Embed Size (px)
Citation preview

Gonadotrophins in PCOS Thessaloniki, ESHRE/ASRM, 2008
Prof Aboubakr Elnashar Benha university Hospital, Egypt
Aboubakr Elnashar
Aim of ovulation induction in PCOS
Singleton live birth.
limited number of developing follicles.
{In PCOS: excessive multiple follicle development} (Brown, 1978; Baird, 1987).
Aboubakr Elnashar

Protocols
I. Step-up:
1. Conventional=Standard
2. Low dose
3. Chronic low dose
II. Step-down
III. Step-up, step-down
Aboubakr Elnashar
I. Step up
Principle:
Stepwise increase in FSH {determine the FSH
threshold for follicular development}
Aboubakr Elnashar

Aboubakr Elnashar

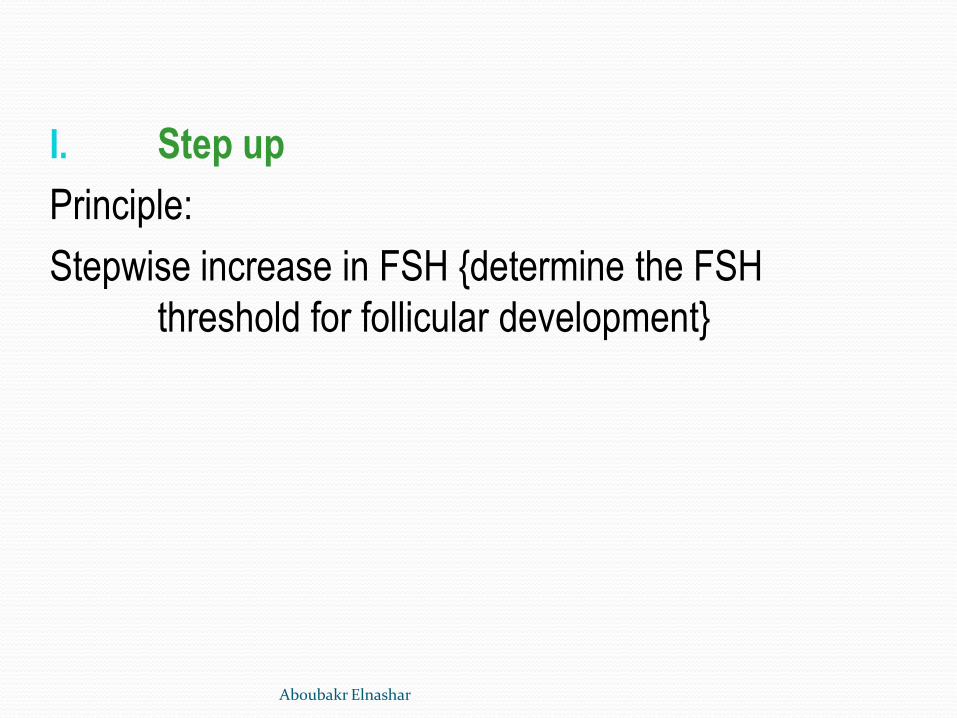
1. Conventional:
Starting dose: 150 IU/d:
Duration of starting dose: 5 d
Increased by: 75 IU/3-5 d
Excessive follicle development
Increased OHSS (Thompson and Hansen, 1970; Dor et al., 1980; Wang and Gemzell, 1980).
No longer recommended (Buvat et al., 1989; Brzyski et al., 1995)
Aboubakr Elnashar
Starting dose : 150 IU/d
2 FSH/hMG/day
Day 3Day 3 Day 7Day 75 days5 days
If
Follicle > 12 mm
E2 > 400U
Continue
2 FSH/d
No response® 3 FSH/day
for 3 more days
Endocrine Rev. 1997; 18: 71 Aboubakr Elnashar

