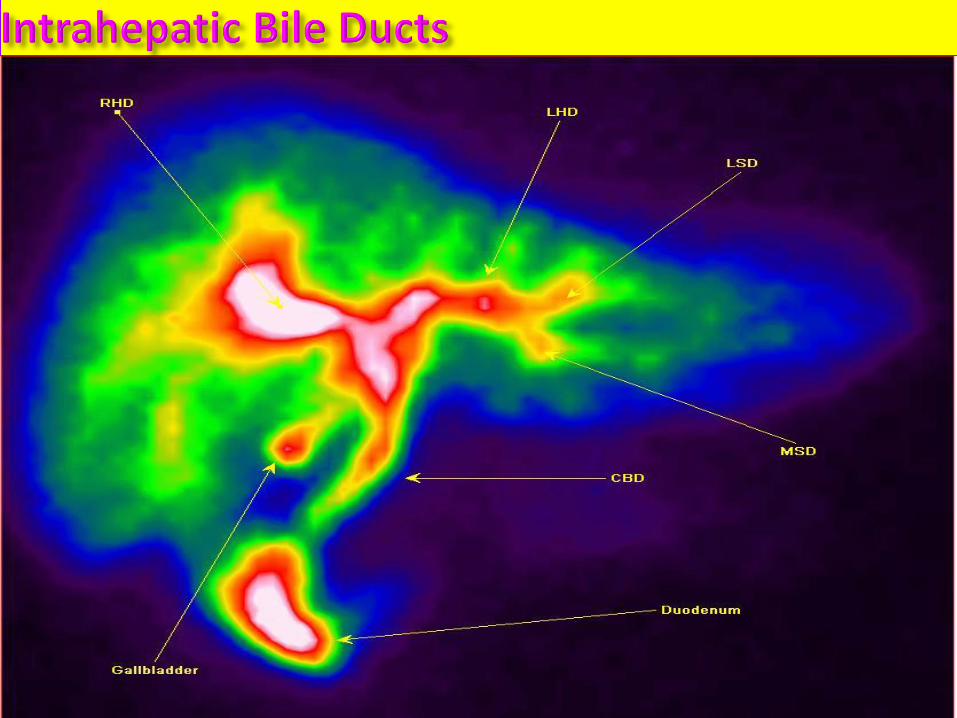
HEPATOBILIARY
IMAGING

BILIARY IMAGING MODALITIES Ultrasonography (USG)
CONVENTIONAL RADIOLOGY Simple X-ray of the Abdomen
Oral Cholecystography (OCG)
Intravenous Cholecycto-Cholangiography (ICCG)
Endoscopic Retrograde Cholangio-Pancreatography ERCP
Percutaneous Transhepatic Cholangiography(PTC)
Per/Postoperative Cholangiography
Nuclear Medicine (Hepato-Biliary Scintigraphy, Hepato-Splenic Scintigraphy, SPECT, PET)
CT
MRI
Magnetic Resonance Cholangio-Pancreatography (MRCP)

Ultrasonography The imaging modality of choice for the gallbladder. It is fast,
real-time, non-invasive, and does not utilize ionizing radiation.
High sensitivity for detection of cholelithiasis. Diagnosis based
on visualization of a mobile, hyperechoic, intraluminal mass
with acoustic shadowing.
High sensitivity for detection of acute cholecystitis. Diagnosis
based on presence of cholelithiasis, gallbladder wall
thickening, pericholecystic fluid.
Limited by skill of operator, and patient’s body habitus.

Acute Cholecystitis

Gallbladder Hydrops. Acute Cholecystitis

A) Acute Cholecystitis
B) Gallbladder Microlitiasis
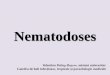
Gallbladder polyp

Gallbladder Adenomatous Polyp

Simple X-ray of the Abdomen This was an imaging technique used in the past, but has
been widely replaced by the ultrasound.
Can be used to visualize calcified stones, emphysematous
cholecystitis (gas within the wall of the gallbladder),
biliary fistula (gas within the biliary system), porcelain
gallbladder.

