker N Meyer MP Crosland P Hampton J Anthraxmeningitis in Zimbabwe Cent Afr J Med 198127101ndash104
46 Bhat P Pereira P Mohan N Primary anthrax meningitis acase report Neurol India 19833171ndash73
47 Chandramukhi A Shankar P Rao TV Sundararajan SSwamy HS Acute leptomeningitis due to Bacillus anthracis acase report Trop Geogr Med 19833579ndash82
48 Khanna N Gokul BN Ravikumar R et al Successfullytreated primary anthrax meningitis Indian J Pathol Micro-biol 198932315ndash317
49 Kanungo R Sujatha S Das AK Rao RS Anthrax meningitisa clinical enigma Indian J Med Microbiol 19906149ndash151
50 Bharathmoorthy Chakravarthy I Swaminathan RP et alHaemorrhagic meningitis due to Bacillus anthrax J AssocPhysicians India 199240134ndash135
51 Tabatabaie P Syadati A Bacillus anthracis as a cause ofbacterial meningitis Pediatr Infect Dis 1993121035ndash1037
52 George S Mathai D Balraj V Lalitha MK John TJ An out-break of anthrax meningoencephalitis Trans R Soc Trop MedHyg 199488206ndash207
53 Berthier M Fauchegravere J-L Perrin J Grignon B Oriot D Ful-minant meningitis due to Bacillus anthracis in 11-year-oldgirl during Ramadan Lancet 1996347828
54 Domiacutenguez E Bustos C Garcia M Recio S Anthrax meningo-encephalitis radiologic findings AJR Am J Roentgenol 1997169317
55 Kwong KL Que TL Wong SN So KT Fatal meningoenceph-alitis due to Bacillus anthracis J Paediatr Child Health 199733539ndash541
56 Garcia AG Jiminez RR Bacillus anthracis meningitis N EnglJ Med 1999341814
57 Ringertz SH Hoiby EA Jensenius M et al Injectional an-thrax in a heroin skin-popper Lancet 20003461574ndash1575
58 Kim HJ Jun WB Lee SH Rho MH CT and MR findings ofanthrax meningoencephalitis report of two cases and reviewof the literature AJNR Am J Neuroradiol 2001221303ndash1305
59 Bush LM Abrams BH Heall A Johnson CC Index case offatal inhalational anthrax due to bioterrorism in the UnitedStates N Engl J Med 20013451607ndash1610
60 Brachman PS Plotkin SA Bumford FH Atchison MM Anepidemic of inhalation anthrax the first in the twentieth cen-tury II Epidemiology Am J Hygiene 1960726ndash23
61 Belluck P Anthrax outbreak of rsquo57 felled a mill but yieldedanswers New York Times October 27 2001B8
62 Meselson M Guillemin J Hugh-Jones M et al The Sverd-lovsk anthrax outbreak of 1979 Science 19942661202ndash1208
August (1 of 2) 2002 NEUROLOGY 59 333
63 Jackson PJ Hugh-Jones ME Adair DM et al PCR analysis oftissue samples from the 1979 Sverdlovsk anthrax victims thepresence of multiple Bacillus anthracis strains in differentvictims Proc Natl Acad Sci USA 1998951224ndash1229
64 Grinberg LM Abramova FA Yampolskaya OV Walker DHSmith JH Quantitative pathology of inhalational anthrax IQuantitative microscopic findings Mod Pathol 200114482ndash495
65 Brookmeyer R Blades N Hugh-Jones M Henderson D Thestatistical analysis of truncated data application to the Sverd-lovsk anthrax outbreak Biostatistics 20012233ndash247
66 Knott FA A note on anthrax infection by shaving brushesLancet 19231227ndash228
67 Bradaric N Punda-Polic V Cutaneous anthrax due topenicillin-resistant Bacillus anthracis transmitted by an in-sect bite Lancet 1992340306ndash307
68 Turell MJ Knudson GB Mechanical transmission of Bacillusanthracis by stable flies (Stomoxys calcitrans) and mosquitoes(Aedes aegypti and Aedes taeniorhynchus) Infect Immun1987551859ndash1861
69 Drake DJ Meningitic anthrax Cent Afr J Med 19711797ndash9870 Czyhlarz EV Beitrag zur Lehre von der Milzbrandmeningitis
Wein Klin Wochenscr 191629768ndash76971 Centers for Disease Control Investigation of anthrax associ-
ated with intentional exposure and interim public healthguidelines October 2001 MMWR Morb Mortal Wkly Rep200150889ndash893
72 Centers for Disease Control Update investigation ofbioterrorism-related anthrax and interim guidelines for expo-sure management and antimicrobial therapy October 2001MMWR Morb Mortal Wkly Rep 200150909ndash919
