Embed Size (px)
Citation preview

NATIONAL TB CONTROL STRATEGIC PLAN
“VISION 2020” January 2014
National TB Control Program Pakistan Ministry of National Health Services, Regulations & Coordination
Islamabad
Foreword
It is a matter of great pleasure and satisfaction that National TB Control Program has taken
initiative towards development of 7 years National Strategic Plan for NTP Pakistan (2014-2020)
titled as “Vision 2020”.
Tuberculosis (TB) is a leading cause of death and a major public health problem not only globally but also in Pakistan as currently the country ranks 5thamongst the 22 HBCs and 4th among 27 MDR high burden countries in the world, constituting 65% of TB burden in EMRO.
Since the revival of NTP Pakistan, subsequent to declaration of TB as national emergency in 2001, the government of Pakistan has committed itself to control of tuberculosis in the country through DOTS strategy. National TB Control Program, working under the Ministry of National Health Services, Regulation & Coordination, integrated with Primary Health Care (PHC) system implemented by the district health authorities with the support of Provincial TB Control Programs (PTPs), is fighting against Tuberculosis in the country to reduce mortality, morbidity and spread of TB infection. NTP entails free of cost diagnosis and treatment of every TB patients through uninterrupted provision of quality assured anti TB drugs. 100% DOTS coverage in public sector was achieved in 2005 and MDG targets of 70% case detection and 85% treatment success rate were achieved by NTP in 2015.
This strategic plan has been developed in response to recent global and national innovative
interventions and approaches towards TB care and control with a vision to ensure universal
access of TB care and achieving Zero TB Death in the country.
Global innovations include “Systematic screening for active TB cases” to effectively address
missed and delayed TB cases, “WHO-approved rapid diagnostics (WRD)” such as Xpert MTB/RIF,
WHO recommended “Revised case definitions & reporting framework 2013” and most
importantly “Global Strategy beyond 2015”involving multi-sectoral strategic approaches and
new international targets for the post-2015to accelerate the global expansion of tuberculosis
care and control.
Of the most significant national developments to revise national strategic plan were,results of
“National TB prevalence survey (2011-12) and “National drug resistance survey” (2012-13)
defining revised targets for incidence and prevalence for both susceptible and drug resistant TB,
health sector devolution, limited public sector financing for TB control, stagnant TB case
notification, high number of undetected/undiagnosed TB cases in the community, Increasing

drug-resistant TB, managerial and governance issues and effects of social determinants
increasing poverty & social inequalities complicating the TB scenario in Pakistan.
National TB Strategic Plan “Vision 2020” entails developing innovative strategies that will:
1. Improve the performance and impact of TB control with maximizing public sector
investment and accountability in TB control activities.
2. Address sensitive and drug resistance TB by: (a) reducing diagnostic delay, (b) reducing
the duration and improving the efficacy of treatment, (c) preventing disease, and (d)
increasing access to DOTS and DR-TB treatment, etc.
3. Invest in new diagnostic and TB management tools and approaches that are less labor
intensive, more cost-effective, and can be delivered close to patients to minimize the
health workforce burden and help improve patient access, thereby increasing case
detection and enhance treatment success rates.
4. Prioritize research that has the potential to change policy and practice in TB care in the
country.
On behalf of Ministry of National Health Services, Regulations & Coordination, we appreciate
the joint efforts made by NTP / PTP / RTP teams and all national / international partners in the
development of this document. We are sure that National Strategic Plan “Vision 2020”will
enable NTP Pakistan to accelerate its pace towards achievement of its vision and targets for TB
care and control in Pakistan.
____________________ Mrs. Saira Afzal Tarar
State Minister, Ministry of National Health Services, Regulations & Coordination
Government of Pakistan Islamabad
________________ Dr. Ejaz Qadeer National Manager
National TB Control Program Pakistan Islamabad
March, 2014
2
NATIONAL STRATEGIC PLAN
“VISION 2020” January 2014
National TB Control Program Pakistan
Ministry of National Health Services, Regulations & Coordination,
Islamabad

3
Contents
1 INTRODUCTION ................................................................................................................... 14 1.1 POLITICAL AND ECONOMIC SITUATION ...................................................................... 14 1.2 SOCIO-DEMOGRAPHY OF PAKISTAN ........................................................................... 15 1.3 HEALTH SITUATION: ..................................................................................................... 15
1.3.1 Health infrastructure: Public sector 15
1.3.2 Health infrastructure: Other Public sector outlets (Other public sector) 17
1.3.3 Health infrastructure: Private sector 17
2 TUBERCULOSIS CONTROL: BURDEN AND EPIDEMIOLOGY ................................................. 21
3 STRATEGIC PLAN “VISION 2020” ......................................................................................... 22 3.1 NATIONAL TB STRATEGIC PLAN: 2012-16 .................................................................... 22 3.2 PROGRESS TOWARDS MDGs ....................................................................................... 23 3.3 IMPLEMENTATION OF STRATEGIC PLANS AND IMPACT ............................................. 23 3.4 INTERNATIONAL TB REVIEW MISSION: NOVEMBER, 2013 ......................................... 26 3.5 DEVELOPMENT PROCESS OF NATIONAL STRATEGIC PLAN “VISION 2020”................. 27
4 NATIONAL TB CONTROL PROGRAM PAKISTAN ................................................................... 35 4.1 EVOLUTIONARY PERSPECTIVE ..................................................................................... 35 4.2 STRUCTURE & FUNCTION ............................................................................................ 35
4.2.1 NTP arrangements for coordination of TB control activities in the country 36
4.3 LEVELS & RESPONSIBILITY............................................................................................ 37 4.4 TB CONTROL IN POST DEVOLUTION CONTEXT ............................................................ 39
5 SITUATION ANALYSIS ........................................................................................................... 42 5.1 POLITICAL COMMITMENT ........................................................................................... 42 5.2 TB CASE NOTIFICATION ............................................................................................... 44
5.2.1 TB burden analysis 44
5.2.2 Re-treatment cases 47
5.2.3 TB care facilities in Pakistan 48
5.2.4 TB Control service delivery in districts 52
5.2.5 Diagnostic algorithms 54
5.3 TB TREATMENT AND CASE HOLDING .......................................................................... 55 5.4 HOSPITAL DOTS LINKAGES ........................................................................................... 57 5.5 EXTRA-PULMONARY TB DIAGNOSIS ............................................................................ 59 5.6 CHILDHOOD TUBERCULOSIS ........................................................................................ 60 5.7 TB/HIV .......................................................................................................................... 61
4
5.8 TB IN ELDERLY .............................................................................................................. 63 5.9 TB, OTHER CHRONIC AILMENTS AND TOBACCO USE .................................................. 63 5.10 TB and diabetes ........................................................................................................... 64 5.11 MANAGEMENT OF CONTACTS .................................................................................... 64 5.12 QUALITY ASSURED BACTERIOLOGY ............................................................................. 65 5.13 DRUG-RESISTANT (DR) TB ............................................................................................ 79 5.14 PUBLIC-PRIVATE MIX ................................................................................................... 95 5.15 DRUG MANAGMENT .................................................................................................. 106 5.16 ACSM .......................................................................................................................... 111 5.17 MONITORING, EVALUATION, RESEARCH AND LEARNING (MERL) ............................ 113 5.18 OPERATIONAL RESEARCH .......................................................................................... 114 5.19 HUMAN RESOURCE DEVELOPMENT .......................................................................... 118
6 SWOT ANALYSIS ................................................................................................................ 120 6.1 POLITICAL COMMITMENT ......................................................................................... 120 6.2 TB CASE NOTIFICATION ............................................................................................. 120 6.3 CONTACT INVESTIGATION ......................................................................................... 121 6.4 CHILDHOOD TB .......................................................................................................... 121 6.5 HOSPITAL DOTS LINKAGE (HDL) i.e. TEACHING HOSPITAL ........................................ 122 6.6 ACSM .......................................................................................................................... 122 6.7 DRUG MANAGEMENT ................................................................................................ 122 6.8 TRAINING ................................................................................................................... 123 6.9 TB CARE IN ELDERLY AND HIGH RISK GROUPS .......................................................... 124 6.10 TB-HIV CO-INFECTION ................................................................................................ 124 6.11 TB AND CHRONIC AILMENTS AND TOBACCO SMOKING ........................................... 124 6.12 LABORATORY NETWORK ........................................................................................... 124 6.13 DRUG RESISTANT-TB .................................................................................................. 129 6.14 PUBLIC PRIVATE MIX (PPM) ....................................................................................... 131 6.15 MONITORING AND SUPERVISION .............................................................................. 133 6.16 OPERATIONAL RESEARCH .......................................................................................... 134 6.17 STOP TB PARTNERSHIP .............................................................................................. 135 6.18 TRANS-BORDER TB ..................................................................................................... 135 6.19 TB AND POVERTY ....................................................................................................... 135
7 GAP ANALYSIS .................................................................................................................... 137 7.1 FUNDING MAINLY DEPENDS ON EXTERNAL SUPPORT .............................................. 137 7.2 LOW TB CASE NOTIFICATION ..................................................................................... 137 7.3 LOW PROPORTION OF TB CONTACT ARE INVESTIGATED FOR TB ............................. 138 7.4 CHILDHOOD TB CASES NOT FULLY REPORTED TO NTP ............................................. 138 7.5 HOSPITAL DOTS LINKAGE (HDL) NOT FULLY OPERATIONAL ...................................... 138 7.6 ACSM STRATEGY NOT ABLE TO CREATE AN IMPACT ON INCREASING CASE FINDING138 7.7 SIGNIFICANT ISSUES IN DRUG MANAGEMENT.......................................................... 139 7.8 SIGNIFICANT ISSUES IN TRAINING IN TB CONTROL ................................................... 139 7.9 NO SPECIFIC ACTIONS HAVE BEEN ESTABLISHED TO TARGET ELDERLY .................... 139 7.10 LIMITED IMPLEMENTATION OF TB/HIV COLLABORATIVE ACTIVITIES ...................... 140

