Embed Size (px)
Citation preview
Management of Arthritis:Recent Trends
Dr. Neeraj Aggarwal MS, FJRS(Mumbai, Germany)
Consultant Orthopaedic & Joint Replacement surgeonConsultant Orthopaedic & Joint Replacement surgeonNarayana Hrudayalaya Hospital
Pratap Nagar, Jaipur.

Objectives of today’s discussion
• Discuss the prevalence of degenerative Knee Osteoarthritis (OA)
• Understand and discuss different approaches to treat Knee OA
• Discuss the Indications, Priority and Clinical outcomes of Knee Replacement

• The knee joint is protected in front by the patella
• Meniscus - acts as a shock absorber
• Articular cartilage allows the surfaces of the knee to glide over each other without damaging the surface
Anatomy of Knee


Prevalence of Knee Pain
(Croft et al, 1998)
7,500• Knee pain, some disability & X-ray OA
12,500• Knee pain with some disability
25,000• 4 weeks of knee pain in past year
• Knee pain, severe disability & X-ray OA 2,000
100,000• Subjects aged 55 years+
2%

• About 7 crore Indians are suffering from knee related problems
• Evidence suggests that women have a higher incidence of OA than men, and overall have an incidence of 2.95 per 1000 population, compared with 1.71 per 1000 population in men
Prevalence of Knee OA

Why is this problem more prevalent in India
• Squatting / Ground sitting habits• Climbing stairs• Indian Toilets• Obesity• Complicated patients• Heredity
Can we prevent Osteoarthritis
Symptoms
• Pain in and around the Knee joint• Morning Stiffness (worse on standing &
attempting to walk)• Swelling of Joint• Occasional night pain
Characteristics of Knee OA
The symptoms of OA may interfere with normal activities, such as walking, dressing and sleep

Characteristics of Knee OA
Signs
• Crepitus on motion • Buckling or instability• Tenderness on pressure • Joint effusion • Malalignment / Joint deformity

Treatment Approaches
• Education
• Behavioural and Environmental changes
• Physical and Mechanical Interventions
• Pharmacological Management
• Surgical Interventions

Practical Approach to Knee OA patient
• Patient A• 45 year, Female, Home maker• Knee pain 1 month• Mild to Moderate• Rarely Analgesics• NO Night pain• Knee ROM full• No Crepitus
Always ask for weight bearing films

Education
• Education of Patients – helps in reducing impact of condition on their
day-to-day lives
• Advice about lifestyle • Impact vs. Non impact activities

WEIGHTWEIGHT

Physical and Mechanical Interventions
• Heat and Cold applications– to reduce inflammation
• Walking aids– reduce the loading on the knee while walking
• Shoe alterations– help the patient get their footwear right
– Knee braces

PRECAUTIONSPRECAUTIONS
• Take rest in between if it is needed
• No squatting on floor
• No cross legged sitting (Alathi – Palathi) on floor
• Reduce climbing stairs
• Cycling is good
• Swimming Mother of all exercises

• Patient B• 54 year, Female, Part
time job• Knee pain 1 year• Mild to moderate,
occasionally severe• Analgesics 2-3 times a
week• Knee swelling• Knee terminally painful• Anterior Knee pain

Pharmacological Management
• Systemic
Paracetamol, NSAIDs
Cox-2 Inhibitors
• Topical
• Intra-articular
Steroids
Hyaluronic Acid

My analgesic of choice…
• Paracetamol+Low dose Tramadol
• Synergistic combination
• Block both pathways
• Dose titration (2-8 tab a day)
• GI safety

D.M.A.R.D.Do we have
D.M.A.OAOA.D.
? ? ?? ? ?
D.M.A.OAOA.D. ? ? ? Texanamic acid – Anti plasmin activator
CMT – Chemically Modified Tetracyclin– Inhibit MMP, Nitric oxygenase formation, prevent cartilage wear in animals
Poly sulfated Glucosamino-glycan.– GOOD animal studies. Limited experiencd in human beings.– Fear of “mad cow disease “, anaphylaxis
Diacerin– Again efficacy not established
Glucosamine– In selected cases
NONE like DMARD yet !NONE like DMARD yet !

Physiotherapy
• Physiotherapy aims to restore function to the maximum degree possible – through exercises– helps reduce pain– increases joint range of movement– improves muscles strength– addresses specific restrictions in activities
• Exercises:
- Static Quadriceps Exercises - Quadriceps Building Exercises - Hamstring Building Exercises - Isokinetic Exercises for knee joint - Progressive resistance Exercises

Intra-articular
Steroids
• Indicated when knee is inflamed
• Confirm intra-articular placement by draining effusion, then injection
• Wide variation in responses

Viscosupplementation
• Replaces pathologic synovial fluid
• Supplements elasticity and viscosity
• Reduces pain and improves mobility

• Patient C
• 65 Years, Female, Retired
• Knee pain 7 years, severe pain, Night pain
• Analgesics daily• Knee Crepitus
• Limp and deformity
• Has taken conservative treatment : no benefit

