Embed Size (px)
Citation preview

Pharmacotherapy of IBD
15/03/12
Definition• Chronic, idiopathic, inflammatory intestinal
conditions
• 2 major subtypes:
1) Ulcerative colitis
2) Crohn’s disease
• 2 minor subtypes
1) IBDU
2) Indeterminate colitis

Montreal classification of IBD
• Ulcerative colitis
1. Ulcerative proctitis
2. Left sided UC (distal UC)
3. Extensive UC (pancolitis)
• Crohn’s Disease (acc. to location)
1. Ileal
2. Colonic
3. Ileocolonic
4. Isolated upper GI disease
Etiology
• IBD is currently considered an inappropriate immune response to the endogenous commensal microbiota within the intestines
• Factors involved are:
Defective immune regulation
Genetic mutations
Exogenous factors
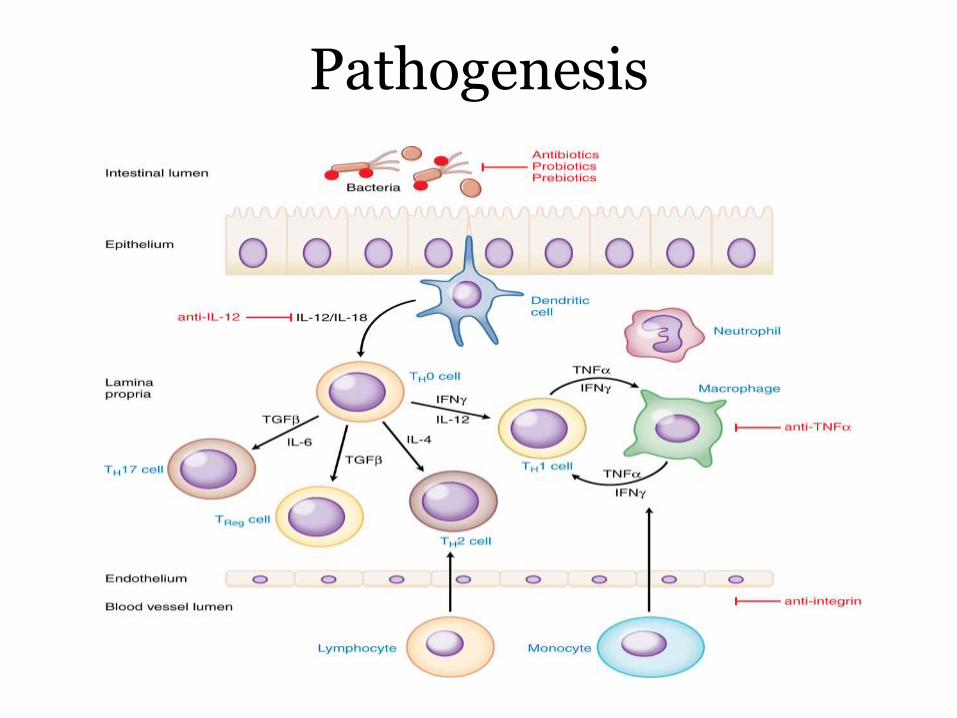
Pathogenesis

Genetics
•About 100 genetic loci have been identified
e.g. NOD2 and CCR6
•Many of these muatations are shared between UC and CD
e.g. JAK2 & IL-23R
•Many loci are also associated with risk of other diseases like rheumatiod arthritis and psoriasis
Exogenous factors
IBD may be triggered by microbes like Bacteriodes, Clostridium difficile & E.coli
• This is proved by presence of antibodies against them e.g. Presence of E.coliOMP2 antibodies & ASCA
Body may also react against normal flora
• This is supported by improvement in symptoms by antibiotics
Psychosocial factors(major life events, daily stress)Cause worsening of symptoms

Clinical features
Ulcerative colitis
Cardinal symptom is bloody diarrhoea
With colicky abdominal pain, urgency or tenesmus
50% patients experience relapse at least once
Crohn’s disease
Abdominal pain, diarrhoea and weight loss
Systemic symptoms- malaise, fever, anorexia- more common
70-80% of patients require surgery during their lifetime

