Embed Size (px)
Citation preview

OBSTRUCTIVE SLEEP OBSTRUCTIVE SLEEP APNEA IS A SYSTEMIC APNEA IS A SYSTEMIC
DISEASEDISEASE
Iman Galal, MDIman Galal, MDAssistant Professor Pulmonary MedicineAssistant Professor Pulmonary Medicine
Ain Shams UniversityAin Shams University

Page 2

Page 3
Al-Furqan, Chapter #25, Verse #47Al-Furqan, Chapter #25, Verse #47

Page 4
Obstructive Sleep Apnea Syndrome & Metabolic Obstructive Sleep Apnea Syndrome & Metabolic
Syndrome.Syndrome.
Obstructive Sleep Apnea Syndrome & Obstructive Sleep Apnea Syndrome &
Cardiovascular Diseases. Cardiovascular Diseases.
Effect of Continuous Positive Airway Pressure Effect of Continuous Positive Airway Pressure
treatment.treatment.
Content:Content:

Page 5
Obstructive Sleep Obstructive Sleep Apnea:Apnea:

Page 6
ObstructivObstructive Sleep e Sleep ApneaApnea
Memory Memory ProblemsProblems
IncreasedIncreased
Insulin Insulin
ResistanceResistance
StrokeStrokeIncreased Increased
Traffic Traffic AccidentsAccidents
Cardiac Cardiac ProblemsProblems
HypertensioHypertensionn

Page 7
Introduction:Introduction:Obstructive sleep apnea, Obstructive sleep apnea,
a highly prevalent a highly prevalent
disease, affecting 4% of disease, affecting 4% of
men & 2% of women, is a men & 2% of women, is a
disorder characterized by disorder characterized by
recurrent episodes of recurrent episodes of
upper airway obstruction, upper airway obstruction,
& is associated with & is associated with
reductions in ventilation, reductions in ventilation,
resulting in recurrent resulting in recurrent
arousals & episodic arousals & episodic
oxyhemoglobin oxyhemoglobin
desaturations during desaturations during
sleep.sleep.

Page 8
A variety of phenomena are implicated in OSAS A variety of phenomena are implicated in OSAS
such as modifications in the autonomic nervous such as modifications in the autonomic nervous
system, hypoxemia–reoxygenation cycles, system, hypoxemia–reoxygenation cycles,
inflammation, & coagulation–fibrinolysis imbalance.inflammation, & coagulation–fibrinolysis imbalance.
OSAS patients also present increased levels of OSAS patients also present increased levels of
certain biomarkers linked to endocrine-metabolic & certain biomarkers linked to endocrine-metabolic &
cardiovascular alterations among other systemic cardiovascular alterations among other systemic
consequences. consequences.
Introduction:Introduction:

Page 9
Metabolic Syndrome:Metabolic Syndrome:The National Cholesterol Education Program (NCEP) Adult The National Cholesterol Education Program (NCEP) Adult
Treatment Treatment
Panel III (ATP III) report recommended the use of 5 variables:Panel III (ATP III) report recommended the use of 5 variables:
1)1) Abdominal Obesity: Abdominal Obesity: waist circumference (≥102 cm in waist circumference (≥102 cm in ♂♂, ,
≥88 cm in ≥88 cm in ♀♀))
2)2) ↑ ↑ TG (≥150 mg/dL or drug treatment)TG (≥150 mg/dL or drug treatment)
3)3) ↓ ↓ HDL (<40 mg/dL in ♂, <50 mg/dL in ♀, or drug treatment)HDL (<40 mg/dL in ♂, <50 mg/dL in ♀, or drug treatment)
4)4) Hypertension: Hypertension: BP (systolic BP ≥130 mmHg, or diastolic BP BP (systolic BP ≥130 mmHg, or diastolic BP
≥ 85 mmHg, or drug treatment for hypertension)≥ 85 mmHg, or drug treatment for hypertension)
5)5) Glucose Intolerance: Glucose Intolerance: fasting glucose (≥100 mg/dL or drug fasting glucose (≥100 mg/dL or drug
treatment)treatment)
Subjects meeting 3 of these 5 criteria are classified as Subjects meeting 3 of these 5 criteria are classified as
having Metabolic Syndrome.having Metabolic Syndrome. Grundy et al. Circulation 2005; 112: 285-90Grundy et al. Circulation 2005; 112: 285-90

Page 10
Metabolic Syndrome:Metabolic Syndrome:
International Diabetes Federation (IDF) Consensus International Diabetes Federation (IDF) Consensus
Definition 2005 Criteria for Identification of the MS:Definition 2005 Criteria for Identification of the MS:
Alberti, Lancet 2005Alberti, Lancet 2005
Abdominal ObesityAbdominal Obesity: : (waist circumference) (waist circumference)
ethnicity specificethnicity specific
for Europids: Men >94 cmfor Europids: Men >94 cm
WomenWomen >80 cm>80 cm
Plus anyPlus any Two Two of the followingof the following
TriglyceridesTriglycerides ≥≥150 mg/dL150 mg/dL
HDL cholesterolHDL cholesterol
MenMen <40 mg/dL<40 mg/dL
WomenWomen <50 mg/dL<50 mg/dL
Blood PressureBlood Pressure ≥≥130 / ≥85mmHg130 / ≥85mmHg
Fasting GlucoseFasting Glucose ≥≥100mg/dL or Type II Diabetes100mg/dL or Type II Diabetes

Page 11
The metabolic disturbances in patients with The metabolic disturbances in patients with
obstructive sleep apnea syndrome (OSAS) include obstructive sleep apnea syndrome (OSAS) include
insulin resistance & elevated levels of pro-insulin resistance & elevated levels of pro-
inflammatory cytokines & vascular adhesion inflammatory cytokines & vascular adhesion
molecules, as well as an elevation of hormones molecules, as well as an elevation of hormones
derived from the adipose tissue as leptin. derived from the adipose tissue as leptin.
OSA & Metabolic SyndromeOSA & Metabolic Syndrome“Syndrome Z”“Syndrome Z”

