Embed Size (px)
Citation preview

By
Dr.Faris Al-Haddad
M.B.Ch.B, PhD AnatomyCollege of Medicine,
Hawler Medical UniversityArbil, Iraq
e-mail: [email protected]
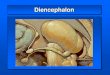
Diencephalon

Diencephalon

GROSS TOPOGRAPHY OF DIENCEPHALON,
“or in-between brain,”• is completely surrounded
by the cerebral hemispheres except at its ventral surface.
Borders :• Anteriorly : Foramen of Monro Lamina terminalis• Posteriorly : Posterior commissure

• Superiorly : forms floor of
lateral ventricle• Medially : forms lateral
wall of 3rdventricle. • laterally : Posterior limb of
internal capsule
Lateral and 3rd ventricles

Diencephalon is also marked medially by : Stria medullaris thalami

• A groove extending between the foramen of Monro and the aqueduct of Sylvius
(The Hypothalamic
Sulcus) that divides
diencephalon into 1. A ventral portion,
The Hypothalamus. 2. A dorsal portion, The Thalamus,

• The two thalami are connected across the midline in about 70% of humans through the (interthalamic adhesion)

Diencephalon includes :
(1)Epithalamus, (2) Thalamus and
Metathalamus, (3) Subthalamus, (4) Hypothalamus.

Epithalamus

Epithalamus : The epithalamus occupies a
position dorsal to the thalamus and includes the following structures :
A. STRIA MEDULLARIS THALAMI This band of nerve fibers connects
the septal (medial olfactory) area with the habenular nuclei.
B. HABENULAR NUCLEI are part of a network that
includes the limbic and olfactory systems, concerned with mechanisms of emotion & behavior.
C. PINEAL GLAND Its an endocrine gland. The
functions of the pineal gland are not well understood. It may have roles in gonadal function and circadian rhythm.

Thalamus

Thalamus :General Appearances• The thalamus is a large,
egg-shaped mass of gray matter that forms the major part of the diencephalon.
• There are two thalami, and one is situated on each side of the third ventricle.

• Anterior end of the thalamus is narrow and rounded
• Posterior end is expanded to form the pulvinar, which overhangs the superior colliculus .
• Usually connected to the opposite thalamus by interthalamic adhesion

Relations :• Anteriorly: interventricular
foramen• Posteriorly : expand as Pulvinar • Superiorly : floor of lateral
ventricle & Tela choroidae of 3rd ventricle
• Inferiorly : It rests on subthalamus & hypothalamus. Midbrain.
• Medially : forms part of lateral wall of the 3rd ventricle. Stria medullaris thalami
• Laterall : Body & tail of caudate nucleus. Posterior limb of internal capsule.

Subdivisions of the Thalamus The gray matter of the
thalamus is divided by a vertical sheet of white matter, internal medullary laminainternal medullary lamina, into medial and lateral halves. thalamus thus is subdivided into three main parts;
1. Anterior part : lies between the limbs of the Y.
2. Medial part : on medial side of Y stem.
3. Lateral part : lie on lateral side of Y stem.
Anterior
Medial
Lateral

• Each of the three parts of the thalamus contains a group of :
THALAMIC NUCLEI.
• Other smaller nuclear groups are :1. Within internal medullary lamina
( intralaminar ), 2. On medial surface of the thalamus 3. On lateral surface of the thalamus.4. Reticular nucleus.

1. Anterior part : • Anterior thalamic
nuclei 2. Medial part : • Dorsomedial nucleus • Several smaller nuclei 3. Lateral part :A. Dorsal Tier of the Nuclei :• Lateral dorsal nucleus
( LD ), • Lateral posterior
nucleus ( LP ), • Pulvinar
B. Ventral Tier of the Nuclei :• Ventral anterior nucleus
( VA ) • Ventral lateral nucleus ( VL )• Ventral posterior nuclei
( VP ):1. Ventral posteromedial ( VPM )2. Ventral posterolateral ( VPL )
Thalamic Nuclei :

Anterior
VA
VL
VIVPM
VPL
VP
LDLP
Pulvinar
MGBLGB
lamin
a
Internal medullary lamina
Median
Medial
Interthalamicadhesion
THALAMIC NUCLEI

Function of the Thalamus Although an enormous amount of research has
been devoted to this area, we still know very little about the functional significance of many of the nuclei.
1.A vast amount of sensory information of all types (except smell that inegrated with taste then) converges on the thalamus and presumably is integrated through the interconnections between the nuclei. The resulting information pattern is distributed to other parts of the central nervous system.
2.The thalamus possesses certain very important nuclei whose connections have been clearly established. These include the ventral ventral posteromedialposteromedial nucleus, the ventral ventral posterolateralposterolateral nucleus, the medial geniculatemedial geniculate body, and the lateral geniculatelateral geniculate body. Their positions and connections should be learned.

