Embed Size (px)
Citation preview
An evidence-based comparison of headgear andfunctional appliance therapy for the correctionof Class II malocclusionsThomas E. Southard, Steven D. Marshall, Veerasathpurush Allareddy,Lina Maria Moreno Uribe, and Nathan E. Holton
The purpose of this literature review is to compare the effects of headgearsand functional appliances in treating children with distoclusions. Thecomparisons are made as a series of key questions addressing short-termeffects, outcomes following fixed appliance treatment, and post-retentioneffects. Headgears and functional appliances are equally effective incorrecting Class II malocclusions in children (before comprehensive treat-ment). Short-term skeletal effects include a small restriction in forwardmaxillary growth with headgear and a small forward positioning of B pointwith functional appliances, leading to an ANB improvement in Class IIpatients of about 11with either appliance. A significant portion of the Class IIcorrection is distal maxillary molar movement with headgears and mesialmandibular molar movement (plus mandibular incisor proclination) withfunctional appliances. Higher levels of evidence, to answer the question ofwhether the effects of headgears and functional appliances are equalfollowing fixed appliances, are lacking and needs to be addressed. (SeminOrthod 2013; 19:174–195.) & 2013 Elsevier Inc. All rights reserved.
T he correction of Class II malocclusions inchildren requires an assessment of both the
etiology and magnitude of the distoclusion.Dental causes include ectopic eruption of max-illary first molars, mesial drift of maxillary firstmolars as a result of premature loss of maxillaryprimary second molars, and mesial drift ofmaxillary first molars as a result of arch lengthreduction from primary tooth caries. Skeletaldisharmony causing a Class II relationship resultsfrom unfavorable differential growth of themaxilla and mandible: excess maxillary hori-zontal growth, deficient mandibular horizontalgrowth, a combination of excess maxillary anddeficient mandibular horizontal growth, orexcess maxillary vertical growth (resulting indownward and backward mandibular rotation).
Conventional wisdom dictated that dis-toclusions resulting from mild apical base dis-crepancies were the most amenable toorthopedic treatment if the child was cooperativeand a favorable mandibular growth vectorremained. In patients with moderate apical basediscrepancies (or with less favorable mandibulargrowth vector remaining), anteroposterior skel-etal correction was considered less likely usingorthopedics. In such cases, a Class I caninerelationship might be achieved by masking theunderlying skeletal discrepancy (mesial trans-lation of the mandibular dentition, distal trans-lation of the maxillary dentition, or clockwisetipping of the occlusal plane). In children withsevere apical base discrepancies, a successfuloutcome was considered unlikely using eitherorthopedics or masking. In such cases, orthog-nathic surgical treatment following growth ces-sation often provided the most prudent course oftreatment.
Traditionally, headgears have been used tocorrect distoclusions by restricting maxillaryhorizontal growth, permitting mandibular hori-zontal growth, and distalizing the maxillarydentition. Patients with steep mandibular plane
& 2013 Elsevier Inc. All rights reserved.1073-8746/13/1801-$30.00/0http://dx.doi.org/10.1053/j.sodo.2013.03.007
Department of Orthodontics, The University of Iowa, Iowa City,IA; Harvard School of Dental Medicine, Boston, MA; Department ofAnthropology, The University of Iowa, Iowa City, IA.
Address correspondence to Thomas E. Southard, DDS, MS,Department of Orthodontics, College of Dentistry, The University ofIowa, Iowa City, Iowa 522424. E-mail: [email protected]
174 Seminars in Orthodontics, Vol 19, No 3 (September), 2013: pp 174–195

angles, vertical maxillary excess, long loweranterior face heights, and anterior open biteshave been treated with high-pull headgears—inan attempt to reduce vertical development whilecorrecting the Class II relationship; while patientswith flat mandibular plane angles, short loweranterior face heights, and deep bites were treatedwith cervical pull headgears—in an attempt toimprove vertical development while correctingthe Class II relationship.
Functional appliances were intended to cor-rect distoclusions by enhancing mandibulargrowth. Although countless variations have beenmarketed, the mode of action is basically thesame for all. As the mandible was postured (andheld) forward in a Class II child, growth of thedistracted condylar head and remodeling of theglenoid fossa would be enhanced to achieveskeletal correction, profile improvement, andideal dental interdigitation. Uprighting of max-illary incisors and proclination of mandibularincisors would also occur. If, as the mandible waspostured forward, the bite was opened in theposterior then the mandibular plane could rotatedown and back as posterior teeth erupted. Tra-ditionally, the ideal patient for functionalappliance treatment was a Class II child withproclined maxillary incisors, upright mandibularincisors, and a normal to flatter mandibularplane.
The purpose of this literature review is tocompare the effects of headgears and functionalappliances in treating children with dis-toclusions. The comparison is made as a series ofnine key questions addressing short-term effects,effects following fixed appliance treatment, andpost-retention effects. Answers to each questionwill be provided using the best evidence currentlyavailable, and questions requiring further inves-tigation are identified.
Q1: Are headgears and functional appliancesequally effective in correcting Class II maloc-clusions in children (before comprehensivetreatment)?
A: YesUnequivocal short-term skeletal effects
include a small restriction in forward maxillarygrowth with headgear (SNA decreases 0.51–31)and a small forward positioning of B point withfunctional appliances (11–21), resulting in anANB improvement in Class II patients of about 11with either appliance. A significant portion of the
Class II correction is distal maxillary molarmovement with headgears and mesial man-dibular molar movement (along with mandibularincisor proclination) with functional appliances.
PubMed and Cochrane Library databasesearches were performed to identify articlesreporting prospective randomized clinical trialsof Class II malocclusions in groups of childrentreated with both headgears and functionalappliances (no comprehensive fixed appliances)in the same trial. Five trials were identified andeach is summarized below, and a concludingsummary is provided.
In the first study, Jakobsson1 followed threegroups of Class II children (19 patients pergroup; average age 8.5 years) who were randomlyassigned to 18 months of treatment with either acervical pull (Kloehn) headgear, treatment withan Andresen activator appliance (mandibleadvanced three quarters of a cusp), or to acontrol group.
The headgear group restricted A point by anaverage of approximately 1.6 mm and distalizedmaxillary molars by an average of 3.7 mm com-pared to the control group. The activator grouprestricted A point by an average of 0.7 mm anddistalized maxillary molars by an average of1.2 mm compared to the control group. A sig-nificant reduction in overjet was found with bothappliances, with the activator group having thegreatest reduction (due to lower incisor procli-nation). No significant change in mandibularlength was found in either the headgear oractivator groups. Both the headgear group andactivator group saw a very slight increase invertical measured at menton (approximately0.1 mm).
A sample of 166 Class II patients with anoverjet exceeding 7 mm and an average age of9.4 years were randomly assigned to one of thethree groups by Tulloch et al.2,3 to be treated for15 months with a combination (straight-pull)headgear, a modified Bionator (minimal verticalopening, 4–6 mm of protrusion), or to be leftuntreated as a control.
The headgear group showed restricted for-ward maxillary growth (0.91 annualized change)while the Bionator group did not. Molar move-ments were not reported. The Bionator groupdemonstrated a greater increase in mandibularunit length compared to controls (approximately1.3-mm annualized increase) than did the
An Evidence-Based Comparison of Headgear and Functional Appliance Therapy 175

headgear group (0.6-mm annualized change,P o 0.05). The Bionator group demonstrated asmall increase in SNB angle (approximately 0.61annualized) while the headgear group did not.Both treatment groups showed an annualizedreduction in overjet (approximately 2.5-mmreduction with Bionator and 1.4-mm reductionwith headgear) compared to controls. Bothshowed a mean annualized reduction in ANBangle of slightly less than 11 compared tocontrols.
In the Keeling et al.4–6 study, Class II subjectswith an average age of 9.5 years were classifiedbased upon the severity of their molar dis-toclusion and treated with headgear (cervicalpull headgear if MPA ≤ 401, high-pull headgear ifMPA4 401; N = 92) plus maxillary flat-plane biteplate, Bionator (occlusal stops, N = 79), or leftuntreated as a control (N = 78). Patients woreappliances until they were bilateral Class I or 2years lapsed.
SNA angle increased in the Bionator (0.511)and the observation groups (0.671), while itdecreased (–0.501) in the headgear/bite plategroup; SNB angle increased in the Bionator(1.361) and the observation groups (0.841),whereas it remained unchanged (0.19) in theheadgear/bite plate group; ANB angle decreasedin the Bionator (–0.851) and the headgear/biteplate groups (–0.721), and was unchanged in theobservation group; and the mandibular planeangle increased (1.301) only in the headgear/biteplane group. Compared to controls, both Bion-ator and headgear treatment corrected Class IImolar relationships, reduced overjet, andreduced apical base discrepancies (approximately1 mm). The headgear group showed a significantdental Class II correction by maxillary molarmovement. Headgear/bite plate and Bionatortreatment enhanced mandibular growth.4
A control group was not included in theGhafari et al.7 study which included 63 bilateralClass II children between the ages of 7 and 13years with ANB angles equal to or greater than4.51. The children were randomly assigned to astraight-pull headgear or a Frankel regulator (FR-II) group until they were ready for Phase IItreatment.
Both treatments were effective in correctingthe Class II, division 1 malocclusion of children.Maxillary growth was restricted with the headgear(SNA restricted by 31) and not with the FR-II
(SNA increases slightly by 0.11). Maxillary molarimprovement in occlusion, toward neutroclusion,was more significant with the headgear by about3 mm compared with the FR-II. The effect ofboth appliances on mandibular length was sim-ilar, but B point was positioned forward by about21 more with the FR-II. Headgear reduced theANB angle more than the FR-II, but the differ-ence was only 1.31. Overjet was reduced with bothappliances but larger with the FR-II. The FR-IIuprights the maxillary incisors (headgearresulted in a slight proclination) and proclinesmandibular incisors. In terms of vertical devel-opment, headgear treatment resulted in a slightincrease in SN–MP angle (11) while FR-II treat-ment resulted in a slight decrease (0.61).
In the final study,8 two groups of 30 Class IIchildren (mean age approximately 10 years) withbilateral distal molar relationships greater thanone-half cusp and an ANB angle of ≥ 4.51 weretreated with a headgear/bite plate or a Bionatorfor a mean period of 1.78 or 1.52 years, respec-tively. They were compared to a matched controlsample (N ¼ 30).
The headgear/bite plane group, but not theBionator group, restricted maxillary growth byabout 11. Mandibular protrusion was increasedin the Bionator group (SNB angle) by 0.81compared to the headgear group, but theincreases in mandibular length did not differsignificantly. The ANB angle was reduced by 11with both treatments. Maxillary incisors wereuprighted with both treatments but more withthe headgear bite plate. Maxillary molarsshowed distal movement of 1.2 mm in theheadgear/bite plate group and slight mesialmovement in the Bionator group. Mandibularmolars moved mesially significantly more in theheadgear/bite plane (2.7 mm) and Bionator(3.3 mm) groups than in the control group(1 mm). Mandibular incisors were proclined(4.21) in the Bionator group and uprighted(2.21) in the headgear/bite plane group.Headgear/bite plate and Bionator treatmentresulted in non-significant changes in the SN–GoGn angle and LAFH.