Page 12
OSA & MS in AdultsOSA & MS in Adults
ReferenceReference DesignDesign ResultsResults
Coughlin et Coughlin et al.,2004al.,2004
Case controlled (matched for Case controlled (matched for BMI) BMI)
OSA: AHI > 15 OSA: AHI > 15
Control subjects: AHI < 5 Control subjects: AHI < 5
MS: NCEP (ATP III) criteria MS: NCEP (ATP III) criteria
Independent* associations between: Independent* associations between:
1.1. OSA & MSOSA & MS
2.2. OSA& systolic and diastolic blood pressure, OSA& systolic and diastolic blood pressure, fasting insulin, triglyceride, HDL, total/HDL fasting insulin, triglyceride, HDL, total/HDL cholesterol cholesterol
Gruber et al., 2006 Gruber et al., 2006
Case controlled Case controlled
OSA: AHI criteria not given OSA: AHI criteria not given
MS: International Diabetes MS: International Diabetes Federation criteria Federation criteria
Independent* association between: Independent* association between:
1.1. OSA & MSOSA & MS
2.2. No independent association between OSA & No independent association between OSA & insulin resistance (assessed by HOMA) insulin resistance (assessed by HOMA)
Lam et al., 2006Lam et al., 2006
Community based Community based
OSA: AHI > 5OSA: AHI > 5
MS: NCEP (ATP III) criteria MS: NCEP (ATP III) criteria
OSA and MS OSA and MS
Independent association between OSA & waist, Independent association between OSA & waist, diastolic blood pressure*, fasting glucose*, MS* diastolic blood pressure*, fasting glucose*, MS*
Independent determinants of OSA: age, gender, Independent determinants of OSA: age, gender, BMI, MS BMI, MS
Sasanabe et Sasanabe et al.,2006al.,2006
OSA: AHI > 15 OSA: AHI > 15
Control subjects: AHI < 5Control subjects: AHI < 5
MS: criteria for Japanese MS: criteria for Japanese populationpopulation
Independent* association between OSA & MS in Independent* association between OSA & MS in ♂♂ not in not in ♀♀
Parish et al., 2007Parish et al., 2007 Retrospective PSG & chart Retrospective PSG & chart review review
Higher prevalence of MS in patients with OSA (60 Higher prevalence of MS in patients with OSA (60 vs.40%) vs.40%)
Coughlin et al., Coughlin et al., 20072007
Randomized, controlled study Randomized, controlled study
MS: NCEP (ATP III) criteria MS: NCEP (ATP III) criteria
No change in proportion of subjects with MS with No change in proportion of subjects with MS with CPAPCPAP
Significant Significant ↓ ↓ in blood pressure in blood pressure

Page 13
OSA & Obesity:OSA & Obesity:OSAS often coexists with obesity.OSAS often coexists with obesity.
OSAS is present in approximately OSAS is present in approximately
40%40% of obese individuals, & of obese individuals, &
about about 70%70% of OSAS patients are of OSAS patients are
obese.obese.
In recent years, much attention In recent years, much attention
has been focused on the has been focused on the
interaction between OSAS & interaction between OSAS &
products released by adipose products released by adipose
tissue such as tissue such as Leptin, Leptin,
Adiponectin, Resistin & Adiponectin, Resistin &
Ghrelin.Ghrelin.

Page 14
OSA & Obesity:OSA & Obesity:
Gate et al., J Nutr Gate et al., J Nutr 20042004

Page 15
Leptin Leptin is an adipocyte-derived hormone thatis an adipocyte-derived hormone that
suppresses appetite & promotes satiety..
Several studies have shown increased levels of Several studies have shown increased levels of
LeptinLeptin in OSAS, suggesting resistance to the in OSAS, suggesting resistance to the
metabolic effects of leptin metabolic effects of leptin (Leptin Resistance).(Leptin Resistance).
Obesity is a major confounding factor in the Obesity is a major confounding factor in the
association between association between LeptinLeptin && OSA.OSA.
Treatment with CPAP reduces leptin levels & also Treatment with CPAP reduces leptin levels & also
may be associated with decreased visceral fat may be associated with decreased visceral fat
accumulation.accumulation.
OSA & Obesity:OSA & Obesity:

Page 16
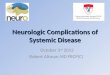
Sleep Apnea & Visceral FatSleep Apnea & Visceral Fat
AH
IA
HI
Visceral Fat (cmVisceral Fat (cm22))
SaO
SaO
22 n
ad
ir n
ad
ir %
%
0
20
40
60
80
100
50 150 250 350 450
r = .70p = .00
0
20
40
60
80
100
50 150 250 350 450
r = -.61p = .001
0
100
200
300
400
OSAOSA Obese Obese ControlsControls
*
Ab
dom
inal
Fat
Ab
dom
inal
Fat
Dis
trib
uti
on
(c
mD
istr
ibu
tion
(c
m22))
Subcutaneous FatSubcutaneous Fat
Visceral FatVisceral Fat
Vgontzas et al. J Clin Endocrin Metab 2000; 85: 1151-8Vgontzas et al. J Clin Endocrin Metab 2000; 85: 1151-8

Page 17
Effect of CPAP on Visceral FatEffect of CPAP on Visceral Fat
Fat
accu
mu
lati
on
(cm
Fat
accu
mu
lati
on
(cm
22))
BW=BW= BW BW
0
BW=BW= BW BW
100
200
300
* **
VisceralVisceral SubcutaneousSubcutaneous
Chin et al., Circulation 1999; 100: 706-12Chin et al., Circulation 1999; 100: 706-12

