Embed Size (px)
Citation preview

Pharmacotherapy of Insomnia

History Problem statement Physiology of sleep wake cycle Pathogenesis Pharmacological management Non Pharmacological approaches Newer targets
Overview

“Insomnia is defined as repeated difficulty with sleep initiation, maintenance, consolidation, or quality that occurs despite adequate time and opportunity for sleep and that results in some form of daytime impairment.”
Definition

History of Pharmacotherapy of Insomnia Antiquity
1912
1959
19th century
•Alcoholic beverages
•Lardanum compound
•Herbal formulations COMPOUNDS
• Bromide • Chloral hydrate • Paraaldehyde • Urethane • Sulfonal
•1903- Barbital 1912- Phenobarbital
Chlordiazepoxide
Present
•Benzodiazepines •1980 Non Benzodiazepines •Melatonin and Analogues

Epidemiology
10- 50% of the population are affected.
20 % of adult population having chronic insomnia
Increases with age
Twice as common in females
•Up to 30 yrs [M/F 1:1]•> 30 years females•> 70 yrs M/F 1:2 ]
Lower educational attainment
Depression
Unemployment
Widowed, divorced

Socioeconomic Impact of Insomnia
Insomnia has a detrimental effect on health related quality of life to the same degree as chronic disorders such as depression and congestive heart failure (Katz & McHorney, 2002).
economic costs that encompass health care use, absenteeism accidents, increased alcohol consumption
(Chilcott & Shapiro, 1996; Stoller, 1994)
annual cost was estimated to be between $35 to$107 billion a year in the US

International Classification of Sleep Disorders, 2nd Edition (ICSD-2)
hAdjustment insomnia
primary insomnia
Paradoxical insomnia
Insomnia due to medical condition
Insomnia due to mental disorder
•Inadequate sleep hygiene
•Insomnia due to drug or substance abuse
•Idiopathic insomnia
•Behavioral insomnia of childhood
•Primary sleep disorders causing insomnia

Types of insomnia The National Institute of Mental Health Consensus Development Conference (1984)
1. Transient insomnia <3 days brief environmental stressor • It may respond to attention to sleep hygiene rules.• If hypnotics are prescribed ,lowest dose for 2-3 nights.
2 . Short-term insomnia lasts from 3 days to 3 weeks personal stressor such as illness, grief, or job problems
• sleep hygiene education is the first step. • Hypnotics may be used adjunctively for 7-10 nights.

3.Long-term insomnia insomnia that has lasted for >3 weeks
No specific stressor may be identifiable.
A more complete medical evaluation is necessary in these patients, but most do not need an all-night sleep study.

Physiology
Promotion of wakefulness
Areas
Medullary reticular formation Thalamus Basal forebrain
Neurotransmitters
Histamine (TMN) posterior hypothalamusNA –(LC)Serotonin – (DRN)Dopamine –(VTA)Acetylcholine – cholinergic neurons of the basal forebrain

Promotion of wakefulness
•A novel neuropeptide, orexin (also known as hypocretin),
•localized to a cluster of neurons in the lateral hypothalamus also appears to be involved in the control of wakefulness.

Promotion of sleepThe anterior hypothalamus includes the ventrolateral preoptic nucleus (VLPO), containing gamma-aminobutyric acid (GABA) and the peptide galanin, which are inhibitory and promote sleep
These project to the TMN and the brainstem arousal regions to inhibit wakefulness.
.

Melatonin and the circadian process
Melatonin synthesis is inhibited by light and stimulated by darkness
The nocturnal rise in melatonin begins between 8 and 10 pm and peaks between 2 and 4 am, then declines gradually over the morning.
Melatonin acts via 2 specific melatonin receptors:
MT1 attenuates the alerting signal, and MT2 phase shifts the SCN clock.
The suprachiasmatic nucleus (SCN) is entrained to the external environment by the cycle of light and darkness.
The retinal ganglion cells transmit light signals via the retinohypothalamic tract to stimulate the SCN.
A multisynaptic pathway from the SCN projects to the pineal gland, which produces melatonin.

