Embed Size (px)
Citation preview

Cassimiro GN, Mata JAL. Adhesion to the use of ferrous sulphate...
English/Portuguese
J Nurs UFPE on line., Recife, 11(Suppl. 5):2156-67, May, 2017 2156
ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.9302-81402-1-RV.1105sup201722
ADHESION TO THE USE OF FERROUS SULPHATE BY PREGNANT WOMEN SERVED IN THE UNIFIED HEALTH SYSTEM
ADESÃO AO USO DE SULFATO FERROSO POR GESTANTES ATENDIDAS NO SISTEMA ÚNICO DE SAÚDE
ADHESIÓN AL USO DE SULFATO FERROSO POR MUJERES EMBARAZADAS ATENDIDAS EN EL SISTEMA UNICO DE SALUD
Gabriele Nogueira Cassimiro¹, Júnia Aparecida Laia da Mata²
ABSTRACT
Objective: to identify the factors that influence the adherence of pregnant women to the use of ferrous sulfate during prenatal care in the Brazilian Unified Health System. Method: a descriptive, exploratory, qualitative approach. We interviewed 11 pregnant women with gestational age of 20 weeks or more, assigned to a Family Health Strategy unit. The data analysis was based on Thematic Content Analysis. Results: three categories emerged: I - Pregnant women's knowledge about the prescription of ferrous sulfate; II - Factors that negatively influence the adhesion to the use of ferrous sulphate; III - Factors that contribute to the good adhesion to the use of ferrous sulfate. Conclusion: forgetfulness and difficulty in accessing the supplement were shown to be factors that hinder the adherence of pregnant women. The influence of the pre-natalist revealed a positive contribution to the adherence. Descriptors: Unified Health System; Nursing; Pregnancy;
Prenatal Care; Ferrous Sulfate.
RESUMO
Objetivo: identificar os fatores que influenciam na adesão de gestantes ao uso de sulfato ferroso durante o pré-natal no Sistema Único de Saúde. Método: estudo descritivo, exploratório, de abordagem qualitativa. Foram entrevistadas 11 gestantes com idade gestacional de 20 semanas ou mais, adstritas a uma unidade de Estratégia de Saúde da Família. A análise dos dados fundamentou-se na Análise Temática de Conteúdo. Resultados: emergiram três categorias: I - Conhecimentos das gestantes acerca da prescrição do sulfato ferroso; II - Fatores que influenciam negativamente na adesão ao uso de sulfato ferroso; III - Fatores que contribuem para a boa adesão ao uso de sulfato ferroso. Conclusão: o esquecimento e a dificuldade de acesso ao suplemento mostraram-se como fatores que prejudicam a adesão das gestantes. A influência do pré-natalista revelou contribuir positivamente na adesão. Descritores: Sistema Único de Saúde; Enfermagem;
Gravidez; Cuidado Pré-natal; Sulfato Ferroso.
RESUMEN Objetivo: identificar los factores que influyen en la adhesión de mujeres embarazadas al uso de sulfato ferroso durante la atención prenatal en el sistema único de salud. Método: descriptivo, exploratorio, cualitativo. Fueron entrevistados a 11 mujeres embarazadas con edad gestacional de 20 semanas o más, sujeto a una unidad de la estrategia de salud de la familia. El análisis de datos se basó en el análisis temático de contenido. Resultados: surgieron tres categorías: I - Conocimiento de las mujeres embarazadas sobre el requisito de sulfato ferroso; II - Factores que influyen negativamente en el uso de sulfato ferroso; III - Factores que contribuyen a la buena adhesión al uso de sulfato ferroso. Conclusión: la falta de memoria y dificultad de acceso al suplemento se demostraron como factores que afectan la adhesión de mujeres embarazadas. La influencia de (el) pré-natalista reveló una contribución positiva en la adhesión.
Descriptores: Sistema Único de Salud; Enfermería; Embarazo; Atención Prenatal; Sulfato Ferroso. 1Nurse, Specialist in Family Health by the Municipal Health Department of Curitiba and Pequeno Príncipe Colleges. Curitiba (PR), Brazil. E-mail: [email protected]; 2Obstetric Nurse, PhD in Nursing, School of Nursing, State University of Campinas - FEnf / UNICAMP. Campinas (SP), Brazil. E-mail: [email protected]
ORIGINAL ARTICLE
Cassimiro GN, Mata JAL. Adhesion to the use of ferrous sulphate...
English/Portuguese
J Nurs UFPE on line., Recife, 11(Suppl. 5):2156-67, May, 2017 2157
ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.9302-81402-1-RV.1105sup201722
The World Health Organization (WHO)
considers iron deficiency anemia as a major
public health problem, and is one of the
major nutritional deficiencies. In 2012, 41.8%
of the pregnant women in the world presented
this aggravation. In Brazil, although there is
no national survey, a prevalence of around
30% is estimated.
Anemia is determined by a condition in
which the concentration of hemoglobin level
is relatively low in the blood and is defined by
values below 10.5 g/dl. About 50% of the
cases have iron deficiency as the main
contributor, and can occur due to several
factors, such as inadequate intake of this
nutrient, parasitic infections or even
conditions that increase the need for iron,
with emphasis on pregnant women and
younger children of two years.2 In the
gestation, the physiological processes
contribute to the decrease in the absorption
of this micronutrient. In contrast, it
considerably increases its need for fetal
growth.3
According to the WHO, the use of ferrous
sulfate improves the development of
gestation, maternal health and mainly reduces
the infant mortality rate. With these results,
prophylaxis is extended worldwide, especially
in developing countries.1
When considering the high prevalence of
iron deficiency anemia, Brazil proposes
strategies for its prevention and control.
Ordinance No. 730, of May 13, 2005, it
instituted the National Iron Supplementation
Program (NISP), which adopts supplementary
measures to stimulate healthy eating and
supplementation in prophylactic doses.2
Adherence to the use of iron in the
Gestational cycle is a crucial point following
the recommendations of the NISP.1
Adherence is defined as the behavior that
indicates user agreement, following the
instructions of health professionals, according
to the dose of medications / supplements and
schedules previously agreed upon. There are
several causes of noncompliance, treated as
preventable and not preventable. Among the
avoidable ones, are forgetfulness, lack of
understanding about prescription or even
barriers to obtaining medication; in relation
to unavoidable ones, untreatable side effects
and adverse events are highlighted.4-5
The evaluation of adherence to the use of
medications and supplements should be
frequent in the daily routine of health
professionals, to monitor the proposed
treatment and promote adherence by the
recipient of the care. It can be done by direct
or indirect methods. The former include
laboratory techniques that quantify the drug,
metabolites or biological fluids, relating to
the use of medication and direct observation
of the user, usually performed in hospitals.