Page 18
OSA & Obesity:OSA & Obesity:
Increased LeptinIncreased Leptin::
Chin Chin et al., Circulationet al., Circulation 1999; 100: 706-12. 1999; 100: 706-12.
Ip Ip et al., Chestet al., Chest 2000; 118: 580-6. 2000; 118: 580-6.
Schafer Schafer et al., Chestet al., Chest 2002; 122: 829-39 2002; 122: 829-39 (Obesity+)(Obesity+)
Shimizu Shimizu et al., Thoraxet al., Thorax 2002; 57: 429-34. 2002; 57: 429-34.
Ozturk Ozturk et al., Arch Otolaryngol Head Neck Surget al., Arch Otolaryngol Head Neck Surg 2003; 129: 538- 2003; 129: 538-
40.40.
Sanner Sanner et al., Eur Respir Jet al., Eur Respir J 2004; 23: 601-4. 2004; 23: 601-4.
Shimura Shimura et al., Chestet al., Chest 2005; 127: 543-9 2005; 127: 543-9 (Hypercapnia+)(Hypercapnia+)
Barcelo Barcelo et al., Am J Respir Crit Care Medet al., Am J Respir Crit Care Med 2005; 171: 183-7 2005; 171: 183-7
(Obesity+)(Obesity+)
Tatsumi Tatsumi et al., Chestet al., Chest 2005; 127: 716-21. 2005; 127: 716-21.
Ulukavak Ciftci Ulukavak Ciftci et al., Respirationet al., Respiration 2005; 72: 395-401. 2005; 72: 395-401.

Page 19
AdiponectinAdiponectin is an adipocyte-derived cytokine with is an adipocyte-derived cytokine with
regulatory functions in both glucose & lipid regulatory functions in both glucose & lipid
metabolism.metabolism.
In addition,In addition, Adiponectin Adiponectin has profound anti-has profound anti-
inflammatory & antiatherogenic effects.inflammatory & antiatherogenic effects.
Plasma levels ofPlasma levels of AdiponectinAdiponectin decreases in obesity decreases in obesity
& metabolic syndromes e.g., OSAS.& metabolic syndromes e.g., OSAS.
CPAP treatment of OSAS does not effectively CPAP treatment of OSAS does not effectively
normalize normalize AdiponectinAdiponectin levels. levels.
OSA & Obesity:OSA & Obesity:
Harsch et al, Respiration 2004; 10: 710-580-6Harsch et al, Respiration 2004; 10: 710-580-6Zhang et al, Chin Med J 2004; 117: 1603-1606Zhang et al, Chin Med J 2004; 117: 1603-1606

Page 20
ResistinResistin is a white adipose tissue hormone whose is a white adipose tissue hormone whose
physiological function has not yet been established.physiological function has not yet been established.
In a study of 20 obese OSA patients, there was a In a study of 20 obese OSA patients, there was a
weak link between weak link between ResistinResistin & & Insulin Sensitivity.Insulin Sensitivity.
CPAP treatment of OSA had no significant influence CPAP treatment of OSA had no significant influence
on on ResistinResistin levels.levels.
OSA & Obesity:OSA & Obesity:
Harsch et al, Med Sci Monit 2004; 10: 510-5Harsch et al, Med Sci Monit 2004; 10: 510-5

Page 21
OSA & Obesity:OSA & Obesity:
AdiponectinAdiponectin:: variable results variable results
Zhang Zhang et al.,et al., Chin Med JChin Med J 2004; 117: 1603-1606 2004; 117: 1603-1606
Harsch Harsch et al., Respirationet al., Respiration 2004; 71: 580-586 (obesity+) 2004; 71: 580-586 (obesity+)
Wolk Wolk et al., Obes Reset al., Obes Res 2005; 13: 186-190 2005; 13: 186-190
Zhang Zhang et al.,et al., RespirationRespiration 2006; 73: 73-77 2006; 73: 73-77
Makino Makino et al., Clin Endocrinolet al., Clin Endocrinol 2006; 64:12-19 2006; 64:12-19
Resistin:Resistin:
Harsch Harsch et al., Med Sci Monitet al., Med Sci Monit 2004; 10: 510-5 2004; 10: 510-5 (insulin sensitivity ±, (insulin sensitivity ±,
inflammation+)inflammation+)
Ghrelin:Ghrelin: variable resultsvariable results
Harsch Harsch et al., Eur Respir Jet al., Eur Respir J 2003; 22:251-257 2003; 22:251-257
Ulukavak Ulukavak et al.,et al., RespirationRespiration 2005; 72: 395-401 = 2005; 72: 395-401 =

Page 22
OSA & Obesity:OSA & Obesity:
OSA is less prevalent in OSA is less prevalent in ♀ than ♂, yet this difference ♀ than ♂, yet this difference
diminishes after menopause 2ry to the decline in estrogen & diminishes after menopause 2ry to the decline in estrogen &
progesteroneprogesterone..
Accordingly, estrogen replacement therapy in Accordingly, estrogen replacement therapy in
menopausal ♀menopausal ♀ lessens the prevalence of OSAS.lessens the prevalence of OSAS.
OSAS in ♂ causes reduced pituitary-gonadal OSAS in ♂ causes reduced pituitary-gonadal
function (possibly 2ry to obesity) function (possibly 2ry to obesity) → → decline in decline in
morning serum testosterone levels, reduced morning serum testosterone levels, reduced
androgen secretion & libido. In addition, androgen secretion & libido. In addition, ↑ ↑ leptin leptin → →
impaired testicular Leyding cell function.impaired testicular Leyding cell function.Anttalainen et al., Acta Obstet Gynecol Scand 2006; 85: 1381-8Anttalainen et al., Acta Obstet Gynecol Scand 2006; 85: 1381-8Wesstrom et al., Acta Obstet Gynecol Scand 2005; 84: 54-7Wesstrom et al., Acta Obstet Gynecol Scand 2005; 84: 54-7Teloken et al., Urology2006; 76:1033-7Teloken et al., Urology2006; 76:1033-7Luboshitzky et al., Obes Res2005;13:780-6Luboshitzky et al., Obes Res2005;13:780-6Ishikawa et al., Andrologia2007;39:22-7Ishikawa et al., Andrologia2007;39:22-7

Page 23
Insulin ResistanceInsulin Resistance
Kasuga, J Clin Invest 2006Kasuga, J Clin Invest 2006
NormalNormal
NormalNormal
IncreasedIncreased
Normal or IGT Normal or IGT Diabetes mellitus Diabetes mellitus
DecreasedDecreased
PancreaticPancreatic IsletsIslets
cell compensationcell compensation cell failurecell failure
InsulinInsulinsecretion secretion by by cells cells
Blood Blood glucoseglucose

