Embed Size (px)
Citation preview
Interactions between anthrax toxin receptors andprotective antigenHeather M Scobie1,2 and John AT Young1
Since the anthrax mail attacks of 2001, much has been learned
about the interactions between anthrax toxin and its receptors.
Two distinct cellular receptors for anthrax toxin have been
identified and are designated capillary morphogenesis protein
2 (CMG2) and anthrax toxin receptor/tumor endothelial marker
8 (ATR/TEM8). The molecular details of the toxin–receptor
interactions have been revealed through crystallographic,
biochemical and genetic studies. In addition, a novel pathway
by which anthrax toxin enters cells is starting to be uncovered.
Addresses1 Infectious Disease Laboratory, The Salk Institute for Biological Studies,
10010 North Torrey Pines Road, La Jolla, CA 92037, USA2 Program in Cellular and Molecular Biology, University of Wisconsin-
Madison, 413 Bock Labs, 1525 Linden Drive, Madison, WI 53706-1596,
USA
Corresponding author: Young, John AT ([email protected])
Current Opinion in Microbiology 2005, 8:106–112
This review comes from a themed issue on
Host–microbe interactions: bacteria
Edited by Pascale Cossart and Jorge Galan
Available online 7th January 2005
1369-5274/$ – see front matter
# 2005 Elsevier Ltd. All rights reserved.
DOI 10.1016/j.mib.2004.12.005
IntroductionAnthrax is caused by the spore-forming, Gram-positive
bacterium Bacillus anthracis. Anthrax toxin is secreted by
the bacteria and is thought to play a critical role in anthrax
pathogenesis and immune system impairment during
infection. Systemic disease is usually fatal if not treated
with antibiotics before symptoms develop, presumably as a
result of high levels of toxin. Therefore, it is thought that a
successful treatment strategy would include the use of
antitoxins [1,2]. In 2001, when the anthrax mail attacks
occurred in the USA, the cellular receptors used by the
anthrax toxin to enter cells had not been described. During
the past three years significant advances have been made in
understanding the interactions between the anthrax toxin
and its receptors. Now we have a three-dimensional,
molecular picture of a toxin-receptor interaction, increased
knowledge of toxin internalization pathways into cells, and
an idea of how toxin–receptor interactions and receptor
biology contribute to pathogenesis.
In this review, we focus upon recent developments that
have dramatically increased our understanding of anthrax
Current Opinion in Microbiology 2005, 8:106–112
toxin entry into cells, and we point the way to future
approaches for anthrax treatment.
Anthrax toxinAnthrax toxin is a bipartite AB-type toxin with a single
receptor-binding B moiety, known as the protective anti-
gen (PA), and two alternative catalytic A moieties: edema
factor (EF) and lethal factor (LF). PA assembles with EF
or LF to generate edema toxin (ET) or lethal toxin (LT),
respectively.
LF is a zinc-dependent metalloprotease that cleaves the
N-terminus of various mitogen-activated protein kinase
kinases (MKKs) [3–7] resulting in their inactivation and
disruption of various cellular signal transduction path-
ways. LT causes the death of endothelial cells and
sensitized macrophages [8–10], impairs dendritic cell
function [11], disrupts glucocorticoid receptor signaling
[12] and kills mice in a hypoxia-mediated manner [13].
EF is a calcium- and calmodulin-dependent adenylate
cyclase [14] that raises intracellular cAMP levels [15],
which causes swelling [16] and blocks neutrophil-depen-
dent phagocytosis [17].
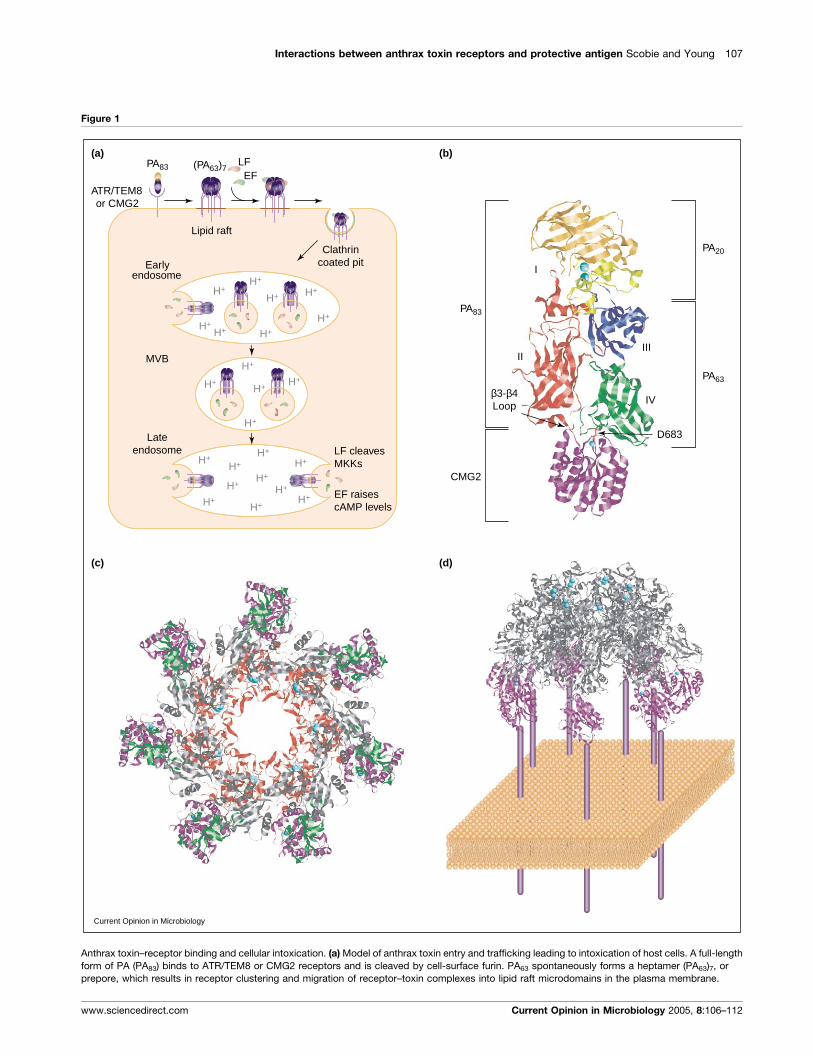
Toxin entryThe current model of toxin entry into host cells is as
follows. A full-length, 83 kDa form of PA (PA83) binds cell
surface receptors (Figure 1a,b) and is subjected to a
necessary cleavage by a cellular furin-like enzyme
[18,19]. The remaining activated PA63 protein then
self-assembles into a heptameric ring structure, or pre-
pore (Figure 1c,d). Binding sites for EF and LF are
