Diabetic Nephropathy
MEGAHID ABUELMAGDENDOCRINOLOGY AND DIABETES UNIT
MANSOURA UNIVERSITY

Epidemiologythe size of the problem:
the evidences
Diabetic nephropathy (ies) represents thefirst and major cause of kidney deficiency
in western and now in many developing countries
Diabetic nephropathy (ies) represents a subpopulation of diabetic subjects
with the highest risk of cardiovascular events

TRENDS IN INCIDENCE AND PREVALENCETRENDS IN INCIDENCE AND PREVALENCE OF ESRD OF ESRD DUE TO DIABETES IN WESTERN DUE TO DIABETES IN WESTERN COUNTRIES COUNTRIES « Europe » 1966-90« Europe » 1966-90
ANNUAL CHANGE OF NUMBER (%) OF ANNUAL CHANGE OF NUMBER (%) OF PATIENTS STARTING DIALYSIS THERAPY PATIENTS STARTING DIALYSIS THERAPY IN JAPAN 1984-2000IN JAPAN 1984-2000

Surv
ival
cur
ve C
V
1
0.90.8
0.7
0.6
0.5
00 10 30 50 70 90 stroke Coronary events
(p < 0.001)In
cide
nce
(%)
Months
AB
C
p < 0.001
0
10
20
30
40
A: U-Prot < 150 mg/l B: U-Prot 150–300 mg/l C: U-Prot > 300 mg/l
Miettinen H et a l. Stroke 1996; 27: 2033-39
Proteinuria : predicitve marker of CV eventsin type 2 DM

Natural history of diabetic nephropathy
• Is it the same story in type 1 and in type 2 diabetic patients ?
• A majority of same features

Diabetic Nephropathy Definition
Normal albuminuria Microalbuminuria Proteinuria patent or clinical(Macroalbuminuria)
30 mg/24h*ou 20 µg/min**
300 mg/24h*ou 200
µg/min**
* urines of 24 hours** recueil sur 4 heures
40% des patients diabétiques de type 2 évoluent vers une néphropathie diabétique1
1 Hollenberg NK. J Hypertens 1997,15(S7): 7-13
Prevention Treatment Treatment

Natural history of type 1 diabetic nephropathy
Hyperglycaemia
Increased GFR
Microalbuminuria
Frank proteinuria
Decreased GFR
Possible development of nephrotic syndrome
End-stage renal disease
NORMAL GFR
INCREASED GFR
DECLINING GFR 5 – 10 years

Natural history of type 2 diabetic nephropathy
Clinical type 2 diabetes
Functional changes
Structural changes
Rising blood pressure
Microalbuminuria
ProteinuriaRising serum
creatinine levelsEnd-stage renal
diseaseCardiovascular death
0 2 5 10 20 30Years

-3
120
1.0
15
0
150
0.8
10
3
150
0.8
10
15
120
1.0
15
20
60
> 2.0
> 30
25
< 10
> 10
< 100
-3
Prior to Onset of Diabetes
0
Onset of
Diabetes
3
Onset of Diabetic Glomerulosclerosis
15
Onset of
Proteinuria
20
Onset of
Azotemia
25
End-stageRenalFailure
GFR (ml/min)
Serum creatinin (mg/dl)
Serum Urea Nitrogen (mg/dl)
Time (Years)
Silent Period
Natural history of diabetic nephropathy

Incidence of DN (%) in type 1 DM according to duration of diabetes
Maximum prevalence reachs 50% of the patients in both diabetes (usually one third)

The classical lesions have been firstly described in type 2 DM
Normal
Diffuse mesangial expansionreduction of open capillaries
KW nodules and thickened Bowman ’s capsule and capillary basement membraneA
B
C
D

Normal capillary surface exchange Mesangial expansionDecrease of capillary surfaceshyperfiltration
Effects on podocytes arrangementand nephron protection
Thickening of GBM

Capillary
GBM
Feets ’ podocytesUS
E
Nephrin
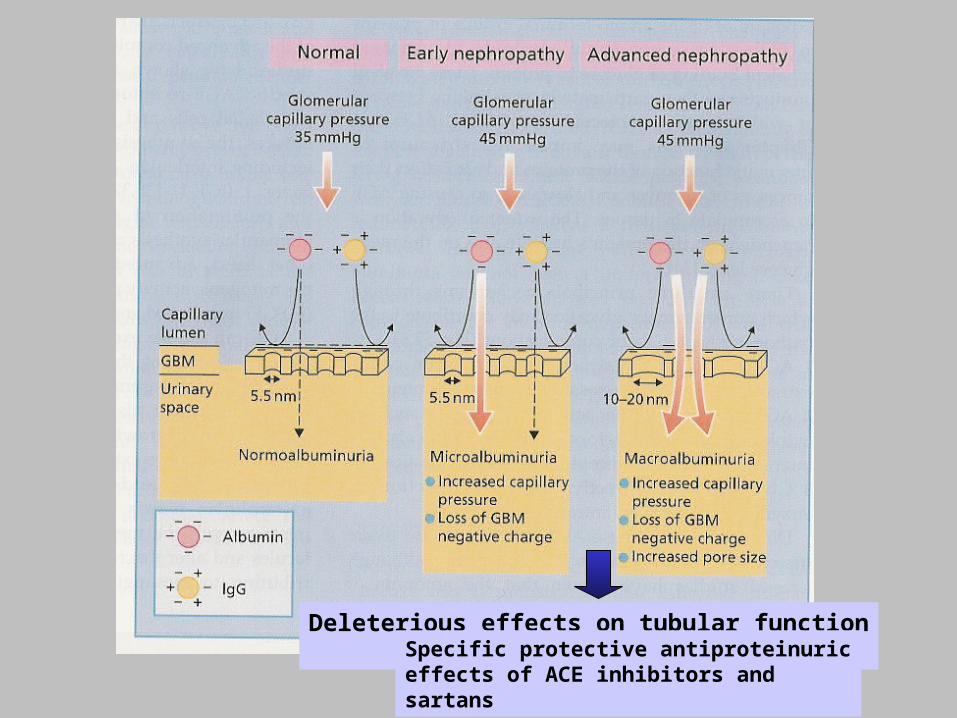
Deleterious effects on tubular functionand interstitiumSpecific protective antiproteinuric
effects of ACE inhibitors andsartans


