Embed Size (px)
Citation preview

Implementation of International Slide Review Criteria for
Improving the Efficiency of the Haematology Laboratory

Review Article
AIM
Reduction in the number of samples requiringmicroscopic blood film review and validation of the slidereview criteria suggested by the international consensusgroup in haematology led by P.W. Barnes, et al. [1].
Materials and Methods
The study was conducted in the haematology laboratoryof Apollo hospitals Bangalore. The period of study wasfrom1st January 2009 to 29th January 2009. 1000 sampleswere selected randomly from both out patient and inpatientpopulations. The samples were run on the haematologyanalyser Beckman Coulter ACTi 5 Diff AL according to thelab Standard Operating Procedure. Blood films wereprepared and stained with Leishmans stain. The stainedslides were reviewed for manual morphological analysisbya senior technologist and a pathologist [2,3]. The peripheralsmears were categorized as positive or negative accordingto the criteria laid down for a positive finding (Table 1) [1].Manual WBC differential count [2,3] was done only whenthe machine differential count was abnormal, abnormal celltype, or vote out. The data released from the haematologyanalyser and the smear review was documented in a spreadsheet which included the sample identification, consensus
IMPLEMENTATION OF INTERNATIONAL SLIDE REVIEW CRITERIA FOR IMPROVINGTHE EFFICIENCY OF THE HAEMATOLOGY LABORATORY
Shabnam RoohiConsultant, Haematology & Clinical Pathology, Apollo Hospitals, 154/11, opp. I.I.M., Bannerghatta Road,
Bangalore 560 076, India.
In the present competitive era of health care delivery, there is a constant pressure on the laboratory to releasereports in the shortest possible time. Manual techniques, especially microscopic examination of stainedblood film have on the one hand complemented the automated analyser results to provide a comprehensivehematology report but on the other hand are time consuming, labour intensive and expensive. Thereforerelease of a comprehensive hemato-logy report in a short time and minimum expenditure, withoutcompromising on the quality is a challenge.
As the main complementary procedure to automated CBC is microscopic slide review, the decision as towhether slide review is necessary for each sample plays an important role in haematology laboratory costs,productivity and speed of reporting. Microscopic review by humans is done to provide information additionalto or missing from the analyser and is most commonly triggered by criteria for visual smear review applied toanalyser results. Each laboratory has developed its own criteria for action after an automated analysis ofblood sample. In our laboratory we followed a set of criteria for smear review after which about 45% of theCBC required smear review. Our objective was to reduce this number as much as possible withoutcompromising on patient care. A literature search revealed an international consensus group forhematology review on suggested criteria for action following automated CBC and WBC Differential analysis.This study was conducted based on the suggestions given in that article.
rule number triggered, number of rules triggered,instrument suspect flags, total number of suspect flagstriggered, positive slide review findings and total numberof slide review findings [1]. The data was analyzed by apathologist who compared the rules that were triggeredwith the peripheral smear findings. If a rule was triggeredand the peripheral smear revealed a positive finding thesample was graded as true positive. If a rule was triggeredand the smear did not show any positive finding then thesample was considered as false positive. If a rule was nottriggered and the smear showed a positive finding thesample was considered as false negative. If no rule wastriggered and the smear also did not show any positivefinding the sample was graded as true negative. The totalnumber of true positives, true negatives, false positive andfalse negatives were determined and their percentageswere calculated.
RESULTS
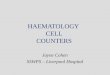
The total numbers of samples analyzed were 1000.These samples were run on Beckman coulter 5 partanalyser. Of the 1000 samples analyzed the true positivewere 226, true negative were 652, false positive were 118and false negative were 4 (Table 2 & Fig. 1).
Apollo Medicine, Vol. 7, No. 4, December 2010 286

Review Article
287 Apollo Medicine, Vol. 7, No. 4, December 2010
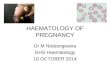
Of the 118 false positive samples some of them hadmore than one false positive finding and each false positiveresult was counted separately. The false positive resultswere mainly due to the machine generated suspect flagswhich included immature cells 43% false positive, atypicallymphocytes 28%, nucleated RBC 22%, large platelets 6%and monocytosis 1% (Fig 2).
The false negatives were only 4 and the machine failedto pickup atypical lymphocytes in all of them.
DISCUSSION
The results obtained in our laboratory were comparableto the results of the consensus group for standardization ofreview criteria for automated CBC and WBC differentialcounts. The comparison is given in Table 3.
The true positive rates were higher in our study whencompared to the consensus findings where as the falsenegatives were lower in our study and were statisticallyinsignificant. The false positive rate was marginally lowerin our study but was comparable to the findings of the
Table 1. Criteria for a positive smear [1]
Morphology 1. RBC morphology at either2+/moderate or greater.The only exception ismalaria, where any findingwill be considered apositive finding.
2. PLT morphology (giantplatelets) at 2+/moderateor greater.
3. Platelet clumps at > rare/occasional.
4. Dohle bodies at 2+/moderate or greater.
5. Toxic granulation at 2+/moderate or greater.
6. Vacuoles at 2+/ moderateor greater.
Abnormal cell types 1. Blast =12. Metamyelocyte >23. Myelocyte/promyelocyte =14. Atypical lymphocyte >55. NRBC (nucleated red
blood cells) =16. Plasma cells =1
Table 3. Comparison
ISLH [1] Apollo lab
Number % Number %
True positive 1483 11.2 226 23
True negative 8953 67.3 652 65
False positive 2476 18.6 118 12
False negative 386 2.9 04 0.4
Total number 13298 1000of samples
Fig 1 Truth table summary.
Fig 2 False positive analysisTable 2. Truth table summary
Number %
True positive 226 23%
True negative 652 65%
False positive 118 12%
False negative 04 0.4%
Total number of samples 1000

Apollo Medicine, Vol. 7, No. 4, December 2010 288
Review Article
consensus group. The false positive rate is largely due tothe instrument generated suspect flagging. The analyzersare intended to be used as screening devises and to flagsuspect abnormal samples for further review. They aredesigned to trigger the suspect flags to preferentially have ahigher rate of false positives so as to not miss potentiallyimportant abnormalities and thus minimize the number offalse negatives.
CONCLUSION
The 41 rules for slide review of automated CBC andWBC differential were validated for the 5 part haematologyanalyzer and were implemented for routine use in thehaematology laboratory of Apollo Hospitals Bangalore, afterthe necessary training of the personnel. The slide reviewrate significantly dropped from 45 to 28%.This lead to a
decrease in the average turn around time for CBC from3.45 hours to 2.1 hours after the implementation of theserules and therefore improving the productivity.
REFERENCES
1. P W Barnes, S L McFadden, S J Machin, E Simson. Theinternational consensus group for hematology review:Suggested criteria for action following automated CBCand WBC differential analysis. Laboratory hematology.2005; 11: 83-90.
2. S M Lewis, B J Bain, I Bates, editors. Dacie and LewisPractical Haematology. 10th ed. London: ChurchillLivingstone 2006;35, 80-110.
3. Henry’s Clinical Diagnosis and Management byLaboratory Methods. Richard A. McPherson, Matthew R.Pincus, editors. 21st ed. New Delhi: Elsevier 2007; 457-483.

Apollo hospitals: http://www.apollohospitals.com/Twitter: https://twitter.com/HospitalsApolloYoutube: http://www.youtube.com/apollohospitalsindiaFacebook: http://www.facebook.com/TheApolloHospitalsSlideshare: http://www.slideshare.net/Apollo_HospitalsLinkedin: http://www.linkedin.com/company/apollo-hospitalsBlog:Blog: http://www.letstalkhealth.in/