
Neonatal stabilization and
transport
Santi Punnahitananda M.D.,M.Sc.(Clinical Epidemiology)
Department of Pediatrics,
Faculty of Medicine
Chulalongkorn University

NEONATAL TRANSPORT
HISTORY:

THE SAFEST AND BEST WAY TO TRANSFER
Interhospital neonatal transport
• in utero transfer has better clinical
outcomes for mother and infant than
transfer after birth
• In utero transfer is not always possible

Reasons for transferring infants
between hospitals
• No appropriate local facilities
• No cots available locally
• Insufficient appropriate staffs available
locally e.g. pediatric surgeon, cardiologist
• Unexpected delivery far from home
• Transfer back to local facility
Neonatal transport :ideal
• A dedicated transport team consisting of
Ambulance personnel, Paediatrician Respiratory
therapist, Neonatal Nurse
• Adequate equipment dedicated for the transport
of the infant only.
• Governmental and private medical facilities
agreeing upon a fixed set of transport guidelines
that are on par with the rest of the world.
If not,
• Medical and nursing staff from either
referring or receiving units undertake the
transport on an ad hoc basis.

Limitation
• Variable experience in neonatal transport
and the equipment used
• The vehicle may not be dedicated for
neonatal use

Neonatal transport: present
• We all know about receiving a baby that is
e.g. cold, faulty equipment, and more
unstable than when it left the transferring
hospital…
• Not enough qualified personnel and
equipment within the different departments
transporting neonates.
Safe transport of the preterm infant
• Early anticipating the need for transfer
• Appropriate preparation for transfer
• Ongoing high quality care during transfer

Anticipation
• An opportunity to seek advice
• Gathering staff with the right skills
• Preparation of appropriate equipment
• Direct communication between senior staff
in the two involved centers

Principles of safe transport
• Team composition
• Communication
• Preparation / planning
• Stabilization

• Documentation
• Prepare for worst case scenario
• Maintenance of equipment
• Safe delivery of the patient
Principles of safe transport
Stabilization
Specific treatments should be considered :
• antibiotic treatment
• surfactant replacement
• volume support or inotrope support
• analgesia, sedation, paralysis
• anticonvulsant treatment
• nitric oxide
Stabilization before transfer
• Any remedial action should be taken before
moving the baby and not during the transport.
• the infant should be in as good a clinical
condition as possible before setting off
• the decision to stabilise the infant further or
institute specific treatments must be weighed
against a delay in transfer

The S.T.A.B.L.E. Mnemonic
S ugar
T emperature
A rtificial/Assisted breathing
B lood pressure
L ab work
E motional support© S.T.A.B.L.E.
®
2001

The Basics Come First!
S.T.A.B.L.E.A B C
© S.T.A.B.L.E.®
2001

Sugar
• Initial IV therapy
– Fluid rates and calculations
• Glucose monitoring
– Hypoglycemia assessment and interventions
• Umbilical catheters
– Placement and safe use

Sugar Summary
Suspect hypoglycemia in SGA, LGA, IDM, sick, or stressed infants
Avoid enteral feedings (PO or NG)
D10W IV fluids at 80 ml/kg/day
Maintain the blood sugar > 50 mg/dl (> 2.8 mmol/L) and monitor frequently
© S.T.A.B.L.E.®
2001
Umbilical Vein Catheter (UVC)
• Placed in the IVC above the
diaphragm at the RA junction
– Don’t leave in the portal system, ductus
venosus, or deep right atrium
• Low placement — below the liver —
appropriate for emergencies until other
IV access established
© S.T.A.B.L.E.®
2001
T12
11
10
9
8
7
6
5
4
3
2
T1
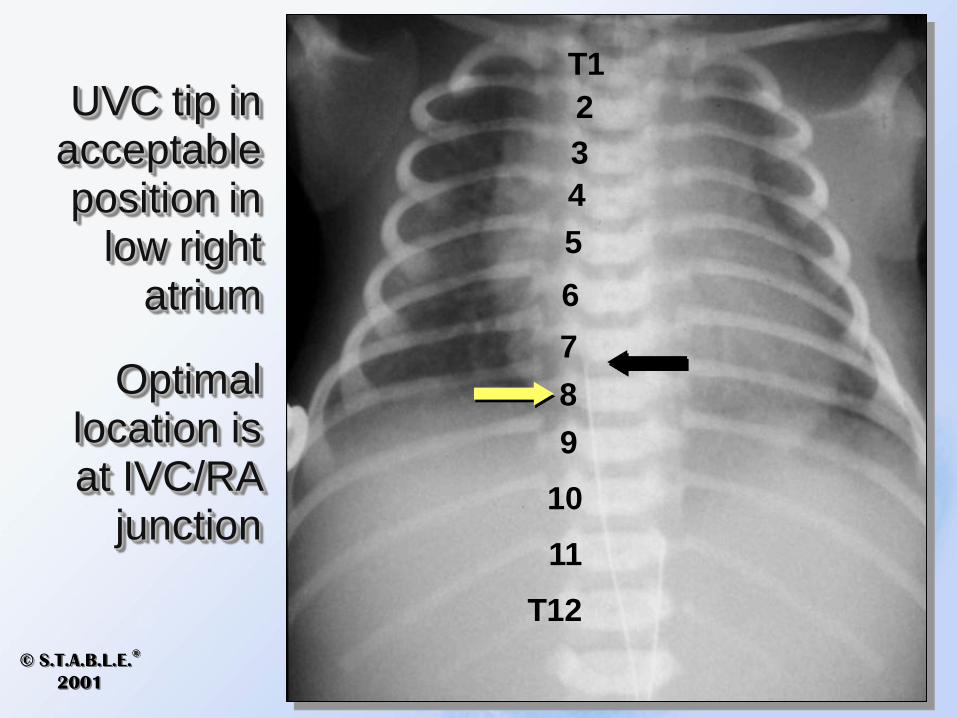
UVC tip in acceptable position in
low right atrium
Optimal location is at IVC/RA
junction
© S.T.A.B.L.E.®
2001

Umbilical Artery Catheter (UAC)
• High lines
– Tip is located between T6 and T9
• Low lines
– Tip is located between L3 and L4
• Confirm placement with x-ray
© S.T.A.B.L.E.®
2001

UAC high line –tip in good position at T9
T12
11
10
9
8
7
T6
© S.T.A.B.L.E.®
2001
Temperature
• Detrimental effects of cold stress
• Vulnerable infants
• How body heat is lost
• Pulmonary vasoconstriction and
shunting
• Warming severely hypothermic infants

Temperature
• Keeping healthy babies warm is an instinctual behavior for caregivers
• Preventing cold stress in sick or small infants can be challenging
© S.T.A.B.L.E.®
2001

Hypothermia
• Extremely vulnerable
infants include:
– Low birth weight
– Those requiring prolonged
resuscitation
© S.T.A.B.L.E.®
2001
Resuscitation and Cold Stress
• Dry quickly — remove wet linens
• Use warm blankets
• Provide radiant warmer heat
– Place infant on ISC/servo control
• Use heated, humidified O2 as soon as
possible
– Remember: cold gas (O2) in, warm exhaled gases
out
© S.T.A.B.L.E.®
2001


Artificial/Assisted Breathing
• Evaluating respiratory distress
• Indications for positive pressure ventilation and endotracheal intubation
• Assisting with intubation
– ET tube sizes
– Securing tubes
– Location on chest x-ray
• Evaluating for pneumothorax

Blood Pressure
• Types and signs of shock
• Treatment of shock
– Hypovolemic
– Cardiogenic
– Septic
• Dopamine infusion
– Calculations and safe use

Blood Pressure Summary
Organ dysfunction results from inadequate perfusion and oxygenation
Evaluate for underlying problems and treat aggressively
Base decision to treat with volume and/or medications on the physical assessment and history, not just the blood pressure
© S.T.A.B.L.E.®
2001
Lab Work
• Initial lab evaluation
• Clinical signs of sepsis
• CBC interpretation
– ANC, I/T ratio, and platelet evaluation
• Antibiotic therapy

Lab Work the 4 B’s
Blood Count
Blood Culture
Blood Sugar
Blood Gas
CBC with differential
Obtain before starting antibiotics
Check early and be vigilant
If respiratory distress or shock suspected© S.T.A.B.L.E.
®
2001

Lab Work Summary
• Review maternal and neonatal history for risk factors for infection
• Watch for signs and symptoms of infection
• Be suspicious even if symptoms are subtle
• Draw a blood culture and start antibiotics promptly© S.T.A.B.L.E.
®
2001

Emotional Support
• Understand how the family may
react during the crisis
• Understand ways health care
providers can support families of
sick infants


Infant care during the journey
• Minimal active intervention should be
needed during the transfer
• The infant's temperature should be
maintained during any journey
• When possible, the environmental
temperature of the vehicle should be
raised.

Minimising heat loss from the infant
during transport
• Raise the environmental temperature of the
vehicle if possible
• Ensure doors of vehicle are closed
• Ensure doors of transport incubator are closed
• Use a heated gel mattress (also helps absorb
vibration and improve general comfort for the
infant)

During transport
• Connect to ambulance power supply if
possible and use ambulance O2
• Incubator and all equipment securely
fixed
• Monitor power and gas supplies
• Do not open portholes unless its
necessary

• Assess baby continuously
• Never perform emergency procedures in
a moving ambulance
• Keep a clear, concise record of events
• On arrival help with stabilization and give
a thorough handover
• Back at base – clean, re-charge, replace,
check (integrity / expiry dates)
During transport
Problems during transport
• Spontaneous clinical deterioration i.e.
pneumothorax
• Equipment i.e. endotracheal tubes and
intravenous lines dislodge
• Equipment to deal with such situations
must be carried.
Communication and documentation
• verbal and written communication
• Use of clinical guidelines, operational
policies, and checklists
• Parents also informed about plans for their
baby's care
• The transport team should meet the
parents when possible

• In some settings informed consent is
needed for transport and care.
• If parents are not travelling in the
ambulance with their infant, they may
need to know how to get to the destination
hospital and what facilities will be available
for them when they arrive.
Communication and documentation
MODE OF TRANSPORT
• Road
• Fixed wing
aircraft
• Helicopter

Choice of vehicle
The mode of transport depends on :
• Resource availability
• Geography
• Clinical pathology,urgency of the situation
• Experience of the staff.

Criteria for deciding which method
• Distance between hospitals
• Traffic density
• Buildings in town or city – hazard for
helicopters
• Weather

Air tranfer
Air transfers
• Needs more organization than road transfers.
• requires specialist training and skills from staffs
• Important physiological effects of flying must be taken into account.– Hypoxia
– barometric pressure drop
– thermal change
– Dehydration
– gravitational forces
– noise, vibration, and fatigue

Transport equipment
• Incubator
• Ventilator
• Gases
• Suction
• Monitors
• Infusion pumps
• Transport bag

Transport equipment
• Equipment for intubation, IV access, chest tube placement
• Drugs
• Portable blood gas analyzer
• Portable blood glucose analyzer

Equipment
• incubator fixed to a transport trolley with
integrated ventilator, monitor, intravenous
pump, and medical gas supply

Transport equipment
• The equipment should be designed to
function while in motion
• all equipment should be run from the
transport vehicle's power supply if possible
• Medical gases sourced from the transport
vehicle should be used whenever
possible.




Personnel and training
• All staff involved (M.D.,RN,paramedics)
should have competency in
– appropriate training in neonatal transport
medicine
– local organizational procedures
– Operation of transport equipment.

Hazards of transportation
• Heavy equipment – E.U. directive =
140kgs
• Noise / vibration
• Road safety - normal driving speeds best
• Traffic Accidents
• Altitude
Recommended

