5
7.11 NOSPECIFIC INTERVENTION HAS BEEN ESTABLISHED TO ADDRESS TB & CHRONIC AILMENTS AND TB &TOBACCO USE .......................................................................... 140
7.12 TB LABORATORY NETWORK NOT FULLY OPTIMIZED ................................................ 140 7.13 MANY CARE PROVIDERS OUTSIDE THE NTP NETWORK ARE NOT INVOLVED IN TB
CARE AND CONTROL EFFORTS ................................................................................... 143 7.14 A HIGH PROPORTION OFDR-TB PATIENTS ARE NOT DETECTED ................................ 145 7.15 ISSUES IN OPERATIONALIZING MONITORING, SUPERVISION AND EVALUATION AT
PROVINCIAL AND DISTRICT LEVELS ............................................................................ 146 7.16 TB CONTROL PROBLEMS NOT ADDRESSED THROUGH OPERATIONAL RESEARCH .... 147 7.17 NON FUNCTIONING NATIONAL STOP TB PARTNERSHIP ........................................... 147 7.18 TB IN TRANS-BORDER POPULATIONS NOT OPERATIONAL........................................ 147 7.19 NOSPECIFIC INTERVENTION HAS BEEN ESTABLISHED TO ADDRESS TB &POVERTY,
Legislation on drug sale, declaring TB as notifiable disease ...................................... 147
8 STRATEGIES AND ACTIVITIES: TB CONTROL “VISION 2020” ............................................. 150 8.1 OVERVIEW: NATIONAL TB STRATEGIC PLAN “VISION 2020” .................................... 150 8.2 GOAL AND OBJECTIVES: ............................................................................................. 151 8.3 PRIORITY PROGRAM AREAS:...................................................................................... 151
9 LIST OF LITERATURE REVIEWED (REFERENCES AND ANNEXURES) ................................... 174
List of Tables
Table 1: Status of health facilities, GoP: 2009 .............................................................................. 16
Table 2: Private health care providers by country/province4 2009-10 ........................................ 18
Table 3: Private health care providers 2009-10 by type, size and province4 ............................... 19
Table 4: Out-patient service providers 2009-10 by type and province3 ...................................... 20
Table 5: Process of Strategic Plan Development .......................................................................... 28
Table 6: NTP Human Resource and funding support .................................................................... 36
Table 7: PSDP allocation- Post devolution (2011-2014) ............................................................... 43
Table 8: PC-1 status in TB Control Pakistan .................................................................................. 43
Table 9:Year-wise notified TB cases and NSS+ Pakistan ............................................................... 45
Table 10: Estimates of TB burden 2012 ........................................................................................ 46
Table 11: Proportion of re-treatment cases reported .................................................................. 48
Table 12: BMUs 2013 (Public i.e. Health Sector) and (Other Government Run Facilities i.e. Other
public sector) ................................................................................................................................ 49
Table 13: BMUs 2013 by source of funding (Private) and (GP clinics) ......................................... 50
Table 14: Districts with urban/sub-urban population ≥ one million ............................................ 51
Table 15: Characteristics of essential Anti-TB drugs..................................................................... 55
Table 16: Type of FDCs recommended by NTP ............................................................................. 56
Table 17: FLDs prescription schedule ........................................................................................... 56
Table 18: Contribution of HDL in core TB DOTS, 2012 ................................................................. 59

6
Table 19: TB/HIV Intervention Sites .............................................................................................. 63
Table 20: Milestones achieved by the laboratory network .......................................................... 66
Table 21: Functional level /location and current defined responsibilities are as follows ............ 66
Table 22: LED numbers by donor support and location ............................................................... 68
Table 23: Microscopy services coverage by population ............................................................... 68
Table 24: Gene-Xpert Expansion Plan ........................................................................................... 70
Table 25: TB Culture expansion plan ............................................................................................ 71
Table 26: Drug resistance pattern at NRL 2012 ............................................................................ 72
Table 27: Training categories for Microscopy network staff ........................................................ 73
Table 28: Laboratory training support in 2012 ............................................................................. 74
Table 29: Diagnostic network in Pakistan ..................................................................................... 75
Table 30: Trend of key laboratory indictors 2006 to 2012 ........................................................... 77
Table 31: Participating Laboratories in National EQA Scheme for DST 2012 ............................... 78
Table 32: Estimates of DR-TB in Pakistan 2012 based on WHO estimates .................................. 80
Table 33: SLDs for DR-TB patients recommended by NTP ........................................................... 85
Table 34: SLDs need assessment .................................................................................................. 86
Table 35: Province wise PMDT sites and cases (2012) ................................................................. 89
Table 36: Province wise TB culture sites and diagnosis and follow-up performance .................. 90
Table 37: TB DST expansion plan 2013 ......................................................................................... 91
Table 38: Status Gene Xpert tests (2012) and expansion plan (2013) ......................................... 92
Table 39:Category and training days for DR-TB ............................................................................ 95
Table 40: GPs involved in TB care by province, 2013 ................................................................. 101
Table 41:Type and number of PHC facilities being management by PPHI/PRSP in Pakistan ..... 103
Table 42: Type and number of facilities: Armed Forces ............................................................. 104
Table 43: Type and number of facilities: Fauji Foundation ........................................................ 105
Table 44: Type and number of facilities: Social Security ............................................................ 106
Table 45: Anti-TB drugs situation................................................................................................ 110
Table 46: ACSM activities status ................................................................................................. 112
Table 47: Recommended staff training in NTP/PTPs .................................................................. 118
Table 48: TB suspects to be identified 2014-2020 ...................................................................... 154
Table 49: TB cases projection 2014-2020 ................................................................................... 155
Table 50: TB treatment success projection 2014-2020 .............................................................. 156
Table 51: Contact management projection 2014-2020 .............................................................. 156
Table 52: Childhood TB case projection 2014-2020 ................................................................... 157
Table 53: Projected TB cases to be screened for HIV at sentinel sites 2014-2020 .................... 160
Table 54: Number of suspects to be identified 2014-2020 ........................................................ 161
Table 55: Number of GeneXpert machines required 2014-2020 ............................................... 162
Table 56: Number of culture laboratories required 2014-2020 ................................................. 163
7
Table 57: Number of DST laboratories required 2014-2020 ...................................................... 163
Table 58: Contribution projected for PPM in country 2014-2020 .............................................. 164
Table 59: DR-TB cases to be enrolled 2014-2020 ....................................................................... 167
List of Figures
Figure 1: Impact of interventions on decrease TB incidence over years ...................................... 24
Figure 2 Impact of interventions on decrease TB prevalence over years .................................... 24
Figure 3 Impact of interventions on decrease TB mortality over years ....................................... 24
Figure 4: Organization of TB control program Pakistan ............................................................... 36
Figure 5: Financial Allocation for National TB Control Program 2004 – 2012 (Million PKR) ........ 42
Figure 6: Contribution to TB control activities by funding source5: 2012-13 ............................... 44
Figure 7: Provincial TB Case notification and population proportion .......................................... 46
Figure 8: Case notification by age (%) – National – 2012 ............................................................. 47
Figure 9: Diagnostic procedure for suspected pulmonary TB ...................................................... 54
Figure 10: Microscopy EQA coverage and performance .............................................................. 75
Figure 11: PPM contribution in total case notification NSS+ (2001-2012) ................................... 98
Figure 12: Case notification: Public - Private 2012 ....................................................................... 99
Figure 13:PPM CONTRIBUTION NSS+ –ALL PROVINCES (Q1 2013) .............................................. 99
Figure 14: Province wise PPM contribution: TB new sputum smear positive cases/ all types .. 100
Figure 15: System of M&E operations in the country ................................................................ 114
Figure 16: Percentage of anti-TB drugs sold in private market .................................................. 117

8
Foreword
•
It is a matter of great pleasure and satisfaction that National TB Control Program has taken
initiative towards development of 7 years National Strategic Plan for NTP Pakistan (2014-
2020)titled as “Vision 2020”.
Tuberculosis (TB) is a leading cause of death and a major public health problem not only
globally but also in Pakistan as currently the country ranks 5thamongst the 22 HBCs and 4th
among 27 MDR high burden countries in the world, constituting 65% of TB burden in EMRO.
Since the revival of NTP Pakistan, subsequent to declaration of TB as national emergency in
2001, the government of Pakistan has committed itself to control of tuberculosis in the country
through DOTS strategy. National TB Control Program, working under the Ministry of National
Health Services, Regulation & Coordination, integrated with Primary Health Care (PHC) system
implemented by the district health authorities with the support of Provincial TB Control
Programs (PTPs), is fighting against Tuberculosis in the country to reduce mortality, morbidity
and spread of TB infection. NTP entails free of cost diagnosis and treatment of every TB
patients through uninterrupted provision of quality assured anti TB drugs.100% DOTS coverage
in public sector was achieved in 2005 and MDG targets of 70% case detection and 85%
treatment success rate were achieved by NTP in 2015.
This strategic plan has been developed in response to recent global and national innovative
interventions and approaches towards TB care and control with a vision to ensure universal
access of TB care and achieving Zero TB Death in the country.
Global innovations include “Systematic screening for active TB cases” to effectively address
missed and delayed TB cases, “WHO-approved rapid diagnostics (WRD)” such as Xpert
MTB/RIF,WHO recommended “Revised case definitions & reporting framework 2013” and most
importantly “Global Strategy beyond 2015”involving multi-sectoral strategic approaches and
new international targets for the post-2015to accelerate the global expansion of tuberculosis
care and control.
Of the most significant national developments to revise national strategic plan were, results of
“National TB prevalence survey (2011-12) and “National drug resistance survey” (2012-13)
defining revised targets for incidence and prevalence for both susceptible and drug resistant TB,
health sector devolution, limited public sector financing for TB control, stagnant TB case
notification, high number of undetected/undiagnosed TB cases in the community, Increasing

