Embed Size (px)
DESCRIPTION
hiv and periodontium
Citation preview

HIV & PERIODONTIUM
1
Presented by
Dr. Dandu Sivasai Prasad
1st yr post graduate
Mamata dental college

CONTENTS Introduction
History
Epidemiology AIDS
CDC definition and classification of AIDS
Virus structure
Mode of transmission
Life cycle of HIV
Clinical features-WHO classification2

Contents…
Classification of oral lesions associated with HIV
Periodontal manifestations of HIV
Periodontal management of HIV infected patients
Diagnostic tests
Occupational exposure and Post-Exposure prophylaxis
Sterilization and precautions to be taken
Conclusion
References3

4
INTRODUCTION:

5
HISTORY:
1959- Scientists isolated earliest known case of AIDs
1978- Gay men in US, Sweden and Hetrosexuals in Tanzania and Haiti- Showed signs
1981, June 5th- CDC reported confirmed CMV and Candidal infection(LAV)
In 1982 july 27th, the term AIDs first used
In 1984, Robert Gallo discovered the HIV virus- HTLV-III

EPIDEMIOLOGY OF AIDS• As of 2012, approximately 35.3 million people are living with
HIV globally. Of these, approximately 17.2 million are men,
16.8 million are women and 3.4 million are less than 15 years
old. There were about 1.8 million deaths from AIDS in 2010,
down from 2.2 million in 2005
• Sub saharan africa is the region most affected. In 2010, 68%
(22.9 million) of all HIV cases.
• 66% of all deaths (1.2 million).6

EPIDEMIOLOGY OF AIDS…
• The total number of people living with HIV in India is
estimated at 2.4 million.
• 61% male and 39% female.
• The four high prevalence states of South India account for
57% of all HIV infections in the country. Andhra Pradesh-
500,000 cases; Maharashtra- 420,000 cases, Karnataka -
250,000 cases and Tamil Nadu-150,000 cases
• IDU-12.22% :MSM- 6.82% :FSW at 5.92%. HIV prevalence
amongst IDU, MSM and FSW is 14.92%, 10.31% and 9.48%
respectively
7

VIRUS STRUCTURE
8
P17
P24
P7

MODE OF TRANSMISSION:
• HIV detected in most body fluids including.
• Blood
• Semen
• Vaginal secretions
• Cerebrospinal fluid
• Breast milk
• Urine
9

MODE OF TRANSMISSION…
• Sexual contact
• Blood transfusion
• Needle sharing
• Perinatal transmission
• Intrauterine Postnatal
• Occupational exposure
• Organ transplantation
• Artificial insemination
10

LIFE CYCLE OF HIV
11

CDC SURVEILLANCE CASE CLASSIFICATION:
• 1982- “presence of oppurtunistic illness or malignancies
secondary to defective immunity in HIV+ individuals”
• 1993-“ inclusion of severe immunodeficiency as
definitive for AIDS”
12

AIDS patients have been grouped as follows, according
to the CDC Surveillance Case Classification (1993);
Category A - Acute symptoms or asymptomatic
diseases,.
Category B - Patients have symptomatic
Category C - Life-threatening conditions.
13

WHO classification of HIV-associated clinical disease CLINICAL STAGE 1 CLINICAL STAGE 2 CLINICAL STAGE 3 CLINICAL STAGE 4
Asymptomatic Unexplained moderate weight loss (<10)
Unexplained severe weight loss (> 10%), diarrhoea /persistent fever (longer than
one month)
Pneumocystis pneumonia
Persistent generalized lymphadenopathy
Recurrent upper RTI Persistent oral candidiasis Recurrent bacterial pneumonia
Herpes zoster Oral hairy leukoplakia Chronic herpes simplex infection
Angular cheilitis Pulmonary tuberculosis Oesophageal candidiasis
Recurrent oral ulceration Severe bacterial infections Extrapulmonary tuberculosis
Papular pruritic eruptions Acute necrotizing ulcerative stomatitis, gingivitis/periodontitis
Kaposi sarcoma /Lymphoma/Invasive cervical carcinoma
Fungal nail infection Unexplained anaemia (<8 g/dl ), neutropenia (< 0.5 x 109/l) and chronic
thrombocytopenia (< 50)
Cytomegalovirus infection
Central nervous system toxoplasmosis
HIV encephalopathy
Extra pulmonary cryptococcosis including meningitis
Disseminated non-tuberculous mycobacteria infection
Chronic cryptosporidiosis
Chronic isosporiasis
Disseminated mycosis
Atypical disseminated leishmaniasis
Symptomatic HIV-associated nephropathy or HIV-associated
cardiomyopathy

