Embed Size (px)
Citation preview

Cytopathology of metastatic neoplasiaDr. Akshay AgarwalModerator: Dr. Hoogar M. B.

Overview Metastatic neoplasia in lymph node Metastatic neoplasia in lung Diagnosis of primary and secondary
lymphomatous effusions

Lymph node metastasis FNAC Imprint cytology Frozen










Microacinar patternProstate, NEC, Thyroid

MucinousBreast, ovary, pancreas


Papillary patternThyroid, ovary, breast

Breast carcinoma Diffuse infiltration involves airways Better differentiated tumors may be
recognized by its cohesive clusters of small glandular cells, with relatively uniform nuclei and a smooth border to the cell group


Nuclei may be moulded but have a more regular chromatin pattern and better defined nuclear membranes than oat cell carcinoma cells
Presence of intracytoplasmic mucin vacuoles favours a breast origin

For poorly differentiated tumors ER/PR S100 CEA

Colorectal carcinoma Palisaded columnar cells with oval
nuclei and apical mucin secretion Cytoplasmic border of the cell group
tends to be linear Cavitatory necrosis


Renal Cell Carcinoma Predeliction for infiltrating mucosal
surfaces. Pleomorphic malignant cells with round
eccentric nuclei, prominent nucleoli and abundant finely vacuolated cytoplasm
Eosinophilic basement membrane material
Fibrovascular papillary cores


Melanoma Free cell pattern Pleomorphic nuclei with prominent
nucleoli, presence of duble nuclei and spindle cell forms
Melanin may or may not be seen Irregular blue-green on MGG And Brown on PAP




Lymphoma NHL, most likely high grade follicular
lymphoma N:C ratio high, narrow blue rim of
cytoplasm with prominent nucleoli HL, lobulated nuclei with macronucleoli,
associated with eosinophils, histiocytes and lymphocytes


Sarcoma Pleomorphic malignant cells with
spindle cell forms, giant cells and vascular cell sheets


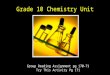
Basic First Line IHC Panel for Detection of Primary Site in Metastasis



mimics Pleomorphic adenoma
Submandibular LN Atypia in epithelial cells
Warthin’s Tumor Lymphoid cells Necrotic debris and epithelial cells

Hashimoto’s Thyroiditis Reactive lymphoid cells Bizarre cytology with hurthle cells
Benign epithelial inclusions Degenerative atypia in branchial cysts

Lung Metastasis Some organs such as the lungs and the
lymph nodes are more commonly affected by metastases than by primary neoplasia and so knowledge of advances is important.

Cytology of metastatic neoplasia in the lung Brushings or sputum Wider range is accessible with FNAC Breast and colorectal carcinomas Prostatic, renal, bladder and head and
neck carcinoma As well as melanoma, lymphoma,
testicular tumours and sarcomas

The diagnosis of metastasis can usually be established by a combination of the cytological appearance, clinical history and pattern of metastasis
IHC may be helpful, but requires cell blocks.

Patterns of spread

Cannon-ball / miliary Colorectal Renal Melanoma Sarcoma Ovarian Medullary carcinoma – thyroid

Diffuse parenchymal infiltration

Lymphangitic Lung and breast carcinoma, lymphoma
Intravascular GIT, liver, Choriocarcinoma
Lepidic Well differentiated AdenoCa of prostate
and pancreas

Mimics of lung cancer

Solitary Renal and colorectal carcinoma,
melanoma, sarcoma Endobronchial
Renal and colorectal carcinoma, sarcoma

Cytological patterns suggestive metastasis High index of suspicion when malignant
cells do not conform to the usual spectrum of appearances in lung cancer.
Final diagnosis always requires clinicopathological correlation and ancillary tests.

Diagnosis of 1o and 2o lymphomatous effusions Majority are secondary Can occur in NHL T/B cell type HL Late manifestation of systemic
lymphomas Pleural fluid in the setting of a
mediastinal or pulmonary mass

Primary Lymphomatous Effusions Lymphomas presenting as primary
pleural effusions are rare. Most are
DLBCL Follicular Lymphoma Small lymphocytic lymphoma
Majority are B cell Phenotype Pleural thickening with mediastinal
lymphadenopathy

Body cavity based NHL that occurs exclusively in HIV positive patients
Pleural / pericardial / peritoneal in the absence of solid tumor masses.
Throughout remain confined to the body cavity.

Morphologically, Large cell Immunoblastic Anaplastic
Abundant amphophilic or basophilic cytoplasm, bizarre cells with irregular nuclei and RS like cells

EBV and HHV-8 associated Diagnosis based on IHC
CD30, CD38, EMA positive Associated with castleman’s syndrome Extremely poor prognosis 2-4 months survival

PEL can be distinguished from secondary body cavity lymphomas by:1. Almost exclusive involvement of body
cavity2. Pleomorphic morphology3. IHC4. HHV-8

Pyothorax-associated Lymphoma Rare lymphomas, occur in setting of long-
standing inflammation of the pleura Underlying cause of chronic inflammation
such as TB, IL-6 associated 20-50 years after initial pleural injury Exclusively in the pleura Not associated with Immunosuppression

Morphology resemble PEL, Immunoblastic Anaplastic Bizarre cells
Do not express pan-B cell markers EBV positive




Conclusion Identification of metastatic diseases in
crucial to upstage the tumor Preliminary diagnosis should follow
thorough search of primary site IHC is mandatory for confirmation and
typing Detailed history should be available