How do we know that the patient needs surgery ?
• Regular pain needing medication
• Deformity of the knee, crepitus in knee
• Night pain, getting up pain
• Altered social or family life due to pain

OSTEO ARTHRITIS
INDICATION – PENALTY POINTS ( 75 PLUS)
Progression + Disability
Pain Deformity ROM Instability 40 20 20
REPLACEMENT SURGERY
20

• FIVE LAKH IS THE NUMBER OF KNEE REPLACEMENT SURGRIES DONE IN USA IN 2008
• IN INDIA THE CORRESPONDING NUMBER IS 35000 IN 2008
• WITH ALL OUR MANFORCE WE ARE ABLE TO TACKLE ONLY 3% OF TOTAL ARTHRITIS PATIENTS
• WHERE ARE WE ???????

Normal kneeNormal knee Arthritic Knee

Total Knee Replacement
• The ultimate solution for OA of knee is to replace the worn-out parts of the knee with an artificial joint
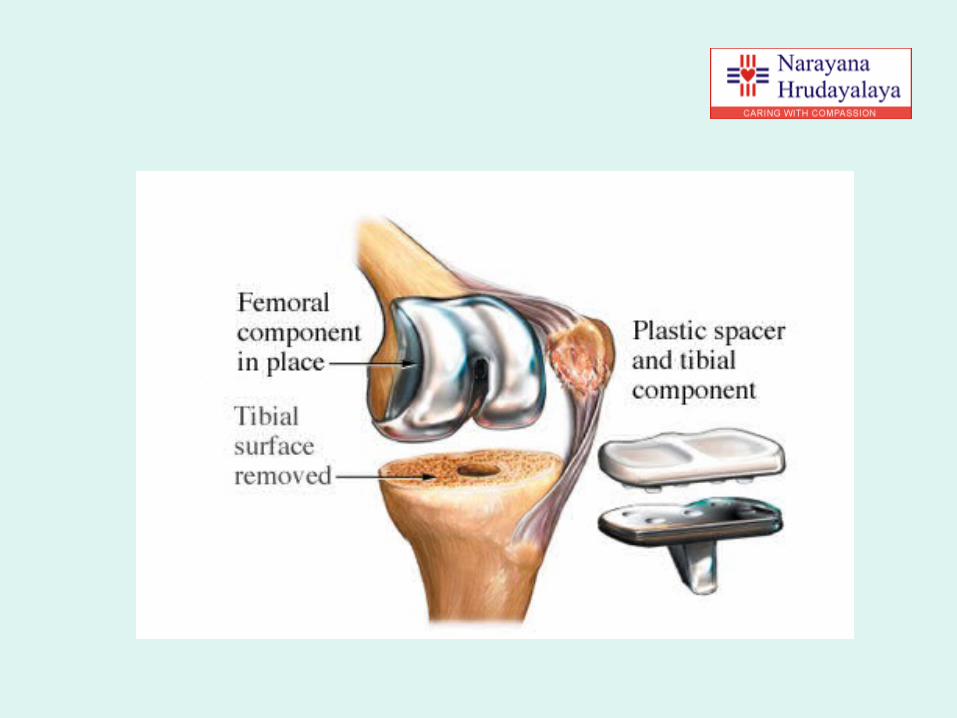
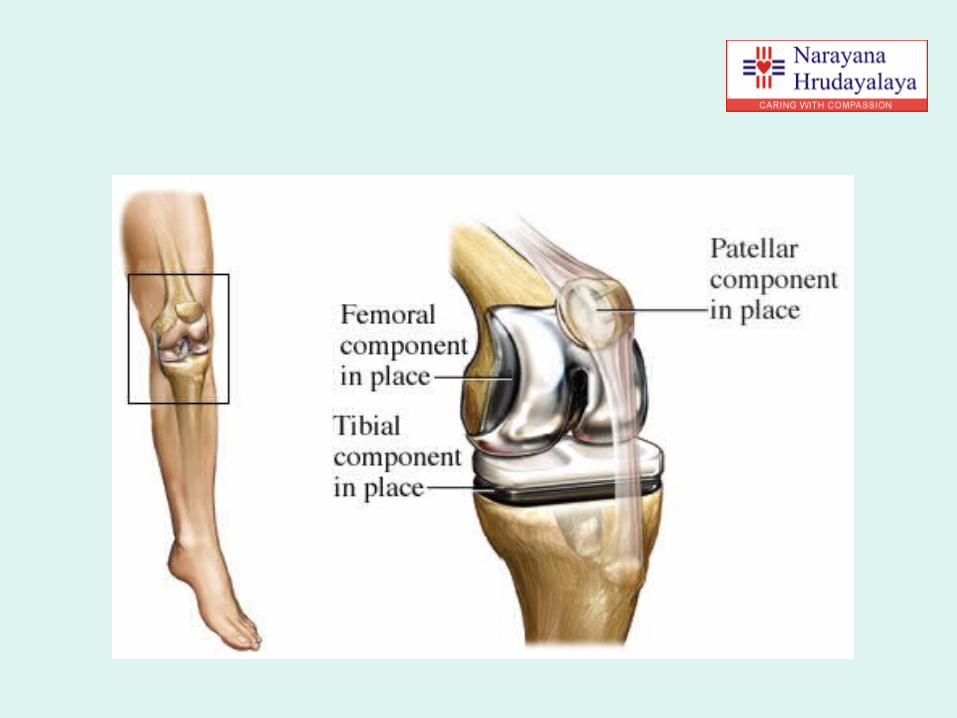
• The prosthesis that is used is made up of plastic and metal and is placed on the joint surface of each bone
• This surgery has been widely used for many years with excellent results especially for knees
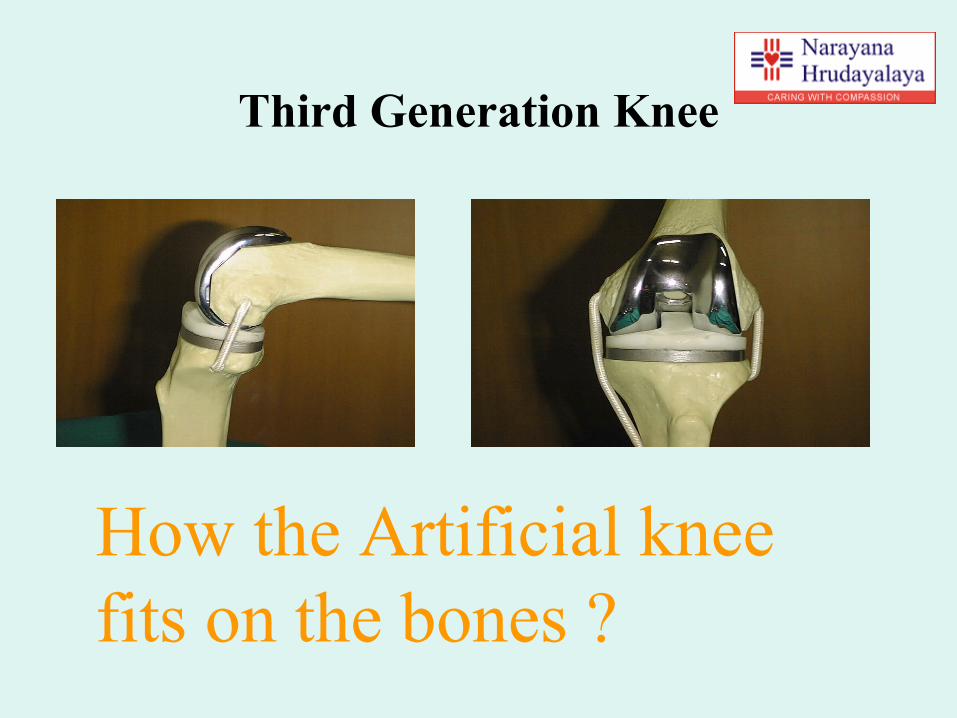
Third Generation Knee
How the Artificial knee fits on the bones ?