Simple abdominal x-ray demonstrating calcified gallbladder stones (opaque)

Calcified gallbladder stones (opaque)

Simple X-ray of the Abdomen
Calcified gallbladder stones
Porcelain gallbladder
Aerobilia - gas within the biliary system.
(cause: bilio-digestive anastomizes , emphysematous cholecystitis)
- replaced by USG
Aerobilia
opaque stones Porcelain
gallbladder
Emphysematous cholecystitis

Oral Cholecystography (OCG)
OCG used to be the imaging modality of choice for detecting cholelithiasis. It is now used as an adjunct to ultrasound. It is obtained when the patient has the symptoms of cholelithiasis, but a negative ultrasound.
It is more useful that ultrasound for visualizing large stones, and also is useful for counting the number of stones present.
Contraindications: Patients with bilirubin > 3mg/dL
Pregnancy.
Technique: Per-oral CM administration 12-16h before X-ray examination
Can be used cholecystokinetic medication or cholecystochinetic meal. X-rays a made at 15’,30’,45’,60’.
Partially replaced by USG.

COLECISTOGRAFIE PER OS:
A) normal contraction after Boyden meal (A meal consisting of three or four egg
yolks, beaten up in milk and sweetened, used to test the evacuation time of the
gallbladder.)
B),C) Gallbladder litiasis (lucent stones)

Percutaneous Transhepatic Cholangiogram
(PTC)
PTC is indicated when percutaneous intervention is
needed and ERCP either is inappropriate or has failed.
Can be used to drain biliary obstructions.

Percutaneous Transhepatic Cholangiogram (PTC)
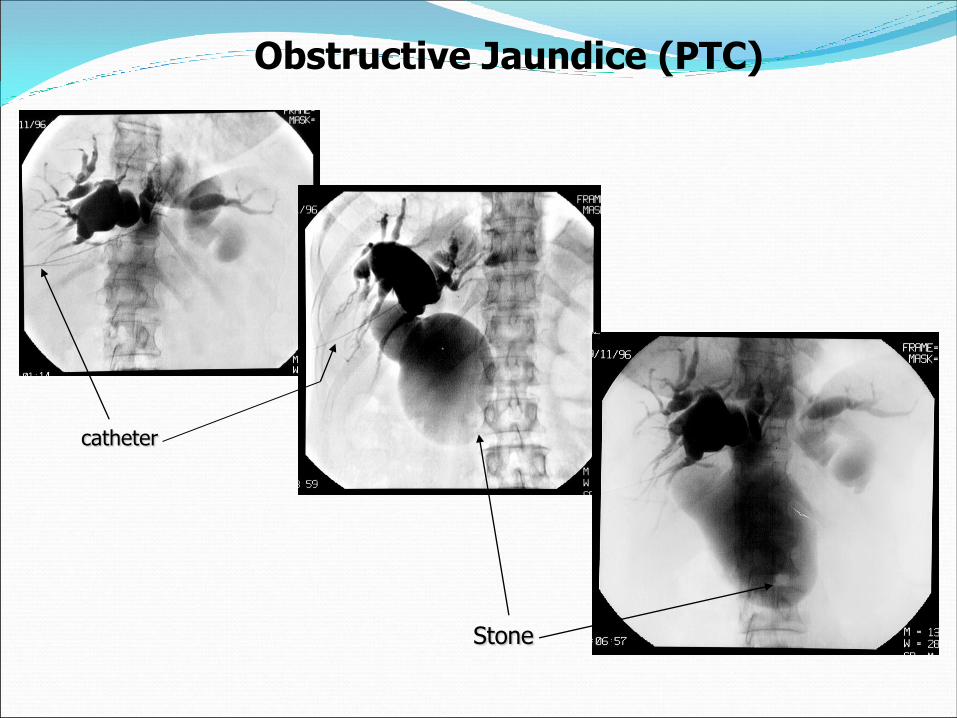
catheter
Stone
Obstructive Jaundice (PTC)
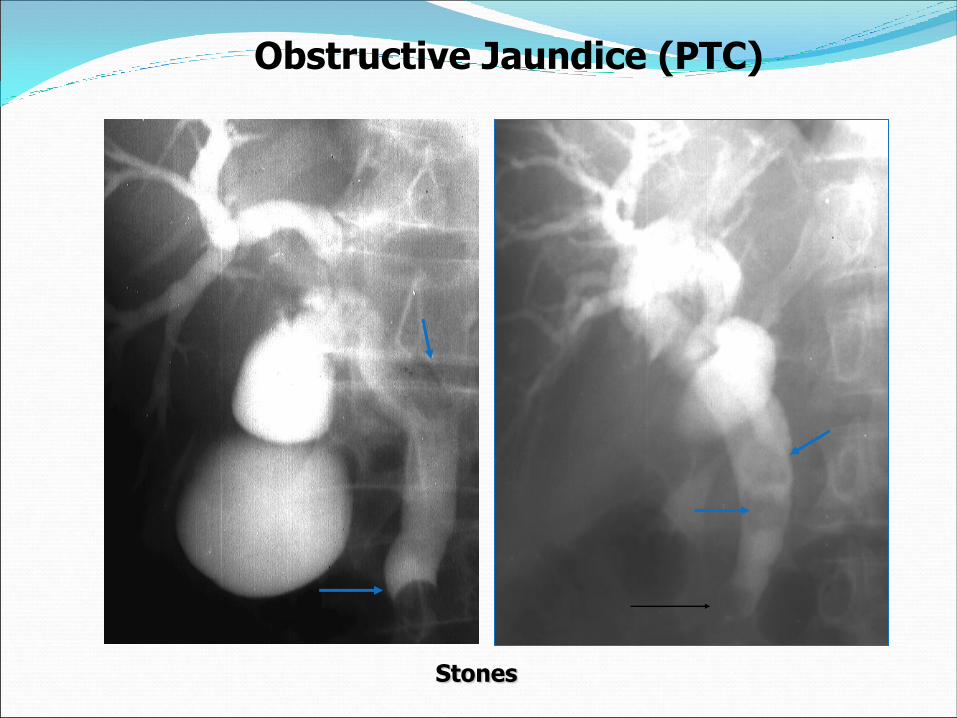
Stones
Obstructive Jaundice (PTC)