Classification and diagnostic criteria for oral lesions in HIV infection. 1993 revised
Group 1: Lesions strongly associated with HIV infection Candidiasis
Erythematous
Pseudomembranous
Hairy leukoplakia Kaposi’s sarcoma Non-Hodgkin’s lymphoma
Periodontal disease Linear gingival erythema Necrotizing (ulcerative) gingivitis Necrotizing (ulcerative) periodontitis
15

Group 2: Lesions less commonly associated with HIV
infection:
Bacterial infections like
Mycobacterium avium - in tracellulare
Mycobacterium tuberculosis
Melanotic hyperpigmentation
Necrotizing (ulcerative) stomatitis
Salivary gland disease
Thrombocytopenic purpura
Ulceration not otherwise specified
Viral infections
Dry mouth due to decreased salivary flow rate
Unilateral or bilateral swelling of major salivary glands
16

• Group 3. Lesions seen in HIV infection
Bacterial infections like
Actinomyces israelii
Escherichia coli
Klebsiella pneumoniae
Cat-scratch disease
Drug reactions (ulcerative, erythema multiforme,
lichenoid, toxic epidermolysis)
Epithelioid (bacillary) angiomatosis
17

Fungal infection other than candidiasis
-Cryptococcus neoformans
-Geotrichum candidum
-Histoplasma capsulatum
-Mucoraceae (mucormycosis / zygomycosis)
-Aspergillus flavus
Nervous system disturbances
-Facial palsy
-Trigeminal neuralgia
Recurrent aphthous stomatitis
Viral infections
Cytomegalovirus
Molluscum contagiosum
18

MEDICAL MANAGEMENT
19

ANTI-RETROVIRAL DRUGS
One that blocks binding of HIV to target cells
One that blocks viral RNA clevage
One that inhibits enzyme reverse transcriptase 20

IDEAL REQUIREMENTS
1. Should be as specific as possible.
2. Should reduce viral production from infected cells.
3. Can be administered orally.
4. Should cross blood- brain barrier easily.
5. Should not develop resistance.
6. Shouldn’t be toxic.21

ART…
• Zidovudine (AZT, ZDV)
• Retrovir
• Didanosine
• Videx
• Zalcitabine
• Hivid
• Stavudine
• Zerit
22
Nucleoside - stop HIV from replicating within cells by inhibiting the reverse transcriptase protein.

ART…
• Nevirapine
• Viramine
• Delaviradine
• Rescriptor
• Efavirenz
• Sustiva
23
Non-nucleoside Reverse transcriptase inhibitors- stop HIV replicating within cells by interfering with HIV's reverse transcriptase protein which it needs to make new
copies of itself

ART…
• .
• Saquinavir
• Invirase
• fortovase
• Ritonavir
• Norvir
• Indinavir
• Crixivan
• Relfiravir
• Viracept
24
Protease inhibitors- binds to the protease molecules and interfere with its cleaving function and are more effective viral inhibitors:

“COCKTAIL” OR TRIPLE-THERAPY
• HAART
• Regimens include atleast one protease inhibitor or non-
nucleoside reverse transcriptse inhibitor in addition to one or
more nucleoside reverse transcriptase inhibitors
• SIDE EFFECTS
25

• Hemo-Modulator
26
works by filtering a patient's blood through the device which blasts
ultraviolet light onto the blood. The ultraviolet light effectively kills
the virus and jump starts the patient's immune system.

PROBIOTICS FOR HIV• Lin Tao (2008) and his colleagues screened
hundreds of bacteria taken from the saliva of volunteers.
Results showed that some lactobacillus strains had
produced proteins capable of binding a sugar found on
HIV envelope, called mannose.
• One strain secreted abundant mannose-binding
protein particles into its surroundings, neutralizing HIV
by binding to its sugar coating.
27

WHAT’S THE ROLE OF DENTIST?????
• 1. Provides routine dental care for HIV-infected individuals.
• 2. Understands the significance of oral lesions associated with
HIV disease, and performs evaluations, diagnostics, and
institutes treatment
• 3. Collaborates with other health care workers and social
support systems involved in the overall care of HIV-infected
patients.
28