Feature Ulcerative colitis Crohn’s disease
Involvement of GIT Large bowel Any part of GIT
Rectal involvement Frequent Rare
Inflammation Superficial Transmural
Skip areas Absent Present
UlcersIf present-Superficial
Deep, serpiginous
Fissures & Fistulae Less comon Very common
HistologyInfiltration is mainly
neutrophilic
Presence of granulomas
diagnostic; infiltration mainly lymphocytic
Smoking ProtectivePredicts a worse
course
Aims of Treatment
Induce remission
Maintain remission
Prevent complications
Maintain nutritional status
Improve quality of life
Drugs used in treatment
1. 5-ASA based therapy
2. Glucocorticoids
3. Immunosupressants
4. Anti- TNFα therapy
5. Antibiotics

5-Amino Salicylic Acid (Meselamine) based therapy
• First-line therapy for mild to moderate UC and Crohn’s colitis
• Effective in inducing remission in both UC and CD
• Effective in maintenance of remission in UC
Mechanism of action
• Not related to COX inhibition
• Its various mechanisms are :
1. Inhibiting IL-1 and TNF-α production
2. Inhibiting Lipo-oxygenase pathway
3. Scavenging of free radicals
4. Inhibiting of NF-κB via PPAR-γ
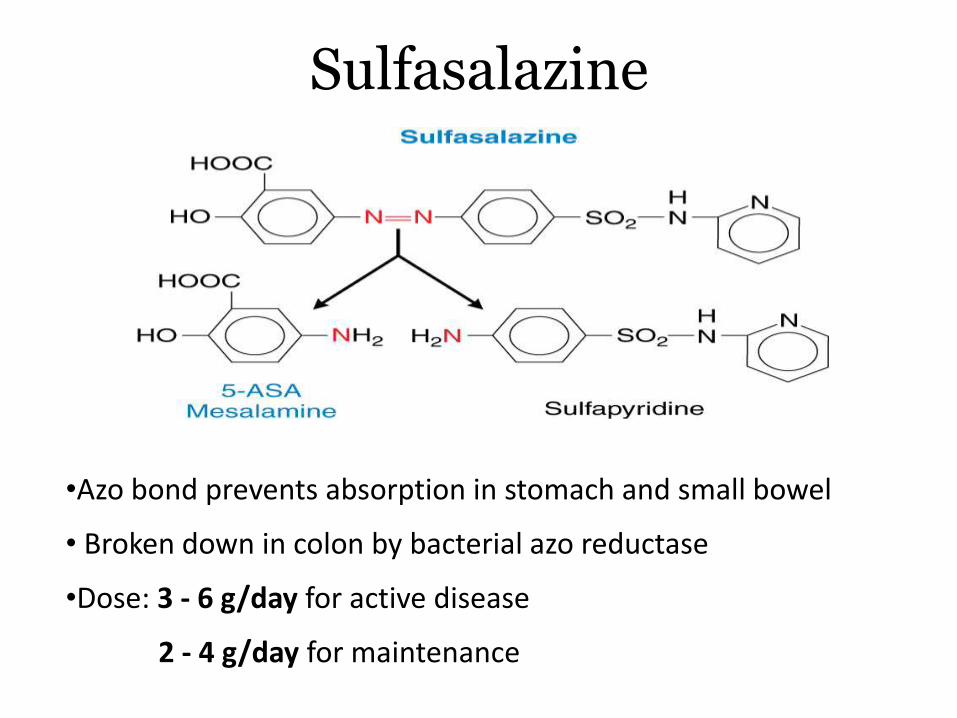
Sulfasalazine
•Azo bond prevents absorption in stomach and small bowel
• Broken down in colon by bacterial azo reductase
•Dose: 3 - 6 g/day for active disease
2 - 4 g/day for maintenance