Negative relation between proteinuria and the loss of kidney function
Yokoka et al. Risk Factors for Progression of Diabetic Nephropathy
Am.J.N,1995;15:48854 p/4,2 ans0
-2
-4
-6
Curve 1/Creat/time
1 2 3Grade
of proteinuria
Comparison of the slope of the regression line for the reciprocal of Cr concentration over time among three groups of patients based on the degree of proteinuria. ANOVA showed a significant difference among three groups (p<0,05), and the slope in patients with grade 3 of proteinuria in dipstick test had greater negative value than in those with grade 1 of proteinuria

Natural course and pathogenic role of
• Hyperglycemia• high blood pressure levels• and genotypes (s) DD/II/ID

Flux/Stretching/Pressure
Vasopeptidases: angiotensins endothelins, NO synthases…..
TGF
VEGF
Glucose
Advanced glycation end products (AGEs)
PKCII
Polyols
Metabolic and Haemodynamic Interactions
Glomerulosclerosis
Interstitial Fibrosis Proteinuria
Cross-linking Extra-cellular Matrix (EMC)
ECM Vascular permeability
O2-

Physiological effects ofangiotensin II on the kidney

VC
VasodilatationVasodilatation
Vasodilatation
Angiotensin 2
P Cap
ACE Inhibitors

Glomerular &Extra glomerular lesions
• Relation angiotensin II and TGF B• tubular• interstitial• capillariy lesions

Colocalisation angio2 - TGFb
Major role of TGFb and Angiotensin II

Histo-morphometric aspect of the progression of the kidney
lesions at 2 years interval without ACE Inh57 years old woman
Cordonnier D, P Zaoui et S Halimi et al. JASN 1999 ; 10 : 1253
Int = + 16.97 %Mésg = + 25.99 %Tub = - 14.05 %
Alb = 3877 mg/24h Alb = 16100 mg/24h
Deterioration of vessels, renal tubules and interstitium with massive proteinuria

Quantification of glomerular and interstitial fibrosis
Magnification x 10 Ph. Zaoui and S Halimi

Renal Dysfunction Is Common in Patients with Type 2 Diabetes
Russo E, et al. Diabetes Metab Syndr Obes. 2013; 6: 161–170.

Young patients with T2DM had greater Young patients with T2DM had greater risks of developing ESRD compared with risks of developing ESRD compared with
patients with T1DMpatients with T1DM
ESRD: End- Stage Renal DiseaseLuk AO, et al. Diabetes Care. 2014 Jan;37(1):149-57

Rate of Kidney Diseases in Egypt is Rate of Kidney Diseases in Egypt is 36.4* with About 5.19% Deaths 36.4* with About 5.19% Deaths
*Per 100,000http://www.worldlifeexpectancy.com/cause-of-death/kidney-disease/by-country/ accessed 2012 Oct.


Current proportional contribution of the most Current proportional contribution of the most common causes of end-stage renal disease in North common causes of end-stage renal disease in North
African countriesAfrican countries
GN: GlomerulonephritisRashad S. Barsoum. Kidney International Supplements (2013) 3, 164–166
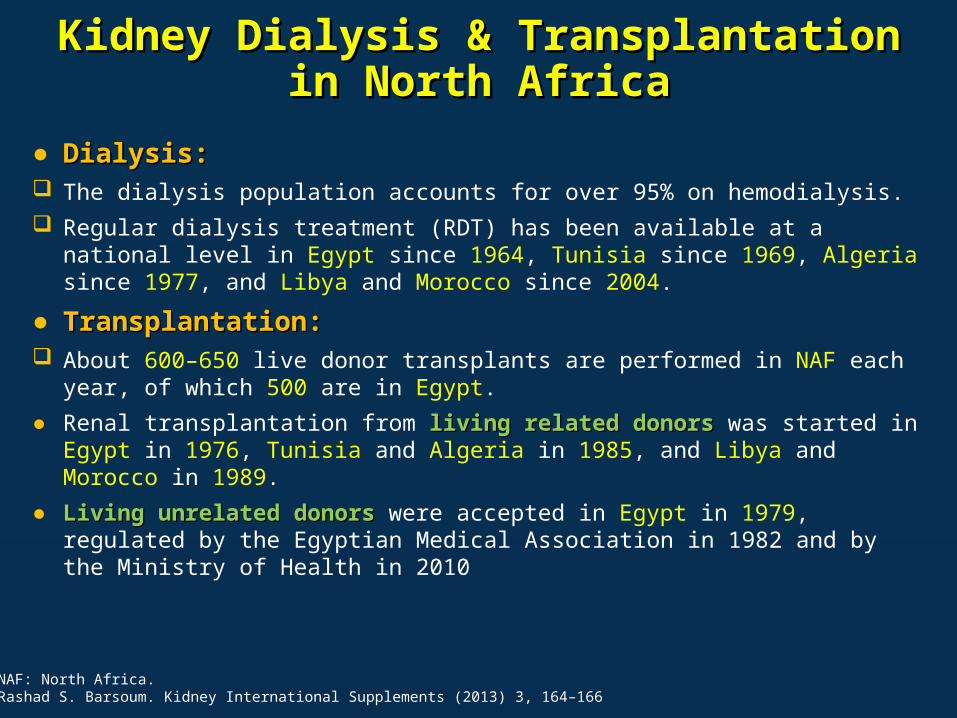
Kidney Dialysis & Transplantation in North Kidney Dialysis & Transplantation in North AfricaAfrica
● Dialysis:Dialysis: The dialysis population accounts for over 95% on hemodialysis. Regular dialysis treatment (RDT) has been available at a national level in
Egypt since 1964, Tunisia since 1969, Algeria since 1977, and Libya and Morocco since 2004.
● Transplantation:Transplantation: About 600–650 live donor transplants are performed in NAF each year, of
which 500 are in Egypt.● Renal transplantation from living related donors living related donors was started in Egypt in
1976, Tunisia and Algeria in 1985, and Libya and Morocco in 1989. ● Living unrelated donors Living unrelated donors were accepted in Egypt in 1979, regulated by the
Egyptian Medical Association in 1982 and by the Ministry of Health in 2010
NAF: North Africa.Rashad S. Barsoum. Kidney International Supplements (2013) 3, 164–166