Summary (bold type indicates agreementbetween all studies, regular type indicatesdisagreement)
" Headgear: Restricts maxillary forward growthslightly (SNA decreases 11–31),1–3,7 B point
Southard et al176

(and SNB angle) does not come forwardcompared to controls,1–3,7 and the result is amean reduction in ANB angle of about 11.2,3,7
Maxillary molars are retracted distally by anaverage of up to 3.7 mm compared to con-trols1 and improve toward neutroclusion by3 mm more than with functional appliances.1,7
Overjet is reduced by approximately1.5 mm.1–3,7 Effect on observed mandibularlength increase ranges from no differencecompared to controls,1 to a small increasecompared to controls,2,3 to an increase similarto a FR-II appliance.7 Vertically, a slightincrease was found when measured atmenton1 and in the SN–MP angle.7
" Headgear with Bite plate: Restricts maxillaryforward growth slightly (0.501–11),6,8 ANBdecreases approximately 11 compared tocontrols,4–6,8 reduction in overjet isobserved,4,5 maxillary incisors uprighted,8
maxillary molars moved distally,4,5,8 mandib-ular molars moved mesially (2.7 mm com-pared to controls of 1 mm),8 and mandibularincisors were uprighted 21.8 No significantchange in SNB angle compared to controls.8
Mandibular length changes ranged from nosignificant difference compared to controls8
to enhanced mandibular growth greater thancontrols and comparable to that of aBionator.4,5 Headgear/bite plate treatmenthas been reported to increase themandibular plane angle (1.31)6 or toproduce non-significant changes in themandibular plane angle and LAFH.8
It is important tomention that a retrospectivecohort study9 examined changes in the Class IIsubjects treated with headgears from theTulloch et al.2 study and headgears/anteriorbite plates from the Keeling et al. study.4 Thebite plate provided no additional benefit whenusing a headgear for Class II treatment.Changes in SNA, SNB, ANB, and mandibularlength were not statistically significantlydifferent between the groups. The maxillaryfirst molars moved posteriorly approximatelythe same average amount in both groups, andthere was no difference in the amount of mesialmovement by the mandibular first molars. Theauthors concluded that headgear/anterior biteplate treatment provides no additionalanteroposterior dental or skeletal benefit overheadgear treatment alone.
" Activator/Bionator/FR-II:Functional appliances demonstrate a small
increase in SNB angle of approximately 0.61annualized compared to controls2,3 for a totalincrease of approximately 11–21.6–8 Thischange results in a mean annualized reductionin ANB angle (apical base discrepancy) ofslightly less than 11 compared to controls2–6
and a total ANB angle reduction of 11.7,8
Mandibular molars move mesially more thancontrols (3.3 mm versus 1 mm),8 maxillaryincisors were uprighted,7,8 and mandibularincisors were proclined (4.21).7,8 Functionalappliance treatment exhibits a large reductionin overjet (annualized 2.5 mm compared tocontrols, approximately 4 mm total).2–5,7
Effect on observed restriction of maxillaryforward growth ranges from a small meandecrease in SNA of approximately 0.7 mm1 tono restriction of maxillary growth in the greatermajority of the studies.2–8 Surprisingly, the effectof functional appliances on mandibular lengthranges from no significant change in mandib-ular length compared to headgears1,7,8 to asmall increase4,5 (unit length increase approx-imately 1.3 mm annualized change).2,3 Maxil-lary molars have been found to either movedistally by an average of nearly 1.2 mm1 or tomove mesially.8 Vertical skeletal effects rangedfrom a slight increase measured at menton1 tonon-significant changes in the mandibularplane angle,6 SN–GoGn angle, and LAFH8 toa slight decrease of the SN–MP angle.7
Q2: Are headgears and functional appliances,followed by fixed orthodontic appliances, equallyeffective in correcting Class II malocclusions inchildren?
A: Headgears and functional appliances (usedin conjunction with fixed orthodontic appliances)can effectively correct Class II malocclusions.But higher levels of evidence to answer thequestion of whether their effects are equal aremissing.
The success rate of full Class II correction inchildren has been reported to exceed 90% withboth headgear and functional appliance treat-ment (followed by fixed appliance treatment).10
However, this study was not a randomized clinicaltrial and an evaluation of higher levels ofevidence was deemed appropriate.
An Evidence-Based Comparison of Headgear and Functional Appliance Therapy 177

Children in the Tulloch et al.2 study (initiallyClass II patients who had been assigned toheadgear, Bionator, and control groups) wererandomized following those first-phase treat-ments and started on a second phase of treat-ment when they reached the early permanentdentition. Comprehensive prescription edgewisefixed appliance treatment (22 slot twin, 18 slottwin, or 18 slot single-wing brackets) was per-formed.3 Records were taken at the completionor discontinuation of comprehensive treatment.
By the end of fixed appliance therapy, theadvantages gained by previous headgear orBionator treatment were lost and there was nosignificant difference between any of the threegroups in terms of anteroposterior, vertical, anddental measures including the following: ANBangle, SNA angle, SNB angle, overjet, and PARscores. The authors point out that their sample(and therefore their findings) excluded childrenwith facial asymmetries, extremely long faces, orextremely short faces.
The weakness of this study was that there wereno restrictions on any treatment methodsemployed during the second phase of treatment.3
One of the advantages of a randomized clinicaltrial is that its designmaximizes the likelihood thatthe observed effect is due to the intervention (inthis case headgear or functional appliancetreatment). By permitting any treatmentmethod to be used during the second phase inthis study, any earlier headgear or functionalappliance effect is combined (or potentially lost)with the unknown second-phase treatment effect.A better design would have required all first-phaseheadgear or functional appliance subjects tocontinue to only use those appliances (in additionto the fixed appliances) during the second phaseof treatment.
After Phase I treatment in the Keeling et al.study,4–6 half of the subjects in the Bionator andheadgear/bite plate groups were randomlyassigned to 6 months of retention followed by 6months of no retention, and the other half of thesubjects had no retention for a year. Theretention protocol consisted of full-time wear ofthe bite plate and nighttime wear of the headgearon alternate nights for the headgear group, andalternate nighttime wear in the Bionator group.11
Records of each patient were reviewed by anaverage of four orthodontists and a consensusPhase II treatment plan formulated. During
Phase II, subjects were usually treated with fullorthodontics appliances.
By the end of full orthodontic treatment, theskeletal differences in all measurements for allthree groups were within 11. When the entiretreatment period was considered, treatmentgroup had no effect. The authors concluded thatthere is temporary skeletal change as a result ofPhase I treatment with both appliances but nodetectable skeletal difference between one-phaseand two-phase treatment of Class II malocclusionby the end of full orthodontic treatment. Also,there were no significant differences with respectto initial PAR or final PAR among the threetreatment protocols.11
Like the Tulloch et al. study,2,3 a better designwould have required all first-phase headgear orfunctional appliance subjects to continue to onlyuse those appliances (in addition to the fixedappliances) during the second phase of treat-ment. Instead, during Phase II, headgear wasused more often (42%) in the original observa-tion group subjects and in the original Bionatorgroup subjects (23%) than in the originalheadgear/bite plate (15%) group subjects. Fur-ther, the retention protocol (e.g. alternatenighttime appliance wear for a year beforestarting Phase II) was reported by the authors tobe only minimally successful at maintainingdental correction5 and must surely have cloudedthe intervention effect.
While one can understand the desire tooptimize care by choosing a treatment planimmediately prior to (or during) Phase II, such amethod shrouds the effect of headgear orfunctional appliance intervention. Betterdesigned studies are needed, but it is unlikelythat funding for another large randomizedcontrolled trial to answer this question will beforthcoming.
Q3: What are the long-term (post-retention)skeletal effects of treatment for Class II maloc-clusions in growing individuals using cervicaltraction headgear?
A: The available evidence, based largely onretrospective non-randomized studies, suggeststhat reduction of the SNA angle by treatment islargely stable, the SNB angle is largely unaffectedby treatment or continued growth, and anyincrease in mandibular plane angle caused bytreatment is recovered during continued facialgrowth. The question of whether cervical traction
Southard et al178

causes a clinically significant change in verticalfacial proportions remains equivocal.
The notion that cervical traction headgearhas a direct skeletal treatment effect on themaxilla in humans was suggested by Mitani andBrodie12 and Weislander13 and later confirmedby Melsen14 in an experiment characterizing thecervical traction treatment effect and the“physiologic recovery” in 20 subjects. By usingBjörk-type implants, serial cephalometry andsuperimposition, Melsen14 identified downwardand backward maxillary rotation, and a similarindirect effect on the mandible, as a direct resultof an 8-month application of cervical traction.After routine fixed edgewise treatment, reten-tion, and cessation of skeletal growth, these 20individuals were again evaluated by ceph-alometry. The skeletal headgear effect appearedto be temporary, as the subjects exhibited, onaverage, normal downward and forward maxil-lary and mandibular growth after being“released” from the growth alteration dictated bythe traction to the maxilla. Also, the dentoal-veolar effect of the headgear (distal maxillaryfirst molar movement) was changed duringcontinued treatment and growth. Mesialmigration of the maxillary first molars relative tocranial base, similar to migration in untreatedcontrols over the same time period, wasaccompanied by downward and forward man-dibular growth to maintain the Class I molarrelationship and preserve the intermaxillarydentoalveolar effect.14 Although individualgrowth patterns appeared to recover from thetemporary alteration of maxillary growth, thequestion of a permanent vertical change in thefacial pattern could not be determined fromthis study.
Further evidentiary support for the long-termeffects of cervical traction consists largely of non-randomized retrospective trials. A search of theliterature pertaining to human trials in all Entrezdatabases from 1978 to present, for the termsClass II malocclusion AND “headgear” OR“extraoral appliance,” returned 317 articlescontaining 43 randomized trials, five systematicreviews, and two meta-analyses. The five sys-tematic reviews evaluate treatment effects but donot analyze long-term skeletal effects.15–19 Add-ing “AND long term” to the query returned 24articles, including three randomized trials, butno systematic reviews or meta-analyses. The
three randomized trials evaluate treatmenteffects and long-term occlusal and soft tissueeffects, but do not evaluate post-retention long-term skeletal effects of treatment with head-gear.20–22 The remaining 21 articles contain nineretrospective studies evaluating skeletal changesinduced by cervical traction longitudinally to atime point after retention. Thus, at present, theevidence for long-term (post-retention) effectfrom the use of cervical traction headgear issupported by nine retrospective post-retentionanalyses. Table 1 summarizes this evidence interms of anteroposterior and vertical skeletalchange.
By and large, these studies appear to supportthe findings of earlier reports. The reduction ofSNA by maxillary traction is maintainedthroughout edgewise treatment. During con-tinued growth, changes in SNA revert to anexpected growth pattern. In contrast, the SNBangle shows little change with treatment andcontinued growth. After a transient increase inmandibular plane angle during treatment, post-treatment change suggests a return to man-dibular plane closure during continued growth.When compared with controls, the changes inmandibular position are not significantly differ-ent, suggesting the effect of cervical traction onchin projection is, on average, clinically insig-nificant. In contrast, the behavior of the Y-axis,which tracks the effect of treatment and growthon the vertical position of the chin, is variable.Two studies have reported that lower anteriorfacial height changes are not significantly dif-ferent from controls, but both studies do notagree for significant change in total face heightcompared to controls.30,31 One additional studyhas reported mandibular posterior rotation as aresult of cervical traction treatment that did notrecover 4 years post-treatment.32
Although retrospective analyses have knownweaknesses, particularly sampling bias, lack ofblinding, and lack of control groups, it is note-worthy that the cervical traction headgeartreatment effects, seemingly reproduced in thelower-quality studies shown in Table 1, aremirrored in prospective trials where headgeartherapy was randomly assigned.1,6,7
Q4: What are the long-term (post-retention)skeletal effects of treatment for Class II maloc-clusions in growing individuals using high-pull orvertical-pull headgear?