The indirect ones evaluate the behavior of the
individual associated with the reported
information and/or estimates, such as, self-
report, the application of structured
questionnaires, the verification of the drug
withdrawal record from the pharmacy and the
evaluation of the clinical response.5-6
The consequences of low adherence are
significant, causing debate in many countries,
as they imply an increase in direct and
indirect health expenditures and social costs
due to the loss or reduction of labor
productivity and the reduction of quality of
life. It is fundamental that managers and
health professionals recognize the problem of
lack of adherence to medication, adopting
actions to improve the performance of the
health system, optimizing resources,
improving health indicators, effectiveness of
interventions and, consequently, impacting
morbidity and mortality.4-5
Studies associate the low adherence to iron
supplementation with its side effects.7-8
Prenatal professionals are considered as
potential identifiers of the elements that
interfere with the continuity of treatment
with ferrous sulfate, and may promote care
that favors greater adherence of pregnant
women.
In professional practice, the authors
realized that only the recommendation of the
Ministry of Health (MH) of Brazil and the
routine prescription of this supplement have
not guaranteed the adoption of women to
their daily use. Therefore, it is argued that it
is important to research and know the factors
that influence adherence, which may support
the elaboration of prenatal care strategies
that potentiate adherence to iron
supplementation, contributing, positively, to
maternal- child health.
Therefore, the objective, of this study, was
to identify the factors that influence the
adherence of pregnant women to the use of
ferrous sulfate during prenatal care in the
Unified Health System (UHS).
It is a descriptive, exploratory, qualitative
study.9-10 It was developed in a Family Health
Strategy (FHS) unit, belonging to the Bairro
Novo Health District, in the city of Curitiba
(PR), Brazil. This service integrates the Mãe
INTRODUCTION
MÉTHOD
Cassimiro GN, Mata JAL. Adhesion to the use of ferrous sulphate...
English/Portuguese
J Nurs UFPE on line., Recife, 11(Suppl. 5):2156-67, May, 2017 2158
ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.9302-81402-1-RV.1105sup201722
Curitibana Program, whose purpose, is to
improve the quality of humanized, qualified
and safe prenatal care. At the time of
collection, it had three teams, each consisting
of: one general practitioner, one nurse, three
Nursing assistants, one dental surgeon, one
oral health assistant, one oral health
technician, and six community health agents
(CHA). It had 9,111 registered users, of whom
93 were pregnant.
Eleven pregnant women with gestational
age of 20 weeks or more, with prescription of
ferrous sulfate, were enrolled in the study.
The type of sample was for convenience and
its size, defined by means of data saturation,
in which the capture of new components is
interrupted when the data obtained present,
in the evaluation of the scientist, a certain
repetition.11
The recruitment of the participants
occurred in two moments: 1 - consultation on
the users in the electronic medical records,
considering the inclusion criteria; 2 -
invitation of the possible participants, through
telephone contact and / or in the waiting
room for prenatal care. All the invited ones
accepted to participate, signing the Free and
Informed Consent Term (FICT). In order to
preserve anonymity, the pregnant women
were coded with Brazilian stone names.
The data were produced between October
and December 2015, and were obtained
through an individual interview, audiograved
by digital recorder, guided by a guide script,
consisting of two parts: A- characterization of
the participants; B- guiding questions. All
interviews were transcribed concomitantly
with the collection.
The analysis and interpretation of the data
were based on the technique of Thematic
Analysis of Content, proposed by Laurence
Bardin.12 They were carried out in three
stages: 1) Pre-analysis, in which the floating
reading of the material was carried out and
the data organized in Categories and themes;
2) Exploitation of the material, in which the
coding units were chosen; 3) Treatment of
results (inference and interpretation), in
which the contents of the speech were
interpreted, basing them on the theoretical
reference of this research.12
This study was approved by the Research
Ethics Committee of the Faculdades Pequeno
Príncipe (CAAE 44283215.5.0000.5580) and
authorized by the Municipal Health
Department of Curitiba (CAAE
44283215.5.3001.0101).
Characterization of Pregnant women
The participants' ages ranged from 18 to 36
years. Six had fixed employment, with a
workday from six to eight hours. The average
monthly income ranged from R$430 to R
$4,300. Ten pregnant women said they were
married. Five were primiparous and six, were
multiparous. Regarding schooling, six of the
interviewees had completed high school;
three had incomplete high school, one,
complete primary and one, incomplete
elementary school.
Six pregnant women were prematurely
prenatal, while five started late after 120
days of gestation. This is a worrying situation,
since the MH maintains that, in order to
ensure a quality and effective prenatal care,
it is essential to link the pregnant woman as
early as possible to pre=natal care.
The number of prenatal consultations,
carried out until the moment of the interview,
remained between three and nine. When
considering the gestational age of the
investigated patients and the periodicity of
the visits, recommended by the MH, it was
verified that all the pregnant women were up
to date with the prenatal calendar. Most of
the consultations were performed by the
medical category. Seven of the interviewees
had undergone only one Nursing consultation,
prevailing the one of bonding.
According to the Nursing Professional
Exercise Law, No. 7.498 / 86, the nurse is
qualified to perform prenatal care, as it has
the technical-scientific competence to
properly perform care for the pregnant
woman. The MH corroborates with this
legislation and affirms that in the basic health
network, the nurse can fully follow the usual
prenatal risk. It also determines, that both
the doctor, and the nurse must perform the
prenatal relationship, which includes filling
out the pregnant woman's card and registering
her in the Pregnancy Monitoring System
(SisPreNatal).13,14 It was verified that, in the
studied scenario, there is the centralization of
bureaucratic functions, such as the user's
registry in SisPreNatal, in the figure of the
Nursing professional, with care under medical
responsibility.
At the time of collection, all participants
stated that they were using ferrous sulfate.
Ten of them also expressed the use of folic
acid; one was taking fluoxetine and one, a
vitamin-mineral supplement.
Prescription of ferrous sulfate before the
20th week of gestation was observed in five
RESULTS AND DISCUSSION
Cassimiro GN, Mata JAL. Adhesion to the use of ferrous sulphate...
English/Portuguese
J Nurs UFPE on line., Recife, 11(Suppl. 5):2156-67, May, 2017 2159
ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.9302-81402-1-RV.1105sup201722
pregnant women, with only one being advised
that it could be used after 20 gestational
weeks. There are recommendations for the
use of supplementary iron starting at 20
weeks of gestation, since, during this period,
there is a significant increase in the
absorption of this micronutrient, decreasing
maternal reserves.15
As for the prescriptions of ferrous sulfate,
nine were made by doctors and only two, by
nurses. It is believed that this situation is
related to the reduced number of
consultations performed by Nursing
professionals in the unit studied.