2. low-dose
•Stating dose: 37.5-75 IU/d (White et al., 1996; Hayden et al., 1999; Balasch et al., 2000; Calaf et al., 2003).
•Duration of starting dose: 5-7 d -No follicle development: increase the dose
by 100%
-Follicle growth: maintain same dose until
follicular selection is achieved.
Aboubakr Elnashar
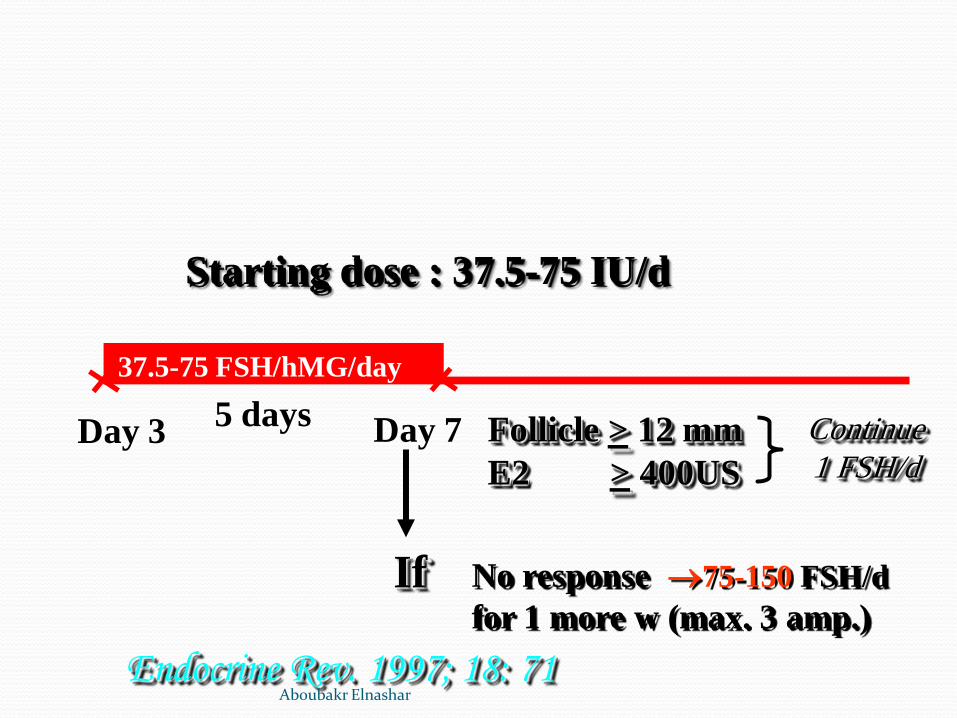
Starting dose : 37.5-75 IU/d
If
Follicle > 12 mm
E2 > 400US
Continue
1 FSH/d
No response 75-150 FSH/d
for 1 more w (max. 3 amp.)
Endocrine Rev. 1997; 18: 71
37.5-75 FSH/hMG/day
Day 3 Day 7 5 days
Aboubakr Elnashar

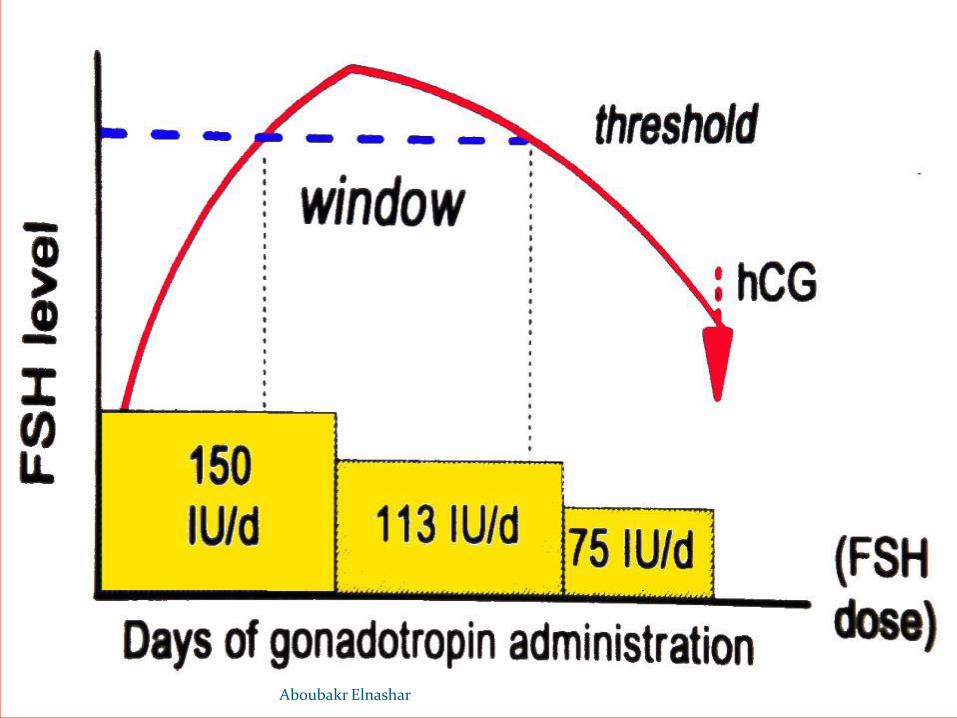
3. Chronic low-dose
•Starting dose: 37.5 IU
•Duration of starting dose:14 d
•The weekly dose increment: reduced from
100% to 50% or 37.5 IU (Seibel et al., 1984; Polson et al., 1987; Sagle et al., 1991; Dale et al., 1993).
:Markedly reduce excessive ov stimulation
Marked dec in OHSS.
Aboubakr Elnashar