Pharmacokinetics• 20 to 30% absorbed in the small intestine, which is excreted
unchanged
• 70% reaches the colon
• Splits to release 5-ASA and sulfapyridine
• Generates 400 mg meselamine for every gram of parent compound
• The sulfapyridine moiety is highly lipid soluble
• It is completely absorbed and undergoes acetylation & glutathione conjugation
Adverse effects
• Primarily due to sulfapyridine
Dose related: Headache, fatigue, nausea
Allergic reactions: Rash, Steven-Johnson syndrome, hepatitis, bone marrow suppression
Decrease in sperm number and motility: reversible
Nephrotoxicity: Risk of interstitial nephritis, hence renal function should be monitored
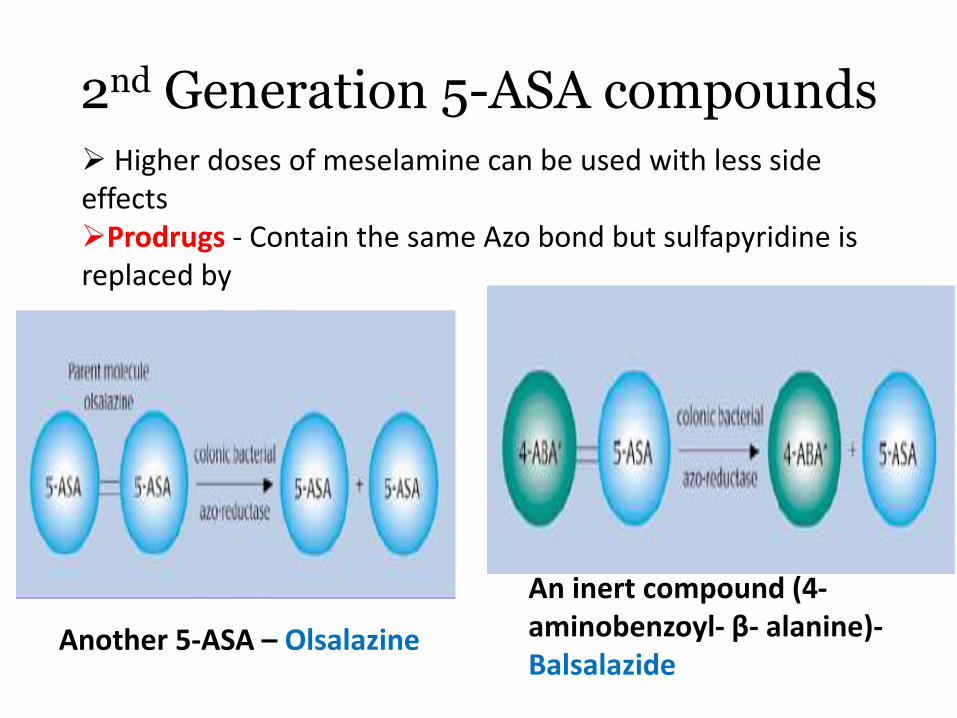
2nd Generation 5-ASA compounds Higher doses of meselamine can be used with less side effectsProdrugs - Contain the same Azo bond but sulfapyridine is replaced by
Another 5-ASA – Olsalazine
An inert compound (4-aminobenzoyl- β- alanine)-Balsalazide
Asacol : Enteric-coated form of meselamine
• 5-ASA is liberated at pH > 7
• Site of release: Terminal ileum and colon
• Dose: 2.4–4.8 g/ day (acute)1.6–4.8 g/ day (maintenance)
• Lialda: MMX (Multi-matrix) Technology
• Encloses 5-ASA inside a lipophilic matrix within a hydrophilic matrix
• It is further encapsulated by a pH-sensitive polymer which releases drug at pH > 7
• Dose: 2.4–4.8 g/ day
Coated drugs

Pentasa: Sustained release formulation of 5 – ASA.
• Disintegration of capsule occurs in the stomach and the microspheres then disperse throughout the entire GIT
• Ethylcellulose coating to allow water absorption into the small beads containing the mesalamine
• Water dissolves the 5-ASA, which then diffuses out of the bead into the lumen

Sites of release of 5-ASA formulations
Topical 5-ASA formulations
Rowasa:
• Mesalamine suspended in a wax matrix suppository
• Effective in active proctitis
Canasa
• Mesalamine suspended in a suspension enema
• Effective in distal ulcerative colitis
• Advantages: Superior to topical hydrocortisone with 70-90%response rates
Glucocorticoids
• Indication: Moderate to severe IBD
• Not effective in maintenance of remission in either Ulcerative colitis or Crohn’s disease
• Once remission has been induced they should be tapered very gradually over many weeks
• According to their response to steroids, patients can be divided into 3 classes:
1) Steroid-responsive - 40 %
2) Steroid-dependent - 30 – 40 %
3) Steroid-unresponsive - 15 – 20 %
Antibiotics• Metronidazole, Ciprofloxacin and Clarithromycin
• Ulcerative colitis: Antibiotics have no role except in pouchitis
• Crohn’s Disease:
a. For active inflammatory, perianal and fistulizing disease: Metronidazole - 15-20 mg/kg/day in 3 divided doses OR
Ciprofloxacin – 500 mg BD
b. For preventing post-op recurrence – Metronidazole
• Adverse effects
• Metronidazole- Nausea,metallic taste, peripheral neuropathy
• Ciprofloxacin: Achilles tendinitis and rupture
• Oral Prednisolone: 40- 60 mg/day for active UC not responding to 5-ASA therapy
• Parenteral (i.v.) drugs: in more severe disease
Hydrocortisone: 300 mg/day
Methylprednisone: 40-60 mg/day
• Adverse effects:
Weight gain, fat redistribution, hyperglycemia, cataract,
Emotional changes, osteoporosis, aseptic osteonecrosis