A1 A2 A3
Normal to mildly
increased
Moderately increased
Severely increased
<30 mg/g <3 mg/mmol
30-300 mg/g 3-30 mg/mmol
>300 mg/g >30 mg/mmol
CURRENT CHRONIC KIDNEY DISEASE CURRENT CHRONIC KIDNEY DISEASE (CKD) NOMENCLATURE USED BY (CKD) NOMENCLATURE USED BY
KDIGOKDIGO• CKD is defined as abnormalities of kidney structure or function, present for >3
months, with implications for health and CKD is classified based on cause, GFR category, and albuminuria category (CGA).
KDIGO Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl. 2013;3:136-150. http://www.kdigo.org/clinical_practice_guidelines/pdf/CKD/KDIGO_2012_CKD_GL.pdf Accessed February 26, 2013
G1 Normal or high ≥90
G2 Mildly decreased 60-89
G3a Mildly to moderately decreased 45-59
G3b Moderately to severely decreased 30-44
G4 Severely decreased 15-29
G5 Kidney failure <15
Persistent albuminuria categories Description and range
Green: low risk (if no other markers of kidney disease, no CKD); Yellow: moderately increased risk; Orange: high risk; Red, very high risk.
Prognosis of CKD by GFR and Albuminuria Categories:
KDIGO 2012

ADA 2014 Definitions of ADA 2014 Definitions of Abnormalities in Albumin ExcretionAbnormalities in Albumin Excretion
Category
Spot collection (µg/mg creatinine)
Normal <30Increased urinary albumin excretion* ≥30
ADA. VI. Prevention, Management of Complications. Diabetes Care 2014;37(suppl 1):S44; Table 11
*Historically, ratios between 30 and 299 have been called microalbuminuria and those 300 or greater have been called macroalbuminuria (or clinical albuminuria).

Stages of Chronic Kidney DiseaseStages of Chronic Kidney Disease
Stage Description
GFR (mL/min per 1.73 m2
body surface area)
1 Kidney damage* with normal or increased GFR
≥90
2 Kidney damage* with mildly decreased GFR
60–89
3 Moderately decreased GFR 30–594 Severely decreased GFR 15–295 Kidney failure <15 or dialysis
*Kidney damage defined as abnormalities on pathologic, urine, blood, or imaging tests. GFR = glomerular filtration rate
ADA. VI. Prevention, Management of Complications. Diabetes Care 2014;37(suppl 1):S44; Table 12

Risk Factors of Diabetic NephropathyRisk Factors of Diabetic Nephropathy
Farag et al, Nephron Clin Pract 2011;119:c317–c323

Fox et al , Lancet 2012; 380: 1662–73

Increasing Mortality Risk 1·2–1·9 times in Increasing Mortality Risk 1·2–1·9 times in participants with diabetes than in those without participants with diabetes than in those without
diabetes across the entire range of eGFRdiabetes across the entire range of eGFR
Fox et al , Lancet 2012; 380: 1662–73



The Evidence Confirms That: The Evidence Confirms That:
• Both studies (UKPDS, DCCT) (UKPDS, DCCT) demonstrated consistent major salutary effects of intensive therapy on microvascular salutary effects of intensive therapy on microvascular complications compared with conventional therapycomplications compared with conventional therapy, with the benefits roughly proportional to the degree of HbA1c separation achieved.
• Moreover, long-term follow- up long-term follow- up of the DCCT and UKPDS cohorts has shown durable effects of early intervention durable effects of early intervention even after the differences in glycaemia between the original intervention groups had dissipated, referred to as metabolic metabolic memory (DCCT) and legacy effect (UKPDS).memory (DCCT) and legacy effect (UKPDS).
Nathan DM. Arch Intern Med. 2012 May 28;172(10):769-70.

Jindal A, et al. Endocrinol Metab Clin North Am. 2013 Dec2013 Dec;42(4):789-808

Cardio-Renal Syndrome Cardio-Renal Syndrome The interrelationship between adiposity and The interrelationship between adiposity and
maladaptive changes in the heart and kidneymaladaptive changes in the heart and kidney
Jindal A, et al. Endocrinol Metab Clin North Am. 2013 Dec2013 Dec;42(4):789-808

ConclusionConclusion
• Better glycemic and blood pressure control can delay the onset and slow the progression of kidney disease in patients with diabetes.
• Older oral hypoglycemic agents is either contraindicated or requires dosage adjustment in CKD.
• New medications for diabetes have been approved recently and many can be used safely in patients with CKD, thus providing treatment alternatives for better glycemic control in patients who are reluctant to use insulin.
CKD: Chronic Kidney Disease.Jindal A, et al. Endocrinol Metab Clin North Am. 2013 Dec2013 Dec;42(4):789-808
Coca, et al. Arch Intern Med. 2012;172(10):761-769
Objective: Objective: To summarize the benefits of intensive vs conventional glucose control on kidney-related outcomes for adults with type 2 diabetes.
Methods: Methods: Evaluated 7 trials involving 28 065 adults for 2 to 15 years. Comparing conventional control, with intensive glucose control in reducing the risk for microalbuminuria and macroalbuminuria.