0 14 21 28 35
75 iu 112.5 iu
150 iu
187.5 iu
225 iu
Days
7
37.5 iu
½ Amp.
One Amp.
42 49
2 Amp.
3 Amp.
White et al. J Clin Endocrinol Metab 1996;81:3821–4 Aboubakr Elnashar

II. Step-down:
Principle:
To achieve the FSH threshold through a
loading dose of FSH with a subsequent
stepwise reduction as soon as follicular
development is observed (Schoot et al., 1992; van Dessel et al., 1996; Fauser and Van Heusden, 1997).
Aboubakr Elnashar
Aboubakr Elnashar

Starting dose:150-225 IU/d for 3-4 d
decreased to 75Iu to maintain f develop
Day 3
2 FSH/d 1½ FSH/d 1 FSH/d
3-4 days. U/S & E2
Foll > 11 mm
2-3 days U/S
hCG
D7
FSH dose may be high or low: • Need to dose.
•Need to dose by one ampoule.
Aboubakr Elnashar
Step up Vs step down:
-Similar high rates of monofollicular development (van Santbrink and Fauser, 1997; Balasch et al., 2001).
-Step-up regimen:
safer in terms of monofollicular development (Christin-Maitre and Hugues, 2003).
monitoring require less experience & skill (van Santbrink et al., 1995).
Aboubakr Elnashar

III. Sequential step-up& step-down
Reduces risk of over-response (Hugues et al., 1996,
2006).
Aboubakr Elnashar

Low dose Step-up Step-down
one FSH/day
Day 3
step-up till 14 mm foll.
step-down
hCG Aboubakr Elnashar

Monitoring I. US
-Baseline:
-Serial
Documentation of all follicles >10 mm {predict
the risk of multiple pregnancies}. Monofollicular cycle:
Single follicle of 16 mm or higher
Single follicle of 16 mm or higher with no other follicle 12 mm or higher (Leader , 2006)
Aboubakr Elnashar
Cycle cancellation
>3 follicles ≥16 mm (White et al., 1996; Homburg and Howles, 1999; Calaf et al., 2003a)
>4 follicles ≥ 14 mm (Kamrava et al., 1982; Hugues et al., 2006).
>2 follicles ≥ 14 mm (Farhi et al., 1996)
>3 follicles ≥ 10 mm (Tur et al., 2001; Dickey et al., 2005).
>3 follicles ≥ 14 mm.
>2 follicles ≥16 mm or
>1 follicle ≥16 mm& 2 additional follicles ≥14
mm (ASRM, ESGRE, 2008)
Aboubakr Elnashar

II. E2 levels:
•Used to
cancel cycles (due to over- or under-response)
adjust the dose of Gnt
•Caution when
rapidly rising or
>2500 pg/ml (ASRM, 2006).
<1000 pg/ml (Tur et al., 2001; Dickey et al., 2005)
Aboubakr Elnashar

Efficacy
low-dose regimens
Monofollicular ovulation: 70%,
Pregnancy: 20% (Homburg and Howles, 1999).
Multiple pregnancies: <6%
OHSS: <1% (Hamilton-Fairley et al., 1991; van Santbrink et al., 1995; White et al., 1996; Balasch et al., 1996).
Conventional dose protocols:
Multiple pregnancies: 36%
Severe OHSS: 4.6% (Hamilton-Fairley and Franks, 1990).
Aboubakr Elnashar

Low dose Conventional
≤6% 36% Multiple pregnancy
≤1% 6% OHSS
Aboubakr Elnashar

Conclusion Low-dose FSH protocols are effective
in achieving ovulation in PCOS Starting dose: 37.5-50 IU/day.
Starting period: 14 d
FSH dose increment: 50% of the initial or previous dose
Intense ovarian response monitoring
Strict cycle cancellation criteria
Aboubakr Elnashar

•Duration: should not exceed 6 ovulatory cycles. •Preventing all multiple pregnancies &OHSS is not possible at this time.
Aboubakr Elnashar

Thanks [email protected] Aboubakr Elnashar