Endoscopic Retrograde
Cholangiopancreatography (ERCP) ERCP is the primary method of direct cholangiography,
and has therapeutic potential. It also allows for examination of the upper GI tract, the papilla of Vater, and the pancreatic duct. Biopsies of multiple sites can be taken using this technique.
ERCP causes less discomfort than PTC, but acute pancreatitis is a common complication (which is rarely seen in PTC).

ERCP: The endoscope is introduced and is threaded around to the sphincter of Oddi.
There, dye can be injected into the ducts. Instruments can also be inserted through the
scope to remove stones, insert drains, remove tissue samples, of perform other treatments.
ERCP The most important indication for ERCP is obstructive
jaundice, as it can demonstrate the cause and extent of the
obstruction.
ERCP is the preferred method of examination of patient
with possible choledocholithiasis, because the stones can
be extracted with balloons or gaskets after sphincterotomy
is performed.


ERCP:
NORMAL
ENDOSCOP
WIRSUNG
COLEDOC

ERCP showing stones
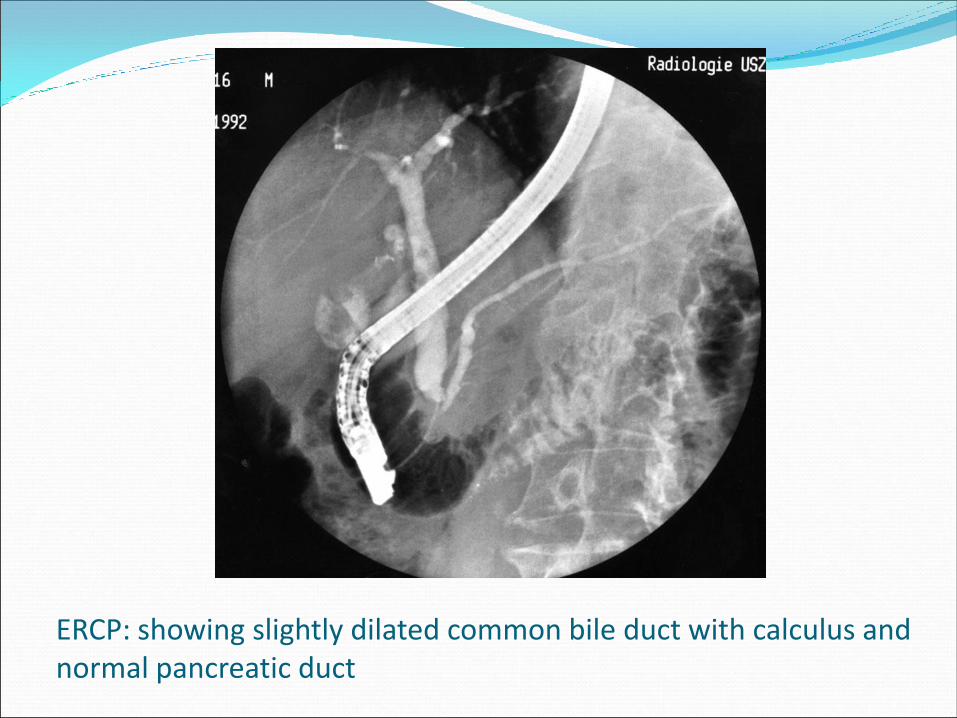
ERCP: showing slightly dilated common bile duct with calculus and normal pancreatic duct

ERCP: demonstrating stone in the duct (arrow)

