Embed Size (px)
Citation preview

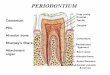
PERIODONTIUM
Oral mic anatomy and embyrology
BEE

PERIODONTIUM
Cementum
PDL
Alveolar bone
Sharpey's fibers
Attachment
organ
Cementum
Periodontal
ligament
Alveolar bone
Apical foramen
Pulp cavity Enamel
Dentin
Gingiva
Root canal
Alveolar vessels
& nerves

TEETH IN-SITU

Periodontium
Four tissue supporting the tooth in the jaw ◦ Cementum
◦ Periodontal ligament
◦ Alveolar bone
◦ Gingivae

Cementum
Thin layer of calcified tissue covering the root in the human teeth
Present in the crowns of some mammals ◦ Adaptation to herbivorous diet
One of four tissues supporting the tooth (periodontium)
The least known of ◦ Periodontium tissues ◦ All mineralized tissues

Role of Cementum
1) It covers and protects the root dentin
(covers the opening of dentinal tubules)
2) It provides attachment of the periodontal
fibers
3) It reverses tooth resorption

Cementum
Varies in thickness ◦ Thick @ apex (50-200 µm) &
inter-radicular regions
◦ Thin cervically (10-15 µm)
Contiguous with PDL Firmly adherent with root
dentine Highly responsive mineralized
tissue ◦ Maintenance of root integrity
◦ Maintenance of functional position of tooth
◦ Tooth repair & regeneration

Varies in thickness: thickest in the apex and
In the inter-radicular areas of multirooted
teeth, and thinnest in the cervical area
10 to 15 m in the cervical areas to
50 to 200 m (can exceed > 600 m) apically

Cementum
Slowly-formed throughout life Allowing continual reattachment of PDL
fibers Cementum can be regarded as a
mineralized component of PDL Precementum - a thin mineralized layer
on the surface of the cellular cementum Similar to bone, however -
◦ Avascular & not innervated ◦ Less rapidly resorbed – orthodontics

Cement-enamel junction
Pattern I ◦ Cementum overlaps enamel for a short distance ◦ Most predominant – 60% of sections
Pattern II ◦ Enamel meet cementum at butt joint ◦ Occurs in 30% of sections
Pattern III ◦ Enamel fails to meet cementum ◦ Dentine between them is exposed ◦ 10% of sections

Physical properties
Pale yellow Softer than dentine Permeability
◦ Varies with age and type of cementum ◦ Decreases with age ◦ Cellular is more permeable ◦ More permeable than dentine
Readily removed by abrasion after gingival recession

Chemical properties
Inorganic Organic Water
By weight 65% 23% 12%
By volume 45% 33% 22%
Hydroxyapatite crystals similar to those in bone More concentration of trace elements (F) at
surface F levels higher in acellular Collagenous organic matrix, primarily type I Molecules involved in PDL fiber reattachment
&/or mineralization ◦ Bone sialoprotein, osteopontin & cementum-specific
elements

Cellular and Acellular Cementum
A: Acellular cementum (primary cementum)
B: Cellular Cementum (secondary cementum)
Acellular cementum: covers the root
adjacent to dentin whereas cellular
cementum is found in the apical area
Cellular: apical area and overlying
acellular cementum. Also common in
interradicular areas
Cementum is more cellular as the
thickness increases in order to maintain
Viability
The thin cervical layer requires no cells
to maintain viability as the fluids bathe
its surface

A: Acellular cementum
B: Hyaline layer of Hopwell-Smith
C: Granular layer of Tomes
D: Root dentin
Cellular: Has cells
Acellular: No cells and has no structure
Cellular cementum usually overlies acellular cementum

Acellular
Cellular
Variations also noted where acellular and cellular reverse in position
and also alternate

Dentin
GT
Lacuna of cementocyte
Canaliculus
CEMENTUM
Acellular cementum
Cellular cementum
Hyaline layer
(of Hopewell Smith)
Granular layer of tomes
Dentin with tubules

Cementoblast and cementocyte
Cementocytes in lacunae and the channels that their processes extend are
called the canaliculi
Cementoid: Young matrix that becomes secondarily mineralized
Cementum is deposited in increments similar to bone and dentin


Are acellular and cellular cementum formed from two different
sources?
One theory is that the structural differences between acellular and cellular
cementum is related to the faster rate of matrix formation for cellular
cementum. Cementoblasts gets incorporated and embedded in the tissue
as cementocytes.
Different rates of cementum formation also reflected in more widely
spaced incremental lines in cellular cementum

