Embed Size (px)
Citation preview

Staged Biventricular Repair for Neonates with Left
Ventricular Outflow Obstruction, Ventricular Septal
Defect, and Aortic Arch Obstruction
Mohammad Shihata, Chawki Elzein, Sujata Subramanian, and Michel Ilbawi
Neonatal LVOTO
• The vast majority of neonates with LVOTO suitable for biventricular repair are managed with balloon or to a lesser extent surgical aortic valvuloplasty.
• The study population comprises a small subset of the neonatal spectrum of LVOTO ( < 4% of the CHSS LVOTO inception cohort from 29 centers, (n=1217, 1994 - 2008).

Complex Neonatal BiV Repair
• If the native LVOT cannot be used as the sole systemic outflow, it needs to be :
• Replaced: Ross ± Konno
• Augmented: Yasui; primary or staged ( Norwood/Rastelli )
• Bypassed: LV to DAo conduit

Neonatal Ross/Konno
• Neonatal Ross±Konno operation is associated with high mortality especially if combined with an arch repair; 33% - 67%. ( CHSS and STS-CHD )
• In the CHSS LVOTO cohort the Ross group had a 40% failure rate (conversion to SV or Transplant).

Staged vs. Primary Yasui
• For the last decade, no one approach has been clearly superior.
• Primary Yasui is associated with the need for early reintervention.
• A staged approach may be necessary in borderline cases.

Study Population

Patient Characteristics% (N) Mean ± SD Min. Max.
Gestational age (wk.) -- 37 ± 2.4 30 41
Preterm 23 (10) -- -- --
Gender (F) 43 (19) -- -- --
Weight (kg) -- 2.9 ± 0.63 1.6 3.9
BSA (m ) -- 0.19 ± 0.03 0.13 0.24
IAA-B 70.5 (31) -- -- --
CoA 29.5 (13) -- -- --
VSD 100 (44) -- -- --
Aortic Stenosis 88.7 (39) -- -- --
Aortic Atresia 11.3 (5) -- -- --
AV annulus (mm) -- 3.3 ± 0.8 1.5 5
AV ( z score ) -- - 5.9 ± 1.9 -10.3 -3.1
Borderline LV 16 (7) -- -- --
Genetic Syndrome 52.2 (23) -- -- --
2