• Enemas: useful in patients whose disease is limited to the rectum (proctitis) and left colon.
• Hydrocortisone is available as a retention enema (100 mg/60 ml),
• Usual dose is one 60-ml enema per night for 2 or 3 weeks.
• Hydrocortisone also can be given once or twice daily as a 10% foam suspension → delivers 80 mg hydrocortisone per application
• Useful in patients who have difficulty retaining the enema fluid
Topical steroids
• Controlled ileal-release preparation
• Equally efficacious to prednisone for ileocolonic CD
• Topical potency 200 times that of hydrocortisone
• Undergoes extensive first-pass metabolism (10% oral bioavailability) hence has fewer systemic side effects
• Topical therapy (e.g. enemas and suppositories) also is effective in treating colitis limited to the left side of the colon.
• Dose: 9 mg/day for 2 to 3 months in mild to moderate Crohn’s Disease
• Its role in maintenance of remission is not yet determined
Budesonide
Immunosuppressants
Thiopurine Derivatives
• Mercaptopurine (6-MP)
• Azathioprine
Methotrexate
Cyclosporine
Azathioprine & 6- Mercaptopurine
• Purine analogs; both are prodrugs
• Mechanism of action: Impair purine biosynthesis & inhibit cell proliferation
• Treatment of steroid-dependent and steroid- resistant disease
• Uses:
a. Maintain remission in both UC and Crohn’s disease
b. To prevent/delay recurrence of Crohn’s disease after surgical resection
c. To treat fistulas in Crohn’s disease

Metabolism
Active moiety
Hepato-toxic

• Differences in TPMT (ThioPurine Methyl Tranferase) determine the drug’s fate
• Metabolism shifted towards 6-thioguanine nucleotides
• Bone marrow suppression
• Weekly monitoring of CBC
Patients with minimal
TPMT activity
• Metabolism shifted towards 6-MMP
• Hepatotoxicity and reduced therapeutic response
• LFT monitoring done
Rapid metabolizers

Drug interactions
• Inhibition of Xanthine oxidase by allopurinol diverts metabolism towards production of 6-thioguanine analogs
• Augments the risk of immunosuppression
• Hence patients on mercaptopurine should be warned about serious interactions with medications used to treat gout and hyperuricemia
• If the patient is already taking allopurinol
dose decreased to 25% of standard dose
Adverse reactions
Idiosyncratic
• Pancreatitis
• Fever, rash
• Arthralgia
• Nausea, vomiting
Dose-related
• Suppression of bone marrow
• Elevation of liver enzymes
Serious ADRs
• Cholestatichepatitis
• Malignancies like non-Hogdkin’slymphoma
Methotrexate
• Mechanism of action:
Impaired DNA synthesis due to Dihydrofolate reductaseinhibition
Decreased IL-1 production
• Use: Induce & maintain remission in Crohn’s disease
• Response is rapid han that seen with thiopurines
• Dose: given by i.m. or s.c. route
For induction: 25mg/week
To maintenance: 15 mg/week

Adverse reactions
• GI toxicity: nausea, vomiting, diarrhoea, stomatitis
Minimized by concurrent administration of folic acid 5mg once weekly
• Hepatotoxicity : Periodic evaluation of liver enzymes
• Leucopenia : Periodic evaluation of CBC
• Pneumonitis

Cyclosporine• Use:
Severe ulcerative colitis that has failed to respond adequately to steroids
To treat fistulas in Crohn’s disease
• Mechanism of action:
Binds to cyclophilin; the complex then inhibits calcineurin
Ultimately inhibits activation of T-cells and production of IL-2
Adverse reactions
Hypertension, gingival hyperplasia, hypertrichosis,
Paresthesias, tremors, headaches
Nephrotoxicity - renal function should be monitored frequently.
Seizures
Opportunistic infections

Tacrolimus
Macrolide antibiotic
MOA - similar to cyclosporine.
Effective in adults with steroid refractory UC and CD
As compared to cyclosporine
• 100 times more potent.
• Have good oral absorption despite proximal small-bowel Crohn's involvement.