3. Anatomically and functionally, the thalamus and the cerebral cortex are closely linked. The fiber connections have been established, and it is known that following removal of the cortex, the thalamus can appreciate crude sensations. However, the cerebral cortex is required for the interpretation of sensations based on past experiences. For example, if the sensory cortex is destroyed :
• one can still appreciate the presence of a hot object in the hand;
• appreciation of the shape, weight, and exact temperature of the object would be impaired.

Connections And Function Of Thalamic Nuclei

Thalamic Nucleus
Afferent Neuronal Loop
Efferent Neuronal Loop Function
AnteriorNucleus
Cingulate gyrus, Hypothalamus
• Emotional tone • Recent memory

Thalamic Nucleus
Afferent Neuronal
Loop
Efferent Neuronal
LoopFunction
Medial Nuclei:
Dorsomedial
Prefrontal cortex, hypothalamus,
other thalamic nuclei
Integration of somatic, visceral, & olfactory information and relation to emotional feelings and subjective states

Thalamic Nucleus
Afferent Neuronal
Loop
Efferent Neuronal
LoopFunction
Dorsal Tier of the Nuclei : Lateral dorsal, Lateral posterior, Pulvinar
Cerebral cortex, other thalamic
nucleiUnknown?

Thalamic Nucleus
Afferent Neuronal
Loop
Efferent Neuronal
LoopFunction
Ventral Tier of the
Nuclei :1. Ventral anterior N.
Reticular formation, substantia nigra, corpus striatum,
premotor cortex, other thalamic
nucleiInfluences activity of
motor cortex
2. Ventral lateral N.
As in VA, but also has : • major input from cerebellum • minor input from red nucleus

Thalamic Nucleus
Afferent Neuronal
Loop
Efferent Neuronal
LoopFunction
3. Ventral posteromedi
al (VPM)
Trigeminal lemniscus, gustatory
fibersPrimary somatic sensory (areas
3,1, 2) in cortex
Relays common
sensations to
consciousness4. Ventral
posterolateral (VPL)
Medial and spinal
lemnisci

Thalamic Nucleus
Afferent Neuronal Loop
Efferent Neuronal
LoopFunction
ReticularCerebral cortex,
reticular formation
Other thalamic
nuclei
Cerebral cortex
regulates thalamus
Intralaminar
Reticular formation,
spinothalamic and
trigeminothalamic tracts
To cerebral
cortex via other
thalamic nuclei, corpus
striatum
Influences levels of
consciousness and
alertness

METATHALAMUS

METATHALAMUS The term metathalamus refers to two thalamic nuclei :
the medial geniculate and lateral geniculate.1.Medial Geniculate Nucleus This is a relay thalamic nucleus in the auditory system. It
receives :• Auditory fibers reach the medial geniculate body via
inferior brachium of the inferior colliculus. • Afferent feedback fibers comes from the primary auditory
cortex in the temporal lobe. • Efferent outflow forms the auditory radiation of the
internal capsule to the primary auditory cortex in the temporal lobe (areas 41 and 42).
• have roles in : 1. spectral analysis of sound, 2. sound pattern recognition, 3. auditory memory, 4. localization of sound in space, 5. matching auditory information with other modalities.

2. Lateral Geniculate Nucleus This is a relay nucleus in the visual system. It
receives : • Visual fibers from the optic tract conveying
impulses from both retinae. • Afferent Feedback fibers also reach the nucleus
from the primary visual cortex (area 17) in the occipital lobes.
• Efferent outflow forms the optic radiation of the internal capsule to the primary visual cortex in the occipital lobe.
• Some of the efferent outflow projects to the pulvinar nucleus and to the secondary visual cortex (areas 18 and 19)

Clinical Notes About Thalamus• Since the thalamus is such an important
relay and integrative center, so following disease of this area there will be profound effects.
• The thalamus may be invaded by neoplasm, undergo degeneration following disease of its arterial supply, or be damaged by hemorrhage.

Lesions of the ThalamusSensory Loss• These lesions usually result from
thrombosis or hemorrhage of one of the arteries supplying the thalamus. Damage to the ventral posteromedial nucleus and the ventral posterolateral nucleus will result in the loss of all forms of sensationresult in the loss of all forms of sensation, including light touch, tactile localization and discrimination, and muscle joint sense from the opposite side of the body.