14
Sleep Wake Cycle___________________________

The flip-flop switch model

Stages of Sleep Non-Rapid Eye Movement (NREM) sleep◦Stage I ◦Stage II◦Stage III◦Stage IV
Rapid Eye Movement (REM) sleep


Normal Sleep Values Normal sleep per day is between 6-8 hours,
although some people can maintain a 4-6 hour cycle
4-6 NREM/REM cycles per night Sleep structure changes throughout life Wakefulness after sleep◦Less than 30 minutes
Sleep Onset Latency (SOL) ◦Less than 30 minutes
REM Sleep Latency◦70-120 minutes

PathogenesisSpielman model 3P’s of Insomnia
PredisposingAnxiety, depression
Precipitating•Sudden change in life•schedule changes, •medications, •medical conditions
Perpetuating
Poor sleep hygieneover concern

Genetic Hypothesis
Fatal familial insomnia autosomal dominant human prion disease caused by changes in the PRNP (prion protein) gene.
Disruption sleep pattern that progresses to hallucinations, a rise in catecholamine levels,autonomic disturbancessignificant cognitive and motor deficits. .
CLOCK and Per2.
A mutation or functional polymorphism in Per2 can lead to circadian rhythm disorders
advanced sleep phase syndromedelayed sleep phase syndrome
A mis sense mutation gene encoding the GABAA beta 3 subunit in a patients with chronic insomnia.

Objective testsSleep DiaryA sleep diary is appropriate when a patient reports an irregular sleep schedule.
Actigraphy
For actigraphy, a portable device is worn around the wrist to record gross motor activity and light/darkness over extended periods.
Polysomnography
To distinguish between other sleep disorders OSA RESTLESS LEG SYNDROME

PHARMACOTHERAPY OF INSOMNIA
BenzodiazepinesNon-benzodiazepine hypnoticsMelatonin receptor agonistsAntidepressantsAntipsychoticsAntihistaminesObsolete drugs

Benzodiazepines
Sedative hypnotic property
7 membered Diazapene ring Benzene ring
5-aryl substituent
SAR OF Diazepam

Structure 2-Keto Benzos◦ Some administered as prodrug
◦ All have active metabolites (commonly desmethyldiazepam)
◦ Long half-lives (most in excess of 60 hours) Diazepam
Chlordiazepoxide (Librium)
Flurazepam
Clonazepam Flunitrazepam

◦ No active metabolites◦ Not metabolized in the liver◦ Intermediate half-lives (most ~ 8-20 hours)
3-hydroxy Benzos
Lorazepam Oxazepam

Triazolo Benzos
Very rapid onset Very short half-life
Alprazolam Triazolam
Additional heterocyclic ring attached at the 1 and 2 positionsSome active metabolitesShort to intermediate half-lives (anywhere from 3-14 hours)

Long acting Diazepam , Flurazepam, Clonazepam, Chlordiazepoxide
Intermediate acting Alprazolam, Estazolam, Temazepam , Lorazepam Nitrazepam Short acting Triazolam , Oxazepam , Midazolam
Classification

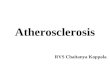
Site and Structure of Action Site of action is the
GABAA receptor
Structure of GABAA receptor comprised of 5 subunits
o 2 α subunits (to which GABA binds)
o 2 β subunits (to which barbiturates bind)
1 γ subunit (to which benzodiazepines bind)

Thus far 16 different subunits have been identified and classified into seven subunit families: α,β,,,ε,θ,π.
six α, three β , three , and single ε,θ,π. and subunits
Benzodiazepine-sensitive · α1, α2, α3, α5 Benzodiazepine-insensitive · α4 and α6

Properties of GABAA receptor Myorelaxant, motor-impairing, and anxiolytic-
like properties thought to be mediated by α2, α3, and/or α5 subunits
Benzodiazepines acting on α2, α3, and/or α5 nonsedative, nonamnesic anxiolytic
properties
Sedative ,Anticonvulsant activity and amnesic properties are thought to be mediated by α1 receptors
Limbic system α2
Ascending RAS

MOA
The benzodiazepines do not substitute for GABA but appear to enhance GABA's effects allosterically without directly activating GABAA receptors or opening the associated chloride channels.
Benzodiazepines increase the affinity of the receptor for GABA, and thus increase Cl - conductance and hyperpolarizing current
increase in the frequency of channel-opening events

Absorption
Except for Midazolam all can be absorbed orally
Distribution
•90% Protien bound • Cross the placental barrier
Metabolism
Phase 1 reactions , metabolites are conjugated in phase 2 reactions
Phase 1 metabolites are pharmacologically active Excretion
Water souluble metabolites


