Biochem 230: 25 Oct 2004
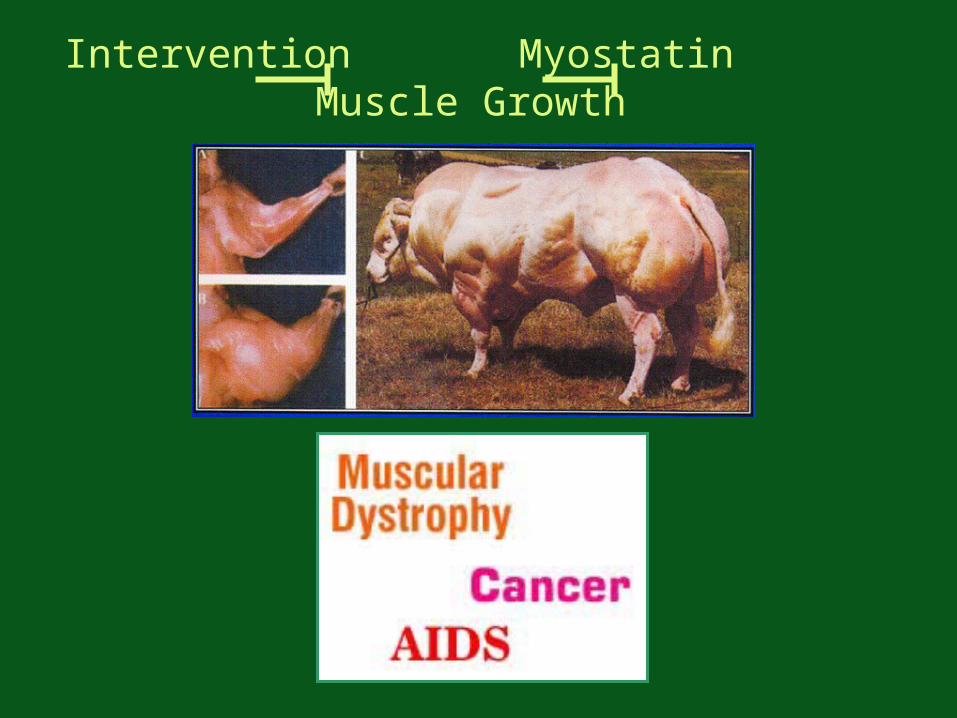
Intervention Myostatin Muscle Growth
Some less noble applications …
Super TGF
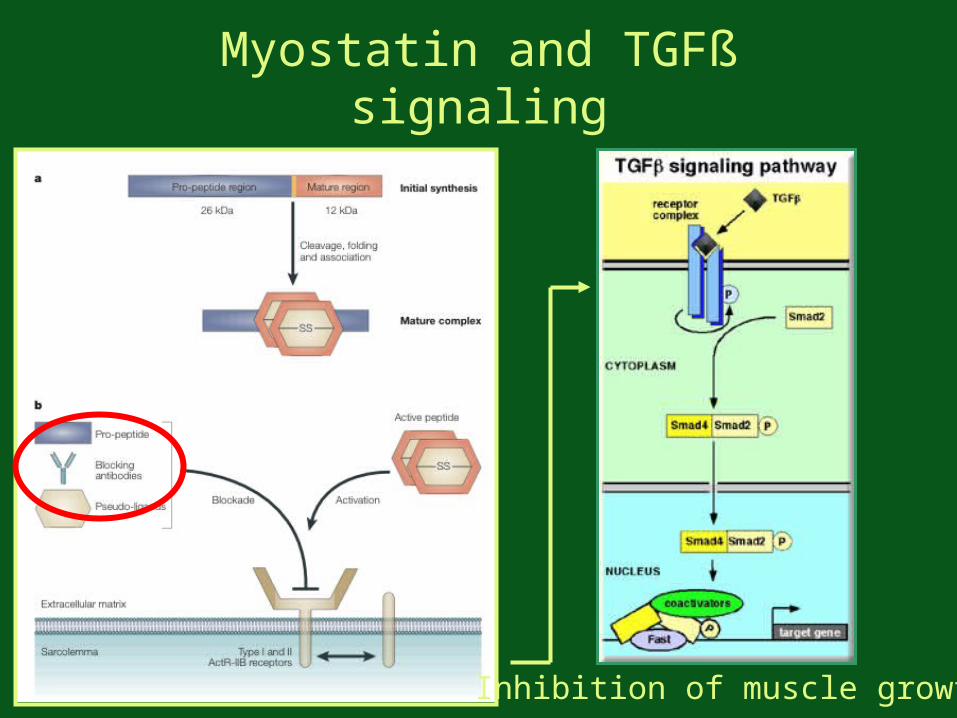
Myostatin and TGFß signaling
Inhibition of muscle growth
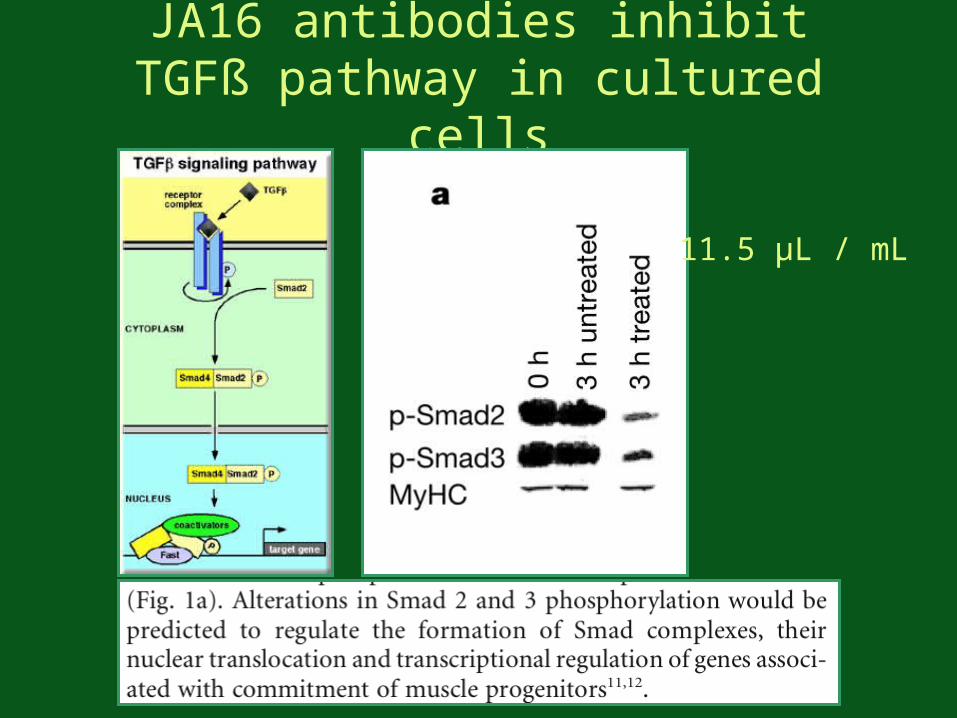
JA16 antibodies inhibit TGFß pathway in cultured cells
11.5 µL / mL
Switch to in vivo . . . • mdx mice widely used: availability, cost, generation time
• but not an ideal phenocopy of MD in humans:
- relatively mild phenotype
- histologically normal muscle at birth