9
drug-resistant TB, managerial and governance issues and effects of social determinants
increasing poverty & social inequalities complicating the TB scenario in Pakistan.
National TB Strategic Plan “Vision 2020” entails developing innovative strategies that will:
1. Improve the performance and impact of TB control with maximizing public sector
investment and accountability in TB control activities.
2. Address sensitive and drug resistance TB by: (a) reducing diagnostic delay, (b) reducing
the duration and improving the efficacy of treatment, (c) preventing disease, and (d)
increasing access to DOTS and DR-TB treatment, etc.
3. Invest in new diagnostic and TB management tools and approaches that are less labor
intensive, more cost-effective, and can be delivered close to patients to minimize the
health workforce burden and help improve patient access, thereby increasing case
detection and enhance treatment success rates.
4. Prioritize research that has the potential to change policy and practice in TB care in the
country.
On behalf of Ministry of National Health Services, Regulations & Coordination, we appreciate
the joint efforts made by NTP / PTP / RTP teams and all national / international partners in the
development of this document. We are sure that National Strategic Plan “Vision 2020”will
enable NTP Pakistan to accelerate its pace towards achievement of its vision and targets for TB
care and control in Pakistan.
____________________
Mrs. SairaAfzalTarar
State Minister,
Ministry of National Health Services, Regulations &
Coordination
Government of Pakistan
Islamabad
________________
Dr. Ejaz Qadeer
National Manager
National TB Control Program
Pakistan
Islamabad
March, 2014
10
LIST OF ABBREVIATION ADR Adverse Drug Reaction AFB Acid Fast Bacilli AJK Azad Jammu Kashmir AKHSP Aga Khan Health Services
Pakistan AKU Aga Khan University BHU Basic Health Unit BMU Basic Management Unit CCM Country Coordinating
Mechanism CDC Communicable Disease Control CHW Community Health Worker CPT Co-trimoxazole Preventive
Therapy DDHO Deputy District Health Officer DGHS Director General Health
Services DHO District Health Officer DHQ District Headquarter Hospital DLS District Laboratory Supervisor DMU Drug Management Unit DTC District TB Coordinator DO Direct Observation DOTS Directly Observed Treatment
(short course) DR TB Drug Resistant TB DRS Drug Resistance Survey DST Drug Sensitivity Testing EDO Executive District Officer EQA External Quality Assurance EPTB Extra Pulmonary TB FATA Federally Administered Tribal
Area FLD First Line Drug GB GilgitBaltistan GDF Global Drug Facility GF Global Fund GFATM Global Fund to Fight Against
AIDS, Tuberculosis and Malaria GP General Practitioner GNP Gross National Product HCP Health Care Practitioner HMIS Health Management
Information System
HIV Human Immunodeficiency Syndrome
HPF High-Power Field IEC Information, Education and
Communication ICT Islamabad Capital Territory INH Isoniazid IPC Interpersonal Communication KP KhyberPakhtunkhwa LED Light Emitting Diode LHW Lady Health Worker LPA Line Probe Assay MALC Marie-Adelaide Leprosy Center MDR-TB Multi-drug Resistant
Tuberculosis MDG Millennium Development Goals M&E Monitoring and Evaluation MO Medical Officer MS Medical Superintendent NGOs Non-government Organizations NSP National Strategic Plan NTP National Tuberculosis Control
Program PATA Pakistan Anti-TB Association PCS Pakistan Chest Society PC-1 Planning Commission Proforma-
1 PSCM Procurement and Supply Chain
Management PHC Primary Health Care PTB Pulmonary TB PMA Pakistan Medical Association PMDT Programmatic Management of
Drug Resistant TB PPHI People’s Primary Health Care
Initiative PPM Public Private Mix PR Principal Recipient PRL Provincial Reference Laboratory PTP Provincial Tuberculosis Control
Program RHC Rural Health Center RR-TB Rifampicin-resistant TB SLD Second Line Drug STAG-TB Strategic and Technical
Advisory Group on TB TB Tuberculosis

11
TBC Tuberculosis Clinic THQ Tehsil Headquarter Hospital XDR-TB Extensively Drug-resistant TB WHO World Health Organization
WRD WHO-approved Rapid Diagnostics
12
LIST OF CONTRIBUTERS
National TB Control Program, Pakistan
Provincial / Regional TB Control Programs
Global/National Experts/Partners
Consultants
Dr. EjazQadeer, National Manager
AJ&K Dr. Shabbir Ahmed Dar - Manager Dr. SaeedAwan, Dr. NajeebAhsan BALOCHISTAN Dr. GhulamMurtaza Shah - Manager Dr. LubnaSiddiqui Dr. Ahmad Wali Dr. Muhammad Ashraf Dr. IrfanRaisani FATA Dr. SartajYousafzai - Manager Dr. Qasim Dr. Nekdad GILGIT BALTISTAN Dr. Mubeen Ahmed - Manager Dr. Ghulam Mustafa KHYBER PAKHTUNKHWA Dr. UbaidHussain – Project Director Dr. Maqsood Ali Khan Dr. Amir Rafiq Dr. Dost Muhammad Dr. SaeedAbid ICT Dr. Azhar DHO ICT Dr. NajeebDurrani Dr. Imtiaz Ali Memon PUNJAB Dr. Muhammad Naeem – Manager Dr. ZarfishanTahir Dr. Ahmed Nadeem Dr. ZakiaParveen Dr. Muhammad Zubair SINDH Dr. Ismat Ara, Director Dr. Amanullah Ansari Dr. Syed Saleem Hassan Dr. Muzaffar Ali Khoharo Dr. MansoorButtoo
Global TB Program WHO-Geneva - Dr. Christpher Gilpin, Scientist/Lab, Diagnostics -Dr.Douglas Fraser Wares,Lab, Diagnostics & Drug Resistance Ines Garcia Baena, Economist - Ms. Soleil Global Fund Werner Buehler Indus Hospital Karachi Dr. Amir Khan W.H.O Dr. GhulamNabiKazi, Stop TB Partnership Dr. Iqtidar Ahmad, ASD Dr. Amir Khan, Mercy Corps Dr. Farah Naureen Dr. Arif Noor Ms. Jennifer Norman ACD Dr. AkmalNaveed Dr. Abdul Latif Ojha Institute Dr. ShahinaQayyum BRIDGE Foundation Dr. Sharaf Ali Shah Greenstar Dr. Khalid Farough Dr. Haroon Ibrahim MSH Edmund Rutta Ms. Maheen Malik Shifa International Prof. Dr. Ejaz Khan MALC Mr. Muhammad Shabbir Pakistan Chest Society Dr. Wajid Ali PIMS Dr. Maqbool Ahmed GIZ Ms. Kathy Fiekert Ms. DarinkaPerisic KFW-Epos Dr. MazharHussain USAID Dr. Muhammad Isa
Dr. Salah Ottmani (International) Dr. Nauman Safdar (National)
Dr. Basharat Javed-NTO, Focal Person for National/Provincial Strategic Plans
PIU Dr. Raja Ayub Dr. FakhraNaheed Dr. Amir Safdar
PR Unit Dr. AbulKhaliqGhauri Dr. Furqan Ahmed
NRL Dr. SabiraTahseen Dr. Laeeq Ahmed
TB-Drug Mgt Unit Dr. Zia Dawar Dr. WaqasRabbani
M&E Unit Dr. FarooqKhattak Mr. Tanveer Ahmed Mr. Mhammad Zia Samad
DR-TB Dr. ZafarIqbalToor Dr. AsifAwan Dr. Salem Barghout
Research Unit Dr. Razia Fatima
Infection Control Col. Dr.Amjad Dr. YasirWaheed
Finance Unit Syed Mubashar Ahmed
IT Unit
Medhi Abas Hemani
PPM Unit Dr. HussainHadi

13
COREPLAN
SECTION A1- BACKGROUND

14
1 INTRODUCTION
1.1 POLITICAL AND ECONOMIC SITUATION The Islamic Republic of Pakistan has a parliamentary system of government. The President of
Pakistan is the head of state, the Prime Minister is head of government, and there is a multi-
party system. Executive power is exercised by the government and legislative power is largely
vested in the parliament. The bicameral federal legislature consists of the Senate (upper house)
and National Assembly (lower house). However, in the past few decades the country went
through several political transitions including parliamentary, presidential or semi-presidential
and marshal law. Pakistan is currently facing challenges within and across the border including
conflicts in a few districts resulting in internally displaced populations.
The Government of Pakistan vide 18th constitutional amendment devolved multiple functions,
including federal units of health programs, to the provinces with effect from 1st July 2011.
However, recognizing the importance of several health functions, including the management of
a few key public health programs, a Federal Ministry of National Health Services, Regulations &
Coordination (NHS, R&C) has been established in Islamabad; the National TB Control Program
(NTP) is being managed by this Ministry.
The country belongs to a group of low-income high TB burden countries, has primarily an
agrarian economy (66% population lives in the rural area), and has diverse cultural and
geographical patterns. Health cannot be segregated from the country’s overall economic and
social development. Pakistan’s Human Development Index (0.515) ranks low 146 out of 187
countries and its GDP per capita is estimated as 2,566 US$. Life expectancy and education are
also low; 0.487, 0.217.1. The annual per capita health expenditures for Pakistan as per National
Health Accounts (NHA) 2009-10 are (Rs.2,611) 31.2 US$2. For comparison, the respective figures
reported to WHO by India and Bangladesh are 51.0 US$ and 25.0 US$, respectively. According
to the NHA, the ratios of health expenditures over GDP (2009-10) are 3.0% while this ratio for
public and private sector health expenditures is 9.2% and 2.5% respectively. In the health
sector, Pakistan is receiving major international grants from the Global Initiative for Vaccination
and Immunization (GAVI), the Global Fund to Fight against AIDS, TB and Malaria (GFATM) and
USAID.
According to the HDI, 60.3% of Pakistan's population lives on under $2 a day and some 21% live
on under $1 a day. Wealth distribution in Pakistan is highly uneven. This situation creates a
severe impact on diseases of poor among which TB is the lead communicable disease.
1United Nations Development Program, HDI report 2013
2 National Health Accounts 2009-10, Pakistan Bureau of Statistics, Government of Pakistan

