
Staged Biventricular Repair for Neonates with Left
Ventricular Outflow Obstruction, Ventricular Septal
Defect, and Aortic Arch Obstruction
Mohammad Shihata, Chawki Elzein, Sujata Subramanian, and Michel Ilbawi
Neonatal LVOTO
• The vast majority of neonates with LVOTO suitable for biventricular repair are managed with balloon or to a lesser extent surgical aortic valvuloplasty.
• The study population comprises a small subset of the neonatal spectrum of LVOTO ( < 4% of the CHSS LVOTO inception cohort from 29 centers, (n=1217, 1994 - 2008).

Complex Neonatal BiV Repair
• If the native LVOT cannot be used as the sole systemic outflow, it needs to be :
• Replaced: Ross ± Konno
• Augmented: Yasui; primary or staged ( Norwood/Rastelli )
• Bypassed: LV to DAo conduit

Neonatal Ross/Konno
• Neonatal Ross±Konno operation is associated with high mortality especially if combined with an arch repair; 33% - 67%. ( CHSS and STS-CHD )
• In the CHSS LVOTO cohort the Ross group had a 40% failure rate (conversion to SV or Transplant).

Staged vs. Primary Yasui
• For the last decade, no one approach has been clearly superior.
• Primary Yasui is associated with the need for early reintervention.
• A staged approach may be necessary in borderline cases.

Study Population

Patient Characteristics% (N) Mean ± SD Min. Max.
Gestational age (wk.) -- 37 ± 2.4 30 41
Preterm 23 (10) -- -- --
Gender (F) 43 (19) -- -- --
Weight (kg) -- 2.9 ± 0.63 1.6 3.9
BSA (m ) -- 0.19 ± 0.03 0.13 0.24
IAA-B 70.5 (31) -- -- --
CoA 29.5 (13) -- -- --
VSD 100 (44) -- -- --
Aortic Stenosis 88.7 (39) -- -- --
Aortic Atresia 11.3 (5) -- -- --
AV annulus (mm) -- 3.3 ± 0.8 1.5 5
AV ( z score ) -- - 5.9 ± 1.9 -10.3 -3.1
Borderline LV 16 (7) -- -- --
Genetic Syndrome 52.2 (23) -- -- --
2