Biological therapy
Anti- TNFα drugs:1. Infliximab
2. Adalimumab
3. Certolizumab pegol
Natalizumab

Anti- TNFα drugs
Infliximab
Chimeric IgG1 antibody (25% mouse, 75% human)
Mechanism : Binds to membrane-bound TNF-α and causes cell lysis by antibody-dependent or cell-mediated cytotoxicity
Effective in
1) active CD patients refractory to steroids and thiopurines
2) CD patients with refractory enterocutaneous fistulas
3) Moderate to severe ulcerative colitis
Dose: 5mg/kg i.v. infusion every 8 weeks
Adverse reactions
Acute - fever, chills, urticaria, or even anaphylaxis.
Subacute - serum sickness-like reaction.
Increased incidence of respiratory infections - tuberculosis or other granulomatous infections.
Contraindicated in patients with severe congestive heart failure (NYHA classes III and IV) .
Possible increased incidence of non-Hodgkin's lymphoma, leukemia and new-onset psoriasis

Antibody formation
Antibodies develop in 10% of patients
Leads to increased risk of infusion reactions and loss of response
Strategies to minimize the development of these antibodies -
Treatment with glucocorticoids or other immunosuppressives.
Increasing the dose of infliximab (10 mg/kg).
Decreasing the interval between infusions.

Adalimumab
• Recombinant human monoclonal IgG1 antibody.
• Binds TNF- α and neutralizes its function by blocking the interaction between TNF and its cell-surface receptor.
• Injected subcutaneously.
• Less immunogenic than infliximab.
• Used in active CD patients refractory to steroids and thiopurines
Certolizumab pegol
• Human monoclonal antibody Fab conjugated with PEG
• Does not contain Fc fragment
• Mechanism of action:
a) Inhibits monocyte cytokine production
b) Inhibits mast cell degranulation
• Effective for induction of clinical response in patients with active inflammatory CD.
• Less immunogenic than infliximab
• Given by s.c. route once monthly
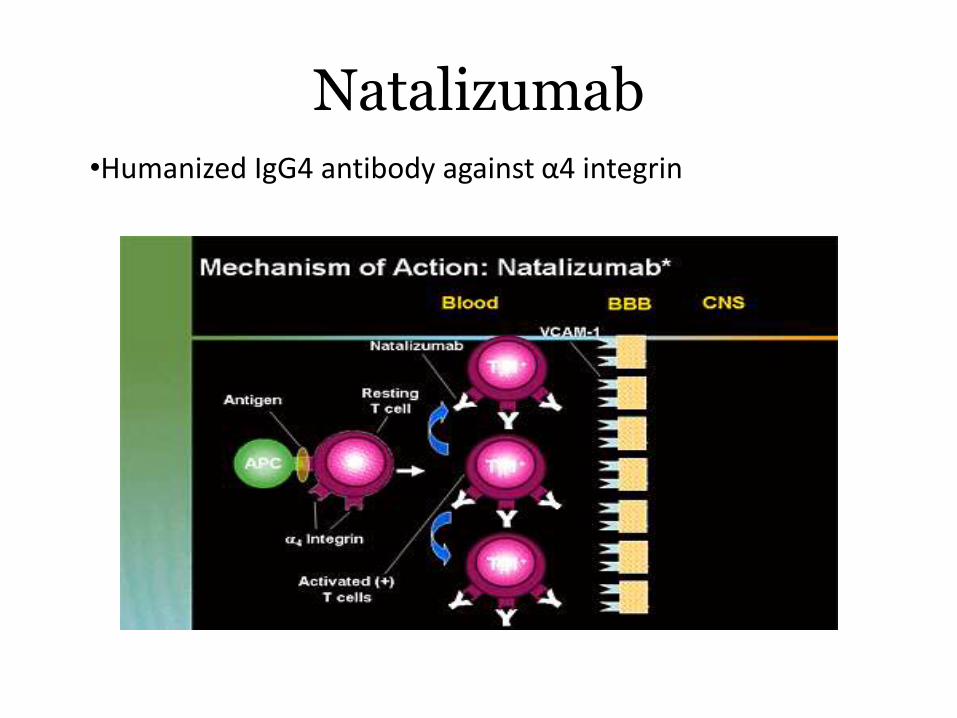
Natalizumab•Humanized IgG4 antibody against α4 integrin
• Approved for induction & maintenance of remission in crohn’s disease
• Especially useful in patients who are refractory or intolerant to anti- TNFα therapy
• Adverse effects:
Leads to Progressive Multifocal Leucoencephalopathy(PML)
Hence its use is contraindicated with other immuno-suppressive drugs- Thiopurines & steroids