15
Globally, a huge loss in income was observed3 before and after TB diagnosis (26% and 33%
respectively).
1.2 SOCIO-DEMOGRAPHY OF PAKISTAN Pakistan belongs to the South Asian region and covers an area of about 796,096 sq. kilometers.
It is bordered by Afghanistan to the north-west and Iran to the west while the People's Republic
of China borders the country in the north and India to the east. The last population census was
done in 1998. Currently the country population4 is estimated at 182.5million with 35% urban
and 65% rural. Pakistan has five provinces; Balochistan, Gilgit-Baltistan (GB), Khyber
Pakhtunkhwa (KP), Punjab, Sindh, and three regions; Azad Jammu Kashmir (AJK), Federally
Administered Tribal Areas (FATA) and Islamabad Capital Territory (ICT). The highest population
density is in Punjab province and lowest in Balochistan province. The population5 between 0-14
is 39%, 15-64 is 57% and above 65 years is 4% whereas, and there are 1.07 male / female in the
country.
The national language of the country is Urdu whereas the official language is English. 98% of
languages spoken in Pakistan are Indo-Iranian (sub-branches: 75% Indo-Aryan and 20% pure
Iranian), a branch of Indo-European family of languages. The major ethnic groups of Pakistan in
numerical size include: Punjabis, Pashtuns, Sindhis, Saraikis, Muhajirs, Balochis, Hindkowans,
Chitralis and other smaller groups.
In past few years, Pakistan has faced several natural disasters including earthquakes and
flooding in several districts across the country and is prone to such natural disasters in future.
1.3 HEALTH SITUATION: In Pakistan the distribution of years lost by causes is mainly due to communicable diseases
(64%)6 followed by non-communicable disease (26%) and injuries (9%). The under-5 mortality
rate (per 1000 live births) is 72, whereas the maternal mortality ratio (per 100,000 live births) is
260 in 2011. Pakistan ranks as the 5th highest TB burden country in the world, 7th globally
among the highest number of people living with diabetes and 9th globally in terms of tobacco
use among men, which is continuously increasing.
1.3.1 Health infrastructure: Public sector
The health system is generally weak and services are highly unregulated. Communicable
diseases are still the leading causes of morbidity and mortality and non-communicable diseases
3Eliminating the financial hardship of TB via universal health coverage and other social protection measures: WHO,
2013. 4 National Institute of Population Studies, Government of Pakistan, 2012
5 Pakistan Demographic and Health Survey, 2012-13
6 Pakistan health profile, WHO, 2013

16
are on the rise. The public sector is the main source for the provision of preventive care and
hospital care to the urban and rural populations. In the provision of curative care for minor
ailments, the public sector caters services to around 25% of the population. Health services in
the public sector are provided by various types of general and specialized hospitals. There is
also a network of primary health care outlets including Rural Health Centers (RHCs), Basic
Health Units (BHUs), dispensaries and Maternity and Child Health (MCH) centers, which are
mainly under the control of the provincial departments of health. Other organized semi-public
sectors include health care institutions established and run by armed forces, police, railways,
fauji foundation, municipal authorities, and employees’ social security institution. Under the
constitutional devolution process in 2001, districts were the implementing units and Executive
District Officer Health was in charge of all preventive, promotional and curative health
programs and services. In each district usually there is one District Headquarter (DHQ) Hospital,
three to four Tehsil Headquarter (THQ) Hospitals, 10 to 15 Rural Health Center (RHC) and 50 to
100 Basic Health Units (BHU). RHC and BHU are first level Primary Health Care facilities and
generally deal with uncomplicated routine cases, in addition to preventive and promotional
activities. DHQ and THQ level hospitals are secondary level facilities and are involved in the
treatment of less complicated cases. There are Tertiary Level Hospitals in Provincial capitals and
in some large districts, which deal with referred and complicated cases. According to MoH data,
the status of the various health facilities are as under:
Table 1: Status of health facilities7, GoP: 2009
Year Number of Facilities Total
Hospital Dispensaries MCH
Centers
RHCs BHUs TBCs Facilities Beds
1971 495 2136 668 87 249 79 3714 34077
1980 602 3466 812 217 736 98 5931 47412
1990 756 3795 1050 459 4213 220 10493 72997
2000 876 4635 856 531 5171 274 12343 93907
2005 919 4632 907 556 5334 289 12637 101490
7Ministry of Health, Government of Pakistan, Year book 2009

17
2007 945 4725 903 560 5349 290 12772 103285
2009 968 4813 906 572 5450 293 13002 103709
The capacity of the district health authorities is generally considered suboptimal and this is one
of the main reasons for unsatisfactory progress in health care delivery and indicators. Another
issue at the district level is lack of coordination among the various stakeholders. This includes
the district health management teams, coordinators of vertical programs and NGOs. The
Government has contracted NGOs such as the Punjab Rural Support Program (PRSP) in Punjab
and People’s Primary Health Care Initiative (PPHI) in Balochistan, Sindh, KP and AJK and the
financial and administrative control of BHUs have been handed over to them. Although the
utilization of health services and availability of drugs improved after this initiative, the focus has
been diverted towards curative services. Preventive programs and routine promotional
activities are not being performed as well as they previously were in these centers8.
1.3.2 Health infrastructure: Other Public sector outlets (Other public sector)
This mainly includes; Hospitals and health care centers being managed by organizations such as
the Pakistan Armed Forces, which has more than 50 hospitals with mostly specialized facilities,
Social Security having a chain of 50 hospitals and health centers in the country, and Fauji
Foundation with almost 70 hospitals and health centers. In addition, there are many health
facilities in the country, which are being managed by the department of Police and Jails,
Railway, etc. These health facilities have an enormous potential to contribute to TB care
delivery in the country.
1.3.3 Health infrastructure: Private sector
The private sector is large and unregulated comprising both qualified and unqualified service
providers in the disciplines of Allopathy, Homeopathy and tibb(Traditional Herbal Medicine).
The private sector caters to about 75% of the population’s curative primary healthcare needs in
addition to low cost hospital care. Qualified providers include the not-for-profit NGOs as well as
for-profit private sector institutions and individual practitioners. The not-for profit NGOs range
from small-scale local setups to a countrywide network of health outlets such as PRSP/PPHI
(managing about 4,000 primary health care facilities in the country). The technical and
managerial capacity of the NGOs varies widely. In context of TB control services there is a vast
network of health centers country-wide, being managed by the Pakistan Anti-TB Association
(PATA), which are exclusively providing TB care services.
8Nishtar, S 2006, p s61

18
Table 2: Private health care providers by country/province4 2009-10
Country/province Urban Rural Total
Number % Number % Number %
Pakistan 83,689 40 123,023 60 206,712 100
Punjab 47,005 36 83,406 64 130,411 63
Sindh 23,642 71 9,637 29 33,279 18
KP 11,047 29 27,052 71 38,099 18
Balochistan 1,995 41 2,928 59 4,923 2
Table 2 shows the total estimated health care providers at the national level was 206, 712 in
2009-10. The distribution of health care providers varies among the provinces. Punjab, being
the most populous province, leads with 63% of the total private sector health care providers. As
the least populated province, Balochistan has only 2% of the total private sector health care
providers. Sindh and Khyber Pakhtunkhwa (KP) contain 16% and 18% of the total private sector
health care providers respectively.
The urban/rural comparison for the provinces shows that Sindh has the highest percentage of
urban health care providers (71%) followed by Balochistan (41%), Punjab (36%) and KP (29%).
With respect to rural health care providers, KP has the highest percentage (71%) followed by
Punjab (64%), Balochistan (59%) and Sindh (29%).

19
Table 3: Private health care providers 2009-10 by type, size and province2
Country/province
Hospitals Out-
patient
service
providers
Laboratory
and
Diagnostic
services
providers
Total Big (>50
beds)
Small
(<50
beds)
Total
Number
Pakistan 125 4,255 4,380 196,843 5,489 206,712
Punjab 66 2,610 2,676 125,171 2,564 130,411
Sindh 46 1,018 1,064 30,742 1,473 33,279
KP 11 568 579 36,205 1,315 38,099
Balochistan 2 59 61 4,725 137 4,923
%
Pakistan 0.1 2.0 2.1 95.2 2.7 100
Punjab 0.1 2.0 2.1 96.0 2.0 100
Sindh 0.1 3.1 3.2 92.4 4.4 100
KP 0.0 1.5 1.5 95.0 3.5 100
Balochistan 0.0 1.2 1.2 96.0 2.8 100
Table 3 above shows the estimated number and percentage of health care providers by three
major service provision categories including the breakdown per size of hospital. As expected,
the number of out-patient service providers are much greater in number than ‘Hospitals’ and
‘Laboratories and diagnostic service providers’. It is estimated that there are 125 big hospitals
and 4,255 small hospitals in Pakistan; for both sizes Punjab has the highest number, followed by
Sindh, KP and Balochistan.

