Embed Size (px)
Citation preview


Maxillary Sinus
Dr. Ahmed M. Adawy Professor Emeritus, Dep. Oral & Maxillofacial Surg.
Former Dean, Faculty of Dental MedicineAl-Azhar University

Paranasal SinusesThere are a total of four paired sinuses, namely; frontal, ethmoidal, maxillary and sphenoid sinuses. They form the various boundaries of the nasal cavity. These sinuses are essentially mucosa-lined airspaces within the bones of the skull

Maxillary Air Sinus Anatomy and physiology
Maxillary sinus, also known as antrum of Highmore. is a hallow cavity lies chiefly within the body of the maxilla. The maxillary sinus is pyramidal in shape with its base at the naso-antral wall and its apex in the root of the zygoma. In the adult, the upper wall or roof is thin and situated under the orbit. The floor of the sinus is the alveolar process of the maxilla. Medially, the nasal wall separates the sinus from the nasal cavity. The nasal cavity contains the outlet from the sinus through the ostium which is situated beneath the roof of the antrum. This situation precludes the possibility of good drainage
(1)

The nerve supply is from the maxillary branch of the 5th cranial nerve. The posterior superior alveolar branch supplies the lining mucosa of the sinus. Its blood supply is derived from the infraorbital artery, a branch of the maxillary artery. The adult maxillary sinus averages 34 mm in antero-posterior direction, 33 mm in height, and 23 mm in width. Its volume is approximately 15 cc. The sinuses are lined by respiratory epithelium, a mucous secreting, pseudo-stratified, ciliated columnar epithelium and periosteum. The cilia and mucus are necessary for drainage of the sinus. Proper ciliary function is especially important because the direction of drainage is against the pull of gravity
Maxillary Air Sinus Anatomy and physiology

Pneumatization of maxillary sinus, though generally complete in adolescence, may still increases during adulthood with further development into the alveolar process especially when posterior maxillary teeth are lost prematurely. In such instance, the antral cavity may be near to the crest of the ridge. The roots of the maxillary second bicuspid, first molar, and second molar are the most frequently involved
Maxillary Air Sinus Anatomy and physiology

Function of paranasal sinuses
The function of paranasal sinuses is: Give resonance to the voice Act as reserve chambers to warm the inspired air. Reduce the weight of the skull. Several anatomic and physiologic features obstruct the flow of drainage from the sinuses thus precipitating infection. These are:
Inadequate anatomic openingsObstructive polypsSeptal deviationHyperplasia of the turbinate

Odontogenic maxillary sinusitisThe intimate anatomical relation of the upper teeth to the maxillary sinus promotes the development of odontogenic infection into the maxillary sinus. Recently, up to 30-40% of chronic maxillary sinusitis cases have been attributed to odontogenic cause . Sinusitis can be broadly defined as inflammation of one or more of the paranasal sinuses. Maxillary sinusitis occurs when the Schneiderian sinus membrane is violated by conditions such as infections of the maxillary posterior teeth, pathologic lesions of the jaws and teeth, maxillary trauma, or by iatrogenic causes such as dental and implant surgery complications and maxillofacial surgery procedures in the posterior maxillary region
(2)

Classic symptoms suggestive of an odontogenic source can include sinonasal symptoms such as unilateral nasal obstruction, rhinorrhea, and/or foul odor and taste . Headaches, unilateral anterior maxillary tenderness and postnasal drip, may be additional symptoms . Tooth ache is present in only 29% of the patients Generally, sinusitis is classified as:Acute when symptoms last less than 4 weeksSubacute when symptoms last 4 to 8 weeksChronic when symptoms last longer than 8 weeksRecurrent when three or more acute episodes a year
Odontogenic maxillary sinusitis Clinical features
(3)
(4)(5)

Odontogenic maxillary sinusitis Diagnosis
Clinical ExaminationPalpation for tenderness over the lateral wall of the sinus. Transillumination of the sinuses is an additional diagnostic test. The light source is placed over the infraorbital rim, in a darkened room and light transmission is observed through the hard palate. Compared with the sinus of the opposite side, the involved sinus shows decreased transmission of light due to accumulation of fluids, debris, pus and thickening of the sinus mucosa.

Radiographic ExaminationsRadiographic examination is an essential aid for the study of pathologic conditions of the maxillary sinus. Interpretation of radiographs is not difficult. The findings in the normal antrum are those to be expected of a rather large air filled cavity surrounded by bone and dental structures. The body of the sinus should appear radiolucent and should be outlined in all peripheral areas by a well demarcated layer of cortical bone.
Odontogenic maxillary sinusitis Diagnosis

Radiographic ExaminationIt is helpful to compare one side to the other when examining the radiograph. There should be no evidence of thickened mucosa on the bony walls (usually indicative of chronic sinus disease), nor air filled levels caused by accumulation of mucus, pus or blood, or foreign bodies. Complete opacification of the maxillary sinus may be caused by the mucosal hypertrophy and fluid accumulation of sinusitis, filling with blood secondary to trauma, or by neoplasia.Dental pathologic conditions such as cysts or granulomas may produce radiolucent lesions that extend into the sinus cavity