The Risk of Microalbuminuria Has Been The Risk of Microalbuminuria Has Been Reduced by 14 % with Intensive TherapyReduced by 14 % with Intensive Therapy
Coca, et al. Arch Intern Med. 2012;172(10):761-769

The Risk of Macroalbuminuria Has Been The Risk of Macroalbuminuria Has Been Reduced by 26 % with Intensive TherapyReduced by 26 % with Intensive Therapy
Coca, et al. Arch Intern Med. 2012;172(10):761-769

Glycemic Management in ESRD and Glycemic Management in ESRD and Earlier Stages of CKDEarlier Stages of CKD
• The management of hyperglycemia in patients with The management of hyperglycemia in patients with kidney failure has special challenges. The difficulty is due kidney failure has special challenges. The difficulty is due in part to the in part to the complexity of treatment complexity of treatment and in part to and in part to lack lack of convincing data supporting the benefits of tight of convincing data supporting the benefits of tight glycemic controlglycemic control..
• Insulin resistance increases Insulin resistance increases in CKD due to accumulation in CKD due to accumulation of of uremic toxinsuremic toxins, , chronic inflammationchronic inflammation, , excess visceral excess visceral fatfat, , oxidative stressoxidative stress, , metabolic acidosimetabolic acidosis, and s, and vitamin D vitamin D deficiencydeficiency..
• HbA1c level may HbA1c level may overestimate glycemic control overestimate glycemic control in kidney in kidney patients: HbA1c levels patients: HbA1c levels appear to be lowerappear to be lower, leading to , leading to underestimation of hyperglycemia.underestimation of hyperglycemia.
Williams ME, et al. Am J Kidney Dis. 2014 Feb2014 Feb;63(2 Suppl 2):S22-38.

Glycemic Management in ESRD and Glycemic Management in ESRD and Earlier Stages of CKDEarlier Stages of CKD
• Other measures of glycemic control, such as Other measures of glycemic control, such as glycated glycated albuminalbumin, may be more useful in CKD. Glycated albumin , may be more useful in CKD. Glycated albumin increasingly is proposed as a increasingly is proposed as a better measure of glycemic better measure of glycemic control in patients with diabetes and CKDcontrol in patients with diabetes and CKD
• aggressive glycemic control has been shown to alter the aggressive glycemic control has been shown to alter the clinical course of early diabetic kidney disease, data clinical course of early diabetic kidney disease, data supporting the benefits of tight glycemic control on supporting the benefits of tight glycemic control on outcomes in patients with advanced CKD (including outcomes in patients with advanced CKD (including ESRD) are lacking. ESRD) are lacking. In the absence of better clinical trial In the absence of better clinical trial datadata, , glycemic management continues to be based on glycemic management continues to be based on individualized decision makingindividualized decision making..
Williams ME, et al. Am J Kidney Dis. 2014 Feb2014 Feb;63(2 Suppl 2):S22-38.

Higher Glycated Albumin Rates are Higher Glycated Albumin Rates are Associated With Increased HospitalizationAssociated With Increased Hospitalization
Williams ME, et al. Am J Kidney Dis. 2014 Feb2014 Feb;63(2 Suppl 2):S22-38.

Use of conventional antidiabetic drugs in Use of conventional antidiabetic drugs in T2DM with CKDT2DM with CKD
Russo E, et al. Diabetes Metab Syndr Obes. 2013; 6: 161–170.
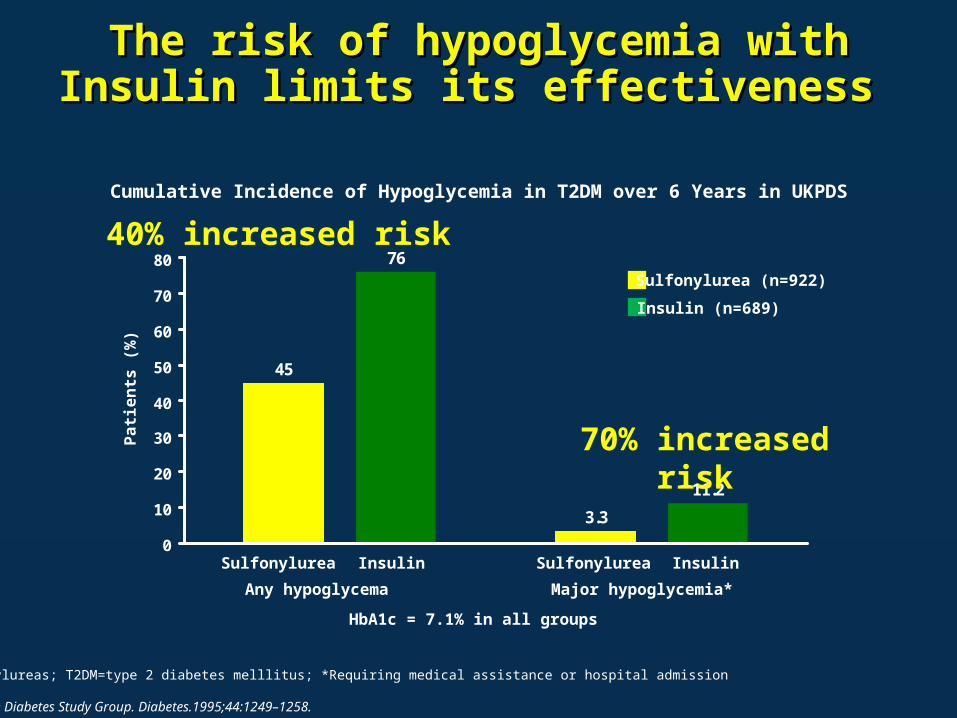
The risk of hypoglycemia with Insulin limits The risk of hypoglycemia with Insulin limits its effectiveness its effectiveness
SUs=sulfonylureas; T2DM=type 2 diabetes melllitus; *Requiring medical assistance or hospital admission
UK Prospective Diabetes Study Group. Diabetes.1995;44:1249–1258.
Cumulative Incidence of Hypoglycemia in T2DM over 6 Years in UKPDS
45
3.3
76
11.2
0
10
20
30
40
50
60
70
80Sulfonylurea (n=922)
Insulin (n=689)
Sulfonylurea Insulin Sulfonylurea Insulin
Patie
nts (
%)
Any hypoglycema Major hypoglycemia*
HbA1c = 7.1% in all groups
70% increased risk
40% increased risk