Page 24
Insulin Signaling in CellsInsulin Signaling in Cells
Kasuga, J Clin Invest 2006Kasuga, J Clin Invest 2006

Page 25
Relation between OSA, MS & Type II DMRelation between OSA, MS & Type II DM
Tasali & Ip, Tasali & Ip, he Proceedings of the American Thoracic Society 2008;5:207-17he Proceedings of the American Thoracic Society 2008;5:207-17

Page 26
OSA & Diabetes Mellitus:OSA & Diabetes Mellitus:
In 2001, El Masry & co-workers proved that the In 2001, El Masry & co-workers proved that the
prevalence of severe OSA was significantly higher in prevalence of severe OSA was significantly higher in
diabetic patients than in normoglycaemic subject diabetic patients than in normoglycaemic subject
independent of BMI.independent of BMI.
Although obesity is the main risk factor for Although obesity is the main risk factor for
diabetes, yet coexistent severe OSA may add to this diabetes, yet coexistent severe OSA may add to this
risk .risk .
El Masry et al., J Intern Med. 2001; 249: 153-61El Masry et al., J Intern Med. 2001; 249: 153-61

Page 27
ReferenceReferenceTTT TTT
PeriodPeriodStudy PopulationStudy Population Measures of Measures of
GlucoseGlucose Main ResultsMain Results
Brooks et al.,1994Brooks et al.,1994 4 ms4 ms10 severely obese 10 severely obese pts with DM with pts with DM with
OSA OSA
Hyperinsulinemic Hyperinsulinemic euglycemic clamp euglycemic clamp
Improvement in Improvement in insulin sensitivity insulin sensitivity
Harsh et al.2004 Harsh et al.2004 3 ms3 ms 40 Pts without DM 40 Pts without DM with OSA with OSA
Hyperinsulinemic Hyperinsulinemic euglycemic clamp euglycemic clamp
Improvement in Improvement in insulin sensitivity insulin sensitivity
Harsh et al.2004 Harsh et al.2004 3 ms3 ms 9 Pts with DM with 9 Pts with DM with OSA OSA
Hyperinsulinemic Hyperinsulinemic euglycemic clamp euglycemic clamp
Improvement in Improvement in insulin sensitivity insulin sensitivity
Babu et al.,2005Babu et al.,2005 3 ms3 ms 25 Pts with DM 25 Pts with DM with OSA with OSA
72-h interstitial 72-h interstitial glucoseHemoglobin glucoseHemoglobin
A1c A1c
Improvement in Improvement in 1h postprandial 1h postprandial
glucose & glucose & decrease in decrease in
hemoglobin A1c hemoglobin A1c
Hassaballa et Hassaballa et al.,2005al.,2005 3-4 ms3-4 ms 38 Pts with DM 38 Pts with DM
with OSA with OSA Hemoglobin A1c Hemoglobin A1c Slight decrease in Slight decrease in hemoglobin A1c hemoglobin A1c
Lindberg et Lindberg et al.,2006 al.,2006 3 wks3 wks
28 28 ♂♂ with OSA with OSA
28 Matched 28 Matched control control ♂♂
Fasting insulin & Fasting insulin & HOMA HOMA
Reductions in Reductions in fasting insulin fasting insulin
levels & IR levels & IR
Effect of CPAP on Glucose Metabolism:Effect of CPAP on Glucose Metabolism:

Page 28
ReferenceReferenceTTT TTT
PerioPeriodd
Study Study PopulationPopulation
Measures of Measures of GlucoseGlucose
Main ResultsMain Results
Saini et al.,1993Saini et al.,1993 1 1 NightNight
8 pts with 8 pts with OSA OSA
Profiles of glucose & Profiles of glucose & insulin at nightinsulin at night
No change in nocturnal glucose & No change in nocturnal glucose & insulin profiles insulin profiles
Cooper et al.1995Cooper et al.1995 1 1 NightNight
6 Obese ♂ 6 Obese ♂ Pts Pts
without without DM with DM with
OSA OSA
Profiles of glucose & Profiles of glucose & insulin at nightinsulin at night
No change in nocturnal glucose & No change in nocturnal glucose & insulin profiles insulin profiles
Stoohs et al.2004 Stoohs et al.2004 2 ms2 ms 5 Pts with 5 Pts with OSA OSA
Fasting glucose & Fasting glucose & insulininsulin
Profiles of glucose & Profiles of glucose & insulin at nightinsulin at night
↑↑ in fasting & nocturnal glucose levelsin fasting & nocturnal glucose levels
No change in fasting or nocturnal No change in fasting or nocturnal insulin levels insulin levels
Saarlainen et Saarlainen et al.,1997al.,1997 3 ms3 ms 7 Pts with 7 Pts with
OSA OSA Hyperinsulinemic Hyperinsulinemic euglycemic clampeuglycemic clamp No improvement in insulin sensitivity No improvement in insulin sensitivity
Ip et al.,2000Ip et al.,2000 6 ms6 ms 9 Pts with 9 Pts with OSA OSA
Fasting glucose & Fasting glucose & insulininsulin
No change in fasting glucose & insulin No change in fasting glucose & insulin levels levels
Sumurra et al.,2006 Sumurra et al.,2006 2 ms2 ms 16 pts with 16 pts with OSAOSA
Hyperinsulinemic Hyperinsulinemic euglycemic clampeuglycemic clamp
OGTTOGTT
No change in insulin sensitivity & No change in insulin sensitivity & glucose tolerance glucose tolerance
Czupryniak et Czupryniak et al.,2005al.,2005
1 1 NightNight
9 pts without 9 pts without DM with DM with
OSAOSA
Nocturnal Intestinal Nocturnal Intestinal glucoseglucose
Fasting insulin & Fasting insulin & HOMAHOMA
↑↑ in nocturnal glucose in nocturnal glucose
No difference in fasting insulin levels No difference in fasting insulin levels & IR& IR
Coughlin et al.,2007 Coughlin et al.,2007 6 wks6 wks 34 Obese pts 34 Obese pts with OSAwith OSA HOMAHOMA
No change in insulin sensitivity with No change in insulin sensitivity with therapeutic CPAP vs. with placebo therapeutic CPAP vs. with placebo
CPAP CPAP
Effect of CPAP on Glucose Metabolism:Effect of CPAP on Glucose Metabolism:

Page 29
OSA & Cardiovascular System:OSA & Cardiovascular System:The association of OSAS & cardiovascular The association of OSAS & cardiovascular
consequences can consequences can
be addressed by 3 key questions:be addressed by 3 key questions:
FirstFirst:: Is OSA an independent cardiovascular risk Is OSA an independent cardiovascular risk
factor? factor?
Second:Second: If so, does treatment of OSA reduce If so, does treatment of OSA reduce
cardiovascular risk, morbidity & cardiovascular risk, morbidity &
mortality?mortality?
ThirdThird:: Is screening for OSAS indicated for Is screening for OSAS indicated for
patients at risk patients at risk
for cardiovascular disease?for cardiovascular disease?

Page 30
Cardiovascular Events In OSA:Cardiovascular Events In OSA:
Abu et al, JAMA. 2003;290:1906-1914 Abu et al, JAMA. 2003;290:1906-1914

Page 31
OSA & Cardiovascular System:OSA & Cardiovascular System:
Somers et al, N Engl J Med. 1993;328:303-307 Somers et al, N Engl J Med. 1993;328:303-307
In healthy individuals, physiologic normal sleep is In healthy individuals, physiologic normal sleep is
associated with distinct sleep stage–related associated with distinct sleep stage–related
changes in cardiovascular regulation.changes in cardiovascular regulation.
Sympathetic nerve traffic to muscles, as well as HR, Sympathetic nerve traffic to muscles, as well as HR,
BP, SV, COP, & SVR, all decrease progressively BP, SV, COP, & SVR, all decrease progressively
during deeper stages of NREM sleep.during deeper stages of NREM sleep.
However, REM sleep is accompanied by striking However, REM sleep is accompanied by striking
increases in sympathetic drive. increases in sympathetic drive.

Page 32
OSA & Cardiovascular System:OSA & Cardiovascular System:
Narkiewicz et al, Circulation 1998;97:943–945Narkiewicz et al, Circulation 1998;97:943–945
The mechanism for increased sympathetic The mechanism for increased sympathetic
activation is not known.activation is not known.
One possibility is that increased chemoreflex gain One possibility is that increased chemoreflex gain
in OSA results in tonic chemoreflex activation even in OSA results in tonic chemoreflex activation even
during normoxia, with consequent increased during normoxia, with consequent increased
sympathetic activity. sympathetic activity.
Administration of 100% oxygen Administration of 100% oxygen (to eliminate tonic (to eliminate tonic
chemoreflex drive)chemoreflex drive) significantly lowers sympathetic significantly lowers sympathetic
activity, HR, & BP in OSA patients during daytime activity, HR, & BP in OSA patients during daytime
wakefulness.wakefulness.

Page 33
Neural & Circulatory Changes in OSA:Neural & Circulatory Changes in OSA:
Somers et al, J Clin Invest. 1995;96:1897-1904 Somers et al, J Clin Invest. 1995;96:1897-1904

Page 34
Somers et al, J Clin Invest 1995Somers et al, J Clin Invest 1995
Neural & Circulatory Changes in OSA:Neural & Circulatory Changes in OSA:

Page 35
Impaired Cardiovascular Variability:Impaired Cardiovascular Variability:
Narkiewicz et al, Circulation 1998;98:1071–77Narkiewicz et al, Circulation 1998;98:1071–77Singh et al, Hypertension 1998;32:293–97 Singh et al, Hypertension 1998;32:293–97 Fratolla et al, J Hypertens 1993;11:1133–37Fratolla et al, J Hypertens 1993;11:1133–37
Compared with similarly obese control subjects, Compared with similarly obese control subjects,
resting awake OSA patients have diminished heart resting awake OSA patients have diminished heart
rate variability & increased BP variability. rate variability & increased BP variability.
The Framingham Heart Study has implicated lower The Framingham Heart Study has implicated lower
HR variability as a precursor to the development of HR variability as a precursor to the development of
future hypertension, & increased BP variability has future hypertension, & increased BP variability has
been implicated in increased risk of end-organ been implicated in increased risk of end-organ
damage in patients with hypertension.damage in patients with hypertension.

Page 36
Heart Rate Variability in OSA:Heart Rate Variability in OSA:
Thurnbeer, Swiss Med Wkly 2007; 137: 217-22Thurnbeer, Swiss Med Wkly 2007; 137: 217-22Var: HR variability, variability of > 6 bpm

Page 37
In OSA, the combination of repetitive hypoxemia & In OSA, the combination of repetitive hypoxemia &
sleep deprivation may be associated with increased sleep deprivation may be associated with increased
levels of plasma cytokines e.g., IL-6, levels of plasma cytokines e.g., IL-6, αα-TNF, CAMs, -TNF, CAMs,
serum amyloid A, & CRP.serum amyloid A, & CRP.
CRP contribute to vascular disease & dysfunction by CRP contribute to vascular disease & dysfunction by
inhibiting nitric oxide synthase & increasing inhibiting nitric oxide synthase & increasing
expression of cell adhesion molecules.expression of cell adhesion molecules.
Adhesion of circulating leukocytes to the endothelial Adhesion of circulating leukocytes to the endothelial
cells is considered one of the initial steps in the cells is considered one of the initial steps in the
pathogenesis of atherosclerosis.pathogenesis of atherosclerosis.
OSA & OSA & Inflammation:Inflammation:
Vgontzas et al, J Clin Endocrinol Metab. Vgontzas et al, J Clin Endocrinol Metab. 1997;82:1313-161997;82:1313-16Shamsuzzaman et al, Circulation. 2002;105:2462-Shamsuzzaman et al, Circulation. 2002;105:2462-6464Venugopa et al, Circulation. 2002;106:1439-41Venugopa et al, Circulation. 2002;106:1439-41Ross et al, Nature;1993;362:801-809Ross et al, Nature;1993;362:801-809