• Surgical Relief of Pain by Thalamic Cauterization :
Cauterization of some nuclei has been shown to relieve severe and intractable pain associated with terminal cancer.
• Thalamic Pain: Thalamic pain may occur as the patient is
recovering from a thalamic infarct. Spontaneous pain, which is often excessive (thalamic overreaction), occurs on the opposite side of the body. The painful sensation may be aroused by light touch or by cold and may fail to respond to powerful analgesic drugs.

Subthalamus The subthalamus is a mass of gray and white
substance in the caudal diencephalon. It is bordered :• Medially by the hypothalamus, • Laterally by the internal capsule, • Dorsally by the thalamus, • Ventrally by the internal capsule. The subthalamus consists of three main structures;
these are :1. Subthalamic Nucleus, 2. Fields Of Forel, 3. Zona Incerta.Function : has wide connections, that engage it in wide
range of functions


Hypothalamus

Hypothalamus Lies in the diencephalon ventral to the
hypothalamic sulcus . Relations:1. Anteriorly : Lamina terminalis 2. Posteriorly : Midbrain. 3. Inferiorly : Antroposteriorly :• Optic chiasma, • Infundibulum forms pituitary stalk. • Floor slopes upwards and backwards to aqueduct,• Floor is marked by the pair of mamillary bodies
and behind them by the posterior perforated substance.
• Floor between opric chiasma & mamillary bodies is Tuber Cinereum.
4 Medially : 3rd ventricle 5. Laterally : Subthalamus

• The fornix divides the hypothalamus 1. The Lateral Zone :
contains mainly the medial forebrain bundle which connects the septal area, hypothalamus & midbrain. Among which are scattered neurons of lateral hypothalamic nuclei which are :
• part of the preoptic nucleus, • part of the suprachiasmatic nucleus, • Supraoptic nucleus, • Lateral nucleus, • Tuberomammillary nucleus, • Lateral tuberal nuclei.


1. Medial Zone : has a cluster of nuclei organized into major groups. From anterior to posterior :
• Preoptic nucleus; • Anterior nucleus, • Suprachiasmatic nucleus;• Paraventricular nucleus; • Dorsomedial nucleus; • Ventromedial nucleus; • Infundibular (arcuate) nucleus• Posterior nucleus.


MAIN AFFERRENT CONNECTIONS OF HYPOTHALAMUS

Origin Pathway Destination
Viscera and somatic
structures
Medial and spinal lemnisci,
tractus solitarius, reticular
formation
Hypothalamic nuclei
Retina Visual fibers Suprachiasmatic nucleus
Olfactory mucous
membraneMedial forebrain
bundleHypothalamic
nuclei
Inner ear Auditory fibers Hypothalamic nuclei

Origin Pathway Destination
Hippocampus
Hippocampo- hypothalamic
fibers ( main output of limbic system)
Nuclei of mammillary body
Frontal lobe of cerebral cortex
Corticohypothalamic fibers
Hypothalamic nuclei
Amygdaloid complex
Amygdalohypothalamic fibers
Dorsomedial and midline nuclei of
thalamusThalamohypothala
mic fibersTegmentum of
midbrain Tegmental fibers

MAIN EFFERRENT CONNECTIONS OF HYPOTHALAMUS

Origin Pathway Destination Preoptic,
anterior, posterior and
lateral nuclei of hypothalamus
Descending fibers in reticular
formation to brainstem and
spinal cord
Parasympathetic &
Sympathetic outflows
Nuclei of mammillary
body
Mammillo thalamic tract
Anterior nucleus of thalamus; relayed to
cingulate gyrus
Mammillo tegmental tract
Reticular formation in
tegmentum of midbrain
Hypothalamic nuclei
Multiple pathways Limbic system

Connections of the Hypothalamus With the Hypophysis Cerebri
The hypothalamus is connected to the hypophysis cerebri (pituitary gland) by two pathways:
(1)nerve fibers that travel from the supraoptic and paraventricular nuclei to the posterior lobe of the hypophysis
(2) long and short portal blood vessels that connect sinusoids in the median eminence and infundibulum with capillary plexuses in anterior lobe of the hypophysis.
• These pathways enable the hypothalamus to influence the activities of the endocrine glands.

