Embed Size (px)
Citation preview
COPD: Small Group Learning Session
Frank Egan, MD, CCFP GP Champion, Island Health, Regional Support Program, Island Health
Gurprit Randhawa, BSc, MSc, PhD(c) Coordinator, Regional Support Program, Island Health
SGLS

Outline
• Background • COPD SGLS
– Learning Objectives – Planning Team & Process – Format and Content – Evaluations – Lessons Learned
• Q&A

Dr. Frank Egan
• Full service FP, solo GP
• Working with PSP since inception
• Hospitalist
• Wellness work with Victoria Mental Health
• Interest in education and EMRs
• Fun Facts – Dad to two daughters
– Volunteer soccer coach
– Has a twin brother

Background
• Request from Island Health
– 2 Hour session on COPD for GPs
• Developed planning team and framework
• Learning objectives developed by team of two respirologists

COPD SGLS: Learning Objectives
As a result of attending this learning session, participants will be able to:
1. Define COPD.
2. Identify who is at risk and how to grade the severity of COPD.
3. Understand the impact of COPD exacerbation on the patient, for both patient and economic factors.
4. Understand evidence-based interventions to help lessen the frequency of COPD exacerbations

Planning Team
• Dr. Frank Egan – Family Physician and GP Champ for the COPD & HF Module
• Dr. John Reid – Respirologist Champion
• Mark Finnis, RRT – Respiratory Education Centre Coordinator, Island Health
• Jean-Marc Priest – Manager, Access & Transitions, Island Health
• Gurprit Randhawa – PSP Coordinator, Island Health

Planning Process
• Planning Meetings
– GP Champ & Coordinator
– Respirologist Champion & Coordinator
– Full Team
• Communication
– Phone
– Face-to-face
Format and Content
• COPD Quiz
• Clinical presentation with VIHA data
• Rapid fire questions
• COPD case studies
• RRT presentation on COPD Adherence and Compliance

Room Setup

Agenda
Time (pm) Activity/Presentation Speaker 2:05-2:10 Learning Session Objectives Val Stevens
2:10 – 2:20
COPD Quiz Dr. Frank Egan
2:20 – 3:00 Optimizing Management of Acute Exacerbations of COPD
Dr. John Reid
3:00 – 3:10 Break N/A
3:10 – 3:20 Rapid Fire Dr. Frank Egan
3:20 – 3:45 COPD Case Studies Dr. Frank Egan
3:45 – 4:00
COPD Adherence and Compliance of COPD
Mark Finnis
4:00 Evaluations and Session Close Gurprit K. Randhawa


1. What % of COPD patients have never smoked?
A. 5%
B. 11%
C. 17%
D. 25%
5%11%
17%25%
25% 25%25%25%

2. What % of COPD exacerbation patients died when admitted to RJH 2014/2015
A. 3.5%
B. 6.5%
C. 10.2%
D. 15%
3.50%
6.50%
10.20%
15%
25% 25%25%25%

Optimizing Management of Acute Exacerbations of COPD
John Reid, MD, FRCPC
Respirologist Champion

Consequences of AECOPD
AECOPD
Reduced health-
related quality of life Increased mortality
Accelerated
decline in lung
function
Increased health
resource utilization
and costs
O’Donnell DE, et al. Can Resp J 2008; 15:1A-8A.

VIHA Data - 2014/15
•Royal Jubilee Hospital –430 discharges
–Total LOS 3,198 days
–Average LOS 7.4 days
•VGH –216 discharges
–Total LOS 1,792 days
–Average LOS of 7 days

Summary •COPD
–Common
– Is diagnosed with spirometry
–Effective pharmacologic AND non-pharmacologic treatment
–A frequent cause of health care utilization
–Associated with poor quality of life and high mortality
•AECOPD – Is defined clinically
– Is associated with disease progression
–Can be prevented / minimized
–Can be treated , BUT…
–Requires resources AND a coordinated effort across the health care spectrum
17

Break
18

20 questions …10 seconds to answer

1. Last book you read and rate of out 10?
20

2. Your favorite Inhaled medicine for COPD?
21

3. Your favorite inhaler device?

4. Your usual go-to antibiotic for acute exacerbation of COPD?

5. Your usual dose of prednisone for the average sized COPD patient?

COPD Case Studies
Facilitators: Dr. Egan, Dr. Reid, Mark

Split into 3 Groups
› Select 1 Spokesperson per group
› Go through case study and answer
questions (10 minutes)
3 minute report out per group
Instructions

Case 1: Mary
• Mary age 81yrs • Copd stage 4 fev1 is 25% FEV1/FEC is 0.51 • Two hospitalisations for exacerbation of COPD in the
past 6 months last admission was 1 week ago..on oxygen, advair discus 500mcg bid spireva 18mcg, ventolin puffer 100mcg 2 QID PRN po avelox 400mg
• Also has hypertension, type two diabetes 20 years on metformin and glicazide..
• Labs: GFR is 45, hb is 150g/l O2 sats on oxygen is 88% at rest… she is unable to walk more than 30 feet without SOB
• Lives in apartment with husband aged 87 yrs
with severe arthritis and cad he is limited in
his ability to help her..
• Questions to Address:
1. What is her prognosis? How do you prevent
another admission to acute care?
2. When is it appropriate to arrange palliative care?
3. How do you go about this?
4. How will this change your approach and her
management?