Supportive therapy
• Iron, calcium and Vitamin D supplementation given in case of deficiency
• Oral folate routinely given to patients receiving 5-ASA therapy
• Vitamin B12 serum levels measured annually in case of ileal Crohn’s
Anti- diarrheal agents (Loperamide, Diphenoxylate) & anti-cholinergic drugs (Dicyclomine)
• To reduce frequency of bowel movements
• To relieve rectal urgency
• Contraindicated in severe disease or suspected obstruction:-can predispose to toxic megacolon
Bile salt binders (Cholestyramine, Colesevalam)
• Prevent bile-salt induced diarrhea in patients with ileo-colic resection

Nutritional therapy• Patients with active Crohn’s: Respond to bowel rest and Total
Parenteral Nutrition (TPN)
• As effective as steroids in inducing remission but not for maintenance
• Enteral nutrition in the form of elemental or peptide-based preparations are also as effective as glucocorticoids or TPN -not palatable.
• Dietary intervention has no role in ulcerative colitis
Prebiotics
• Non-digestable carbohydrates such as fructo-oligosaccharides
• Broken down by gut flora to short-chain fatty acids
• Their efficacy is unproven till date
Probiotics
• Bacteria or yeast ingested orally as therapy
• Administered as a single organism or as a defined mixture
• Mechanism of action:
a) Production of bacteriocins
b) Production of butyrate, necessary for colonocytefunction
c) Ability to downregulate inflammation
• Examples:
• A combination product VSL #3 prevents recurrent pouchitis
• E. coli Nissle- Equivalent to meselamine in maintaining remission in UC
IBD and Pregnancy
Effect of IBD on fertility:
1. Scarring of fallopian tubes- either due to involvement of terminal ileum or as a sequalae of pouch surgery
2. Dyspareunia- due to perirectaland perianal abscess and fistulae
3. Decreased sperm count-secondary to 5-ASA therapy; it is reversible
Effect of IBD on Pregnancy:
1. In mild or quiescent disease, fetal outcome is nearly normal
2. Spontaneous abortions, stillbirths, and developmental defects are increased with increased disease activity, not medications. Hence any flare-up is treated aggressively
3. Patients should be in remission for 6 months before conceiving
4. Most patients of CD can deliver vaginally but C-section is preferred in case of anorectal and perirectal abcess/ fistulae.
Safety of drugs
5-ASA based therapy
• FDA category B drugs
• Oral Sulfasalazine, Meselamine, Balsalazide & Topical 5-ASA agents- Safe for use in pregnancy and breast-feeding
• Additional folate supplementation is given- 2mg/day

Glucocorticoids
• FDA category C drug
• Generally considered safe in pregnancy
• Indicated for patients with moderate to severe disease activity
• Are secreted in breast milk in minute amounts and do not have any significant effect on the nursing infant
Antibiotics
• Safest antibiotics to use for short periods of time (for few weeks)- Ampicillin and Cephalosporins
• Metronidazole can be used after 1st trimester
• Ciprofloxacin (FDA category C drug) should be avoided
• Tetracyclines - Contraindicated
Thiopurine drugs
• FDA category D drugs
• Pose minimal risk during pregnancy
• Secreted in negligible amounts in breast milk; pose minimal risk to the infant
• Scenarios for use:
a) If the patient cannot be weaned from the drug
b) In case of an exacerbation which requires these drugs
Cyclosporine A
• FDA Category C drug
• Very limited data on its use in pregnancy
• Avoided unless the patient requires surgery
Methotrexate
• Teratogenic and hence absolutely contraindicated