Panoramic radiograph is particularly useful for evaluation of the degree of pneumatization of maxillary sinus and its relationship to the roots of maxillary teeth

Mucous retention cyst, Lt maxillary sinus

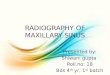
Water’s (occipito-mental) projection. Rt. side maxillary sinusitis. Please note the “fluid level”

Water’s projection, showing complete opacification of the Rt. maxillary sinus

CT scan - coronal section, carious maxillary first molars with periapical lesions are associated with localized thickening of mucosa in both maxillary sinuses

Axial CT scan demonstrates a trimalar fracture involving the anterior and posterolateral walls of the left maxillary sinus and the zygomatic arch (arrows) Note partial opacification of the sinus

Although CT remains the gold standard in the diagnosis of maxillary sinus diseases due to its high resolution and ability to visualize detailed anatomy, MRI is best used to evaluate soft tissue structures, and can distinguish between inflammatory and malignant disease
(6)
MRI: T2 axial and coronal sections showing a large hypointense tumor mass in the left maxillary sinus

Complications associated with sinusitis
Although rare, complications of acute sinusitis can occur through direct, local extension. Clinical presentation may include facial edema, cellulitis, orbital, visual, and meningeal involvement

1. Elimination of the source of the infection 2. Amoxicillin is the first line of antibiotic choice. Purulent
material is submitted for culture and sensitivity testing 3.The result of the culture and sensitivity tests should be
evaluated and changes of the prescribed antibiotics should be made if indicated
4. Local and systemic decongestants are used to decrease mucosal edema and inflammation and to promote drainage
5. Contrary to acute form, chronic sinusitis do not respond will to long term antibiotics. Instead, corticosteroids are more efficacious
6. Surgical management may be indicated in cases refractory to medical treatment
Management

Caldwell-Luc operationIndications for the Caldwell-Luc operation:1. Retrieval of a root or tooth from the sinus2. Enucleation of odontogenic cysts or mucoceles from the sinus3. Removal of odontogenic tumor from the sinus4. Treatment of acute maxillary sinusitis resistant to medical therapy or showing evidence of extending beyond the sinus5. Treatment of chronic sinusitis6. Management of oroantral fistula 7. Repair of fractures of the antrum or zygoma

Caldwell-Luc operation comprises osteotomy of the anterior sinus wall and creation of artificial opening of the sinus into the inferior nasal meatus. The procedure is criticized as aggressive surgery with relatively high incidence of complications. Most important, the efficacy of inferior meatal antrostomy, is doubtful, as the mucociliary clearance remains directed toward the natural sinus ostium in the middle meatus. Further, opening of the sinus on its anterior wall has to be performed, which results in permanent defect of anterior maxilla, sclerosis of the antral walls and collapse of the sinus cavity
Caldwell-Luc operation
(7)

Caldwell-Luc operation

Because of less traumatic approach, lower rate of complications and better preservation of antral lining, functional endoscope sinus surgery has gained popularity for last decades against Caldwell-Luc procedure in treatment of chronic sinusitis of dental origin
Caldwell-Luc operation
(8)

Oroantral CommunicationsOroantral communications are rare complications of oral surgery. Extraction of maxillary posterior teeth is the most common cause. Maxillary cysts, benign or malignant tumors and trauma can be other causes. It must be emphasized that unlike the oro-antral communication, oro-antral fistula is characterized by the presence of epithelium arising from the oral mucosa and/or from the antral sinus mucosa that, if not removed, could inhibit spontaneous healing. Closing this communication is important to avoid food and saliva contamination that could lead to bacterial infection, impaired healing and chronic sinusitis.

The size of the fistula depends on the depth and range of the surgical stress. Defects less than 3 mm and without epithelialization might heal spontaneously in the absence of infections. In the latter case, infection must be cured before surgery to avoid impaired drainage. Communications wider than 5mm require surgical treatment.
Oroantral Communications

Buccal sliding flap , is usually employed for immediate closure of oro-antral communications. After cutting the communication edges, two vertical release incisions are made to provide a flap with dimensions suitable for closure of the antral communication. Mobilization of the flap is facilitated by horizontal releasing incision of the periosteum and by reduction of the alveolar bone height. The flap is then positioned over the defect by means of mattress sutures from the buccal flap to the palatal mucosa
Oroantral Communications(9)

Buccal sliding flap

Oro-antral fistulaIn most instances, patients who present with a chronic oroantral fistula not only require closure of the fistula but also require management of the inflammatory sinus disease that co-exists with the fistula. The most common cause of failure is insufficient control of maxillary sinusitis. For this reason, foreign bodies, infected and degenerated polypoid mucosa and infected bone should be removed. Functional endoscopic sinus surgery and Caldwell-Luc procedure are the most important surgical techniques used. Whatever, the used technique, excision of the epithelialized fistulas tract should be performed first