BZD are the choice of drugs for treatment of insomnia Drug with most suitable pharmacokinetic profile is chosen
Treatment of insomnia
Transient insomnia ( 3 DAYS )
Rapidly acting , rapidly eliminated BZD like
Triazolam (0.125-0.25mg) HSEffective in sleep initiation problems
Temazepam 15-30mg at bed time Effective in sleep maintenance
Used intermittently

Long term insomnia > 3 weeks
Intermittent use of
Flurazepam (15-30mg) HS rebound insomnia and withdrawal effects are less Nitrazepam (5-10mg) HS
Short Term insomnia 3days -3 weeks
Tremazepam (15-30mg)HS effective in sleep maintainence Flurazepam(15-30mg)HS effective in early morning awakeningEstazolam(1-2mg) HS

Drug Peak Blood Level (hours)
Elimination Half-Life1 (hours)
Comments
Alprazolam 1-2 12-15 Rapid oral absorption
Chlordiazepoxide 2-4 15-40 Active metabolites; erratic bioavailability from IM injection
Clorazepate 1-2 (nordiazepam) 50-100 Prodrug; hydrolyzed to active form in stomach
Diazepam 1-2 20-80 Active metabolites; erratic bioavailability from IM injection
Eszopiclone 1 6 Minor active metabolites
Flurazepam 1-2 40-100 Active metabolites with long half-lives
Lorazepam 1-6 10-20 No active metabolites
Oxazepam 2-4 10-20 No active metabolites
Temazepam 2-3 10-40 Slow oral absorption
Triazolam 1 2-3 Rapid onset; short duration of action
Zaleplon <1 1-2 Metabolized via aldehyde dehydrogenase
Zolpidem 1-3 1.5-3.5 No active metabolites1Includes half-lives of major metabolites.
Pharmacokinetic properties of some benzodiazepines and newer hypnotics in humans

Effect of hypnotics on sleep architecture DRUG EFFECT ON SLEEP
CYCLE SYMPTOMS
Benzodiazepines Partial disruption of the NREM/REM ratio Slight decrease in REM
Decreased stage 1 and stage 3 and 4 Increased duration of stage 2
On withdrawal- vivid dreams Due to slight increase in REM
Sleep latency shortened
Episodes of wakeing between stage 4 and REM decreased
Non Benzodiazepines Does not interfere with sleep cycle
Decrease in stage 0 and stage 1
Increased stage 3 and 4
No increase in REM on withdrawal
Decreased sleep latencyAnd awakening
Refereshing sleep

Barbiturates Decreases the duration of REM sleep
Alters the NREM/REM RATIO
REM buildup
Severely alters the sleep cycles Decreased stage 0Decreases the stage 1 And stage 4
On withdrawal
Nightmares
Decreased sleep latency
Decreased night time awakening

1. Long-acting agents taken at bedtime
daytime sedation the following day Cognitive impacts are considerable: Inhibition of learning behaviors, academic performance,
and psychomotor functioning common
2. Short-acting agents taken at bedtime early-morning wakening rebound insomnia the following night
ADVERSE REACTIONS

3. Advancing age retards Phase 1 metabolism of BZD
4. Respiration is not seriously depressed, unless benzo is taken concurrently with another CNS depressant (i.e., alcohol)
5. Benzodiazepine Poisoning Treated with the BZD receptor antagonist
iv. Flumazenil 0.2mg/min max 5mg till the symptoms of respiratory depression , confusion lathargy , congnitive symptoms disappear .

DependenceMECHANISMDue to the gradual down regulation of the GABA receptors
Taken for prolonged periods of time Drugs with Short to medium half life
WITHDRAWAL SYMPTOMS
anxiety state, increases in rebound insomnia, restlessness, agitation, irritability, etc

Tolerence to the sedative effects developes slowly mechaniasm is unclear
May be dude to self induction of benzodiazepines
Tolerance
CYP3A4 CYP2C9 Potentiate the effects of other CNS depressants alcohol, hypnotics and neuroleptics anticonvulsants
Enzyme inhibitors like cimitidine, ketoconazole enhance BZD action Smoking and aminophylline antagonises the activity of BZD
DRUG INTERACTIONS