Stage 1
% (N) Mean ± SD Median
Age (d) -- 11.7 ± 9.6 8
Norwood BT 45 (20) -- --
Norwood RV PA 48 (21) -- --
Hybrid 7 (3) -- --
CPB (min.) -- 135 ± 46 120
Cross Clamp (min.) -- 65.5 ± 26 59
Selective Perfusion (min.)
-- 38.2 ± 13.6 36
ECMO 9.1 (4) -- --
Ventilation (d) -- 6 ± 1.5 6
ICU stay -- 11.9 ± 4 11.5
Hospital stay (d) -- 36.3 ± 56.7 21
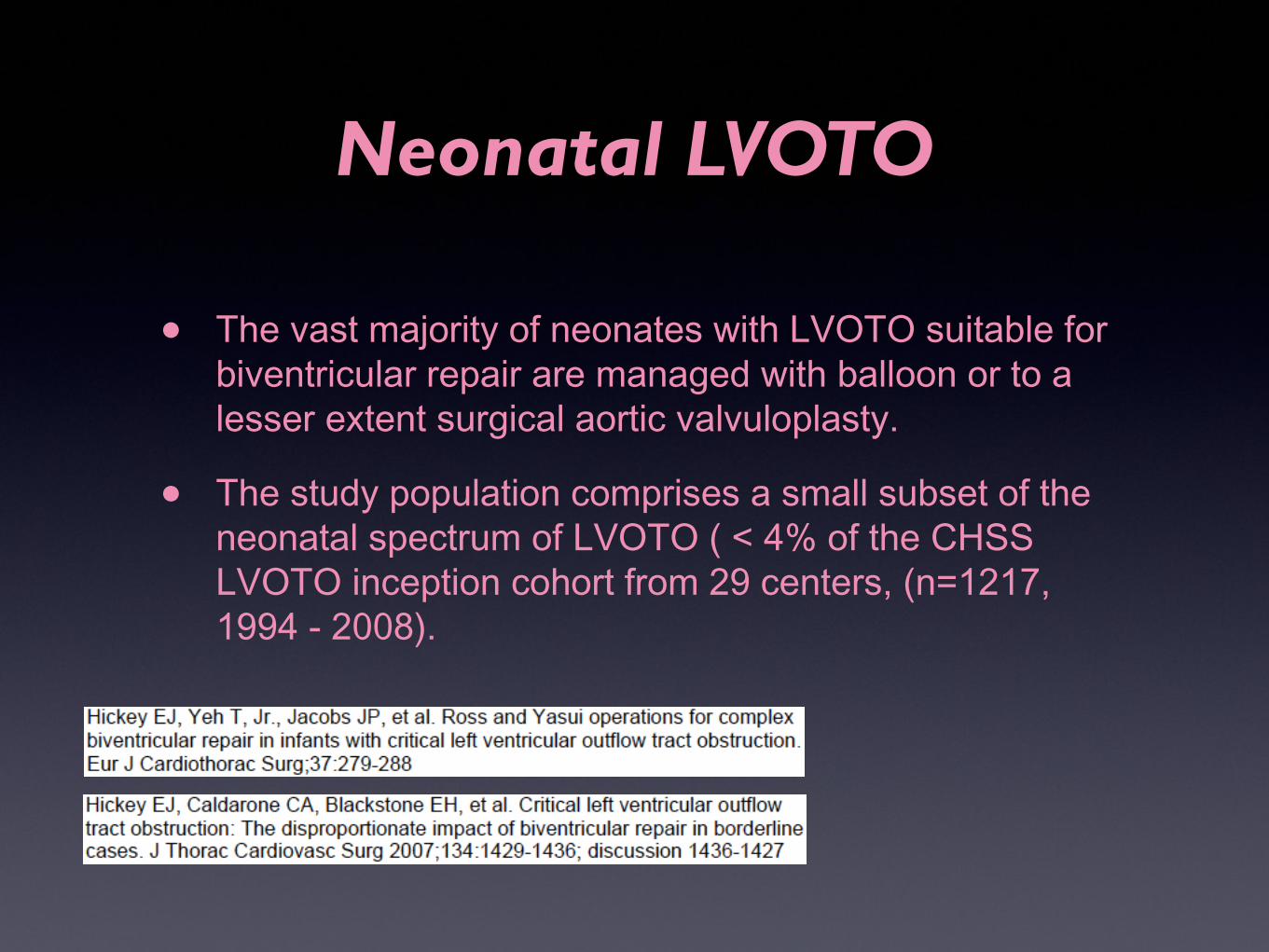
Post Norwood Survival

