Embed Size (px)
Citation preview
Leptospirosis: A Neglected Infectious Disease In The Tropics
Fadel Muhammad Garishah, BSc
Department of General Medicine
Faculty of Medicine Diponegoro University
Overview of Leptospirosis
Zoonotic disease caused by Leptospiral pathogens
Systemic infection characterized by fever, thrombocytopathy, liver failure, respiratory failure and acute tubular necrosis
An overlooked infectious disease due to poorly availability of diagnostic tools
Relatively simple medication

Important to Understand
Leptospirosis typically presents as a nonspecific, acute febrile illness characterized by fever, myalgia, and headache and may be confused with other entities such as influenza and dengue fever.
Endemic regions, professions, history of possible exposures affect Clinical Judgement

Epidemiology
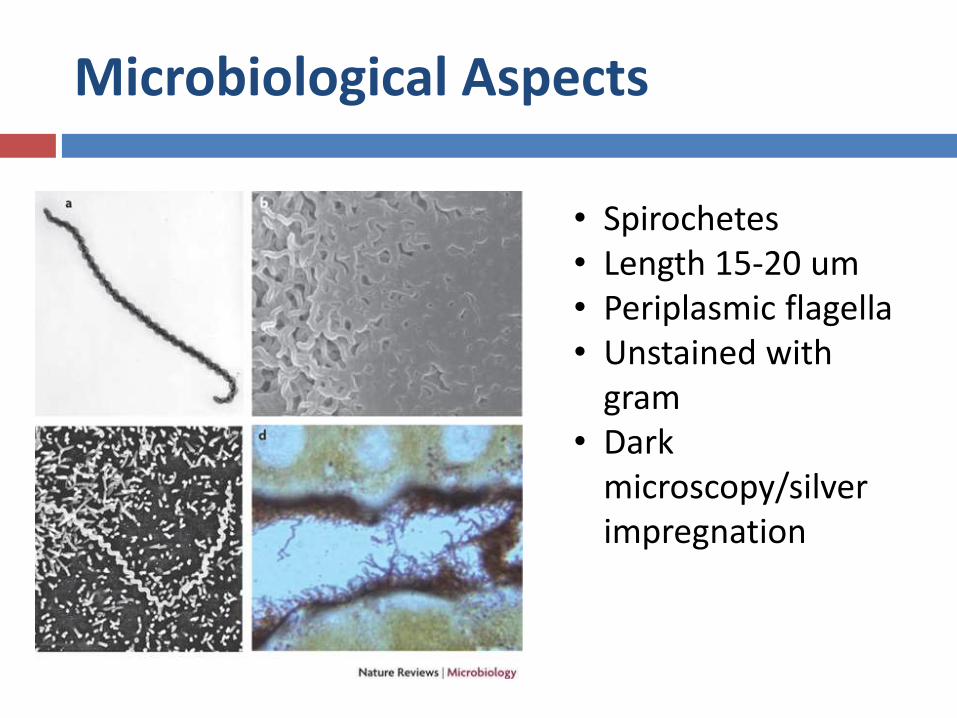
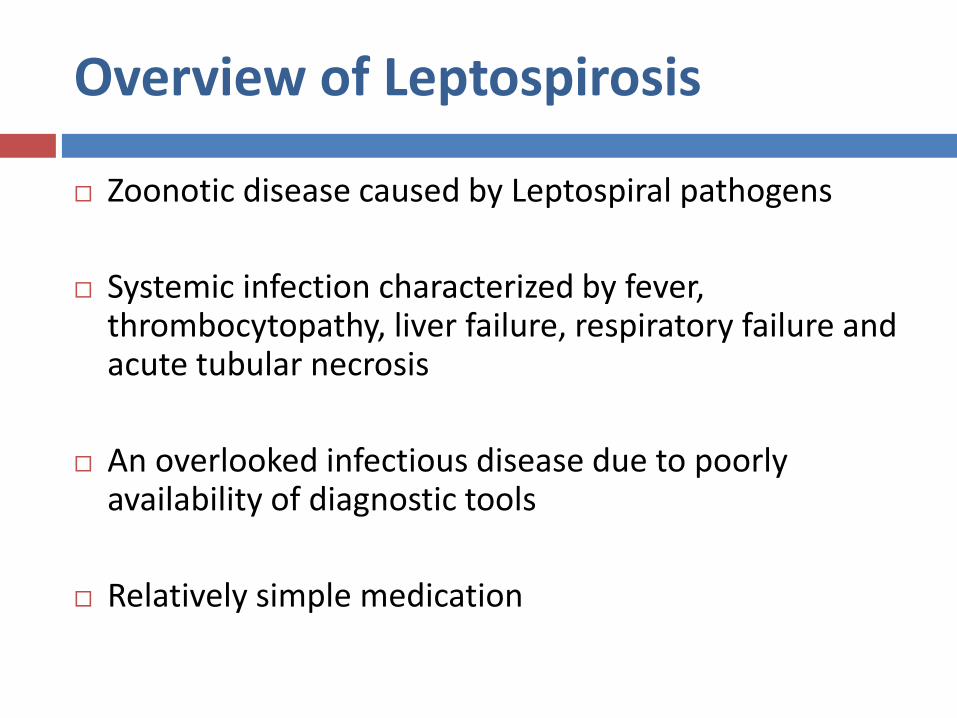
Microbiological Aspects
• Spirochetes• Length 15-20 um• Periplasmic flagella• Unstained with
gram• Dark