Classification of cementum
Presence or absence of cells ◦ Cellular cementum
◦ Acellular cementum
Nature & origin of organic matrix ◦ Extrinsic fiber cementum
◦ Intrinsic fiber cementum
◦ Mixed fiber cementum
Combinations

Acellular cementum
Most common pattern- adjacent to dentine
Structureless Afibrillar cementum
◦ Exists between Acellular cementum
Hyaline layer (of Hopewell-Smith)
◦ Mineralized GS ◦ Covers cervical enamel ◦ Results following loss of REE

Acellular cementum •Root dentine
•Fibres of
Periodontal
Ligament
•Cementum •Epithelial
Rests

Cellular cementum
Most common pattern ◦ Apical area ◦ Inter-radicular areas ◦ Overlying acellular dentine
Cementocytes ◦ Inactive ◦ In lacunae – appear dark in GS ◦ Processes present in canaliculi ◦ Processes connected via gap junctions

Cellular cementum

Cementum simulates bone
Organic fibrous framework, ground
substance, crystal type, development
Lacunae
Canaliculi
Cellular component
Incremental lines (also known as “resting”
lines; they are produced by continuous but
phasic, deposition of cementum)

Clinical Correlation
Cementum is more resistant to resorption: Important in permitting
orthodontic tooth movement

Cementocytes vs. osteocytes
Cementocytes ◦ More widely dispersed
◦ Randomly arranged
◦ Canaliculi oriented towards PDL – nutrition
Osteocytes ◦ Osteon – Haversian system
◦ Organized cells
◦ Circumferential lamellae

Relationship between acellular & cellular cementum
More common pattern ◦ Acellular – cervically
◦ Acellular closer to dentine
◦ Cellular – apically
◦ Cellular covers acellular
Less common patterns ◦ Alternating
◦ Acellular overlies cellular

Extrinsic & intrinsic fiber cementum
Extrinsic fiber cementum ◦ Fibers derived from inserting Sharpy’s fibers of PDL
Intrinsic fiber cementum ◦ Run parallel to root surface at right angles to extrinsic fibers
◦ Fibers derived from cementoblasts

Acellular extrinsic fiber cementum
AEFC Over cervical half – 2/3s of the root Bulk of cementum in premolars First formed cementum - acellular Thickness of 15 µm All collagen are from Sharpy’s fibers Though GS from cementoblasts Fibers well-mineralized

Cellular intrinsic fiber cementum
CIFC Fibers deposited by cementoblasts Fibers run parallel to root surface No role of tooth attachment In apical 1/3 & inter-radicular areas May be
◦ Temporary – extrinsic fibers gain reattachment ◦ Permanent – without attaching fibers

Acellular intrinsic fiber cemetum
If cementum forms slowly in CIFC

Cellular mixed stratified cementum
Alternating AEFC with CIFC
Root apex
Furcation areas

Mixed-fiber cementum
Collagen fibers derived from ◦ Extrinsic fibers ◦ Intrinsic fibers
Intrinsic fibers run between the extrinsic fibers
Two types – rate of formation ◦ Acellular mixed-fiber cementum Well mineralized fibers
◦ Cellular mixed-fiber cementum Less well mineralized fibers

Cemental incremental lines
Irregular rhythm of deposition Not related to activity & quiescence Related to
◦ Difference in the degree of mineralization ◦ Composition of organic matrix
Imprecise periodicity Acellular – closer, thinner & regular lines Cellular - farther apart, thicker & irregular
lines

Development of Cementum
Cementum formation occurs along the
entire tooth
Hertwig’s epithelial root sheath (HERS) –
Extension of the inner and outer dental
epithelium
HERS sends inductive signal to ectomesen-
chymal pulp cells to secrete predentin by
differentiating into odontoblasts
HERS becomes interrupted
Ectomesenchymal cells from the inner portion
of the dental follicle come in with predentin by
differentiating into cementoblasts
Cementoblasts lay down cementum

How cementoblasts get activated to lay down
cementum is not known
3 theories:
1. Infiltrating dental follicle cells receive reciprocal signal from
the dentin or the surrounding HERS cells and differentiate
into cementoblasts
2. HERS cells directly differentiate into cementoblasts
3. What are the function of epithelial cell rests of Malassez?