An Evidence-Based Comparison of Headgear and Functional Appliance Therapy 179
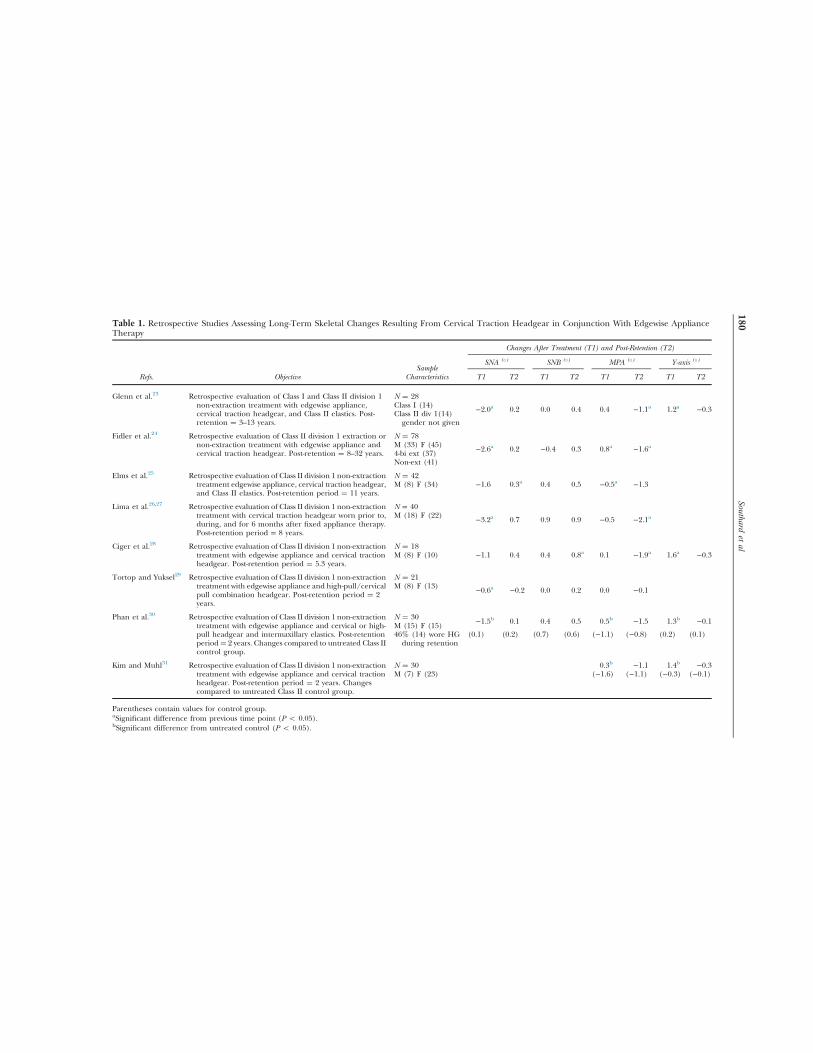
Table 1. Retrospective Studies Assessing Long-Term Skeletal Changes Resulting From Cervical Traction Headgear in Conjunction With Edgewise ApplianceTherapy
Changes After Treatment (T1) and Post-Retention (T2)
SampleSNA (1) SNB (1) MPA (1) Y-axis (1)
Refs. Objective Characteristics T1 T2 T1 T2 T1 T2 T1 T2
Glenn et al.23 Retrospective evaluation of Class I and Class II division 1non-extraction treatment with edgewise appliance,cervical traction headgear, and Class II elastics. Post-retention ¼ 3–13 years.
N ¼ 28
−2.0a 0.2 0.0 0.4 0.4 −1.1a 1.2a −0.3Class I (14)Class II div 1(14)gender not given
Fidler et al.24 Retrospective evaluation of Class II division 1 extraction ornon-extraction treatment with edgewise appliance andcervical traction headgear. Post-retention ¼ 8–32 years.
N ¼ 78
−2.6a 0.2 −0.4 0.3 0.8a −1.6aM (33) F (45)4-bi ext (37)Non-ext (41)
Elms et al.25 Retrospective evaluation of Class II division 1 non-extractiontreatment edgewise appliance, cervical traction headgear,and Class II elastics. Post-retention period ¼ 11 years.
N ¼ 42−1.6 0.3a 0.4 0.5 −0.5a −1.3M (8) F (34)
Lima et al.26,27 Retrospective evaluation of Class II division 1 non-extractiontreatment with cervical traction headgear worn prior to,during, and for 6 months after fixed appliance therapy.Post-retention period = 8 years.
N = 40
−3.2a 0.7 0.9 0.9 −0.5 −2.1aM (18) F (22)
Ciger et al.28 Retrospective evaluation of Class II division 1 non-extractiontreatment with edgewise appliance and cervical tractionheadgear. Post-retention period ¼ 5.3 years.
N ¼ 18−1.1 0.4 0.4 0.8a 0.1 −1.9a 1.6a −0.3M (8) F (10)
Tortop and Yuksel29 Retrospective evaluation of Class II division 1 non-extractiontreatment with edgewise appliance and high-pull/cervicalpull combination headgear. Post-retention period ¼ 2years.
N ¼ 21
−0.6a −0.2 0.0 0.2 0.0 −0.1M (8) F (13)
Phan et al.30 Retrospective evaluation of Class II division 1 non-extractiontreatment with edgewise appliance and cervical or high-pull headgear and intermaxillary elastics. Post-retentionperiod¼ 2 years. Changes compared to untreated Class IIcontrol group.
N ¼ 30 −1.5b 0.1 0.4 0.5 0.5b −1.5 1.3b −0.1M (15) F (15)46% (14) wore HGduring retention
(0.1) (0.2) (0.7) (0.6) (−1.1) (−0.8) (0.2) (0.1)
Kim and Muhl31 Retrospective evaluation of Class II division 1 non-extractiontreatment with edgewise appliance and cervical tractionheadgear. Post-retention period ¼ 2 years. Changescompared to untreated Class II control group.
N ¼ 30 0.3b −1.1 1.4b −0.3M (7) F (23) (−1.6) (−1.1) (−0.3) (−0.1)
Parentheses contain values for control group.aSignificant difference from previous time point (P o 0.05).bSignificant difference from untreated control (P o 0.05).
Southardet
al180

A: The immediate skeletal effects of high-pulland vertical-pull headgears are thought to be dif-ferent from that of cervical traction headgear.33–36
However, at present, a similar analysis of high-pull or vertical-pull headgear is not possiblebecause no long-term evaluations involving theexclusive use of these treatment modalities withor without edgewise treatment are available.
Q5: What are the long-term (post-retention)skeletal effects of treatment for Class II maloc-clusions in growing individuals using functionalappliances?
A: The available evidence, based largely onretrospective non-randomized studies, suggeststhat, over the long-term, functional appliances donot modify the inherited facial growth patternsignificantly. A lasting enhancement of horizontalmandibular growth is not supported for Biona-tor, Headgear–Activator, or Herbst appliances,and remains equivocal for the Fränkel FR-2appliance.
Adaptive changes in condylar growth in animalssubjected to altered (protrusive) mandibular posi-tion forms the historical basis for the clinical use offunctional appliances.37–40 However, functionalappliance use in humans has not reproduced thedramatic effects seen in animals. The magnitude ofshort-term adaptive mandibular changes in humanswas shown to be smaller, and the basis for short-termoverall increase in mandibular length was equivocal,being attributed to increased condylar growth,41–44
or the result of altered condylar growth directionwithout increased condylar growth.4,7,45–47
Long-term adaptive changes were firstaddressed in 1996, when Dermaut and Aelbers48
reviewed the scientific data on outcomes fromtreatment with various functional appliances andconcluded that, “there is so far little scientificevidence to support the idea that they have anypermanent orthopedic effect.” Within the next10 years, evaluation of more recent literatureprovided more specific support to Dermaut andAelbers' conclusion, no clinically significantanteroposterior skeletal effects aredemonstrable in long term.49–51 Additionally, itwas suggested that the findings of increasedmandibular length from functional applianceuse4,7,41–47 may be a result of adaptive change incondylar growth direction rather than condylargrowth magnitude.52 The strength of evidencefor these conclusions is considered secondary asit is based on a small number of studies.
The issue of adaptive changes to functionalappliances in the vertical dimension has receivedless attention. Numerous studies have reportedshort-term increases in anterior facial height withthe use of functional appliances,42,43,53–56 andwhether physiologic recovery occurs in the ver-tical dimension remains poorly understood.
The few long-term studies on functionalappliances that have potential answers to thesequestions are non-randomized and retrospectivein design, often without a comparison to con-trols. A summary of the long-term studies forvarious functional appliances follows.
Bionator
Although there is a long history of Class IItreatment using the Bionator,57 the skeletaltreatment effect in humans was poorlyunderstood until characterized by Buschangand co-workers in a prospective randomizedcontrolled trial using Bjork-type metallicimplants.52 Compared to control Class II subjects,Bionator therapy resulted in altered condylargrowth in a more posterior direction but nodifference in total condylar growth. Moreimportantly, Bionator therapy appeared to alterthe normal pattern of downward and forwarddisplacement of the mandible by limiting forwardmandibular rotation during growth.
The assessment of the long-term skeletal effectof Bionator therapy has not been widely studied.A search of PubMed for the terms (Class IImalocclusion) AND “Bionator” resulted in 75articles. Including the search query “AND long-term” resulted in eight articles, of which, onlyfour report longitudinal results after a retentionperiod or a post-retention period. Reporting ofcephalometric skeletal parameters is not con-sistent among the studies, with angular measuresbeing the most common. A summary of theresults of four studies reporting long-term eval-uation of changes in A point, B point, and themandibular plane angle are shown in Table 2.Treatment changes in SNA suggest the Bionatorproduces less maxillary retrusion than headgearwhile having a more protrusive effect on B pointwhen used without edgewise appliance therapy.Bionator followed by edgewise appliance therapyappears to show treatment changes in SNBremarkably similar to those found for cervicaltraction headgear followed by edgewise
An Evidence-Based Comparison of Headgear and Functional Appliance Therapy 181
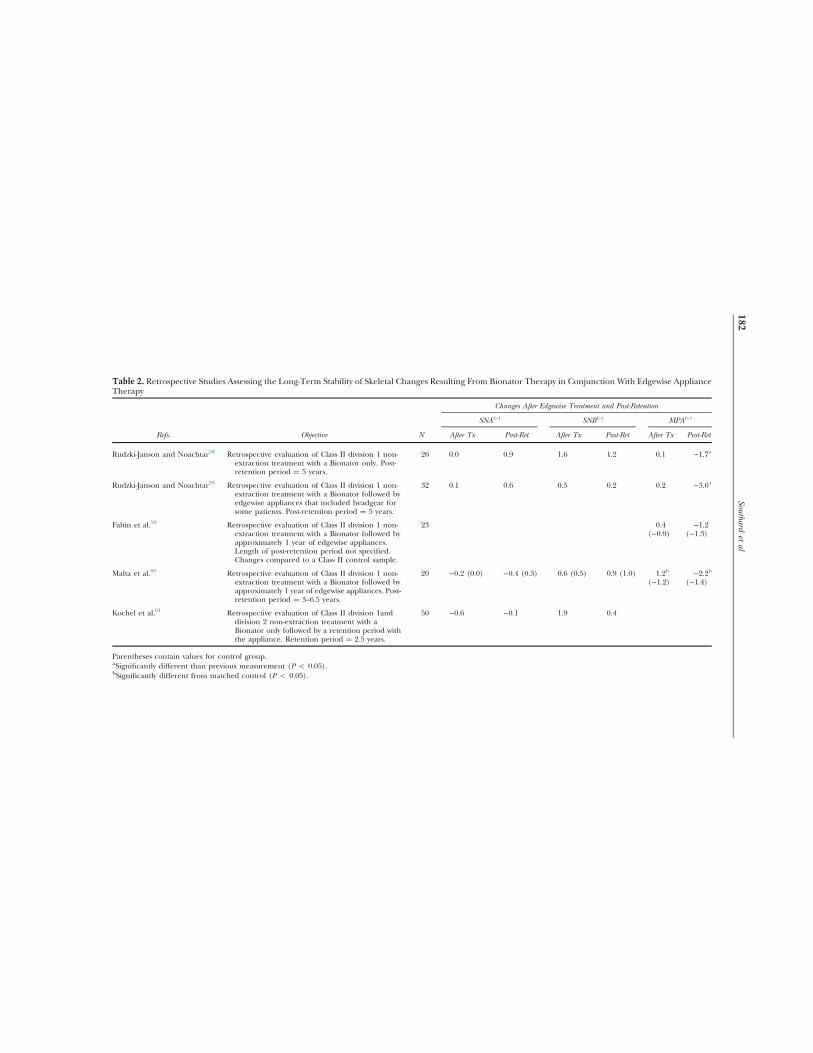
Table 2. Retrospective Studies Assessing the Long-Term Stability of Skeletal Changes Resulting From Bionator Therapy in Conjunction With Edgewise ApplianceTherapy
Changes After Edgewise Treatment and Post-Retention
SNA(1) SNB(1) MPA(1)
Refs. Objective N After Tx Post-Ret After Tx Post-Ret After Tx Post-Ret
Rudzki-Janson and Noachtar58 Retrospective evaluation of Class II division 1 non-extraction treatment with a Bionator only. Post-retention period ¼ 5 years.