Only two prescriptions contained the
dosage: one performed by a doctor and
another, by a nurse. Only four pregnant
women reported having been instructed on
the use of ferrous sulfate until the third
month after delivery. It was identified that,
the recommendations of the WHO and the Mãe
Curitibana Program regarding the prescription
of ferrous sulfate and orientation of the users
were not followed in the care of the majority
of the pregnant women (six).
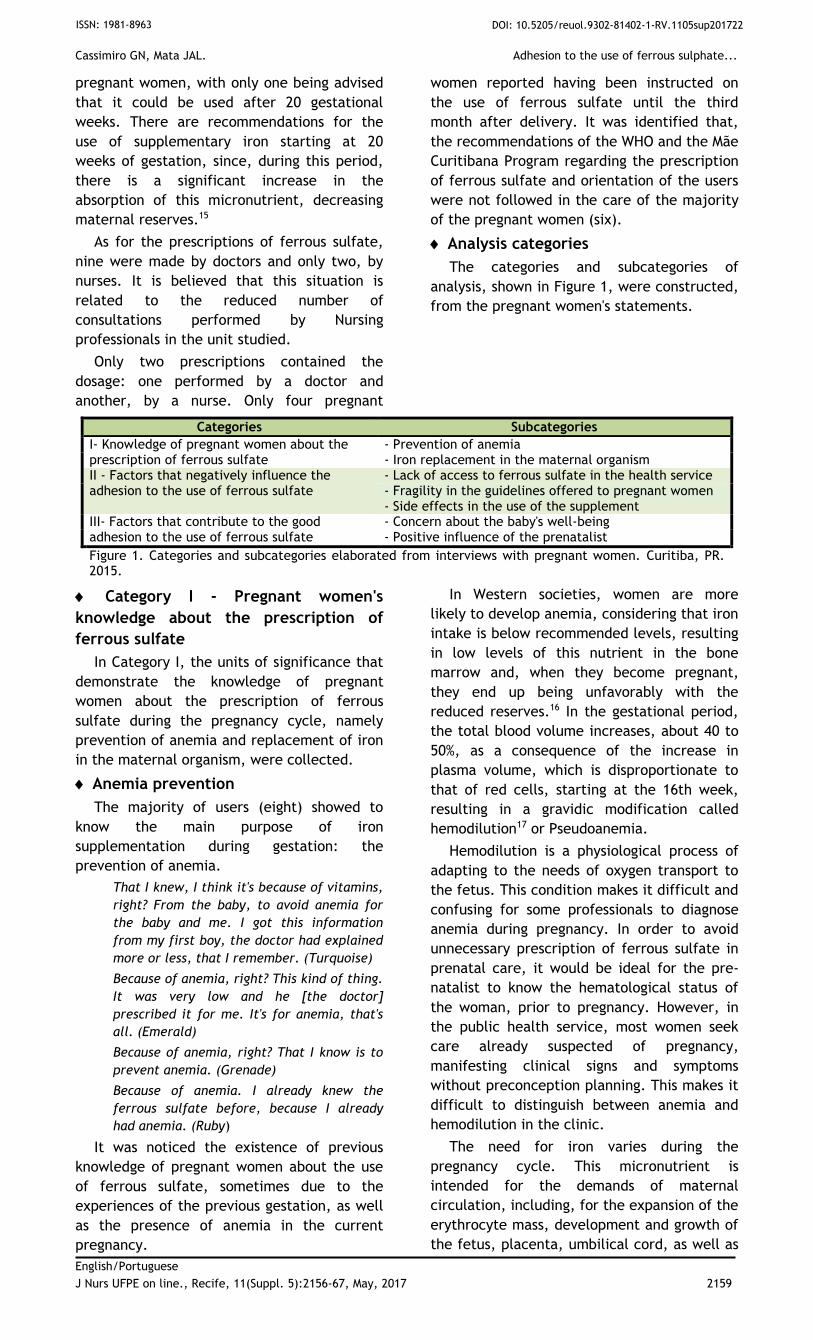
Analysis categories
The categories and subcategories of
analysis, shown in Figure 1, were constructed,
from the pregnant women's statements.
Categories Subcategories
I- Knowledge of pregnant women about the prescription of ferrous sulfate
- Prevention of anemia - Iron replacement in the maternal organism
II - Factors that negatively influence the adhesion to the use of ferrous sulfate
- Lack of access to ferrous sulfate in the health service - Fragility in the guidelines offered to pregnant women - Side effects in the use of the supplement
III- Factors that contribute to the good adhesion to the use of ferrous sulfate
- Concern about the baby's well-being - Positive influence of the prenatalist
Figure 1. Categories and subcategories elaborated from interviews with pregnant women. Curitiba, PR. 2015.
Category I - Pregnant women's
knowledge about the prescription of
ferrous sulfate
In Category I, the units of significance that
demonstrate the knowledge of pregnant
women about the prescription of ferrous
sulfate during the pregnancy cycle, namely
prevention of anemia and replacement of iron
in the maternal organism, were collected.
Anemia prevention
The majority of users (eight) showed to
know the main purpose of iron
supplementation during gestation: the
prevention of anemia.
That I knew, I think it's because of vitamins,
right? From the baby, to avoid anemia for
the baby and me. I got this information
from my first boy, the doctor had explained
more or less, that I remember. (Turquoise)
Because of anemia, right? This kind of thing.
It was very low and he [the doctor]
prescribed it for me. It's for anemia, that's
all. (Emerald)
Because of anemia, right? That I know is to
prevent anemia. (Grenade)
Because of anemia. I already knew the
ferrous sulfate before, because I already
had anemia. (Ruby)
It was noticed the existence of previous
knowledge of pregnant women about the use
of ferrous sulfate, sometimes due to the
experiences of the previous gestation, as well
as the presence of anemia in the current
pregnancy.
In Western societies, women are more
likely to develop anemia, considering that iron
intake is below recommended levels, resulting
in low levels of this nutrient in the bone
marrow and, when they become pregnant,
they end up being unfavorably with the
reduced reserves.16 In the gestational period,
the total blood volume increases, about 40 to
50%, as a consequence of the increase in
plasma volume, which is disproportionate to
that of red cells, starting at the 16th week,
resulting in a gravidic modification called
hemodilution17 or Pseudoanemia.
