“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 1
#POMAD8#ChoosePOMA
Emergent and Urgent
Dermatology, Eruptions,
and Wound Care
G. Scott Drew, DO, FAAD, FAOCD
Dermatology Associates of Mid Ohio
POMA District 8
February 3, 2019
#POMAD8#ChoosePOMA
Disclosures Dr. Drew is a consultant for AbbVie, Inc., Sun
Pharmaceutical Industries, Ltd, Pfizer, Inc.,
Centocor Biopharmaceutical, Ortho
Pharmaceutical Corp., Galderma Laboratories, LP,
Medimetriks Pharmaceuticals, Inc., and Novartis
Pharmaceuticals Corp.
#POMAD8#ChoosePOMA
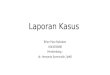
Acute Cutaneous Lupus
1
2
3
“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 2
#POMAD8#ChoosePOMA
Acute Cutaneous Lupus
#POMAD8#ChoosePOMA
Acute Cutaneous Lupus
ANA positive, Anti Ro, La Positive
Photo distributive
Need Systemic Work up
Initial tx, systemic corticosteroids, SPF
Antimalarials following negative G6PD
#POMAD8#ChoosePOMA
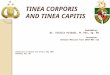
Subacute Cutaneous Lupus
4
5
6
“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 3
#POMAD8#ChoosePOMA
Subacute Sutaneous Lupus
Erythematosis
ANA negative, Ro and La positive
Fewer systemic symptoms
Less systemic co morbidities
Corticosteroids and steroid sparing agents, spf
#POMAD8#ChoosePOMA
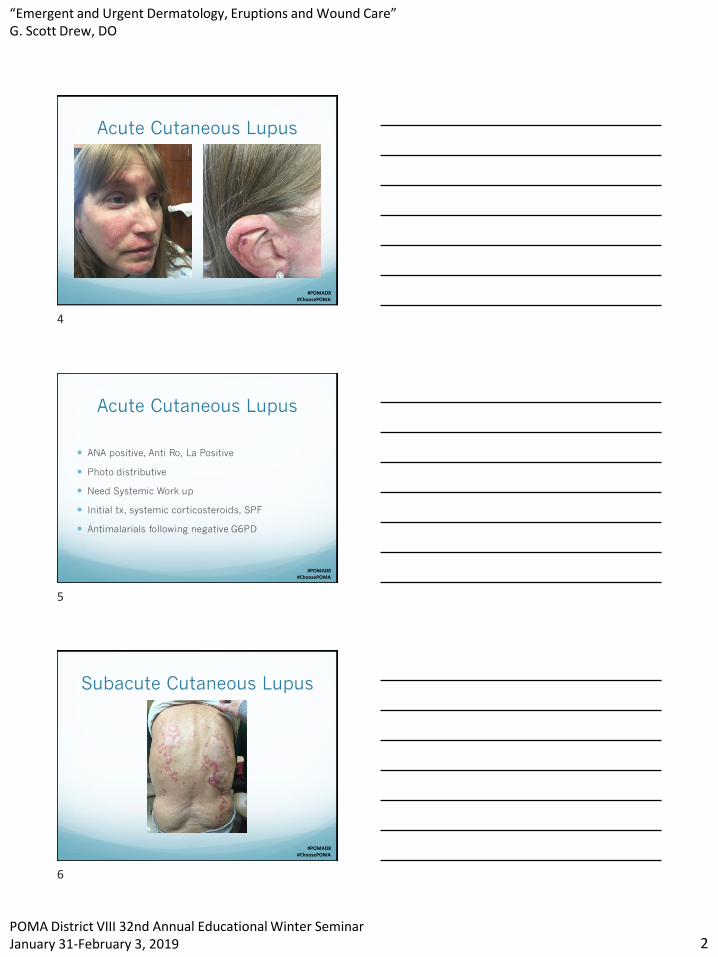
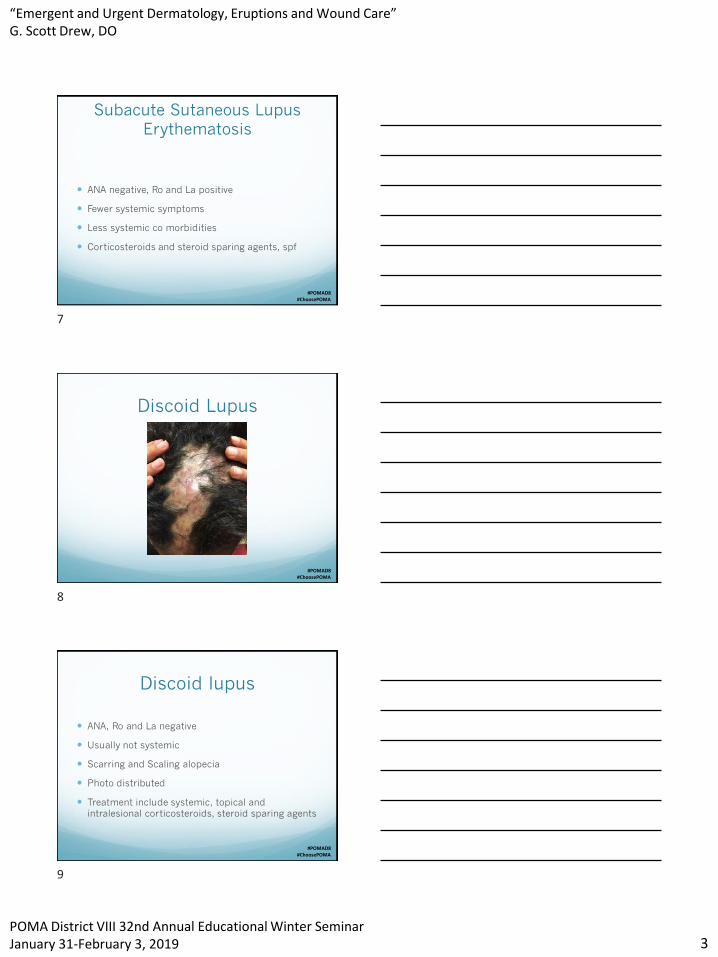
Discoid Lupus
#POMAD8#ChoosePOMA
Discoid lupus
ANA, Ro and La negative
Usually not systemic
Scarring and Scaling alopecia
Photo distributed
Treatment include systemic, topical and
intralesional corticosteroids, steroid sparing agents
7
8
9

“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 4
#POMAD8#ChoosePOMA
Acral Lentiginous Melanoma
#POMAD8#ChoosePOMA
Acral Lentiginous Melanoma Highest morbidity and Mortality of the Melanomas
Due to delay in Diagnosis
Bob Marley’s demise
Breslow depth
Work up and wide excision based on Breslow depth
FSE monthly by patient, quarterly by physician
Excision, not biopsy
#POMAD8#ChoosePOMA
Congential Nevus
10
11
12