Renal impairment is a well recognized Renal impairment is a well recognized predisposing factor to hypoglycemia predisposing factor to hypoglycemia
• About 40% to 50% of the insulin reaching the About 40% to 50% of the insulin reaching the circulation is circulation is metabolizedmetabolized by the kidney , A process by the kidney , A process that is obviously that is obviously compromised in patients with renal compromised in patients with renal failure.failure.
• GluconeogenesisGluconeogenesis occurs mainly in the liver with a occurs mainly in the liver with a small amount also occurring in small amount also occurring in the cortex of the the cortex of the kidneykidney
• Accumulation of hypoglycemic agents Accumulation of hypoglycemic agents
Russo E, et al. Diabetes Metab Syndr Obes. 2013; 6: 161–170.http://www.medscape.org/viewarticle/437273http://www.elmhurst.edu/~chm/vchembook/604glycogenesis.html

Accordingly, Recommended Goals for Accordingly, Recommended Goals for Management of HyperglycemiaManagement of Hyperglycemia
– Target hemoglobin A1c (HbA1c) of ̴ 7.0% to prevent or delay progression of the microvascular complications of diabetes, including DKD
– An HbA1c target of <7.0% in patients at risk of hypoglycemia.
– Target HbA1c be extended above 7.0% in individuals with co-morbidities or limited life expectancy and risk of hypoglycemia
National Kidney Foundation. KDOQI Clinical Practice Guideline for Diabetes and CKD: 2012 update. Am J Kidney Dis. 2012;60(5):850-886.

The vicious circle leads to worsen of RI The vicious circle leads to worsen of RI
Adapted from: Jindal A, et al. Endocrinol Metab Clin North Am. 2013 Dec;42(4):789-808

Effective Management of CKD in Effective Management of CKD in DiabetesDiabetes
• Intensive control of blood glucose • Control of blood pressure• Treatment with Angiotensin Converting
Enzyme (ACE) Inhibitors and Angiotensin Receptor Blockers (ARBs)
• Multifactorial interventions including a combination of improved glucose control, blood pressure control, lipid lowering, aspirin, smoking cessation, exercise programs and dietary intervention
NICE Diabetes with Kidney Disease: Key Facts MARCH 2011

Current proportional contribution of the most Current proportional contribution of the most common causes of end-stage renal disease in North common causes of end-stage renal disease in North
African countriesAfrican countries
GN: GlomerulonephritisRashad S. Barsoum. Kidney International Supplements (2013) 3, 164–166

Young patients with T2DM had greater Young patients with T2DM had greater risks of developing ESRD compared with risks of developing ESRD compared with
patients with T1DMpatients with T1DM
ESRD: End- Stage Renal DiseaseLuk AO, et al. Diabetes Care. 2014 Jan;37(1):149-57

Control of Blood PressureControl of Blood Pressure

CHEP 2014 (BP target)CHEP 2014 (BP target)¹¹Target Blood pressure Should be less than 140/90 mmHg in most patients, Target Blood pressure Should be less than 140/90 mmHg in most patients,
including those with chronic kidney disease. including those with chronic kidney disease.
ESC 2013 (BP target)ESC 2013 (BP target)²²Target Blood pressure <140/90 mmHg should be considered in patients with Target Blood pressure <140/90 mmHg should be considered in patients with
diabetic or non-diabetic CKD.diabetic or non-diabetic CKD.
JNC IV (BP target)JNC IV (BP target)³³In patients with CKD, initiate treatment at SBP ≥140 mmHg or DBP ≥90 In patients with CKD, initiate treatment at SBP ≥140 mmHg or DBP ≥90
mmHg, and treat to achieve SBP <140 mmHg and DBP <90 mmHg.mmHg, and treat to achieve SBP <140 mmHg and DBP <90 mmHg.
Blood Pressure Target Goals in CKD Blood Pressure Target Goals in CKD patientspatients
1: Canadian Hypertension Education Program (CHEP) 2014 Recommendation, adopted from: https://www.hypertension.ca/chep. Accessed at 5/2/20142: Mancia G, et al. J Hypertens. 2013 Jul;31(7):1281-3573: James PA, et al. JAMA. 2013 Dec 18. [Epub ahead of print]

BP and RAAS interruption BP and RAAS interruption 1/21/2
• Individualize BP targets and agents.• Inquire about postural dizziness and check for postural
hypotension regularly when treating CKD patients with BP-lowering drugs.
• We recommend that in both diabetic and non-diabetic adults with CKD and urine albumin excretion ≥30 mg/ 24 hours whose office BP is consistently >140/90mm Hg be treated with BP-lowering drugs to maintain a BP that is consistently ≤140/90mm Hg
• We suggest that in both diabetic and non-diabetic adults with CKD and with urine albumin excretion of ≥30 mg/24 hours whose office BP is consistently >130/80mm Hg be treated with BP-lowering drugs to maintain a BP that is consistently ≤130/80mm Hg
KDIGO Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl. 2013;3:136-150. http://www.kdigo.org/clinical_practice_guidelines/pdf/CKD/KDIGO_2012_CKD_GL.pdf Accessed February 26, 2013

BP and RAAS interruption BP and RAAS interruption 2/22/2
• We suggest that an ARB or ACE-I be used in diabetic adults with CKD and urine albumin excretion 30–300 mg/ 24 hours.
• We recommend that an ARB or ACE-I be used in both diabetic and non-diabetic adults with CKD and urine albumin excretion >300 mg/24 hours
• There is insufficient evidence to recommend combining an ACE-I with ARBs to prevent progression of CKD.
• We suggest that an ARB or ACE-I be used in children with CKD in whom treatment with BP-lowering drugs is indicated, irrespective of the level of proteinuria.
KDIGO Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl. 2013;3:136-150. http://www.kdigo.org/clinical_practice_guidelines/pdf/CKD/KDIGO_2012_CKD_GL.pdf Accessed February 26, 2013

RAAS System Blockers in Diabetic RAAS System Blockers in Diabetic Nephropathy Nephropathy
National Kidney Foundation. KDOQI Clinical Practice Guideline for Diabetes and CKD: 2012 update. Am J Kidney Dis. 2012;60(5):850-886.

