Embed Size (px)
Citation preview

Biological treatments of OCD
Dr.S.Santhosh Goud
Chairperson;Dr.Ravi Awchar

DSM 5-OCD and related disorders• OCD• BDD• Hoarding disorder• Trichitillo mania/HPD• Excoriation/skin picking disorder• Substance/medication induced OCD• OCD due to another medical condition

Ocd criteria
DSM 5 criteria
• Presence of obsession/compulsion
• Time consumption>1 hr/clinically significant distress or impairment
• Rule out role of substance/other medical condition
• Not due to other mental disorder

• Obsessions are persistent, uncontrollable thoughts, impulses, or images that are intrusive, unwanted and disturbing. They cause anxiety or discomfort that significantly interferes with normal life
• Individuals who have OCD feel compelled to perform repetitive actions called compulsions, or rituals, in an attempt to relieve the distress caused by the obsessions

Neuro biology of OCD
Emotional brain controls the reasoning brain
The part of the brain responsible for ocd, functions very much on the same emotional level as that of a two year old.
Reasoned argument is, therefore, pointless…!

Loss of filtering
• Thalamus-sensory gating
• Caudate nuleus-thought filtering

• Orbito frontal cortex-combines thoughts and emotions
• Cingulate gyrus in the middle of brain
• Helps in shifting attention from one thought/behavior to another
• CG also acts as a signaling center for danger so forces to do compulsion


Structural changes• Volume reduction of the OFC• Cingulate cortex• Decreased OFC with increased thalamic
volume constant finding in refractory cases

Functional studies• FDG-PET increased glucose metabolism
in ofc,caudate,thalamus,pfc and acc

Neurotransmitter changes• Serotonin• Autoreceptors (5HT1D) require higher
SSRI dose• Role of 5HT 7 receptors Dopamine• Quinpirole treated rats-compulsive
checking

Glutamate• OCD is a hyperglutaminergic state of
prefrontal brain-(Carlsson)• SSRI, Clomipramine do regulate this Glutamate regulators used in resistant
cases

Neuroimmunology• Auto immunity to basal ganglia• Sydenham chorea, PANDAS• D8/17 B lymphocyte antigen more prone• Plasmapheresis, iv immunogloblin useful

Genetics
• Higher concordance in monozygotic twins
• 5HTTLPR
• Role of DRD4 variant
• COMT variation
• polymorphisms of MAOA genes

Course and prognosis
• Adolescent onset~65%
• <15% after 35 yrs of age
• Nearly 70 percent of patients report a continuous course of symptoms, and 23 percent experience a waxing and waning course
• Average time to treatment after meeting diagnostic criteria for OCD is 11 years
(The Brown Longitudinal Obsessive Compulsive Study,2006)
Naturalistic follow up studies from pre-sri/cbt era
• Improvement in 66% recovery in 32%(lewis,1936)
Pollitt study-101 patients
• 3 months-15yrs(mean 3.4yrs) out come
• 34 leucotomized
• 67 non leucotomized
• 40% good response;most of them with in 2 years
• Most of the patients having waxing waning course

• Skoog &skoog study 1999
• 250 patients admitted between 1947-1953
• Reexamined between 1989-1993
• 75 died,32 lost follow up
• 144 patients data could be collected
• Shneiders ocd criteria

• Improvement in 83%
• Recovery 48%
• Complete recovery 20% subclinical symptoms 28%
• 38% recovered in first decade
• Hal of them had illness for >30yrs

Recent studies
• Full remission 20-45%(Y-BOCS <3)
• Partial remission 20-55%( 4-14)
• Clinical ocd10-60%(>15)
• 40-60% unsatisfactory response
• Predictors of treatment response..?
• Hoarding disorder poor response to SSRI
• High scores on sexual/religious obsessions poor response to SRI/CBT(Matix-colas et al)
• Somatic obsessions had poorer insight and less response to drugs(expect MAO-I)


FDA approved drugs
• Anafranil (clomipramine)-c10
• Prozac (fluoxetine)-c7
• Luvox (fluvoxamine)-c8
• Paxil (paroxetine hydrochloride)
• Zoloft (sertraline)-c6
“Off-label" OCD medications
• Celexa (citalopram)
• Lexapro (escitalopram)
• Effexor (venlafaxine)
• Cymbalta (duloxetine)
• Remeron (mirtazapine)

Augmenting agents
• Antipsychotic medications(Risperdal (risperidone)Zyprexa (olanzapine)Seroquel (quetiapine))
• Other augmenting agents
• B blocker
• 5HT1 agonist
• Ondansetron
• Riluzole
• Memantine