LESIONS COMMONLY ASSOCIATED WITH HIV
INFECTION
29

30
Pseudomembranous Candidiasis Erythematous candidiasis
Hyperplastic candidiasis Angular cheilitis
ORAL CANDIDIASIS

MANAGEMENT• 1. More advanced lesions including hyperplastic candidiasis may require
systemic antifungal drugs.
• 2. Early oral lesions of HIV-related candidiasis are usually responsive to
topical antifungal therapy.
• 3. Most oral topical antifungal agents contain large quantities of sucrose,
which may be cariogenic after long-term use.
• 4. Sucrose-free nystatin, itraconazole and amphotericin-B are available.
• 5. Fluconazole oral suspension, chlorhexidine and cetyl pyridinium
chloride oral rinses may also be effective against oral candidal infection.
• 6. Systemic antifungal agents such as ketoconazole, fluconazole,
itraconazole and amphotericin-B are effective in treatment of oral
candidiasis.
31

long-term use of ketoconazole may induce liver damage in
individuals with preexistent liver disease.
The increased risk of chronic hepatitis B or hepatitis C
infection in immunosuppressed individuals may put some
patients at risk for ketoconazole induced liver damage.
If ketoconazole is prescribed, patients should receive liver
function tests at baseline and at least monthly during
therapy.
The drug is contraindicated if the patient's aspartate
transaminase (AST) level is greater than 2.5 times normal.
Its absorption also may be hampered by the gastropathy
experienced by many HIV-infected individuals
32

• TOPICAL DRUGS
• 1.Clotrimazole 10mg tablets: dissolve in mouth 3-5tablets daily for 7-14days
• 2.Nystatin
• a.Oral suspension (100,000 U/ml : Disp 240ml) Rinse with 1tsp qid.
• b.Oral suspension (extemporaneous) mix 1/8tsp with 4 oz water
• c.Tablets(500,000U): Dissolve 1tablet in mouth 4-5times daily.
• d.Pastilles (200,000U) disolve 1-2 pastilles in mouth,4-5times daily.
• e.Ointment 15g tube: Apply to affected area 3-4times daily.
• 3. Clotrimazole ointment 15g tube: apply to affected area qid.
• 4. Miconazole 2% ointment 15g tube: qid application.
• 5. Itraconazole oral suspension 100-200mg once daily for 7-28 days.
• 6. Fluconazole oral suspension 200mg of 1st day followed by 100mg once daily for atleast
2weeks.
• 7. Amphotericin B oral suspension 100mg four times daily for 2 weeks.

34
SYSTEMIC DRUGS
1. Ketoconazole (Nyzoral) 200mg tablets: take 2 tablets immediately,
then 1-2 tablets daily for 5-14days.
2. Fluconazole (Diflucan) 100mg tablets: take 2 tablets immediately,
then 1 tablet daily for 7-14 days.
3. Itraconazole (Sporanox) 100mg capsules: 200mg once daily with
meals for 4 weeks.

ORAL HAIRY LEUKOPLAKIA
• Microscopically, the lesion shows
A hyperparakeratotic surface with
projections that often resemble hairs.
• Beneath parakeratotic surface are
acanthosis and some characteristic balloon
cells resembling koilocytes.
• Epithelial displasia is not a feature and in
most OHL lesions little or no inflammatory
infiltrate in underlying C.T is seen
35

MANAGEMENT:
• 1. Oral hairy leukoplakia generally does not require
treatment.
• 2. Resolution has been reported after therapy with
acyclovir, zidovudine, podophyllin and interferon, but
usually recurs when treatment is discontinued.
• 3. Laser or Conventional surgery.
• 4. The incidence of OHL has been markedly reduced
since the advent of multidrug antiviral therapy for HIV
infection.
36

NON-HODGKIN’S LYMPHOMA
• Occurrence is more common in the gingiva.
• Has a characteristic white verrucous surface or necrosis of the
gingiva resembling ANUG.
• TREATMENT
• 1. Anti-malignancy drugs
• 2. Surgical excision
• 3. Radiation therapy37

KAPOSI’S SARCOMA• Kaposi’s sarcoma is a rare, multifocal
vascular. • Median survival time after onset of KS
is 7 to 31 months• Histologic picture:• Endothelial cell proliferation with
formation of atypical vascular channels• Extravascular hemorrhage with
hemosiderin deposition• Spindle cell proliferation• Mononuclear inflammatory infiltrate,
consisting mainly of plasma cells38