Radiolucent stone in ductus choledocus (ERCP)
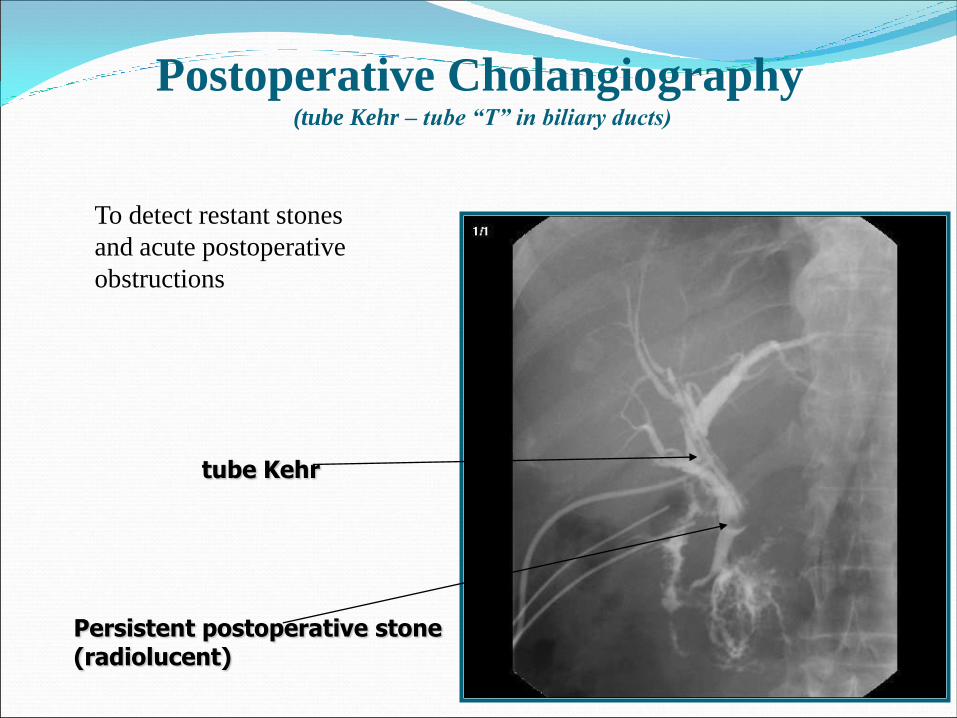
tube Kehr
Persistent postoperative stone(radiolucent)
Postoperative Cholangiography (tube Kehr – tube “T” in biliary ducts)
To detect restant stones
and acute postoperative
obstructions
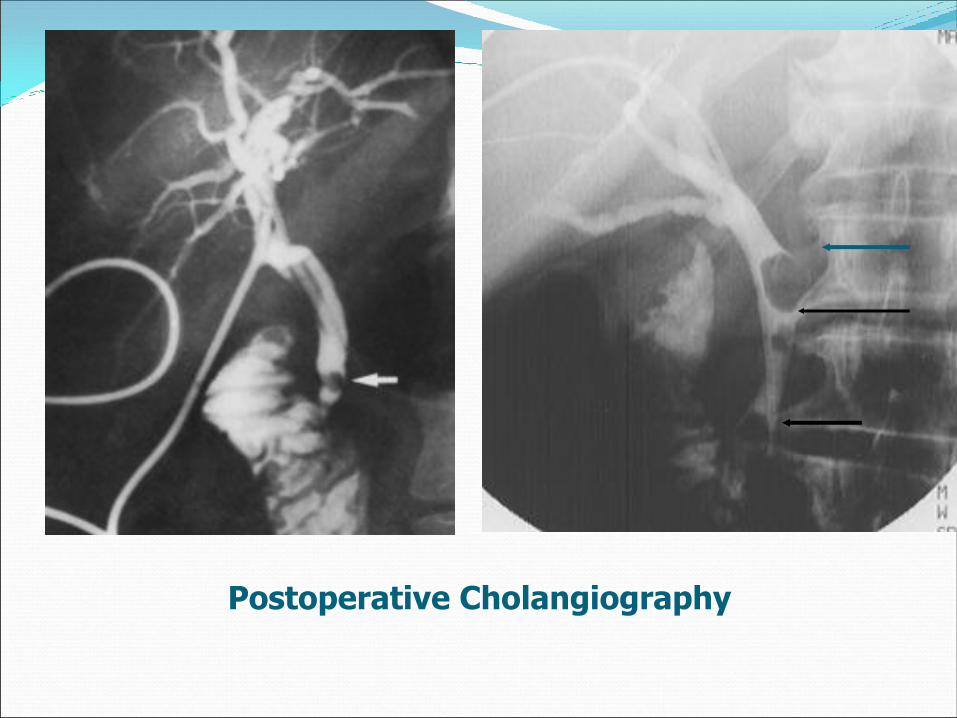
Postoperative Cholangiography
Magnetic Resonance
Cholangiopancreatography (MRCP)
MRCP is becoming a more viable imaging technique, as MRI technology improves. However, CT and ultrasound are faster, easier, and more readily available, so they are used more frequently than MRCP.
MRCP is emerging as a new tool for non-invasive evaluation of the pancreatic and biliary ductalsystems.
MRCP is gradually replacing PTC and ERCP for diagnostic purposes.

MRCP
Bile ducts anatomyIntrahepatic
- Right hepatic duct:
- posterior rhd
- anterior rhd
- Left hepatic duct