26 0.0 0.9 1.6 1.2 0.1 −1.7a
Rudzki-Janson and Noachtar58 Retrospective evaluation of Class II division 1 non-extraction treatment with a Bionator followed byedgewise appliances that included headgear forsome patients. Post-retention period ¼ 5 years.
32 0.1 0.6 0.5 0.2 0.2 −3.6a
Faltin et al.59 Retrospective evaluation of Class II division 1 non-extraction treatment with a Bionator followed byapproximately 1 year of edgewise appliances.Length of post-retention period not specified.Changes compared to a Class II control sample.
23 0.4 −1.2(−0.9) (−1.3)
Malta et al.60 Retrospective evaluation of Class II division 1 non-extraction treatment with a Bionator followed byapproximately 1 year of edgewise appliances. Post-retention period ¼ 3–6.5 years.
20 −0.2 (0.0) −0.4 (0.3) 0.6 (0.5) 0.9 (1.0) 1.2b −2.2b(−1.2) (−1.4)
Kochel et al.61 Retrospective evaluation of Class II division 1anddivision 2 non-extraction treatment with aBionator only followed by a retention period withthe appliance. Retention period ¼ 2.5 years.
50 −0.6 −0.1 1.9 0.4
Parentheses contain values for control group.aSignificantly different than previous measurement (P o 0.05).bSignificantly different from matched control (P o 0.05).
Southardet
al182

appliance therapy (Table 2). Long-term changesappear to be the result of reversion to theexpected pattern of growth. The treatment effecton the mandibular plane angle and the recoveryafter treatment is also similar to that seen inlongitudinal cervical headgear studies (Table 2).One study60 reported a lasting increase inmandibular length and anterior face heightcompared to matched controls but without aconcomitant improvement in mandibularprojection as measured by SNB. Independentconfirmation of these findings is not yet available.Lasting increases in anterior facial height couldnegate the desired increase in chin projectionsought by functional appliance use.
Fränkel FR-2 Appliance
Studies evaluating the short-term effects of FR-2therapy have reported various results includingrestriction of maxillary growth, enhancement ofmandibular growth, increased lower facialheight, and occlusal correction resulting from agreater proportion of dentoalveolar compared toskeletal effects.18,42,54,62–64 The assessment oflong-term skeletal change comes from a fewstudies. A search of PubMed for the terms (ClassII malocclusion) AND “Fränkel” resulted in 97articles. Including the search query “AND long-term” resulted in five articles, only three of whichreport longitudinal results after a retentionperiod or a post-retention period for the FR-2appliance alone. Table 3 summarizes the long-term changes for selected skeletal parameterscommon between the studies. The treatmenteffects of mild restraint of maxillary horizontalgrowth and adaptive changes in mandibulargrowth and position appear to revert to ananticipated pattern over the long-term.Enlargement of mandibular size or significanttreatment effects on vertical dimension remainequivocal.
Headgear–Activator appliance
Studies evaluating the short-term effects oftreatment with a headgear–activator applianceare controversial, with reports of mainly skeletaleffects,68,69 mainly dentoalveolar effects.1,70,71 Asearch of PubMed for the terms (Class II mal-occlusion) AND “Activator” OR “HeadgearActivator” AND “long-term” resulted in four
retrospective studies evaluating skeletal effectspost-treatment and after a period of follow-up.Table 4 summarizes the long-term changes forselected skeletal parameters common betweenthe studies. The results suggest skeletal effects donot differ markedly from the use of headgearalone and appear to revert to a normal pattern ofgrowth during the post-treatment period.
Herbst appliance
By far, the most studied functional appliance, interms of long-term effect, is the Herbst appli-ance (Table 5). The results of many long-termstudies suggest that the skeletal effects of theappliance are temporary. Over the long-term,facial growth reverts to the inherited patternwith no evidence of enhanced skeletalgrowth.76–83 Studies also suggest the short-termeffect of mandibular protrusion on condylargrowth is directed more posteriorly than supe-riorly, promoting a temporary posterior man-dibular rotation56,57,82 which recovers to a moresuperiorly directed vector during growthrecovery after treatment.
Q6: Is it equally effective to correct Class IImalocclusions in growing children in early andlate mixed dentition (using headgears andfunctional appliances)?
A: YesCurrent evidence that is based on randomized
controlled trials and the Cochrane libraryreview2,3,6,7,15 suggest that there is no significantdifference in final outcomes (skeletal, dental,and soft tissue parameters) between single-phase(comprehensive orthodontic treatment follow-ing eruption of all permanent teeth) and two-phase treatments (a first-phase treatment withhead gears and functional appliances in the earlymixed dentition followed by a second-phase offixed orthodontic appliances treatment).
A systematic review conducted by Harrisonet al.15 demonstrated that a two-phase ortho-dontic treatment in children with prominentmaxillary incisors (treatment started when thechild is 7–9 years old) has no significant advan-tages over a one-phase treatment that is providedin early adolescence. This review included dataon 592 children (aged≤ 6 years) drawn from ninerandomized controlled trials examining out-comes including overjet, ANB angle, PAR scores,sagittal relationships, perception of self-esteem,
An Evidence-Based Comparison of Headgear and Functional Appliance Therapy 183

Table 3. Retrospective Studies Assessing the Long-Term Stability of Skeletal Changes Resulting From FR-2 Therapy With or Without Adjunctive EdgewiseAppliance Therapy
Authors, Year Perillo et al.65 Perillo et al.66 Freeman et al.67
Objectives
Retrospective evaluation of patients classified as ClassII division 1 specifically associated with skeletalmandibular retrusion. Treatment with the FR-2appliance 18 h/d for at least 1 year. Applianceconstruction according to Fränkel. Supplementaltreatment after FR-2 included 6–12 months offixed edgewise appliances or removableappliances to refine the occlusion. Among thepatients, 42% (6) were retained with an activatorappliance to maintain sagittal relationships.N ¼ 14; M (8) F (6). (T0–T1) ¼ FR-2 treatmentperiod including supplemental treatment.(T1–T2) ¼ post-treatment period.
Retrospective evaluation of patients classified as ClassII division 1 specifically associated with skeletalmandibular retrusion. Subjects with initial valuesof SNA 4 841; SNB 4 781; and SN–GoMe 4 361were excluded. Treatment with the FR-2 appliance18 h/d for at least 1 year. Appliance constructionaccording to Fränkel. Supplemental treatmentafter FR-2 included 6–12 months of fixed edgewiseappliances with headgear for some patients.
Retrospective evaluation of patients classified as ClassII division 1 specifically associated with excessiveoverjet and full-step Class II molar relationship.Treatment with FR-2 for 2–2.5 years of full-timewear, 1.5–2 years of 16 h/d wear, and 1.5 years of 8h/d wear. Appliance construction according toFränkel. No other treatment performed. N ¼ 30;M (17) F (13). (T0–T2) ¼ FR-2 treatment periodand post-treatment period.
N ¼ 19; M (8) F (11). (T0–T1) ¼ FR-2 treatmentperiod including supplemental treatment.(T1–T2) ¼ post-treatment period.
Control samples
T0–T1 controls from University of Naples matchedfor age, sex, and skeletal characteristics. N¼ 14; M(8) F (6). Observation period ¼ 1.5 years.
T0–T1 controls from University of Naples matchedfor age, sex, and skeletal characteristics. N ¼ 9; M(6) F (3). Observation period ¼ 1.5 years.
T0–T2 controls from University of MichiganElementary and Secondary School Growth Studymatched for age, sex, and skeletal maturity.N ¼ 20; M (11) F (9). Observation period ¼ 9.7years.
T1–T2 controls from University of MichiganElementary and Secondary School Growth Studymatched for age, and sex. N ¼ 14; M (8) F (6).Observation period ¼ 5.2 years.
No controls compared for the period T1–T2.
Observation period T0–T1 ¼ 1.5 years T1–T2 ¼ 5.2 years T0–T1 ¼ 1.5 years T1–T2 ¼ 10 years T0–T2 ¼ 9.9 yearsSNA (1) −0.3 (0.2) −0.5 (0.4) −0.5 (0.5)a −0.4 0.0 (0.7)SNB (1) 1.2 (0.5) 1.0 (1.1) 1.0 (0.9) 1.0 3.5a (1.8)ANB (1) −1.5 (−0.3)a −1.6 (−0.7) −1.4 (0.1)a −1.4 –3.5 (−1.3)cSn–GoMe (1) 0 (−0.5) −2.1 (−2.7) −0.8 (0.0) −1.7FMA (1) −0.9 (0.0) −2.0 –2.1 (−2.8)Gonial Angle (1) −1.3 (−0.3) −3.1 (−3.3) −0.5 (−0.3) 4.6 −5.0 (−5.6)Ar–Go (mm) 2.6 (2.0) 7.3 (4.3)Go–Pg (mm) 3.8 (1.7)b 7.8 (6.1) 2.9 (2.0) 8.3Ar–Gn (mm) 5.0 (2.7)a 14.0 (10.3)Co–Gn (mm) 4.4 (3.6) 12.5 20.6 (17.6)a
Parentheses contain values for control group.aSignificant difference at P o 0.05.bP o 0.01.cP o 0.001.