- necrosis begins in week 3, continues for about 1 month
- regeneration compensates for muscle damage
- mdx muscle does not resemble advanced MD
Are myostatin-associated effects dependent on mdx mouse context?

Anti-myostatin associated increases in body weight
1 month old mice60 mg/kg antibody weekly for three months
n=12P < 0.03(t-test)
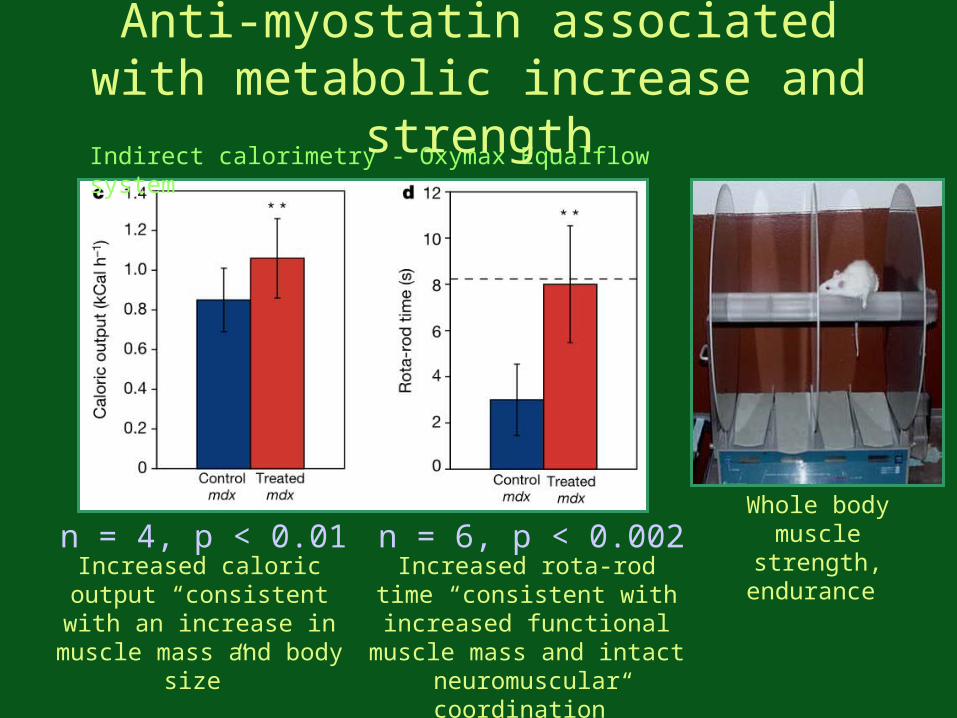
Whole body muscle strength,
endurance Increased caloric output “consistent with an
increase in muscle mass and body size”
Increased rota-rod time “consistent with
