Embed Size (px)
Citation preview

Prof. Dr. Tarek Abd ElGhaffar
Consultant Cardiologist , NHI
Dr. Kareem Mandour
Resident of Cardiology , NHI

The term myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting consistent with myocardial ischaemia. Under these conditions any one of the following criteria meets the diagnosis for myocardial infarction: • Detection of rise and/or fall of cardiac biomarkers
(preferably troponin) with at least one value above the 99th percentile of the upper reference limit (URL) together with evidence of myocardial ischaemia with at least one of
the following: • Symptoms of ischaemia. • ECG changes indicative of new ischaemia (new ST-T
changes or new left bundle branch block [LBBB]). • Development of pathological Q waves in the ECG. • Imaging evidence of new loss of viable myocardium or new
regional wall motion abnormality. (Kristian Thygesen, et al 2007)

Complications
Electrical Complications
Mechanical complications
Heart Failure
Pericarditis
Post Infarction Angina or ReInfarction .
Take Home Message

Cardiogenic shock and heart failure are the most
common causes of death in patients hospitalized
with acute myocardial infarction.
At least 75% of patients with acute myocardial
infarction (MI) have an arrhythmia during the periinfarct period.

Electrical Complications : In acute M.I , Arrythmias are mainly due to reentry
caused by inhomogenicity of ischaemic myocardium . While Reperfusion Arrythmias are due to washout of the accumlated ions and metabolites .
Ventricular Arrythmias
1. Ventricular premature beats ( PVCs ) No correlation to the development of primary vent. Fibrillation .Treated by correction of the electrolyte or metabolic disturbances . If associated with sinus tachycardia , Beta Blockers are used to suppress the sympathetic overdrive.

2. Accelerated idioventricular rhythm :occurs in 20% of patients with STEMI , most often after successful reperfusion .
3. Ventricular Tachycardia : Non-Sustained V.Tach. isn’t associated with increase mortality during hospitalization or one year after .Sustained V.tach with haemodynamic stability should be treated immediately by amiodarone or procainamide , while if it's not aborted or associated with chest pain or haemodynamic deterioration , DC shock should be used for cardioversion .

4. Ventricular fibrillation :
Primary V.F
Secondary V.F
Late V.F
- Treatment Consists of:
Unsynchronized DC shock with at least 200 – 300 joules monophsic
Amiodarone I.V , helps interruption of the attack and prevent recurrence .
Treatment of hypokalaemia and magnesium deficits . ( aim K ≥ 4.5
Prophylactic Lidocaine is no longer recommended .

Supraventricular Arrythmias
1. Sinus Tachycardia :
very common in patients with acute M.I esp. Ant. M.I , it may be caused by other post-infarction causes as anxiety , persistant pain , LV dysfunction , fever , hypotension , hypovolaemia , pericarditis , pulmonary embolism , etc …..
2. Premature Atrial beats : may be due to atrial ischaemia or pericarditis .No specific therapy is indicated .
3. Paroxysmal SVT :usually transient and needs rate control using carotid massage , adenosine , verapamil , diltiazem or Beta blockers .

4. Atrial Flutter and Fibrillation :both are usually transient and may occur with patients with LV dysfunction , extension of ischaemia or pulmonary embolism .
Bradyarrythmias
1. Sinus Bradycardia : it’s common especially in Inferior and posterior Infarctions . If heart rate is below 40-50 , Atropine is administered .
2. First Degree A-V block : it may be caused by the use of Beta blockers or Calcium channel blockers

3. Second degree AV block :Type I: Does not require treatment except if ventricular
rate is below 50 bpm , then atropine is indicated.
Type II: has a potential to progress to complete heart block so temporary pacing is indicated and set at about 60 bpm.
4. Complete AV block : If associated with Inferior infarctions , it’s usually transient and
resolves within 72 hrs . Pacing is indicated if Ventricular rate is less than 40- 50 bpm
If associated with with anterior infarction , it usually occurs suddenly , after 12-24 hrs , they have unstable escape rhythm and a wide complexes at a rate ≤ 40 bpm . They are associated with an extensive septal necrosis and may need permenantpacing .