Hemodilution is a physiological process of
adapting to the needs of oxygen transport to
the fetus. This condition makes it difficult and
confusing for some professionals to diagnose
anemia during pregnancy. In order to avoid
unnecessary prescription of ferrous sulfate in
prenatal care, it would be ideal for the pre-
natalist to know the hematological status of
the woman, prior to pregnancy. However, in
the public health service, most women seek
care already suspected of pregnancy,
manifesting clinical signs and symptoms
without preconception planning. This makes it
difficult to distinguish between anemia and
hemodilution in the clinic.
The need for iron varies during the
pregnancy cycle. This micronutrient is
intended for the demands of maternal
circulation, including, for the expansion of the
erythrocyte mass, development and growth of
the fetus, placenta, umbilical cord, as well as
Cassimiro GN, Mata JAL. Adhesion to the use of ferrous sulphate...
English/Portuguese
J Nurs UFPE on line., Recife, 11(Suppl. 5):2156-67, May, 2017 2160
ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.9302-81402-1-RV.1105sup201722
eventual losses (during childbirth and
puerperium). 17
Anemia has implications for maternal and
child health in the short and long term.
Pregnant women may present with fatigue,
dizziness, headache, impaired muscular
performance, reduced physical fitness for
work and behavioral disorders including
depression, irritability, emotional instability,
difficulty concentrating and attention.18 One
of the pregnant women demonstrated
knowledge about some of the changes that
Anemia cause:
In order not to let anemia, not to let it
weaken me, to prevent it from
strengthening during pregnancy, I have been
taking ferrous sulfate for a long time,
because I have always had anemia, that, is
something, I know. (Amber)
Anemia prevention measures, adopted in
Brazil, include nutritional and food education
actions, so that nutrition is healthy and
adequate, taking into account individual
needs; fortification of wheat and maize flour;
control of parasitic diseases; improvement of
sanitation conditions; and prophylactic
supplementation with iron and folic acid,
especially, in pregnancy and in children.2
Health education is a relevant strategy in
promoting knowledge during prenatal care.
Among the points to be addressed by the
prenatalist, prophylactic iron supplementation
should be presented to the pregnant woman in
order to aggregate previous knowledge,
orienting her on the importance of adherence
to treatment, on possible side effects that
may during the use of the supplement, and
the importance of its use until the third
month after giving birth.2
Iron replacement in the maternal
organism
Some pregnant women (four) stated that
ferrous sulfate was prescribed to replace iron
in their body in order to supply their needs
and of the baby.
I know it is to raise the iron level of the
body because of gestation and the baby's
iron. (Agate)
To raise the level of iron in the blood
because I'm having anemia and that could
happen to the baby. (Amethyst)
It serves to replace the iron that I do not
have in the body. (Crystal)
Iron plays important roles in the human
body. The concentration of iron in the body is
about three to five grams, being
approximately 30 to 50 mg / kg, varying
according to sex, age, tissue examined and
geographical regions in which The
bioavailability of iron is altered, both, for
excess and shortage. 19
For the monitoring of circulating iron
levels, hemoglobin concentration is often used
because it is simple and inexpensive.
However, it is not sufficient to evaluate,
being necessary the complementation with
biomarkers, as for example, the concentration
of serum ferritin and transferrin receptors.
These complementary exams are not always
available and have limitations in their
interpretations, in some cases, where there
are infections such as malaria, HIV / AIDS and
vaginosis during pregnancy.20,21
Food is the main source for obtaining iron,
and foods of plant origin, such as, dark green
leafy vegetables, and legumes have low
bioavailability, requiring the recommendation
of the ingestion associated with foods that
improve their absorption, which contain
vitamin C or A, available in fruits like lemon,
orange, papaya and mango. Foods of animal
origin, such as red meat, poultry, pork, fish
and shellfish have better absorption.2
Iron deficiency is a clinical problem
associated with several negative consequences
for maternal and child health. So, ensuring an
adequate level of this micronutrient in the
pregnant woman's body is necessary to avoid
complications as well as to improve the
development and maturity of the fetus.20
The aforementioned statements were
identified in the discourses of pregnant
women, which reveals a level of knowledge
about iron supplementation, whether acquired
through information obtained in previous
pregnancies, or even due to the need for
anemia treatment prior to pregnancy. The
information facilitates the process of
adherence, since it promotes the user's
understanding of the importance and motive
of the treatment proposed during the
pregnancy-puerperal cycle.
Category II - Factors that influence
negatively in adherence to the use of
ferrous sulfate
In Category II, meaning units were
identified that reveal the factors that
negatively affect the adherence of pregnant
women to the use of ferrous sulfate, being:
the lack of access to ferrous sulfate in the
health service; fragilities in the guidelines
offered to the pregnant woman and side
effects in the use of the supplement.
Lack of access to ferrous sulfate in the
health service
Pharmaceutical assistance in UHS is
organized in levels of complexity, financed by
blocks classified into three components: basic,
Cassimiro GN, Mata JAL. Adhesion to the use of ferrous sulphate...
English/Portuguese
J Nurs UFPE on line., Recife, 11(Suppl. 5):2156-67, May, 2017 2161
ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.9302-81402-1-RV.1105sup201722
specialized and strategic. Currently, the
National List of Essential Medicines - RENAME,
guided by the National Policy on
Pharmaceutical Care, lists all medicines that
citizens should have the right to free access,
considered essential to guarantee improved
access to the health of the population.22
For a quality prenatal care, it is necessary
to guarantee some elements, such as the
availability and access to basic medicines,
such as ferrous sulfate and folic acid.2 Some
disrespect to this recommendation has been
identified. The interviewees expressed that
they had ceased the use of ferrous sulfate
because of difficulty in accessing the
supplement in the health unit, noting that it
was missing for a certain period.
So until these days I made a stop, because I
was missing here, it's still in the truth,
there I bought it yesterday. Stay for about
two weeks without the medication. I think
even, I do not know, but I needed it, the
body got used, right? And then I stopped.
And it was at this time that my immunity
went down a lot, that even I went to
maternity because it gave a little problem, I
do not know if it has to do right? But when
the immunity of the low people gives of
everything in the people and gave of
everything in me, type urinary infection, I
was very bad. (Amber)
I do not take it just now, because it does
not have in the unit, I have to inform myself
today. (Tourmaline)
The lack of the supplement in the health
unit made it difficult to join and to continue
the treatment of the aforementioned
participants. Since the supply of a drug,
considered as basic in the public health
network, is interrupted, it directly affects the
UHS principles, influencing the quality of the
care provided and the expected results.