generated at the dimer interface between two PA mono-
mers so that each heptamer can bind up to three mole-
cules of either EF and/or LF [20]. PA oligomerization is
accompanied by receptor clustering into lipid raft
domains of the plasma membrane. The receptor–toxin
complex is then taken up into cells by clathrin-dependent
endocytosis (Figure 1a) [21�].
Translocation of LF and EF into the cytosol requires a
low pH-dependent conformational change in the PA
prepore that results in pore formation in an intracellular
membrane (reviewed in [22]; Figure 1a). It was long
believed that the PA heptamer was inserted solely into
the membrane of an endosome, or an endosomal carrier
vesicle, and that the toxin A-moieties were translocated
directly from those compartments into the cytosol. How-
ever, a new model has instead invoked that the PA
heptamer inserts predominantly into the membranes of
intraluminal vesicles within early endosomes and that LF
www.sciencedirect.com
Interactions between anthrax toxin receptors and protective antigen Scobie and Young 107
Figure 1
CMG2
I
IIIII
IV
D683
Earlyendosome
Lipid raft
MVB
LFEF
(a) (b)
(c) (d)
Current Opinion in Microbiology
ATR/TEM8or CMG2
PA83 (PA63)7
Clathrincoated pit
Lateendosome LF cleaves
MKKs
EF raisescAMP levels
H+
H+
H+
H+H+
H+
H+H+
H+H+
H+
H+
H+
H+
H+ H+
H+
H+ H+
H+ H+
H+
H+
PA83
β3-β4Loop
PA63
PA20
Anthrax toxin–receptor binding and cellular intoxication. (a) Model of anthrax toxin entry and trafficking leading to intoxication of host cells. A full-length
form of PA (PA83) binds to ATR/TEM8 or CMG2 receptors and is cleaved by cell-surface furin. PA63 spontaneously forms a heptamer (PA63)7, or
prepore, which results in receptor clustering and migration of receptor–toxin complexes into lipid raft microdomains in the plasma membrane.
www.sciencedirect.com Current Opinion in Microbiology 2005, 8:106–112

108 Host–microbe interactions: bacteria
translocates into the lumen of these vesicles before trans-
port to late endosomes via multivesicular bodies. LF can
then be released into the cytosol when these vesicles fuse
with the limiting membrane of the late endosome
(Figure 1a) [23��]. However, many of the details of this
proposed toxin entry pathway, such as the trafficking
itineraries followed by the two types of anthrax toxin
receptor, remain to be characterized.
Anthrax toxin receptorsAnthrax toxin receptor/tumor endothelial marker 8 (ATR/
TEM8) was the first anthrax toxin receptor identified
using an approach that combined somatic cell mutagen-
esis in chinese hamster ovary cells with human cDNA
complementation [24]. The related capillary morphogen-
esis gene 2 (CMG2) protein was subsequently shown to
have anthrax toxin receptor function [25��].
ATR/TEM8 and CMG2 are type 1 transmembrane
proteins with single membrane spanning domains.
Their most distinctive feature is an extracellular region
approximately 200 amino acids long that binds directly
to PA and is related to the von Willebrand factor A
(vWFA) domains and most closely related to a-integrin-
like inserted (I) domains (Figures 1b and 2). Although
the amino acid sequences of both anthrax toxin recep-
tors are only 40% identical overall, their I domains are
approximately 60% identical. At present, three differ-
ent protein isoforms of each anthrax toxin receptor have
been described and are the result of alternative mRNA
splicing (Figure 2) [24,25��]. Although the precise dis-
tribution and levels of each of these proteins in differ-
ent tissues remain to be established, northern blot and
RT-PCR analysis has indicated that the CMG2 gene is
likely to be expressed in most human tissues, whereas
ATR/TEM8 expression may be restricted to tumor
endothelial and cancer cells [25��,26–30]. However,
ATR/TEM8 expression is modestly upregulated in
response to interleukin-1b treatment [31], raising the
possibility that the level and tissue distribution of this
receptor might fluctuate during the course of a bacterial
infection.