20
Table 4: Out-patient service providers 2009-10 by type and province3
For all of Pakistan, the estimated total number of out-patient health service providers is
196,843; of these, individually run solo clinics (Allopathic clinics) have the highest proportion
(49%) followed by Traditional Birth Attendant/ Dai (15%), Hakeem/Herbalist clinics (14.7%),
Homeopathic clinics (14%), Dental clinics (3.3%) and others (3.3%). Punjab has the highest
proportion (64%) of the total out-patient service providers followed by KP (18%), Sindh (16%)
and Balochistan (2%).
In addition, anecdotal information suggests that there are three times more unqualified than
qualified providers in Pakistan.
Co
un
try pro
vince
Ind
ividu
ally run
solo
clin
ics
Ou
t-patien
t cen
ters
Den
tal clinics
Ho
meo
path
ic clinic
Hakee
m/H
erbalist
clinic
Traditio
nalb
irth
attend
ant/D
ai
Oth
ers
Total
Number
Pakistan 96,645 916 6,443 27,819 28,985 29,445 6,590 196,843
Punjab 47,749 541 3,865 22,584 23,402 21,264 5,766 125,171
Sindh 19,548 99 1,214 2,241 3,062 4,169 409 30,742
KP 26,222 258 1,230 2,830 2,2225 3,049 391 36,205
Balochistan 3,126 18 134 164 296 963 24 4,725
%
Pakistan 49.1 0.5 3.3 14.1 14.7 15.0 3.3 100
Punjab 38.1 0.4 3.1 18.0 18.7 17.0 4.6 100
Sindh 63.6 0.3 3.9 7.3 10.0 13.6 1.3 100
KP 72.4 0.7 3.4 7.8 6.1 8.4 1.1 100
Balochistan 66.2 0.4 2.8 3.5 6.3 20.4 0.5 100
21
2 TUBERCULOSIS CONTROL: BURDEN AND EPIDEMIOLOGY
Tuberculosis (TB) is a serious, debilitating and highly contagious disease affecting millions of
people worldwide and if treated properly, is curable. Until the mid-20th century, it remained a
leading cause of death in the developed world, and still a public health problem in many
developing countries. Treating TB is challenging, even in developed countries where there is a
modern health care system and infrastructure. Despite efforts to control and treat tuberculosis,
there were an estimated 8.7 million incident cases of TB globally in 2011 (13% co-infected with
HIV). There were also 1.4 million deaths from TB (990,000 deaths among HIV-negative
individuals and 430,000 among people who were HIV-positive). These deaths included 0.5
million among women, making TB one of the top killers of women worldwide9.
Drug resistance, including multi- and extensively drug resistant TB (MDR-TB and XDR-TB),
coupled with the growing number of people co-infected with TB and HIV, make the pandemic
more threatening and more deadly.
Globally, about two billion people are infected with TB, about one out of every three people on
the planet. Mycobacterium tuberculosis (MTB), causing tuberculosis, is present in one-third of
the world's population, though not everyone shows signs of the disease.
Pakistan ranks 5thamongst the 22 HBCs and 4th among 27 MDR high burden countries in the
world10. Pakistan contributes about 65% of the tuberculosis burden in the Eastern
Mediterranean Region. According to national prevalence survey results (2010-11), the incidence
of ‘all type’ TB cases in Pakistan is 276/100,000 population or around 420,000 TB cases. The
prevalence of the disease is estimated at 348/100,000 population or approximately 620,000
cases11. In 2013, 298,476 TB cases (all ages, all forms) were notified in Pakistan.
Globally, the impact targets are “to halt and begin to reverse the incidence of TB by 2015, and
to reduce by 50%, prevalence and mortality rates by 2015, relative to the 1990 levels.” The
incidence target is part of target 6.c of the MDGs, while targets for reducing prevalence and
death rates are based on a resolution passed in the 2000 meeting of the Group of Eight (G-8)
industrialized countries in Kinawa, Japan. The outcome targets i.e. “to achieve a case detection
rate of at least 70% for new SS+ cases and to reach a treatment success rate of at least 85% for
such cases,” were first established by the World Health Assembly (WHA) in 1991. Within the
MDG framework, these indicators are defined as the proportion of cases detected and cured
under DOTS. The ultimate goal of eliminating TB, defined as the occurrence of less than 1 case
per million population per year by 2050, was stipulated by the Stop TB Partnership.
9 WHO Global Tuberculosis Report 2013
10WHO. Global Tuberculosis Control; WHO Report 2013
11National TB Prevalence Survey Report, NTP Pakistan, 2012-13
22
According to WHO Global Report 2013, the estimated incidence of DR TB was 3.5% among new
TB cases and 32% among retreatment TB cases.
The NTP has addressed the reduction of death rate i.e. the number of cases that died during the
course of treatment out of the total number of cases under treatment was 2% in 2012.
However, the case fatality rate i.e. the number of cases that died due to TB out of the total
number of incident TB cases in the country is not possible to measure in Pakistan due to the
unavailability of vital registration data in the country. The mortality rate i.e. the number of total
deaths due to TB was 34/100,000 in 2012.
Further details are given in the situation analysis section.
3 STRATEGIC PLAN “VISION 2020”
National TB Strategic Plan is a “full expression of demand” and is an advocacy tool to primarily
provide insight for the TB program, sensitize policy makers and partners and provide a basis to
generate resources. The following sections provide the background which led to the
development of the National TB Strategic Plan “Vision 2020”.
3.1 NATIONAL TB STRATEGIC PLAN: 2012-16 The last National Strategic Plan12 (2012-16) set the stage for implementation of the six key
elements of the strategy in Pakistan, which are in line with the components of the Stop TB
Strategy, i.e. a) pursuing high quality DOTS, b) addressing TB-HIV, MDR-TB and other challenges,
c) contributing to health systems strengthening, d) enabling all care providers, e) empowering
people with TB, and communities, f) enabling and promoting operational research. The
program objectives were developed in light of the ‘Global Plan to Stop TB 2011-2015’ which
included a) sustain and consolidate the achievement of 70/85 targets, and b) achieve the
targets to effectively engage all care providers, enhance program capacity to detect and
manage 80% of incident smear-positive MDR-TB cases, and reduce TB prevalence and mortality
by 50%. The total requirements for these five years were estimated at US$ 476 million. This
plan emphasized the importance of sustaining and consolidating the program achievements.
However, at the time of development of NSP 2012-16, the devolution process was in the early
phase of implementation and roles and responsibilities of provinces were not very clear. As a
result, the strategic plan was unable to capture the provincial TB control context in devolution.
Many intervention models at that time were not able to contribute substantially to increasing
12
STOP TB Strategic Plan 2012-16, National TB Control Program, MoH ,GoP