Stage 1
% (N) Mean ± SD Median
Age (d) -- 11.7 ± 9.6 8
Norwood BT 45 (20) -- --
Norwood RV PA 48 (21) -- --
Hybrid 7 (3) -- --
CPB (min.) -- 135 ± 46 120
Cross Clamp (min.) -- 65.5 ± 26 59
Selective Perfusion (min.)
-- 38.2 ± 13.6 36
ECMO 9.1 (4) -- --
Ventilation (d) -- 6 ± 1.5 6
ICU stay -- 11.9 ± 4 11.5
Hospital stay (d) -- 36.3 ± 56.7 21
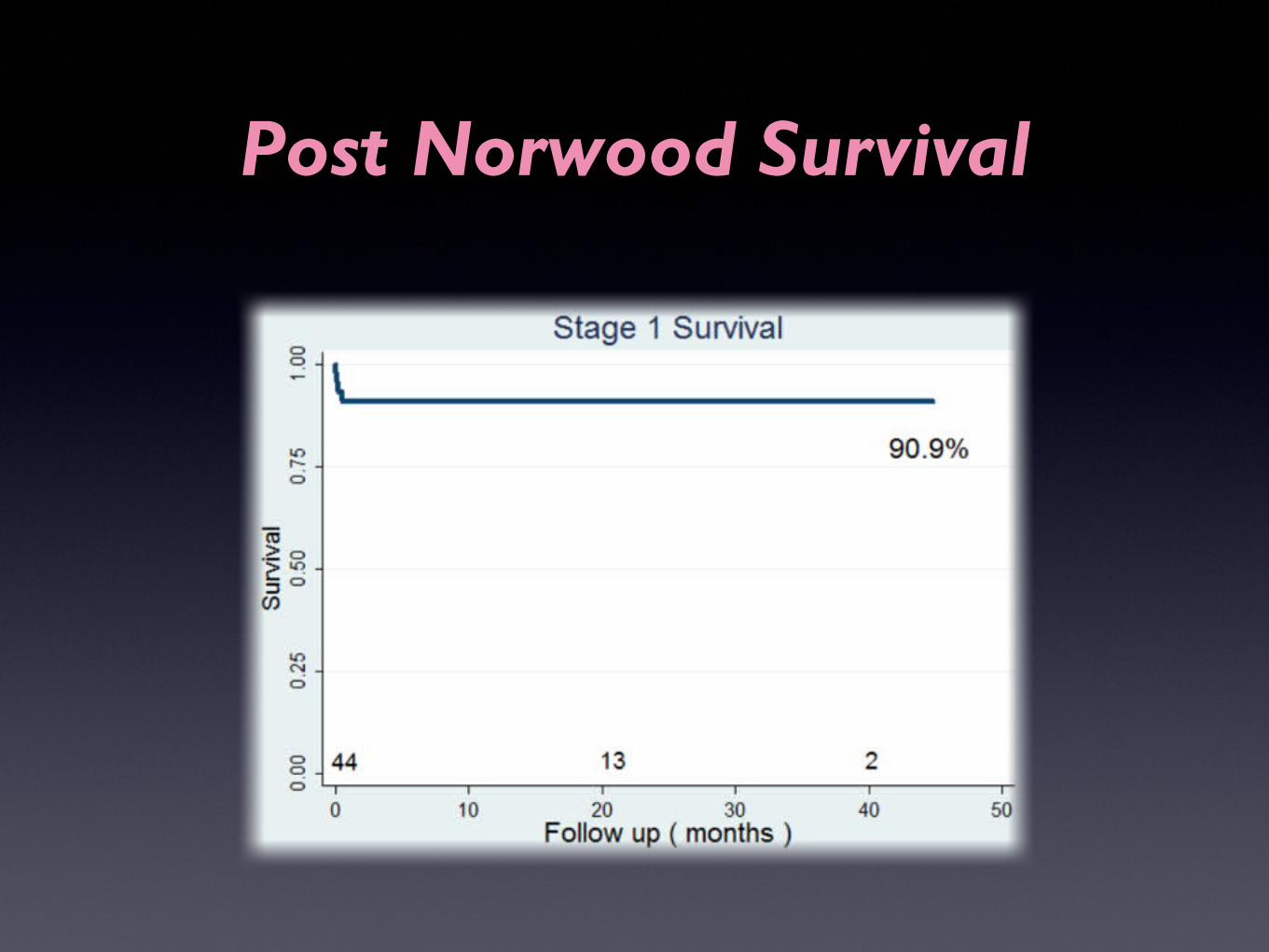
Post Norwood Survival