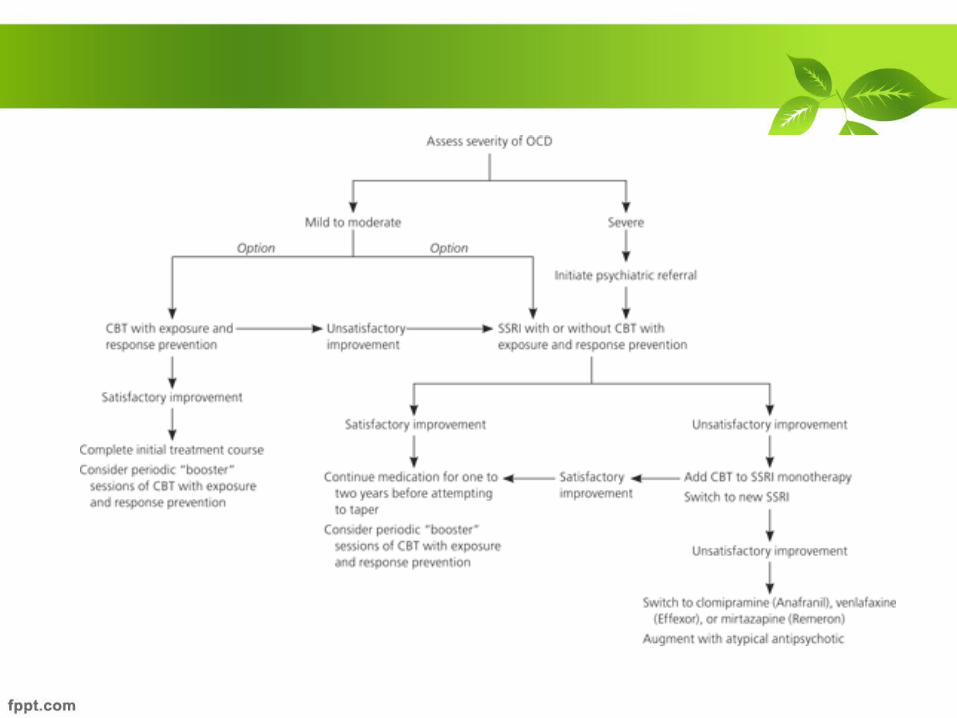
How to choose the right drug
• Diagnosis;severity;comorbid illness
• Medical history;the potential side effects of each medication, and the possibility of an adverse interaction with another drug the person is taking

drug Starting dose Target dose(mg/day)
Usual Maximum dose
Occassional max dose
Fluoxetine 20 40-60 80 120
Sertraline 50 200 200 400
Fluvoxamine 50 200 300 450
Paroxetine 20 40-60 60 100
escitalopram 10 20 40 60
clomipramine 25 100-250 300
Resistence vs refractoriness
• Rauch and Jenike, in 1994, established the difference between "resistant" and "refractory" patients.
• They defined as "resistant" those who participate in a trial with any first-line therapy and do not have a satisfactory response, while the "refractory" patients are those who do not respond appropriately to several treatments administered in an adequate manner
• Pallanti et al
• No response -<25% reduction in YBOCS score CGI-I 4
• Refractory- failure to respond to all available treatments
• Pseudo resistance..?

Predictors of treatment non-response
• Early age of onset
• Longer ocd
• Mixed ocd
• Sexual obsessions
• Washing compulsons
• Hoarding
• Poor insight
• Schizotypal pd
• Tic disorders

• Switching to another SSRI(~50%)
• Switch to Clomipramine(upto300mg)
(min 2 SSRI trails;NIMHANS ocd clinic)
• IV Clomipramine (~43%)
• Min 14 infusions
• 250mg/day
• More side effects

• SSRI to venlafaxine or Mirtazepine
Augmentation
• Best evidence with Risperidone(0.5-6mg)
• First doc for augmentation
• Other drugs haloperidol(1.5-5mg),olanzepine(2.5-20),quetiapine(50-300)
• Clonazepam(upto 6.5mg)
• Buspirone(60-90mg),

• Nicotine,cbzp,lamotrigene,gabapentine,
reboxetine,psychostimulants,nac,
Aripiprazole less evidence
• Lithium, thyroid,l-tryptophan(2gm) ineffective;useful for comorbidities
• once-weekly oral morphine sulfate
• Other less well-supported monotherapies include dextroamphetamine (Dextrostat), tramadol (Ultram), monoamine oxidase inhibitors, ondansetron (Zofran)

• When to change augmentation?
• no desired response by 6-8wks
• Augmentation for how long?