23
the TB case notification in the country. Moreover, the TB prevalence survey findings were not
available and the projection of TB cases was based on WHO estimates.
3.2 PROGRESS TOWARDS MDGs The country is progressing towards achieving the 2015 MDG-6, Target 8: i) Indicator 23 i.e. to
have halted by 2015 and begun to reverse the incidence, prevalence and deaths associated
with TB and; ii) indicator 24 i.e. proportion of TB cases detected and cured under DOTS.
Similarly the TB control program is working to achieve the 2050 - Stop TB Partnership targets
i.e. by 2015: reduce TB prevalence and death rates by 50% relative to 1990 and; by 2050:
eliminate TB as a public health problem (1 case per million population).
However, more support and efforts at the national and provincial levels for TB control activities
would help in fully meeting these targets within the given time period.
3.3 IMPLEMENTATION OF STRATEGIC PLANS AND IMPACT Two NSPs were developed before the current one. The first covered the years 2005-2010 and
the second 2011-2015. The 2011-2015 NSP was not continued beyond 2013. A great deal of
strategic interventions specified in these two formers NSPs were funded by Global Fund
through the Rounds 2, 6, 8 and 9; the Rounds 6, 8 and 9 grants were merged in a single stream
of funding in 2012 which will end up in June 2015. The first NSP focused on expanding DOTS in
order to reach the WHO global targets (detecting 70% of estimated TB cases and treating
successfully 85% of detected TB cases). The second NSP targeted the MDGs (halving TB
prevalence and mortality by 2015 compared to 1990) and focused on the implementation of
the 6 components of the Stop TB Strategy of WHO.
100% population DOTS coverage was achieved at the end of 2005 in the public health sector.
The number of notified TB cases was 20,707 in 2001, when DOTS was initiated, and 97,245 in
2004, just prior to 2005-2010 NSP implementation, and reached 298,981 in 2013. The
treatment success rate increased from 77% in 2001 to 91% in 2007 and remained, since then, at
this level. It is worthwhile to highlight that 1.9 million TB patients were successfully treated in
Pakistan between 2001and 2012.
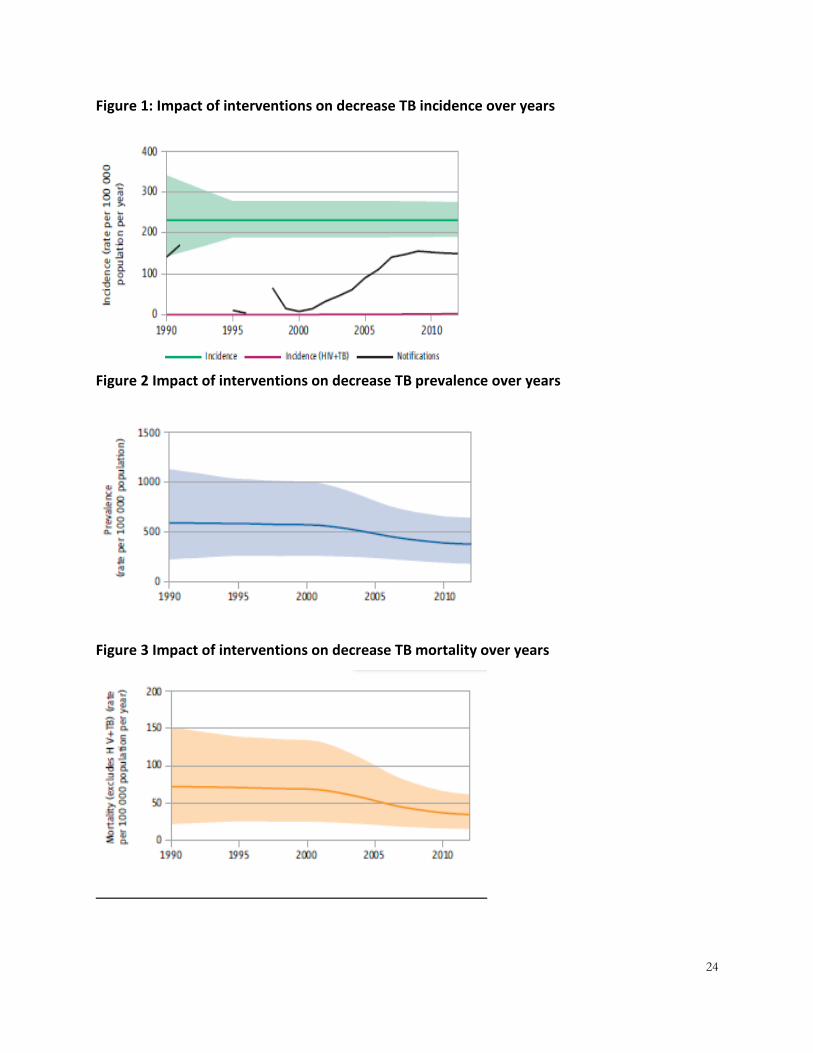
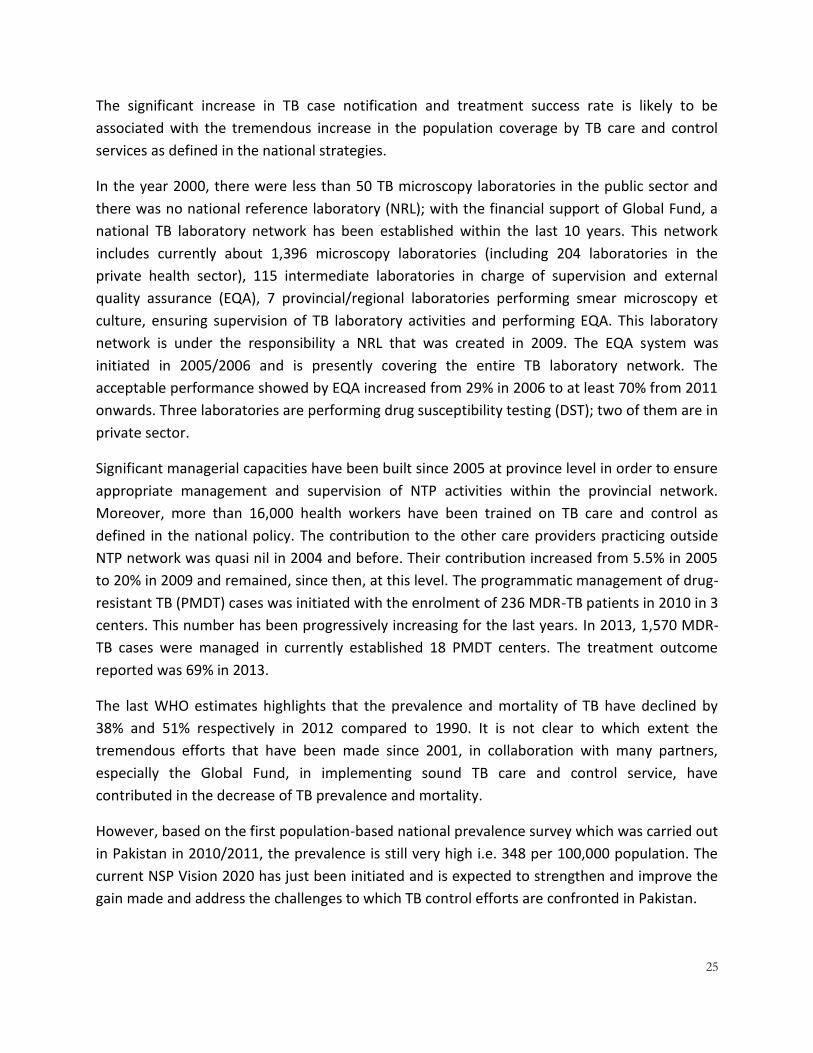
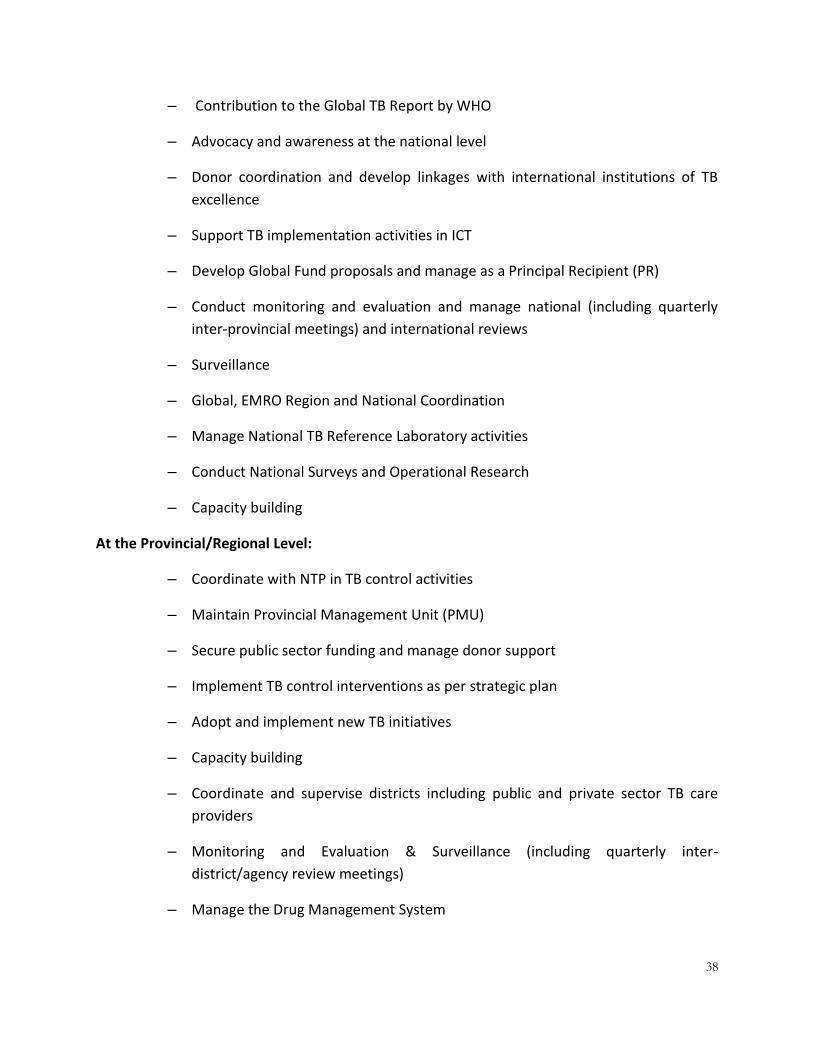
The decline in estimated incidence and prevalence due to implementation of various
interventions has been presented in the figure 1-3 below. The incidence is falling at a rate of 1-9
per year, prevalence has declined 38% since 1990 and 51% reduction in TB related mortality
since 1990.
24
Figure 1: Impact of interventions on decrease TB incidence over years
Figure 2 Impact of interventions on decrease TB prevalence over years
Figure 3 Impact of interventions on decrease TB mortality over years
25
The significant increase in TB case notification and treatment success rate is likely to be
associated with the tremendous increase in the population coverage by TB care and control
services as defined in the national strategies.
In the year 2000, there were less than 50 TB microscopy laboratories in the public sector and
there was no national reference laboratory (NRL); with the financial support of Global Fund, a
national TB laboratory network has been established within the last 10 years. This network
includes currently about 1,396 microscopy laboratories (including 204 laboratories in the
private health sector), 115 intermediate laboratories in charge of supervision and external
quality assurance (EQA), 7 provincial/regional laboratories performing smear microscopy et
culture, ensuring supervision of TB laboratory activities and performing EQA. This laboratory
network is under the responsibility a NRL that was created in 2009. The EQA system was
initiated in 2005/2006 and is presently covering the entire TB laboratory network. The
acceptable performance showed by EQA increased from 29% in 2006 to at least 70% from 2011
onwards. Three laboratories are performing drug susceptibility testing (DST); two of them are in
private sector.
Significant managerial capacities have been built since 2005 at province level in order to ensure
appropriate management and supervision of NTP activities within the provincial network.
Moreover, more than 16,000 health workers have been trained on TB care and control as
defined in the national policy. The contribution to the other care providers practicing outside
NTP network was quasi nil in 2004 and before. Their contribution increased from 5.5% in 2005
to 20% in 2009 and remained, since then, at this level. The programmatic management of drug-
resistant TB (PMDT) cases was initiated with the enrolment of 236 MDR-TB patients in 2010 in 3
centers. This number has been progressively increasing for the last years. In 2013, 1,570 MDR-
TB cases were managed in currently established 18 PMDT centers. The treatment outcome
reported was 69% in 2013.
The last WHO estimates highlights that the prevalence and mortality of TB have declined by
38% and 51% respectively in 2012 compared to 1990. It is not clear to which extent the
tremendous efforts that have been made since 2001, in collaboration with many partners,
especially the Global Fund, in implementing sound TB care and control service, have
contributed in the decrease of TB prevalence and mortality.
However, based on the first population-based national prevalence survey which was carried out
in Pakistan in 2010/2011, the prevalence is still very high i.e. 348 per 100,000 population. The
current NSP Vision 2020 has just been initiated and is expected to strengthen and improve the
gain made and address the challenges to which TB control efforts are confronted in Pakistan.

26
3.4 INTERNATIONAL TB REVIEW MISSION: NOVEMBER, 2013 In a recent international review of TB care activities in the country, several sets of
recommendations were given to the program to more comprehensively address the TB control
challenges in the country. The major set of recommendations were focused on: the importance
of developing a long-term plan for sustainable financing of the different components of the TB
program as well as; the need for a robust program, with strong NTP leadership, to support the
various TB interventions in the country, such as active case finding and contact tracing as per
WHO recommendations, re-examining the role of Xpert MTB/RIF in TB case finding, especially
for SS- and extra-pulmonary cases and; introducing the revised WHO TB definitions and
reporting framework. In addition, there were several recommendations to address major
program components such as:
laboratory, by adopting SOPs for culture & DST and infection control and strengthening
supervision
childhood TB by improving case detection in children (eg, symptomatic screening at
school entry; use of gastric aspirate) and systematic contact screening
interventions in monitoring and evaluation
PMDT interventions such as procurement of Gene Xpert machines to match the
continued roll-out of PMDT centres
consideration for introducing a short-term regimen and interventions in infection
control
TB/HIV
ACSM
PPM recognized as a major need to address for reaching additional cases
The annexure-1 gives the detailed recommendations from the international review mission in
November, 2013.
The NSP Vision 2020 has ensured that the strategic interventions proposed in the plan are in-
line with the major recommendation of this international review mission.

