-
8/11/2019 Introduction of Pharmacotherapy
1/51
Pharmacotherapy I
By : Lolita
-
8/11/2019 Introduction of Pharmacotherapy
2/51
Component of Assessment
Mid term exam : 30%
Final term exam : 30%
Task : 35% Other component / attendance : 5%
-
8/11/2019 Introduction of Pharmacotherapy
3/51
Main Theme by System
Before mid
Rational Pharmacotherapy (1x) : Mrs. Lolita
Pain and Inflammation (4x) : Mrs. Lolita
Gastrointestinal (2x) : Mrs Woro Supadmi
After mid
Gastrointestinal (4x) : Mrs. Woro Supadmi
Infection (3x) : bacterial, viral, parasite, protozoa :
Mrs Sudewi and Lolita
-
8/11/2019 Introduction of Pharmacotherapy
4/51
Specific Issues
Pain & Inflammation1. Nociceptic & Neuropatic pain :
central,
peripheral
2. Headache disorders/cephalgia (migraine,vertigo, tension,
cluster, sinus)
3. Joint pain : (osteoarthritis, rheumatoid
arthritis, gout, bursitis)4. Post-operative pain & cancer
pain
-
8/11/2019 Introduction of Pharmacotherapy
5/51
Learning Indicator
Patophysiology
Clinical Data Interpretation
Pharmacotherapy Specification of Drug
-
8/11/2019 Introduction of Pharmacotherapy
6/51
ReferencesPrimary :
Dipiro, JT., Hamilton, CW.,Schwinghammer, TL., and Wells,BG,
2000, PharmacotherapyHandbook, McGraw Hill, NewYork.
Greene, RJ and ND Harris, 2000,Patology and Therapeutics
forPharmacists : a basic for clinicalpharmacy practice
Secondary :
Lacy C. F., Armstrong L. L.,Goldman M. P., Lance L. L.,
2010,Drug Information Handbook, Lexi-Comp Inc., Ohio.
-
8/11/2019 Introduction of Pharmacotherapy
7/51
The Benefit Outcomes
Assist students in understanding the use of the
drug in specific disease
Students are able to choose the right medicine
Students are able to provide drug information (for
example about the side effects of drugs, drug
contraindications, drug interactions with other
drugs or drug interactions with food, and etc)
Students are able to interact with physicians andother medical
personnel
Students help patients perform self-medication
-
8/11/2019 Introduction of Pharmacotherapy
8/51
RationalePharmacotherapy
-
8/11/2019 Introduction of Pharmacotherapy
9/51
Pharmacotherapy
Greek : Pharmacon & Therapeia
Pharmacotherapyis the treatment of disease through
the administration of drugs.
Choose a drug based on the types and signs of disease.
Area of pharmacy practice that is responsible for
ensuring the safe, appropriate, and economical use of
drugs in patient care.
-
8/11/2019 Introduction of Pharmacotherapy
10/51
Therapy
Approach
Nonpharmacology
Pharmacology
Pharmacotherapy
Alternative therapy
Radiotherapy
Surgery
Genetherapy
Drug therapy
Imunotherapy
1600 chemical agents40.000 formulations100.000 OTC
-
8/11/2019 Introduction of Pharmacotherapy
11/51
Pharmacotherapy Process
Symtoms/Signs
Diagnose
Treatment Methods
DRUG THERAPY
Drug Selection
Dosage Adjustment
Prescription
Drug Administration
Drug Utilization
Effect
Bad Response Good response
-
8/11/2019 Introduction of Pharmacotherapy
12/51
Rational Drug Therapy
Prescribing and choosing the drug in manner
that maximizes clinical effect (maximizing
efficacy and minimazing toxicity), functional
status, overall patient satisfaction, health
quality of life at the lowest possible total cost.