MANAGEMENT
• 1. Treatment includes use of antiretroviral agents,
laser excision, radiation therapy or intralesional
injection with vinblastine, interferon α, or other
chemotherapeutic drugs.
• 2. Nicholas et al in 1993 described the successful
use of intralesional injection of vinblastine at a
dosage of 0.1 mg/cm2 using a 0.2mg/ml solution of
vinblastine sulfate in saline.
• 3. Intralesional injections with sodium tetradecyl
sulfate
39

• Destructive periodontitis has also been reported in
conjunction with gingival KS. In such instances, scaling and root
planing and other periodontal therapy may be indicated in
addition to intralesional or systemic chemotherapy.
40

ATYPICAL ULCERATIONS
• Most reported oral ulcers are to herpes simplex
virus, CMV, EBV, histoplasmosis, herpes zoster
and mainly recurrent apthous ulcers are often
associated.
• Resistant viral strains are treated with foscarnet,
ganciclovir or valacyclovir hydrochloride.
• Topical corticosteroid therapy (fluocinonide gel
applied three to six times daily) is safe
41

ORAL HYPERPIGMENTATION:
• Often appear as spots or striations in the buccal mucosa, soft palate and the gingiva or tongue.
• The pigmentation may relate to prolonged use of drugs such as zidovudine, ketoconazole or clofazimine.
• Zidovudine is also associated with excessive pigmentation of the skin and nails.
Oral pigmentation may be caused by: Adrenocorticoid insufficiency caused by
prolonged use of ketoconazole Pneumocystitis carinii infection Cytomegalovirus infection
42

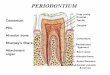
PERIODONTAL CONSIDERATIONS
43

Periodontal considerations…
Dennisn et al- first report linking periodontal disease and
HIV
Parra & slots- HIV in GCF
Barr et al- HIV RNA quantification in oral fluids
Shugers et al- serum viral load corelates with the salivary
viral load
Mononuclear cells present in GCF harbour HIV-1 DNA that
represents as a sourse of HIV in the oral cavity in the
presence or absence of bleeding- Maticic et al. 2000
44

LINEAR GINGIVAL ERYTHEMA:
Clinical features:
• A persistent, linear, easily bleeding,
erythematous gingivitis (LGE) has
been described in some HIV-positive
patients.
• May be localised or generalised
• No evidence of pocketing or
attachment loss.
45

Causes and pathogenesis
• candidal infection-Robinson
• Velegrakiet et al - Candida dubliniensis
• Winkler et al- CD4+ T cell depletion
• Barr et al46

LGE treatment…
Treatment:
- Does not respond well to plaque removal
- Conventional therapy plus rinsing with 0.12% chlorhexidine
gluconate twice daily has shown significant improvement after 3
months (Grassi M et al).
- Povidone-iodine substantially reduced pain associated with the
lesions (winkler et al).
47

LGE treatment…
• Step 1: Instruct the patient in performance of meticulous
oral hygiene.
• Step 2: Oral prophylaxis.
• Step 3: Chlorhexidine gluconate mouthrinse.
• Step 4: Reevaluate the patient in 2 to 3 weeks. If lesions
persist, evaluate for possible candidiasis. Consider empiric
administration of a systemic antifungal agent such as
fluconazole for 7 to 10 days.
• Step 5: Re-treat if necessary.
• Step 6: Place the patient on 2- to 3-month recall.
48

NECROTIZING GINGIVITIS: Clinical features:
• HIV-related necrotizing gingivitis is
defined by EC-WHO as destruction of one
or more interdental papillae.
• In the acute stage -ulceration,
necrosis and sloughing may be seen with
ready hemorrhage and characteristic fetor
• The anterior gingiva is most
commonly affected (Greenspan1993).
49

NUG…
• Causes and pathogenesis
• The isolated organisms include Borrelia, gram-positive
cocci, P-hemolytic streptococci and C. albicans (reichert et al)
• Thompson et al
• Barr et al
50

Treatment
• Basic treatment may consist of cleaning and
debridement of affected areas with a cotton pellet
soaked in peroxide after application of a topical
anesthetic.
• Escharotic oral rinses such as hydrogen
peroxide should only rarely be used, however, and are
especially contraindicated in immuno-compromised
individuals.
• Patient should be seen daily or every other day
for the first week
• The periodontium should be re-evaluated 1
month after resolution of acute symptoms to assess the
results of treatment and determine the need for further
therapy.
51