Combination strategies
• SSRI and clomipramine
• Superior to switching(Pallanti et al)
• Look for serotonin syndrome

Intensive residential therapy
• IP treatment
• Multidisciplinary approach
• Pharmacotherapy
• Daily CBT 2-4 hours
• Group therapy
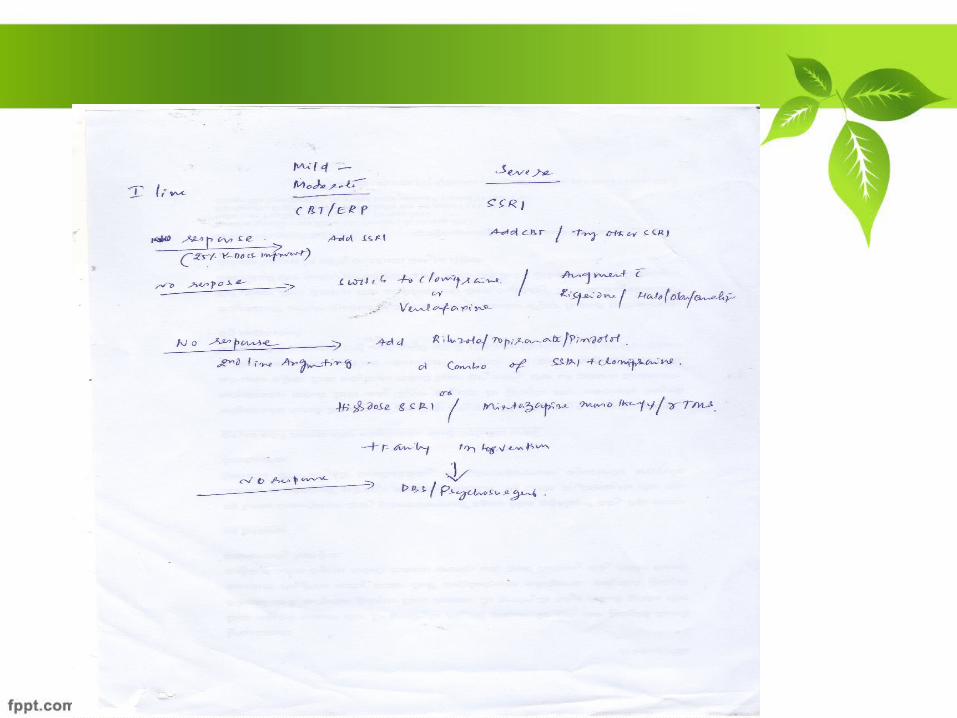

Other somatic therapies
• r-TMS
• DBS
• ECT
• Vagal stimulation

r-TMS
• Since 1997, in published trials, a total of 110 OCD patients have been treated with rTMS
• Greenberg et al.inhibition of the prefrontal activity with rTMS might reduce obsessive-compulsive symptoms.

• 1) stimulation of the dorsolateral prefrontal cortex (DLPFC)
• 2) inhibition of the orbitofrontal cortex (OFC) directly
• 3) inhibition of the supplementary motor area (SMA).
Deep brain stimulation
• Nucleus accumbens
• Anterior capsule
• Caudate nucleus
• Subthalamic nucleus

ECT• The primary indication would be the
severe depression with which intractable OCD is often associated(Bulletin of Clinical Psychopharmacology
• ECT Use in Refractory Obsessive-Compulsive Disorder Nesrin B. Tomruk Omer Saatcioglu)

Vagus nerve stimulation
Neurosurgical procedures Criteria• Diagnosis by standard criteria• Severe ocd• Long standing(>5 yrs)• At least 3 serotenergic(one should be
clomipramine),2 augmenting agents, for 12 weeks
• Adequate cbt (20hrs)• Less than 25% improvement with treatment

Procedures
• Anterior capsulotomy
• Anterior cingulotomy
• Subcaudate tractotomy
• Limbic leukotomy(subcaudate tractotomy with anterior cingulotomy)
Gamma knife capsulotomy safer and non-invasive

Further reading on psycho surgery in OCD
• Indian J Psychiatry. 2009 Jul-Sep; 51(3): 216–221 Surgical treatment of obsessive compulsive disorders: Current status Paresh K. Doshi