According to the NISP, obtaining the
supplements should be performed by planning
through the basic component of
Pharmaceutical Assistance, with tripartite
responsibility. For the acquisition, the
municipalities can perform the prioritization
of the population to be served and must
stipulate the amount of necessary inputs, as
well as the costs of the program so that it is
always available to SUS users. The absence of
these inputs reflects the resolubility of actions
and programs and compromises the
performance of services and professionals.2
Research shows that one of the main points
to check adherence is to assess whether the
drug is available for free or even at low cost,
as well as the accessibility of medication in
pharmaceutical care. Consideration is given to
whether the patient has the financial
resources to join, if he or she does not have
public health availability.23
It is important to emphasize that the
adhesion to ferrous sulfate depends directly
on the distribution of the drug free of charge,
because, when the user does not have
financial resources or even have difficulty
accessing it, it will hardly have a good
adherence.
In a scientific study, which evaluated
prenatal care in Brazil's basic network,
analyzing several points, such as the physical
evaluation of the place, human resources,
materials, norms, activities, procedures and
the reference system, it was verified the
existence Of unsatisfactory and precarious
resources, such as the lack of medication,
which limits the follow-up of pregnant women
and weakens the quality of prenatal care as a
whole.24 It can be seen that the reality
investigated in this study is not unrelated to
other Brazilian scenarios, and it is
fundamental to reflect and address the issue
of the user's access to qualified, resolutive
and safe prenatal care.
The promotion of adherence to the use of
supplements, when indicated, in the
pregnancy-puerperal cycle, is not limited to
aspects of care. It also involves the
management of public health services, which
must be in line with current public policies,
ensuring compliance with its guidelines by
Through a strategic planning that considers
the profile and needs of the assisted
population and an ethical and responsible
administration, committed to the principles
that govern UHS.
Fragility in the guidelines offered to
pregnant women
The majority of pregnant women (ten)
expressed weaknesses in the guidelines
received regarding the use of ferrous sulfate
during prenatal care, such as: prescription
with total lack of information; lack of
information about the reason for the use;
dosage and effects Collaterals.
In fact, she [prenatalist] only told me what
it was and passed me, she said it was to be
able to help in the "thing" of the blood and
for the baby and only. (Amethyst)
No, I did not receive any guidance in this
gestation. (Turquoise)
I did not receive any information. (Sapphire)
No, just said it [professionals], that I was
having anemia and passed me the ferrous
sulfate. (Tourmaline)
One of the important factors raised as
determinants of adherence is the relationship
between professional and user. It is necessary
to understand the client as an active subject
Cassimiro GN, Mata JAL. Adhesion to the use of ferrous sulphate...
English/Portuguese
J Nurs UFPE on line., Recife, 11(Suppl. 5):2156-67, May, 2017 2162
ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.9302-81402-1-RV.1105sup201722
in their treatment, participating in the
decisions and assuming the responsibilities
proposed in an agreed and not imposed
manner. Professional attitudes also deserve
attention, such as the language used during
the service, the time spent, the questioning,
the guidelines and motivations for compliance
with the treatment.23
In scientific research, the importance of
achieving a good prescription was verified.
However, it is not usually observed and
performed because the prescriber does not
encourage the user to participate in the
choice of treatment, often imposing what
should be done and also does not provide
enough information about his or her health
problem and the proposed treatment, positive
for the individual to adhere to its
recommendations. Another point identified in
the study was that the professional does not
verify the understanding about what was
exposed to the user, and still less about its
acceptability. All behaviors become especially
detrimental to the client, who does not know
and does not receive the necessary
information about their health condition and
the importance of the recommended
treatment.25
The pre-natalist has a strong influence on
the quality of the care given to the pregnant
woman. It should consider, in the attendance,
the relevance of the practice of health
education that, if performed in a satisfactory
manner, generates a positive impact on the
professional-user relationship, providing a
more complete information exchange,
influencing the decision power of the
pregnant woman about her health, promoting
a healthy and pleasant gestational cycle for
the woman.25
Other participants reported that they
received guidance regarding the use of ferrous
sulfate, however, it is noted, in the
statements, that the users felt a lack of
something (frequent occurrence of the word
"alone"), perhaps some recommendation or
the clarification of doubts.
Just for use, one capsule a day next to some
food and only. (Crystal)
He [the doctor] just told me how to take it.
(Emerald)
He [the doctor] just said it was for me to
take once a day, half an hour before lunch.
(Grenade)
Just from the use, it was to take one tablet
a day, up to three months after gestation.
(Jade)
The Mãe Curitibana Protocol recommends
the prescription of a 40mg ferrous sulfate
tablet for prophylaxis, with daily use for
prophylaxis, as well as the orientation of
regular use at the same time, daily, between
meals, being at least 30 minutes before
feeding and, Preferably with vitamin C-rich
juice. In case of forgetfulness should be taken
soon after feeding.15
It is important to discuss with the pregnant
woman about the uninterrupted use until the
end of gestation. For this, it is necessary to
clarify about the possible effects, that can
generate the resistance in the continuation of
the supplementation and, in cases of
intolerance, guide to take at least twice a
week.15
Nonadherence to treatment may be linked
to both the pregnant and the pre-natal, which
does not adequately guide the importance of
the use, continuity, risks to which women are
exposed and, often, Does not perform health
education, so significant for the performance
of a prenatal resolution.23
Two participants showed adequate
guidelines regarding dosage and the reason for
the prescription. One of them had anemia
prior to pregnancy. Prescriptions were
performed by nurses.
[...] that I take three times a day, every
eight hours, not to weaken and help during
pregnancy. (Amber)
[...] for me to take it once a day until the
third month after the baby is born. (Agate)
The daily dose of ferrous sulfate, as
reported by the interviewees, was in
accordance with the prescription made by the
professional and recorded in the medical
record. In this way, it was verified that the
investigated ones were following the
recommendations of the pre-natalistas that
prescribed.
Seven participants reported having
forgotten to take the supplement as
prescribed, a factor that also interferes with
adherence.
Sometimes we forget. I did not tell the
doctor. Oh, it was only one day. (Jade)
Already [stopped taking] because I forgot. I
did not tell the doctor. (Emerald)
Yes [stopped taking], by forgetting.
(Grenade)
Just to have forgotten, I never stopped
taking no, sometimes I forget. (Ruby)
Oh, there are two times I forgot [to take].
(Sapphire)
The WHO cites forgetting as a problem of
preventable noncompliance, being a factor
connected to the user. Adherence is related
to the motivation and meaning that the
subject has with the recommended
treatment, the importance that is seen for
health and well-being, demonstrating that the
Cassimiro GN, Mata JAL. Adhesion to the use of ferrous sulphate...