NUG…
• Does not always respond to conventional treatment with
scaling and improved oral hygiene (winkler jr et al).
• Adjunctive use of metronidazole & Antimycotic agents in
these patients is reported to be extremely effective in reducing
acute pain and promoting rapid healing (scully et al)
52

NECROTIZING PERIODONTITIS:
• Clinical features:
• According to the description by
EC-WHO necrotizing periodontitis is
periodontitis characterized by soft tissue
loss as a result of ulceration or necrosis.
Exposure, destruction or sequestration of
bone may be seen.
• The distinctive feature- loss
attachment
53

NUP…
• NUP is severely painful in onset and immediate therapy
is necessary
• On occasions, however, patients undergo spontaneous
resolution of the lesions, leaving painless, deep interproximal
craters that are difficult to clean and may lead to conventional
periodontitis 54

NUP…
Causes and pathogenesis:
• Higher proportions of C. albicans and C. rectus.
- Debilitating health and progression of disease
- However, some studies have also indicated that the association
between HIV-related immune depletion and periodontal
destruction is less strong (Martinez-Canut P, Guarinos J, jp
1996)
55

Treatment
Local debridement
Scaling and Root planing,
Irrigation with an effective antimicrobial agent.
In severe NUP, antibiotic therapy may be necessary
but should be used with caution in HIV-infected patients to
avoid an opportunistic and potentially serious localized
candidiasis or even candidal septicemia.
56

NUP…
• Does not always respond to conventional treatment with
scaling and improved oral hygiene (winkler jr et al).
• Prophylactic prescription of a topical or systemic
antifungal agent is prudent if an antibiotic is used.
• 57

INDICATIONS FOR HIV TESTING OF DENTAL PATIENTS
58

DIAGNOSTIC TESTS:
DIAGNOSTIC TESTS
ELISA
WESTERN BLOT (WB)
(PCR)P24 ANTIGEN
LAB-ON-A-CHIP
59

60

OCCUPATIONAL EXPOSURES AND POSTEXPOSURE PROPHYLAXIS (PEP):
61

62

GENERAL PRECAUTIONS TO BE TAKEN
• 1. Surgical gloves should be worn when touching
blood, saliva or mucous membranes.
• 2. Surgical masks and protective eyewear should be
worn.
• 3. Disposable or washable gowns should be used.
• 4. Instruments should be sterilized by autoclaving.
• 5. Debris should be removed by scrubbing with soap
and water before sterilization.63

GENERAL PRECAUTIONS TO BE TAKEN…
• 6. Surfaces should be decontaminated with sodium
hypochlorite.
• 7. Needles should be disposed with safety guard.
• 8. Droplets and aerosol production should be avoided where
possible by use of rubber dam and high-speed evacuation.
• 9. Apparent Fumigation of the operating room is required as a
part of disinfection.
64

CONCLUSION:
The pathogenesis periodontal diseases in HIV+
subjects may be due to the microflora, the effects of HIV
and other viral agents, and/or alterations in the host
response. These factors should be taken into
consideration in the treatment and prevention of
periodontal diseases in the HIV patient.
65

REFERENCES• Textbook of clinical periodontology- Carranza 10th Edition• Textbook of clinical periodontology- Carranza 9th Edition• Textbook of periodontology and implantology- Linde 5th Edition• Textbook of periodontology- Rose & Mealey• Textbook of periodontology- Eley & Manson• Textbook of Microbiology- AnanthNarayana• Textbook of Immunology- Roitt’s• The American Academy of Oral Medicine, Clinician’s guide to
HIV- infected patients. 3rd Edition.• Periodontology 2000,vol 60, 2012: 78-97• Periodontology 2000,Vol 50, 2009: 52–64• Periodontology 2000,vol 44, 2007: 55-81 66

References…• DCNA 2003, 467-492• R.G. Nair et al. Coinfections associated with HIV
infection: Workshop 1A. Adv Dent Res 2011;23(1): 97-105
• Scheutz F et al. Is there an association between periodontal condition and HIV infection. JCP 1997, 24: 580-587
• Murray et al. the Microbiology of HIV- Associated periodontal lesions. JCP 1989; 16: 636-642
• Angelika Langford. Gingival and periodontal alterations associated with infection with HIV. Quintessence Int 1994; 25: 375-387
• http://www.ambha.org/new-hiv-aids-treatment-methods.html
67

68
Thank u…




![PERIODONTIUM (10) [EDocFind.com]](https://img.dokumen.tips/doc/110x75/577d2ee51a28ab4e1eb0488d/periodontium-10-edocfindcom.jpg)