MOA – Benzodiazepine receptor 1 (BZ1) -- alfa 1 subunit
Antianxiety , sedative in nature Do not alter REM Sleep Pattern Minimal day time residual sleepiness Risk of tolerance and dependence is much less than BZD
Non Benzodiazepines
Drug t1/2 Action Use
Zolpidem(10-20mg)
2-3 hrs Faster onset Transient insomnia
Zaleplon(10-20mg) 3-4 hrs Shorter duration of hypnosis
Short term insomnia
Zopiclone(7.5mg) 6-8 hrs Longer acting
Eszopiclone(1-3mg)
6 hrs

Melatonin Congeners
Ramelteon
Melatonin levels in the suprachiastmatic nucleus rise and fall in a circadian fashion,
Two GPCRs for melatonin, MT1 and MT2, are found in the suprachiasmatic nucleus,
MT1 receptors promotes the onset of sleepMT2 receptors shifts the timing of the circadian system
Ramelteon binds to both MT1 and MT2 receptors with high affinity but, unlike melatonin, it does not bind appreciably to quinone reductase 2, the structurally unrelated MT3 receptor

Pharmacokinetics of ramelteon
Absorption -rapidly GI tract ,peak serum concentration obtained in 1 hr significant first-pass metabolism that occurs after oral administration, ramelteon bioavailability is <2%
Distribution In the bloodstream, ~80% of ramelteon is protein bound
Metabolism hepatic CYPs 1A2, 2C9 t1/2 of ~2 hours in humans.
Of the four metabolites, one, M-II, acts as an agonist at MT1 and MT2 receptors
Inhibitors CYP1A2- Ciprofloxacin Fluvoxamine CYP2C9- FluconazoleInducer- refampin

Indications - transient and chronic insomnia specifically sleep onset difficulties
Dosage 8-mg tablet be taken ~30 minutes before bedtime
ADVERSE REACTIONS
dizziness, somnolence, fatigue, and endocrine changes as well as ↓ testosterone and increases in prolactin.Infertility

Antidepressants
TCA
Amitriptyline doxepin
Side effects: dry mouth, urinary retention, dizziness, daytime sedation
Used at much lower doses for insomnia
Mirtazapine
Associated with weight gain, increased appetite, daytime sedation and dizziness
Trazodone- off label use at low doses
Major side effects: sedation, dizziness, dry mouth, orthostatic hypotension, priapism (rare)
No good research to support its use

Antipsychotics Called the “atypical antipsychotics” Block dopamine from binding to receptors in the
brain Examples:◦ risperidone (Risperdal)◦ olanzapine (Zyprexa)◦ quetiapine (Seroquel)◦ ziprasidone (Geodon)

Antipsychotics Not FDA approved for insomnia
Typically used at doses much lower than those for treating psychosis
Quite sedating but also associated with weight gain, increased risk for diabetes, high blood pressure, restless leg syndrome, muscle spasm or parkinson-like symptoms
Quetiapine and ziprasidone have been shown to increase total sleep time as well as sleep efficiency

Non Prescription Antihistamines Diphenhydramine Doxylamine Promethazine 25mg HS 10mg in children
Commonly used in pediatric population as sedatives
Little evidence to support their use Side effects: dry mouth, urinary retention, blurred vision, dizziness,
sedation, next day hangover

Barbiturates
Paraaldehyde Chloral hydrate Meprobamate
Obsolete drugs

BARBITURATESClassification
(1) Ultra-short-acting barbiturates: act within seconds, and their duration of action is 30min. Therapeutic use of Thiopental: anesthesia
(2) Short-acting barbiturates: have a duration of action of about 2h. The principal use of Secobarbital, : sleep-inducing hypnotics.
(3)Intermediate-acting barbiturates: effect lasting 3-5h.eg Amobarbital
(4)Long-acting barbiturates: >6h. Such as Barbital and Phenobarbital. Therapeutic uses: hypnotics and sedative, and antiepileptic agents at low doses.

BARBITURATES Barbiturates depress the CNS at all level in a dose-
dependent fashion. Now it mainly used in anaesthesia and treatment
of epilepsy; use as sedative-hypnotic agents is no longer recommended.
Reasons: (1) have a narrow therapeutic-to-toxic dosage range. (2) suppress REM sleep. (3) Tolerance develops relatively quickly. (4) have a high potential for physical dependence and abuse. (5) potent inducers of hepatic drug-metabolising enzymes

MOA Barbiturates share with benzodiazepines the ability to
enhance the action of GABA, but they bind a different site on the GABA-receptor/chloride channel, and their action seems to prolong the duration of the opening of GABA-activated chloride channels.
PK High lipid solubility cross the blood-brain barrier and results in a short onset.
redistribution to the other tissues results in short duration of action.
Metabolized by Phase 1 reaction in the liver
Barbiturates and their metabolites the excretion via the renal route.