Page 38
0
0.5
1
1.5
2
2.5
3
0
1
2
3
4
pg/mL
Normal OSA Narcolepsy Idiopathic Hypersomnia
TN
F
IL-6
**
Normal OSAOSA NarcolepsyNarcolepsy Idiopathic Idiopathic HypersomniaHypersomnia
Cytokines & Disorders of EDS:Cytokines & Disorders of EDS:
Vgontzas et.al., 1997Vgontzas et.al., 1997

Page 39
OSA & Adhesion OSA & Adhesion Molecules:Molecules:
Galal IH (2007)Galal IH (2007)
0
100
200
300
400
500
600
700
0 1 2 3 4
sICAM-1
ng/mL
0
500
1000
1500
2000
2500
3000
3500
0 1 2 3 4
sVCAM-1
ng/mL

Page 40
In OSA, the hypoxia/reoxygenation phenomenon In OSA, the hypoxia/reoxygenation phenomenon
that occurs in response to apneas followed by that occurs in response to apneas followed by
hyperventilation, may elicit increased vascular hyperventilation, may elicit increased vascular
oxidative stress.oxidative stress.
Low oxygen tension is a trigger for activation of Low oxygen tension is a trigger for activation of
polymorphonuclear neutrophils, which adhere to polymorphonuclear neutrophils, which adhere to
the endothelium & release free oxygen radicals.the endothelium & release free oxygen radicals.
Prevention of OSA by CPAP reduces production of Prevention of OSA by CPAP reduces production of
superoxide.superoxide.
OSA & Oxidative OSA & Oxidative Stress:Stress:
Schulz et al, Am J Respir Crit Care Med. 2000;162:566-Schulz et al, Am J Respir Crit Care Med. 2000;162:566-7070Prabhakar et al, Am J Respir Crit Care Med. Prabhakar et al, Am J Respir Crit Care Med. 2002;165:859-602002;165:859-60

Page 41
Hypercoagulability in OSAS results from the Hypercoagulability in OSAS results from the
imbalance between coagulation & fibrinolysis.imbalance between coagulation & fibrinolysis.
Increases in hematocrit, nocturnal & daytime levels Increases in hematocrit, nocturnal & daytime levels
of fibrinogen, platelet aggregation, blood viscosity, of fibrinogen, platelet aggregation, blood viscosity,
FVIIa, FXIIa, VWF, D-dimer & fibrinolysis-inhibiting FVIIa, FXIIa, VWF, D-dimer & fibrinolysis-inhibiting
enzyme plasminogen inhibitor (PAI-1) in OSA, likely enzyme plasminogen inhibitor (PAI-1) in OSA, likely
contribute to predisposition to clot formation & contribute to predisposition to clot formation &
atherosclerosis.atherosclerosis.
CPAP therapy can alleviate some of these CPAP therapy can alleviate some of these
abnormalities & can reduce factor VII clotting abnormalities & can reduce factor VII clotting
activity.activity.
OSA & OSA & Hpercoagulability:Hpercoagulability:
Hoffstein al, Chest. 1994;106:787-91Hoffstein al, Chest. 1994;106:787-91Chin et al, Am J Resp Crit Care Med. 1996;153:1972-76Chin et al, Am J Resp Crit Care Med. 1996;153:1972-76Nobil et al, Clin Hemorheol Microcirc. 2000;22:21-27Nobil et al, Clin Hemorheol Microcirc. 2000;22:21-27Wessendorf et al, Am J Resp Crit Care Med. Wessendorf et al, Am J Resp Crit Care Med. 2000;162:2039-422000;162:2039-42

Page 42
OSA & Endothelial Dysfunction:OSA & Endothelial Dysfunction:
The hypoxia, hypercapnia, & pressor surges accompanying The hypoxia, hypercapnia, & pressor surges accompanying
obstructive apneic events serve as potent stimuli for obstructive apneic events serve as potent stimuli for ↑ ↑ inin the the
release of endothelin & release of endothelin & ↓↓ in NO in NO → → endothelial dysfunction.endothelial dysfunction.
Endothelial dysfunction is often seen with OSA comorbidites Endothelial dysfunction is often seen with OSA comorbidites
e.g., HTN, hyperlipidemia, DM, or smoking → e.g., HTN, hyperlipidemia, DM, or smoking → ↑↑ risk of risk of
cardiovascular events.cardiovascular events.
In addition, OSA itself may be an independent risk factor for In addition, OSA itself may be an independent risk factor for
the development of endothelial dysfunction.the development of endothelial dysfunction.
CPAP treatment plays an important role in the improvement CPAP treatment plays an important role in the improvement
& protection of vascular endothelial dysfunction.& protection of vascular endothelial dysfunction.Zhang et al, Chin Med J. 200;116:844-7Zhang et al, Chin Med J. 200;116:844-7Zamarron et al., Eur J Inten Med.2008;19:390-8 Zamarron et al., Eur J Inten Med.2008;19:390-8

Page 43
Cardiovascular Events In OSA:Cardiovascular Events In OSA:
Abu et al, JAMA. 2003;290:1906-14 Abu et al, JAMA. 2003;290:1906-14

Page 44
It is estimated that 50% of It is estimated that 50% of
OSA patients are OSA patients are
hypertensive, & 30% of hypertensive, & 30% of
hypertensive patients also hypertensive patients also
have OSA, often have OSA, often
undiagnosed.undiagnosed.
OSA & Hypertension:OSA & Hypertension:
Silverberg et al, Curr Opin Nephrol Hypertens. Silverberg et al, Curr Opin Nephrol Hypertens. 1998;7:353–71998;7:353–7Fletcher et al., Ann Intern Med. 1985;103:190 –5Fletcher et al., Ann Intern Med. 1985;103:190 –5