73 Centers for Disease Control Investigation of bioterrorism-related anthrax and interim guidelines for clinical evaluationof persons with possible anthrax MMWR Morb Mortal WklyRep 200150941ndash948
74 Centers for Disease Control Updated recommendations forantimicrobial prophylaxis among asymptomatic pregnantwomen after exposure to Bacillus anthracis MMWR MorbMortal Wkly Rep 200150960
75 Bonventure PF Sueoka W True CW Klein F Lincoln RAttempts to implicate the central nervous system as a pri-
mary site of action for Bacillus anthracis lethal toxin FedProc 1967261549ndash1553
76 Friedlander AM Anthrax In Sidell FR Takafuji ET FranzDR eds Textbook of military medicine medical aspects ofchemical and biological warfare Washington DC Office ofthe Surgeon General 1997467ndash478
77 Vick JA Lincoln RE Klein F Mahlandt BG Walker JS FishDC Neurological and physiological responses of the primateto anthrax toxin J Infect Dis 196811885ndash96
78 Klein F Lincoln RE Dobbs JP Mahlandt BG Remmele NSWalker JS Neurological and physiological responses of theprimate to anthrax infection J Infect Dis 196811897ndash103
79 Remmele NS Klein F Vick JA Walker JS Mahlandt BGLincoln RE Anthrax toxin primary site of action J Infect Dis1968118104ndash113
80 Doganay M Hanagasi R Zora A [Evaluation of penicillinalone and penicillin combined with anti-anthrax serum in ex-perimental anthrax in mice] Mikrobiyol Bul 19851957ndash64
81 Associated Press Government may offer anthrax treatmentNew York Times January 7 2002
82 Davis LE Acute bacterial meningitis In Johnson RT GriffinJW eds Current therapy in neurologic disease 5th ed StLouis Mosby 1997120ndash127
83 Viladrich PF Gudiol F Lintildeares J et al Evaluation of vanco-mycin for therapy of adult pneumococcal meningitis Antimi-crob Agents Chemother 1991352467ndash2472
84 Pariacutes M Hickey SM Uscher MI Shelton S Olsen KD Mc-Cracken GH Jr Effect of dexamethasone on therapy of exper-imental penicillin- and cephalosporin-resistant pneumococcalmeningitis Antimicrob Agents Chemother 1994381320ndash1324
85 Cabellos C Martinez-Lacasa J Martos A et al Influence ofdexamethasone on efficacy of ceftriaxone and vancomycintherapy in experimental pneumococcal meningitis AntimicrobAgents Chemother 1995392158ndash2160
86 Ahmed A Jafri H Lutsar I et al Pharmacodynamics of van-comycin for the treatment of experimental penicillin- andcephalosporin-resistant pneumococcal meningitis AntimicrobAgents Chemother 199943876ndash881
334 NEUROLOGY 59 August (1 of 2) 2002
DOI 101212WNL593327200259327-334 Neurology
Douglas J LanskaAnthrax meningoencephalitis
This information is current as of August 13 2002
ServicesUpdated Information amp
httpwwwneurologyorgcontent593327fullhtmlincluding high resolution figures can be found at
Supplementary Material
htmlhttpwwwneurologyorgneurologysuppl20020716593327DC2
htmlhttpwwwneurologyorgneurologysuppl20020716593327DC1Supplementary material can be found at
References httpwwwneurologyorgcontent593327fullhtmlref-list-1
This article cites 73 articles 15 of which you can access for free at
Citations httpwwwneurologyorgcontent593327fullhtmlotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpwwwneurologyorgcgicollectionmeningitisMeningitis
httpwwwneurologyorgcgicollectionencephalitisEncephalitis
httpwwwneurologyorgcgicollectionbacterial_infectionsBacterial infections
httpwwwneurologyorgcgicollectionall_infectionsAll Infectionsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsin its entirety can be found online atInformation about reproducing this article in parts (figurestables) or
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

3 Inglesby TV Henderson DA Bartlett JG et al Anthrax as abiological weapon medical and public health managementJAMA 19992811735ndash1745