5. Intraventricular block :
RBBB with ant. MI is associated with increased mortality .

Indications of Temporary Pacing in Acute M.I :
1. Asystole
2. Symptomatic bradycardia not responsive to atropine
3. Complete Heart Block
4. Second degree H.B ( Mobitz type II )
5. New Bifasicular block
6. Bilateral Bundle branch block
7. Sinus pauses > 3 sec. , not resposive to atropine
8. Incessant Vent. Tachycardia ( overdrive pacing )

Mechanical complications1. Acute Mitral Regurge :
Papillary muscle dysfunction: Caused by posteromedial papillary ms dysfunction , It’s usually
transient during ischaemia . It usually presents with an apical systolic murmur , confirmed by
echocardiography . It requires no specific therapy , in intermediate cases it may require
antifailure treatment , while in severe cases it requires treatment like that of papiilary ms rupture .
Papillary ms Rupture : It occurs with Inferior Infarction 6-12 times more than Anterior
infarctions . It may present with acute pulmonary oedema or even sudden cardiac
death , it can occur upto 2-7 days post infarction . Intra-Aortic Balloon , vasodilators or inotropic therapy may be
required for temporary stabilization before surgery ( CABG + Mitral Valve Repair or Replacement )

Papillary muscle rupture complicating acute inferior myocardial infarction; magnified four-chamber view. The ruptured head of the posteromedialpapillary muscle (arrow) prolapses freely into the left atrium; the posterior mitral valve leaflet (arrowhead) is flail.

2. Ventricular Septal Rupture It occurs within the first week post-Infarction .
It occurs equally with Inferior and Anterior infarctions.
Rupture with Anterior Infarctions tend to be apical while it’s basal and has a worse prognosis with inferior infarctions .
It usually presents with a new onset murmur ( new harsh holosystolic murmur along the left sternal border ) . The patient is usually stable and develops sudden clinical deterioration .
Patients with acute VSR usually lie flat , while patients with acute MR develop pulmonary oedema & cann’t Lie flat .
Medical therapy is ineffective , Emergency Surgical Intervention is the treatment of choice .
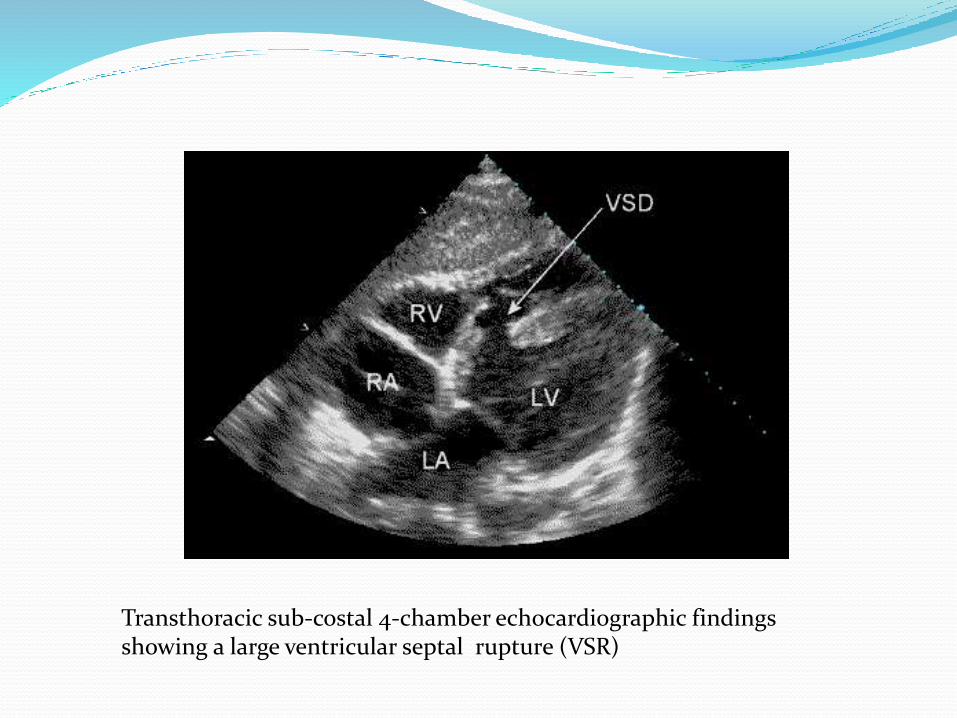
Transthoracic sub-costal 4-chamber echocardiographic findings showing a large ventricular septal rupture (VSR)
3. Free wall Rupture : Occurs within 2 weeks , and most common cause of death after
cardiogenic shock and arrythmias .
Early use of thrombolytic therapy appears to reduce the incidence of cardiac rupture , while late use appears to increase the incidence .
It usually presents by sudden Death. Few cases can be salvaged by immediate pericardiocentesis ,
emergency Thoracotomy and surgical repair .

