Embed Size (px)
Citation preview

WOUND CARE:IT’S ALL GREEK TO ME
BYCHERYL MARZOLI RN BHScN IIWCC

OBJECTIVES
• Provide a better understanding of wound care
• How to: assess, provide interventions and document about wounds.
• Understanding moist wound healing• Discuss categories of dressing products, the
use of the products, NPT (negative pressure therapy) and treatment of wounds.

WOUND
• DEFINITION: A wound is a bodily injury caused by physical means, with disruption of the normal continuity of structures. This can be identified as an acute or a chronic wound.
• ACUTE: Heals in approximately 2 weeks to 6 months
• CHRONIC: Takes 6 months or more.

ACUTE WOUND
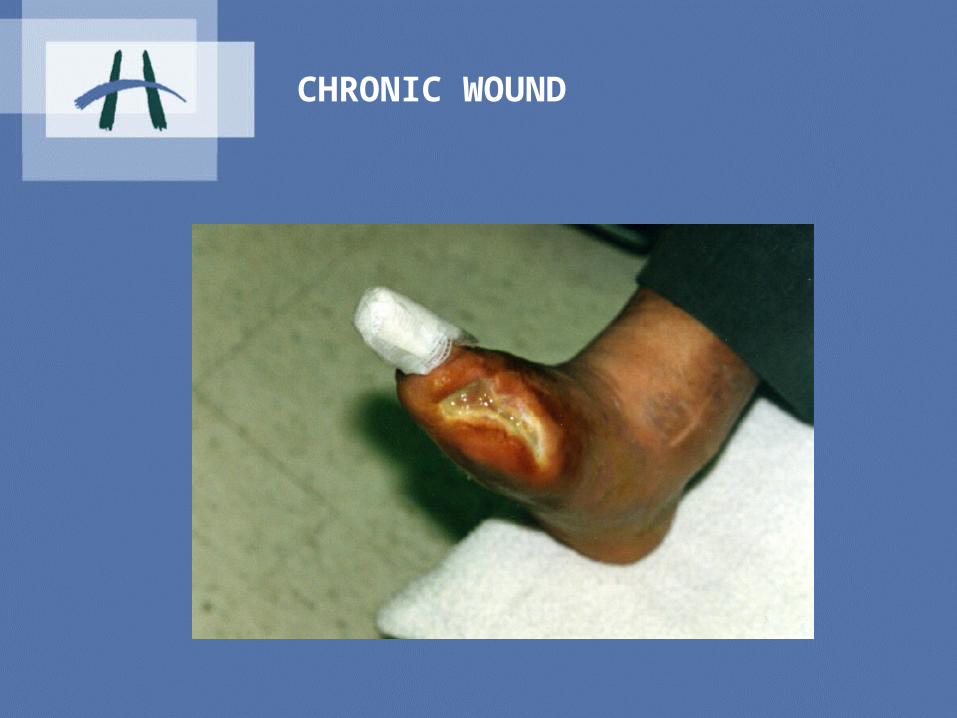
CHRONIC WOUND

PHASES OF WOUND HEALING
• Stages of wound healing: Hemostasis: immediate response Inflammation: 0-4 days Proliferation: 4-21 days Granulation (Epithelialization) :4-21 days Remodeling: up to 2 years * this is for acute wounds, chronic wounds fail to progress
naturally

House building theory
PHASE GOAL PRINCIPLE WOUND CELL HOUSE BUILDING CONTRACTOR
1 HEMOSTASIS PLATELETS CAPPING OFF OFFENDING CONDUITS
2 INFLAMMATION NEUTROPHILS UNSKILLED LABORERS CLEAR THE SITE
3 PROLIFERATION
GRANULATION
CONTRACTURE
MACROPHAGES
LYMPHOCYTES
ANGIOCYTES,NEUROCYTESFIBROBLASTS, KERATINOCYTES
SUPERVISOR CELL
SPECIFIC PREPARERS OF SITEPLUMBER, ELECTRICIANFRAMERSROOFERS/SIDERS
4 REMODELING FIBROCYTES REMODELERS*Krasner, et al

STAGES OF PRESSURE ULCERS
Stage 1: reddened skinStage 2: blister (painful), shallow, pink ulcerStage 3: through the dermisStage 4: through to underlying structures (bone, tendons, etc.)Unable to stage: unable to visualize wound bed due to eschar/slough

Suspected Deep Tissue Injury (SDTI): purple localized area of discolored intact skin, boggy, warmer or cooler compared to adjacent tissues.
NOTE: NO reverse staging i.e. once a stage 3 always a stage 3, never changes to stage 2

STAGE ONE
•Epidermis intact•Area reddened•Does not disappear when pressure relieved•No drainage•Reversible

STAGE TWO
Break in the epidermisAbrasion or blisterPeriwound area redUsually serous drainageWound base pinkpainful

STAGE THREE
Breakdown in epidermis through the dermisDrainage serous or purulentShallow craterMay include sinus tracks, undermining

STAGE FOUR
Breakdown into subcutaneous tissue, muscle and/or boneDrainage presentSinuses and extensive underminingUsually not painful

UNABLE TO STAGE
Eschar/slough covering wound bedNo drainageDebridement necessary

WHAT STAGE?

STAGING ALL OTHER WOUNDSNOT PRESSURE ULCERS
Classification is based on the 3 layers of skinClassify as superficial, partial or full thicknessi.e. a burn can be partial thickness (second
layer).

PARTIAL THICKNESS BURN

ASSESS THE PATIENT
1.Look at the whole patient not just the hole.2. What are the patient’s concerns?3. Is the wound new or old and how old?4. Is this wound healable?5. What are the patient’s co-morbidities?6. How is the patients nutritional status7. What medications if any could interfere
with wound healing?

Probe the wound!!!!

Try and correct the causes that may delay wound healing
• Edema • Nutrition/Dietary consult• Alter medications• Glycemic control• Treat infection • OT/Physio consult

Documentation
• Slough * Location• Eschar * Size LxWxD• Granulation• Undermining• Erythema• Maceration• Exudate• Odor
Moist Wound HealingMotto…
If its wet……..DRY it!If its dry………MOISTEN it!If its irritated…SOOTHE it!If its chronic…IRRITATE it!If its palliative..COMFORT it!

Contamination, Colonization or Infection
Contamination: Bacteria-not attached to wound bed -are not replicating Colonization: - Bacteria are attached to the wound surface but
are not replicating
Infected: -Bacteria are invasive, replication and interfering with wound healing process
-may lead to a “HOST RESPONSE” leading to systemic
infection

SWABS
• Always take a swab from a newly cleaned wound.
• Cleanse with normal saline or sterile water• Take a swab by moving in a “Z” pattern
over the wound and turning the swab at the same time
• Punch biopsy (Physician only)• Do Not swab necrotic or slough tissue

Wound Cleansing
- Normal Saline or Sterile Water
– Irrigate with 20-30 ml syringe
– Use 18 angiocath
– 4-6 inches above the wound
– 5-15 PSI
• **MMP’S( matrix metalloproteases)

ANTISEPTIC SOLUTIONS
• Acetic acid: pseudomonas• Proviodine: broad spectrum effectiveness• Hygeol: staph. and strep. • mechanical debridement• control odour• *acetic acid and hygeol are available
through the pharmacy

Wound Care Products
– Liquid barrier– Transparent films -non adherent dressings– Hydrocolloids -debriding agents– Gauze dressings -antiseptic – Hydrogels – Foam dressings– Absorptive dressings– Calcium alginate– Charcoal dressings– Silver coated dressings

LIQUID BARRIER

TRANSPARENT FILM

HYDROCOLLOID
•

GAUZE DRESSINGS
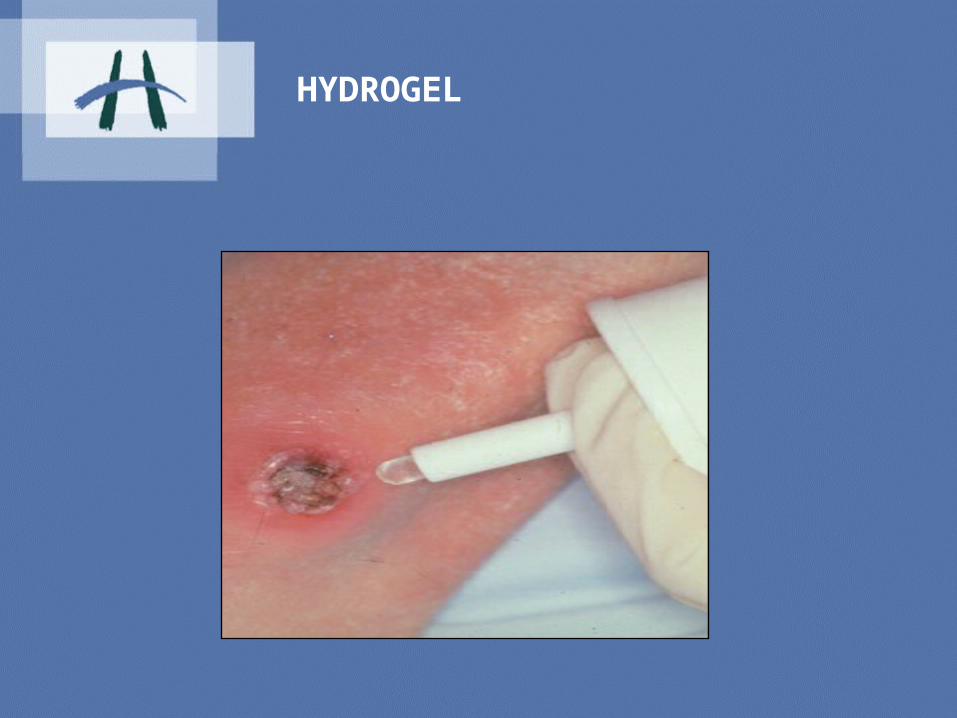
HYDROGEL

FOAM DRESSING

ABSORBENT DRESSINGS

CALCIUM ALGINATE

ODOUR CONTROLCHARCOAL DRESSINGS

ANTIMICROBIAL DRESSING

OTHER DRESSINGS
• Non adherent dressings- • i.e.- mepital• Debriding agents-mesalt, iodosorb• Antiseptic- bactigras with a chlorhexidine
base

BIOLOGIC DRESSINGS

BIOLOGIC DRESSINGS

NEGATIVE PRESSURE THERAPY
• WATCH FOR PRECAUTIONS AND CONTRAINDICATIONS WHEN ORDERING
• MAKE SURE WOUND IS MEASURED ON INITIAL APPLICATION
• IF NO CHANGE WITHIN 2-2I/2 WEEKS THEN DISCONTINUE
• E-Z CARE IS A NEW NEGATIVE PRESSURE THERAPY

GOOD CANDIDATE FOR NEGATIVE PRESSURE

QUESTIONS
THANKYOU






