4 Swartz MN Recognition and management of anthrax an up-date N Engl J Med 20013451621ndash1626
5 Jernigan JA Stephens DS Ashford DA et al Bioterrorism-related inhalational anthrax the first 10 cases reported in theUnited States Emerg Infect Dis 20017933ndash944
6 Inglesby TV OrsquoToole T Henderson DA et al Anthrax as abiological weapon 2002 updated recommendations for man-agement JAMA 20022872236ndash2252
7 Miller JK Human anthrax in New York State NY StateJ Med 1961612046ndash2053
8 Brachman PS Human anthrax in the United States Antimi-crob Agents Chemother 19655111ndash114
9 Kumar A Kanungo R Bhattacharya S Badrinath S DuttaTK Swaminathan RP Human anthrax in India urgent needfor effective prevention J Commun Dis 200032240ndash246
10 Dutz W Kohout E Anthrax Pathol Annu 197162009ndash224811 Trivedy JR Case of anthrax meningitis survival Cent Afr
J Med 19812716612 Roberts CJ Chambers PG An outbreak of anthrax in the
Mondoro Tribal Trust lands Cent Afr J Med 19752173ndash7613 Kindler D Recovery from anthrax meningitis Ind Med Surg
195221487ndash48814 Shanahan RH Griffin JR Von Auersperg AP Anthrax men-
ingitis report of a case of internal anthrax with recoveryAm J Clin Pathol 194717719ndash722
15 Griffin JR Shanahan RH DeAngelis CE Treatment of cuta-neous anthrax with penicillin NY State J Med 1948481718ndash1721
16 Boudin G Lauras A Vaillant C Etat de mal eacutepileptiquereacuteveacutelateur drsquoune meacuteningite charbonneuse etude anatamo-clinique Bull Mem Soc Med Hop Paris 1964115183ndash187
17 Rapun Pac JL Ull Laita M Meningitis carbuncosa Arch Neu-robiol (Madr) 197235143ndash148
18 Baltiev A Besleaga E Cuciureanu G Obreja E Meningo-encefalita carbunoasa la un copil cu pustula cutanata necarac-teristica Rev Med Chir Soc Med Nat Iasi 197377885ndash888
19 Beer K Milzbrandmeningitis Path Microbiol 19733912ndash1320 Bach I Simon L Baacuten E Toacuteth L Kovaacutecs M Haemorrhagiaacutes
meningitises apoplexia anthrax sepsisben Orv Hetil 19781191797ndash1799
21 Marandian MH Kamali A Meacuteningite charbonneuse un casen apparence primitif Nouv Presse Med 1981101747ndash1748
22 Duumlrst UN Bartenstein J Buumlhlmann H Wuumlst J Spiegel MVAnthraxmeningitis Schweiz Med Wochenschr 19861161222ndash1228
23 Gonzalez A Rodriguez E Castillo M Ortega I Ramirez EFajardo J Lesioacuten necroacutetica en mentoacuten en paciente con siacuten-drome meniacutengeo Enferm Infecc Mircobiol Clin 199715163ndash164
24 Abramova AA Grinberg LM [Pathology of anthrax sepsisaccording to materials of the infectious outbreak in 1979 inSverdlovsk (macroscopic changes)] Arkh Patol 19935512ndash17
25 Abramova AA Grinberg LM [Pathology of anthrax sepsisaccording to materials of infectious outbreak in 1979 in Sverd-lovsk (microscopic changes)] Arkh Patol 19935518ndash23
26 Grinberg LM Abramova AA [Pathology of anthrax sepsisaccording to materials of the infectious outbreak in 1979 inSverdlovsk (various aspects of morpho- patho- and thanato-genesis] Arkh Patol 19935523ndash26
27 Weinstein L Oliver CS The treatment of human anthraxwith penicillin Am Pract 19482533ndash538
28 Raper AB Anthrax meningo-encephalitis East Afr Med J195330399-401
29 Albrink WS Brooks SM Biron RE Kopel M Human inhala-tional anthrax a report of three fatal cases Am J Pathol196036457ndash468
30 Plotkin SA Brachman PS Utell M Bumford FH AtchisonMM An epidemic of inhalation anthrax the first in the twen-tieth century I Clinical features Am J Med 196029992ndash1001
31 Brachman PS Pagano JS Albrink WS Two cases of fatalinhalation anthrax one associated with sarcoidosis N EnglJ Med 1961265203ndash208
32 Brachman PS Inhalation anthrax Ann NY Acad Sci 198035383ndash93
33 Vita A Secu A Cuciureanu G Leibovici M Bejanariu C CujuG Considerations on 3 cases of meningo-encephalitis due toanthrax bacilli Rom Med Rev 1961536ndash39