Therapeutic uses1. Sedative-hypnotic agents(obsolete )2. convulsions as in status epilepticus.3. Anesthetic (or be given before anesthetic)4. Combination with antipyretic-analgesic5. Treatment of hyperbilirubinemia and kernicterus in
the neonate.
Adverse effectsAfter effect: hangover, automatism, amnesiaToleranceDependence: including psychologic and physiologic dependence. Depressant effect on respirationAllergic Skin eruptions and porphyria

Barbiturate poisoning Mostly sucidal
Charaterised by respiratory failure , cardiovascular collapse Coma Renal failure
Treatment
1. Gastric lavage 2. Artificial respiration 3. Forced alkaline diuresis with mannitol and sodium
bicarbonate

Chloral hydrate (obsolete )
Chloral hydrate was used for the short-term treatment of insomnia mid-20th century.
It is also still used as a sedative prior to EEG procedures, few available sedatives that does not suppress epileptiform discharges.
Misc Drugs
Paraaldehyde(obsolete )
Paraldehyde is a polymer of acetaldehyde
It was commonly used to induce sleep in sufferers from delirium tremens
Meprobamate
Was marketed as a anxiolytic and sedative
MOA – Acts at the GABAA receptor in the limbic system

The Non-pharmacologic Approach
Cognitive Behavioral Therapy for Insomnia (CBTi)
◦Stimulus control therapy◦Sleep restriction therapy◦Relaxation training◦Cognitive therapy◦Sleep hygiene education

Sleep Hygiene Exercise earlier during the day, and no more than 4-6 hours before
sleep
Keep bedroom dark and quiet, to be used only for sleep
Curtail time in bed to only when sleepy
Fixed sleep/wake times for 365 days
Avoid naps
Avoid stimulus or stimulating activities before sleep or in bed
No alcohol at least 4 hours before sleep, no caffeine after noon, and quit smoking!!
Light snack before bedtime

Stimulus Control Use bedroom for sleep
Go to bed only when tired and sleepy
Remove clock from the bedroom to avoid constantly watching it
Regular sleep/wake times
Light therapy if required
No bright lights when you wake up at night

Sleep Restriction An effective form of treatment
Estimate the time actually asleep then limit bedtime to that amount, but no less than 5 hours
Add time in bed gradually once the patient sleeps more than 85% of that time

Cognitive therapy and relaxation therapy
The patient is educated to correct inaccurate beliefs about sleep•To reduce catastrophic thinking •excessive worrying about the consequences of failing to obtain adequate sleep.
Relaxation therapypatient is taught to recognize and control tension through a series of exercises
Biofeedback techniques can also be used. provide patients with immediate feedback regarding their level of tension and rapidly teaching them how to relax.

HERBAL MEDICATIONS
Valerian root Induction of sleep Lavender Sleeping aidsChamomile tea

Newer targets
Orexins
They excitatory neuropeptides that have a critical role in maintaining wakefulness.
Orexin receptor antagonists promote sleep in animals and humans
SB-649,868, 0rexin receptor antagonist in development by GlaxoSmithKline.
Currently in Phase 2 development,
Bettica P, "Phase I studies on the safety, tolerability, pharmacokinetics and pharmacodynamics of SB-649868, a novel dual orexin receptor antagonist". J. Psychopharmacol. (Oxford)

Suvorexant (MK-4305) is a dual in development by Merck & Co.
Suvorexant works by turning off wakefulness rather than by inducing sleep.
It is not currently approved for commercial use, but it has completed three Phase III trials
FDA Review
Increased somnolence the next day and users of higher doses had an increased rate of suicidal ideation

Conclusions
•Treatment of insomnia requires a multimodal approach of cognitive and behavioral therapy and pharmacotherapy
•Non Benzodiazepines are the most favored hypnotics , followed by Benzodiazepines
•Looking into the future , Orexin antagonists could emerge as a new treatment for insomnia

THANK YOUTHA