(Figure 1 legend continued) Up to three molecules of LF or EF can bind t
clathrin-mediated endocytosis. The toxin–receptor complex is trafficked in a
PA domain II and domain IV is thought to prevent membrane pore formatio
translocated into the vesicle lumen and gain access to the cytoplasm prima
endosome where they back-fuse with the limiting membrane, or alternativel
mitogen activated kinase kinases (MKKs) and EF raises cAMP in a calmodu
determined for the full-length and catalytic portions of these proteins, respe
monomer (Protein Database 1T6B [33��]). The CMG2 I domain (purple) adopt
a site of PA binding. PA domain I (orange and yellow) contains two Ca2+ ions
PA63 and PA20 fragment (orange). PA domain II (red) lines the PA pore, is in
that results in membrane pore formation. b3–b4 loop contacts with CMG2 a
involved in oligomerization and domain IV (green) is a discrete receptor-bind
(pink stick representation) makes contact with the metal cation at the recep
(Protein Database 1TZN [40��]). CMG2 I domains (purple) punctuate the low
domains IV (green) and II (red). The CMG2 MIDAS Mg2+ and PA Ca2+ ions a
in panel (c) modeled on a schematic of the plasma membrane. The structur
solved and it is depicted as a purple stalk. LF and/or EF (not shown) bind t
Current Opinion in Microbiology 2005, 8:106–112
In the case of ATR/TEM8, mRNA isoforms are known as
splice variants (sv) 1–3. The ATR/TEM8 proteins
encoded by sv1 and sv2 are transmembrane proteins with
differing cytoplasmic regions and both function as anthrax
toxin receptors (Figure 2) [24,32�]. Interestingly, the
cytoplasmic domains of ATR/TEM8 proteins are not
essential for toxin binding and entry since they can be
deleted or replaced with a glycosylphosphatidylinositol
(GPI) anchor sequence and still support intoxication
[32�]. The sv3 mRNA encodes a secreted ATR/TEM8
protein that does not serve as an anthrax toxin receptor
(Figure 2) [32�].
The three CMG2 protein isoforms are transmembrane
proteins consisting of either 386, 488 or 489 amino acids
that we have designated as CMG2386, CMG2488 and
CMG2489, respectively. CMG2489 and CMG2488 are iden-
tical except for the 12–13 amino acids located at their
C-termini (Figure 2), and both proteins function as
anthrax toxin receptors ([25��]; HM Scobie et al., unpub-
lished). The cytoplasmic domain of CMG2386 is the same
as CMG2489 but is lacking two C-terminal residues of the
I domain as well as a 100 amino acid membrane proximal
domain present in the two longer protein isoforms
(Figure 2) [25��]. Although the CMG2386 I domain can
bind PA [33��], the full-length version of this protein
cannot support intoxication (HM Scobie et al., unpub-
lished). The precise defect associated with the CMG2386
protein remains to be determined.
ATR/TEM8 and CMG2 proteins are conserved
between diverse species, including mouse, rat and zeb-
rafish, suggesting that they fulfill an important physio-
logical function. Their precise function is unknown, but
evidence suggests they are cell adhesion molecules
involved in angiogenesis. ATR/TEM8 proteins bind
to collagen a3(VI) [29]. ATR/TEM8 is preferentially
expressed in the vasculature of different types of human
tumors [26,29,30,34], as well as developing mouse
embryos [30]. CMG2 binds to collagen IV and laminin,
and its gene is specifically upregulated in human umbi-
lical vein endothelial cells induced to undergo capillary
he PA heptamer, and after assembly, the complex is taken up via
n intraluminal vesicle to the early endosome. Receptor contact with
n until exposure to this low pH environment. Toxin A moieties are
rily after vesicle trafficking via multivesicular bodies (MVB) to the late
y after fusion with the early endosomal membrane. LF cleaves cellular
lin- and calcium-dependent manner. Crystal structures have been
ctively [3,14]. (b) Ribbon diagram of a CMG2 I domain bound to PA83
s a Rossmann fold with a metal cation (Mn2+; cyan) bound at its MIDAS,
(cyan) and is cleaved by furin to generate EF and LF binding sites and a
volved in oligomerization, and undergoes a conformational change
re hypothesized to inhibit this change. PA domain III (blue) is primarily
ing domain. The carboxylate side-chain from PA residue Asp683
tor MIDAS. (c) Overhead view of CMG2 I domain/PA heptamer complex
er, outer surface of the PA prepore (grey) making contact with PA
re colored cyan. (d) Side-view of the CMG2–PA heptamer complex
e of the CMG2 receptor membrane proximal domain (MPD) was not
o the top surface of the PA heptamer.