Extrahepatic
MRCP
Bile ducts anatomy

MRCP

MRCP with stones in the duct

MRCP with stone in the bile duct

MRCP with stones in the gallbladder

MRCP
Tumor of the head of the pancreas
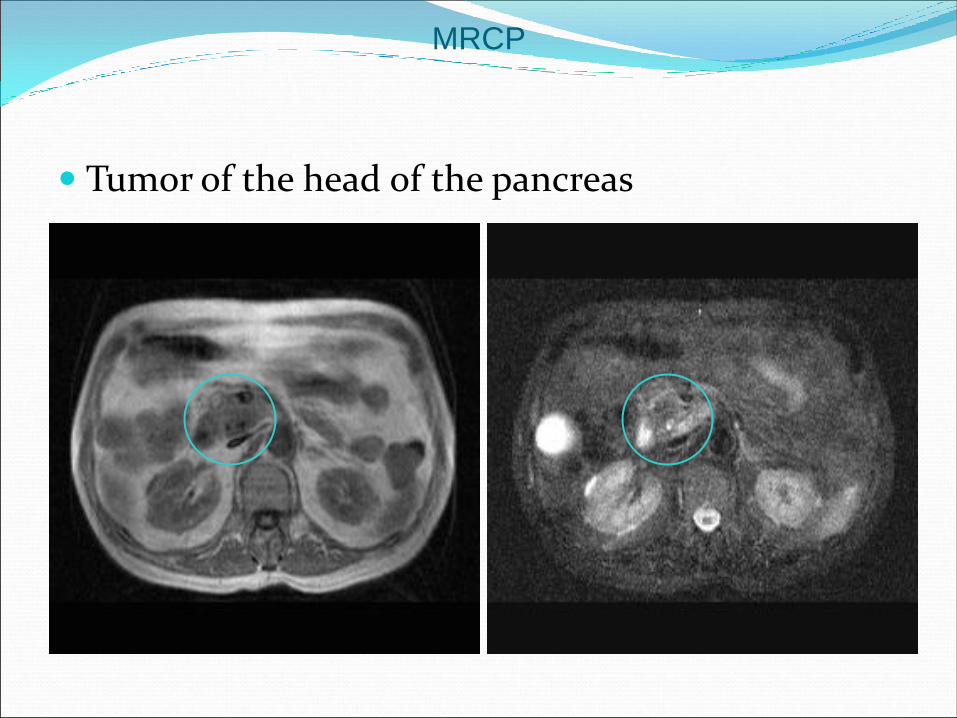
MRCP
Tumor of the head of the pancreas