“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 5
#POMAD8#ChoosePOMA
Congential (Hairy) Nevus
Very low malignant risk
High parental concern
Watch for changes
#POMAD8#ChoosePOMA
Bullous Pemphigoid
#POMAD8#ChoosePOMA
Bullous Pemphigoid Differentiate from Pemphigus, a far more serious Dx
H & E and DIF biopsy
Systemic corticosteroids
Steroid Sparing agents
Often burns out
13
14
15
“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 6
#POMAD8#ChoosePOMA
Stasis dermatitis
#POMAD8#ChoosePOMA
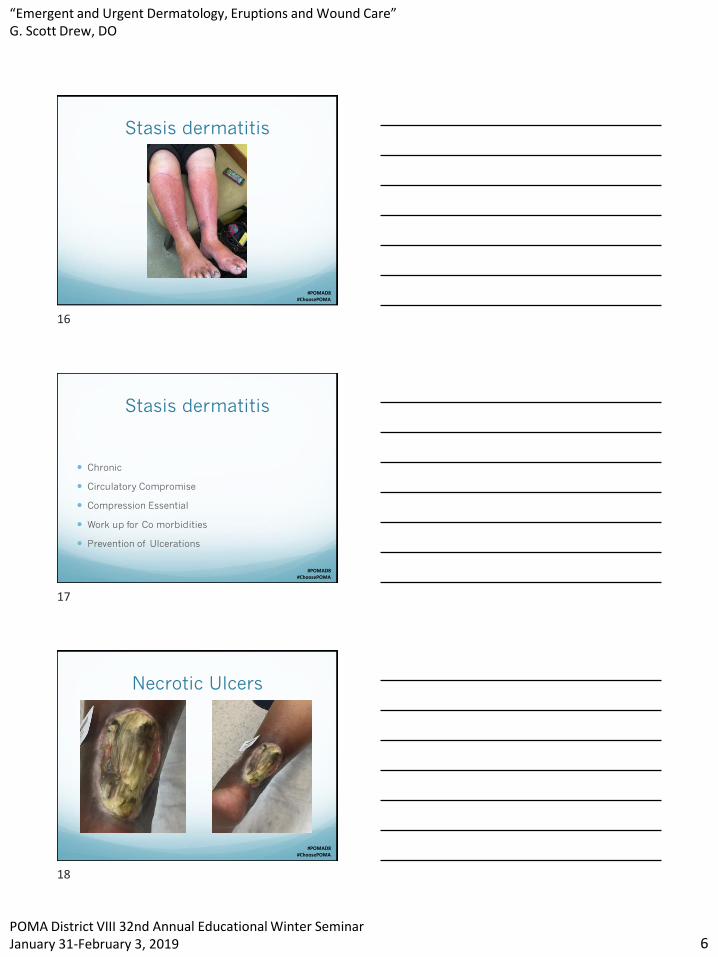
Stasis dermatitis
Chronic
Circulatory Compromise
Compression Essential
Work up for Co morbidities
Prevention of Ulcerations
#POMAD8#ChoosePOMA
Necrotic Ulcers
16
17
18
“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 7
#POMAD8#ChoosePOMA
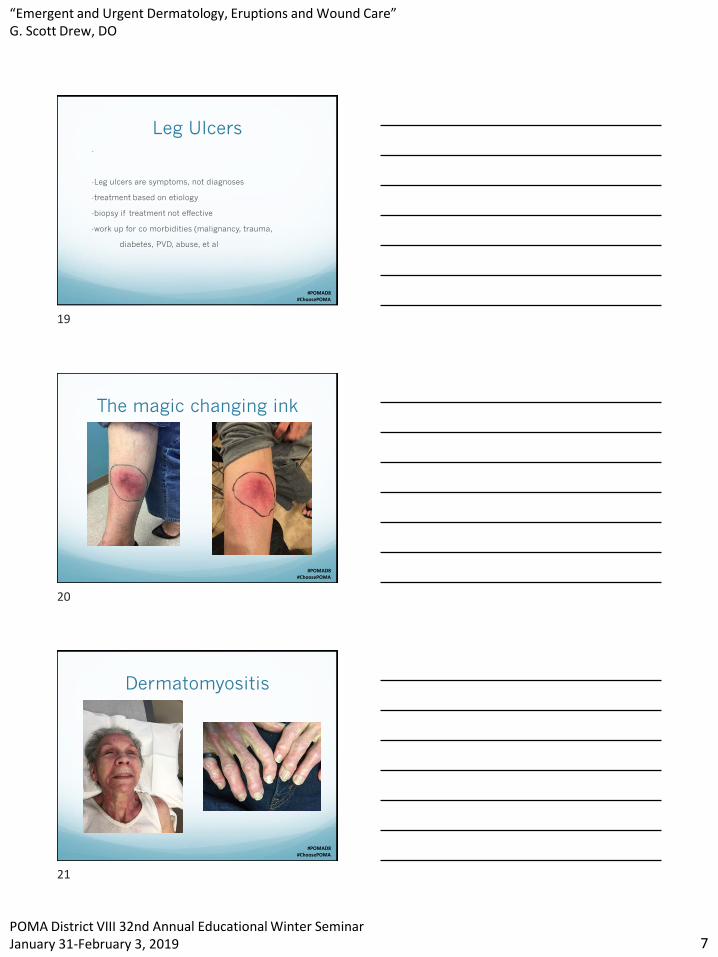
Leg Ulcers-
-Leg ulcers are symptoms, not diagnoses
-treatment based on etiology
-biopsy if treatment not effective
-work up for co morbidities (malignancy, trauma,