27
3.5 DEVELOPMENT PROCESS OF NATIONAL STRATEGIC PLAN “VISION 2020” The last national strategic plan (NSP)13which covered the years 2010-2015to control TB in
Pakistan focused on the implementation of the six components of the Stop TB Strategy as
recommended by WHO and other international agencies. In line with the Global Plan to Stop TB
2006-2015,the goals of this NSP was to contribute to reducing by 50% TB prevalence and
mortality by 2015 compared to 1990 and its objectives were to achieve 70% TB case detection
by 2015 and to maintain TB treatment success rate at 85% at least. The total budget to
implement the strategic interventions identified in this NSP was estimated at US$ 476 million.
When the implementation of the NSP 2010-2015 was initiated, the devolution process was also
at its early stage of implementation in provinces; however, the roles and responsibilities of
provinces were not very clearly defined. As a result, the new context of devolution could not
be reflected in the existing NSP for TB care and control. Moreover, the findings of the national
population-based TB prevalence (2010-11) and drug resistance surveys (2012-13) resulted in
the revision of the estimates of TB burden and, therefore, pointed out the need for revision of
targets of TB control. Meanwhile, innovations in TB diagnosis and management have occurred
after the year 2010. The process of devolution, the establishment of new estimates of TB
burden and the introduction, at global level, of new approaches for TB care and control, all, led
the NTP to take the decision to re-formulate a new national strategic plan for TB control which
covers the years 2014-2020. The development process of the new NSP was initiated in mid-
2013. It started with a consultative meeting involving the core team members of the NTP
Central Unit to approve and initiate development process and identify the focal person and
potential consultants. Then, it passed through broad-based and multi-stage consultations which
involved national, provincial, regional, community and international stakeholders, including
partners. Indeed, preliminary meetings were organized in each province and region on the need
of development of provincial/regional strategic plans for TB control. Then, a notional workshop
on the methodology to develop a strategic plan for TB control was organized, by the NTP
Central Unit, in Islamabad with in August 2013. The workshop was attended by the teams’
members of the NTP Coordination Units of the five provinces and the three regions, partners
and NGOs, involved in TB control efforts in Pakistan, and facilitated by a WHO consultant.
Following this workshop, the teams of the nine coordination unit of NTP developed their
strategic plan for TB control for their respective province and region, in collaboration with the
local partners and the relevant NGOs, with the support of the relevant staff of NTP Central Unit.
Meanwhile, a review of the NTP, involving national and international experts, was undertaken
in early November 2013. Based on the provincial and regional strategic plans that were
prepared, a draft of the 2014-2020 NSP for TB control, with its relevant components, was
developed. This draft was then revised and discussed in an international workshop on NSP
13
STOP TB Strategic Plan 2010-2015, National TB Control Program, Ministry of Health,Government of Pakistan; 2009.

28
development that was held in November 2013, in Cepina, Italy. The two professionals, who are
in charge of the development of Pakistan NSP within the NTP Central Unit, attended this
workshop. The NSP was then refined according to the revision and comments made in the
international workshop of Cepina and the findings and recommendations of the review of NTP.
It was labelled: National Strategic Plan For TB Control – Vision 2020. The budget to implement
the strategic interventions and activities specified in the NSP is estimated at US $ 876 million.
Table 5: Process of Strategic Plan Development
DATE ACTIVITY PARTICIPANTS OUTCOME
April 15,
2013
NTP initiative by
National Manager NTP
NTP Core team • Consultation with NTP core
team.
• Approval of draft inception
“VISION 2020”
April22,
2013
• Nomination of
focal person
• Engaging
consultants
National Manager NTP • Focal person nominated
• Consultants engaged
14 June 1st National
Consultative Meeting
• Consultants
• Focal person
• NTP/PTPs
• Partners
• Outline of NSP defined
• Way forward agreed
24 June 2nd National
Consultative Meeting
Technical and
Implementing Partners
• Strategic outlines formulated
• Technical Working Groups/focal
points formed
1 July -12
August
-Template formulated
for TWG
-Information gathered
-Members TWG
-National Consultant
Recommendations received from TWG
August 12,
2013
3rd National
Consultative Meeting
• Consultant
• Focal Person NSP
• Members TWG
Finalization of inputs from TECHNICAL
WORKING GROUPS
For initiation of “Zero Draft”

29
August 19-
22, 2013
4th National
Consultative Meeting
Consultants/Focal
person NSP
NTP/PTPs Technical
Partners
• Orientation of PTPs on NSP
formulation process
• “Zero draft” developed &
circulated to PTPs/Focal persons
for review and adaptation
August 23-
26, 2013
Intra NTP meetings of
focal persons with
consultants
• Consultants
• NTP focal
persons
- Goals and objectives defined
- Gap Analysis done
September-
October,
2013
1st Round - Provincial
/Regional Consultative
Meetings
Balochistan (5-7 Sep)
Punjab (10-11 Sep)
KPK (23-24 Sep)
Sindh (25-26 Sep)
ICT (27 Sep)
AJK (28 Sep)
GB (30 Sep)
FATA (2 Oct)
Focal Person NTP/
Consultant
PTP Manager, Deputy
Manager, PRL team,
NPOs
-Provincial /Regional “Zero Draft” of Core
Plan(Objectives, Background, Situation,
SWOT, Gap analysis, Strategic
interventions, Activities)
October 3-
5, 2013
Refinement of
Provincial Core
Strategic Plans
-PTPs
-Focal person NSP
-Consultants
-Completed “First Draft” of Provincial
Core Strategic Plans (05) and Regions
(03)
October 7-
9, 2013
5th National
Consultative Meeting
(Costing , M& E and
Operational plan and
TA Plan)
• Provincial
Technical and
Financial expert
• National Focal
Persons and
financial expert
• Consultants
• Provincial Core Strategic Plan
• Costing
• M&E Plan
• Operational Plan
• Technical Assistance Plan

30
October 10-
20, 2013
Refinement of
National Strategic Plan
• National
Technical group
• Focal person NSP
• Consultants
Completion of “First Draft” of National
Strategic Plan
November
17-27, 2013
Global workshop on
“Development of
National Strategic
Plan)” at Cepina (Italy)
Consultants:
NTP Focal Person:
Refinement of draft core plan
Development of Budget Plan
based on WHO Budgeting &
Planning Template
December
2013
2nd Round
Provincial /Regional
Consultative Meetings
Balochistan, Punjab,
KPK, Sindh, FATA, GB,
AJK, ICT
PTP Manager, Deputy
Manager, PRL team,
NPOs
-Provincial /Regional “Preliminary Draft”
of Strategic Plan including;
1 – Core Plan
2 – Epidemiological Projections
3 – Operational Plan
4 – Budget Plan
January 31,
2014
Refinement of NSP NTP/Consultant NSP Preliminary draft and circulated to
NTP focal persons for review and
refinement
March 12,
2014
6th National
Consultative Meeting
for finalization of
Provincial/National
Strategic Plans
NTP/PTPs Technical
Partners
Preparation of Final Draft
Submission to NTP for approval from
Ministry of NHSR&C

31
1st National Consultative Meeting
June, 2013 - Islamabad

32
2nd National Consultative Meeting
July, 2013 - Islamabad

33
3rd National Consultative Meeting
September, 2013 - Islamabad

34
Global Consultative Workshop
November, 2013 – Italy

35
4 NATIONAL TB CONTROL PROGRAM PAKISTAN
4.1 EVOLUTIONARY PERSPECTIVE WHO declared TB a global emergency in year 1993 which was endorsed by the Government of
Pakistan. The TB Control Program (TCP) was revived in 2001 and TB was declared as National
emergency. The NTP Pakistan embarked upon the implementation of DOTS in year 2000/2001
and achieved 100% public sector DOTS coverage in country by year 2005. High government
commitment coupled with strong technical leadership in the program resulted in a clear vision,
which was translated into a multi-year strategic plan (2001 – 2005) to achieve 100% DOTS
coverage by the year 2005. The strategic plan was revised in 2005 for the period from 2005 to
2010. TB Control Program recently revised a strategic plan for 2012 – 2016.
A well-functioning DOTS Program is the key to success to TB control in a country. The
Government has accorded high priority for the control of communicable diseases (including
tuberculosis) as embodied in its National Health Policy (existing as well as new i.e. 2009 - draft).
4.2 STRUCTURE & FUNCTION National TB Control program (NTP) is fighting against Tuberculosis in the country with the
support of Provincial TB Control Programs (PTPs). TB control program is a horizontal program
integrated into Primary Health Care (PHC). The NTP is responsible for overall coordination of
the TB Control Program in the country. The NTP is not directly involved in TB care delivery,
which is the responsibility of the provincial/regional/district health authorities. The main
responsibilities of the NTP includes; policy formulation and strategic planning, technical support
to the provinces, supervision, monitoring and evaluation, coordination and communication
with partners, and research and development.
The Provincial Tuberculosis Control Programs (PTPs), under their respective departments of
health, are responsible for coordinating the planning, implementing, managing and financing of
the tuberculosis control activities in their respective provinces/regions. The PTPs are involved in
supporting the district health services, teaching hospitals, and other partners for effective
implementation of DOTS in their respective constituencies. The main responsibilities of the PTP
includes; participation in strategic, program and operational planning, technical and material
support to the districts and partners, supervision, monitoring and evaluation support to the
districts and coordination and communication with partners.
In the devolution context, the district authorities are primarily responsible for advocating,
planning, financing, implementing, and monitoring TB care services in their respective districts.
The delivery and management of TB care has been integrated within district healthcare services
so that continuing care can be provided close to the patient's home.