Interstage Survival
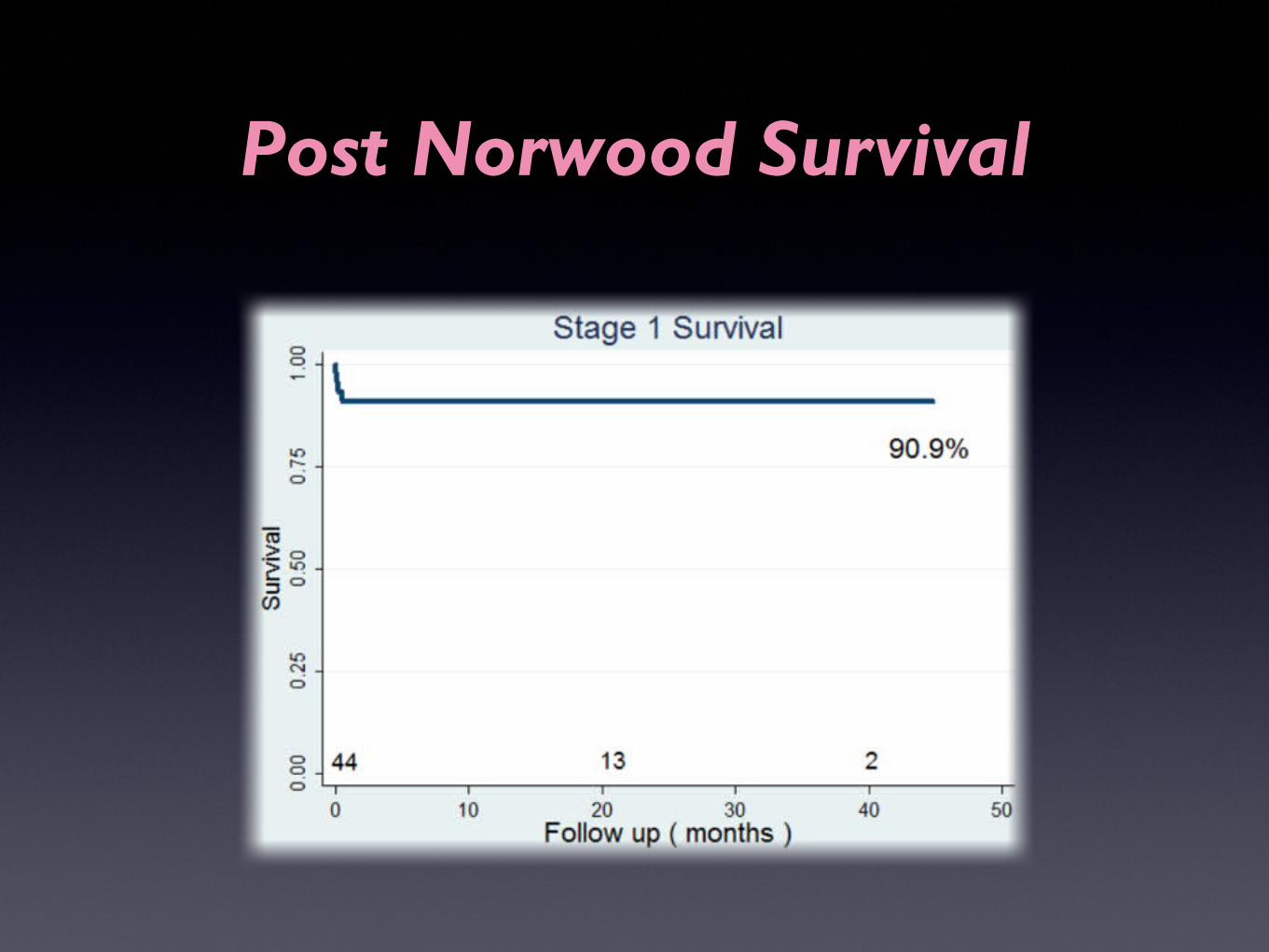
Interstage Procedures
% (N) Mean ± SD
Age (months) -- 7.6 ± 4.8
BPA plasty 5 (2) --
BT shunt 53 (21) --
Emergency BT shunt 5 (2) --
CoA Ballooning 7.5 (3) --
21/24 (88%) of completed BiV had interstage procedures
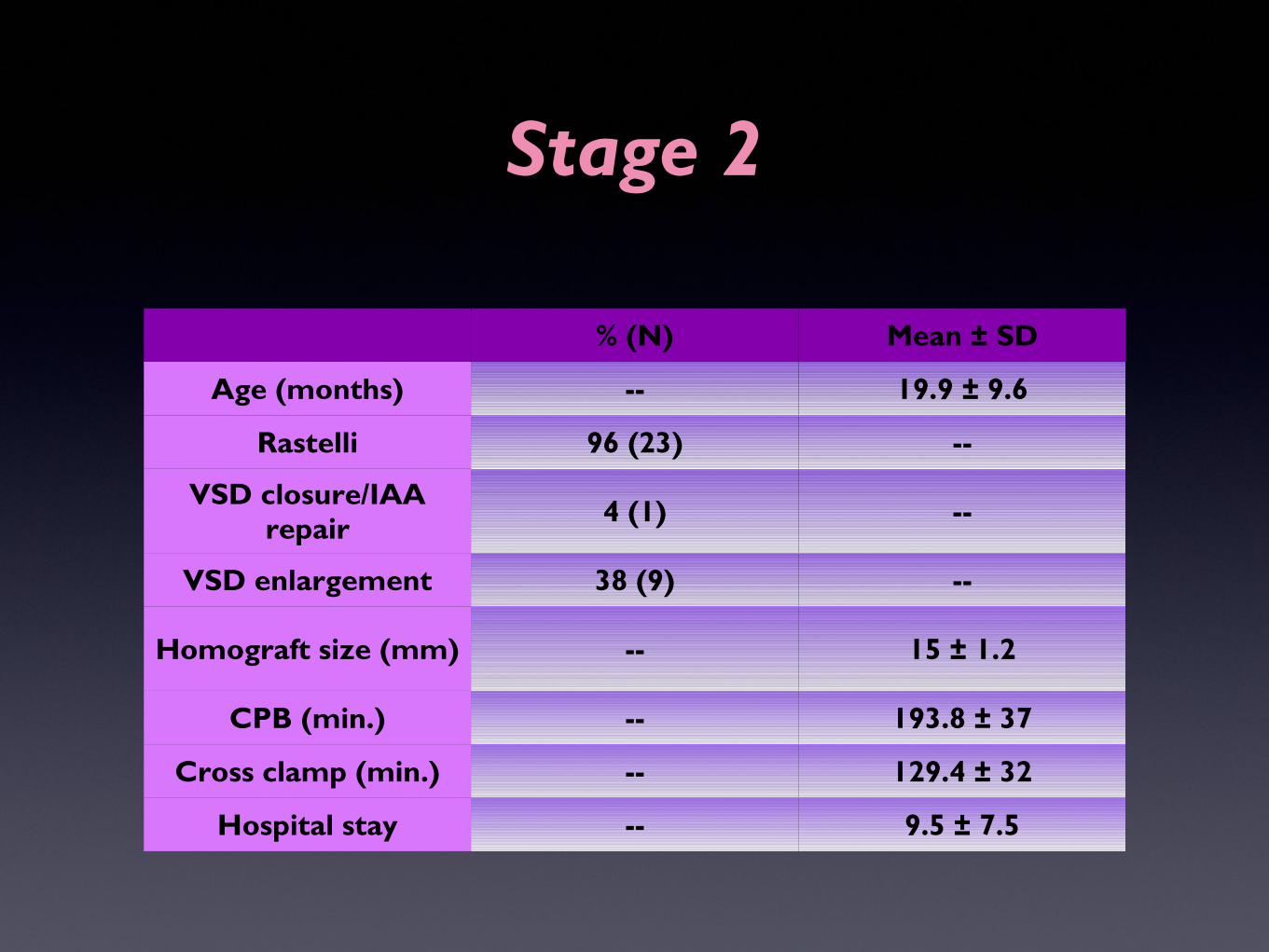
Stage 2
% (N) Mean ± SD
Age (months) -- 19.9 ± 9.6
Rastelli 96 (23) --
VSD closure/IAA repair 4 (1) --
VSD enlargement 38 (9) --
Homograft size (mm) -- 15 ± 1.2
CPB (min.) -- 193.8 ± 37
Cross clamp (min.) -- 129.4 ± 32
Hospital stay -- 9.5 ± 7.5