diabetes, PVD, abuse, et al
#POMAD8#ChoosePOMA
The magic changing ink
#POMAD8#ChoosePOMA
Dermatomyositis
19
20
21

“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 8
#POMAD8#ChoosePOMA
Dermatomyositis Classic but subtle clinical presentation, including
Heliotrope rash, shawl sign, gottron’s papule
Work up essential: CK, Aldolase, LDH, etc
50% with associated malignancy
Biopsy confirmation
Treatment systemic corticosteroids, steroid sparing
agents, spf, others
#POMAD8#ChoosePOMA
Pyogenic Granuloma
Etiology often trauma and microtrauma. Surgical treatment
asap
#POMAD8#ChoosePOMA
Foreign Body Granuloma
22
23
24
“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 9
#POMAD8#ChoosePOMA
Foreign Body Granuloma
History of injury important
Can be recent, usually remote
#POMAD8#ChoosePOMA
Erythema Multiforme Minor
#POMAD8#ChoosePOMA
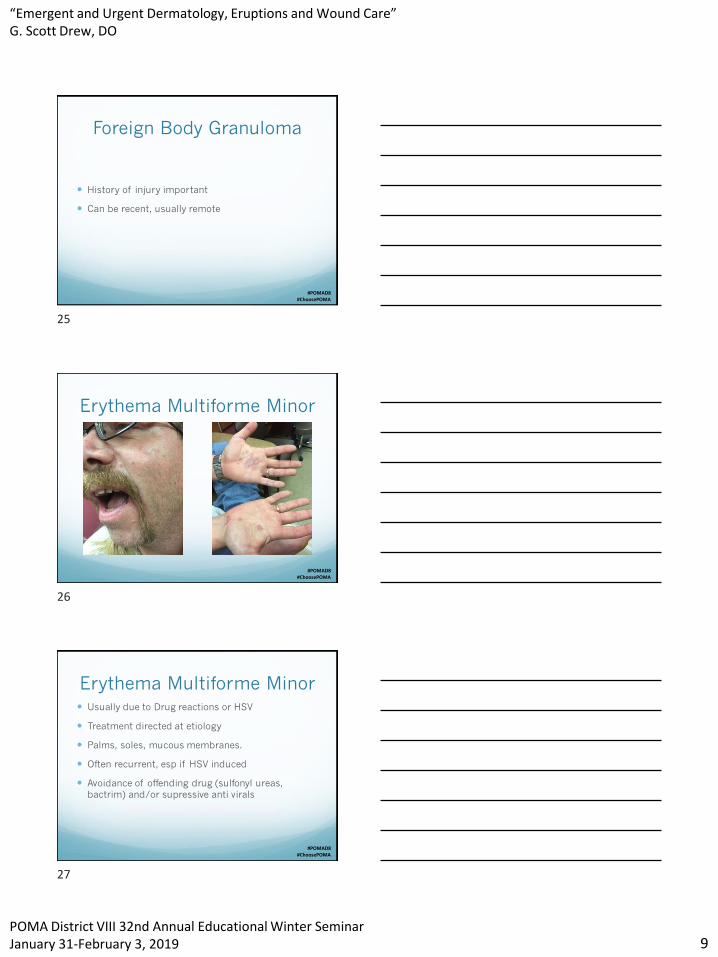
Erythema Multiforme Minor Usually due to Drug reactions or HSV
Treatment directed at etiology
Palms, soles, mucous membranes.