www.sciencedirect.com
Interactions between anthrax toxin receptors and protective antigen Scobie and Young 109
Figure 2
5641 27 44 216 320 343
3191 27 44 216 333
sv1
sv2
sv3
1 27 44 216 320 343 368364
1 33 44 212 215 233 386
1 33 44 214 318 336 488477
1 33 44 214 318 336 489
489
488
386
MIDAS
SP TMMPD
Current Opinion in Microbiology
ATR/ TEM8:
CMG2:
vWFA/ I domain
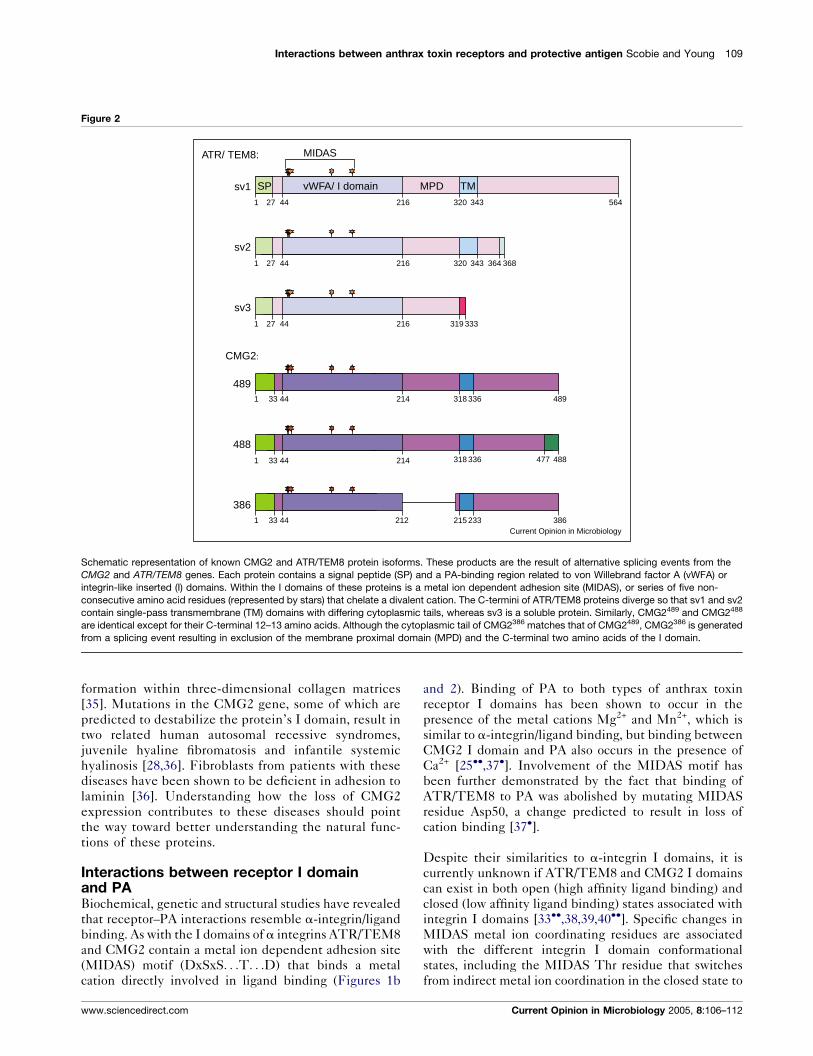
Schematic representation of known CMG2 and ATR/TEM8 protein isoforms. These products are the result of alternative splicing events from the
CMG2 and ATR/TEM8 genes. Each protein contains a signal peptide (SP) and a PA-binding region related to von Willebrand factor A (vWFA) or
integrin-like inserted (I) domains. Within the I domains of these proteins is a metal ion dependent adhesion site (MIDAS), or series of five non-
consecutive amino acid residues (represented by stars) that chelate a divalent cation. The C-termini of ATR/TEM8 proteins diverge so that sv1 and sv2
contain single-pass transmembrane (TM) domains with differing cytoplasmic tails, whereas sv3 is a soluble protein. Similarly, CMG2489 and CMG2488
are identical except for their C-terminal 12–13 amino acids. Although the cytoplasmic tail of CMG2386 matches that of CMG2489, CMG2386 is generated
from a splicing event resulting in exclusion of the membrane proximal domain (MPD) and the C-terminal two amino acids of the I domain.
formation within three-dimensional collagen matrices
[35]. Mutations in the CMG2 gene, some of which are
predicted to destabilize the protein’s I domain, result in
two related human autosomal recessive syndromes,
juvenile hyaline fibromatosis and infantile systemic
hyalinosis [28,36]. Fibroblasts from patients with these
diseases have been shown to be deficient in adhesion to
laminin [36]. Understanding how the loss of CMG2
expression contributes to these diseases should point
the way toward better understanding the natural func-
tions of these proteins.
Interactions between receptor I domainand PABiochemical, genetic and structural studies have revealed
that receptor–PA interactions resemble a-integrin/ligand
binding. As with the I domains of a integrins ATR/TEM8
and CMG2 contain a metal ion dependent adhesion site
(MIDAS) motif (DxSxS. . .T. . .D) that binds a metal
cation directly involved in ligand binding (Figures 1b
www.sciencedirect.com
and 2). Binding of PA to both types of anthrax toxin
receptor I domains has been shown to occur in the
presence of the metal cations Mg2+ and Mn2+, which is
similar to a-integrin/ligand binding, but binding between
CMG2 I domain and PA also occurs in the presence of
Ca2+ [25��,37�]. Involvement of the MIDAS motif has
been further demonstrated by the fact that binding of
ATR/TEM8 to PA was abolished by mutating MIDAS
residue Asp50, a change predicted to result in loss of
cation binding [37�].
