Embed Size (px)
Citation preview

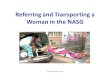
TRANSFER OF PATIENTWITH PPHPROF GOMATHY NARAYANANPROF NARAYANAN RPROF SHEELA V MANE
PPH Module

When to transfer the patient with PPH?
From PHC to First Referral unit: Clinical assessment Class I / Retained placenta / Traumatic PPH
From Nursing home with OT to Hospital with HDU & ICU:
Uncontrolled Class II From Labor room to OT: Class II / Retained placenta / Traumatic PPH
(Do not wait till Class III & IV)

Prerequisites for Transfer Informed consent Anti shock Garment (NASG) Check availability of bed/Doctor in the
referral hospital Referral documents Indwelling catheter with Urosac Vaginal pack in traumatic PPH Tamponade in atonic PPH Record presence of Pack/Tamponade – Do
not remove until destination

Referral Documents Antenatal Record with risk factors Intranatal events: Delivery notes: Vaginal/Instrumental / Caesarean section Time of delivery of Baby/Placenta Episiotomy/Vaginal laceration/Cervical tear Investigation results Sequence of events Medication administered with time & dose Fluids administered Condition on Transfer

On transfer Nasal Oxygen on flow Two IV lines (#16/18) with fluid on flow Nurse or Doctor & Patient’s able
attendant to accompany

Non-Pneumatic Anti Shock Garment(NASG)

NASG (Life Wrap) It applies pressure on the legs & abdomen Blood returns to vital organs curbing
internal bleed Stabilizes BP until patient reaches
appropriate hospital Easy to apply Application time takes < 60 seconds in
trained hands

How does NASG work? It is a First Aid Controls bleeding through direct pressure Auto transfusion of blood in upward
direction Ball in abdominal segment applies
focused pressure to uterus Circumferential pressure on lower half of
the body reduces the total vascular space Vital organs get increased blood supply &
oxygenation Stabilization of patient during transport

How does NASG work?

About NASG NASG is light weight (1500 G) Compression suit made of Neoprene Six segments enclosing ankle, calves,
thigh, pelvis & abdomen Velcro fastenings to keep garment tight A small foam ball in the abdominal
segment applies pressure on the uterus Markings on the sections show how to
apply

About NASG
Correct tight application supplies 20 to 40 mm Hg of circumferential pressure to lower body effectively reversing hypovolemic shock
Can be easily packed back into carry bag

NASG (Life wrap)

Applying NASGStep 1: Place NASG under the woman with the top
at the level of lowest rib Close segment 1 tightly around ankle on
both sides Snap it until you hear a sharp soundStep 2: Close segment 2 around calf muscle Leave the knee joint free

Applying NASG Step 3: Apply segment 3 around the thighs Step 4: Apply segment 4 all around the woman
with the lower edge at the level of pubic bone

Applying NASG Step 5: Place segment 5 with pressure ball
directly over umbilicus Close the NSAG using segment 6 Only one person should close segment 4
& 5 Should not be too tight to restrict breathing

Applying NASG Step 6: Ensure patient is breathing normally
after the application In case of uterine atony administer
uterotonics & massage the uterus without removing the NASG
NASG is flexible enough to allow the massaging

Vaginal Procedures with NASG in situ
Pelvic examination Lithotomy position Repair of episiotomy /
Perineal tear / Vaginal laceration / Cervical tear
MRP Bimanual compression D&C / D&E / MVA

Surgery with NASG in situ
Laparotomy (Keep segments 1,2&3 in situ and open pelvic & abdominal segments 4,5&6 just prior to incision)
Steep Trendelenberg position Operate quickly Replace segment 4, 5 & 6 after
procedure

Special situations
Obese women Short stature Need for defecation Replacing soiled
NASG

Questions to ask the patient
Are you comfortable? Any breathing difficulty? Is it hot inside NASG? Do you feel itchy?

When to remove NASG? Patient must be stable for 2 hours Bleeding <50 ml/hr Pulse <100 BPM Systolic BP 90-100 mm Hg Hb >7G% Patient conscious & aware

How to remove NASG?
Remove segment 1 & wait for 15 mts Check pulse & BP If pulse rate increases >20 BPM or BP
falls by 20 mm Hg: Reapply segment 1 If vitals stable remove segment 2 Follow same principles till removal of
segment 6

Do not remove NASG before all vital signs are restored
Early removal of NASG can be dangerous or even fatal

Caution
If BP falls by 20 mm Hg or Pulse increases by 20 BPM after removal of any segment, rapidly replace all segments
Consider need for crystalloids / Blood If recurrent bleeding, determine source
and arrest

Storing NASG Clean NASG with running water & disinfectant
and dry Keep folded NASG in a clear plastic bag Store NASG in a place where it is visible &
accessible Always store at the same place Ensure every one knows place of storage Storage place should be displayed
prominently The referral center must send a replacement
NASG after receiving the patient

Relative contraindications
Cardiac failure Pre existing Mitral stenosis / Pulmonary
edema Advanced pregnancy with live fetus
(APH) Abdominal evisceration Open pelvic fracture

Principles to be observed
One person alone can apply NASG Two persons needed when patient is
unconscious Urine output should be measured Ensure airway protection & Prevent
aspiration Ensure one on one nursing care

Advantages of NASG
50-78% Reduction in blood loss 50-55% Reduction in Maternal Mortality
& related Morbidity WHO includes NASG in recommendations Cost effective Reusable

World Scenario 2013Used in 16 Countries
UK & USARemote Rural areas
Jehova’s witness
Zambia &ZimbabwePeri urban
centers
Tamil NaduAll levels
Ambulance#108