Interstage Survival
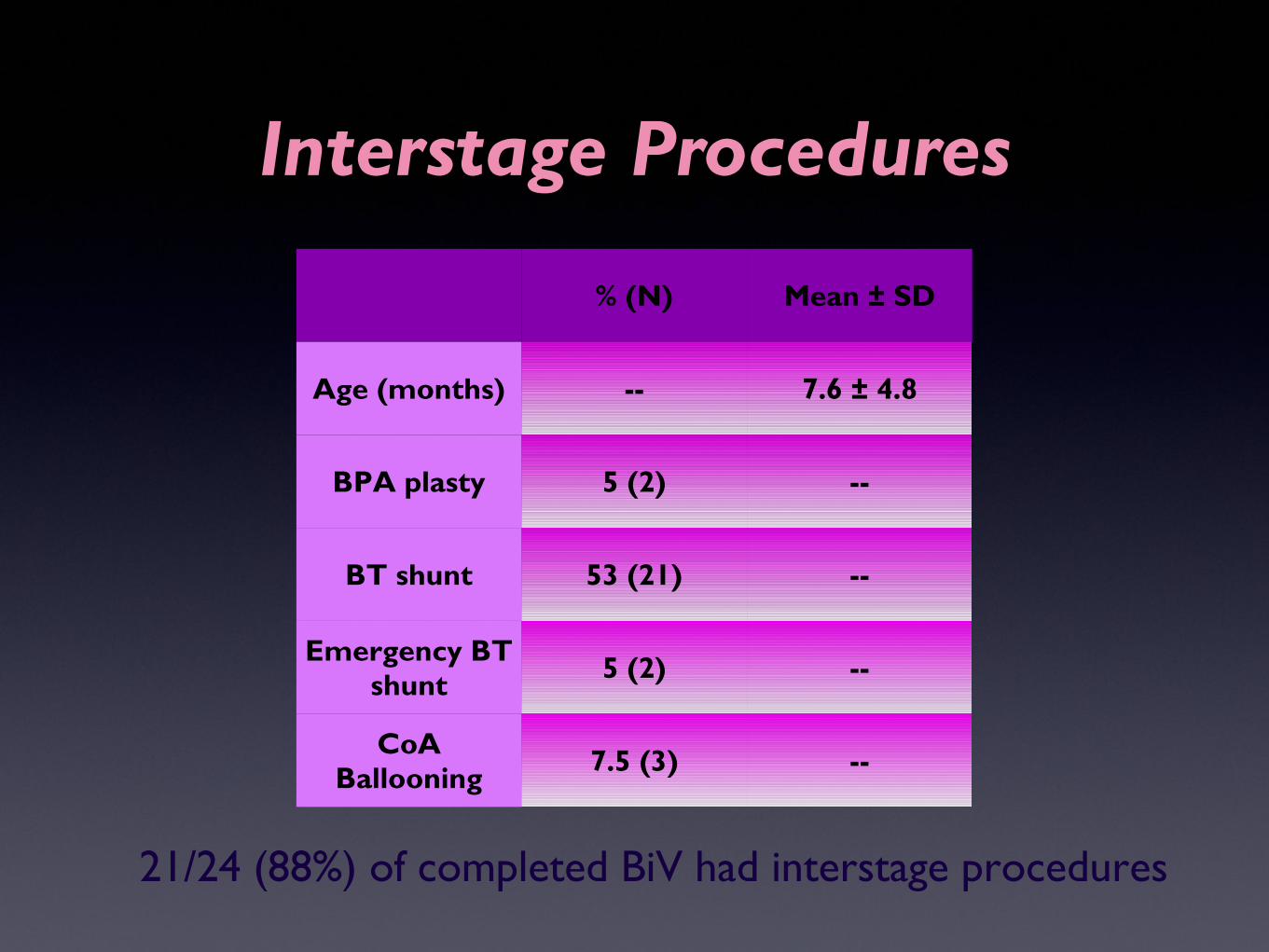
Interstage Procedures
% (N) Mean ± SD
Age (months) -- 7.6 ± 4.8
BPA plasty 5 (2) --
BT shunt 53 (21) --
Emergency BT shunt 5 (2) --
CoA Ballooning 7.5 (3) --
21/24 (88%) of completed BiV had interstage procedures
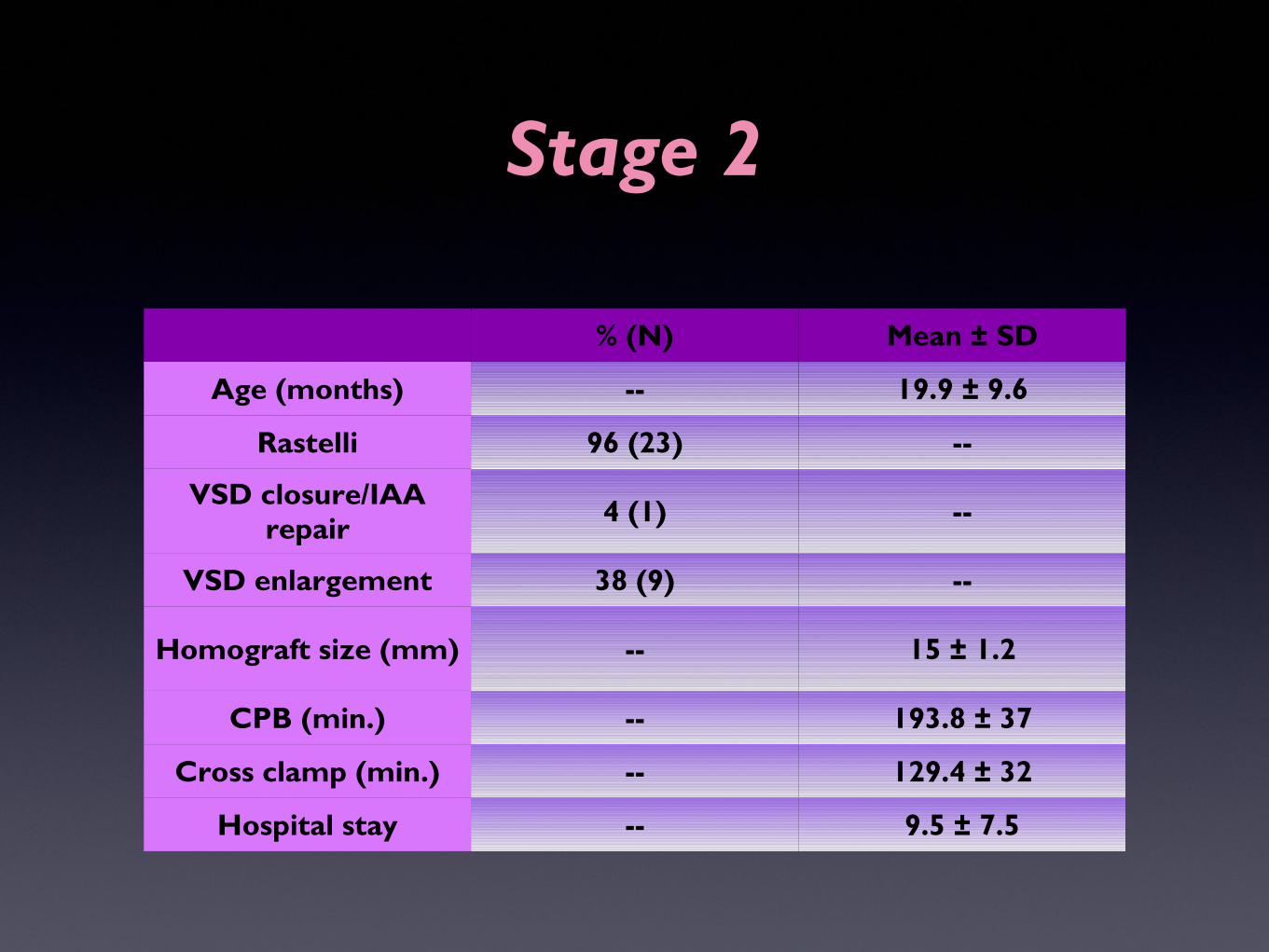
Stage 2
% (N) Mean ± SD
Age (months) -- 19.9 ± 9.6
Rastelli 96 (23) --
VSD closure/IAA repair 4 (1) --
VSD enlargement 38 (9) --
Homograft size (mm) -- 15 ± 1.2
CPB (min.) -- 193.8 ± 37
Cross clamp (min.) -- 129.4 ± 32
Hospital stay -- 9.5 ± 7.5