increased functional muscle mass and intact
neuromuscular coordination”
n = 4, p < 0.01 n = 6, p < 0.002
Indirect calorimetry - Oxymax Equalflow system
Anti-myostatin associated with metabolic increase and strength
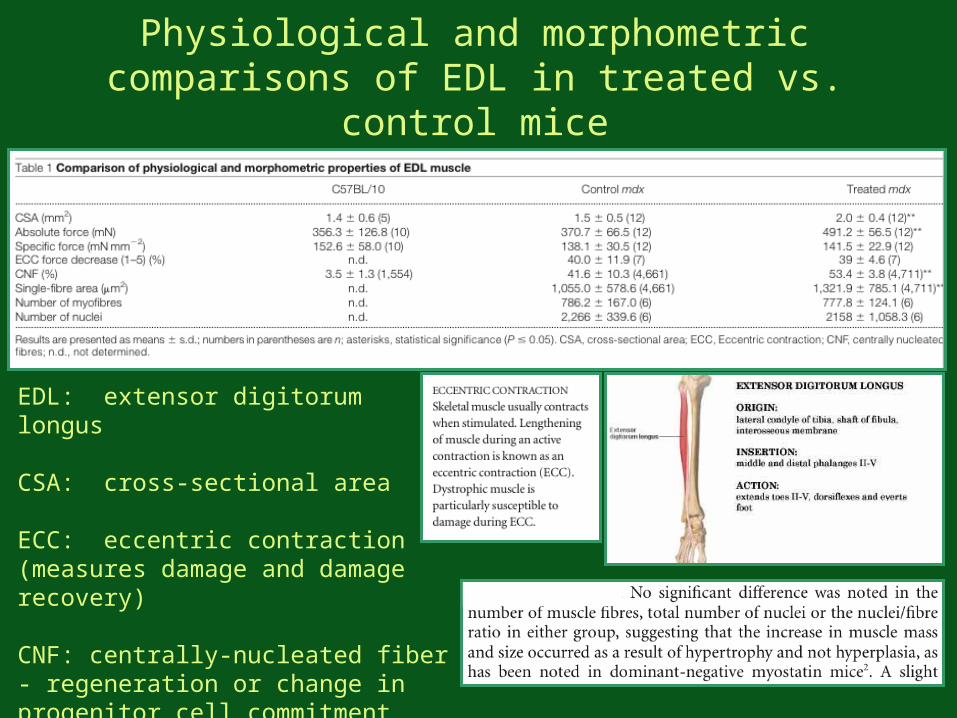
Physiological and morphometric comparisons of EDL in treated vs. control mice
EDL: extensor digitorum longus
CSA: cross-sectional area
ECC: eccentric contraction (measures damage and damage recovery)
CNF: centrally-nucleated fiber - regeneration or change in progenitor cell commitment