ScreeningScreening• Assess urine albumin excretion annually
– In type 1 diabetic patients with diabetes duration of ≥5 years
– In all type 2 diabetic patients at diagnosis
ADA 2014 Recommendations:ADA 2014 Recommendations:Nephropathy (1)Nephropathy (1)
ADA. VI. Prevention, Management of Complications. Diabetes Care 2014;37(suppl 1):S42

Treatment (1)Treatment (1)• ACE inhibitor, ARB not recommended in diabetic patients
with normal blood pressure, albumin excretion <30 mg/24 h for primary prevention of diabetic kidney disease
• Nonpregnant patient with modestly elevated (30–299 mg/day) or higher levels (>300 mg/day) of urinary albumin excretion
– Use either ACE inhibitors or ARBs (not both)
ADA 2014 Recommendations:ADA 2014 Recommendations:Nephropathy (2)Nephropathy (2)
ADA. VI. Prevention, Management of Complications. Diabetes Care 2014;37(suppl 1):S42
Treatment (2)Treatment (2)• For people with diabetes and diabetic kidney disease
(albuminuria >30 mg/24 h), reducing dietary protein below usual intake not recommended
– When ACE inhibitors, ARBs, or diuretics are used, monitor serum creatinine, potassium levels for increased creatinine or changes in potassium
ADA 2014 Recommendations:ADA 2014 Recommendations:Nephropathy (3)Nephropathy (3)
ADA. VI. Prevention, Management of Complications. Diabetes Care 2014;37(suppl 1):S42–S43
Treatment (3)Treatment (3)• Reasonable to continue monitoring urine albumin
excretion to assess both response to therapy and disease progression
• When eGFR is <60 mL/min/1.73 m2, evaluate and manage potential complications of CKD
• Consider referral to a physician experienced in care of kidney disease
– Uncertainty about etiology; difficult management issues; advanced kidney disease
ADA 2014 Recommendations:ADA 2014 Recommendations:Nephropathy (4)Nephropathy (4)
ADA. VI. Prevention, Management of Complications. Diabetes Care 2014;37(suppl 1):S43

Management of Dyslipidemia in Management of Dyslipidemia in Diabetes and CKDDiabetes and CKD

Management of Dyslipidemia in Diabetes Management of Dyslipidemia in Diabetes and CKDand CKD
• NKF recommend using LDL-C lowering medicines, such as statins or statin/ezetimibe combination, to reduce risk of major atherosclerotic events in patients with diabetes and CKD, including those who have received a kidney transplant.
• NKF recommend not initiating statin therapy in patients with diabetes who are treated by dialysis
NK: National Kidney Foundation. KDOQI Clinical Practice Guideline for Diabetes and CKD: 2012 update. Am J Kidney Dis. 2012;60(5):850-886.

Thanks

Interstitial fibrosis Results of masks IAS animal models
0
10
20
30
40
50
controlD2 UntreatedCaptoprilOmapatrilat
% of interstitial collagen
*§ §
* p<0.01 vs CTRL
§ p<0.05 vs D2UPh. Zaoui and S Halimi


Genetic?Angiotensin II
Apo EeNOS
Glut 1 polymorphism...

Influence of the genotype DDon the angiotensin II plasma concentrations after angiotensin I infusion
DD
II


Prevention & Treatment of early and late DN
• Intensive control of glycemia and • Blood pressure with all anti hypertensive
drugs ? BUT• specific roles of angiotensin system acting
drugs: ACE I and Sartans• Smoking• Lipids

Type 1 DMDCCT and EDIC study
• 1993 and 2002• prevention of DN by tight blood glucose
control• the benefit is still present 6 years after the
end of the trial

Renal lesions are reversed 10 years after pancreatic transplantation
Fioretto P. N Engl J Med 1998; 339: 69
Thickness of the Glomerular Basement Membrane, Thickness of the Tubular Basement Membrane, Mesangial Fractional Volume, and Mesangial-Matrix Fractional Volume at Base Line and 5 and 10 Years after Pancreas Transplantation.
The mesangial fractional volume is the proportion of the glomerulus occupied by the mesangium; the mesangial-matrix fractional volume is the proportion of the glomerulus occupied by mesangial matrix. The shaded areas represent the normal ranges obtained in the 66 age- and sex-matched normal controls (means ±2 SD). Data for individual patients are connected by lines.
Type 1 DM

Type 2 DM Kumamoto study: effect of intensifiedglycemic control
Developt of Microalbuminuria Incidence of all forms of DN: micro and macro, proteinuria

Type 2 DM-UKPDS

-14
-12
-10
-8
-6
-4
-2
095 98 101 104 107 110 113 116 119
Mean BP (mmHg)
DFG (ml/min/an)
130/85 140/90
Untreated Hypertension
Bakris GL. Am J Kidney Dis 2000; 36: 646-61
Blood pressure control and progression of DN to ESRD