Despite their similarities to a-integrin I domains, it is
currently unknown if ATR/TEM8 and CMG2 I domains
can exist in both open (high affinity ligand binding) and
closed (low affinity ligand binding) states associated with
integrin I domains [33��,38,39,40��]. Specific changes in
MIDAS metal ion coordinating residues are associated
with the different integrin I domain conformational
states, including the MIDAS Thr residue that switches
from indirect metal ion coordination in the closed state to
Current Opinion in Microbiology 2005, 8:106–112

110 Host–microbe interactions: bacteria
direct coordination in the open state [41]. Mutation of the
corresponding residue (T118) in ATR/TEM8 reduced
receptor activity by 100–1000-fold, a result that was
consistent with the idea that this receptor might have
to adopt an open-like binding state to bind PA [37�]. This
view is supported by X-ray crystallographic studies that
have demonstrated that residue T118 of CMG2 makes
direct contact with the metal ion in PA–CMG2 complexes
[33��,40��].
Ligands bound to the open conformation of a-integrin I
domains contribute a carboxylate-containing amino acid
side-chain that completes the MIDAS metal ion coordi-
nation sphere [41]. On the basis of mutagenesis studies,
the D683 residue of PA was postulated to perform a
similar role in the ATR/TEM8 interaction [37�,42].
Again, crystallographic studies of PA–CMG2 complexes
have revealed that D683 makes direct contact with the
metal ion bound at the receptor MIDAS (Figure 1b).
Other conformational changes that accompany the
a-integrin I domain conversion between closed and open
conformations include a dramatic 10A movement of the
C-terminal a-helix and insertion of different hydrophobic
residues into the domain’s hydrophobic pockets to stabi-
lize the two conformations [39,41]. Because the CMG2 I
domain appears to lack the hydrophobic residue for
stabilizing a putative closed conformation, it has been
argued that this receptor might never adopt a closed-like
state [39]. However, a crystal structure of the CMG2386 I
domain lacking the residue that stabilizes the open
CMG2489 I domain is able to bind to PA in an open
conformation manner using a different stabilizing hydro-
phobic residue [33��]. This raises the possibility that other
local hydrophobic residues might help stabilize alterna-
tive conformations of this domain.
A striking difference between CMG2–PA and a integrin/
ligand interactions is found at the level of binding affi-
nities. The binding affinities that are associated with
a-integrin interactions with physiological ligands are
typically in the mM to mM range [38]. By contrast,
PA binds the CMG2 I domain with an extremely high
affinity (KD = 170 pM or 780 pM in the presence of Mg2+
or Ca2+ ions, respectively) [43�]. Indeed, this receptor can
still bind PA in the absence of metal ions at a level
(KD = 960 nM) [43�] on par with a-integrin/ligand inter-
actions in the presence of metal ions. These differences
in binding affinity are likely explained by the fact that
the PA–CMG2 interaction buries approximately 2000A2
of protein surface, whereas a-integrin/ligand interactions
typically bury only 1300A2 of protein surface [33��,40��].In contrast to CMG2, the ATR/TEM8 I domain binds
much less tightly to PA (HM Scobie et al., unpublished); a
property that may be explained by several amino acid
differences between the PA-binding interfaces of both
receptors [33��,40��]. The high binding affinity between
Current Opinion in Microbiology 2005, 8:106–112
CMG2 and PA is currently being exploited for the devel-
opment of soluble receptor-based antitoxins [2,25��].
A role for receptor in low pH-dependentPA pore formationPA consists of four discrete domains (I–IV) with different
functions (Figure 1b). Prior to the crystal structures of
monomeric PA83 with the CMG2386 I domain (2.5A
resolution; Figure 1b) and heptameric PA63 with the
CMG2489 I domain (4.3A resolution; Figure 1c,d), it
was believed that domain IV was the only receptor-
binding region of PA [33��,40��]. Indeed, domain IV
contains the D683 residue that binds the MIDAS metal
and also contains other residues that make contact with
the CMG2 I domain (Figure 1b) [33��,40��]. However,
the co-crystal structures unexpectedly revealed that the
b3–b4 loop of PA domain II, a domain that is primarily
involved in forming the pore thought to translocate EF
and LF, also contributes significantly to the receptor
interaction (Figure 1b,c) [33��,40��].
The binding of the CMG2 I domain to regions of PA
domain II and IV have helped to explain one of the
puzzling features of PA pore formation, namely that it
occurs at a higher pH value in artificial membranes than in
cells that have receptors [44]. The bound CMG2 I domain
serves as a clamp that, at neutral pH, blocks subsequent
rearrangements of PA domain II necessary for pore for-
mation. This action would ensure that the PA pore would
form only after proper trafficking of the toxin–receptor
complex to an endosomal compartment with low pH
(Figure 1a) [33��,40��]. Consistent with this idea, PA63
prepore to pore conversion in solution has been demon-
strated to occur at neutral pH in the absence of the
receptor but only at acidic pH in its presence [40��]. It
has been postulated that this triggering mechanism
involves the protonation of histidine residues located at
the PA–receptor binding interface and at regions of PA
that are thought to undergo structural rearrangements
upon pore conversion [33��].