Cholangiocarcinoma
MRCP

Plain Radiography
Ultrasound
CT
MRI
Nuclear Medicine
HEPATIC IMAGING MODALITIES

PLAIN RADIOGRAPHY Limited value for assessing the liver
Can demonstrate gross hepatomegaly and hepatic calcification.
True borders of the normal liver can only be identified if directly outlined by fat or by free intraperitoneal air.
The lungs and diaphragm delineate the apparent superior liver border but a subphrenic collection or a subpulmonary effusion may be misinterpreted as part of the liver itself.
As the anterior and inferior border of the liver often extends inferior to the gas-containing lumina of the stomach, duodenum and hepatic flexure of the colon, these gas-filled structures are unreliable guides to the inferior border.
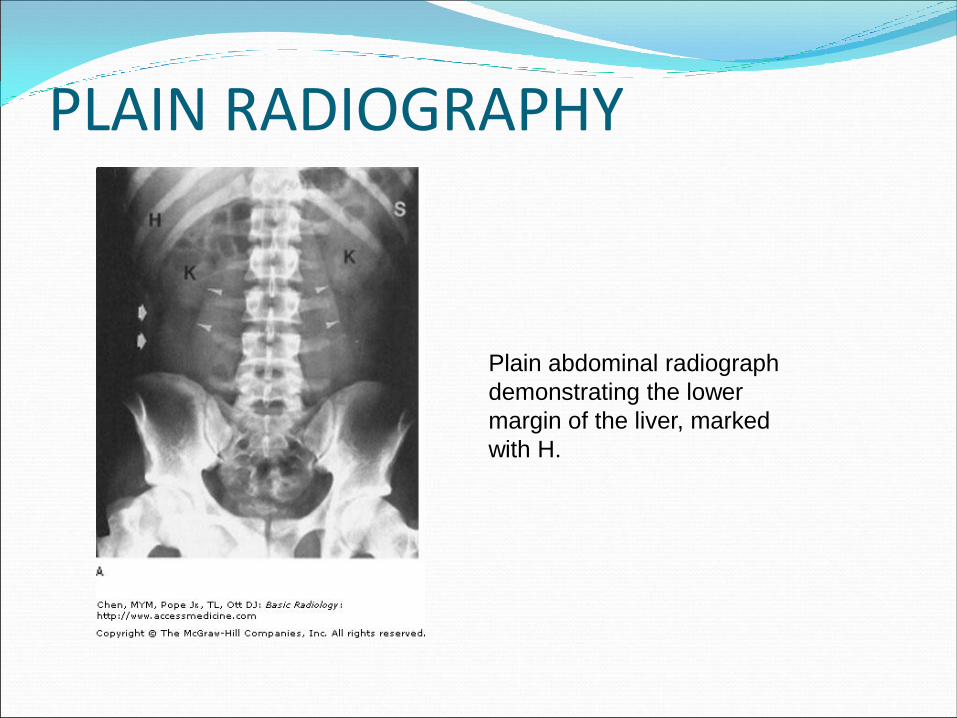
PLAIN RADIOGRAPHY
Plain abdominal radiograph
demonstrating the lower
margin of the liver, marked
with H.
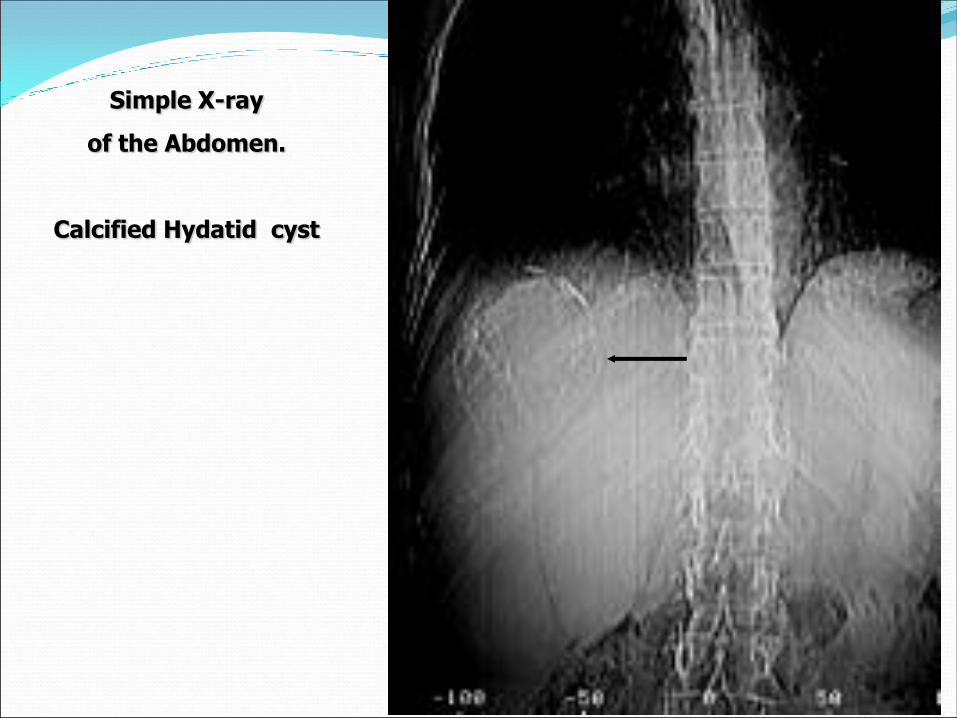
Simple X-ray
of the Abdomen.
Calcified Hydatid cyst
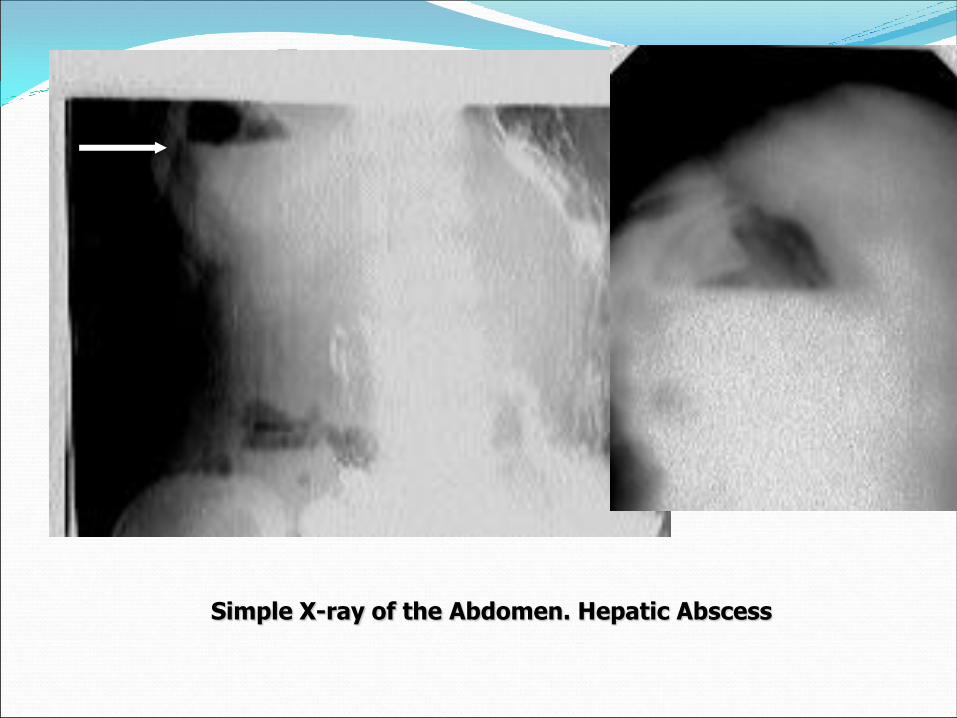
Simple X-ray of the Abdomen. Hepatic Abscess