Southardet
al184
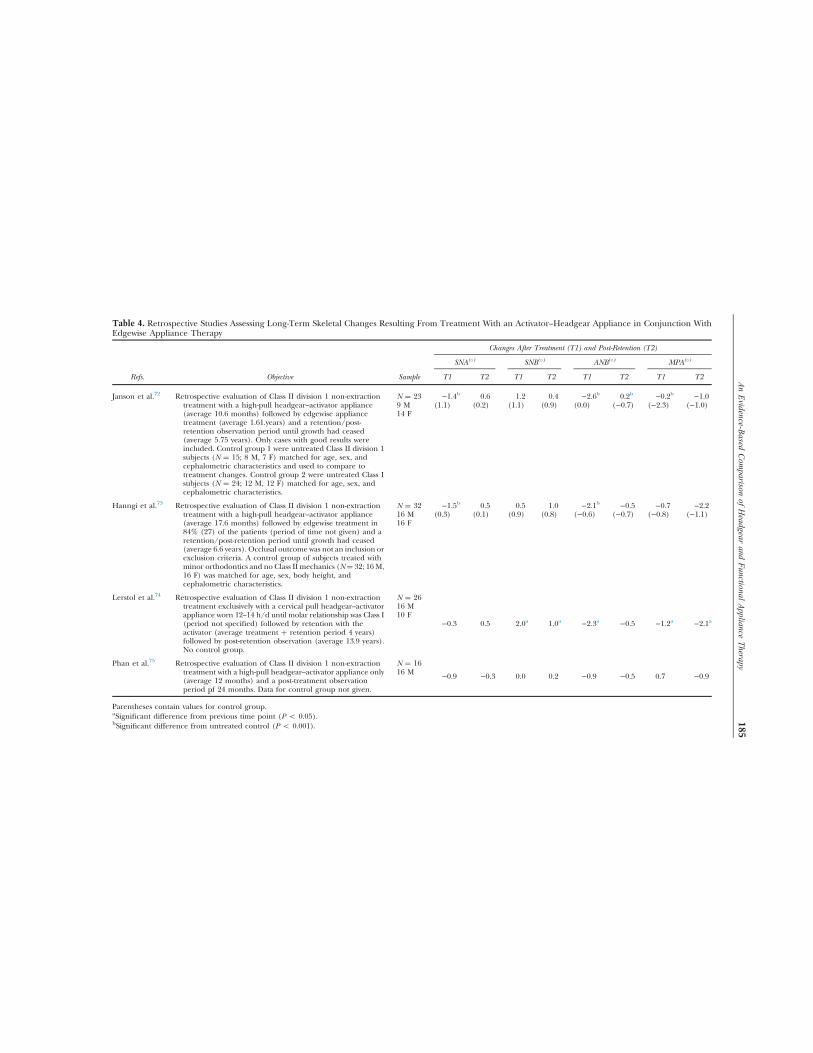
Table 4. Retrospective Studies Assessing Long-Term Skeletal Changes Resulting From Treatment With an Activator–Headgear Appliance in Conjunction WithEdgewise Appliance Therapy
Changes After Treatment (T1) and Post-Retention (T2)
SNA(1) SNB(1) ANB(1) MPA(1)
Refs. Objective Sample T1 T2 T1 T2 T1 T2 T1 T2
Janson et al.72 Retrospective evaluation of Class II division 1 non-extractiontreatment with a high-pull headgear–activator appliance(average 10.6 months) followed by edgewise appliancetreatment (average 1.61.years) and a retention/post-retention observation period until growth had ceased(average 5.75 years). Only cases with good results wereincluded. Control group 1 were untreated Class II division 1subjects (N ¼ 15; 8 M, 7 F) matched for age, sex, andcephalometric characteristics and used to compare totreatment changes. Control group 2 were untreated Class Isubjects (N ¼ 24; 12 M, 12 F) matched for age, sex, andcephalometric characteristics.
N ¼ 23 −1.4b 0.6 1.2 0.4 −2.6b 0.2b −0.2b −1.09 M (1.1) (0.2) (1.1) (0.9) (0.0) (−0.7) (−2.3) (−1.0)14 F
Hanngi et al.73 Retrospective evaluation of Class II division 1 non-extractiontreatment with a high-pull headgear–activator appliance(average 17.6 months) followed by edgewise treatment in84% (27) of the patients (period of time not given) and aretention/post-retention period until growth had ceased(average 6.6 years). Occlusal outcome was not an inclusion orexclusion criteria. A control group of subjects treated withminor orthodontics and no Class II mechanics (N¼ 32; 16 M,16 F) was matched for age, sex, body height, andcephalometric characteristics.
N ¼ 32 −1.5b 0.5 0.5 1.0 −2.1b −0.5 −0.7 −2.216 M (0.3) (0.1) (0.9) (0.8) (−0.6) (−0.7) (−0.8) (−1.1)16 F
Lerstol et al.74 Retrospective evaluation of Class II division 1 non-extractiontreatment exclusively with a cervical pull headgear–activatorappliance worn 12–14 h/d until molar relationship was Class I(period not specified) followed by retention with theactivator (average treatment þ retention period 4 years)followed by post-retention observation (average 13.9 years).No control group.
N ¼ 26
−0.3 0.5 2.0a 1.0a −2.3a −0.5 −1.2a −2.1a
16 M10 F
Phan et al.75 Retrospective evaluation of Class II division 1 non-extractiontreatment with a high-pull headgear–activator appliance only(average 12 months) and a post-treatment observationperiod pf 24 months. Data for control group not given.
N ¼ 16
−0.9 −0.3 0.0 0.2 −0.9 −0.5 0.7 −0.916 M
Parentheses contain values for control group.aSignificant difference from previous time point (P o 0.05).bSignificant difference from untreated control (P o 0.001).
AnEvidence-B
asedCom
parisonof
Headgear
andFunctional
Appliance
Therapy185
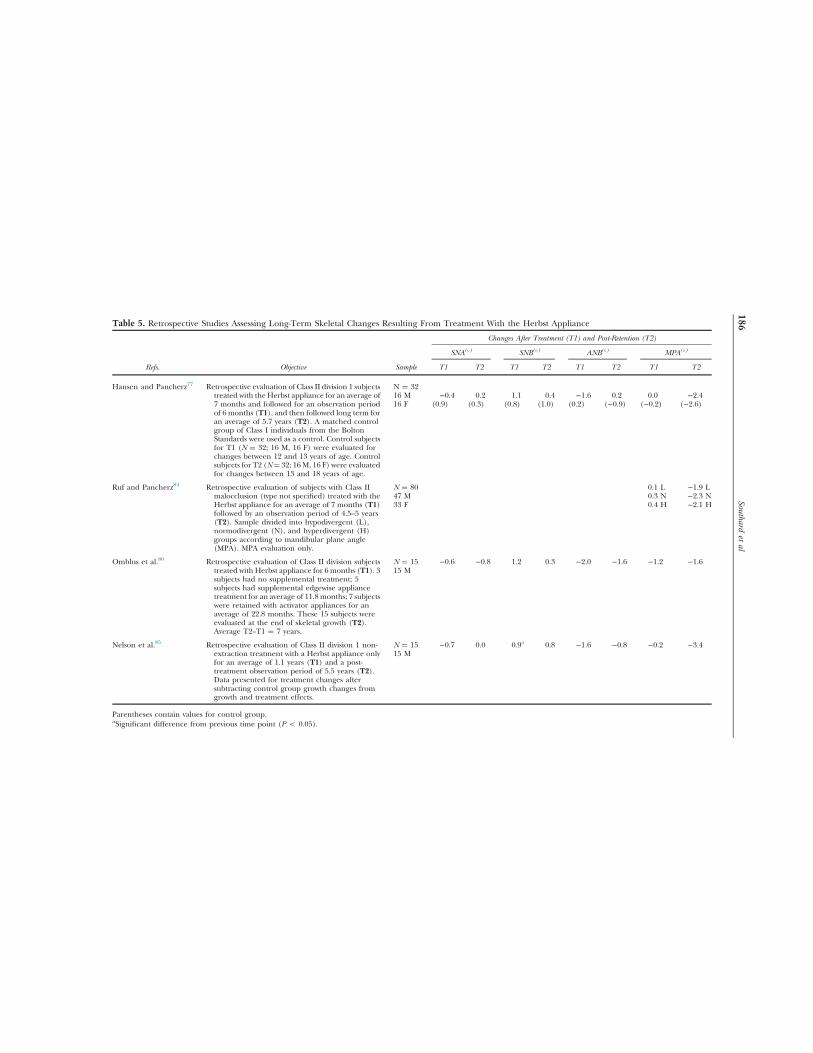
Table 5. Retrospective Studies Assessing Long-Term Skeletal Changes Resulting From Treatment With the Herbst Appliance
Changes After Treatment (T1) and Post-Retention (T2)
SNA(1) SNB(1) ANB(1) MPA(1)
Refs. Objective Sample T1 T2 T1 T2 T1 T2 T1 T2
Hansen and Pancherz77 Retrospective evaluation of Class II division 1 subjectstreated with the Herbst appliance for an average of7 months and followed for an observation periodof 6 months (T1), and then followed long term foran average of 5.7 years (T2). A matched controlgroup of Class I individuals from the BoltonStandards were used as a control. Control subjectsfor T1 (N ¼ 32; 16 M, 16 F) were evaluated forchanges between 12 and 13 years of age. Controlsubjects for T2 (N¼ 32; 16 M, 16 F) were evaluatedfor changes between 13 and 18 years of age.
N ¼ 3216 M −0.4 0.2 1.1 0.4 −1.6 0.2 0.0 −2.416 F (0.9) (0.3) (0.8) (1.0) (0.2) (−0.9) (−0.2) (−2.6)
Ruf and Pancherz84 Retrospective evaluation of subjects with Class IImalocclusion (type not specified) treated with theHerbst appliance for an average of 7 months (T1)followed by an observation period of 4.5–5 years(T2). Sample divided into hypodivergent (L),normodivergent (N), and hyperdivergent (H)groups according to mandibular plane angle(MPA). MPA evaluation only.
N ¼ 80 0.1 L −1.9 L47 M 0.3 N −2.3 N33 F 0.4 H −2.1 H
Omblus et al.80 Retrospective evaluation of Class II division subjectstreated with Herbst appliance for 6 months (T1). 3subjects had no supplemental treatment; 5subjects had supplemental edgewise appliancetreatment for an average of 11.8 months; 7 subjectswere retained with activator appliances for anaverage of 22.8 months. These 15 subjects wereevaluated at the end of skeletal growth (T2).Average T2–T1 ¼ 7 years.
N ¼ 15 −0.6 −0.8 1.2 0.3 −2.0 −1.6 −1.2 −1.615 M
Nelson et al.85 Retrospective evaluation of Class II division 1 non-extraction treatment with a Herbst appliance onlyfor an average of 1.1 years (T1) and a post-treatment observation period of 5.5 years (T2).Data presented for treatment changes aftersubtracting control group growth changes fromgrowth and treatment effects.
N ¼ 15 −0.7 0.0 0.9a 0.8 −1.6 −0.8 −0.2 −3.415 M
Parentheses contain values for control group.aSignificant difference from previous time point (P o 0.05).
Southardet
al186

injury to maxillary anterior teeth, tempor-omandibular joint problems, patient satisfaction,and number of visits needed to complete treat-ment. The included randomized trials were car-ried out in several countries, included samplesthat were representative of the population groupof interest, and were deemed to be of moderate tohigh quality. Consequently, the results are con-sidered to be both internally and externally valid.In summary, following a Phase I treatment withheadgears and functional appliances, the resultsof the review indicated that the children treatedwith headgears had a small but significant effecton reducing overjet (−1.07 mm) compared tountreated controls. There were no significantdifferences in overjet or ANB angle changes whenthe effects were compared between headgear andfunctional appliances groups. Results of thereview indicate that at the end of final fixedappliances therapy that started during ado-lescence, there were no significant differences inoverjet, ANB angle, or PAR scores between chil-dren who had a Phase I treatment with headgearor a functional appliance and those who did nothave a Phase I treatment.
Ghafari et al.7 conducted a randomized clinicaltrial to evaluate outcomes following early treatmentof Class II division I malocclusion with headgearand Frankel regulator in a sample of 63 prepubertalchildren. Outcomes examined included molar andcanine relationships, overjet, and intermolar/intercanine distances. The results of this trialshowed that both headgears and Frankelregulators are equally effective in correcting ClassII division I malocclusions. However, treatment inlate childhood is as effective as treatment in mid-childhood. The results suggest that the headgearhas a distalizing effect on the maxilla and maxillaryfirst molars while having minimal effects on max-illary incisors. On the other hand, the Frankelregulator restrains the growth of A point, causesretroclination of the maxillary incisors, proclinationof the mandibular incisors, and more forwardpositioning of the mandible.
Dolce et al.6 conducted a randomized clinicaltrial over a ten-year period comparing differ-ences in efficacy of one-phase and two-phasetreatments in 261 children with Class II maloc-clusions. During the Phase I treatment, theeffects of Bionator and headgear/bite plane werecompared with each other and with untreatedcontrols. The results of the early intervention
showed that treatment with either Bionator orheadgear/bite plane decreased the ANB anglecompared to controls. Treatment with head-gear/bite plane increased the mandibular planeangle compared to controls. When skeletal out-comes were compared between children thatunderwent one-phase treatment (fixed ortho-dontic appliances on permanent teeth) andthose that underwent a two-phase treatment(Bionator or headgear/bite plane in the firstphase followed by fixed orthodontic appliancesin the second phase), there were no clinicallymeaningful differences between the two treat-ment modalities.