34 LaForce FM Bumford FH Freely JC Stokes SL Snow DBEpidemiologic study of a fatal case of inhalation anthrax ArchEnviron Health 196918798ndash805
35 Rangel RA Gonzaacutelez DA Bacillus anthracis meningitis Neu-rology 197525525ndash530
36 Tahernia AC Hashemi G Survival in anthrax meningitisPediatrics 197250329ndash333
37 Tengio FU Anthrax meningitis report of two cases East AfrMed J 197350337ndash339
38 Viratchai C Anthrax gastro-enteritis and meningitis J MedAssoc Thai 197457147ndash150
39 Pluot M Vital C Aubertin J Croix JC Pire JC Poisot DAnthrax meningitis report of two cases with autopsies ActaNeuropathol (Berl) 197636339ndash345
40 Suffin SC Carnes WH Kaufman AF Inhalation anthrax in ahome craftsman Hum Pathol 19789594ndash597
41 Al-Dulaimy SB Al-Allaf GA Anthrax meningitis Trans R SocTrop Med Hyg 197872315
42 Manios S Kavaliotis I Anthrax in children a long forgottenpotentially fatal condition Scand J Infect Dis 197911203ndash206
43 Koshi G Lalitha MK Daniel J Chacko A Pulimood BMAnthrax meningitis a rare clinical entity J Assoc PhysiciansIndia 19812959ndash62
44 Abramova FA Grinberg LM Tampolskaya OV Walker DHPathology of inhalational anthrax in 42 cases from the Sverd-lovsk outbreak of 1979 Proc Natl Acad Sci USA 1993902291ndash2294
45 Levy L Baker N Meyer MP Crosland P Hampton J Anthraxmeningitis in Zimbabwe Cent Afr J Med 198127101ndash104
46 Bhat P Pereira P Mohan N Primary anthrax meningitis acase report Neurol India 19833171ndash73
47 Chandramukhi A Shankar P Rao TV Sundararajan SSwamy HS Acute leptomeningitis due to Bacillus anthracis acase report Trop Geogr Med 19833579ndash82
48 Khanna N Gokul BN Ravikumar R et al Successfullytreated primary anthrax meningitis Indian J Pathol Micro-biol 198932315ndash317
49 Kanungo R Sujatha S Das AK Rao RS Anthrax meningitisa clinical enigma Indian J Med Microbiol 19906149ndash151
50 Bharathmoorthy Chakravarthy I Swaminathan RP et alHaemorrhagic meningitis due to Bacillus anthrax J AssocPhysicians India 199240134ndash135
51 Tabatabaie P Syadati A Bacillus anthracis as a cause ofbacterial meningitis Pediatr Infect Dis 1993121035ndash1037
52 George S Mathai D Balraj V Lalitha MK John TJ An out-break of anthrax meningoencephalitis Trans R Soc Trop MedHyg 199488206ndash207
53 Berthier M Fauchegravere J-L Perrin J Grignon B Oriot D Ful-minant meningitis due to Bacillus anthracis in 11-year-oldgirl during Ramadan Lancet 1996347828
54 Domiacutenguez E Bustos C Garcia M Recio S Anthrax meningo-encephalitis radiologic findings AJR Am J Roentgenol 1997169317
55 Kwong KL Que TL Wong SN So KT Fatal meningoenceph-alitis due to Bacillus anthracis J Paediatr Child Health 199733539ndash541
56 Garcia AG Jiminez RR Bacillus anthracis meningitis N EnglJ Med 1999341814
57 Ringertz SH Hoiby EA Jensenius M et al Injectional an-thrax in a heroin skin-popper Lancet 20003461574ndash1575
58 Kim HJ Jun WB Lee SH Rho MH CT and MR findings ofanthrax meningoencephalitis report of two cases and reviewof the literature AJNR Am J Neuroradiol 2001221303ndash1305
59 Bush LM Abrams BH Heall A Johnson CC Index case offatal inhalational anthrax due to bioterrorism in the UnitedStates N Engl J Med 20013451607ndash1610
60 Brachman PS Plotkin SA Bumford FH Atchison MM Anepidemic of inhalation anthrax the first in the twentieth cen-tury II Epidemiology Am J Hygiene 1960726ndash23
61 Belluck P Anthrax outbreak of rsquo57 felled a mill but yieldedanswers New York Times October 27 2001B8
62 Meselson M Guillemin J Hugh-Jones M et al The Sverd-lovsk anthrax outbreak of 1979 Science 19942661202ndash1208
August (1 of 2) 2002 NEUROLOGY 59 333
63 Jackson PJ Hugh-Jones ME Adair DM et al PCR analysis oftissue samples from the 1979 Sverdlovsk anthrax victims thepresence of multiple Bacillus anthracis strains in differentvictims Proc Natl Acad Sci USA 1998951224ndash1229