-
8/11/2019 Introduction of Pharmacotherapy
13/51
The rational use of drugs requires that patients
receive medications appropriate to their clinical
needs, in doses that meet their own individual
requirements for an adequate period of time, and at
the lowest cost to them and their community. correct drug
appropriate indication appropriate drug considering efficacy,
safety, suitability
for the patient, and cost
appropriate dosage, administration, duration no
contraindications correct dispensing, including appropriate
information for
patients patient adherence to treatment
WHO conference of experts Nairobi 1985
-
8/11/2019 Introduction of Pharmacotherapy
14/51
Clinical
featuresof illness
Patientexpectations
Potentialconsequences
Presentingsymptoms
2. Understanding
pathophysiology
1. Making Dx
3. Reviewing menuof Rx options
4. Selectingoptimal drug/dose for patient
5. Choosingendpointsto follow
6. Making alliancewith patient,followingendpoints
Clinical
outcomesefficacytoxicitymorbiditymortality
Patient
satisfaations
Costsdirectindirect
Functional Outcomerelief of symptoms
Patient Presentation Process of Rational
Therapeutics
Result of
Intervention
Process of rational drug therapy
-
8/11/2019 Introduction of Pharmacotherapy
15/51
The Purpose of Prescribing
Maximise
effectiveness
Minimise risks
Minimise costs
Respect patients choice
The most effective
The most safest
The most affordable
-
8/11/2019 Introduction of Pharmacotherapy
16/51
The challenge of
prescription
Prescribing
Patient Compulsion
Economic
Pressure
Limited time
Individual
preference
Unknowledge
Pharmaceutical Companies Interference
-
8/11/2019 Introduction of Pharmacotherapy
17/51
Rational Drug Used
Right
Follow upDiagnosis
Indication
Types of drug Information
Dosage, route and frequence
Patient condition
-
8/11/2019 Introduction of Pharmacotherapy
18/51
Why Rational Use ?
Drug explosion
Efforts to prevent the development of
resistance Growing awareness
Increased cost of the treatment
Consumer Protection Act. (CPA)
-
8/11/2019 Introduction of Pharmacotherapy
19/51
% Primary Health Care patients treated
according to guidelines
0
10
20
30
40
50
60
70
1990/1 1992/3 1994/5 1996/7 1998/9 2000/1
Africa Asia
Source: WHO database on drug use 2003
-
8/11/2019 Introduction of Pharmacotherapy
20/51
WHO, Dept. Essential Drugs and Medicines Policy
% drugs that are prescribed unnecessarilyestimated by a
comparison of expected versus actual prescription
Chalker HPP 1996, Hogerzeil et al Lancet 1989, Isah et al
2000
010
20
30
40
50
60
70
80
Nepal Yemen Nigeria
% antibiotics % injections % drugs % cost
-
8/11/2019 Introduction of Pharmacotherapy
21/51
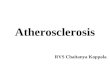
5-55% of PHC patients receive injections -
90% may be medically unnecessary
0% 10% 20% 30% 40% 50% 60%
Eastern Caribean
Jamaica
El Salvador
Guatemala
Ecuador
L.AM ER. & CA R.
Nepal
Indonesia
Yem en
ASIA
Zimbabwe
Tanzania
Sudan
Nigeria
Cameroon
Ghana
A FR IC A
% of primary care patients receiving injections
Source: Quick et al, 1997, Managing Drug Supply
15 billion injections per year globally
half are with unsterilized needle/syringe
2.3-4.7 million infections of hepatitis B/C
and up to 160,000 infections of HIV peryear associated with
injections
-
8/11/2019 Introduction of Pharmacotherapy
22/51
30 to 60 % of PHC patients receive antibiotics -
perhaps twice what is clinically needed
0% 10% 20% 30% 40% 50% 60% 70%
Guatemala
Jamaica
El Salvador
Eastern Caribean
L.AMER. & CAR.