0
20
40
60
80
100
Albuminuria (%)
(final vs basal value)
- 27%- 42%
Per/Ind n= 233
Ena n= 224
final
Ead : 0,76 95%CI : [0,62-0,92]
Pnoninf<0,001
Change in Change in microalbuminuria microalbuminuria (ITT)(ITT)
n=457 Type 2 DM with microalbuminriaOne year follow up Preterax vs Enalapril
Ead : estimated effect of treatment adjusted on the basal value and the country
Psup=0,002
Coordinator: Carl-Erik MOGENSENCo-coordinator: Serge HALIMIExpert Albuminuria : Giancarlo VIBERTI
J of Hypertension in press 2003

CALM Study
Candesartan16 mg n=42
Lisinopril20 mg n=43
Candesartan16 mg +Lisinopril20 mg
n=46
-60
-50
-40
-30
-20
-10
0
p=0.04
Mogensen CE et al, BMJ 2000;321:1440-4
Decrease albuminuria %
p=NSAdjusted for variation ofBP and BW

DN in type 2 DMThe same disease, the same
patients• Time course of hypertension and DN
(microalbuminuria)• same histological lesions• presence of diabetic retinopathy• presence of other histological lesions (other nephropathies)
• arterial stenosis

BP 140/ 90 mm Hg
Tarnow L et al. Diabetes Care 1994; 17: 1247-51
Normal (n = 323)Micro-albuminuria (n = 151)Macro-albuminuria (n = 75)
0
102030405060
708090
100
Prevalencehypertension (%)
Prevalence of hypertension in type 2 diabetic patientshypertension early present at the very beginning of type 2 DM
and often starts before

-10 -5 0 5 10 15 20 years
Type 2 diabetes preceded by components of the Metabolic Syndrome
Hypertension
Begining of diabetes:Begining of diabetes: Chronic HyperglycemiaChronic Hyperglycemia
Begining of the Begining of the metabolic syndromemetabolic syndromeInsulin-resistanceInsulin-resistanceHypertension -Hypertension - Dyslipidemia- OthersDyslipidemia- Others
Hypertension
Ageing
Early presence of albuminuriaEarly presence of albuminuria
Begining of diabetes:Begining of diabetes: Chronic HyperglycemiaChronic Hyperglycemia
Type 1 diabetesHypertension
alb
Type 2 diabetes
HypertensionAgeing
alb
alb

Large heterogeneity of structural changes in glomeruli, vessels & interstitial tissue in microalbuminuric type 2 diabetic patients P Fioretto t al

Blood Pressure / UAE in IGT Pima indians
0
5
10
15
20
25
30
35
< 140 149-159 > 160Alb
/Ceé
at >
0,1
(% su
bjec
ts)
SBP mmHg
(Ismaïl et al. Kidney Int. 1999; 55, 1-28)

Monoclonal IgM kappa nephropathy
in an 71 years old man
From 10 to 50% of non DN in type 2 diabetic patients with proteinuria

Renal stenosisand Type 2 DM

RECENT ASPECTS AND NEW TREATMENTS
StatinsSartansAminoguanidin


Diabetes feb 2003

Conclusion• We must look for and to start the treatment of DN as soon as
possible• optimal BG and BP control (new targets)• specific effects of Renin angiotensin acting drugs on albumin
excretion rate and renal protection: ACE inh + Sartans ?• New drugs: acting on AGEs, TGFb, Oxidative stress, new oral
antidiabetic drugs, statins…. • Need for new markers and• New values for the normal range of microalbuminuria and BP,
place of ambulatory BP measurements• Do we prevent « DN Sd » in all diabetic patients ?

Therapeutic failure in diabetes
• When a patient reaches end stage renal failure
• When a patient becomes blind or severely visually impaired
• When a patient has a leg or foot amputated
• When a patient suffers from MI or stroke

Screening/detection of late diabetic complications
• Ophthalmoscopy / fundusphotography and visual acuity
• Urinary albumin excretion (A/C) and s creatinine
• Blood pressure
• Foot inspection, pulse and vibration threshold

Diabetic Nephropathy
40 %
Diabetic nephropathy- costs
•Dialysis
75,000 $/year
•Transplantation
15,000 $/year

Prevention and treatment of diabetic nephropathy
• Primary prevention:
• Secondary prevention:
• Tertiary prevention:
Progression from normo- to microalbuminuria
Progression from microalbuminuria to DN
Progression from DN to ESRD

• Blood pressure reduction
• ↓ UAE T1D: ACEiT2D: A2A
• Improved metabolic control
• Low protein diet ?
Treatment modalities in normo- and Treatment modalities in normo- and hypertensive patients with incipient and hypertensive patients with incipient and
overt diabetic nephropathyovert diabetic nephropathy

Treatment of patients with diabetes and microalbuminuria
• Strict metabolic control• Antihypertensive treatment• Blockade of the angiotensin
system– ACE – inhibition– Angiotensin II receptor blocking

• 62 % reduction in progression to nephropathy
• 3 times in regression to normoalbuminuria
• 50 % reduction in UAE at 2 years • Preservation of GFR
Should all Type 1 diabetic microalbuminuric patients Should all Type 1 diabetic microalbuminuric patients receive ACE inhibitors ?receive ACE inhibitors ?
- a meta regression analysis (n=698)- a meta regression analysis (n=698)
Chaturvedi, Ann Intern Med, 2001

Primary prevention ACEI vs placebo in normoalbuminuria
Risk reduction for development of MA / progression in UAE
EUCLID 12.7% ( -2.9 to 26%)Ravid et al. 12.5% ( 2 to 23%)MICRO-HOPE 9.0% ( - 4 to 20%)

In summary: primary prevention of development of diabetic
nephropathy
• Strict metabolic control• ACE – inhibition • Lipid lowering drugs?• Low protein diet?