Cementoblasts
Derive from dental follicle
Transformation of epithelial cells

Incremental lines
Cementum is formed rhythmically and can be seen as being composed of layers

Resorption & repair of cementum
Less susceptibility to resorption than bone Localized resorption areas occur Could be caused by microtrauma May continue to root dentine By multinucleated odontoclasts Resorption filled by mineralized tissue
(resembles cellular cementum) Reversal line

Reparative cementum vs. cementum
Wider uncalcified zone
Less mineralized
Smaller crystals
Calcific globules are present
Differences are related to different speed of formation

Clinical considerations
Cemental callus ◦ Root fracture
◦ No remodeling to original dimensions of the root
Cementicles ◦ Free or attached pieces in PDL
◦ Microtrauma
◦ Apical & middle 1/3s of root
◦ Root furcation

Clinical considerations
Supra-eruption of teeth Tooth wear Local hypercementosis
◦ Reaction to PA inflammation ◦ Difficulty in extraction ◦ Paget’s disease – multiple teeth with hypercementosis
Cementum narrowing root canal and shifting the junction between dental pulp & PDL cervically ◦ Pulp removal in RCT up to that point


Periodontal ligament PDL
Dense fibrous connective tissue
Occupies the area between the root of the tooth and the walls of the alveolar socket
Derived from the dental follicle
Continuous with ◦ the connective tissue of the gingiva above the alveolar crest
◦ The dental pulp at the apical foramen

Periodontal ligament space
Variable in width, average 0.2 mm
looks hourglass in shape Reduced in unerupted &
non-functional teeth Increased in teeth
subjected to heavy occlusal stress
Narrows slightly with age
Narrower in permanent teeth

Functions of PDL
Attachment Has a role in tooth eruption and support
Its cells repair the alveolar bone & cementum
Neurological control of mastication through its mechanoreceptors

Components of PDL
Fibers
Ground substance
Cells

Fibers of PDL
Collagen ◦ Type I (70% of fibers)
◦ Type III (20% of fibers) Found in the periphery of Sharpy’s fibers attachment into
alveolar bone
◦ Small amounts of type V, VI as well as basement membrane collagen IV & VII associated with the epithelial rests
◦ Highest turnover of collagen is in PDL Higher near apex
Even across the width of PDL
Rate could be related to the amount of occlusal stress
Oxytalan (in humans) or elastin ◦ Attached into cementum
◦ May have a role in tooth support

Principal fibers of PDL
Fibers exist as bundles (principal fibers) running in different orientations in different regions ◦ Dentoalveolar crest fibers ◦ Horizontal fibers ◦ Oblique fibers ◦ Apical fibers ◦ Interradicular fibers From crest of interradicular septum to furcation

Principal fibers of PDL

Sharpy’s fibers
Principal fibers embedded into cementum and bone
More numerous but smaller at cemental end
Mineralized and unmineralized parts

Ground substance of PDL
60% of PDL by volume Main components
◦ Hyaluronate GAGs ◦ Proteoglycans ◦ Glycoproteins
Functions of GS ◦ Ion and water binding & exchange ◦ Control of collagen fibrillogenesis & fiber orientation
◦ Tooth support & eruption - high tissue fluid pressure

Cells of PDL Fibroblasts
◦ Fusiform cells with many processes
◦ Functions – secretion and turnover of fibers Regeneration of tooth
support apparatus Adaptive responses to
mechanical loading
Cementoblasts ◦ Cement-forming cells lining cemental surface
◦ Cuboidal cells Osteoblasts
◦ Bone-forming cells lining tooth socket
◦ Resemble cementoblasts

Cells of PDL
Cementoclasts & osteoclasts ◦ Resorbing cells
◦ Howship’s lacunae
Epithelial rests cells ◦ Cuboidal cells that stain deeply
◦ Close to cemental surface
Defence cells ◦ Macrophages
◦ Mast cells
◦ Eosinophils

Blood vessels of PDL
Separate from those entering pulp
Some from alveolar bone through foramina
Some from pulp through accessory canals
Major vessels lie between principal fiber bundle close to alveolar bone
Capillary plexus around the tooth
Crevicular plexus of capillary loops
Veins do not follow arteries but drain into intraalveolar venous networks

Innervation of PDL
Sensory ◦ Nociception
◦ Mechanoreception
Sensitivity to occlusal loads
Guidance to intercuspation
Autonomic ◦ Associated with blood vessels

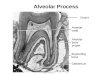
Alveolar process
The alveolar process develops during the eruption of teeth
Grows at a rapid rate at the free border
Proliferates at the alveolar crest
No distinct boundary exists between the body of the maxilla or mandible and the alveolar process
If teeth are lost the alveolar bone disappears

Development of bony crypt
Deciduous tooth & permanent successor initially share crypt
Bone subsequently forms to encase permanent tooth
















![PERIODONTIUM (10) [EDocFind.com]](https://img.dokumen.tips/doc/110x75/577d2ee51a28ab4e1eb0488d/periodontium-10-edocfindcom.jpg)