Embed Size (px)
Citation preview
Microalbuminuria

object .• Introduction for renal system• protein & urine• Define microalbuminuria• Causes • consequence • Pathogenesis • Sign & symptoms • Possible Mangement & prophylaxis
Introduction for renal system
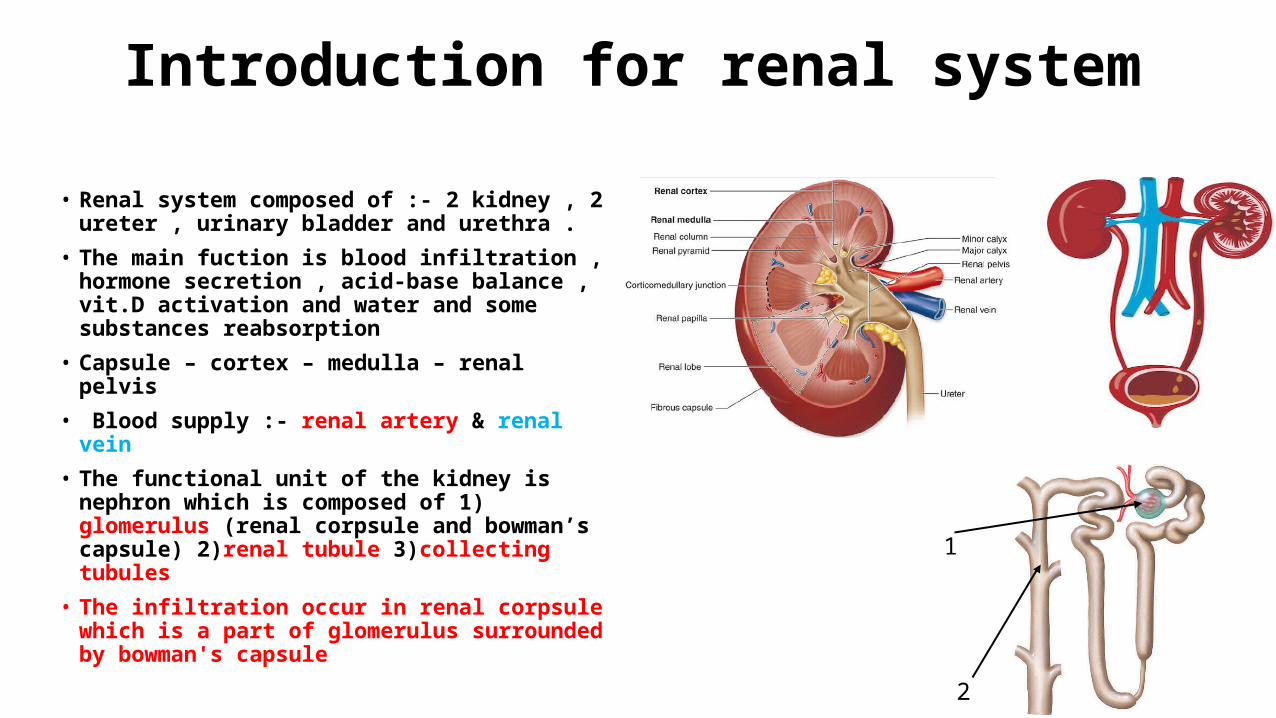
• Renal system composed of :- 2 kidney , 2 ureter , urinary bladder and urethra .
• The main fuction is blood infiltration , hormone secretion , acid-base balance , vit.D activation and water and some substances reabsorption