Bangladesh
Nepal
Indonesia
ASIA
Zimbabwe
Tanzania
Ghana
Cameroon
Swaziland
Sudan
AFRICA
% of PHC patients receiving antibiotics
Source: Quick et al, 1997, Managing Drug Supply
-
8/11/2019 Introduction of Pharmacotherapy
23/51
WHO, Dept. Essential Drugs and Medicines Policy
Prescribing by dispensing and non-dispensing doctors in
ZimbabweTrap et al 2000
2.31
28.4
58
8.65
1.67
9.5
48
13
0 10 20 30 40 50 60 70
no.drug items/Px
% Px with injections
% Px with antibiotics
consultation time (mins)
dispensing doctors non-dispensing doctors
-
8/11/2019 Introduction of Pharmacotherapy
24/51
Problems with Irrational Pharmacotherapy :
1. Complex diseases or health problems:Example: A patient has
many symptoms, but is embarrassed totalk about the main one, so the
situation does not get addressed
2. Lack of appropriate training skills by prescribers to
giveproper diagnosis:Example: Prescriber does not do a physical
exam and prescribesdrugs based solely on oral information provided
by the patient
Diagnosis
3. Overworked prescribers:Example: health facility has only one
prescriber, and an average of 300 patients per day
to consult
4. Lack of basic diagnostic equipment and testsExample 1: No
microscope or reagents to examine blood & urine
Example 2: No x-ray machine to test a patient suspected of
having
tuberculosis
-
8/11/2019 Introduction of Pharmacotherapy
25/51
Prescribing
1. Using expensive drugs when equivalent ones are
availableExample 1: The antibiotic cefalexin is more expensive than
co-trimoxazole in
treating simple infectionsExample 2: Ampicillin injection is
prescribed when the patient could
take ampicillin tablets, which are cheaper, easy to take,
andinvolve lower risk of side effects
2. Selecting the wrong drug for the patients illnessExample: An
antidiarrhoeal drug is prescribed when the patient is
dehydrated with simple diarrhoea and only ORS is needed
3. Prescribing several drugs when fewer drugs wouldprovide the
same effect
Example: Sulfadoxine/pyrimethamine and paracetamol are
prescribed whenthe patient has fever, but not malaria
4. Prescribing drugs when the disease is self limiting andthe
patient would get better without taking any drugs
Example: Ampicillin is prescribed when the patient has a simple
cold, withoutsore throat, cough or fever
-
8/11/2019 Introduction of Pharmacotherapy
26/51
1. Wrong interpretation of the prescription:Example: Ampicillin
is prescribed, but amoxicillin is dispensed.
2. Wrong quantity dispensedExample: Artemether/Lumefantrine is
prescribed to be taken four
tablets two times daily for three days (should be a total of 24
tablets),but the patient only receives 16 tablets, which is
sufficient for only 2 days
3. Labelling incorrect or inadequateExample:
Sulphadoxine/pyrimethamine (white tablet) is dispensed, but
the name of the drug is not written on the container
label,meaning that the drug will be unidentifiable once the
patientleaves the pharmacy
Dispensing
-
8/11/2019 Introduction of Pharmacotherapy
27/51
4. Incorrect/insufficient dispensing information:
Example: paracetamol 250mg is prescribed for a
child, but only paracetamol 500mg isavailable in the pharmacy.
The higherdosage pill is given to the childs motherwithout telling
her to divide the tabletbefore giving it to the child
5. Unsanitary practices:
Example: 20 tablets of paracetamol 500mg werebeing counted, when
some tablets fell to the floor.These were picked up and dispensed
to be given to the
patient anyway
-
8/11/2019 Introduction of Pharmacotherapy
28/51
Packaging
1. Poor quality of packaging material
Example: packaging material must protect the drug against
the
sun and humidity in order to ensure the integrity and
quality of the dosage form required by the patient
2. Inadequate container size when repackaging the product
Example: the size of the packaging material must conform to
the
quantity of medication dispensed. In the case of oral
drugs, too large a container could cause break-up ofthe items
packed within
-
8/11/2019 Introduction of Pharmacotherapy
29/51
-
8/11/2019 Introduction of Pharmacotherapy
30/51
Poor Compliance
Compliance is the degree to which the patientcarries out the
physicians instructions onhow to take the prescribed drug and
treatment.Many studies about outpatient compliance carriedout in
developing countries indicate that only about50% of patients follow
the instructions given by the
physician
-
8/11/2019 Introduction of Pharmacotherapy
31/51
Poor Compliance
Causes of poor compliance include:
1. Improper labelling
Neither the name of the patient, nor the name of thedrug is on
the container labels when dispensed. If
two or more drugs are dispensed together, thepatent does not
know which drug he/she is taking
2. Inadequate instructions:
The instructions on dosage frequency must be
written on the drug label, or the patient couldforget how to
take it when he/she arrives home andbecomes involved in other
activities
-
8/11/2019 Introduction of Pharmacotherapy
32/51
3. Treatment /instructions that do not consider the
socio-economic and cultural aspects of thepatient
Example: In cases where the patient does not know how
to read, proper instructions would includegraphic symbols of how
to take the drug.