Page 45
OSAS is identified as an independent risk factor for OSAS is identified as an independent risk factor for
the onset of arterial hypertension.the onset of arterial hypertension.
A clear dose-effect is evident: the more apneas/ hr A clear dose-effect is evident: the more apneas/ hr
of sleep, the higher the chance for becoming of sleep, the higher the chance for becoming
hypertensive.hypertensive.
In 2003, theIn 2003, the “Joint National Council on High Blood “Joint National Council on High Blood
Pressure” listed OSA as the first identifiable cause Pressure” listed OSA as the first identifiable cause
of arterial hypertension.of arterial hypertension.Harsch et al, Med Sci Monit 2004; 10: 510-5Harsch et al, Med Sci Monit 2004; 10: 510-5
OSA & Hypertension:OSA & Hypertension:

Page 46
Potential mechanisms linking OSA with Potential mechanisms linking OSA with HTN:HTN:
Hoffmann et al, Minerva Med. 2004;95:281-90Hoffmann et al, Minerva Med. 2004;95:281-90
Obstructive Sleep ApneaObstructive Sleep Apnea
HYPERTENSIONHYPERTENSION
Chemoreflex activationChemoreflex activationBaroreflex dysfunctionBaroreflex dysfunction
ArousalsArousalsIntrathoracic pressure Intrathoracic pressure
changeschanges
Sympathetic activationSympathetic activation Leptin RLeptin RInsulin RInsulin R
InflammationInflammation
Oxidative Oxidative stressstress
ObesityObesity
RAS RAS activatioactivatio
nn
EndothelialEndothelialdysfunctiondysfunction

Page 47
Drug-Resistant HypertensionDrug-Resistant Hypertension:: (clinical blood (clinical blood
pressure of >140/90mmHg while taking a sensible pressure of >140/90mmHg while taking a sensible
combination of ≥ antihypertensive drugs) a high combination of ≥ antihypertensive drugs) a high
prevalence of OSAS has been reported.prevalence of OSAS has been reported.
(Fletcher EC 1985, Isaksson (Fletcher EC 1985, Isaksson
H, 1991)H, 1991)
In a group of 41 patients taking a mean of 3.6 In a group of 41 patients taking a mean of 3.6
different antihypertensive medications daily:different antihypertensive medications daily:
96%96% of the men & of the men & 65%65% of the women had OSAS, of the women had OSAS,
with men suffering from more severe OSAS (AHI with men suffering from more severe OSAS (AHI
32 vs. 14). 32 vs. 14).
(Logan AG, (Logan AG,
2001)2001)
OSA & Hypertension:OSA & Hypertension:

Page 48
60
80
100
120
140
MAP
(mmH
g)
baseline
effective nCPAP
715 pm 1115 pm 315 am 715 am315 pm 1115 am
Becker, Circulation 2003Becker, Circulation 2003
Effect of nCPAP on Blood Pressure in Effect of nCPAP on Blood Pressure in OSA:OSA:
-25
-20
-15
-10
-5
0
5
10
15
mmHg
* * *
MAP systolic diastolic

Page 49
OSA & Heart Failure:OSA & Heart Failure:
Marin et al., Lancet. 2005; 365:1 046 –Marin et al., Lancet. 2005; 365:1 046 –5353
OSA contribute to the progression of heart OSA contribute to the progression of heart
failurefailure
through several pathological mechanisms:through several pathological mechanisms:
1)1) by eliciting greater sympathetic outflow to the heart, kidney, by eliciting greater sympathetic outflow to the heart, kidney,
& resistance vessels during wakefulness & sleep. & resistance vessels during wakefulness & sleep.
2)2) by increasing left ventricular afterload both acutely & by increasing left ventricular afterload both acutely &
chronically. chronically.
3)3) by inducing hypoxia & 2ry increases in right ventricular by inducing hypoxia & 2ry increases in right ventricular
afterload. afterload.
4)4) by increasing the risk of myocardial infarction.by increasing the risk of myocardial infarction.
However, yet to be established is whether OSA can However, yet to be established is whether OSA can
causecause
heart failure. In addition, whether the presence of heart failure. In addition, whether the presence of
OSA inOSA in
Heart failure accelerates mortality remains unclear.Heart failure accelerates mortality remains unclear.

Page 50
Heart failure patients with CPAP-treated OSA have Heart failure patients with CPAP-treated OSA have
low mortality rate compared with untreated OSA.low mortality rate compared with untreated OSA.
Effect of treatment on OSA on HF:Effect of treatment on OSA on HF:
Wang et al., J Am Coll CardiolWang et al., J Am Coll Cardiol. . 2007;49:1625-312007;49:1625-31

Page 51
Epidemiological data suggest that OSA is Epidemiological data suggest that OSA is
overrepresented in patients with CAD.overrepresented in patients with CAD.
Conversely, the clinical course of CAD is initiated Conversely, the clinical course of CAD is initiated
(or) accelerated by the presence of OSA.(or) accelerated by the presence of OSA.
More than half of sudden cardiac deaths in patients More than half of sudden cardiac deaths in patients
with proven OSA occur during the sleeping hours with proven OSA occur during the sleeping hours
(between 10 PM & 6 AM). Thus, OSA appears to (between 10 PM & 6 AM). Thus, OSA appears to
affect the timing of sudden cardiac death.affect the timing of sudden cardiac death.
OSA & CAD:OSA & CAD:
Hedner et al., 2005Hedner et al., 2005Somers et al., JACC 2008;52:686–Somers et al., JACC 2008;52:686–717717

Page 52
In patients with combined OSA & CAD, treatment
of OSA was associated with a decrease in the
occurrence of new cardiovascular events.
Repots from patients’ spouses describe marked
changes in sleep patterns, snoring severity, &
witnessed apneas after bypass surgery and
sometimes even after angioplasty.
Effect of treatment on OSA & CAD:Effect of treatment on OSA & CAD:
Milleron et al., Eur Heart J. 2004;25:728 Milleron et al., Eur Heart J. 2004;25:728 –34–34Somers et al., JACC 2008;52:686–717Somers et al., JACC 2008;52:686–717