• Capsule – cortex – medulla – renal pelvis• Blood supply :- renal artery & renal vein • The functional unit of the kidney is nephron
which is composed of 1) glomerulus (renal corpsule and bowman’s capsule) 2)renal tubule 3)collecting tubules
• The infiltration occur in renal corpsule which is a part of glomerulus surrounded by bowman's capsule
1
2
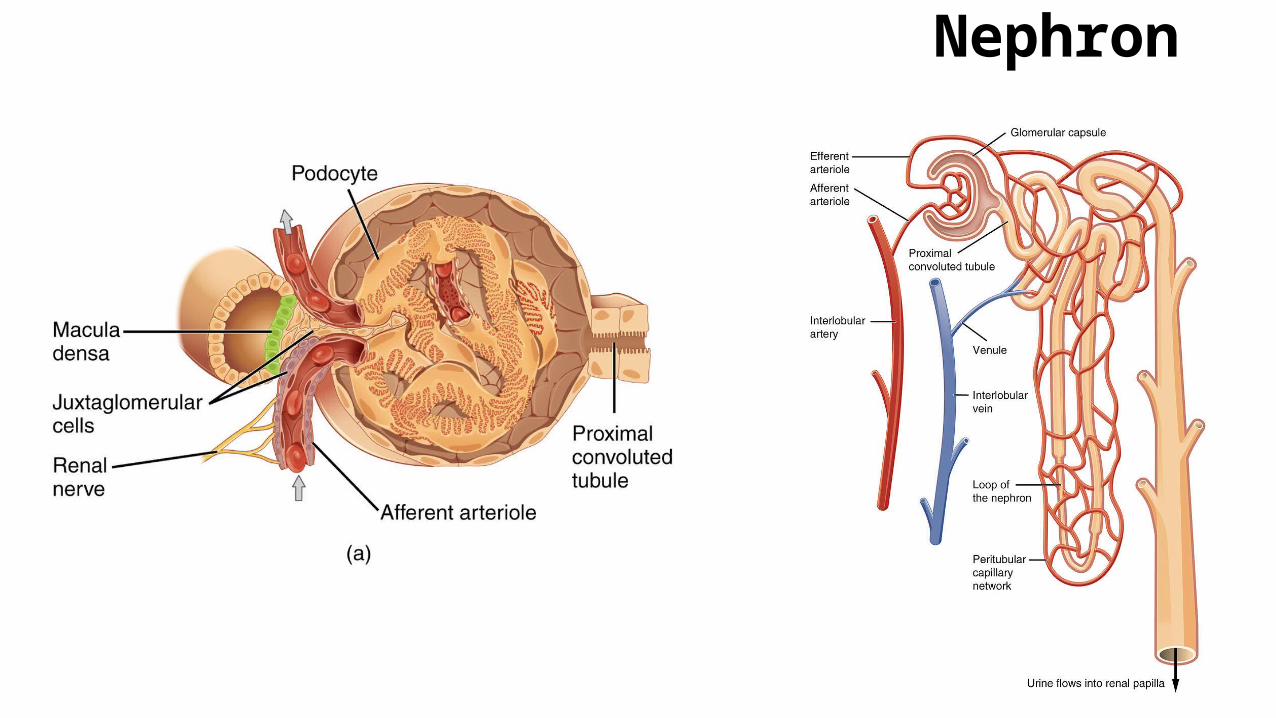
Nephron
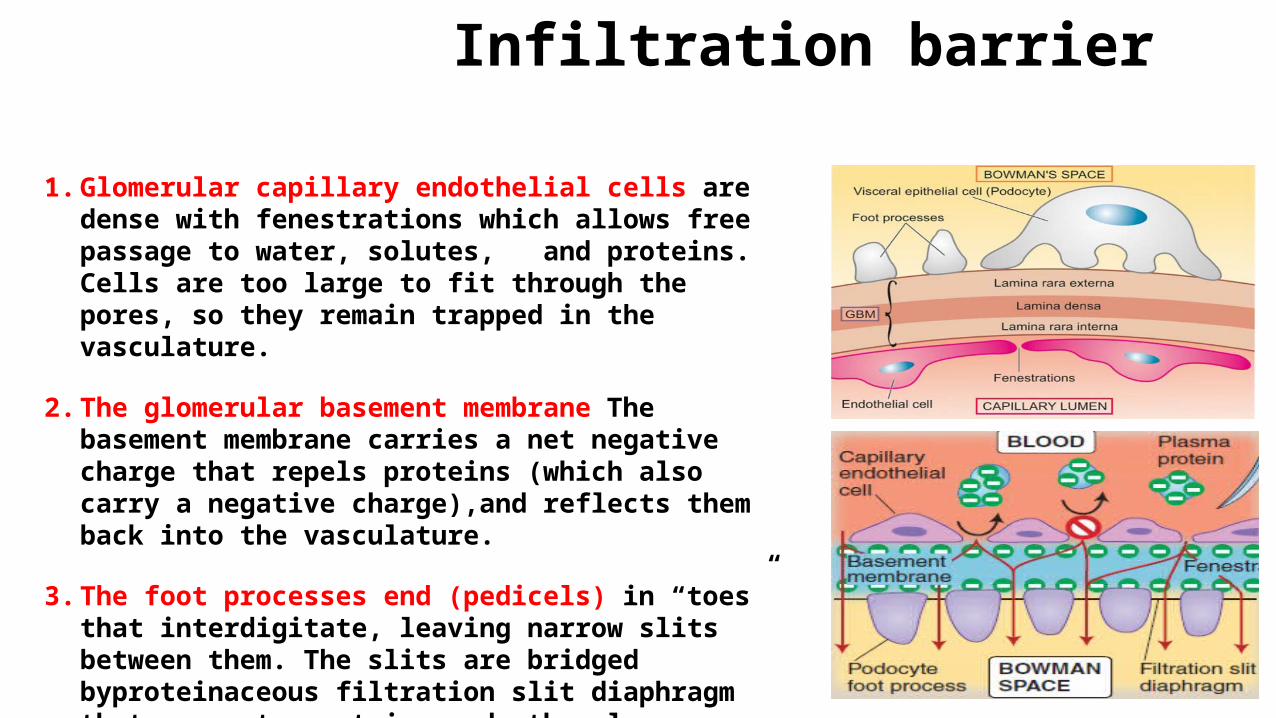
Infiltration barrier 1. Glomerular capillary endothelial cells are dense with
fenestrations which allows free passage to water, solutes, and proteins. Cells are too large to fit through the pores, so they remain trapped in the vasculature.
2. The glomerular basement membrane The basement membrane carries a net negative charge that repels proteins (which also carry a negative charge),and reflects them back into the vasculature.
3. The foot processes end (pedicels) in “toes” that interdigitate, leaving narrow slits between them. The slits are bridged byproteinaceous filtration slit diaphragm that prevents proteins and other large molecules from entering the Bowman space