English/Portuguese
J Nurs UFPE on line., Recife, 11(Suppl. 5):2156-67, May, 2017 2163
ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.9302-81402-1-RV.1105sup201722
trust and belief that is deposited in the
therapy outweigh the effects or even the
change in lifestyle necessary to achieve better
results.4 In the consultations, it is essential
that the prenatal care provider verify that the
pregnant woman has followed the dosage,
reinforcing the need for maternal and fetal
health supplementation.
Side effects of supplement use
Side effects, caused by ferrous sulphate,
appeared in the pregnant women's speeches,
being revealed as factors that influenced the
adhesion.
I had a lot of dryness, I had constipation, so
I talked to my doctor, who advised to eat
more greens, drink plenty of liquids, eat
fruits. The doctor advised that it could be
for ferrous sulfate, yes. (Turquoise)
I stopped taking it, I took it for three
months in a row, along with folic acid, but I
always put it out, I always vomited, from
there I stopped drinking. And then,when I
did the blood test again, gave it again right?
That I was close to having anemia, so I went
back to taking only the ferrous sulfate. I
told the doctor and he fought with me, he
directed to return to use. Nobody told me
that the vomit was related to the ferrous
sulfate, but I took it with the folic acid
together and consequently I vomited, hence
that iron taste was strong in the mouth and
from there I interrupted. (Crystal)
It was verified, in the speeches, that the
most common side effects experienced by the
interviewees were: constipation and vomiting.
Research shows that one of the main
reasons for the difficulty in adhering to the
use of ferrous sulfate is the side effects,
especially, those related to the
gastrointestinal tract. These include epigastric
pain, nausea, vomiting, dark stools,
abdominal cramps, constipation, and less
frequently, diarrhea and heartburn.7-8
Some authors propose the use of different
doses of ferrous sulfate, since, they
demonstrate that, in smaller doses, this
supplement presents better results, reducing
the side effects. There are debates on daily or
weekly supplementation, on its benefits and,
especially, on the impact of reducing anemia
rates.7,21
Category III - Factors that contribute
to good adhesion to the use of ferrous
sulfate
Concern about baby's well-being
In the interviews, there was a frequent
appearance of concern about the health of
the baby, a factor that contributed to the
frequent use of ferrous sulfate by pregnant
women.
Because it's good right, for the baby to be
born healthy, important for me too, right?
(Turquoise)
Because I'm scared to death [something
happens to the baby], I actually, think it's
very important for the baby. (Agate)
[...] because I'm having anemia and this
could happen to the baby. (Amethyst)
Oh, because of the baby, right, to avoid
passing anything to the baby. (Grenade)
Prenatal care is a time when the pregnant
woman experiences the gestational process
proactively and has many worries and doubts
about her well-being and the baby. Among the
concerns shown by women, studies have
revealed that concern about fetal
abnormalities is one of the most cited, as well
as the chance of spontaneous abortion. Some
doubts assume specific stages in gestation,
which increases anxiety in these periods. The
performance of procedures, examinations and
educational activities are valued in the hope
of the child's health and also in the prevention
of complications during the pregnancy cycle.26
The fetus, during its development, has high
dependence on the mother to reach its
nutritional needs and, among the main
micronutrients, the iron is outstanding. In
order for the baby to receive adequate
amounts, this nutrient is supplied to the
mother from body stores, absorption through
feeding or even hemolysis, and she transfers it
to the baby, who is a major consumer of
iron.27 Iron Is an essential element for the
development and growth of various organs of
the fetus, especially the hematopoietic ones,
which are very important for the healthy
formation of the brain.20
Studies have shown that children of women
who have iron deficiency during pregnancy
have a lower cognitive development and even
a lower level of intelligence when compared
to the children of mothers who did not
present the deficiency in pregnancy.
Therefore, babies born with iron deficiency
have many negative repercussions on their
health, especially, on the nervous system,
affecting their behavioral development and
intelligence in childhood.20
Iron deficiency anemia is associated with
risk factors such as premature labor,
increased complications or adverse events,
and low birth weight. In addition to increasing
the chance of developing postpartum
depression, difficulty in mother-child
interaction and the compromise of the
important emotional ties in the puerperium,
especially, for breastfeeding.20
Iron deficiency in the baby may be due to
factors such as impaired absorption of this
Cassimiro GN, Mata JAL. Adhesion to the use of ferrous sulphate...
English/Portuguese
J Nurs UFPE on line., Recife, 11(Suppl. 5):2156-67, May, 2017 2164
ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.9302-81402-1-RV.1105sup201722
micronutrient, cord clamping time, time of
introduction of complementary foods,
frequency of infections, excessive blood loss,
malnutrition, parasitic diseases and other
diseases. 28 These factors elucidate the
relevance in promoting prenatal strategies
that promote adequate adherence to the use
of ferrous sulfate in women who require this
supplement.
The recognition by the pregnant women of
the importance of the supplementation for
the health of the baby can be considered a
promoter of the adhesion, after all, taking the
ferrous sulfate means for them the guarantee
of the well-being of their child, as well as the
prevention of aggravations that may affect it,
taking them to follow the recommendations
made by the pre-natalist.
Positive influence of the prenatalist
When asked about adherence to the use of
ferrous sulfate, three investigators reported
that they were following supplementation
because their prescriptions had been
prescribed by their pre-natalist, highlighting
the influence of the professional figure on
adherence.
I have taken it. Because she [the
prenatalist] has passed, so I take.
(Amethyst)
Yes [takes]. Because the doctor prescribed
and because of the baby, right? (Jade)
As I am, because the doctor prescribed me.
(Emerald)
It was identified, in the speeches, the
influence that the prenatalist exerted on the
volunteers, overcoming the lack of
information about the treatment, the side
effects, etc. They have shown great
confidence in the prescription of
professionals. A study shows that the main
references of pregnant women are health
professionals. Confidence is an important link
that must be built during prenatal care,
facilitating the professional-user relationship
and, in addition, improving the exchange of
information on pregnancy, childbirth and the
puerperium.29
Iron absorption depends on a number of
factors, including the nutritional orientation
associated with measures that promote the
change in micronutrient consumption habits.30
Thus, health education, related to nutritional
aspects in pregnancy, becomes indispensable
in the care offered .
When there is a good relationship between
the pregnant woman and the prenatal care
provider, the information offered throughout
the gestational cycle goes beyond mere
transmission and becomes significant for the
use of the recommendations in the daily
routine of the pregnant woman. It is
important to raise the awareness of the health
professional to deal with maternal and child
care, taking into account the innumerable and
large changes that involve pregnancy.29
Continuing health education can be a strategy
adopted to keep professionals up-to-date on
the related guidelines Prenatal care,
enhancing adoption and respect for WHO
recommendations, public policies and national
protocols.