Tulloch et al.3 conducted a randomizedclinical trial to examine differences intreatment outcomes in patients with severeClass II malocclusions (overjet 4 7 mm) thatunderwent a two-phase treatment versus a one-phase treatment. This study examined outcomesin 137 patients that completed treatment. Bothan intention-to-treat analysis and efficacy analysiswere conducted to assess the effectiveness of thetwo treatment modalities. For those that under-went the two-phase treatment, during the firstphase (started before adolescence in the mixeddentition), head gears or functional applianceswere used and compared with untreated con-trols. During adolescence, both treatment groupsreceived fixed orthodontic appliances and fol-lowed till completion of treatment. The results ofthis trial demonstrated that a two-phase treat-ment was no more effective than a one-phasetreatment. Early intervention did not reduce thecomplexity for later fixed appliance treatmentnor did it significantly reduce the proportion ofpatients that necessitated extractions andorthognathic surgery.
Q7: How good is the current empiricalframework examining the efficacy of functionalappliances and headgears for Class II correction?
A: A quality assessment of 12 meta-analysis/systematic reviews examining the efficacy offunctional appliances and headgears for Class IIcorrection was conducted. Overall, the quality ofthe meta-analysis/systematic reviews was “Moder-ate to High.” There is a paucity of well-conductedcontrolled clinical trials, and conclusions drawnfrom these meta-analysis/systematic reviews arebased on a secondary level of evidence. The resultsof the meta-analysis and systematic reviews suggestthat early treatment with functional appliances and
An Evidence-Based Comparison of Headgear and Functional Appliance Therapy 187

headgears result in only mild skeletal changes thatmay not be clinically meaningful. A two-phasedtreatment with these appliances does not confersignificant advantages over a one-phasedtreatment.
In orthodontics, as in all other medical anddental specialties, there is an increasing emphasison following evidence-based protocols for clinicaldecision making. Well-conducted meta-analysisand systematic reviews based on randomizedcontrolled clinical trials occupy the highestechelon of evidence-based framework. ThePubMed query tool was used to select “Meta-analysis” and “Systematic Reviews” that focused on“Functional Appliance Treatment for Class IImalocclusions,” “Orthodontic Headgear,” or“Headgear for Class II malocclusions” during theyears 2000 through June 2012. Only English lan-guage articles that examined outcomes in humansubjects were reviewed. A measurement tool toassess systematic reviews (AMSTAR) guidelineswas used for evaluating the quality of meta-analyses and systematic reviews.86,87 AMSTAR isreported to be one of the most reliable, valid, andfeasible tool to assess meta-analysis/systematicreviews.86,87 There are 11 checklist items in theAMSTAR guideline tool and a score of 1 wasassigned for each criterion that the includedarticles met/satisfied.
A total of 12 meta-analysis/systematic reviewsmet the inclusion criteria and were analyzed bythe AMSTAR tool.15,64,88–97 Of these 12 studies,only five conducted a formal meta-analysis andpresented pooled estimates (Table 6). Thewide heterogeneity of the patient populationprecluded the investigators from obtainingpooled estimates for various outcomes in theremaining seven studies. Only one meta-analysis/systematic review conducted a testfor publication bias using a funnel plot or anEgger regression test.89 Two studies mentionedthat they could not conduct a statisticalassessment of publication bias because of thelow number of clinical trials included in theirreview.15,97 Overall, the quality score rangedfrom a low of 7 to a high of 10, thus suggestingthat the quality of meta-analysis and systematicreviews were “Moderate to High” (Table 7).The majority of the published meta-analysis/systematic reviews reported that theirconclusions were drawn from a secondarylevel of evidence owing to the paucity of
methodologically rigorously conducted trueexperimental designs such as randomizedcontrolled trials. Other critical issues thatthese meta-analysis/systematic reviewshighlight include lack of sufficient samplesize, non-conduct of power analysis, errors inuse of statistical testing, retrospective nature ofthe design, and lack of adequate control groupsin the included studies.
The conclusions of the meta-analyses and sys-tematic reviews are summarized in Table 7. Insummary, the results suggest that functionalappliances induce dental, skeletal, and soft tissuechanges in subjects with Class II malocclusions.However, some of these changes may not beclinically significant. When one-phase and two-phase treatments were compared; it was found thata two-phase treatment with the use of headgears orfunctional appliances did not confer clinicallymeaningful advantages over an one-phased treat-ment option. When the anchorage potential ofheadgears and surgically reinforced devices such aspalatal implants ormini-implants were examined, itwas evident that surgically assisted anchoragereinforcements were more effective in preventinganchorage loss. It should also be kept in perspectivethat the conclusions of the meta-analyses/system-atic reviews were drawn mostly from a secondarylevel of evidence thus warranting the need formore rigorously conducted controlled clinical trialsfor clinical decision making.
Q8: Is profile improvement better in growingClass II patients treated with headgear or Herbstappliances?
A: Both treatments result in significantlyimproved profiles that are similarly attractive.
Although the skeletal and dental effects oftreatment with Herbst appliances or headgearsdiffer, both treatments are effective in correctingClass II malocclusions. To study their effects onprofile, lateral cephalometric radiographs ofclosely matched pairs of growing Class II division 1patients treated with either the Herbst applianceor headgear (both combined with fixed appli-ances and treated to a Class I molar relationship)were used to generate pretreatment and post-treatment standardized silhouettes.98 Thesilhouettes were randomly arranged and judgedby laypeople. Significant profile improvementswith treatment occurred with both Herbsttreatment and headgear treatment. There wereno statistically significant differences between
Southard et al188

Table 6. AMSTAR Checklista and the Number of Studies That Satisfied Each of the Criteria
Items AMSTAR QuestionDone,N (%)
Not Done,N (%)
Cannot Tell,N (%)
Not Applicable,N (%)
1 Was an ‘a priori’ design provided? 12 (100) 0 0 0The research question and inclusion criteria should be established before the conduct of the review.
2 Was there duplicate study selection and data extraction? 9 (75) 3 (25) 0 0There should be at least two independent data extractors and a consensus procedure for disagreementsshould be in place.
3 Was a comprehensive literature search performed? 11 (92) 1 (8) 0 0At least two electronic sources should be searched. The report must include years and databases used(e.g. Central, EMBASE, and MEDLINE). Key words and/or MESH terms must be stated and wherefeasible the search strategy should be provided.
4 Was the status of publication (i.e. grey literature) used as an inclusion criterion? 12 (100) 0 0 0The authors should state that they searched for reports regardless of their publication type. The authorsshould state whether or not they excluded any reports (from the systematic review), based on theirpublication status, language, etc.
5 Was a list of studies (included and excluded) provided? 12 (100) 0 0 0A list of included and excluded studies should be provided.
6 Were the characteristics of the included studies provided? 12 (100) 0 0 0In an aggregated form such as a table, data from the original studies should be provided on theparticipants, interventions, and outcomes.
7 Was the scientific quality of the included studies assessed and documented? 12 (100) 0 0 0‘A priori’ methods of assessment should be provided (e.g., for effectiveness studies if the author(s)chose to include only randomized, double-blind, placebo-controlled studies, or allocation concealmentas inclusion criteria); for other types of studies alternative items will be relevant.
8 Was the scientific quality of the included studies used appropriately in formulating conclusions? 12 (100) 0 0 0The results of the methodological rigor and scientific quality should be considered in the analysis andthe conclusions of the review, and explicitly stated in formulating recommendations.
9 Were the methods used to combine the findings of studies appropriate? 5 (42) 0 0 7 (58)For the pooled results, a test should be done to ensure the studies were combinable to assess theirhomogeneity (i.e. Chi-squared test for homogeneity).
10 Was the likelihood of publication bias assessed? 1 (8) 9 (75) 2 (17) 0An assessment of publication bias should include a combination of graphical aids (e.g., funnel plot,other available tests) and/or statistical tests (e.g., Egger regression test).
11 Was the conflict of interest stated? 12 (100)bPotential sources of support should be clearly acknowledged in both the systematic review and theincluded studies.
aAMSTAR checklist obtained from Shea and Hamel.87bAll journals require authors to submit a “Conflict of Interest” statement. Regardless of the actual mention of this in the published article, it was assumed that all meta-analyses,systematic reviews, and included studies met this criteria.
AnEvidence-B
asedCom
parisonof
Headgear
andFunctional
Appliance
Therapy189
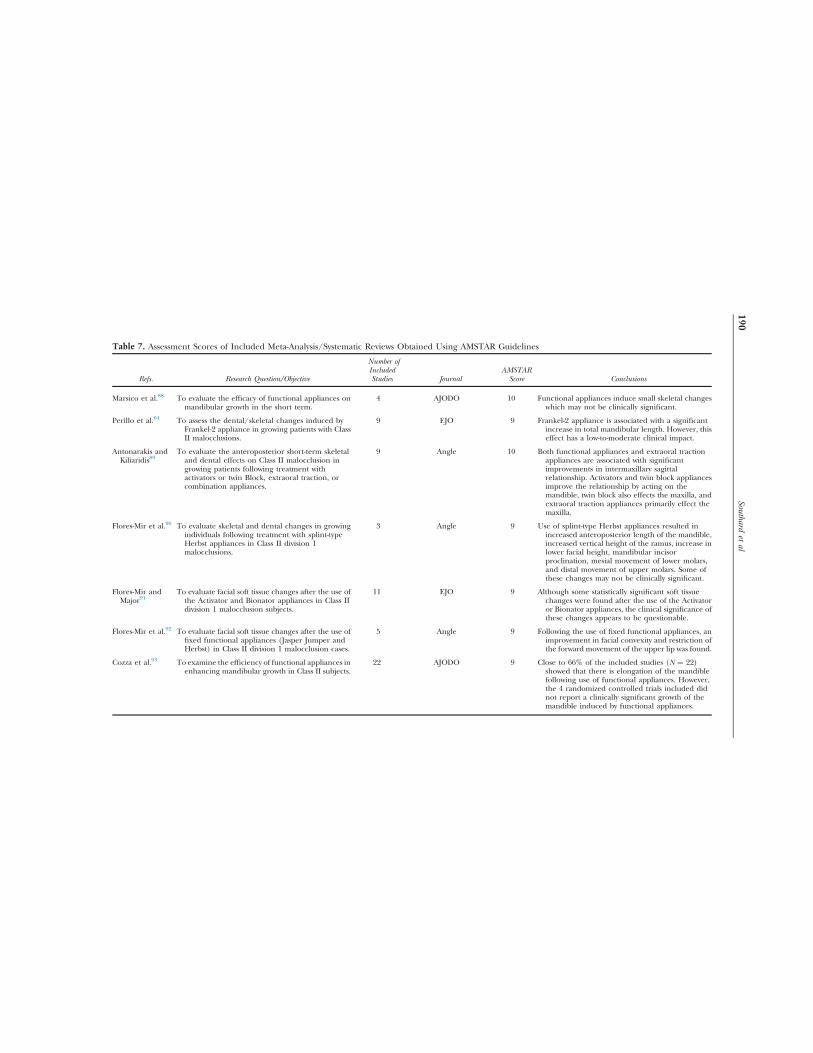
Table 7. Assessment Scores of Included Meta-Analysis/Systematic Reviews Obtained Using AMSTAR Guidelines
Refs. Research Question/Objective
Number ofIncludedStudies Journal
AMSTARScore Conclusions
Marsico et al.88 To evaluate the efficacy of functional appliances onmandibular growth in the short term.
4 AJODO 10 Functional appliances induce small skeletal changeswhich may not be clinically significant.
Perillo et al.64 To assess the dental/skeletal changes induced byFrankel-2 appliance in growing patients with ClassII malocclusions.
9 EJO 9 Frankel-2 appliance is associated with a significantincrease in total mandibular length. However, thiseffect has a low-to-moderate clinical impact.
Antonarakis andKiliaridis89
To evaluate the anteroposterior short-term skeletaland dental effects on Class II malocclusion ingrowing patients following treatment withactivators or twin Block, extraoral traction, orcombination appliances.