Anti- TNFα drugs
• FDA category B drugs
• Infliximab, adalimumab, certolizumab- can be used in
pregnancy and lactation
• No increased risk of stillbirth or abortion
• Natalizumab- Category C drug; limited data available,
hence avoided
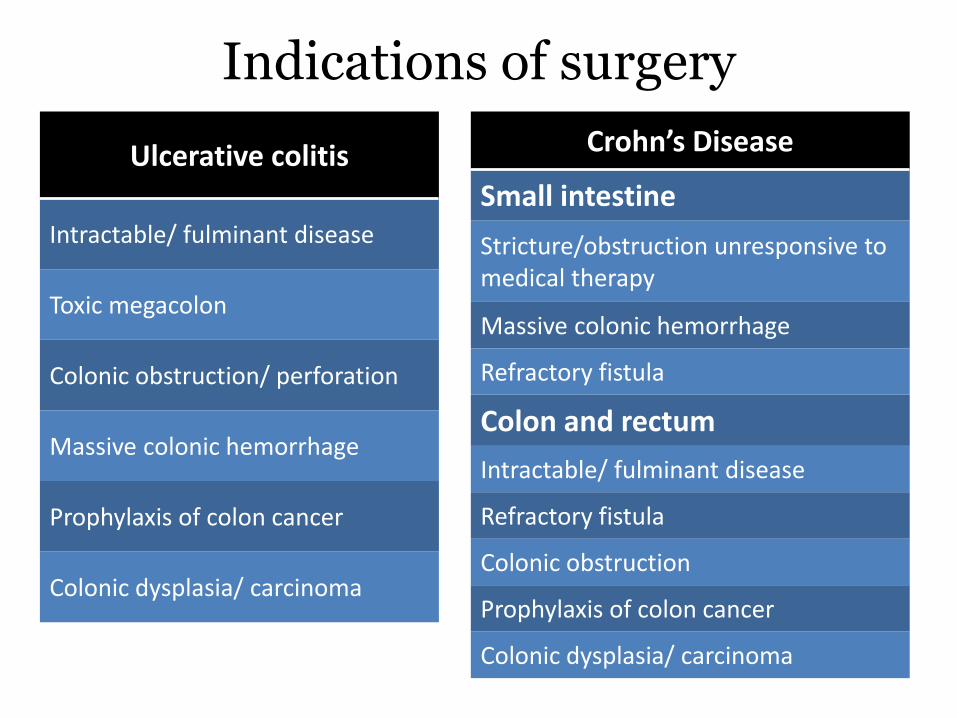
Indications of surgery
Ulcerative colitis
Intractable/ fulminant disease
Toxic megacolon
Colonic obstruction/ perforation
Massive colonic hemorrhage
Prophylaxis of colon cancer
Colonic dysplasia/ carcinoma
Crohn’s Disease
Small intestine
Stricture/obstruction unresponsive to medical therapy
Massive colonic hemorrhage
Refractory fistula
Colon and rectum
Intractable/ fulminant disease
Refractory fistula
Colonic obstruction
Prophylaxis of colon cancer
Colonic dysplasia/ carcinoma
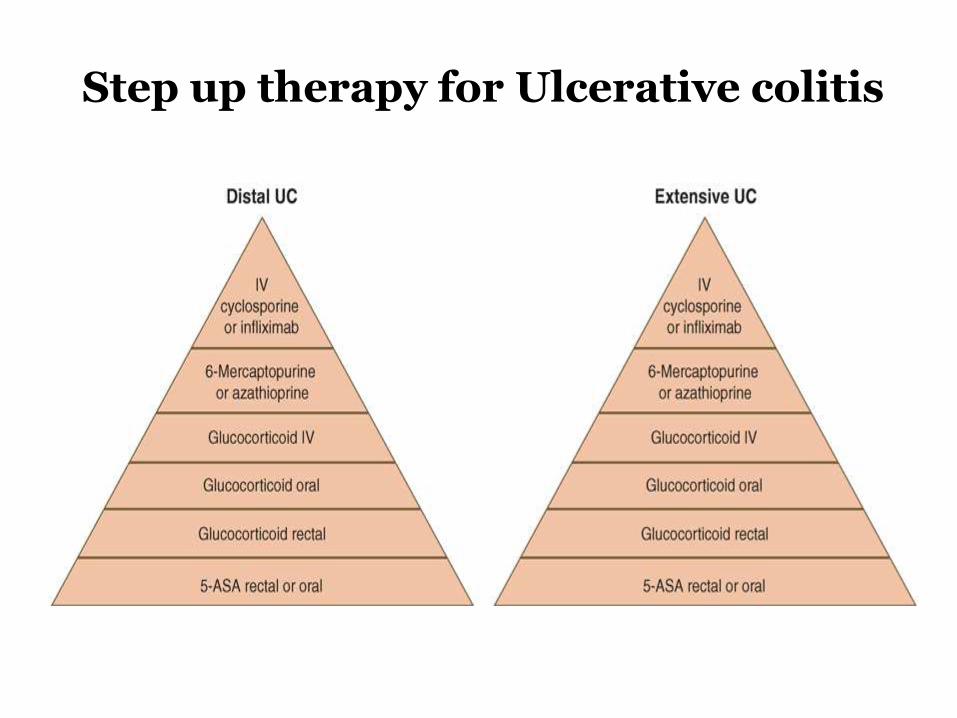
Step up therapy for Ulcerative colitis