For a treatment of three days, for example, you could number
the days 1 to 3, and then below each day, make a mark for
eachtime the drug must be taken that day
-
8/11/2019 Introduction of Pharmacotherapy
33/51
Explanations Poor Compliance :
Lack of knowledge
Influenced by others
Negative attitudes
Own experience
Own perceptions
Difficult/complicated regimenExtremes of age and need for
assistance
-
8/11/2019 Introduction of Pharmacotherapy
34/51
Consequences in Irrational Therapy
-
8/11/2019 Introduction of Pharmacotherapy
35/51
Public Health and Economic Consequences
Adverse possibil i ty lethal effects, e.g. due to antibiotic
misuse or inappropriate use of drugs in selfmedications
L imited eff icacy, e.g. in the case of under-therapeutic
dosage of antibiotic, tuberculosis or leprosy drugs
Antibiotic resistance, due to widespread overuse of
antibiotics as well as their use in under-therapeutic
dosage
Drug dependence, e.g. due to daily use of pain killersand of
tranquilizers
Risk of infection due to improper use of injections:
abscesses, polio, hepatitis and HIV/AIDS
-
8/11/2019 Introduction of Pharmacotherapy
36/51
WHO, Dept. Essential Drugs and Medicines Policy
Adverse drug eventsReview by White et al, Pharmacoeconomics,
1999, 15(5):445-458
4-6th leading cause of death in the USA
Estimated costs from drug-related morbidity &
mortality 30 million-130 billion US$ in the USA
4-6% of hospitalisations in the USA & Australia
commonest, costliest events include bleeding,
cardiac arrhythmia, confusion, diarrhoea, fever,
hypotension, itching, vomiting, rash, renal failure
-
8/11/2019 Introduction of Pharmacotherapy
37/51
WHO, Dept. Essential Drugs and Medicines Policy
Overuse and misuse of antimicrobials contributes
to antimicrobial resistance
Malaria
choroquine resistance in 81/92 countries
Tuberculosis
2 - 40 % primary multi-drug resistance
Gonorrhoea 5 - 98 % penicillin resistance in N. gonorrhoeae
Pneumonia and bacterial meningitis
12 - 55 % penicillin resistance in S. pneumoniae
Diarrhoea: shigellosis
10-90+ % amp, 5-95% TMP/SMZ resistance
Source: DAP, EMC, GTB, CHD (1997)
-
8/11/2019 Introduction of Pharmacotherapy
38/51
Ecomomic consequences
Inappropriate drug use or irrational therapyhave also a impact
on household and nationalhealth budgets,
Example :- the use of expensive brand-name product
while cheaper generic drug are available,
- combinations preparation,- multi-drug prescribing
-
8/11/2019 Introduction of Pharmacotherapy
39/51
Improve Rational Therapy
-
8/11/2019 Introduction of Pharmacotherapy
40/51
Educational
InterventionType
Managerial
Financial
Regulatory
Prescribers
Consumers
-
8/11/2019 Introduction of Pharmacotherapy
41/51
-
8/11/2019 Introduction of Pharmacotherapy
42/51
3. Managerial Strategies Essential drug list
Kit system distribution
Pre-printed order form
Stock control
Course-of-therapy packaging
Effective package labelling
4. Financial interventions Drugs are sold at a slightly higher
price to create a fund for
improving PHC services
Making people pay for drugs could reduce overconsumption
Improve drug supply and cost-sharing
5. Regulatory strategies Banning unsafe drugs
Limiting the import of drugs on the market
I i d / i
-
8/11/2019 Introduction of Pharmacotherapy
43/51
Interventions targeted at consumers/patients
1. Educational materials
Patient education Public education
2. Managerial stategies
Course of therapy packagingBlister packs facilitated patient
adherence to
leprosy treatment
The use of antimalarial drug packaging resulted
in a significant improvement in patientcompliance
-
8/11/2019 Introduction of Pharmacotherapy
44/51
3. Financial interventions
Community revolving drug funds
4. Regulatory strategies Regulatory strategies are not targeted
at
consumers
-
8/11/2019 Introduction of Pharmacotherapy
45/51
Six Key Steps When Practising
Approach Pharmacotherapeutics
1. Making an accurate diagnosis
2. Understanding the pathophysiology of disease
3. Reviewing the menu of pharmacotherapeutic options
4. Selecting patient-spesific drug and dose
5. Selection end point to follow
6. Maintaining a therapeutic alliance with the patient
-
8/11/2019 Introduction of Pharmacotherapy
46/51
Approach to rational therapeutics
1. Knowing the diagnosis with reasonable certainly
i. Problem that lead to empiric therapy
Febrile leukemic patient, now neutropenic
with chemotherapy, who is approptriately
started on broad-spectrum antibiotics.