9 Angle 10 Both functional appliances and extraoral tractionappliances are associated with significantimprovements in intermaxillary sagittalrelationship. Activators and twin block appliancesimprove the relationship by acting on themandible, twin block also effects the maxilla, andextraoral traction appliances primarily effect themaxilla.
Flores-Mir et al.90 To evaluate skeletal and dental changes in growingindividuals following treatment with splint-typeHerbst appliances in Class II division 1malocclusions.
3 Angle 9 Use of splint-type Herbst appliances resulted inincreased anteroposterior length of the mandible,increased vertical height of the ramus, increase inlower facial height, mandibular incisorproclination, mesial movement of lower molars,and distal movement of upper molars. Some ofthese changes may not be clinically significant.
Flores-Mir andMajor91
To evaluate facial soft tissue changes after the use ofthe Activator and Bionator appliances in Class IIdivision 1 malocclusion subjects.
11 EJO 9 Although some statistically significant soft tissuechanges were found after the use of the Activatoror Bionator appliances, the clinical significance ofthese changes appears to be questionable.
Flores-Mir et al.92 To evaluate facial soft tissue changes after the use offixed functional appliances (Jasper Jumper andHerbst) in Class II division 1 malocclusion cases.
5 Angle 9 Following the use of fixed functional appliances, animprovement in facial convexity and restriction ofthe forward movement of the upper lip was found.
Cozza et al.93 To examine the efficiency of functional appliances inenhancing mandibular growth in Class II subjects.
22 AJODO 9 Close to 66% of the included studies (N ¼ 22)showed that there is elongation of the mandiblefollowing use of functional appliances. However,the 4 randomized controlled trials included didnot report a clinically significant growth of themandible induced by functional appliances.
Southardet
al190

Chen et al.94 To examine if functional appliances enhancemandibular growth in the treatment of skeletalClass II malocclusions.
6 AJODO 7 There is no definitive evidence on the efficacy offunctional appliance therapy.
Flores-Mir andMajor95
To evaluate facial soft tissue changes after the use ofthe twin block appliance in Class II division 1malocclusion cases.
2 Angle 9 There is no evidence that twin block appliancesimproves facial convexity.
Harrison et al.15 To examine the effectiveness of early orthodontictreatment (with functional appliances or headgears) in patients (aged 7–9 years ) with Class IImalocclusions.
8 Cochrane DatabaseSystematic Review
10 Use of functional appliances or headgears results inreduction in prominence of maxillary incisors.However, the overall outcomes (overjet, ANBangle, or PAR scores) between one-phase and two-phase treatment groups are not dissimilar at theend of treatment. A two-phase treatment confersno clinically meaningful advantages over a one-phase treatment.
Li et al.96 To compare the effects of implants and headgear onanterior teeth retraction in patients with Class IIdivision I malocclusions or anterior segmentcrowding.
8 Angle 10 Skeletal anchorage through mid-palatal implants,mini-implants, and onplants are more effectivethan headgears for maintaining anchorage duringanterior teeth retraction.
Skeggs et al.97 To compare the anchorage potential of surgicallyassisted anchorage reinforcement devices (such asmid-palatal implants) and headgears.
1 Cochrane DatabaseSystematic Review
9 Mid-palatal implants could serve as an acceptablealternative to headgear-reinforced anchorage.However, this need further empirical supportfrom well-conducted controlled clinical trials.
Table 7. (continued)
Refs. Research Question/Objective
Number ofIncludedStudies Journal
AMSTAR ScoreConclusions
AnEvidence-B
asedCom
parisonof
Headgear
andFunctional
Appliance
Therapy191

Herbst or headgear treatment in average finalprofile scores. Example silhouettes of patients whodemonstrated the mean esthetic improvement fortheir respective treatment group are shown inFig. 1 (headgear group) and Fig. 2 (Herbstgroup). In another study,10 Herbst treatmenthad a greater favorable impact on soft tissuechin advancement compared to headgeartreatment, but one must remember that profilesinclude many features in addition to chinprojection.
Q9: Do functional appliance and headgeartherapies differ when it comes to a child's qualityof life during treatment?
A: No.Oral health-related quality of life was studied
in groups of children treated with headgears andfunctional appliances (twin blocks).99 Childrenresponded to questions concerning frequency ofbad breath and mouth sores, functionallimitations, emotional well-being, and socialwell-being. Results revealed that functional and
Figure 1. Initial (left) and final (right) silhouettes for a headgear patient demonstrating mean headgear groupimprovement.
Figure 2. Initial (left) and final (right) silhouettes for a Herbst patient demonstrating mean Herbst groupimprovement.
Southard et al192
headgear appliances do not differ in terms ofimpact on daily life during treatment.
References1. Jakobsson S: Cephalometric evaluation of treatment
effect on Class II, division 1 malocclusions. Am J Orthod53:446-457, 1967
2. Tulloch C, Phillips C, Koch G, et al: The effect of earlyintervention on skeletal pattern in Class II malocclusion:a randomized clinical trial. Am J Orthod DentofacialOrthop 111:391-400, 1997
3. Tulloch C, Proffit W, Phillips C: Outcomes in a 2-phaserandomized clinical trial of early Class II treatment. Am JOrthod Dentofacial Orthop 125:657-667, 2004
4. Keeling S, Wheeler T, King G, et al: Anteroposteriorskeletal and dental changes after early Class II treatmentwith Bionators and headgear. Am J Orthod DentofacialOrthop 113:40-50, 1998
5. Wheeler T, McGorray S, Dolce C, et al: Effectiveness ofearly treatment of Class II malocclusion. Am J OrthodDentofacial Orthop 121:9-17, 2002
6. Dolce C, McGorray S, Brazeau L, et al: Timing of Class IItreatment: skeletal changes comparing 1-phase and2-phase treatment. Am J Orthod Dentofacial Orthop132:481-489, 2007
7. Ghafari J, Shofer F, Jacobsson-Hunt U, et al: Headgearversus function regulator in the early treatment of ClassII, division 1 malocclusion: a randomized clinical trial.Am J Orthod Dentofacial Orthop 113:51-61, 1998
8. Almeida-Pedrin R, Almeida M, Almeida R, et al: Treat-ment effects of headgear biteplane and Bionator appli-ances. Am J Orthod Dentofacial Orthop 132:191-198,2007
9. Thurman M, King G, Ramsay D, et al: The effect of ananterior biteplate on dental and skeletal Class IIcorrection using headgears: a cephalometric study.Orthod Craniofac Res 14:213-221, 2011
10. Baccetti T, Franchi L, Stahl F: Comparison of 2comprehensive Class II treatment protocols includingthe bonded Herbst and headgear appliances: a double-blind study of consecutively treated patients at puberty.Am J Orthod Dentofacial Orthop 135:698.e1-698.e10,2009
11. King G, McGorray S, Wheeler T, et al: Comparison ofpeer assessment ratings (PAR) from 1-phase and 2-phasetreatment protocols for Class II malocclusions. Am JOrthod Dentofacial Orthop 123:489-496, 2003
12. Mitani H, Brodie AG: Three plane analysis of toothmovement, growth and angular changes with cervicaltraction. Angle Orthod 40:80, 1970
13. Wieslander L: The effect of force on crania-facialdevelopment. Am J Orthod 65:531-538, 1974
14. Melsen B: Effect of cervical anchorage during and aftertreatment: an implant study. Am J Orthod 73:526-540,1978
15. Harrison JE, O'Brien KD, Worthington HV: Orthodontictreatment for prominent upper front teeth in children.Cochrane Database Syst Rev 18(3):CD003452, 2007
16. Hans MG, Teng CM, Liao CC, et al: An evidence-basedapproach to treatment of open bite and deep bite: casereports. World J Orthod 8(1):45-64, 2007
17. Millett DT, Cunningham SJ, O'Brien KD, et al: Ortho-dontic treatment for deep bite and retroclined upperfront teeth in children. Cochrane Database Syst Rev 18(4):CD005972, 2006
18. Bondemark L, Karlsson I: Extraoral vs intraoral appliancefor distal movement of maxillary first molars: a random-ized controlled trial. Angle Orthod 75(5):699-706, 2005
19. Tulloch JF, Medland W, Tuncay OC: Methods used toevaluate growth modification in Class II malocclusion.Am J Orthod Dentofacial Orthop 98(4):340-347, 1990
20. Virkkula T, Kantomaa T, Julku J, et al: Long-term soft-tissue response to orthodontic treatment with earlycervical headgear—a randomized study. Am J OrthodDentofacial Orthop 135(5):586-596, 2009
21. Krusinskiene V, Kiuttu P, Julku J, et al: A randomizedcontrolled study of early headgear treatment on occlusalstability—a 13 year follow-up. Eur J Orthod 30(4):418-424, 2008
22. Pirttiniemi P, Kantomaa T, Mäntysaari R, et al: Theeffects of early headgear treatment on dental arches andcraniofacial morphology: an 8 year report of a random-ized study. Eur J Orthod 27(5):429-436, 2005
23. Glenn G, Sinclair PM, Alexander RG: Nonextractionorthodontic therapy: posttreatment dental and skeletalstability. Am J Orthod Dentofacial Orthop 92:321-328,1987
24. Fidler BC, Årtun J, Joondeph RD, et al: Long-termstability of angle Class II, division 1 malocclusions withsuccessful occlusal results at end of active treatment. Am JOrthod Dentofacial Orthop 107:276-285, 1995
25. Elms TN, Buschang PH, Alexander RG: Long-termstability of Class II, division 1, nonextraction cervicalface-bow therapy: II. Cephalometric analysis. Am JOrthod Dentofacial Orthop 109:386-392, 1996
26. Lima Filho RMA, Lima AL, de Oliveira Ruellas AC:Mandibular changes in skeletal Class II patients treatedwith Kloehn cervical headgear. Am J Orthod DentofacialOrthop 124:83-90, 2003
27. Lima Filho RMA, Lima AL, de Oliveira Ruellas AC:Longitudinal study of anteroposterior and vertical max-illary changes in skeletal Class II patients treated withKloehn cervical headgear. Angle Orthod 73:187-193, 2003
28. Ciger S, Aksu M, Germec D: Evaluation of posttreatmentchanges in Class II division 1 patients after nonextractionorthodontic treatment: cephalometric and model anal-ysis. Am J Orthod Dentofacial Orthop 127:219-223, 2005
29. Tortop T, Yuksel S: Treatment and posttreatmentchanges with combined headgear therapy. Angle Orthod77:857-863, 2007
30. Phan XL, Schneider BJ, Sadowsky C, et al: Effects oforthodontic treatment on mandibular rotation anddisplacement in angle Class II division 1 malocclusions.Angle Orthod 74:174-183, 2004
31. Kim KR, Muhl ZF: Changes in mandibular growthdirection during and after cervical headgear treatment.Am J Orthod Dentofacial Orthop 119:522-530, 2001
32. Ryan MJ, Schneider BJ, BeGole EA, et al: Openingrotations of the mandible during and after treatment. AmJ Orthod Dentofacial Orthop 114:142-149, 1998
An Evidence-Based Comparison of Headgear and Functional Appliance Therapy 193
33. Firouz M, Zernik J, Nanda R: Dental and orthopediceffects of high-pull headgear in treatment of Class II,division 1 malocclusion. Am J Orthod DentofacialOrthop 102:197-205, 1992