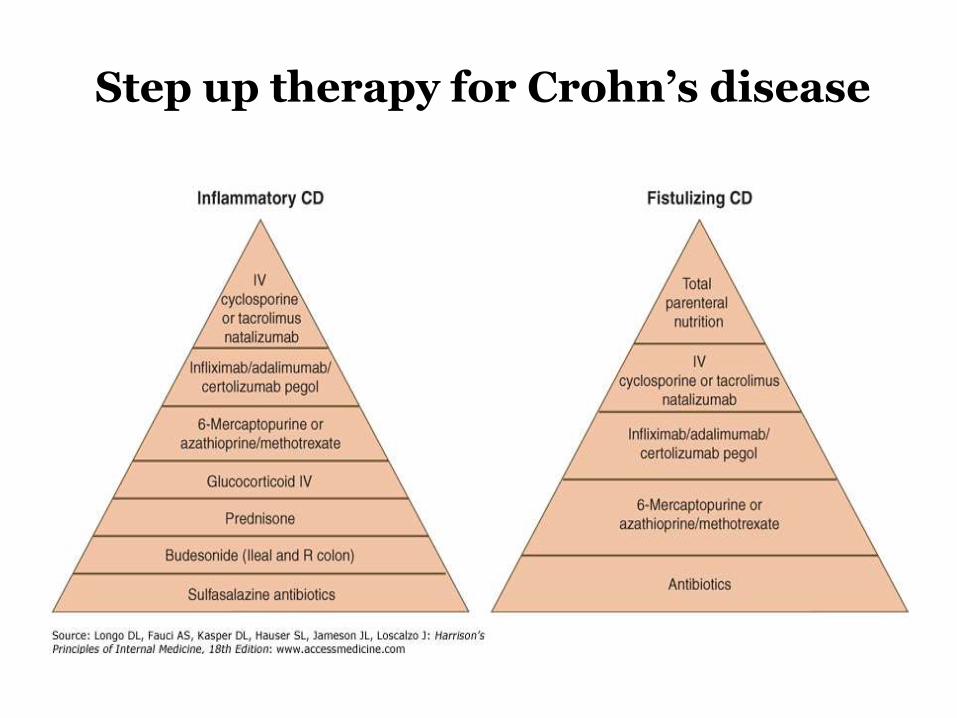
Step up therapy for Crohn’s disease

Top down Therapy?

Pitfalls
Safety issues: ed risk of TB, opportunistic infections, malignancies
Cost factor
Majority of patients have mild disease & will be overtreated
Drugs in the pipeline
Adhesion molecule inhibitors:
• Vedolizumab- Anti α4β7 antibody
• Anti MAdCAM-1 antibody
• Alicaforsen: anti ICAM-1 antisense oligonucleotide;
inhibits ICAM-1 production by endothelium by
preventing translation of its m-RNA
L.lactis secreting IL-10
Non-invasive non-colonizing bacterium
Genetically modified to secrete IL-10 , a potent anti-
inflammatory molecule
Allows delivery directly at the intestinal site and thus obviates
systemic exposure
Ustekinumab
Anti IL-12/IL-23 antibody
Inhibit cellular activation & cytokine production

Thank You!