64 Grinberg LM Abramova FA Yampolskaya OV Walker DHSmith JH Quantitative pathology of inhalational anthrax IQuantitative microscopic findings Mod Pathol 200114482ndash495
65 Brookmeyer R Blades N Hugh-Jones M Henderson D Thestatistical analysis of truncated data application to the Sverd-lovsk anthrax outbreak Biostatistics 20012233ndash247
66 Knott FA A note on anthrax infection by shaving brushesLancet 19231227ndash228
67 Bradaric N Punda-Polic V Cutaneous anthrax due topenicillin-resistant Bacillus anthracis transmitted by an in-sect bite Lancet 1992340306ndash307
68 Turell MJ Knudson GB Mechanical transmission of Bacillusanthracis by stable flies (Stomoxys calcitrans) and mosquitoes(Aedes aegypti and Aedes taeniorhynchus) Infect Immun1987551859ndash1861
69 Drake DJ Meningitic anthrax Cent Afr J Med 19711797ndash9870 Czyhlarz EV Beitrag zur Lehre von der Milzbrandmeningitis
Wein Klin Wochenscr 191629768ndash76971 Centers for Disease Control Investigation of anthrax associ-
ated with intentional exposure and interim public healthguidelines October 2001 MMWR Morb Mortal Wkly Rep200150889ndash893
72 Centers for Disease Control Update investigation ofbioterrorism-related anthrax and interim guidelines for expo-sure management and antimicrobial therapy October 2001MMWR Morb Mortal Wkly Rep 200150909ndash919
73 Centers for Disease Control Investigation of bioterrorism-related anthrax and interim guidelines for clinical evaluationof persons with possible anthrax MMWR Morb Mortal WklyRep 200150941ndash948
74 Centers for Disease Control Updated recommendations forantimicrobial prophylaxis among asymptomatic pregnantwomen after exposure to Bacillus anthracis MMWR MorbMortal Wkly Rep 200150960
75 Bonventure PF Sueoka W True CW Klein F Lincoln RAttempts to implicate the central nervous system as a pri-
mary site of action for Bacillus anthracis lethal toxin FedProc 1967261549ndash1553
76 Friedlander AM Anthrax In Sidell FR Takafuji ET FranzDR eds Textbook of military medicine medical aspects ofchemical and biological warfare Washington DC Office ofthe Surgeon General 1997467ndash478
77 Vick JA Lincoln RE Klein F Mahlandt BG Walker JS FishDC Neurological and physiological responses of the primateto anthrax toxin J Infect Dis 196811885ndash96
78 Klein F Lincoln RE Dobbs JP Mahlandt BG Remmele NSWalker JS Neurological and physiological responses of theprimate to anthrax infection J Infect Dis 196811897ndash103
79 Remmele NS Klein F Vick JA Walker JS Mahlandt BGLincoln RE Anthrax toxin primary site of action J Infect Dis1968118104ndash113
80 Doganay M Hanagasi R Zora A [Evaluation of penicillinalone and penicillin combined with anti-anthrax serum in ex-perimental anthrax in mice] Mikrobiyol Bul 19851957ndash64
81 Associated Press Government may offer anthrax treatmentNew York Times January 7 2002
82 Davis LE Acute bacterial meningitis In Johnson RT GriffinJW eds Current therapy in neurologic disease 5th ed StLouis Mosby 1997120ndash127
83 Viladrich PF Gudiol F Lintildeares J et al Evaluation of vanco-mycin for therapy of adult pneumococcal meningitis Antimi-crob Agents Chemother 1991352467ndash2472
84 Pariacutes M Hickey SM Uscher MI Shelton S Olsen KD Mc-Cracken GH Jr Effect of dexamethasone on therapy of exper-imental penicillin- and cephalosporin-resistant pneumococcalmeningitis Antimicrob Agents Chemother 1994381320ndash1324
85 Cabellos C Martinez-Lacasa J Martos A et al Influence ofdexamethasone on efficacy of ceftriaxone and vancomycintherapy in experimental pneumococcal meningitis AntimicrobAgents Chemother 1995392158ndash2160
86 Ahmed A Jafri H Lutsar I et al Pharmacodynamics of van-comycin for the treatment of experimental penicillin- andcephalosporin-resistant pneumococcal meningitis AntimicrobAgents Chemother 199943876ndash881
334 NEUROLOGY 59 August (1 of 2) 2002
DOI 101212WNL593327200259327-334 Neurology
Douglas J LanskaAnthrax meningoencephalitis