ConclusionsThe first step in anthrax intoxication involves PA binding
to the I domain of either of two cell surface receptors,
ATR/TEM8 or CMG2. These binding interactions
resemble those between a-integrins and their ligands
in that the MIDAS of the receptor, as well as a carbox-
ylate-containing residue of PA, serve important roles. The
recently obtained X-ray crystal structures of monomeric,
and heptameric PA with the CMG2 I domain have
revealed the molecular details of the toxin–receptor inter-
action. These structures have led to the identification of
shared residues that are presumably important for PA-
specific binding, and have uncovered an unexpected role
for the receptor in acting as a molecular clamp to ensure
that the PA heptameric pore forms only within the acidic
lumen of an endosomal compartment. Cell biological
www.sciencedirect.com
Interactions between anthrax toxin receptors and protective antigen Scobie and Young 111
studies have led to the proposal that pore formation and
LF translocation occur in intraluminal vesicles within
endosomes and that LF is not delivered into the cytosol
directly, as was previously thought, but instead when
these vesicles fuse with limiting endosomal membranes.
The continued study of anthrax toxins and their receptors
promises to yield more exciting discoveries in the fields of
microbiology and cell biology, and should aid in the
development of antitoxins aimed at preventing toxin
entry into the cell.
AcknowledgementsThe authors acknowledge support for this work from NIH grantsAI48489 and AI56013, and thank G Jonah Rainey and Kenneth Bradleyfor their critical feedback on the manuscript.
References and recommended readingPapers of particular interest, published within the annual period ofreview, have been highlighted as:
� of special interest�� of outstanding interest
1. Inglesby TV, O’Toole T, Henderson DA, Bartlett JG, Ascher MS,Eitzen E, Friedlander AM, Gerberding J, Hauer J, Hughes J et al.:Anthrax as a biological weapon, 2002: updatedrecommendations for management. JAMA 2002,287:2236-2252.
2. Rainey GJA, Young JAT: Antitoxins: novel strategies to targetagents of bioterrorism. Nat Rev Microbiol 2004, 2:721-726.
3. Pannifer AD, Wong TY, Schwarzenbacher R, Renatus M, Petosa C,Bienkowska J, Lacy DB, Collier RJ, Park S, Leppla SH et al.:Crystal structure of the anthrax lethal factor. Nature 2001,414:229-233.
4. Vitale G, Bernardi L, Napolitani G, Mock M, Montecucco C:Susceptibility of mitogen-activated protein kinase kinasefamily members to proteolysis by anthrax lethal factor.Biochem J 2000, 352:739-745.
5. Vitale G, Pellizzari R, Recchi C, Napolitani G, Mock M, MontecuccoC: Anthrax lethal factor cleaves the N-terminus of MAPKKsand induces tyrosine/threonine phosphorylation of MAPKs incultured macrophages. Biochem Biophys Res Commun 1998,248:706-711.
6. Duesbery NS, Webb CP, Leppla SH, Gordon VM, Klimpel KR,Copeland TD, Ahn NG, Oskarsson MK, Fukasawa K, Paull KD etal.: Proteolytic inactivation of MAP-kinase-kinase by anthraxlethal factor. Science 1998, 280:734-737.
7. Chopra AP, Boone SA, Liang X, Duesbery NS: Anthrax lethalfactor proteolysis and inactivation of MAP-kinase-kinase.J Biol Chem 2003, 278:9402-9406.
8. Park JM, Greten FR, Li ZW, Karin M: Macrophage apoptosis byanthrax lethal factor through p38 MAP kinase inhibition.Science 2002, 297:2048-2051.
9. Kirby JE: Anthrax lethal toxin induces human endothelial cellapoptosis. Infect Immun 2004, 72:430-439.
10. Kim SO, Jing Q, Hoebe K, Beutler B, Duesbery NS, Han J:Sensitizing anthrax lethal toxin-resistant macrophages tolethal toxin-induced killing by tumor necrosis factor-alpha.J Biol Chem 2003, 278:7413-7421.
11. Agrawal A, Lingappa J, Leppla SH, Agrawal S, Jabbar A, Quinn C,Pulendran B: Impairment of dendritic cells and adaptiveimmunity by anthrax lethal toxin. Nature 2003, 424:329-334.
12. Webster JI, Tonelli LH, Moayeri M, Simons SS Jr, Leppla SH,Sternberg EM: Anthrax lethal factor represses glucocorticoidand progesterone receptor activity. Proc Natl Acad Sci USA2003, 100:5706-5711.
www.sciencedirect.com
13. Moayeri M, Haines D, Young HA, Leppla SH: Bacillus anthracislethal toxin induces TNF-alpha-independent hypoxia-mediated toxicity in mice. J Clin Invest 2003, 112:670-682.
14. Drum CL, Yan SZ, Bard J, Shen YQ, Lu D, Soelaiman S,Grabarek Z, Bohm A, Tang WJ: Structural basis for theactivation of anthrax adenylyl cyclase exotoxin by calmodulin.Nature 2002, 415:396-402.
15. Leppla SH: Anthrax toxin edema factor: a bacterial adenylatecyclase that increases cyclic AMP concentrations ofeukaryotic cells. Proc Natl Acad Sci USA 1982, 79:3162-3166.
16. Pezard C, Berche P, Mock M: Contribution of individual toxincomponents to virulence of Bacillus anthracis. Infect Immun1991, 59:3472-3477.