microscopy/silver impregnation
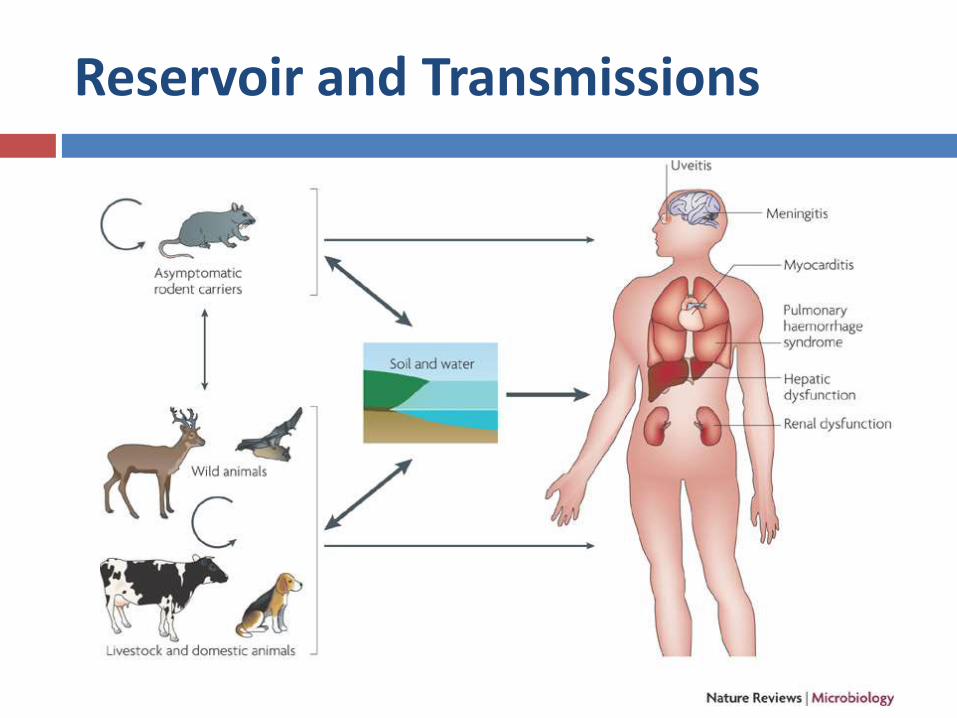
Reservoir and Transmissions
Transmission
transmitted to humans by direct contact with reservoir animals
by exposure to environmental surface water or soil that is contaminated with their urine
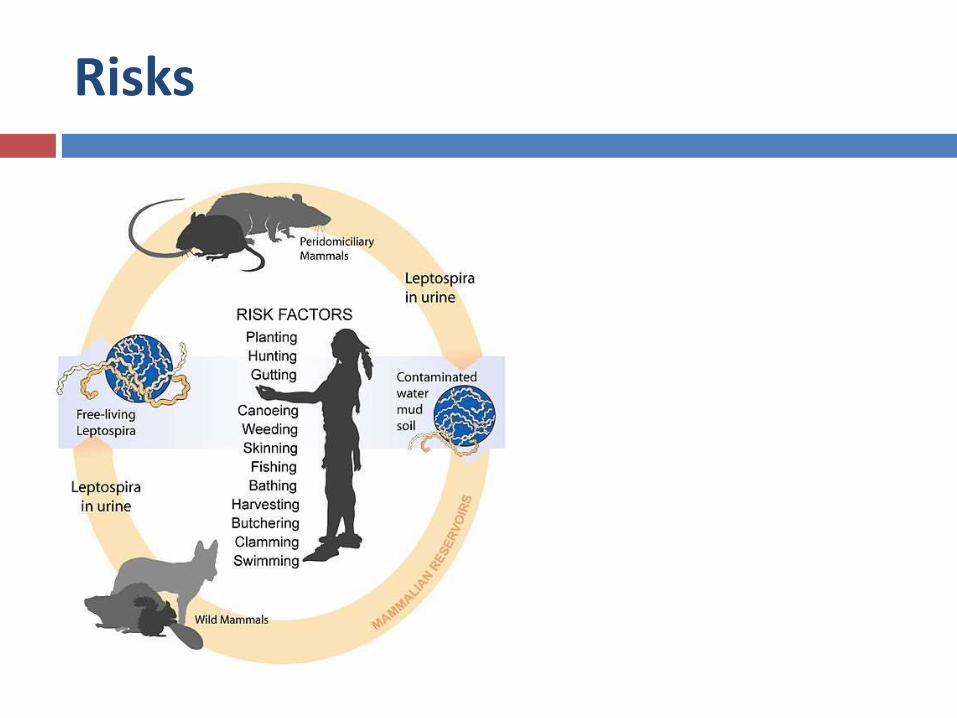
Risks
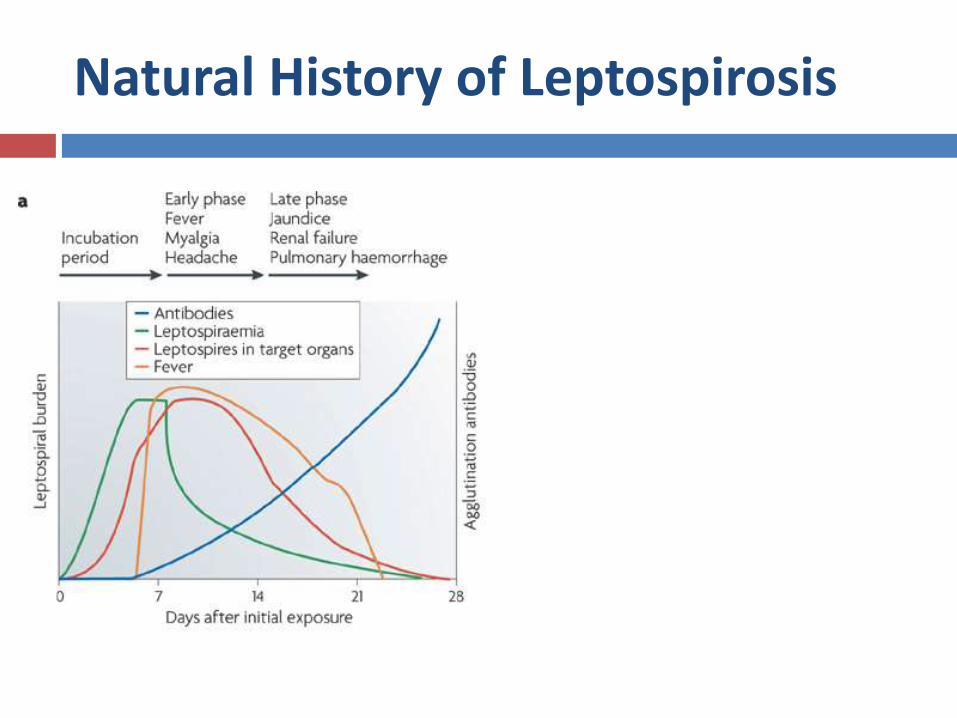
Natural History of Leptospirosis
Pathobiology
Patients progressing to multisystem organ failure have widespread hematogenous dissemination of pathogens.