Where to undergo Surgery…

Post-Op TKR
AP Lateral

Common Post-Operative (TKR) Course
• Day 1 Standing, bending and sitting out in a chairMay take a few steps with help
• Day 2 Walking (with aids)
• Day 4/5 Stair climbing
• Day 5-7 Home (with 2 walking sticks)
• Week 6 Walking unaided (or 1 stick) Driving
• Week 10-12 Full recovery

Benefits of TKR
• TKR can relieve pain that doesn't respond to other
treatment options
• Pain reduction in 90 to 95% of the patients
• Reduced stiffness and improved joint movement
• Increased walking ability
• Improved alignment of deformed joints

Myths
• Hip replacement works but knee replacement doesn’t
• Knee replacements are still experimental
• Knee replacements only last 8-10 years may be 15 years maximum
• I am too fat - my implants might break

• TKR surgery is too costly
• TKR is not successful
• After TKR, I have to be bedridden for 3 months
• A total knee replacement implies that everything about the joint is being replaced
Myths
Question about ?
• Team
• Availability
• Approachability
• Economy: we offer cost effective packages for joint replacement surgery

Summary
• Knee OA, which has not responded to conservative treatment can be effectively treated by various surgical interventions
• Effective grading of patients, counceling and management serves as a tool to combat osteoarthritis
• Knee replacement surgery is a highly successful (90-95%) and safe procedure
• Prioritising and effective screening by GPs and Physicians who can identify those individuals that are likely to benefit from TKR

Future ………
• Robotics with navigation
• Custom Implants and Instruments
• Stem cell therapy
A p p r e c i a t e y o u r A p p r e c i a t e y o u r a t t e n t i o na t t e n t i o n





