17. O’Brien J, Friedlander A, Dreier T, Ezzell J, Leppla S: Effectsof anthrax toxin components on human neutrophils.Infect Immun 1985, 47:306-310.
18. Beauregard KE, Collier RJ, Swanson JA: Proteolytic activation ofreceptor-bound anthrax protective antigen on macrophagespromotes its internalization. Cell Microbiol 2000, 2:251-258.
19. Klimpel KR, Molloy SS, Thomas G, Leppla SH: Anthrax toxinprotective antigen is activated by a cell surface protease withthe sequence specificity and catalytic properties of furin.Proc Natl Acad Sci USA 1992, 89:10277-10281.
20. Mogridge J, Cunningham K, Collier RJ: Stoichiometry of anthraxtoxin complexes. Biochemistry 2002, 41:1079-1082.
21.�
Abrami L, Liu S, Cosson P, Leppla SH, van der Goot FG: Anthraxtoxin triggers endocytosis of its receptor via a lipid raft-mediated clathrin-dependent process. J Cell Biol 2003,160:321-328.
This study shows that PA oligomerization leads to receptor redistributioninto lipid rafts of the plasma membrane followed by clathrin-dependentendocytosis of toxin–receptor complexes.
22. Collier RJ, Young JA: Anthrax toxin. Annu Rev Cell Dev Biol 2003,19:45-70.
23.��
Abrami L, Lindsay M, Parton RG, Leppla SH, Van Der Goot FG:Membrane insertion of anthrax protective antigen andcytoplasmic delivery of lethal factor occur at different stagesof the endocytic pathway. J Cell Biol 2004, 166:645-651.
This recent study, which employed inhibitors of endosomal trafficking andfunction, has led to a new model for anthrax toxin trafficking andtranslocation. The PA pore inserts predominantly into the membraneof intraluminal vesicles within early endosomes. Lethal factor is thentranslocated into the lumen of these vesicles and trafficked via multi-vesicular bodies to late endosomes, where toxin is finally released intothe cytoplasm after vesicle back-fusion with the limiting endosomalmembrane.
24. Bradley KA, Mogridge J, Mourez M, Collier RJ, Young JA:Identification of the cellular receptor for anthrax toxin.Nature 2001, 414:225-229.
25.��
Scobie HM, Rainey GJ, Bradley KA, Young JA: Human capillarymorphogenesis protein 2 functions as an anthrax toxinreceptor. Proc Natl Acad Sci USA 2003, 100:5170-5174.
CMG2 is identified as a second anthrax toxin receptor based upon itsability to confer PA binding and susceptibility to intoxication whenexpressed in PA receptor-deficient cells. Northern blot analysis showsbroad expression of the receptor in human tissues that may be relevantfor intoxication. Also, a soluble version of the CMG2 I domain is shown tobe a very efficient receptor decoy, blocking cell intoxication when mixedwith PA at a 3:1 ratio.
26. Davies G, Mason MD, Martin TA, Parr C, Watkins G, Lane J,Matsumoto K, Nakamura T, Jiang WG: The HGF/SF antagonistNK4 reverses fibroblast- and HGF-induced prostate tumorgrowth and angiogenesis in vivo. Int J Cancer 2003,106:348-354.
27. De Preter K, Pattyn F, Berx G, Strumane K, Menten B, Van Roy F,De Paepe A, Speleman F, Vandesompele J: Combinedsubtractive cDNA cloning and array CGH: an efficientapproach for identification of overexpressed genes in DNAamplicons. BMC Genomics 2004, 5:11.
28. Hanks S, Adams S, Douglas J, Arbour L, Atherton DJ, Balci S,Bode H, Campbell ME, Feingold M, Keser G et al.: Mutations in
Current Opinion in Microbiology 2005, 8:106–112
112 Host–microbe interactions: bacteria
the gene encoding capillary morphogenesis protein 2 causejuvenile hyaline fibromatosis and infantile systemic hyalinosis.Am J Hum Genet 2003, 73:791-800.
29. Nanda A, Carson-Walter EB, Seaman S, Barber TD, Stampfl J,Singh S, Vogelstein B, Kinzler KW, St Croix B: TEM8 interactswith the cleaved C5 domain of collagen alpha 3(VI).Cancer Res 2004, 64:817-820.
30. Carson-Walter EB, Watkins DN, Nanda A, Vogelstein B,Kinzler KW, St Croix B: Cell surface tumor endothelial markersare conserved in mice and humans. Cancer Res 2001,61:6649-6655.
31. Rmali KA, Al-Rawi MA, Parr C, Puntis MC, Jiang WG:Upregulation of tumour endothelial marker-8 by interleukin-1beta and its impact in IL-1beta induced angiogenesis.Int J Mol Med 2004, 14:75-80.
32.�
Liu S, Leppla SH: Cell surface tumor endothelium marker 8cytoplasmic tail-independent anthrax toxin binding,proteolytic processing, oligomer formation, andinternalization. J Biol Chem 2003, 278:5227-5234.
The authors demonstrate that, as with ATR/TEM8 sv2, ATR/TEM8 sv1also functions as an anthrax toxin receptor. In addition, the cytoplasmictail of the receptor is shown to be dispensable, because replacement ofthis region with a GPI anchor does not impair the ability of the receptor tosupport intoxication.
