Cardiopulmonary Resuscitation
Department of Anesthesiology & Reanimation Faculty of Medicine, Padjadjaran University/ Hasan Sadikin General Hospital
Bandung

Objective:
• Identification phases of resuscitation
• Algorythm of CPR initiation
• Airway management
• Breathing support
• Circulation Support
• Drug s and fluids

Introduction1961 : Safar devided CPR into 3 phases
• Phase I :
Basic Life Support, goals of this phase action ( ABC) Emergency Oxygenation
• Phase II :
Advanced Life Support, goals of this phase action (DEF) Restoration of spontaneous circulation and stabilization of the cardiopulmonary system
• Phase III :
Prolonged Life Support, goals ( GHI) Post resuscitative brain oriented and intensive care

Awake? / No
Breath ? / No
Airway management
Breath ?/No
Breathing Support 2x
Carotid Pulse / No
Circulation support

Airway management:
The most common site of airway obstruction in comatouse patients :
• relaxed tongue , when patients head is in flexed or mid position
•Foreign matter : vomitus, blood
•stimulation in stuporous or lightly comatose patients Laryngospasm is usually caused by upper airway
• could be complete or partial obstruction, in complete obstrc (if not corrected) leads to apnea and cardiac arrest within 5 – 10 minute , in partial obstrc must be corrected promptly can result in brain damage or even cardiac arrest

Recognition of Airway obtruction ;
•Can not hear and feel of air flow at the mouth and nose for complete airway obstruction
• When patients still breathing inspiratory retraction of intercostal and supraclavicular
• Partial airway obstruction : snoring, crowing, gurgling, wheezing
• Hypercarbia : somnolence
• Hypoxemia : sympathetic stimulation

Manual clearing of the airway:
•The crossed finger maneuver
•Finger behind teeth manuever
•Tongue jaw lift manuever
Clearing the airway by suction


Technique for foreign body clearing
If the victim is conscious ,
• encourage to expel by coughing and spitting it out
•Apply abdominal thrust s or back blows
If the victim is unconscious
• Apply back blows or abdominal thrust in horizontal position



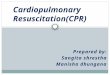
Positioning to open the airway
• Head tilt
• Neck lift
• Chin lift
• Jaw thrust
Open the airway using equipment
• Oropharyngeal airway
• Nasopharyngeal airway
• Endotracheal intubation
• Cricothyroidotomy and Tracheostomy

H
Chin Lift Neck Lift




Breathing support
Without equipment
Mouth to mouth and Mouth to nose
Mouth to adjunct ventilation
Bag Valve Mask with oxygen
Giving positive pressure during inspiration and spontaneous expiration


Mouth to mouth or mouth to nose ventilation
Exhalation consist of 16 - 18 % of oxygen



Recognition of cardiac arrest
unconsciousness, apnea or gasping, death like appearance(cyanosis, or pallor), absence of pulse in large arteries ( carotid or femoral )


Circulation Support
Cardiac arrest :
• Primary : Ventricular fibrillation, asystole caused by myocardial infarction
• Secondary : exsanguination, asphyxia
The most common caused of cardiac arrest : Ventricular fibrillation

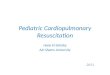
Closed chest cardiac compressions
External cardiac compression (C) in combination with airway control ( A ) , breathing support (B) Made it possible to promptly initiate attempts at reversal of clinical death
The aims of cardiac compression : Initiate artificial circulation



1 operator

2 operators

Monitoring the effectiveness of CPR
•Cheking whether the spontaneously pulse has returned at first after 1 minute CPR, and every 2 – 5 minute there after
• intermittently palpating the carotid pulse

Emergency management of hemorrhage
• Control of external hemorrhage without surgical measures, by elevation and compression
•Positioning of conscious patients in horizontal with leg elevated
•ABC resuscitation initiation in unconscious patients


Drugs and Fluids
•Routes for drugs and fluid :
• Peripheral intravenous route for the administration of drugs and fluids should be establish as quicly as possible after the initiation of CPR without interrupting CPR


Drugs
Epinephrine ( Adrenaline ) may help restore spontaneous circulation in cardiac arrest of 1 – 2 minute duration
Alpha and beta receptor activity
Alpha receptor activity is the most important in cardiac arrest
Vasoconstriction, diastolic pressure raises, improve myocardial and cerebral blood flow
Recommended