COPD: An educators’ journey…*
Or
“Why the h*@# don’t people use their inhalers?!!”
Or
“Compliance/Adherence on discharge from hospital: What’s the difference and does it
really matter?”
Mark Finnis, RRT, CRE
Respiratory Education Centre (REC) Coordinator
Island Health

Pitfalls on discharge from hospital…
Research has shown that people are more adherent to treatment (both pharmacological and non pharmacological) if certain conditions are met:
• Patients need practical skills…education alone does not save people.
• Partnerships with family physicians, patients and…pharmacists/respiratory educators/dietitians produce the “best results”.
• Behaviour change must occur for self management to be successful.

Education or self management “pitfalls”…
We’ll ignore the fact that for many patients an admission for an AECOPD is their introduction to the fact that they have COPD!
• Patients need to know what got them there, so they can reduce their chance for readmission.
• Most people wait too long to seek help - many because they really don’t know the warning signs of an AECOPD.
• We need a COPD Meter!! The patient is the measuring instrument, but they need to know what to “measure”.
• CTS/ATS/ERS all recommend COPD Action Plans but what should they look like and what should they “tell” patients to do?

Participants
• Attendance
– Morning Session (8-10 am): 21 GPs
– Afternoon Session (2-4 pm): 21 GPs

Session Evaluations By Learning Objective
29%
29%
54%
39%
58%
54%
46%
52%
13%
17%
0%
0%
0%
0%
0% 20% 40% 60% 80% 100%
Ability to Define COPD.
Identify who is at risk and how to gradethe severity of COPD.
Understand the impact of COPDexacerbation on the patient, for both
patient and economic factors.
Understand evidence-basedinterventions to help lessen the
frequency of COPD exacerbations.
SignificantlyIncreased
Increased
No Change
Decreased
SignificantlyDecreased
N/A
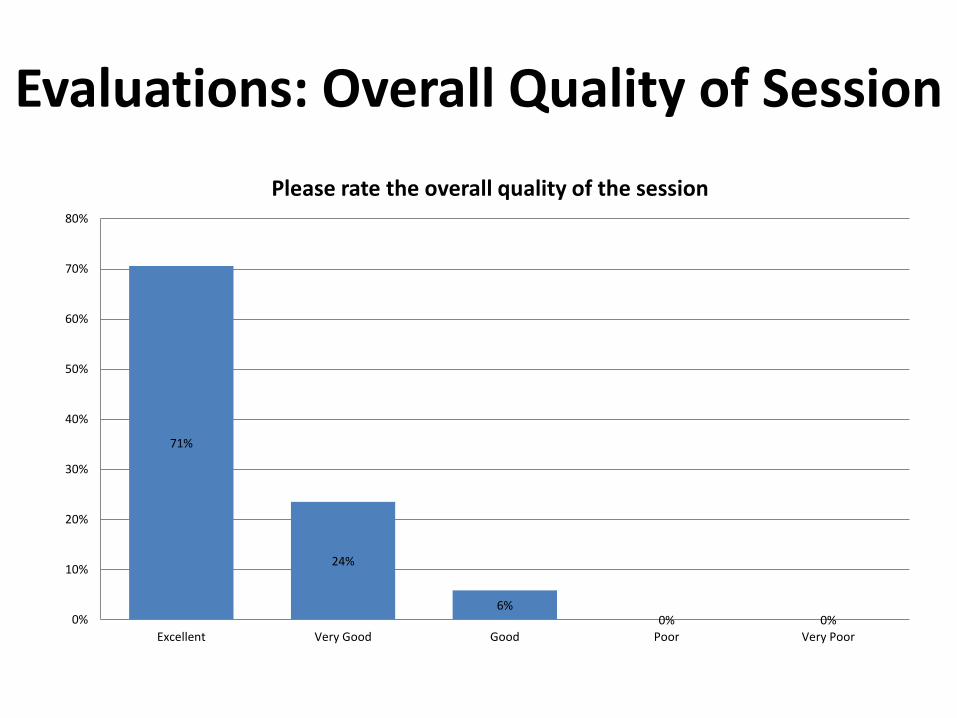
Evaluations: Overall Quality of Session
71%
24%
6% 0% 0% 0%
10%
20%
30%
40%
50%
60%
70%
80%
Excellent Very Good Good Poor Very Poor
Please rate the overall quality of the session

Evaluation: Open-ended Feedback • Format
– Format was superb. Rapid Fire, Didactive, care, physical props…it was all good together.
– Very relevant-we need more of this! Good as 2 hour session. Thanks!
– SGLS was excellent. I appreciate the formatDo more of these! "Prizes" + clickers was super fun.
• Relevance/Usefulness – Follow-up session would be wonderful. Learned so much-
incredible. Lots of great tips for me to put into practice in my office. Inspiring.
– Yes the [follow-up] session will be useful!!! – Very useful-thanks! Practical-will help me improve my
practice with patients. – This was really helpful.
Follow-Up Session
• In Spring 2016, a follow up COPD learning session will also be offered (date TBD) to discuss the impact of the first SGLS in practice
• Model successes of first session • New material to cover:
– Medications (new treatments and remedies) – COPD Action Plan – Inhaler demo – Four more cases – Smoking Cessation – Panel Discussion – Resource/Speaker Cafe

Takeaways: Lessons Learned
• Include variety
• Having 3 engaged and passionate speakers
• Making the entire SGLS interactive
• Benefits of SGLS
– Shorter (easier to accommodate in GP schedule)
– Smaller group size (more effective learning)

QUESTIONS?





