33.��
Santelli E, Bankston LA, Leppla SH, Liddington RC: Crystalstructure of a complex between anthrax toxin and its host cellreceptor. Nature 2004, 430:905-908.
The crystal structure of monomeric PA with the CMG2 I domain isdescribed. The structure reveals a large buried protein surface at thePA-CMG2 interface and, along with the paper by Lacy et al. [40��], showsthat domain II of PA makes unexpected contact with the receptor. Theauthors suggest that the bound CMG2 moiety might serve as a molecularbrace to prevent domain II rearrangements necessary for pore formationuntil the complex is exposed to a low pH environment, at which time theprotonation of specific histidine residues located at the PA–CMG2 inter-face and within mobile segments of PA might drive PA prepore to poreconversion.
34. St Croix B, Rago C, Velculescu V, Traverso G, Romans KE,Montgomery E, Lal A, Riggins GJ, Lengauer C, Vogelstein B et al.:Genes expressed in human tumor endothelium. Science 2000,289:1197-1202.
35. Bell SE, Mavila A, Salazar R, Bayless KJ, Kanagala S, Maxwell SA,Davis GE: Differential gene expression during capillarymorphogenesis in 3D collagen matrices: regulated expressionof genes involved in basement membrane matrix assembly,cell cycle progression, cellular differentiation and G-proteinsignaling. J Cell Sci 2001, 114:2755-2773.
36. Dowling O, Difeo A, Ramirez MC, Tukel T, Narla G, Bonafe L,Kayserili H, Yuksel-Apak M, Paller AS, Norton K et al.: Mutationsin capillary morphogenesis gene-2 result in the allelic
Current Opinion in Microbiology 2005, 8:106–112
disorders juvenile hyaline fibromatosis and infantile systemichyalinosis. Am J Hum Genet 2003, 73:957-966.
37.�
Bradley KA, Mogridge J, Jonah G, Rainey A, Batty S,Young JA: Binding of anthrax toxin to its receptor is similarto alpha integrin-ligand interactions. J Biol Chem 2003,278:49342-49347.
Anthrax toxin–receptor interactions are shown to resemble thosebetween a-integrin I domains and their physiological ligands in thatATR/TEM8–PA binding requires an open-like conformation of the recep-tor with a divalent cation bound to the MIDAS as well as a carboxylateside-chain from PA.
38. Shimaoka M, Xiao T, Liu JH, Yang Y, Dong Y, Jun CD, McCormackA, Zhang R, Joachimiak A, Takagi J et al.: Structures of the alphaL I domain and its complex with ICAM-1 reveal a shape-shifting pathway for integrin regulation. Cell 2003, 112:99-111.
39. Lacy DB, Wigelsworth DJ, Scobie HM, Young JA, Collier RJ:Crystal structure of the von Willebrand factor A domain ofhuman capillary morphogenesis protein 2: an anthrax toxinreceptor. Proc Natl Acad Sci USA 2004, 101:6367-6372.
40.��
Lacy DB, Wigelsworth DJ, Melnyk RA, Harrison SC, Collier RJ:Structure of heptameric protective antigen bound to ananthrax toxin receptor: A role for receptor in pH-dependentpore formation. Proc Natl Acad Sci USA 2004, 101:13147-13151.
The co-crystal structure of seven CMG2 I domains bound to the PAheptamer is presented and, along with the paper by Santelli et al. [33��],shows that there is a large CMG2–PA contact surface and that PA domainII makes unexpected contact with receptor. This structure also reveals theplacement of the domain II membrane insertion loop in the PA prepore.The authors demonstrate that CMG2 binding imposes a low pH depen-dence on pore formation, presumably preventing premature translocationof the toxin A subunits.
41. Emsley J, Knight CG, Farndale RW, Barnes MJ, Liddington RC:Structural basis of collagen recognition by integrinalpha2beta1. Cell 2000, 101:47-56.
42. Rosovitz MJ, Schuck P, Varughese M, Chopra AP, Mehra V,Singh Y, McGinnis LM, Leppla SH: Alanine-scanning mutationsin domain 4 of anthrax toxin protective antigen reveal residuesimportant for binding to the cellular receptor and to aneutralizing monoclonal antibody. J Biol Chem 2003,278:30936-30944.
43.�
Wigelsworth DJ, Krantz BA, Christensen KA, Lacy DB, Juris SJ,Collier RJ: Binding stoichiometry and kinetics of the interactionof a human anthrax toxin receptor, CMG2, with protectiveantigen. J Biol Chem 2004, 279:23349-23356.
The PA heptamer is shown to bind seven copies of the CMG2 I domain andthe binding affinity of the monomeric PA–CMG2 I domain interaction isfound to be very high in the presence of either magnesium or calcium ions.
44. Miller CJ, Elliott JL, Collier RJ: Anthrax protective antigen:prepore-to-pore conversion. Biochemistry 1999,38:10432-10441.
www.sciencedirect.com






![A plant based protective antigen [PA(dIV)] vaccine expressed in chloroplasts demonstrates protective immunity in mice against anthrax](https://img.dokumen.tips/doc/110x75/631a60b4bb40f9952b01fa9e/a-plant-based-protective-antigen-padiv-vaccine-expressed-in-chloroplasts-demonstrates.jpg)






