ii. Inappropriate acceptance of empiric treatment
The rule for treatment of febrile
immunosuppressed patient often are
generalized and applied to other populationof patient who donot
cancer, have not
recieved chemotherapy, are not
immunosuppressed and are not neutropenic.
-
8/11/2019 Introduction of Pharmacotherapy
47/51
2. Understanding the pathophysiology of the patients
disease
i. Confusion between syndrome and disease
Hyponatremia (psychogenic polydepsia,
bronchogenic carcinoma, servere lossed of
salt and water, adrenal insufficiency)
ii. Being misled by a name Lupus erythematosus and lupus
anticoagulant
iii. Further advantages of understanding the disease
Proper understanding of disease not onlyleads to appropriate
therapeutic plan but also
appropriate preventive measures as well
-
8/11/2019 Introduction of Pharmacotherapy
48/51
3. Understanding the pharmacology of useful
drugsi. Drugs that have no evidence of efficacy
ii. Prescribing drugs because it makes
sense
iii. Factors that perpetuate incorrect
information about drugs
4 O ti i i l ti f d d d
-
8/11/2019 Introduction of Pharmacotherapy
49/51
4. Optimizing selection of drug and dose
The option of not using a drug.
New drug information not provided by the
manufacture Increasing knowledge of drugsadverse effects
Impact of drug costs
Irrational beliefs
Detailing and counterdetailing
Conflicts of interest.5. Selection of appropriate therapeutic
end point
Appropriate end points of efficacy
End point reflecting toxicity
The prescription as an experiment
6. The physician-patient relationship
Patient-physician communication can affect the
choice of therapy and its outcome
Attention to rational therapeutics
Guiding Principles of Pharmacotherapy
-
8/11/2019 Introduction of Pharmacotherapy
50/51
Guiding Principles of Pharmacotherapy
1. There should be justified and documented indication for
everymedication that is used
2. A medication should be used at the lowest dosage and for
the
shorten duration that is likely to achieve the desired
outcome.3. When patient is adequated treated with a single
dose,
monotherapy is preferred4. Newly approach medication should be
used only if there are clear
advantages over older medication.5. Whenever possible, the
selection of a medication regimen should
be based upon evidence obtained from controlled clinical
trial.6. The timing of drug administration should be considered as
a
possible influence on drug efficacy, adverse effects,
andinteractions with other drugs and food.
7. A medication regimen should be simplified as much as possible
to
enhance patient adherence.8. A patients prescription of illness
or the risks and benefits oftherapy may affect adherence and
treatment outcome.
9. Careful observation of a patients response to treatment
isnecessary to confirm efficacy, prevent, detect, or manage
adverseeffect, assess compliance, and determine the need for
dosage
adjustment or discontinuation of drug therapy.
Guiding Principles of Pharmacotherapy (cont )
-
8/11/2019 Introduction of Pharmacotherapy
51/51
10. A medication should not be given by injection when givingby
mouth would be just as effective and safe.
11. Before medications are used, lifestyle modification shouldbe
made, when indicated, to obviate the need for drugtherapy or to
enhance pharmacotherapy outcome.
12. Initiation of drug regimen should be done with
fullrecognition that a medication may cause a disease, sign,
symptom, syndrome or abnormal laboratory test.13. When a variety
of drugs are equally efficacious and equallysafe, the drug that
result in the lowest health care cost or ismost convenient for the
patient should be chosen.
14. When making a decision about drug therapy for
individualpatients, societal effects should be considered.
15. The possible reasons for failure of medication
regimeninclude inappropriate drug selection, poor
adherence,improper drug dose or interval, misdiagnosis,
concurrentillness, interaction with foods or drugs,
environmentalfactors, or genetic factors.
Guiding Principles of Pharmacotherapy (cont. .)