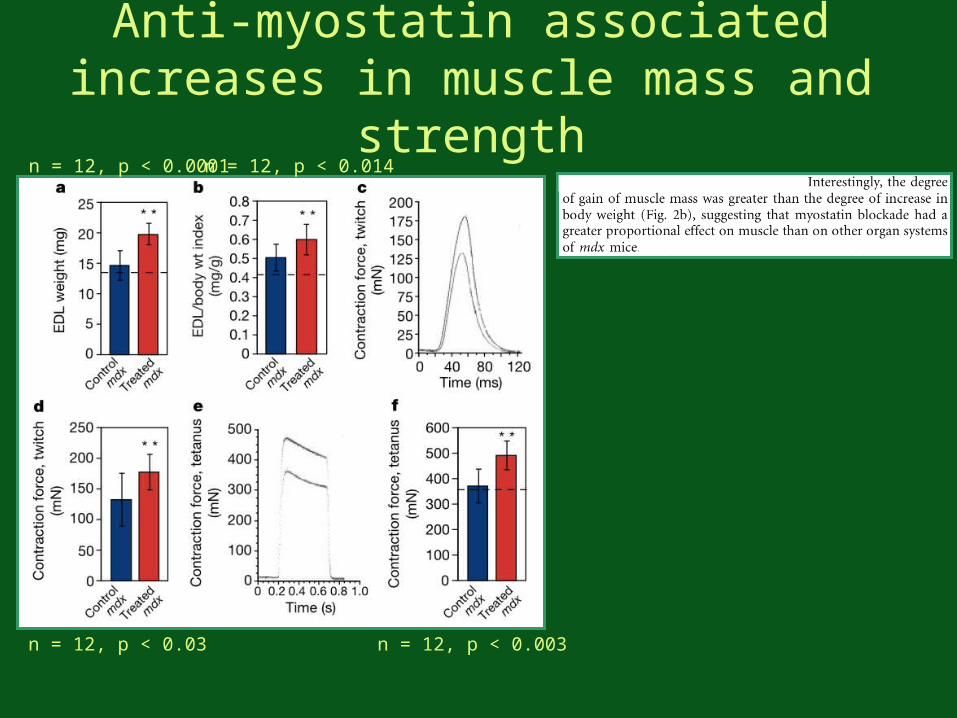
Anti-myostatin associated increases in muscle mass and
strengthn = 12, p < 0.0001n = 12, p < 0.014
n = 12, p < 0.03 n = 12, p < 0.003
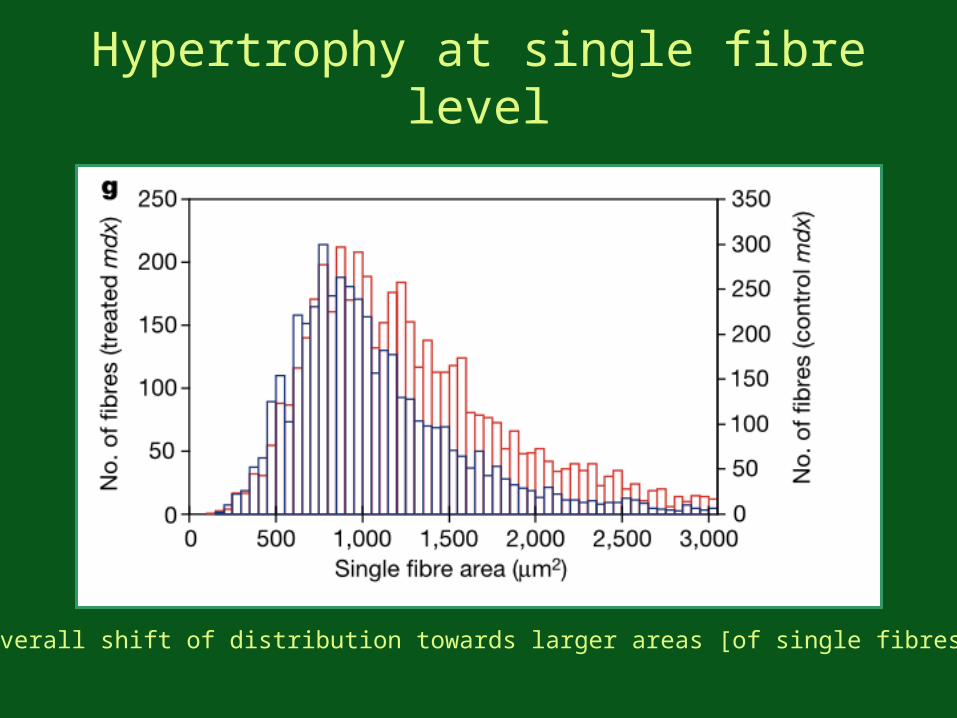
Hypertrophy at single fibre level
“…overall shift of distribution towards larger areas [of single fibres]”
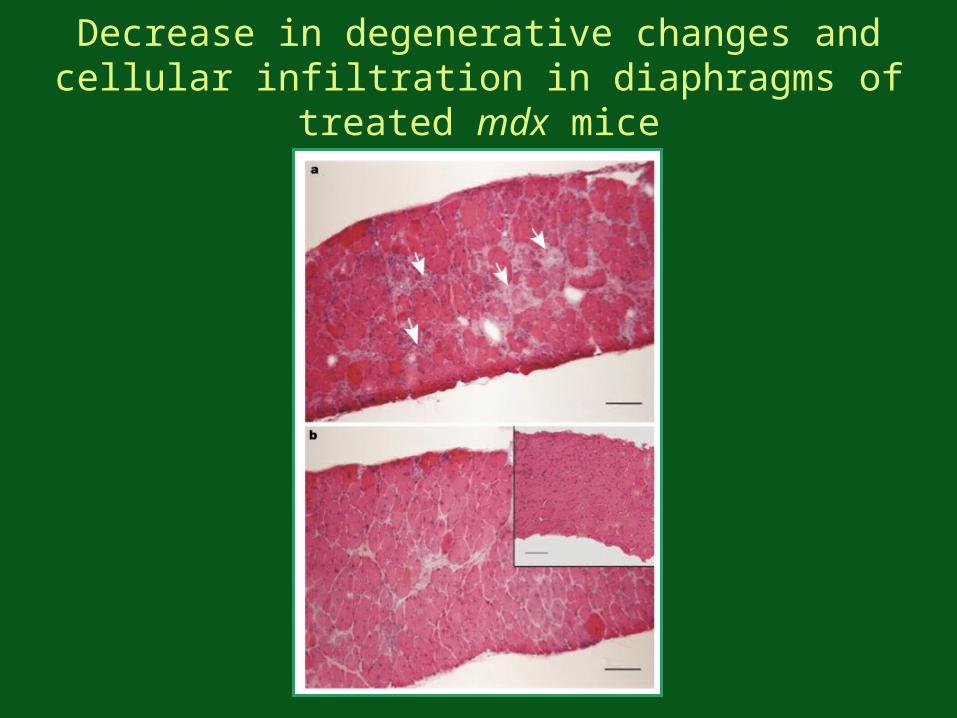
Decrease in degenerative changes and cellular infiltration in diaphragms of treated mdx mice
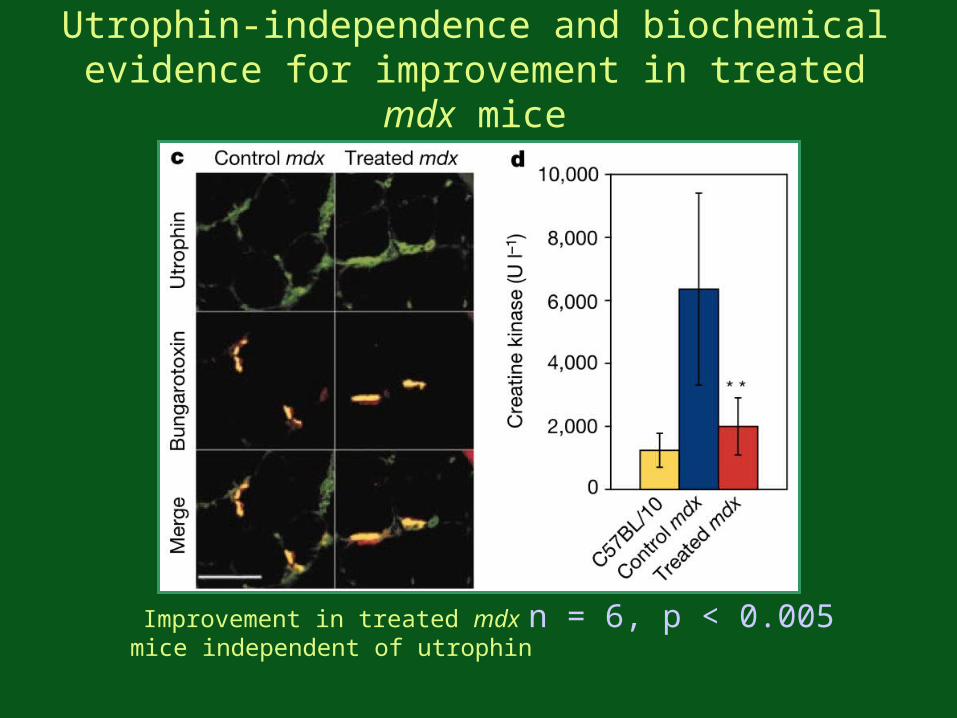
Utrophin-independence and biochemical evidence for improvement in treated mdx
mice
Improvement in treated mdx mice independent of utrophin
n = 6, p < 0.005
Outlook
• Improvement of dystrophic phenotype in mdx mice by anatomical, physiological, and biochemical criteria
• Not all dystrophic changes helped: susceptibility to damage by lengthening contractions not improved
• Proposed treatment for MD or other causes of muscle loss (aging, infections, immobilization, disease)
• Relatively simple compared with gene or cell based therapies
• Low toxicity concerns.
Recommended

















