Embed Size (px)
DESCRIPTION
Citation preview

Martin B. Leon, MD
on behalf of the
PARTNER Investigators
TCT 2010; Washington, DC; September 23, 2010
Transcatheter Aortic Valve Implantation in Inoperable Patients
with Severe Aortic Stenosis
Press Conference

Symptomatic Severe Aortic StenosisSymptomatic Severe Aortic Stenosis
ASSESSMENT: High Risk AVR Candidate3105 Total Patients Screened
ASSESSMENT: High Risk AVR Candidate3105 Total Patients Screened
PARTNER Study Design
High Risk TAHigh Risk TA
ASSESSMENT: Transfemoral
Access
ASSESSMENT: Transfemoral
Access
TAVITrans
femoral
TAVITrans
femoral
Surgical AVR
Surgical AVR
High Risk TFHigh Risk TF
Primary Endpoint: All Cause Mortality (1 yr)(Non-inferiority)
Primary Endpoint: All Cause Mortality (1 yr)(Non-inferiority)
TAVITrans
femoral
TAVITrans
femoral
Surgical AVR
Surgical AVR
1:1 Randomization1:1 Randomization1:1 Randomization1:1 Randomization
VS
VS
Standard Therapy
(usually BAV)
Standard Therapy
(usually BAV)
ASSESSMENT: Transfemoral
Access
ASSESSMENT: Transfemoral
Access
Not In StudyNot In Study
TAVITrans
femoral
TAVITrans
femoral
Primary Endpoint: All Cause Mortality over length of trial (Superiority)
Primary Endpoint: All Cause Mortality over length of trial (Superiority)
1:1 Randomization1:1 Randomization
VS
Total = 1058 patientsTotal = 1058 patients
2 Parallel Trials: Individually Powered
2 Parallel Trials: Individually Powered
High Riskn= 700n= 700 Inoperable n=358n=358

Primary and Co-Primary Endpoints
• PRIMARY: All-cause mortality over the duration of the study
Superiority test (two-sided), 85% power to detect a difference, α = 0.05, sample size = 350 total patients
• CO-PRIMARY: Hierarchical composite of all-cause mortality and repeat hospitalization Non-parametric method described by Finkelstein and
Schoenfeld (multiple pair-wise comparisons) > 95% power to detect a difference, α = 0.05
• Positive study if both endpoints P < 0.05, or if either endpoint is < 0.025

Study Devices
Retroflex 1Edwards-SAPIEN THV
23mm and 26mmvalve sizes
22F and 24Fsheath sizes

Inclusion Criteria
• Severe calcific aortic stenosis defined as echo derived valve area of < 0.8 cm2 (EOA index <0.5cm2), and mean gradient > 40 mmHg or jet velocity > 4.0 m/s
• NYHA functional class II or greater• Risk of death or serious irreversible
morbidity as assessed by cardiologist and two surgeons must exceed 50%

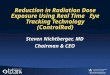
All Cause Mortality
Numbers at Risk
TAVI 179 138 122 67 26 Standard Rx 179 121 83 41 12
All
-cau
se m
ort
alit
y (%
)
Months
HR [95% CI] =0.54 [0.38, 0.78]
P (log rank) < 0.0001
Standard Rx
TAVI

All Cause Mortality
Numbers at Risk
TAVI 179 138 122 67 26 Standard Rx 179 121 83 41 12
Standard Rx
TAVI
All
-cau
se m
ort
alit
y (%
)
Months
∆ at 1 yr = 20.0%NNT = 5.0 pts
50.7%
30.7%

• Compare, at random, every TAVI patient with every Standard Rx patient; 179 x 179 (32,041) patient pairs, which did better?
• #1, compare “time to death” 72% chance that we know who died first If so, 63% chance that Standard Rx patient died first and
37% chance that TAVI patient died first
• #2, if necessary, compare “time to repeat hospitalization” 17% chance that we know who had repeat hosp first If so, 75% chance that Standard Rx patient had repeat
hosp first and 25% chance that TAVI patient had repeat hosp first
Finklestein & Schoenfeld Analysis(hierarchical multiple pair-wise comparison)
FS MethodProduces a
P-value< 0.0001

Outcome 30 Days n=179
TAVI Standard Rx P-value
1 Year n=179
TAVI Standard Rx P-value
Clinical Outcomes at 30 Days & 1 Year
Myocardial infarction
All (%) 0 0 . 0.6 0.6 1.00 Peri-procedural (% 0 0 . 0 0 .
Stroke or TIA
All (%) 6.7 1.7 0.03 10.6 4.5 0.04 TIA (%) 0 0 . 0.6 0 1.00
Minor stroke (%) 1.7 0.6 0.62 2.2 0.6 0.37
Major stroke (%) 5.0 1.1 0.06 7.8 3.9 0.18
Death (all) or major stroke (%) 8.4 3.9 0.12 33.0 50.3 0.001
Repeat hospitalization (%) 5.6 10.1 0.17 22.3 44.1 <.0001
Death (all) or repeat hosp (%) 10.6 12.3 0.74 42.5 70.4 <.0001
Death
All (%) 5.0 2.8 0.41 30.7 49.7 0.0004
Cardiovascular (%) 4.5 1.7 0.22 19.6 41.9 <.0001