This information is current as of August 13 2002
ServicesUpdated Information amp
httpwwwneurologyorgcontent593327fullhtmlincluding high resolution figures can be found at
Supplementary Material
htmlhttpwwwneurologyorgneurologysuppl20020716593327DC2
htmlhttpwwwneurologyorgneurologysuppl20020716593327DC1Supplementary material can be found at
References httpwwwneurologyorgcontent593327fullhtmlref-list-1
This article cites 73 articles 15 of which you can access for free at
Citations httpwwwneurologyorgcontent593327fullhtmlotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpwwwneurologyorgcgicollectionmeningitisMeningitis
httpwwwneurologyorgcgicollectionencephalitisEncephalitis
httpwwwneurologyorgcgicollectionbacterial_infectionsBacterial infections
httpwwwneurologyorgcgicollectionall_infectionsAll Infectionsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsin its entirety can be found online atInformation about reproducing this article in parts (figurestables) or
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

63 Jackson PJ Hugh-Jones ME Adair DM et al PCR analysis oftissue samples from the 1979 Sverdlovsk anthrax victims thepresence of multiple Bacillus anthracis strains in differentvictims Proc Natl Acad Sci USA 1998951224ndash1229
64 Grinberg LM Abramova FA Yampolskaya OV Walker DHSmith JH Quantitative pathology of inhalational anthrax IQuantitative microscopic findings Mod Pathol 200114482ndash495
65 Brookmeyer R Blades N Hugh-Jones M Henderson D Thestatistical analysis of truncated data application to the Sverd-lovsk anthrax outbreak Biostatistics 20012233ndash247
66 Knott FA A note on anthrax infection by shaving brushesLancet 19231227ndash228
67 Bradaric N Punda-Polic V Cutaneous anthrax due topenicillin-resistant Bacillus anthracis transmitted by an in-sect bite Lancet 1992340306ndash307
68 Turell MJ Knudson GB Mechanical transmission of Bacillusanthracis by stable flies (Stomoxys calcitrans) and mosquitoes(Aedes aegypti and Aedes taeniorhynchus) Infect Immun1987551859ndash1861
69 Drake DJ Meningitic anthrax Cent Afr J Med 19711797ndash9870 Czyhlarz EV Beitrag zur Lehre von der Milzbrandmeningitis
Wein Klin Wochenscr 191629768ndash76971 Centers for Disease Control Investigation of anthrax associ-
ated with intentional exposure and interim public healthguidelines October 2001 MMWR Morb Mortal Wkly Rep200150889ndash893
72 Centers for Disease Control Update investigation ofbioterrorism-related anthrax and interim guidelines for expo-sure management and antimicrobial therapy October 2001MMWR Morb Mortal Wkly Rep 200150909ndash919
73 Centers for Disease Control Investigation of bioterrorism-related anthrax and interim guidelines for clinical evaluationof persons with possible anthrax MMWR Morb Mortal WklyRep 200150941ndash948
74 Centers for Disease Control Updated recommendations forantimicrobial prophylaxis among asymptomatic pregnantwomen after exposure to Bacillus anthracis MMWR MorbMortal Wkly Rep 200150960
75 Bonventure PF Sueoka W True CW Klein F Lincoln RAttempts to implicate the central nervous system as a pri-
mary site of action for Bacillus anthracis lethal toxin FedProc 1967261549ndash1553
76 Friedlander AM Anthrax In Sidell FR Takafuji ET FranzDR eds Textbook of military medicine medical aspects ofchemical and biological warfare Washington DC Office ofthe Surgeon General 1997467ndash478
77 Vick JA Lincoln RE Klein F Mahlandt BG Walker JS FishDC Neurological and physiological responses of the primateto anthrax toxin J Infect Dis 196811885ndash96
78 Klein F Lincoln RE Dobbs JP Mahlandt BG Remmele NSWalker JS Neurological and physiological responses of theprimate to anthrax infection J Infect Dis 196811897ndash103
79 Remmele NS Klein F Vick JA Walker JS Mahlandt BGLincoln RE Anthrax toxin primary site of action J Infect Dis1968118104ndash113