In this research, prenatal care issues, were
identified, that should be reflected and
discussed, with the purpose of promoting the
improvement of the quality and safety of the
care offered to pregnant women in the
scenario studied. It was verified the existence
of fragilities that directly interfere in the
assistance performed by the prenatalists, such
as: the lack of medication and the non-
effective communication between
professional-user.
Brazilian maternal and child health has
protocols, ordinances, laws and resolutions,
which were elaborated with the objective of
improving health care in the country.
However, this study failed to meet some
recommendations of the Ministry of Health
and WHO, such as access to necessary
supplies, the application of health education
and qualified human resources in prenatal
care.
Despite the increasing drop in maternal and
infant mortality rates in Brazil, rates for
preventable causes are worrying, which points
to the current discussions on the issue of
increased prenatal coverage. It is argued that
it is necessary to go much further than the
extension of coverage, since the need to
qualify the health service and to improve the
skills and commitment of prenatal care
providers is emerging.
It was evidenced, in the research, that
inadequate communication between pregnant
women, with lack of information and lack of
clarity, or lack of communication, when
essential guidelines were not offered to
women, may negatively influence adherence
to iron supplementation. Effective
communication is an important prenatal tool.
Building a relationship of trust with the user
makes it more positive, facilitating the
exchange of knowledge and stimulating the
adherence of pregnant women to the
practices and recommendations of the
prenatalist.
CONCLUSION
Cassimiro GN, Mata JAL. Adhesion to the use of ferrous sulphate...
English/Portuguese
J Nurs UFPE on line., Recife, 11(Suppl. 5):2156-67, May, 2017 2165
ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.9302-81402-1-RV.1105sup201722
It was observed that one of the reasons
that led the pregnant women to stop taking
ferrous sulfate was oblivion and that they did
not communicate it to the health professional.
It is necessary to be attentive and frequently
check adherence to the prescribed therapy,
identifying the reasons that caused the
interruption, guiding pregnant women about
the need to use the supplement and its
importance and conducting health education
on an ongoing basis.
Health education is a fundamental point in
prenatal care and, to exercise it, professionals
must always update their knowledge, based
on protocols and scientific evidence. This
facilitates the fulfillment and the
accomplishment of an integral care, with
greater security and quality.
When considering the importance of the
topic of this study, it is recommended to carry
out new work on the subject, including, in the
municipality of this research scenario, so that
health professionals reflect how essential it is
to perform a responsible, safe, Qualified to
promote the adherence of iron
supplementation as a form of protection and
promotion of maternal and child health.
1. World Health Organization. Guideline:
daily iron and folic acid supplementation in
pregnant women [Internet]. Geneva: WHO;
2012 [cited 2015 Nov 15]. Available from:
http://apps.who.int/iris/bitstream/10665/77
770/1/9789241501 996_eng.pdf
2. Ministério da Saúde (BR), Secretaria de
Atenção à Saúde, Departamento de Atenção
Básica. Programa Nacional de Suplementação
de ferro: manual de condutas [Internet].
Brasília: Ministério da Saúde; 2013 [cited 2015
Nov 12]. Available from
http://bvsms.saude.gov.br/bvs/publicacoes/
manual_suplementacao_ferro_condutas_gerais
3. Ministério da Saúde (BR), Agência
Nacional de Vigilância Sanitária. Resolução
RDC nº 269, de 22 de setembro de 2005.
Regulamento técnico sobre ingestão diária
recomendada (IDR) para proteína, vitaminas e
minerais [Internet]. Brasília: ANVISA; 2005
[cited 2015 Nov 15]. Available from:
http://www.saude.rj.gov.br/comum/code/Mo
strarArquivo.php?C=MjIxNQ%2C%2C
4. World Health Organization. Guideline
Adherence to long-term therapies: evidence
for action [Internet]. Geneva: WHO; 2003
[cited 2015 Nov 13]. Available from:
http://apps.who.int/iris/bitstream/10665/42
682/1/9241545992.pdf
5. Neihelseil MB, Wheleer KJ, Roberts ME.
Medication adherence part one:
Understanding and assessing the problem. J
Am Assoc Nurse Pract. 2013 Jan;26(1):49-55.
Doi: 10.1002/2327-6924.12099.
6. Obreli Neto PR, Baldoni AO, Guidoni CM,
Bergamini D, Hernandes KC, Luz RT, et al.
Methods for estimating adherence to the
pharmacotherapy. Rev Bras Farm [Internet].
2012 [cited 2015 Nov 13];93(4):403-10.
Available from:
http://www.rbfarma.org.br/files/rbf-2012-
93-4-2.pdf
7. Souza AI, Batista Filho M, Bresani CC,
Ferreira LOC, Figueiroa JN. Adherence and
side effects of three ferrous sulfate treatment
regimens on anemic pregnant women in
clinical trials. Cad Saúde Pública [Internet].
2009 June [cited 2015 Nov 12];25(6):1225-33.
Available from:
http://www.scielo.br/pdf/csp/v25n6/05.pdf
8. Pereira DIA, Irving SSC, Lomer MCE,
Powell JJ. A rapid, simple questionnaire to
assess gastrointestinal symptoms after oral
ferrous sulphate supplementation. BMC
Gastroenterol [Internet]. 2014 June [cited
2015 Nov 12];14(103). Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/
PMC4082414/pdf/1471-230X-14-103.pdf
9. Gil AC. Métodos e técnicas de pesquisa
social. 6 th ed. São Paulo: Atlas; 2008.
10. Minayo MCS. Pesquisa social: teoria,
método e criatividade. 18th ed. Petrópolis:
Vozes; 2001.
11. Fontanella BJB, Ricas J, Turato ER.
Saturation sampling in qualitative health
research: theoretical contributions. Cad Saúde
Pública [Internet]. 2008 Jan [cited 2015 Nov
13];24(1):17-27. Available from:
http://www.scielo.br/pdf/csp/v24n1/02.pdf
12. Bardin L. Análise de conteúdo. São Paulo:
Edições 70; 2011.
13. Lei 7.498, de 25 de junho de 1986 (BR).
Dispõe sobre a Regulamentação do Exercício
da Enfermagem e dá outras providências.
Diário Oficial da União [Internet]. 25 June
1986 [cited 2015 Nov 13]. Available from
http://www.planalto.gov.br/ccivil_03/leis/L7
498.htm.