Page 53
OSA & Arrhythmia:OSA & Arrhythmia:
Zwillich et al, J Clin Invest. Zwillich et al, J Clin Invest. 1982;69:1286-921982;69:1286-92Somers et al., JACC 2008;52:686–717Somers et al., JACC 2008;52:686–717
Nocturnal arrhythmias have been Nocturnal arrhythmias have been
reported in reported in up to 50% of patients patients
with OSA even in absence of pre-with OSA even in absence of pre-
existing cardiac disease.existing cardiac disease.
The most common arrhythmias The most common arrhythmias
include include 22ndnd degree heart block degree heart block, ,
AFAF, , ventricular extrasystoleventricular extrasystole & &
sinus bradycardiasinus bradycardia, representing , representing
in part the diving reflex response in part the diving reflex response
to apnea & hypoxiato apnea & hypoxia

Page 54
Recurrence of AF After Cardioversion:Recurrence of AF After Cardioversion:
0102030405060708090
100
Controls (n=79) Treated OSA(n=12)
Untreated Osa(n=27)
% Recurrence at 12 Months
**
Kanagola et al, Circ 107:2589, 2003Kanagola et al, Circ 107:2589, 2003

Page 55
In small series of patients with OSA In small series of patients with OSA (without (without
clinical history of chronic obstructive pulmonary clinical history of chronic obstructive pulmonary
disorder)disorder) the reported daytime pulmonary arterial the reported daytime pulmonary arterial
hypertension was found in 20- 42% of caseshypertension was found in 20- 42% of cases
The most likely primary mechanism OSA-related The most likely primary mechanism OSA-related
PAH is hypoxemia, which is known to reflexively PAH is hypoxemia, which is known to reflexively
induce an acute increase in PAP.induce an acute increase in PAP.
OSA & PAH:OSA & PAH:
Yamakawa et al, Psychiatry Clin Yamakawa et al, Psychiatry Clin Neurosci.,2002;56:311–12Neurosci.,2002;56:311–12Voelkel, Am Rev Respir Dis. 1986;133:1186 –95Voelkel, Am Rev Respir Dis. 1986;133:1186 –95

Page 56Buchner et al. AJRCCM 2007Buchner et al. AJRCCM 2007
CPAP Treatment & Cardiovascular Risk:CPAP Treatment & Cardiovascular Risk:

Page 57
*
Cardiovascular Disease & Mortality in Cardiovascular Disease & Mortality in OSAS:OSAS:
Doherty et al. Chest 2005; 127: 2076-84Doherty et al. Chest 2005; 127: 2076-84

Page 58
Memories are formed in the mammillary bodies.Memories are formed in the mammillary bodies.
When UCLA neuroscientists* scanned the brains of 43 sleep When UCLA neuroscientists* scanned the brains of 43 sleep
apnea patients & 66 healthy volunteers using magnetic MRI, apnea patients & 66 healthy volunteers using magnetic MRI,
they discovered that the OSA patients’ mammillary bodies they discovered that the OSA patients’ mammillary bodies
were nearly 20% smaller than those of the untroubled were nearly 20% smaller than those of the untroubled
sleepers. sleepers.
OSA & Memory Affection:OSA & Memory Affection:
*Newswise: Study Links Common Sleep Disorder to Memory Loss Retrieved on June 11, 2008*Newswise: Study Links Common Sleep Disorder to Memory Loss Retrieved on June 11, 2008

Page 59
Stroke has been linked to OSA & sleep apnea is Stroke has been linked to OSA & sleep apnea is
highly prevalent in patients with stroke.highly prevalent in patients with stroke.
Mechanisms that have been implicated in any Mechanisms that have been implicated in any
increased risk of stroke in OSA include BP swings, increased risk of stroke in OSA include BP swings,
reduction in cerebral blood flow, altered cerebral reduction in cerebral blood flow, altered cerebral
autoregulation, impaired endothelial function, autoregulation, impaired endothelial function,
accelerated atherogenesis, & prothrombotic & accelerated atherogenesis, & prothrombotic &
proinflammatory states.proinflammatory states.
OSA & Stroke:OSA & Stroke:
Somers et al., JACC 2008;52:686–717Somers et al., JACC 2008;52:686–717

Page 60
OSA & Stroke:OSA & Stroke:
Bassetti & Aldrich, Sleep 22:217, 1999Bassetti & Aldrich, Sleep 22:217, 1999
0
5
10
15
20
25
30
35
Stroke (n=48) TIA (n=32) Controls (n=25)
Ave
rage
AH
I (E
piso
des/
hour
)

Page 61
The prevalence of OSA in ESRD ranged from 40% - The prevalence of OSA in ESRD ranged from 40% -
60%.60%.
Long-standing OSA contributes to the origin of Long-standing OSA contributes to the origin of
ESRD by inducing chronic elevations in BP & ESRD by inducing chronic elevations in BP &
increasing sympathetic nerve discharge directed at increasing sympathetic nerve discharge directed at
the kidney & other vascular beds.the kidney & other vascular beds.
OSA & End-Stage Renal Disease:OSA & End-Stage Renal Disease:
Hanly, Semin Dial. 2004;17:109 –14Hanly, Semin Dial. 2004;17:109 –14

Page 62
ConclusionConclusion

Page 63
Zamarron, Eur J Int Med Zamarron, Eur J Int Med 2008; 19: 390-982008; 19: 390-98

Page 64
The Association of OSAS with The Association of OSAS with
Endocrine-Metabolic & Endocrine-Metabolic &
Cardiovascular Alternations Cardiovascular Alternations
indicates that, More than a indicates that, More than a
Local Abnormality, OSAS should Local Abnormality, OSAS should
be considered a Systemic be considered a Systemic
Disease. Disease.

Page 65

Page 66
Ar-Room, Chapter #30, Verse #23Ar-Room, Chapter #30, Verse #23

Page 67













![AAU-Hematologic Aspect of Systemic Disease[1]](https://img.dokumen.tips/doc/110x75/546874efb4af9f533f8b5d3f/aau-hematologic-aspect-of-systemic-disease1.jpg)