Post Rastelli Survival

Reintervention Post BiVRepairRepair

Reintervention Procedures
% (N)
RV-PA conduit replacement 45.8 (11)
Patch PA plasty 8.3 (2)
PA Stent 4 (1)
VSD enlargement 8.3 (2)
Pacemaker 4 (1)

Overall Survival

COX PH - Predictors of Overall Survival
Univariable HR Multivariable HR
HR p value HR p value
Term vs. Prem. 0.3 0.22 0.1 0.04
Birth wt. 0.6 0.36 -- --
Gender (M) 0.6 0.4 -- --
nSYN vs. SYN 0.1 0.01 0.06 0.02
Norwood vs. Hybrid
0.2 0.07 -- --
Sano vs. BT 1.02 0.9 -- --
ECMO 0.9 0.9 -- --

Total # AAI/CoA GeneticSyndrome
YasuiP vs S
EarlyMortality
BiV # OverallSurvival
Reintervention
Ann Arbor1999 20 90% N/A P (11)
S (9)5% 19 P (73%)
S (89%)N/A
Cincinnati2003 8 87% N/A S 0% 6 100 33% (3y)
Philadelphia2006 21 29% 31% P 0% 21 95% 67% (10y)
Boston2006 17 80% 18% P 18% 17 82% 63% (3y)
Birmingham, UK2007 16 75% 31% P 19% 16 46% 80% (5y)
Riyadh, KSA2010 14 79% N/A P (13)
S (1)21% 14 79% surg. 43%
(5y)
Atlanta2012 21 81% 48% P (6)
S (15)0% 21 nSYN (100%)
SYN (65%) 79% (3y)
Current Study
44 100% 52% S 9% 24 nSYN (86%)SYN (43%) 46% (6y)

Conclusion
• Staged BiV repair for complex LVOTO,VSD & AAO is safe, reproducible, and sometimes necessary.
• It allows for a bigger size RV-PA conduit at the time of completion, delaying the need for subsequent interventions.
• Genetic syndromes and prematurity are significant negative predictors of long term survival.

Thank You