14. Ministério da Saúde (BR), Secretaria de
Atenção à Saúde, Departamento de Atenção
Básica. Atenção ao pré-natal de baixo risco
[Internet]. Brasília: Ministério da Saúde; 2012
[cited 2015 Nov 13]. Available from:
http://bvsms.saude.gov.br/bvs/publicacoes/c
adernos_atencao_basica_32_prenatal.pdf
15. Curitiba (PR), Secretaria Municipal de
Saúde. Programa Mãe Curitibana: Pré-natal,
parto, puerpério e atenção ao recém-nascido:
REFERENCES
Cassimiro GN, Mata JAL. Adhesion to the use of ferrous sulphate...
English/Portuguese
J Nurs UFPE on line., Recife, 11(Suppl. 5):2156-67, May, 2017 2166
ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.9302-81402-1-RV.1105sup201722
2012 [Internet]. Curitiba: Secretaria Municipal
de Curitiba; 2012 [cited 2015 Nov 13].
Available from:
http://www.saude.curitiba.pr.gov.br/progra
mas/mae-curitibana.html
16. Milman N. Oral Iron Prophylaxis in
Pregnancy: not too little and not toomuch!
Review Article. J Pregnancy [Internet]. 2012
[cited 2015 Nov 13];2012(2012):ID514345.
Available from:
http://www.hindawi.com/journals/jp/2012/5
14345/
17. Souza AI, Batista Filho M, Ferreira LOC.
Alterações hematológicas e gravidez. Rev Bras
Hematol Hemoter [Internet]. 2002 [cited 2015
Nov 13];24(1):29-36. Available from:
http://www.scielo.br/pdf/rbhh/v24n1/a06v2
4n1.pdf
18. Carvalho MC, Baracat ECE, Sgarbieri VC.
Anemia Ferropriva e Anemia de Doença
Crônica: Distúrbios do Metabolismo de Ferro.
Segurança Alimentar Nutricional [Internet].
2006 [cited 2015 Nov 13];13(2):54-63.
Available from:
http://periodicos.sbu.unicamp.br/ojs/index.p
hp/san/article/view/1832/1885
19. Lemos SB, Liberali R, Coutinho VF,
Assumpção CO. Biodisponibilidade de ferro e a
Anemia Ferropriva na infância. Ensaios Ciênc
[Internet]. 2012 [cited 2015 Nov
13];16(4):213-28. Available from:
http://www.redalyc.org/pdf/260/2602923601
6.pdf
20. Milman N. Anemia—still a major health
problem in many parts of the world! Ann
Hematol. 2011 Apr;90(4):369-77. Doi:
10.1007/s00277-010-1144-5.
21. Penã-Rosas JP, Viteri FE. Effects of
routine oral iron supplementation with or
without folic acid for women during pregnancy
(Review).Cochrane Database Syst Rev
[Internet]. 2009 July [cited 2015 Nov
13]:19(3): CD004736. Available from:
http://onlinelibrary.wiley.com/doi/10.1002/1
4651858.CD004736.pub2/full
22. Ministério da Saúde (BR), Secretaria de
Ciência, Tecnologia e Insumos Estratégicos,
Departamento de Assistência Farmacêutica e
Insumos Estratégicos. Relação Nacional de
medicamentos essenciais: RENAME 2014
[Internet]. 9th ed. Brasília: Ministério da
Saúde; 2015. Available from:
http://www.saude.pr.gov.br/arquivos/File/0
DAF/RENAME2014ed2015.pdf
23. Leite SN, Vasconcellos MPC. Adesão à
terapêutica medicamentosa: elementos para a
discussão de conceitos e pressupostos
adotados na literatura. Ciênc Saúde Coletiva
[Internet]. 2003 [cited 2015 Nov 13];8(3):775-
82. Available from:
http://www.scielo.br/pdf/csc/v8n3/17457.pd
f
24. Silveira DS, Santos IS, Costa JSD. Atenção
pré-natal na rede básica: uma avaliação da
estrutura e do processo. Cad Saúde Pública
[Internet]. 2001 Jan/Feb [cited 2015 Nov
13];17(1):131-9. Available from:
http://www.scielo.br/pdf/csp/v17n1/4068.pd
f
25. Rios CTF, Vieira NFC. Ações educativas no
pré-natal: reflexão sobre a consulta de
enfermagem como um espaço para educação
em saúde. Ciênc Saúde coletiva [Internet].
2007 Mar/Apr [cited 2015 Nov 13];12(2):477-
86. Available from:
http://www.scielo.br/pdf/csc/v12n2/a24v12n
2.pdf
26. Nazaré B, Fonseca A, Canavarro MC.
Avaliação das preocupações sentidas durante
a gravidez: Estudos psicométricos da versão
portuguesa da Cambridge Worry Scale (CWS).
Lab Psicol [Internet]. 2012 [cited 2015 Nov
13];10(1):81-95. Available from:
http://publicacoes.ispa.pt/index.php/lp/artic
le/view/625/612
27. Mcardle HJ, Gambling L, Kennedy C. Iron
deficiency during pregnancy: the
consequences for placental function and fetal
outcome. Proc Nutr Soc. 2014 Feb;73(1):9-15.
Doi: 10.1017/S0029665113003637
28. Anand T, Rahi M, Sharma P, Ingle GK.
Issues in prevention of iron deficiency anemia
in India. Nutrition. 2014 July/Aug;30(7-8):764-
70. Doi: 10.1016/j.nut.2013.11.022
29. Piccinini CA, Carvalho FT, Ourique LR,
Lopes RS. Percepções e Sentimentos de
Gestantes sobre o Pré-natal. Psic: Teor e Pesq
[Internet]. 2012 Jan/Mar [cited 2015 Nov
15];28(1):27-33. Available from:
http://www.scielo.br/pdf/ptp/v28n1/04.pdf
30. Silva DC, Santos ACF, Magalhães RCSM,
Silva LMMO, Melo TMTC, Alencar GCA. Anemia
em mulheres universitárias e sua associação
com o consumo de alimentos. Rev enferm
UFPE online [Internet]. 2016 Jan [cited 2016
Fev 08];10(1):284-8. Available from:
https://periodicos.ufpe.br/revistas/revistaenf
ermagem/article/view/10951/12264

Cassimiro GN, Mata JAL. Adhesion to the use of ferrous sulphate...
English/Portuguese
J Nurs UFPE on line., Recife, 11(Suppl. 5):2156-67, May, 2017 2167
ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.9302-81402-1-RV.1105sup201722
Submission: 2016/02/08 Accepted: 2016/04/11 Publishing: 2017/05/15
Corresponding Address
Gabriele Nogueira Cassimiro Rua Vereador Engenheiro Ernani Batista Rosas, 3131, Bloco 23, Ap. 1 Bairro Jardim Carvalho
CEP: 840150150 Ponta Grossa (PR), Brazil





