Outcome 30 Days n=179
TAVI Standard Rx P-value
1 Year n=179
TAVI Standard Rx P-value
Clinical Outcomes at 30 Days & 1 Year
Acute kidney injury Creatinine >3 mg/dL (%) 0 1 1.00 1.1 2.8 0.45 RRT (%) 1.1 1.7 1.00 1.7 3.4 0.50
Cardiac re-intervention
BAV (%) 0.6 1.1 1.0 0.6 36.9 <.0001
Re-TAVI (%) 1.7 na 1.7 na
AVR (%) 0 1.7 0.25 1.1 9.5 <.0001
Endocarditis (%) 0 0 . 1.1 0.6 0.31
Vascular complications
All (%) 30.7 5.0 <.0001 32.4 7.3 <.0001
Major (%) 16.2 1.1 <.0001 16.8 2.2 <.0001
Bleeding - major (%) 16.8 3.9 <.0001 22.3 11.2 0.007
Arrhythmias
New atrial fibrillation (%) 0.6 1.1 1.00 0.6 1.7 0.62
New pacemaker (%) 3.4 5.0 0.60 4.5 7.8 0.27

TAVI Standard Rx0
20
40
60
80
100
120
140
160
73
55
100
65
120
84
Walking Distance
P = 0.002
Wal
king
dis
tanc
e (m
eter
s)
Baseline 30 Days
Six-Minute Walk Tests
P = 0.004
1 Year
P = 0.67
P = 0.55

NYHA Class Over TimeSurvivors
P = 0.68 P < 0.0001 P < 0.0001 P < 0.0001
I II III IV
TAVI Standard Rx TAVI Standard Rx TAVI Standard Rx TAVI Standard Rx
Per
cen
t
TreatmentVisit
Baseline 30 Day 6 Month 1 Year

BaselineN=163
30 DayN=143
6 MonthsN=100
1 YearN=89
Mea
n G
rad
ien
t (m
m H
g)
50
40
30
20
60
70
10
0
Error bars = ± 1 Std Dev
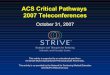
Mean Gradients Over Time
P < 0.0001
33.0
39.5
44.4
43.2 12.111.310.8
44.6
Standard Rx
TAVI

Paravalvular Regurgitation: TAVI
No changes over time
None/Trace
Mild
Moderate
Severe
30 Day 6 Month 1 Year

Conclusions - 1
In patients with severe AS and symptoms, who are not suitable candidates for surgery…
• Standard therapy (including BAV in 83.8% of pts) did not alter the dismal natural history of AS; all-cause and cardiovascular mortality at 1 year was 50.7% and 44.6% respectively
• Transfemoral balloon-expandable TAVI, despite limited operator experience and an early version of the system, was associated with acceptable 30-day survival (5% after randomization in the intention-to-treat population)

Conclusions - 2
• TAVI was superior to standard therapy, markedly reducing the rate of… all-cause mortality by 46%, P < 0.0001,
NNT = 5.0 pts cardiovascular mortality by 61%, P < 0.0001,
NNT = 4.1 pts all-cause mortality and repeat hospitalization
hierarchical (FS method), P < 0.0001 non-hierarchical (KM analysis) by 54%,
P < 0.0001, NNT = 3.4 pts

Conclusions - 3
• TAVI improved cardiac symptoms (NYHA class, P < 0.0001) and six minute walking distance (P = 0.002), after 1-year follow-up
• TAVI resulted in more frequent complications at 30 days, including… major vascular complications, 16.2% vs.
1.1%, P < 0.0001 major bleeding episodes, 16.8% vs. 3.9%,
P < 0.0001 major strokes, 5.0% vs. 1.1%, P = 0.06

Conclusions - 4
• Serial echocardiograms in TAVI patients indicated… reduced mean gradients (P < 0.0001) which
were unchanged during 1-year FU frequent paravalvular AR, which was usually
trace or mild (~90%), remained stable during 1-year FU, and rarely required further Rx.

Clinical Implications
• Balloon-expandable TAVI should be the new standard of care for patients with aortic stenosis who are not suitable candidates for surgery!
• Next generation devices (e.g. SAPIEN XT) may help to reduce the frequency of procedure-related complications in the future.
• The ultimate value of TAVI will depend on careful assessment of bioprosthetic valve durability, which will mandate obligatory long-term clinical and echocardiography FU of all TAVI patients.

September 22, 2010 on NEJM.org