Often recurrent, esp if HSV induced
Avoidance of offending drug (sulfonyl ureas,
bactrim) and/or supressive anti virals
25
26
27

“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 10
#POMAD8#ChoosePOMA
EM Major/SJS
#POMAD8#ChoosePOMA
Molluscum contagiosum
#POMAD8#ChoosePOMA
Molluscum contagiosum
In toddlers, almost always associated with atopic
dermatitis.
If fewer than 10, treat the AD first
If greater than 10, treat the MC
If associated with wrestling, sports, STD, treat the
MC
28
29
30

“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 11
#POMAD8#ChoosePOMA
Atopic dermatitis
#POMAD8#ChoosePOMA
Atopic Dermatitis
A lifestyle, not a tube of hydrocortisone
Increased risk of Bacterial, viral, fungal and
parasitic skin infections
Associated allergy, otitis, asthma
Treatment: steroid sparing agents, emollients, mild
cleaners, food, mild detergents, anti pruritics,
bleach baths. Limited corticosteroids
#POMAD8#ChoosePOMA
31
32
33

“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 12
#POMAD8#ChoosePOMA
#POMAD8#ChoosePOMA
#POMAD8#ChoosePOMA
Pityriasis alba
34
35
36

“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 13
#POMAD8#ChoosePOMA
#POMAD8#ChoosePOMA
Cellulitis
#POMAD8#ChoosePOMA
Cellulits
Usually staph or strep
Community acquired vs Hospital acquired MRSA
Topical, oral, systemic antibiotics
History of prior manipulation, puncture,
penetration with home sterilized safety pins, awls,