80 Doganay M Hanagasi R Zora A [Evaluation of penicillinalone and penicillin combined with anti-anthrax serum in ex-perimental anthrax in mice] Mikrobiyol Bul 19851957ndash64
81 Associated Press Government may offer anthrax treatmentNew York Times January 7 2002
82 Davis LE Acute bacterial meningitis In Johnson RT GriffinJW eds Current therapy in neurologic disease 5th ed StLouis Mosby 1997120ndash127
83 Viladrich PF Gudiol F Lintildeares J et al Evaluation of vanco-mycin for therapy of adult pneumococcal meningitis Antimi-crob Agents Chemother 1991352467ndash2472
84 Pariacutes M Hickey SM Uscher MI Shelton S Olsen KD Mc-Cracken GH Jr Effect of dexamethasone on therapy of exper-imental penicillin- and cephalosporin-resistant pneumococcalmeningitis Antimicrob Agents Chemother 1994381320ndash1324
85 Cabellos C Martinez-Lacasa J Martos A et al Influence ofdexamethasone on efficacy of ceftriaxone and vancomycintherapy in experimental pneumococcal meningitis AntimicrobAgents Chemother 1995392158ndash2160
86 Ahmed A Jafri H Lutsar I et al Pharmacodynamics of van-comycin for the treatment of experimental penicillin- andcephalosporin-resistant pneumococcal meningitis AntimicrobAgents Chemother 199943876ndash881
334 NEUROLOGY 59 August (1 of 2) 2002
DOI 101212WNL593327200259327-334 Neurology
Douglas J LanskaAnthrax meningoencephalitis
This information is current as of August 13 2002
ServicesUpdated Information amp
httpwwwneurologyorgcontent593327fullhtmlincluding high resolution figures can be found at
Supplementary Material
htmlhttpwwwneurologyorgneurologysuppl20020716593327DC2
htmlhttpwwwneurologyorgneurologysuppl20020716593327DC1Supplementary material can be found at
References httpwwwneurologyorgcontent593327fullhtmlref-list-1
This article cites 73 articles 15 of which you can access for free at
Citations httpwwwneurologyorgcontent593327fullhtmlotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpwwwneurologyorgcgicollectionmeningitisMeningitis
httpwwwneurologyorgcgicollectionencephalitisEncephalitis
httpwwwneurologyorgcgicollectionbacterial_infectionsBacterial infections
httpwwwneurologyorgcgicollectionall_infectionsAll Infectionsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsin its entirety can be found online atInformation about reproducing this article in parts (figurestables) or
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
DOI 101212WNL593327200259327-334 Neurology
Douglas J LanskaAnthrax meningoencephalitis
This information is current as of August 13 2002
ServicesUpdated Information amp
httpwwwneurologyorgcontent593327fullhtmlincluding high resolution figures can be found at
Supplementary Material
htmlhttpwwwneurologyorgneurologysuppl20020716593327DC2
htmlhttpwwwneurologyorgneurologysuppl20020716593327DC1Supplementary material can be found at
References httpwwwneurologyorgcontent593327fullhtmlref-list-1
This article cites 73 articles 15 of which you can access for free at
Citations httpwwwneurologyorgcontent593327fullhtmlotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpwwwneurologyorgcgicollectionmeningitisMeningitis
httpwwwneurologyorgcgicollectionencephalitisEncephalitis
httpwwwneurologyorgcgicollectionbacterial_infectionsBacterial infections
httpwwwneurologyorgcgicollectionall_infectionsAll Infectionsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsin its entirety can be found online atInformation about reproducing this article in parts (figurestables) or
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online







![A plant based protective antigen [PA(dIV)] vaccine expressed in chloroplasts demonstrates protective immunity in mice against anthrax](https://img.dokumen.tips/doc/110x75/631a60b4bb40f9952b01fa9e/a-plant-based-protective-antigen-padiv-vaccine-expressed-in-chloroplasts-demonstrates.jpg)





