Protein & urine • Moderate amounts of low molecular weight protein pass
through the healthy infiltration barrier .• Less than150 mg/day of protein normally appears in urine • Low molecular weight proteins may appear in the urine in
larger quantities than 150 mg/day, indicating failure of reabsorption by damaged tubular cells , i.e. ‘tubular proteinuria
• Proteinuria is usually asymptomatic , although large amounts may make urine froth easily.
• In investigation Quantification in a 24-hour urine collection (dipstick test) may be useful but this test is arduous , often inaccurate and influence by urine concentration .
• Greater consistency in results can be achieved by using first morning urine samples .
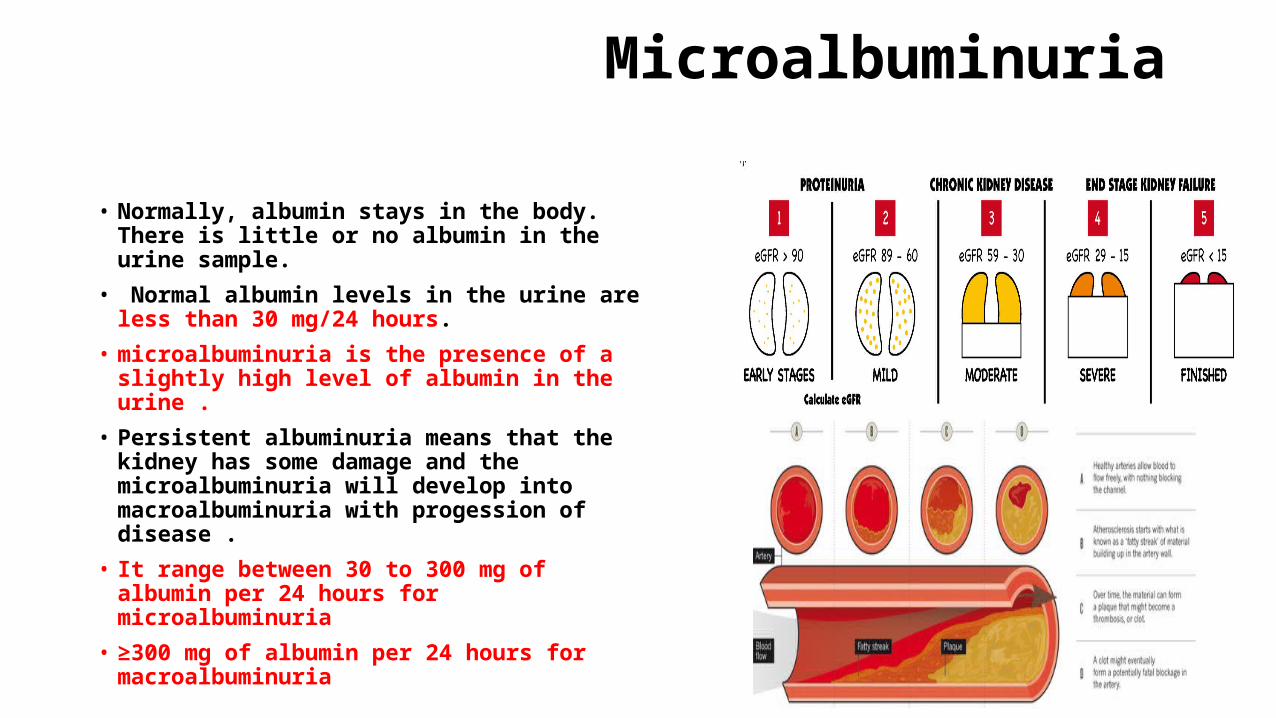
Microalbuminuria • Normally, albumin stays in the body. There is
little or no albumin in the urine sample.• Normal albumin levels in the urine are less
than 30 mg/24 hours.• microalbuminuria is the presence of a slightly
high level of albumin in the urine .• Persistent albuminuria means that the kidney
has some damage and the microalbuminuria will develop into macroalbuminuria with progession of disease .
• It range between 30 to 300 mg of albumin per 24 hours for microalbuminuria
• ≥300 mg of albumin per 24 hours for macroalbuminuria