needles, razors
37
38
39

“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 14
#POMAD8#ChoosePOMA
Pityriasis Rosea
#POMAD8#ChoosePOMA
Pityriasis Rosea Herald Patch
Self limited
Pruritis variable
Rx supportive, accurate diagnosis
DDX includes parapsoriasis, guttate psoriasis,
tinea, et al
#POMAD8#ChoosePOMA
Hidradenitis supprativa
40
41
42

“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 15
#POMAD8#ChoosePOMA
Hidradenitis supprativa
#POMAD8#ChoosePOMA
Hidradenitis Supprativa Symptoms progressive and can be debilitating
Surgical tx as a LAST resort
TNF alfa inhibitors are first line treatment
Alternative tx include isotretinoin, rifampin,
minocyline, spirinolactone, surgery
#POMAD8#ChoosePOMA
Basal Cell Carcinoma
43
44
45
“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 16
#POMAD8#ChoosePOMA
Basal Cell Carcinoma
Most common Human Malignancy >
1,000,000/year
Rare metastasis
Surgical excision is ToC
Radiation, MOHS, ED&C, Imiquimod, vismodegib
#POMAD8#ChoosePOMA
SCC
#POMAD8#ChoosePOMA
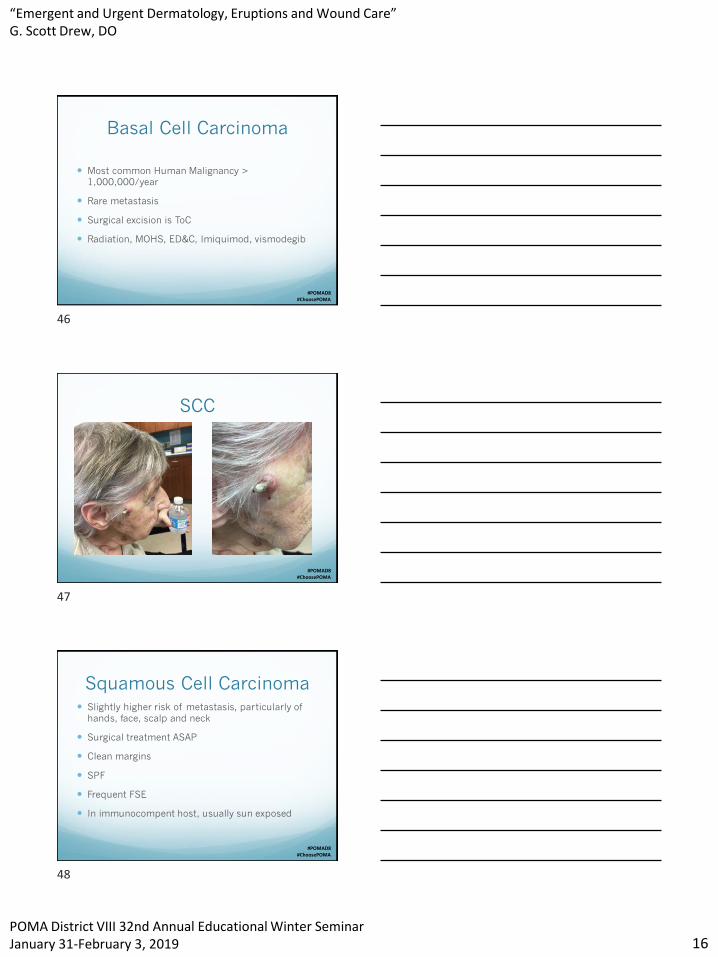
Squamous Cell Carcinoma Slightly higher risk of metastasis, particularly of
hands, face, scalp and neck
Surgical treatment ASAP
Clean margins
SPF
Frequent FSE
In immunocompent host, usually sun exposed
46
47
48

“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 17
#POMAD8#ChoosePOMA
Squamous Cell Carcinoma
#POMAD8#ChoosePOMA
Squamous Cell Carcinoma