Hypophyseal Portal Hypophyseal Portal SystemSystem
is formed on each side from the
• Superior hypophyseal artery, which is a branch of the internal carotid artery.
• The artery divides into tufts of capillaries.
• These capillaries drain into long and short descending vessels that end in the anterior lobe of the hypophysis by dividing into vascular sinusoids that pass between the secretory cells of the anterior lobe.

Hypothalamic Releasing and Inhibitory
Hormones and Their Effects on
Anterior Lobe of Hypophysis (Pituitary)

Hypothalamic
Regulatory Hormone
Presumed nuclei of origin
Anterior Pituitary Hormoneproduces
Functional Result
Growth Hormone–Releasing Hormone (GHRH)
Infundibular (arcuate nucleus)
Growth hormone
(GH)
Stimulates linear
growth in epiphyseal cartilages
Growth Hormone–Inhibiting Hormone (GHIH) or
Somatostatin
Suprachiasmatic nucleus
Growth hormone (reduced
production)
Reduces linear
growth in epiphyseal cartilages

Hypothalamic
Regulatory Hormone
Presumed nuclei of origin
Anterior Pituitary Hormone
Functional Result
Prolactin-Releasing Hormone
(PRH)?
Prolactin (luteotropic hormone,
LTH)
Stimulates lactogenesi
s
Prolactin-Inhibiting Hormone
(PIH), Dopamine
Prolactin (luteotropic hormone,
LTH) (reduced production)
Reduces lactogenesi
s

Hypothalamic
Regulatory Hormone
Presumed nuclei of origin
Anterior Pituitary Hormone
Functional Result
Corticotropin-Releasing Hormone
(CRH)
Paraventricular nuclei
Adrenocorticotropic hormone (ACTH)
Stimulates adrenal gland to produce
corticosteroids and sex hormones
Thyrotropin-Releasing Hormone
(TRH)
Paraventricular ,
dorsomedial nuclei and adjacent
areas
Thyroid-stimulating hormone
(TSH)
Stimulates thyroid gland to produce
thyroxine

Hypothalamic
Regulatory Hormone
Presumed nuclei of origin
Anterior Pituitary Hormone
Functional Result
Luteinizing Hormone–Releasing Hormone (LHRH), ? Follicle-
Stimulating Releasing Hormone
(FRH)
Preoptic and
anterior nuclei
Luteinizing hormone (LH) and follicle-
stimulating hormone
(FSH)
Stimulates ovarian follicles
and production of estrogen
and progestero
ne

Main Functions of Hypothalamus

Hypothalamic Nucleus Presumed Function
Supraoptic Synthesizes antidiuretic hormoneParaventricular Synthesizes oxytocin
Preoptic & anterior
Control parasympathetic system
Posterior & lateral
Control sympathetic system
Anterior Regulate temperature (response to heat)
Posterior Regulate temperature (response to cold)
Lateral Increase food intake (hunger center )
Medial Reduce food intake (satiety center )
Lateral Increase water intake (thirst center )
Suprachiasmatic Controls circadian rhythms

Clinical Notes

General Considerations :• Afferent haypothalamic pathways are
received from a. central nervous system (especially from the limbic system and the prefrontal cortex)
b. plasma levels of circulating hormones. • It exerts its influence on bodily functions
through the autonomic nervous system & endocrine system.

1. Obesity and Wasting :• It is generally associated with genital
hypoplasia or atrophy.• Wasting is less common than obesity in
hypothalamic disease. • Severe cachexia is suggestive of damage
to pituitary gland.2. Sexual Disorders :• In children, there may be sexual
retardation. After puberty, the patient with hypothalamic disease may have impotence or amenorrhea.

3. Hyperthermia and Hypothermia :• The patient with hyperthermia is otherwise normal
and has no signs of malaise, which occurs with pyrexia secondary to infections.
• Hypothermia also can follow a lesion of the hypothalamus.
4. Diabetes Insipidus : Diabetes insipidus results from a lesion of the
supraoptic nucleus or from the interruption of the nervous pathway to the posterior lobe of the hypophysis. Characteristically, the patient passes large volumes of urine of low specific gravity. As a result, the patient is extremely thirsty and drinks large quantities of fluids. The condition must be distinguished from diabetes mellitus, in which there is glucosuria.

1. Disturbances of Sleep :• Short periods of sleep during the waking
hours • Or insomnia has been observed in
patients with hypothalamic lesions.
2. Emotional Disorders : Attacks of unexplained weeping or
laughter, uncontrollable rage, depressive reactions, and even maniacal outbursts all have been observed in patients with hypothalamic lesions.