Post Rastelli Survival

Reintervention Post BiVRepairRepair

Reintervention Procedures
% (N)
RV-PA conduit replacement 45.8 (11)
Patch PA plasty 8.3 (2)
PA Stent 4 (1)
VSD enlargement 8.3 (2)
Pacemaker 4 (1)

Overall Survival

COX PH - Predictors of Overall Survival
Univariable HR Multivariable HR
HR p value HR p value
Term vs. Prem. 0.3 0.22 0.1 0.04
Birth wt. 0.6 0.36 -- --
Gender (M) 0.6 0.4 -- --
nSYN vs. SYN 0.1 0.01 0.06 0.02
Norwood vs. Hybrid
0.2 0.07 -- --
Sano vs. BT 1.02 0.9 -- --
ECMO 0.9 0.9 -- --

Total # AAI/CoA GeneticSyndrome
YasuiP vs S
EarlyMortality
BiV # OverallSurvival
Reintervention
Ann Arbor1999 20 90% N/A P (11)
S (9)5% 19 P (73%)
S (89%)N/A
Cincinnati2003 8 87% N/A S 0% 6 100 33% (3y)
Philadelphia2006 21 29% 31% P 0% 21 95% 67% (10y)
Boston2006 17 80% 18% P 18% 17 82% 63% (3y)
Birmingham, UK2007 16 75% 31% P 19% 16 46% 80% (5y)
Riyadh, KSA2010 14 79% N/A P (13)
S (1)21% 14 79% surg. 43%
(5y)
Atlanta2012 21 81% 48% P (6)
S (15)0% 21 nSYN (100%)
SYN (65%) 79% (3y)
Current Study
44 100% 52% S 9% 24 nSYN (86%)SYN (43%) 46% (6y)

Conclusion
• Staged BiV repair for complex LVOTO,VSD & AAO is safe, reproducible, and sometimes necessary.
• It allows for a bigger size RV-PA conduit at the time of completion, delaying the need for subsequent interventions.
• Genetic syndromes and prematurity are significant negative predictors of long term survival.

Thank You
Recommended

