#POMAD8#ChoosePOMA
49
50
51
“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 18
#POMAD8#ChoosePOMA
#POMAD8#ChoosePOMA
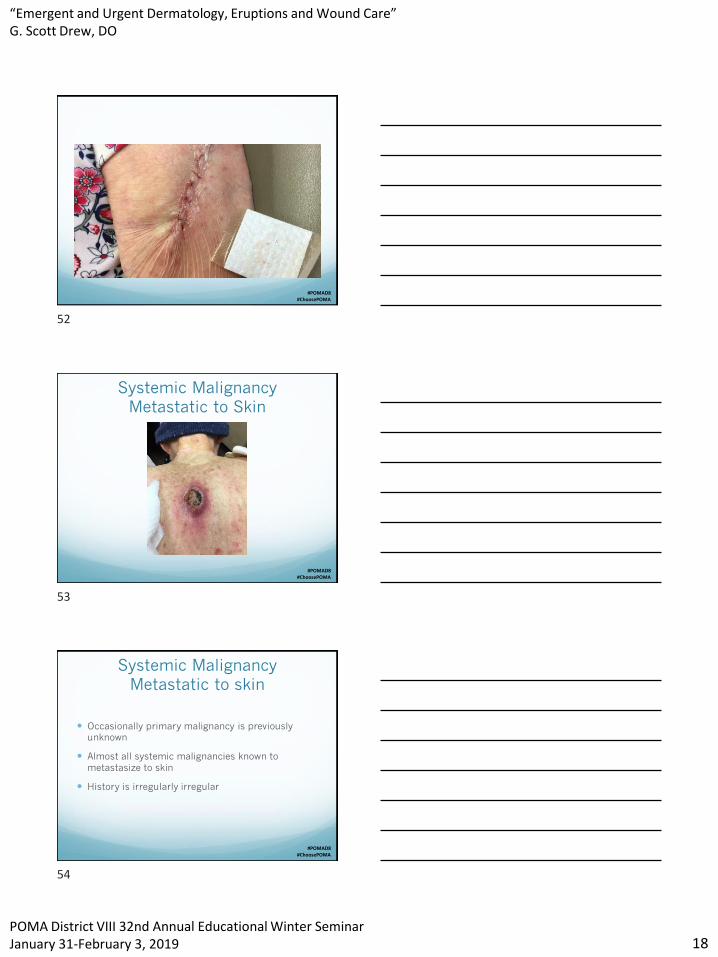
Systemic Malignancy
Metastatic to Skin
#POMAD8#ChoosePOMA
Systemic Malignancy
Metastatic to skin
Occasionally primary malignancy is previously
unknown
Almost all systemic malignancies known to
metastasize to skin
History is irregularly irregular
52
53
54
“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 19
#POMAD8#ChoosePOMA
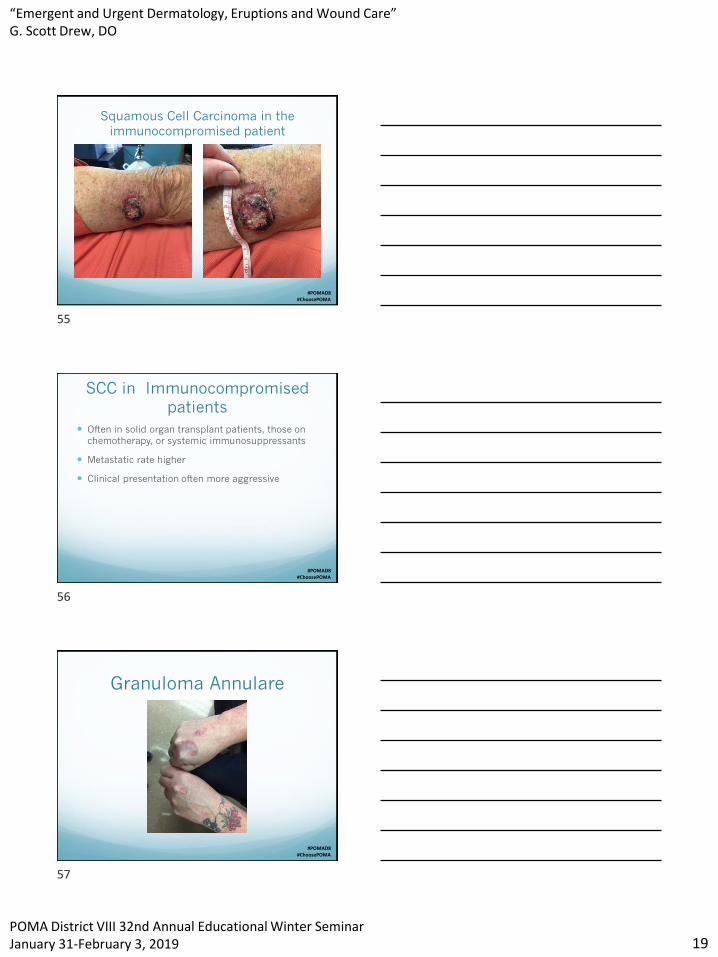
Squamous Cell Carcinoma in the
immunocompromised patient
#POMAD8#ChoosePOMA
SCC in Immunocompromised
patients
Often in solid organ transplant patients, those on
chemotherapy, or systemic immunosuppressants
Metastatic rate higher
Clinical presentation often more aggressive
#POMAD8#ChoosePOMA
Granuloma Annulare
55
56
57

“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 20
#POMAD8#ChoosePOMA
Granuloma Annulare
Distinct presentations in pediatrics vs adult pts
Often confused with tinea (no scale with GA)
Can be associated with DM
#POMAD8#ChoosePOMA
Tinea Capitis with Kerion
#POMAD8#ChoosePOMA
Tinea Capitis with Kerion Epidermophyton, Microsporum and Trichophyton
spp are causative organisms
Usually associated with regional adenopathy
Tinea capitis requires oral treatment
Griseofulvin 20mg/kg x 6 weeks, terbinafine by
weight
Kerion is a late sequellae.