• Higher prevalence of retinopathy, neuropathy and foot ulcers
• Enhanced cardiovascular morbidity
• Enhanced all-cause mortality, especially cardiovascular
• Predict development of diabetic nephropathy
MicroalbuminuriaMicroalbuminuria

In summary: secondary prevention of development of diabetic nephropathy
• Strict metabolic control• Antihypertensive treatment
– ACE – inhibition – Angiotensin receptor blockers– Both ?
• Multifactorial intervention

In summary: tertiary prevention of progression to ESRF
• Antihypertensive treatment• Strict glucose control • Low protein diet ?• Lipid lowering drugs ?• Stop smoking ?

Late diabetic complications
Prevention is better than cure

ARBs in Type II Diabetic Hypertensives with Renal
Disease



111
Deleterious effects of Angiotensin II
Ang IIAbnormal
vasoconstriction
ActivateSNS
Aldosterone
Vasopressin
Endothelin
PAI-1/thrombosis
Plateletaggregation
Superoxideproduction
CollagenVascular
smooth musclegrowth
Myocytegrowth
Remodeling
Burnier M, Brunner HR. Lancet. 2000;355:637-45.Brown NJ, Vaughn DE. Adv Intern Med. 2000;45:419-29.SNS = Sympathetic nervous system



Managing Hypertensive Patients with Chronic Kidney Disease (ESH/ESC Guidelines) Renal protection in diabetes has two main requirements:
Strict BP control (<130/80 mmHg and even lower if proteinuria >1 g/day is present) Lowering proteinuria to values as near to normal as possible
Microalbuminuria in Type 1 or 2 diabetics: RAAS blockers should be used
Proteinuria: either an ARB, an ACE-I or both is required
To achieve BP goal: combination therapy of several agents (including loop diuretics)
An integrated therapeutic intervention involving various drug classes should be considered in patients with renal damage
ESH/ESC = European Society of Hypertension/European Society of Cardiology
ESH/ESC Task Force Members.J Hypertens 2007;25:1105–87

Managing Hypertensive Patients with Chronic Kidney Disease (JNC 7 Guidelines)
In patients with either a GFR <60 mL/min per 1.73 m2 or albuminuria (>300 mg/day or >200 mg albumin per g of creatinine): Aggressive BP management is advocated, using 3 or more drugs
(including ACE-I or ARBs) to reach BP goals <130/80 mmHg
In patients with advanced renal disease (GFR <30 mL/min, corresponding to a serum creatinine of 2.5–3.0 mg/mL), increasing doses of loop diuretics are required in combination with other drug classes
Chobanian et al. JAMA 2003;289:2560–72
GFR = glomerular filtration rate

Microalbuminuria Reduction With Valsartan (MARVAL) Study: Background Increased UAER is a modifiable risk factor for renal and CV disease in Type 2
diabetes (T2D)
RAAS blockade lowers UAER, but whether this effect is independent of BP reduction remains controversial
MARVAL: designed to evaluate BP-independent effect of DIOVAN on UAER in 332 patients with T2D and microalbuminuria, with or without hypertension
Patients randomised to 80 mg DIOVAN or 5 mg amlodipine for24 weeks
A target BP of 135/85 mmHg was aimed for by dose-doubling followed by addition of bendrofluazide and doxazosin whenever needed
The primary endpoint was the % change in UAER from baseline to24 weeks
Viberti et al. Circulation 2002;106:672–8UAER = urinary albumin excretion rate

MARVAL: Both DIOVAN and Amlodipine Reduce BP to a Similar Extent
Decrease in BP from baseline in subgroup with hypertension at Week 24
Adapted from Viberti et al. Circulation 2002;106:672–8
DIOVAN80/160 mg(n=169)
Amlodipine 5/10 mg(n=163)
Tolerability:
7.4% of amlodipine patients experienced ankle oedema vs 1.2% of DIOVAN patients (difference 6.2%, p=0.006)
DBP SBP
Dec
reas
e in
BP
(mm
Hg)
p=NS
p=NS
–8–6–4–20
–10–12–14–16–18
Patients with Type 2 diabetes and microalbuminuria, with or without hypertension

Recommendation
ESH/ESC guidelines states that :
urinary protein excretion (including Microalbuminuria), eGFR, and ECG should be considered routinely for total cardiovascular risk quantification
Sub-clinical organ damage should be assessed both at screening and during treatment to evaluate whether the selected treatment is protecting patients
from progressing organ damage and potentially from cardiovascular events.

Recommendation
ESH/ESC guidelines states that :
Diuretics, ACE inhibitors, CCB, ARBs, and B-blockers do not differ significantly for their overall ability to reduce BP in hypertension.
Diuretics, ACE inhibitors, CCB, ARBs, and B-blockers can all be considered suitable for initiation of antihypertensive treatment, as well as for its maintenance.
The choice of drug(s) should be made according to the evidence. i.e. The traditional ranking of drugs into first, second, third, and subsequent choice, with an average
patient as reference, has now little scientific and practical justification and should be avoided.

Recommendation
ESH/ESC guidelines states that :
Tight blood glucose control (HbA1c to 6.5%) is beneficial, particularly on microvascular complications. Both effective BG & BP control increases
protection
Tight blood glucose control should be monitored closely to avoid severe hypoglycemic episodes.
Microvascular complications of diabetes in different organs are differently affected by treatment. Antihypertensive treatment exerts a major protective
effect against renal complications, whereas evidence of a similar effect on eye and neural complications is less consistent.

Recommendation
The choice of drugs should be made according to the evidence
Combination Therapy used for treatment initiation, particularly in patients at high cardiovascular risk where early BP control is desirable.
SPC is preferred for patients compliance
For Diabetic Hypertensive patient an ARB should always be included because of the evidence of its superior protective effect against initiation or progression of nephropathy.
BP Goal (Below 130/80mmHg) for diabetic patients is not supported by outcome evidence from trials, as it’s very difficult to achieve in the majority of the patients. So a sizeable BP reduction is recommended without indicating a goal.

Recommendation
ESH/ESC guidelines states that :
When three drugs are required, the most rational combination appears to be a RAAS blocker, a CCB, and a diuretic at
effective doses.

Thank you for your attention
Recommended

