Causes
• Renal disease • Diabetes mellitus • Cardiovascular disease • immune disease • Other factor such as strenuous exercise

Microalbuminuria
Atherosclerosis
DM
Such as Hypertention
Immune disease Cardiovascular disease
Hypersensitivity reaction(i.e type IV HSR )
Autoimmune disease (i.e after streptococcal infection )
Metabolic disorder such as hyperlipidemia
Renal disease (i.e. glomerular disease)

Atherosclerosis
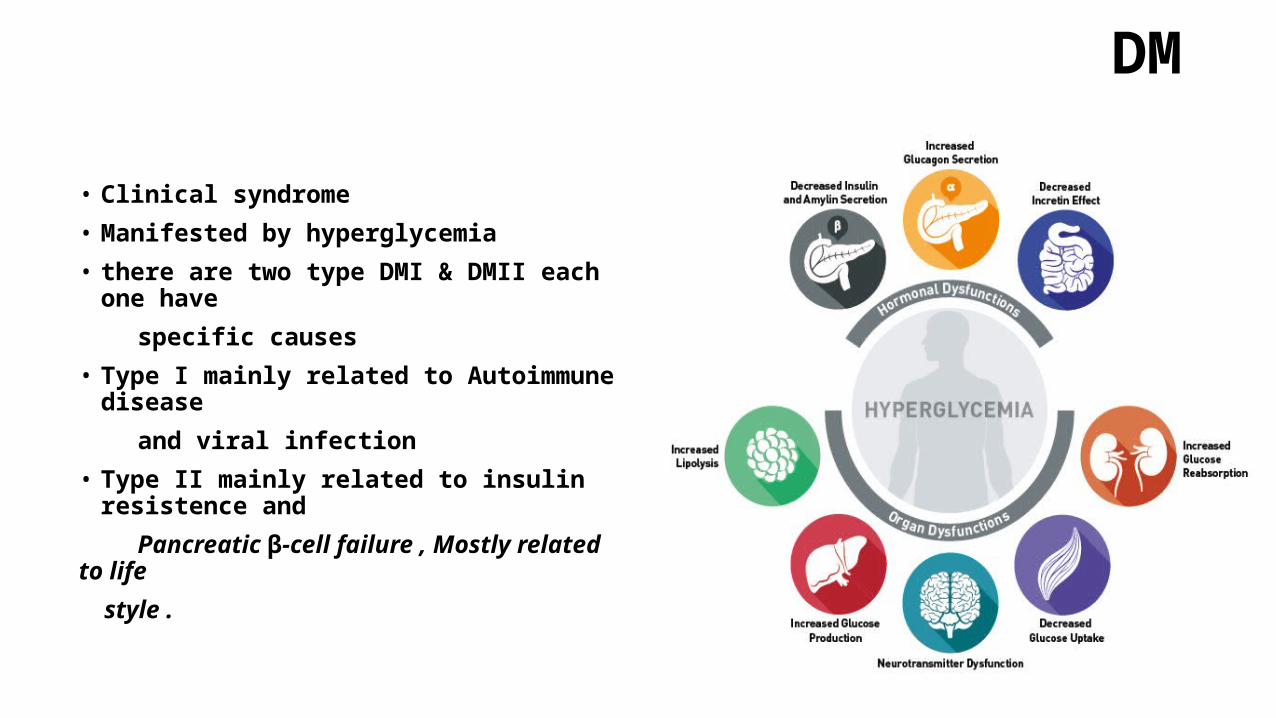
DM • Clinical syndrome• Manifested by hyperglycemia • there are two type DMI & DMII each one have specific causes • Type I mainly related to Autoimmune disease and viral infection • Type II mainly related to insulin resistence and Pancreatic β-cell failure , Mostly related to life style .

Hypertension • Hypertension results from excessive arteriolar
constriction and peripheral vascular resistance in relation to the blood volume and, when sustained, leads to hypertensive cardiovascular
• BP >140/90 mmHg • Genetic factors. • High salt intake. • Alcohol
excess. • Obesity. • Lack of exercise.• Impaired intrauterine growth.
• Benign & malignant hypertension • hyaline arteriolosclerosis. (benign) • hyperplastic arteriolosclerosis and fibrinoid
necrosis (malignant)

Pathogenesis • The kidney can regulate its own blood flow and GFR over a wide
range of perfusion pressures.• When the perfusion pressure falls—as in hypovolaemia, shock, heart
failure or narrowing of the renal arteries—the resistance vessels in the kidney dilate to facilitate flow. Vasodilator prostaglandins are important, and this mechanism is markedly impaired by NSAIDs
• If autoregulation of blood flow fails, the GFR can still be maintained by selective constriction of the post-glomerular (efferent) arteriole. This is mediated through the release of renin and generation of angiotensin II, which preferentially constricts this vessel.More severe or prolonged underperfusion of the kidneys may lead to failure of these compensatory mechanisms and hence an acute decline in GFR. This leads to the formation of a low volume of urine which is concentrated. These urinary changes may be absent in patients with pre-existing renal impairment or those who have received diuretics.

Symptoms • Changes in Urination • Swelling• Fatigue• Skin Rash/Itching• Metallic Taste in Mouth/Ammonia Breath• Nausea and Vomiting• Shortness of Breath• Feeling Cold• Dizziness and Trouble Concentrating• Leg/Flank Pain

Signs

Thank you





