Liver Anatomy
The anatomic divisions of the
liver showing the vasculature
and biliary system.
CT of the normal liver showing
general anatomy.

Liver Anatomy
A more inferior CT of the
normal liver with adjacent
structures.
MRI of the normal liver with
labeled adjacent structures.


Ultrasound First choice imaging modality for pains, abnormal or suspected liver masses.
Relatively inexpensive, widely available, and moderately sensitive to localized lesions.
Limited utility in the presence of diffuse diseases such as cirrhosis or fatty infiltration, or when air is present.
The liver is typically homogeneous in appearance.
In general, fluid is anechoic so intrahepatic vessels including portal veins and hepatic veins are visible.
The biliary ducts are thin tubes, the walls of which are 1.5 mm or less. The ducts increase in caliber distally from the liver.

Ultrasound
Transverse US liver,
showing homogeneous
parenchyma, the
hyperechoic
diaphragm the linear
portal vein, and the
parallel biliary duct
(arrow).
Hepatic vein branches
may be identified by their
radiating pattern as they
enter the IVC.
Normal liver doppler.

CT CT is often employed after US to image focal disease.
It is easy to compare in serial studies.
Air and bone do not interfere with CT examinations as with US.
CT angiography is a noninvasive means of imaging hepatic vasculature.
For diffuse hepatocellular disease, CT is probably the first study used, however not
as sensitive to liver lesions as MRI.
CT is the only commonly accepted means for analyzing abdominal trauma,
particularly of the liver. CT is reasonably accurate in the detection of trauma-related
abnormalities of the liver, biliary system, and pancreas.
MRI
MR imaging may be the most sensitive modality for detecting and characterizing diffuse diseases of the liver, including cirrhosis and hemochromatosis, especially when combined with contrast agents.
Newer MR pulse sequences, contrast agents, and fast scanning techniques arguably make MR imaging the optimal means for both detection and characterization of focal liver lesions of all types.
Often used to characterize focal lesions discovered during survey techniques like US or CT.
Angiography may be used to study collateral formation in cirrhosis.

Nuclear Medicine
It is most often used to further evaluate masses or tumors.
NM has only infrequent applications in diffuse disease.
Better utility in focal disease such as malignancy or
hemangioma.

Hepatobiliarry scintigraphy

Hepatobiliarry scintigraphy


Recommended