Power of a Nickel (Powerofanickel.org) and DOcare
58
59
60
“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 21
#POMAD8#ChoosePOMA
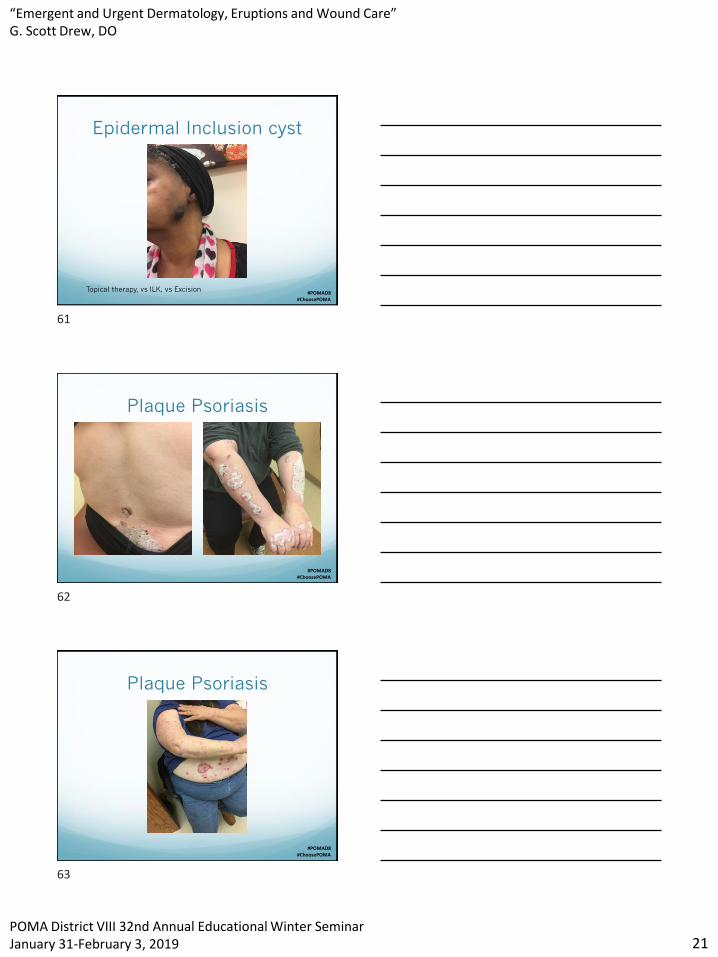
Epidermal Inclusion cyst
Topical therapy, vs ILK, vs Excision
#POMAD8#ChoosePOMA
Plaque Psoriasis
#POMAD8#ChoosePOMA
Plaque Psoriasis
61
62
63

“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 22
#POMAD8#ChoosePOMA
Treatment Options
for BSA > 10%
Narrowband UVB
Methotrexate
Acetretin
Apremilast (PDE 4 inhibitors)
Biologics
Combinaiton theraby
#POMAD8#ChoosePOMA
Sebopsoriasis with Isomorphic
phenoenon
#POMAD8#ChoosePOMA
Pediatric psoriasis
64
65
66

“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 23
#POMAD8#ChoosePOMA
One month of adalimumab
#POMAD8#ChoosePOMA
Compulsive excoriation
#POMAD8#ChoosePOMA
Compulsive
Excoriation/Neurodermatitis
Rarely a primary dermatitis
Often require multidisciplinary approach
Recognition of the patients participation in the
disease
Elimination of the picking/scratching/digging
Often requires psychoactive agents (doxepin,
fluvoxamine, benzodiazapines)
67
68
69

“Emergent and Urgent Dermatology, Eruptions and Wound Care”G. Scott Drew, DO
POMA District VIII 32nd Annual Educational Winter SeminarJanuary 31-February 3, 2019 24
#POMAD8#ChoosePOMA
Cutaneous Sarcoid
#POMAD8#ChoosePOMA
Diabetic foot disease
70
71
Recommended