Cardiac free wall rupture post myocardialinfarction.
Pericardial tamponade from left ventricular freewall rupture and hemopericardium.

4. Ventricular Aneurysm :Diff. between True and Pseudo-aneurysm .
True Aneurysm Pseudo-Aneurysm
Clinically : abnormal precordial impulse in the 3rd left intercostal space
ECG : ST Seg. Elevation persists more than 2 weeks . ( it may indicate a large infarction with RWMA not necessarily Aneurysm ) .
Other Mechanical Complications
5. Pulmonary Embolism : • Post-infarction patients have greater tendancies for Pulmonary
embolism ( P.E ) due to decreased cardiac output and immoblization ,
• Early mobilization and treatment aiming to increase Cardiac output are the most effective prophylactic methods .

7. Systemic embolism : LV thrombi occurs in 20-40 % of ant. Infarction Patients .
If LV thrombus is clearly demonstrated in Echocardiography , Systemic anticoagulation should be given for 3-6 months .

Heart Failure and Cardiogenic shock: Heart Failure occurs when LV function decrease by 30% of
normal function .
Killip Class: Clinical Examination
I No S3 or rales
II Rales in less than half of lung field
III Rales in more than half of lung field
IV Cardiogenic shock
May present acutely after MI ( killip class II or III ) or as a delayed presentation ( NYHA II-IV) .

Cardiogenic shock is persistent hypotension with a systolic pressure <80 mm Hg for more than 30 minutes in the absence of hypovolemia. It occurs when ≥ 40 % of myocardium is affected .
The most common causes of cardiogenic shock include 1) large left ventricular infarct (usually >40% of
left ventricle) seen in about 80% of shock patients
2)right ventricular infarct in 10% of shock patients
3) mechanical complications of myocardial infarction
(ventricular septal defect, acute mitral regurgitation,
tamponade) in 10% of shock patients.

Pericarditis :
1. Early post-infarction Pericarditis Occurs 2-4 days following acute infarction .
Patients who develop this condition usually have larger infarcts , lower EF and higher incidence of CHF .
Presented by Fever , Chest pain and friction rub .
Pain is aggrevated by movement and inspiration , Radiated to the trapezius .
Treated by Aspirin 160 – 325 mg daily ( although higher doses may be required 650 mg / 4-6 hrs ) , Anticoagulants are relatively contraindicated .

2. Post MI syndrome ( Dressler’s Syndrome )
Fever , chest pain , friction Rub .
Occurs after 1 week up to several weeks of MI .
Treatment as that of early post-MI pericarditis except that an oral corticosteroid course maybe required .
Anti-Coagulants should be stopped .
May cause pericardial effusion but rarely tamponading .

Take Home Message
Cardiac Rehabilitation and extended follow up of the post-Infarction patient clinically and by imaging modalities are as important as the early follow up.
Anticipate complications in every patient , so you won’t miss it when it occurs .





















![Mi Complications[1]](https://img.dokumen.tips/doc/110x75/577d238e1a28ab4e1e9a1f55/mi-complications1.jpg)