34. Caldwell SF, Hymas TA, Timm TA: Maxillary tractionsplint: a cephalometric evaluation. Am J Orthod 85:376-384, 1984
35. Uner O, Yucel-Eroglu E: Effects of a modified maxillaryorthopaedic splint: a cephalometric evaluation. Eur JOrthod 18:269-286, 1996
36. Iscan HN, Dincer M, Gultan A, et al: Effects of verticalchincap therapy on the mandibular morphology in open-bite patients. Am J Orthod Dentofacial Orthop 122:506-511, 2002
37. Harvold E, Vargervik K: Morphogenetic response toactivator treatment. Am J Orthod 60:479-490, 1971
38. Stockli R, Willert H: Tissue reactions in the tempor-omandibular joint resulting from anterior displacementof the mandible in the monkey. Am J Orthod 60:141-155,1971
39. Woodside DG, Altuna G, Harvold E, et al: Primateexperiments in malocclusion and bone induction. Am JOrthod 83:460-468, 1983
40. McNamara JA, Bryan FA: Long-term mandibular adapta-tions to protrusive function: an experimental study inMacaca mulatta. Am J Orthod Dentofacial Orthop 92:98-108, 1987
41. Op Heij DG, Callaert H, Opdebeeck HM: The effect ofthe amount of protrusion built into the Bionator oncondylar growth and displacement: a clinical study. Am JOrthod Dentofacial Orthop 95(5):401-409, 1989
42. McNamara JA Jr, Howe RP, Dischinger TG: A comparisonof the Herbst and Fränkel appliances in the treatment ofClass II malocclusion. Am J Orthod Dentofacial Orthop98:134-144, 1990
43. Mills JRE: The effect of functional appliances on theskeletal pattern. Br J Orthod 18:267-275, 1991
44. Nelson C, Harkness M, Herbison P: Mandibular changesduring functional appliance treatment. Am J OrthodDentofacial Orthop 104:153-161, 1993
45. Illing HM, Morris DO, Lee RT: A prospective evaluationof bass, Bionator and twin block appliances. Part I—thehard tissues. Eur J Orthod 20:501-516, 1998
46. Toth LR, McNamara JA Jr.: Treatment effects producedby the twin block appliance and the FR-2 appliance ofFränkel compared with an untreated Class II sample. AmJ Orthod Dentofacial Orthop 116:597-609, 1999
47. Almeida MR, Henriques JFC, Ursi W: Comparative studyof Fränkel (FR-2) and Bionator appliances in the treat-ment of Class II malocclusion. Am J Orthod DentofacialOrthop 121:458-466, 2002
48. Dermaut LR, Aelbers CMF: Orthopedics in orthodontics:fiction or reality. A review of the literature Part II. Am JOrthod Dentofacial Orthop 110:667-671, 1996
49. Huang G, et al: Functional appliances and long-termeffects on mandibular growth. Am J Orthod DentofacialOrthop 128:271-272, 2005
50. Johnston LE: If wishes were horses: functional appliancesand growth modification. Prog Orthod 6(1):36-47, 2005
51. Johnston LE: Commentary on “Mandibular changesproduced by functional appliances in Class II
malocclusion: a systematic review”. Am J Orthod Dento-facial Orthop 129:e1-e4, 2006
52. Araujo AM, Buschang PH, Melo AC: Adaptive condylargrowth and mandibular remodeling changes with Bionatortherapy—an implant study. Eur J Orthod 26:515-522, 2004
53. Righellis EG: Treatment effects of Fränkel, activator andextraoral traction appliances. Angle Orthod 53:107-121,1983
54. Nielsen IL: Facial growth during treatment with thefunctional regulator appliance. Am J Orthod 85:401,1984
55. Pancherz H, Haag U: Dentofacial orthopedics in relationto somatic maturation. Am J Orthod 88:273-287, 1985
56. Croft RS, Buschang PH, English JD, et al: A cephalo-metric and tomographic evaluation of Herbst treatmentin the mixed dentition. Am J Orthod Dentofacial Orthop116:435-443, 1999
57. Ascher F: The Bionator In Graber T, Neumann B eds.Removable Orthodontic Appliances. Philadelphia, W. B.Saunders, 1977
58. Rudzki-Janson I, Noachtar R: Functional appliancetherapy with the Bionator. Semin Orthod 4:33-45, 1998
59. Faltin KJ, Faltin RM, Baccetti T, et al: Long-termeffectiveness and treatment timing for Bionator therapy.Angle Orthod 73:221-230, 2003
60. Malta LA, Baccetti T, Franchi L, et al: Long-termdentoskeletal effects and facial profile changes inducedby Bionator therapy. Angle Orthod 80:10-17, 2010
61. Kochel J, Meyer-Marcotty P, Witt E, et al: Effectiveness ofBionator therapy for Class II malocclusions. J OrofacOrthop 73:91-103, 2012
62. Owen AH 3rd: Morphologic changes in the sagittaldimension using the Fränkel appliance. Am J Orthod80:573-603, 1981
63. Janson GR, Toruño JL, Martins DR, et al: Class IItreatment effects of the Fränkel appliance. Eur J Orthod25:301-309, 2003
64. Perillo L, Cannavale R, Ferro F, et al: Meta-analysis ofskeletal mandibular changes during Frankel appliancetreatment. Eur J Orthod 33(1):84-92, 2011
65. Perillo L, Johnston LE Jr, Ferro A: Permanence of skeletalchanges after function regulator (FR-2) treatment ofpatients with retrusive Class II malocclusions. Am JOrthod Dentofacial Orthop 109:132-139, 1996
66. Perillo L, Castaldo MI, Cannavale R, et al: Evaluation oflong-term effects in patients treated with Frankel-2appliance. Eur J Paediatr Dent 12:261-266, 2011
67. Freeman DC, McNamara JA, Baccetti T, et al: Long-termtreatment effects of the FR-2 appliance of Frankel. Am JOrthod Dentofacial Orthop 135:570.e1-570.e6, 2009
68. Sari Z, Goyenc Y, Doruk C, Usumez S: Comparativeevaluation of a new removable Jasper Jumper functionalappliance vs an activator–headgear combination. AngleOrthod 73:286-293, 2003
69. Cozza P, De Toffol L, Iacopini L: An analysis of thecorrective contribution in activator treatment. AngleOrthod 74:741-748, 2004
70. Wieslander L, Lagerström L: The effect of activatortreatment on Class II malocclusions. Am J Orthod 75:20-26, 1979
71. Cura N, Saraç M, Öztürk Y, Sürmeli N: Orthodontic andorthopedic effects of activator, activator-HG
Southard et al194
combination, and Bass appliances: a comparative study.Am J Orthod Dentofacial Orthop 110:36-45, 1996
72. Janson G, Caffer DC, Henriques JFC, et al: Stability ofClass II division 1 treatment with the headgear–activatorcombination followed by the edgewise appliance. AngleOrthod 74:594-604, 2004
73. Hänggi MP, Teuscher UM, Roos M, et al: Long-termchanges in pharyngeal airway dimensions followingactivator–headgear and fixed appliance treatment. EurJ Orthod 30:598-605, 2008
74. Lerstøl M, Torget Ø, Vandevska-Radunovic V: Long-termstability of dentoalveolar and skeletal changes after activa-tor–headgear treatment. Eur J Orthod 32:28-35, 2010
75. Phan KLD, Bendeus M, Hägg U, et al: Comparison of theheadgear activator and Herbst appliance—effects andposttreatment changes. Eur J Orthod 28:594-604, 2006
76. Pancherz H, Fackel U: The skeletofacial growth patternpre- and post-dentofacial orthopaedics: a long-term studyof Class 11 malocclusions treated with the Herbstappliance. Eur J Orthod 12:209-218, 1990
77. Hansen K, Pancherz H: Long-term effects of Herbsttreatment in relation to normal growth development: acephalometric study. Eur J Orthod 14:285-295, 1992
78. Pancherz H, Anchus-Pancherz M: The headgear effect ofthe Herhst appliance: a cephalometric long-term study.Am J Orthod Dentofacial Orthop 103:510-520, 1993
79. Hansen K, Pancherz H, Flagg U: Long-term effects of theHerbst appliance in relation to the treatment growth period:a cephalometric study. Eur J Orthod 13:471-481, 1991
80. Omblus J, Malmgren O, Pancherz H, et al: Long-termeffects of Class II correction in Herbst and Bass therapy.Eur J Orthod 19(2):185-193, 1997
81. Pancherz H: The effects, limitations, and long-termdentofacial adaptations to treatment with the Herbstappliance. Semin Orthod 3(4):232-243, 1997
82. Pancherz H, Ruf S, Kohlhas P: “Effective condylargrowth” and chin position changes in Herbst treatment:a cephalometric roentgenographic long-term study. Am JOrthod Dentofacial Orthop 114(4):437-446, 1998
83. Pancherz H, Fischer S: Amount and direction oftemporomandibular joint growth changes in Herbsttreatment: a cephalometric long-term investigation.Angle Orthod 73(5):493-501, 2003
84. Ruf S, Pancherz H: The effect of Herbst appliancetreatment on the mandibular plane angle: a cephalo-metric roentgenographic study. Am J Orthod DentofacialOrthop 110:225-229 [AJODO], 1996
85. Nelson B, Hagg U, Hansen K, et al: A long-term follow-upstudy of Class II malocclusion correction after treatmentwith Class II elastics or fixed functional appliances. Am JOrthod Dentofacial Orthop 132:499-503, 2007
86. Shea BJ, Grimshaw JM, Wells GA, et al: Developmentof AMSTAR: a measurement tool to assess the
methodological quality of systematic reviews. BMC MedRes Methodol 7:7-10, 2007
87. Shea BJ, Hamel C: AMSTAR is a reliable and validmeasurement tool to assess the methodological quality ofsystematic reviews. J Clin Epidemiol 62(10):1013-1020,2009
88. Marsico E, Gatto E, Burrascano M, et al: Effectiveness oforthodontic treatment with functional appliances onmandibular growth in the short term. Am J OrthodDentofacial Orthop 139(1):24-36, 2011
89. Antonarakis GS, Kiliaridis S: Short-term anteroposteriortreatment effects of functional appliances and extraoraltraction on class II malocclusion. A meta-analysis. AngleOrthod 77(5):907-914, 2007
90. Flores-Mir C, Ayeh A, Goswani A, et al: Skeletal anddental changes in Class II division 1 malocclusionstreated with splint-type Herbst appliances. A systematicreview. Angle Orthod 77(2):376-381, 2007
91. Flores-Mir C, Major PW: A systematic review of cepha-lometric facial soft tissue changes with the Activator andBionator appliances in Class II division 1 subjects. Eur JOrthod 28(6):586-593 [Epub 2006 Nov 9], 2006
92. Flores-Mir C, Major MP, Major PW: Soft tissue changeswith fixed functional appliances in Class II division 1.Angle Orthod 76(4):712-720, 2006
93. Cozza P, Baccetti T, Franchi L, et al: Mandibular changesproduced by functional appliances in Class II malocclu-sion: a systematic review. Am J Orthod DentofacialOrthop 129(5):599 [e1–12; discussion e1–6], 2006
94. Chen JY, Will LA, Niederman R: Analysis of efficacy offunctional appliances on mandibular growth. Am JOrthod Dentofacial Orthop 122(5):470-476, 2002
95. Flores-Mir C, Major PW: Cephalometric facial soft tissuechanges with the twin block appliance in Class II division1 malocclusion patients. A systematic review. AngleOrthod 76(5):876-881, 2006
96. Li F, Hu HK, Chen JW, et al: Comparison of anchoragecapacity between implant and headgear during anteriorsegment retraction. Angle Orthod 81(5):915-922, 2011
97. Skeggs RM, Benson PE, Dyer F: Reinforcement ofanchorage during orthodontic brace treatment withimplants or other surgical methods. Cochrane DatabaseSyst Rev 18(3):CD005098, 2007
98. Erin AC, Sloss E, Southard K, et al: Comparison of soft-tissue profiles after treatment with headgear or Herbstappliance. Am J Orthod Dentofacial Orthop 133:509-514,2008
99. Kadkhoda S, Nedjat S, Shiraz IM: Comparison of oral-health-related quality of life during treatment withheadgear and functional appliances. Int J Paediatr Dent21:369-373, 2011
An Evidence-Based Comparison of Headgear and Functional Appliance Therapy 195





