Oro-antral fistula

The most common surgical technique for the closure of an oroantral fistula is the buccal sliding flap. The advantage of the buccal flap procedure is that it allows the Caldwell-Luc operation and the closure of the oroantral fistula to be performed simultaneously if sinus disease is present. The disadvantage is that nearly 50% of patients experience permanent reduction of vestibular depth, and therefore needs for a vestibuloplasty
Oro-antral fistula

Rotated palatal pedicle full thickness flap based on greater palatine artery has been frequently used for closure of oro-antral fistula . In contrast to the buccal flap, palatal flap is more resilient, less prone to infection and does not lead to lowering of the vestibule. The blood supply of palatal flap is better than buccal flap and it is preferred in large and recurrent oroantral fistulas. The drawbacks of this technique include mild palatal surface denudation and the kink that occurs along the arch of rotation which may jeopardize the vascularity causing flap necrosis.
Oro-antral fistula
(10)

Rotated palatal pedicle flap

Various modifications of palatal flaps have been described for closure of oroantral fistulas. One modification is the Tunnel technique . The technique is characterized by leaving a band of tissue between the pedicle flap and the fistula on the palatal side. The pedicle flap is then tunneled under the bridge of tissue before closing the fistula. This reduce tension on the flap and help protect and stabilize it. In addition, because flotation and upsurge are minimized in the region of the mucoperiosteal flap, postoperative discomfort can be relieved.
(11)

Tunnel Technique for the Closure of Oroantral Fistula

The palatal island flap is another modification that is used to correct large palatal defect involving soft palate. Sub mucosal connective tissue pedicle flap is an additional modification by which the epithelial layer is used to cover the bone surface at the donor site
Oro-antral fistula

Buccal fat pad is another alternative that can be used to close medium to large sized defect, particularly when the fistula is located at the posterior region of the maxilla. The tongue flap, whether anterior, lateral or posterior based, can also be used to correct ore-antral fistulae with large bony defect. Various materials like gold foil, gold plate, tantalum plate, soft polymethylmethacrylate and bone graft have been used to repair oro-antral fistula with varying degrees of success
Oro-antral fistula

Sinus Lift Procedure
Sinus lift, sometimes called a sinus augmentation is indicated when there is no enough bone in the upper jaw (atrophic), or when the sinus is too close to the jaw, and there is a need for dental implant to be placed. Elevation of the maxillary sinus floor is an option in solving this problem. Various surgical techniques have been presented to enter the sinus cavity elevating the sinus membrane and placing bone grafts. The use of autogenous bone grafts are considered the gold standard due to their maintenance of cellular viability and osteogenic capacity
(12)

To date, two main techniques of sinus floor elevation are in use: a two-stage technique with a lateral window approach, followed by implant placement after a healing period, and a one-stage technique using either a lateral or transalveolar approach. The decision to apply the one or the two-stage techniques is based on the amount of residual bone available and the possibility of achieving primary stability for the inserted implants
Sinus Lift Procedure

Dental implants after sinus lifting procedure, two years follow-up radiograph


1.Harold A. DeHaven Jr. Anatomy and Physiology of the Maxillary Sinus. in Clinical Maxillary Sinus Elevation Surgery. Kao DWK (Editor), Wiley-Blackwell,2014.2. Patel NA, Ferguson BJ. Odontogenic sinusitis: an ancient but under-appreciated cause of maxillary sinusitis. Curr Opin Otolaryngol Head Neck Surg ;20:24, 2012.3. Patel NA, Ferguson BJ. Odontogenic sinusitis: an ancient but under-appreciated cause of maxillary sinusitis. Curr Opin Otolaryngol Head Neck Surg ;20:24,2012. 4. Brook I. Sinusitis of odontogenic origin. Otolaryngol Head Neck Surg; 135:349,2006. 5. Longhini AB, Ferguson BJ. Clinical aspects of odontogenic maxillary sinusitis: a case series. Int Forum Allergy Rhinol; 1:409,2011.6. Fatterpekar GM, Delman BN, Som PM. Imaging the paranasal sinuses: where we are and where we are going. Anat Rec,291:1564,2008.7. Nemec SF, et al. Sinonasal imaging after Caldwell-Luc surgery: MDCT findings of an abandoned procedure in times of functional endoscopic sinus surgery. Eur.J Radio. 70,31,2009.
References:

8. Andric, M. Endoscopic surgery of the maxillary sinuses in oral and maxillofacial surgery practice: a literature review. Hellenic Archives of Oral & Maxillofac Surg. 2, 57.2010.9. Rehrmann A. A method of closure of oroantral perforation. Dtsch Zahnarztl Z.; 39:1136,1936.10. Ashley R.E. A Method of closing antroalveolar fistula. Ann.OtoI.Rhino. Laryngo. 48: 632,1939. 11. Sakakibara A, et al. Tunnel Technique for the Closure of an Oroantral Fistula with a Pedicled Palatal Mucoperiosteal Flap. J. Maxillofac. Oral Surg. 14:868,2015. 12. Pjetursson BE, et al. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation Part I: Lateral approach. J Clin Periodontol. 35 : 216,2008.
References: