Embed Size (px)
Citation preview


World Kidney DayKidney Disease and Children.
Better Knowledge, Better Care.
10 March 2016
Dr . Fatemeh BeiraghdarPediatric Nephrologist

Kidneys check the nutrients
that you get from food
They make urine to get rid of extra water and waste products

Maintain the right amount of water in the body

When Kidneysdon’t work well

Your body can work with only 1 kidney

If both kidneys
stop working for
good
Dialysis
Trans-plantation

Transplantation

Dialysis
Haemodialysis
Peritoneal dialysis
Hemodialysis in Children

Introduction• In children with chronic kidney disease as GFR declines to less 30ml/min/1.73 m2 (Stage
4 CKD)
• Preparation for renal replacement therapy are needed.
• The child and his family should be provided with information related to preemptive kidney transplantation
• Peritoneal dialysis
• Hemodialysis
• Renal replacement therapy is initiated in children with CKD stage 5 in some children with CKD stage 4
• Hemodialysis in children progress over last 20 years
• Morbidity of the session has decreased
• Technically all children can underwent HD even infants 12

Indication of RRT • Renal function, ?GFR
• Before uremic symptoms
• Fluid status
• Biochemical abnormalities
• Acute renal failure• Oligoanuric
• Resistant volume overload to medical treatment
• Hyperkalamia resistant to medical treatment
• Persistent metabolic acidosis resistant to medical treatment
• Uremic encephalopathy
• Uremic pericarditis
• Inborn error of metabolism
• Intoxication 13

Incidence of ESRD in Children• ESRD in children is uncommon• Incidence in USA 14.8 / Million
New Zealand 13.6 / million Japan 4 / million
• The choice of RRT children:• ¼ underwent preemptive renal transplantation• ½ started in peritoneal dialysis• ¼ started in hemodialysis• Preemptive kidney transplantation which is performed prior to the need of
dialysis.• Renal transplantation is associated with better quality of life (Growth and
Development)
14

Chronic Renal failure in children in Western Area of Saudi Arabia
Jameela A. Kari Saudi Journal of Kidney Disease and Transplantation year 2006 V17 Issue I pp 19-2415

Choices of Dialysis
• When preemptive transplantation is not an option
• the choices between the two forms of dialysis is generally dictated by patients age, technical, social, compliance issues and family preference.
16

17
Principle of Vascular Access• Deliver adequate flow rate
• Has long use life
• Has low rate of complications
• - Infection
• - Stenosis
• - Thrombosis
• - Aneurysm
• - Limb ischemia
18
• The best is AVF
• USA - CVC used most often more than AVF and graft
- CVC 89% For children<13 Years
64% 13-19 YEARS
• Review of 2006 annual reports (NAPRTCS) reveals that in a family of pediatric patients 78.9% receiving HD have CVC as primary access.
• AVF 12.3%
• AVG 8.5%
19
• Advantage of AVG
1.Shorter time to use
2.High primary potency rate
3.Ease of technical creation
• Sheath et al reported creation of 24 AVF and 28 AVG respectively .
• The most common site of AVG is the thigh -50% of patients
• Disadvantages of AVG
1.Thrombosis
2.Stenosis
3.Infection
Sheath et al permanent vascular access survival in children and adolescent with end stage renal disease 2002 Kidney Int 62:1864-1869
20

CENTRAL VENOUS CATHETER• Central venous catheter are the most commonly used vascular access in
children in north America data from USRDS 40% of children who were receiving chronic HD continued to use catheter
• Data from ANZDATA 2008 showed the catheters were used exclusively below 10 years of age
• NAPRTCS 2008• 78% catheters• 12% AVF• 7% AVG
• European Pediatric Dialysis Working Group• 60% catheters• 38% AVF• 2%AVG
21
CENTRAL VENOUS CATHETER
First choice in patient require urgent HD
2. Stage V CKD
3. As abridge from a patient who is expected to receive planned transplant
4. Is training to transfer to PD
- Advantage
- It can be used immediately
- Disadvantage
1. Short life span
2. Thrombosis
3.Infection
4. Malfunction
5. Possible fibrin sheath formation
- Median survival times of CVC is 4 months – 10.6 months
22
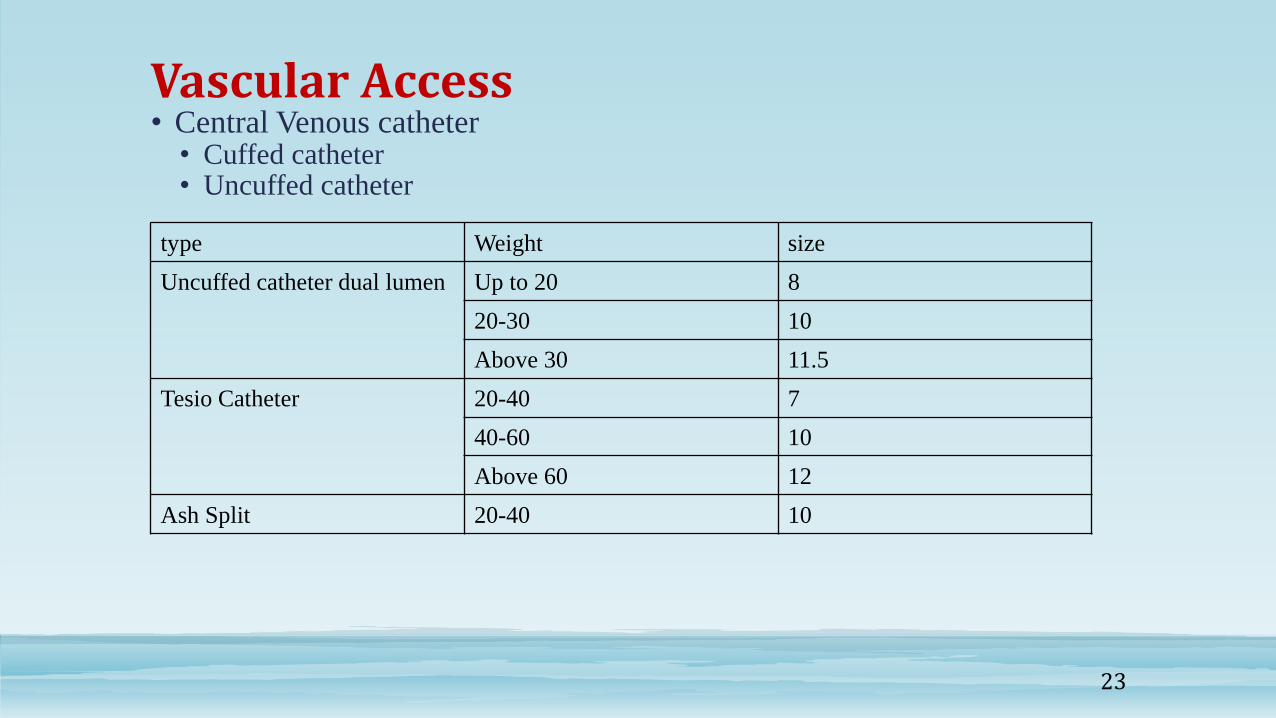
Vascular Access• Central Venous catheter
• Cuffed catheter• Uncuffed catheter
sizeWeighttype
8Up to 20Uncuffed catheter dual lumen
1020-30
11.5Above 30
720-40Tesio Catheter
1040-60
12Above 60
1020-40Ash Split
23

Complications of CVC• USRDS data have shown sepsis rate with CVCs approximate 80/100
patient as compared to 10/100 patient for AVF
• Potential sequences of CVC include:
- Septic shock
- Subacute bacterial endocarditis
- Osteomyelitis
- Epidural abscess
• One study evaluated potential differences in infection rate based on use of three agents for exit site care
- 2% chlorhexidine found infection rate is 0.5%
- 10% povidine iodine found infection rate is 2.5%
- 70% alcohol found infection rate is 2.3%
• Different antimicrobial catheter lock studies suggest that citrate is ideal
24

Access Monitoring
• 1. Inspection: the access should be assessed weekly through inspection, palpation, and auscultation by the nursing staff.
• - With specific attention to arm swelling.
• - Prolonged bleeding after needle removal.
• - Change in thrills or bruits.
• -The nephrologist should inspect the access at each physical examination.
• 2. Surveillance ↓KT/V or URR. Determination of access recirculation should be documented on a monthly basis.
• Ultrasound dilution/month if not available do Doppler U/S /month.
25
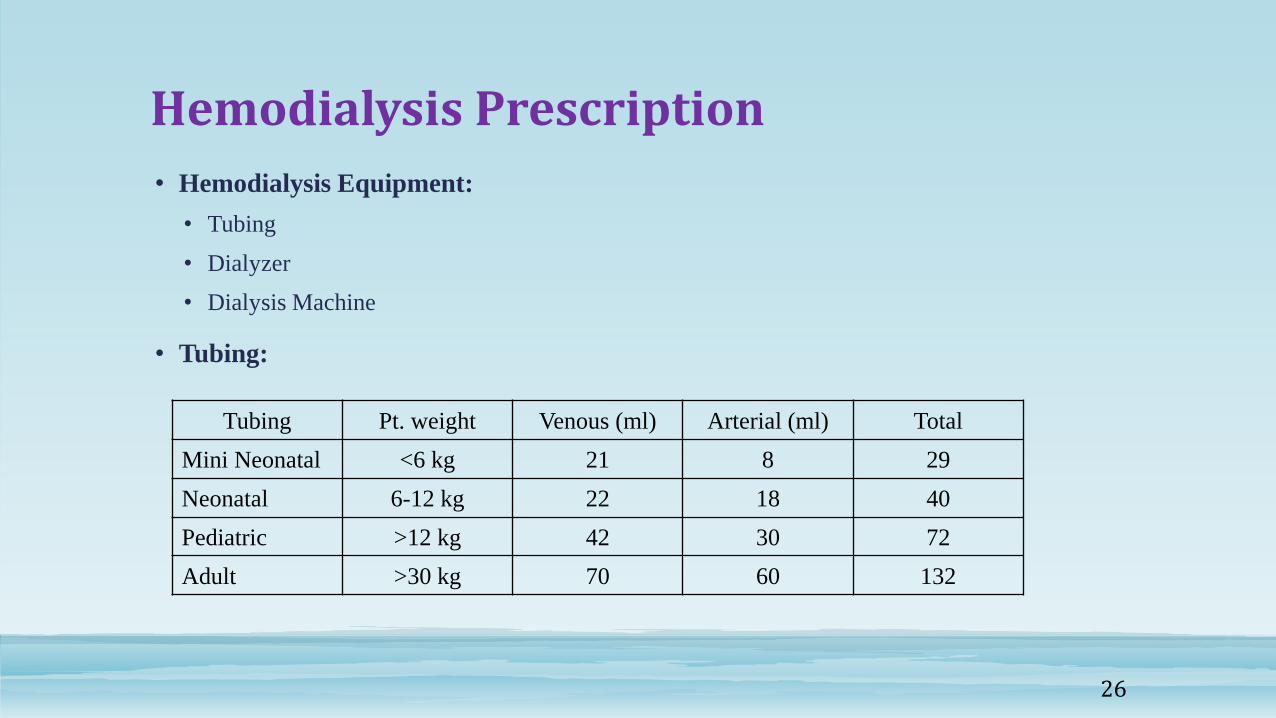
Hemodialysis Prescription
• Hemodialysis Equipment:
• Tubing
• Dialyzer
• Dialysis Machine
• Tubing:
TotalArterial (ml)Venous (ml)Pt. weightTubing
29821<6 kgMini Neonatal
4018226-12 kgNeonatal
723042>12 kgPediatric
1326070>30 kgAdult
26

Types of Dialyzer
• Dialyzer:
• Types of Membrane
• Blood volume capacity
• Service area
• UF coefficient
• Clearance of various substances
• Sterilization
27
Hemodialysis Prescription• Types of Dialyzer
• Low flux (KUF <10 ml/hr/mmHg)
• High flux KUF 15-60 ml/mmHg
• Hallow fiber (capillary)
• Parallel Plate
• Types of Membranes
• Unmodified cellulose low flux
• Modified cellulose (Low & high flux)
• Synthetic (low & high flux)
• Synthetic noncellulose membranes are more biocompatible, size of
dialyzer shouldn’t exceed 75-100% of patient service area
28

Selection of Dialyzer that can be used in children
DialyzerSurface Area(m2)
Fill Volume(ml)
UF Coefficient (ml/min/mmHg)
Gambro Polyflux 14L1.3779.5
Polyflux 17L1.710312.5
Polyflux 11S1.18153
Polyflux 14S1.410262
Polyflux 17S1.712171
2H (HF)0.21715
6H (HF) 0.65233
Fresenius F3 0.4281.7
F4 HPS0.7424.3
F5 HPS1.0636.2
F6 HPS1.3828.5
F7 HPS1.61029.8
F8 HPS1.811411.1
Xenium 110 (HF)1.16949
130 (HF)1.37862
150(HF)1.59163
210(HF)2.112680
Baxter CA-50 (LF)0.5352.5
FB 110GA1.1658.129

Hemodialysis Prescription con’t.
• Dialysis Machine:
• Precise control of UF, volumetric assessment
• Capable of low blood flow speeds
• Ability to use lines of varying blood volume
• Measure removal of very small amount of fluids
• Continuous blood volume monitoring
30

Hemodialysis Prescription• Blood Flow rate
• 1st session 90 ml/m2
2-3 ml/kg/min
• Latter
5-7 ml/kg/min 150-200 ml/m2
• Dialysate: It compose
• Treated water
• Electrolytes Na 140 mmol/L, K 2-3 mmol/L. Cl 100-102 meq/L, HCO3
40 meq/L, Mg 1.5-2 meq/L, Ca 1.25-1.5 mmol/L
• Acid Buffers
• Glucose 100 g/L
• Dialysate Flow rate 2 times more than blood flow rate, standard 500 ml/min
• UF: Standard weight 1.5-2 % of BW/hr. not more than 5% BW/HD session
31
Hemodialysis Prescription cont.
• Anticoagulation
• Heparin loading – 2000 IU/m2
20 IU/kg
10 IU/kg in infant
• Maintenance – 400 IU/m2
10-20 IU/kg to be discontinued 30 minutes prior to the end of dialysis
aPTT 120-160 or more than 50% above baseline of ACT
• Heparin lock: with concentrated heparin 50 U/kg/lumen for weight less than
10 kg
• 1000 U/ml BW (10-20 kg)
• 2500 U/ml BW>20 kg
32

Hemodialysis Prescription Components
ComponentsComments
Blood LinePediatric/Neonatal according to the patient’s size
Dialyzer SizeThe size of the dialyzer should not exceed 75-100% of the patient SA
Blood-flow rate90mL/m2/min to maximum of 150-200 ml/m2/min*
Dialysate-flow rate500 ml./min is the standard, may vary 300-800 ml/min
Dialysate Composition* SodiumPotassiumBicarbonateCalcium
140 mmol/l2-3 mmol/l40mEq/l1.25-1.5 mmol/L
Ultrafiltration Rate1.5 to 2% of body weight/hr and not more than 5% body weight/dialysis session*
AnticoagulationHeparin is the standard; Loading dose 2000 IU/m2
followed by 400 IU/m2/hr*
Treatment duration and Frequency of Hemodialysis Sessions
Three sessions per week for 3 to 4 h per session to achieve the minimum target prescription of 1.2 to 1.4 Kt/V
33
Hemodialysis Adequacy• Hemodialysis adequacy: Minimum adequate dose of HD
given 3/times/week to patient with Kr less than
2ml/min/173m2, spkt/v 1.2/dialysis
• URR of 65%
• Target dose HD 3 times/week
• spkt/v 1.4/dialysis not including residual kidney function
• URR 70% single port kt/v
34

Methods of Measurement of Delivered Dose of Hemodialysis
Single-pool Kt/V calculated by Daugirdas II Formula
• Equation I:
• spKt/V = - In (C1/C0 – 0.008 x t) + (4 – 3.5 x C1/C0) x UF/W
• Equilibrated kt/V
• Equation II:
• estBUN = ([BUN15min – BUN30secs]/0.69) + BUN30secs
KDOQI Guidelines 2006Cherry Mammen, Goldstein White Standard kt/V threshold to accurately predict single pool kt/V target for children receiving thrice weekly maintenance HD. Nephrology Dialysis Transplant 2010
35

Methods of Measurement of Delivered Dose of Hemodialysis
• Equation III:
• cKt/V (Goldstein) = -1n (estBUN/CO – 0.008 x t)+ (4-3.5 x estBUN/C0) x UF/W
• Equation IV:
• stdKt/V = 168 * [1-exp[-eKt/V]/t]/
• [1 – exp [ - eKt/V]/spKt/V] + [168/(N * t) – 1]
• Equation V:
• URR = 100x(estBUN – BUN30secs)/ BUN30secs
• Equation VI:
• %UFF = 100 – [(pre-treatment weight – post-treatment weight)/post-treatment
weight]
Cherry Mammen, Goldstein White Standard kt/V threshold to accurately predict single pool kt/V target for children receiving thrice weekly maintenance HD. Nephrology Dialysis Transplant 2010
36
Lower Kt/V causes
• If spKt/V is lower than expected:
• Blood flow rate
• Duration of treatment
• Dialysate flow
• Dialyzer specification and KoA
• Intradialytic hypotension
• Undetected early termination of treatment
• Was the anticoagulation adequate?
• Was post dialysis blood sampling appropriate?
• Was the needle size and placement appropriate and optimal?
• Was the blood pump adequately calibrated?
• Was the blood pump segment wrong?
• Was parenteral nutrition infused during treatment?
37

They help the body
make red blood cells

Anemia Management in ESRD in children
• Hb 11-12 g/dl
• Serum ferritin target level >100 mg/ml
• Tsat >20%
• Monthly (CBC & reticulocyte count)
• Every 3/12 serum ferritin, serum Tsat and serum iron.
• with change therapy CBC weekly for 6/52
39
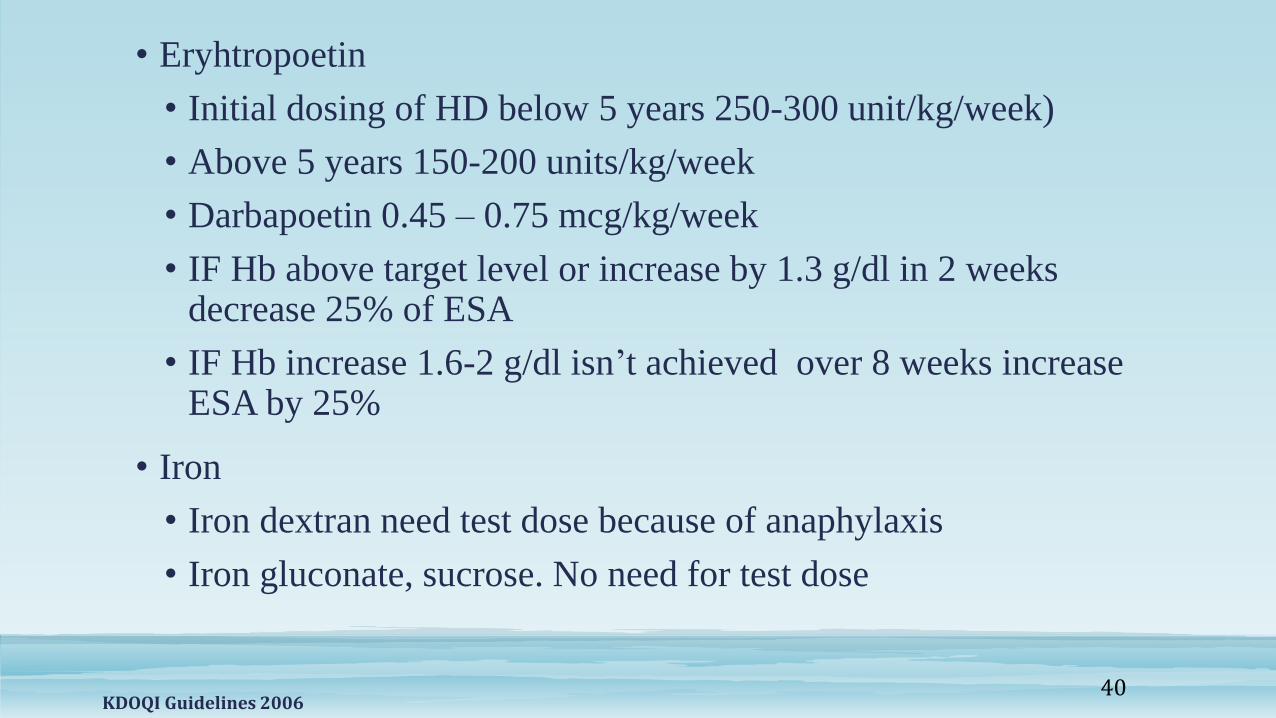
• Eryhtropoetin
• Initial dosing of HD below 5 years 250-300 unit/kg/week)
• Above 5 years 150-200 units/kg/week
• Darbapoetin 0.45 – 0.75 mcg/kg/week
• IF Hb above target level or increase by 1.3 g/dl in 2 weeks decrease 25% of ESA
• IF Hb increase 1.6-2 g/dl isn’t achieved over 8 weeks increase ESA by 25%
• Iron
• Iron dextran need test dose because of anaphylaxis
• Iron gluconate, sucrose. No need for test dose
KDOQI Guidelines 200640

They produce
active vitamin D

• Serum phosphorus
• Children 1-12 years 4-6 mg/dl (1.26-1.93 mmol/L)
• Children over 12 years – 3.5-5.5 mg/dl (1.13-1.78 mmol/L)
• Serum calcium
• 8.8-9.5 mg/dl
• 2.20-2.37 mmol/L
• Ca x phosphate products should be less than 5 mmol/L
• Total eliminated Ca should not exceed 2500 mg/day
• Metabolic acidosis HCO 22 mmol/L
Bone Mineral Management in ESRD
KDOQI Guidelines 2006 42
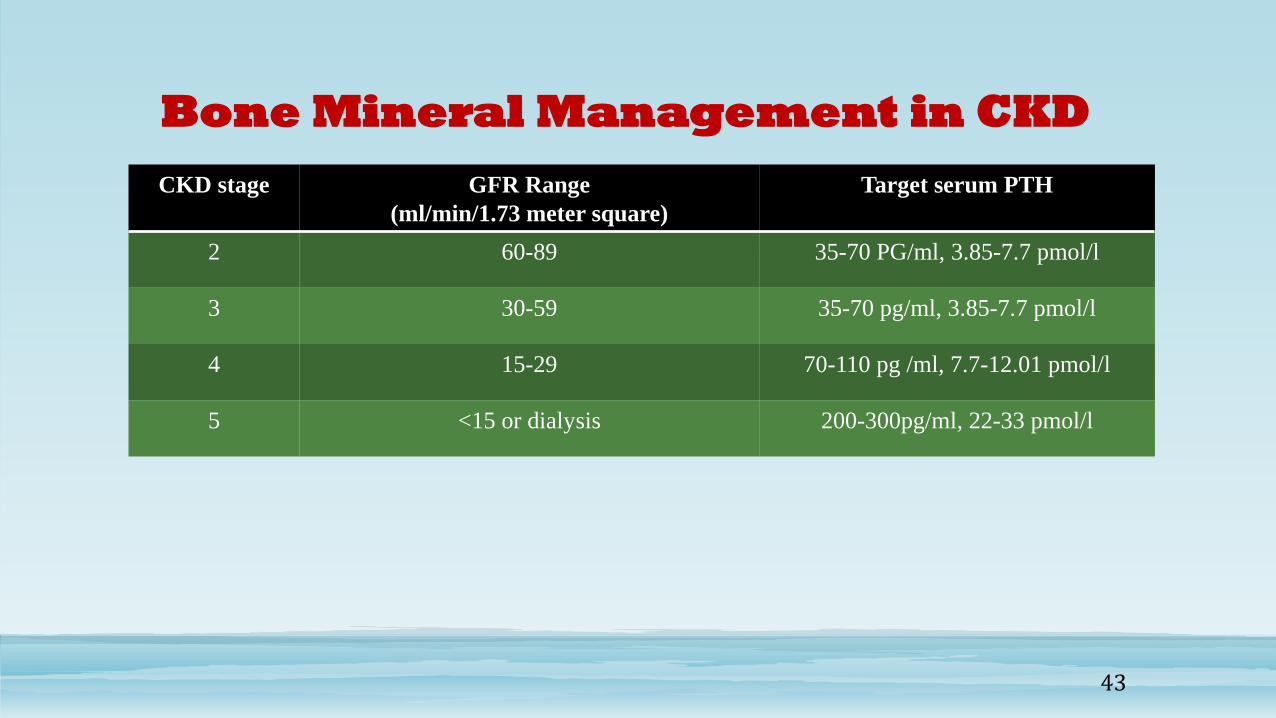
Bone Mineral Management in CKD
Target serum PTHGFR Range
(ml/min/1.73 meter square)
CKD stage
35-70 PG/ml, 3.85-7.7 pmol/l60-892
35-70 pg/ml, 3.85-7.7 pmol/l30-593
70-110 pg /ml, 7.7-12.01 pmol/l15-294
200-300pg/ml, 22-33 pmol/l<15 or dialysis5
43
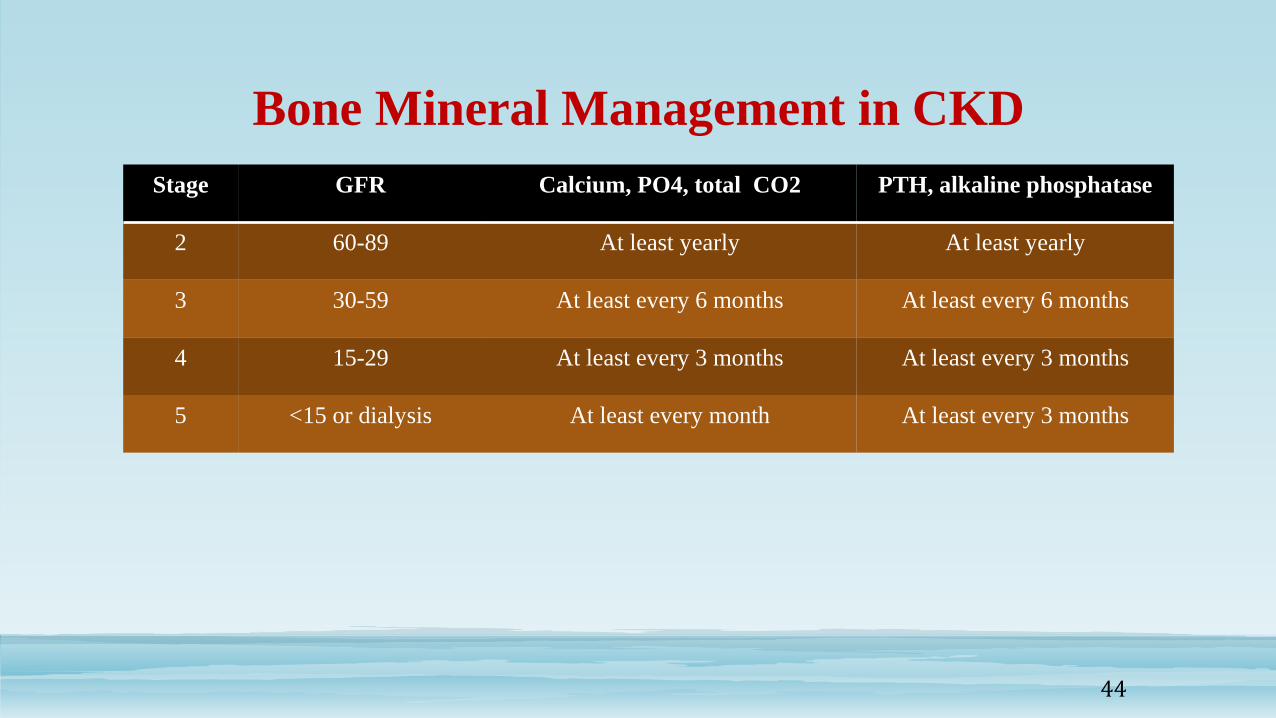
PTH, alkaline phosphataseCalcium, PO4, total CO2GFRStage
At least yearlyAt least yearly60-892
At least every 6 monthsAt least every 6 months30-593
At least every 3 monthsAt least every 3 months15-294
At least every 3 monthsAt least every month<15 or dialysis5
Bone Mineral Management in CKD
44

Nutritional Status• Phosphorus – CKD 3 – 5 and 5D decrease dietary phosphate to 80% of DRI for age
when PTH above target range of CKD and phosphate exceed normal reference
• Protein – dietary protein 100-140 of daily protein requirement for CKD 3-5
• Carbohydrate: Normal carbohydrate compare to age match healthy child
• Vitamins – B1, B2, B3, B5, B6, B8, B12, vitamin C, A, K, folic acid, copper, zinc should be 100% of daily requirement
• Trace elements 100% if clinical evidence of deficiency
• Free water & Na supplementation should be consider for polyuric child.
• Na supplements should be consider for all infants in PD due to substantial loss even anuric and to be restricted for hypertensive child
• Potassium should be restricted for CKD 2-5
• Acidosis is to be corrected to HCO3 22 mmol/l
KDOQI Guidelines 2006
45
Nutritional Status
• Growth
• Growth hormone CKD 2-5 for short stature or height /age <3rd centile persist for 3 months
despite adequate nutritional treatment and correction of metabolic abnormalities
• Calories should be 100% maintaining its chronological age
46

Complications During Hemodialysis
• Disequilibrium symptoms – movement of water to brain cell by osmosis due to sudden drop of urea in plasma
• Presentation: Nausea, headache, dizziness and seizure, coma
• Treatment: Blood flow, dialyzer, duration of treatment
• Mannitol of infusion 1g/kg over 1 h
• 1st session 30% drop, increase 50%, target 70-75% urea reduction
• Ct/C0 = e –kt/V
• Ct urea after t minutes of dialysis
• C0 urea at initiation of dialysis
• K – specific dialyser urea clearance ml/min
• V = Patient urea volume of distribution
47
Complications During Hemodialysis• Hypotension:
• Intravascular volume depletion due to slow refiling from extravascular space
• Use of dialysate Na lower than plasma
• Exchanging UF
• Impaired sympathetic activity
• Warm dialysate – vasodilation
• Splanching pooling of blood while eating during dialysis
• Use of antihypertensive medication on day of dialysis
• Treatment:
• NS 5 ml/kg
• Cessation of UF
• Reassessment of target eight daily fluid allowance review
• Separate UF from dialysis
• Na ramping
• Hct monitoring48

Complications During Hemodialysis• Intradialysis hemolysis
• Symptoms: Pain & nausea
• Presentation: Dark appearance to venous blood due to over heating, contamination, hypertonicity of dialysate, kinking of line, malfunctioning of pump
• Treatment: Stop dialysis, check potassium
• Urticaria: antihistamine or hydrocort
• Air embolism: rare as air detection will clamp the return line 1 ml/kg
• Symptoms: Seizure, coma, chest symptoms
• Treatment: Clamp lines, stop pump, put head down, give 100% oxygen
• Air may need to be aspirated from ventricles
49
Complication Post-Dialysis• Malnutrition is common is children receiving hemodialysis.
The risk of death is reported:
• 54% for each 1 g/dl fall in albumin
• 57% reduced if serum albumin >4g/dl
• 14% increased with each decrease of one height of standard deviation score below normal at start of dialysis
• Neuropsychologial outcomes: One study showed children below 18 months have:
• 42% neuropsychological impairment
• 58% attend regular school
50

Social & Psychological Issues
• Dialysis Unit
• Vacation
• School
• Economic status
• Transfer of Service
51

Complication Post-Dialysis
• Renal osteodystrophy
• Cardiovascular Disease
• Hypertension – in one case series 624 children in HD 79% of them was with hypertension and with 62% receiving antihypertensive medications
• Left ventricular hypertrophy up to 80%
52

Mortality
• Mortality risk in children in dialysis is >30 times higher than age and gender match normal children
• US 5 years survival of 2867 patient starting dialysis at age 1, 1-5, and >5 years was 60, 80, and 85%
• ANZATA- RRT 1963-2002 demonstrated a 10 years and 20 years survival 79% and 66%.
• Mortality is higher in children in dialysis and less post transplant as noted by ANZATA
• UK Network 10 fold higher risk of death in children on dialysis compared to those were transplanted
• Cause of Death is CVD 1000 fold higher in young adults on dialysis than age match normal
• USRDS – 22.5% of death due to CVD
• ANZATA 45% of death due to CVD
• Dutch 41% of death due to CVD
53
Mortality• Age at start of dialysis
• NAPRTCS report lower survival for children who begin HD before 1 year of age with survival rate of 82, 73 63% at 1, 2, 3 years after initiation of dialysis.
• Comparison of survival between Hemodialysis and PD
• Italian registry showed no difference between 5-15 years but below 5 years who were most exclusively managed by PD had a poorer 5 years survival
• USRDS showed no difference in 5 years survival between PD and hemodialysis at any age
54

Mortality
2013 USRDS Annual Data Report, Pediatric ESRD volume 2 55
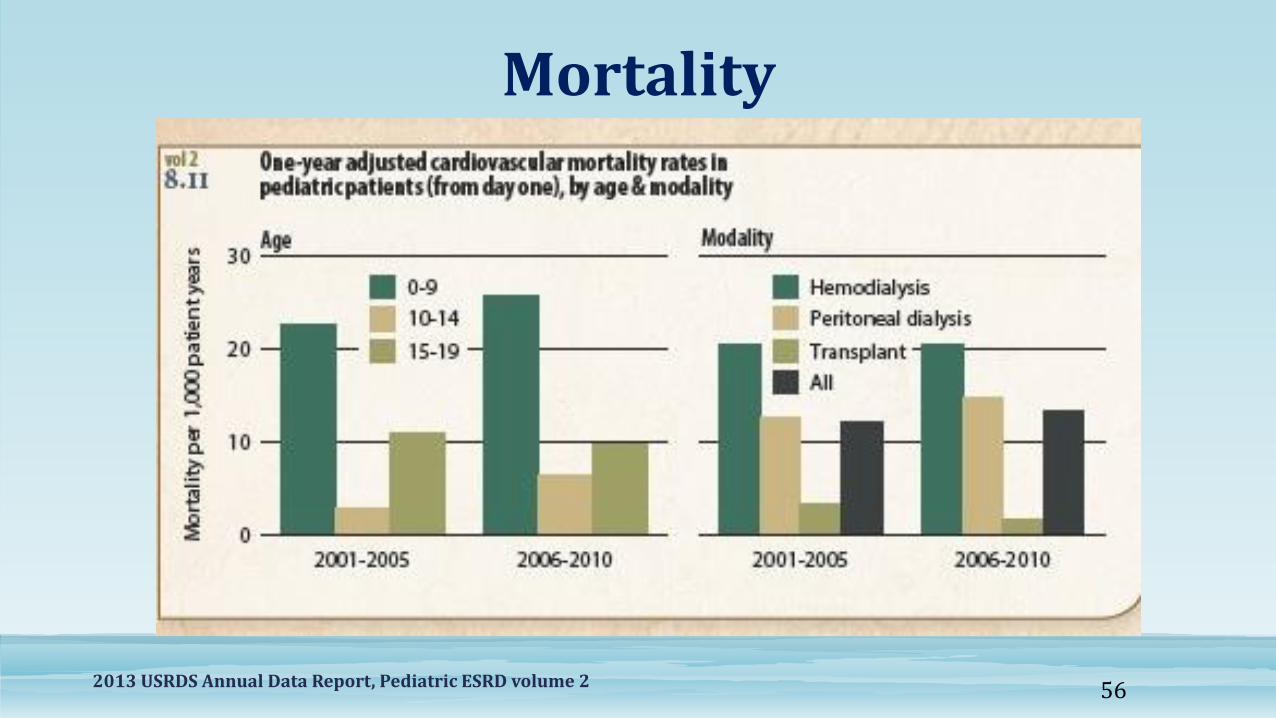
Mortality
2013 USRDS Annual Data Report, Pediatric ESRD volume 2 56

Mortality
2013 USRDS Annual Data Report, Pediatric ESRD volume 257

Mortality
2013 USRDS Annual Data Report, Pediatric ESRD volume 258

Summary of Hemodialysis in Children
• Although principles of hemodialysis are similar for adult and children there are fundamental differences in technical aspect of procedures and complications
• Optimal care is provided by multidisciplinary team (Pediatric Nephrologist, skilled nurses, dietician, vascular access coordinator, vascular surgeon, radiologist, psychologist, and social worker)
• Good vascular access is essential for the success of hemodialysis
• Hemodialysis equipment must be modified for pediatric patient
• Long-term quality of life is lower in children on dialysis compared with normal healthy control and children receiving renal transplant
59

60
Peritoneal Dialysis (PD)

61
Principles of PD
• Dialysis fluid is introduced to the peritoneal cavity through a catheter placed inthe lower part of the abdomen.
• A thin membrane, called the peritoneum, lines the walls of the peritonealcavity and covers all the organs contained in it.
• In PD the peritoneum serves as the dialysis membrane. The peritoneal cavitycan often hold more then 3 litres, but in clinical practice only 1.5 – 2.5L of fluidare used.
• This is an intra-corporeal blood purification as no blood ever leaves the bodyof the patient.
62
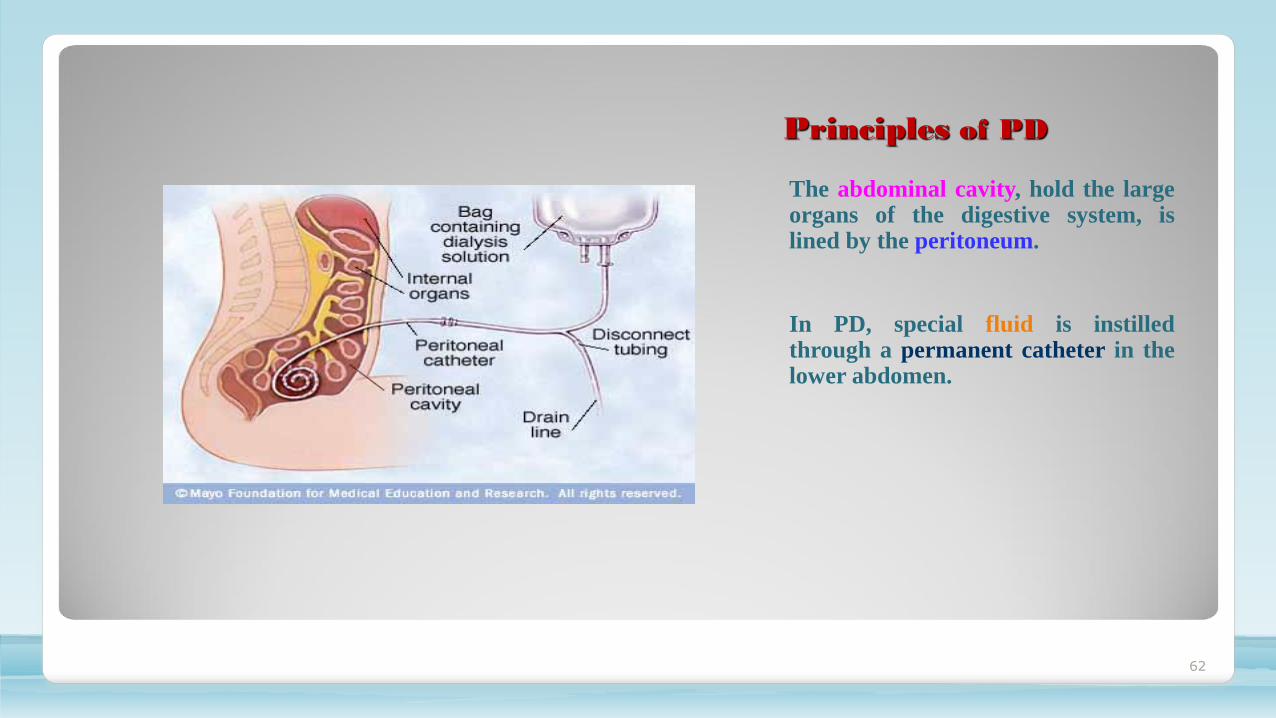
Principles of PD
The abdominal cavity, hold the largeorgans of the digestive system, islined by the peritoneum.
In PD, special fluid is instilledthrough a permanent catheter in thelower abdomen.

63
Principles of PD
• An osmotic pressure gradient is applied by the addition to the dialysis fluid of an osmotic agent which will “suck” fluid from the blood.
• The concentration of this osmotic agent is chosen to give just the fluid removal needed. In most cases glucose is used to create the osmotic pressure.
• Fluid is removed by ultrafiltration driven by an osmotic pressure gradient. (Eg. Yellow/Green/Red Bags)
64
Principles of PD
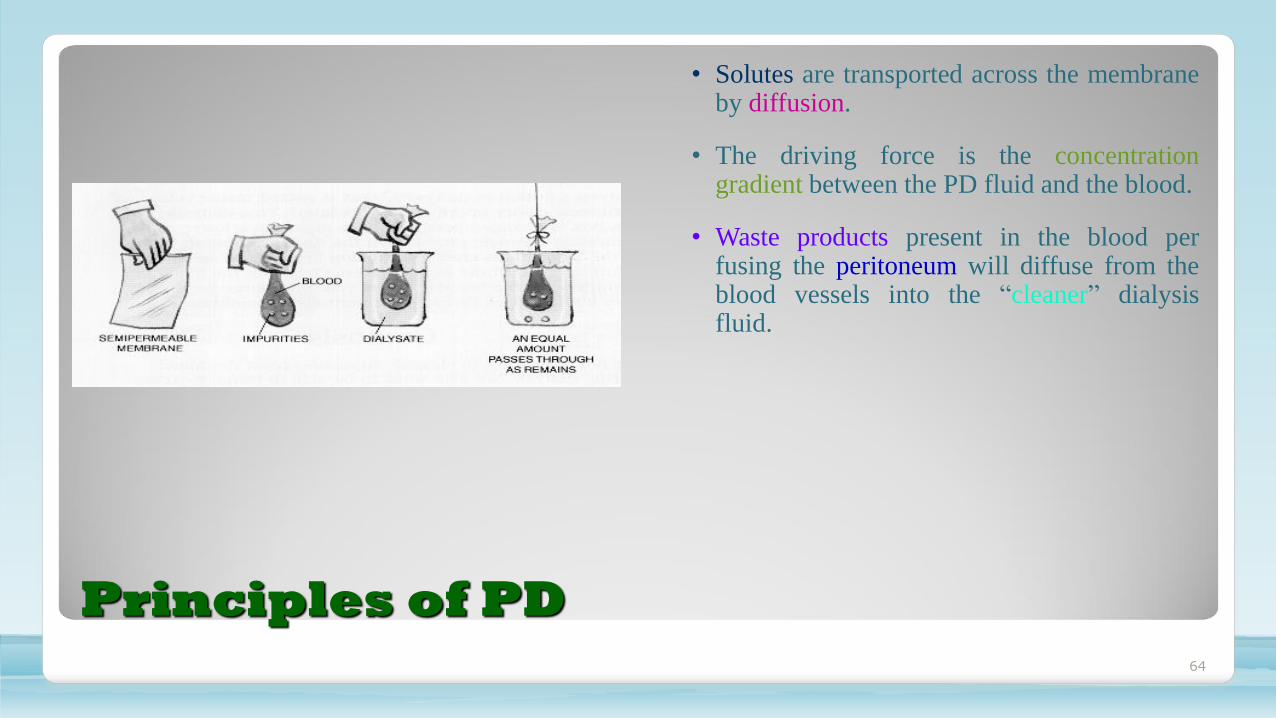
• Solutes are transported across the membraneby diffusion.
• The driving force is the concentrationgradient between the PD fluid and the blood.
• Waste products present in the blood perfusing the peritoneum will diffuse from theblood vessels into the “cleaner” dialysisfluid.
65
Principles of PD
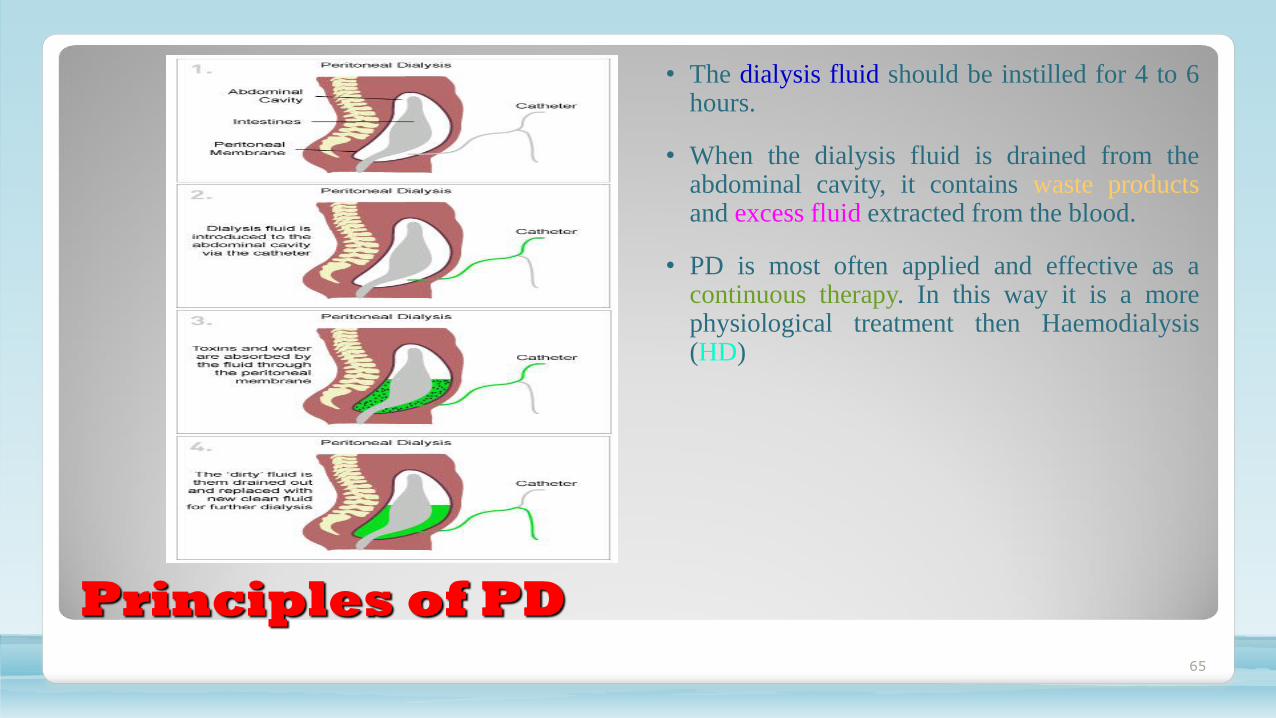
• The dialysis fluid should be instilled for 4 to 6hours.
• When the dialysis fluid is drained from theabdominal cavity, it contains waste productsand excess fluid extracted from the blood.
• PD is most often applied and effective as acontinuous therapy. In this way it is a morephysiological treatment then Haemodialysis(HD)

66
Principles PD / HD

67
Fluid Removal
• The osmotic agent normally used in PD fluid is glucose.
• Not an ideal osmotic agent, as it is readily transported across the peritoneum.
• Large concentration glucose creates a temporary osmotic gradient before being adsorbed into theblood.
• The higher the glucose concentration, the larger the osmotic pressure, resulting in a larger fluidremoval.
• If PD exchanges are missed or dwell more than 6-8 hours, fluid may be gained by the patient ratherthen lost.
• The Volume of dialysis solution administered is also important for the total fluid removal, as it willtake longer for the concentration gradient to decline in a large volume of fluid.

68
Solute Removal
• The most important principle for solute removalin PD is diffusion, for which the driving force isthe concentration gradient between the blood andthe dialysis fluid.
• Small solutes move quickly through themembrane creating an equilibrium during thedwell period.
• Larger solutes move slowly across theperitoneum, reaching equilibrium point takes along time.

69
Fluid Removal
• So………………………………………………………………Both solute and fluid removal in PD iscontrolled by
• 1) glucose concentration
• 2) dwell time
• 3) volume
• 4) peritoneal membrane characteristics

70
PD Fluid
• Components of PD fluid can be divided in into electrolytes, buffer and osmotic agents.
• The most abundant electrolyte in PD fluid is sodium. It’s hyponatremic, so it has a concentrationlower than blood to ensure sufficient removal of sodium.
• Standard PD fluid contains no potassium.
• Today, there is a tendency to use normcalcemic PD fluid as many patients receive extra calcium fromphosphate-binding drugs.
• The buffer normally used in PD is lactate. Lactate is metabolised to form bicarbonate, the mostimportant buffer in the blood.
71
Treatment Modes CAPD/APD
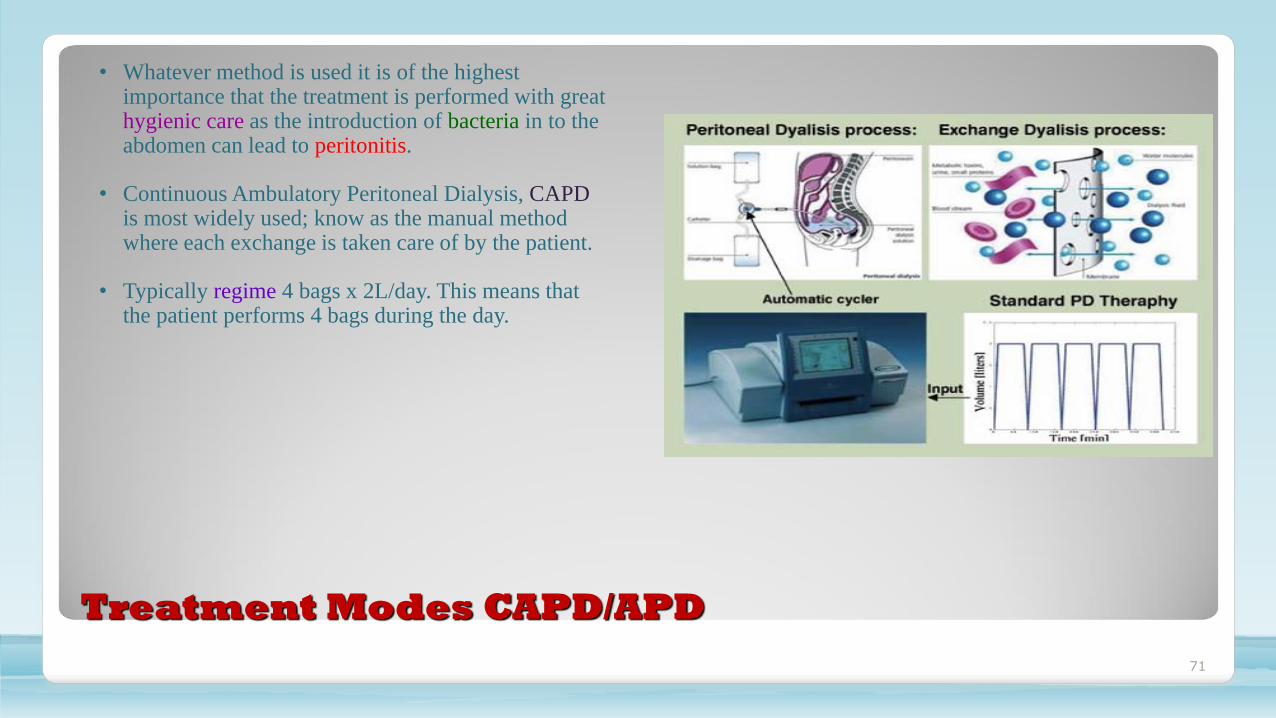
• Whatever method is used it is of the highest importance that the treatment is performed with great hygienic care as the introduction of bacteria in to the abdomen can lead to peritonitis.
• Continuous Ambulatory Peritoneal Dialysis, CAPDis most widely used; know as the manual method where each exchange is taken care of by the patient.
• Typically regime 4 bags x 2L/day. This means that the patient performs 4 bags during the day.
72
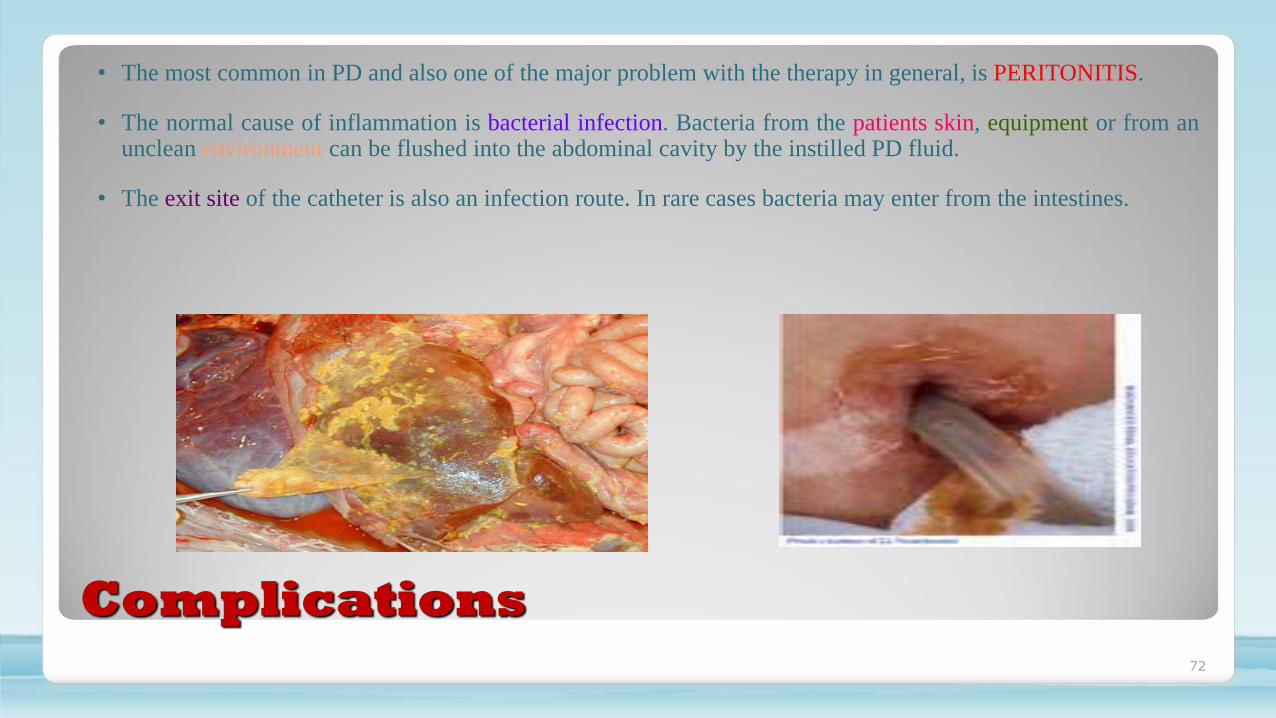
Complications
• The most common in PD and also one of the major problem with the therapy in general, is PERITONITIS.
• The normal cause of inflammation is bacterial infection. Bacteria from the patients skin, equipment or from anunclean environment can be flushed into the abdominal cavity by the instilled PD fluid.
• The exit site of the catheter is also an infection route. In rare cases bacteria may enter from the intestines.
73
Treatment Strategy
•Many factors are considered and assessed to ascertain the best effective treatment for each individual patient…………………………………………
•Personal needs and preferences are of great importance, to suit lifestyle.
•Some prefer nightly treatments and are comfortable operating a machine
•PD is often chosen as a temporary treatment of transplant candidates, waiting for a suitable kidney.
•PD is often the best choice for pediatric patients; as the continued blood purification is probably the reason why children grow better than HD.
•Cardiovascular problems and blood access problems can be impossible to treat on HD; PD is an alternative.
•The peritoneal membrane characteristics, ie. The transport properties of the peritoneum can vary widely among patients. A small person may have a large peritoneal surface area with many pores available for transport. However, a large person who needs much more
dialysis, may have only a small peritoneum.

Keep
your
kidneys
healthy

Drink enough
water every day.
Kidneys like
water a LOT!

Don’t eat food with too much salt!

Don’t eat food with too much sugar
and avoidsoft drinks!

Eat lots of fruit and vegetables!

Keep active!Play sports!
Do NOT smoke!

Do NOT
take drugs!

82





