Nonoliguric (high output) renal dysfunction should be supported with fluids and electrolytes.
Elevated bilirubin levels are due to hepatocellular damage and disruption of intercellular junctions between hepatocytes, resulting in leaking of bilirubin out of bile caniliculi.
Hemorrhagic complications are common and are associated with coagulation abnormalities.
Severe pulmonary hemorrhage syndrome due to extensive alveolar hemorrhage has a fatality rate of >50 %.
Clinical Manifestations
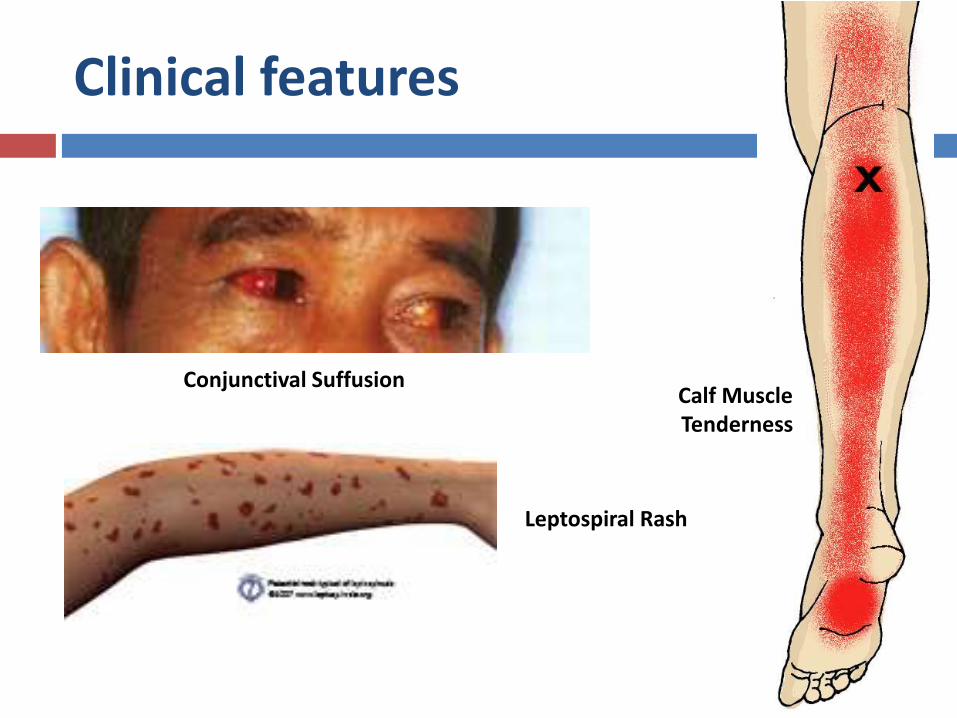
Clinical features
Conjunctival SuffusionCalf MuscleTenderness
Leptospiral Rash

Diagnostic Terms
Suspect case
Probable case
Confirmed case
Suspect Case
Acute fever > 38,5C; with/out severe headache
Myalgia
Prostration
Conjunctival suffusion
History of exposure!
Probable case
Calf tenderness
Cough with/without hemoptysis
Jaundice
Hemorrhagic
Meningism
Anuria/oliguria/proteinuria
Breathlessness
Cardiac arrythmia
Skin rashes
With Positive Rapid IgM Test or MAT 200/single sample
Diagnostic Tools
Dark field microscopy/Ink stain
Microscopic Agglutination Test
ELISA
PCR
Cultur EMJH/Fletcher’s Medium
Confirmed case
Suspect/Probable Case
With isolation of Leptospira spp.
PCR positive
Seroconversion of MAT 4 folds
MAT titre 400/single sample

Chemotherapeutics
Mild
Doxycyline 2 x 100 mg for 7 days
Amoxicillin/Ampicillin 2 g/day for 7 days
Severe Case
Penicillin G 2 MU IV/6hours for 7 days
Ceftriaxon 1 g/day for 7 days
Supportive managements
Renal (Dialysis)
Hepatic
Pulmonary (Ventilators)
Hemorrhages (Transfusions)