36
4.2.1 NTP arrangements for coordination of TB control activities in the country
NTP has the stewardship role in TB control efforts in the country. The figure below reflects the
organization of TB control activities in the country.
Figure 4: Organization of TB control program Pakistan
The NTP has various categories of management, technical and administrative staff working at
the national and provincial levels.
Table 6: NTP Human Resource and funding support
Human Resource (from public sector) Human Resource (from GF and USAID)
• Sociologist (2)
• Filed officer (0)
• Deputy Head Lab (1)
• C. Operator (1)
• Lab Technicians (7)
• Microscopist (2)
• PTO (4)
• NPO (31)
• Microbiologist (5)
• Microscopist (1)
• Lab Technicians (06)
• Logistic officer (3)
PTP Manager PTP Medical Officers GF Staff
Federal Level NTP (MoNHSR&C)
GF Grant Management Resource
mobilization Technical support to
PTP
Public Sector BMU/TC
Care Provider DOTS facilitator Microscopist
GF grant implementation Coordination with SRs Logistics support to Dist
Recording and reporting
Private Sector GP Clinics/Labs
District Level
Provincial Level PTP (MoH)
EDO/DHO DTC DLS
National Manager PIU
Program Implementation
Recording and reporting
Monitoring
TB Case Management
C O M M U N I T Y
ORGANIZTION - TB CONTROL PROGRAM

37
• Lab Attendants (2)
• Office Assistant (1)
• Drivers (80)
• Field Officer 1 (vacant)
• UDC (1)
• NaibQasid (1)
• Sweepers (1)
• Stock officer (3)
• ACSM coordinator (03)
• Data Management Officers (1)
• IT Assistant (1)
• Office Assistants (2)
• Resource Center Person (1)
• HR Officer (1)
• SLS (11)
• MDR Staff (11)
• Drivers (4)
Total: 100 Total: 88
The table above shows that more than 95% of the human resources provided through public
sector resources is support staff, whereas the situation is entirely opposite as more than 95% of
the human resources provided through donor support is technical staff which has also high cost
implications as far as sustainability is concerned. Almost 50% of the donor-supported human
resources provided to the NTP are based in provinces and regions to supports provincial and
regional TB control programs. The annexure-3 provides, in detail, the functions of these staff.
About 95% of the technical staff is supported through donor funding, mainly from Global Fund
grants.
4.3 LEVELS & RESPONSIBILITY The different level of responsibilities are summarized below:
At the NTP Level:
– Secure public and donor sector funding to support TB control activities
– Develop TB control national policies and TB standards for TB management
including diagnostic algorithms and treatment protocols, patient education
material, recording and reporting forms, etc
– Adapt and pilot innovative approaches to TB diagnosis and ensuring patient
compliance
– Procure/ Arrange new diagnostic equipment (such as GeneXpert, LED
microscope) and supplies and FLDs and SLDs to address gaps in the provinces
– Manage the national data base and report to the Government of Pakistan, UN
agencies and Donor agencies
38
– Contribution to the Global TB Report by WHO
– Advocacy and awareness at the national level
– Donor coordination and develop linkages with international institutions of TB
excellence
– Support TB implementation activities in ICT
– Develop Global Fund proposals and manage as a Principal Recipient (PR)
– Conduct monitoring and evaluation and manage national (including quarterly
inter-provincial meetings) and international reviews
– Surveillance
– Global, EMRO Region and National Coordination
– Manage National TB Reference Laboratory activities
– Conduct National Surveys and Operational Research
– Capacity building
At the Provincial/Regional Level:
– Coordinate with NTP in TB control activities
– Maintain Provincial Management Unit (PMU)
– Secure public sector funding and manage donor support
– Implement TB control interventions as per strategic plan
– Adopt and implement new TB initiatives
– Capacity building
– Coordinate and supervise districts including public and private sector TB care
providers
– Monitoring and Evaluation & Surveillance (including quarterly inter-
district/agency review meetings)
– Manage the Drug Management System

39
– Manage Provincial/Regional Reference Laboratory (PRL/RRL) activities
At the District/Agency Level:
– Coordinate with PTP/RTP in TB control activities
– Service Delivery (Diagnose, Manage, Treat and Report TB Patients) in TB care
facilities in public and private sector
– Train Critical Mass of Human Resources
– Monitor and supervise public (including other public health sector) and private
sectors ( including quarterly intra-district/agency meetings)
– Receive, Store , and Consume Logistics (ATT ,Lab Reagents, Equipment)
– Maintain Quality Lab Services and implement EQA
– Prepare and submit Quarterly TB Reports
– Coordinate with Sub Recipients
4.4 TB CONTROL IN POST DEVOLUTION CONTEXT Since the inception of the TB control program, its activities have been integrated in Primary
Health Care (PHC) in the country. The NTP, in consultation with the project management team,
has developed the following strategy to contribute to the devolution process and to devolve
future Global Fund and other grants, to the extent which is acceptable to both donors and
provinces. This implies:
- Capacity building of the provinces to implement new interventions, including donor
grants, and to become eligible as Sub-Recipients in subsequent grants
- Active support to provinces in implementation including addressing uniform policies
and standards, supplies and logistics gaps, capacity gaps, M&E, research, etc.
- Establishment of provincial grant management units and devolution of certain
activities and funds related to these activities for institutional strengthening at the
provincial level
- Capacity building/ trainings
According to the operational details laid out under the devolution process, international/
donor funded projects are affiliated with the Economic Affair Division. It disburses the funds to

40
the concerned departments who are in turn responsible for the management of the funds and
implementation of the funded activities.
In contrary to other donor funding, Global Fund Grants are performance-based and are
disbursed in the countries only through Principal Recipients. Later, keeping in view the
requirements of Global Fund grants and in order to comply with the procedures laid out by the
CCM, the three public sector PRs (National TB Control Program, National AIDs Control program
and Directorate of Malaria) were affiliated and placed under administrative control of the
newly established Ministry of National Health Services, Regulations & Coordination (NHS,R&C).
At this time, the NTP is implementing three grants with the support of Global Fund i.e. Round 6,
8 and 9 grants, consolidated as per policy of the Global Fund in Single Stream Funding (SSF) to
facilitate the process of grant implementation and reporting. The NTP has signed a contract to
receive these grants as Principal Recipient. The Project Management Unit, established with
grant support and under the supervision of the National Manager, TB Control has successfully
been implementing these grants.
The NTP presence is necessary at the central levels for maintaining national stewardship and
fulfilling global commitment towards the MDGs. The recent review of NTP roles and
achievements has also highlighted the need to address the challenges due to on-going
decentralization of health programs in the country14. The NTP will act as a collaborating body at
the central level for development of uniform policies and strategies, which is also a
requirement of financial partners; for example the GFATM. The NTP at the central level will
facilitate donor liaison at the national and international levels. Disease surveillance is another
important area at the national level for impact evaluation, tracking toward policy development.
Currently the NTP is maintaining electronic surveillance for reporting to the MoH, WHO and
other donors and partners.
14
Third-party evaluation of NTP, TRF 2011
41
SECTION A2–
A2/1: SITUATION ANALYSIS
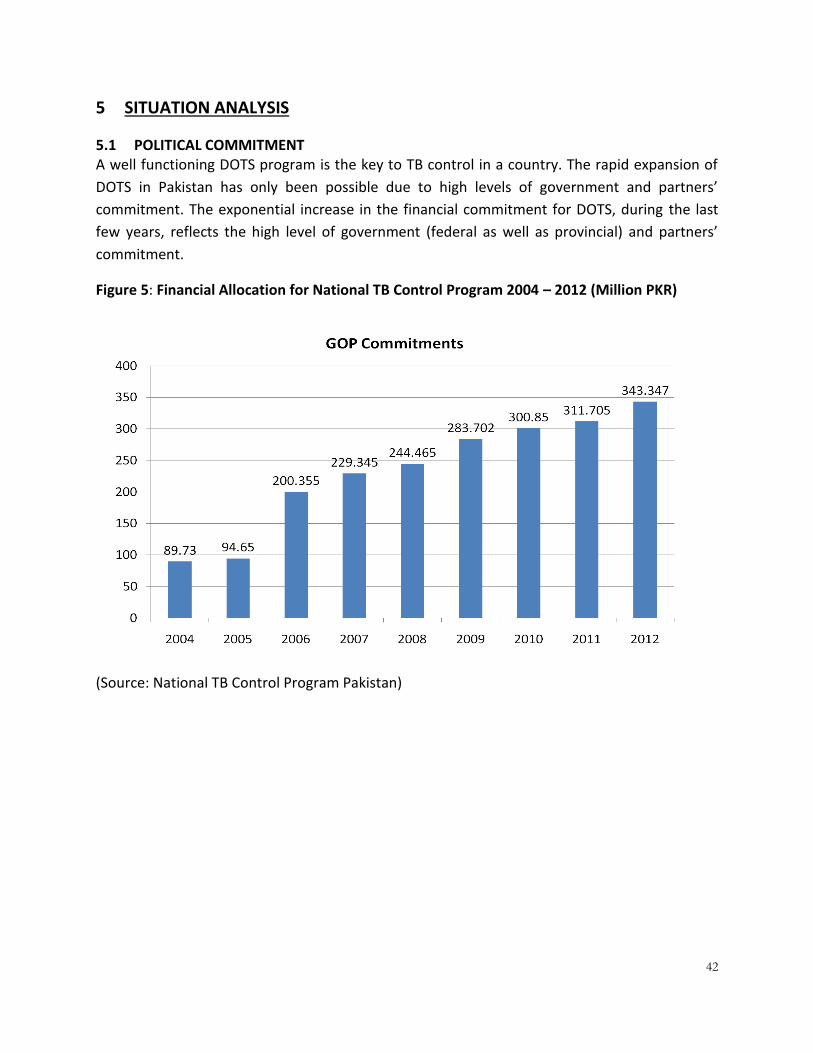
42
5 SITUATION ANALYSIS
5.1 POLITICAL COMMITMENT A well functioning DOTS program is the key to TB control in a country. The rapid expansion of
DOTS in Pakistan has only been possible due to high levels of government and partners’
commitment. The exponential increase in the financial commitment for DOTS, during the last
few years, reflects the high level of government (federal as well as provincial) and partners’
commitment.
Figure 5: Financial Allocation for National TB Control Program 2004 – 2012 (Million PKR)
(Source: National TB Control Program Pakistan)
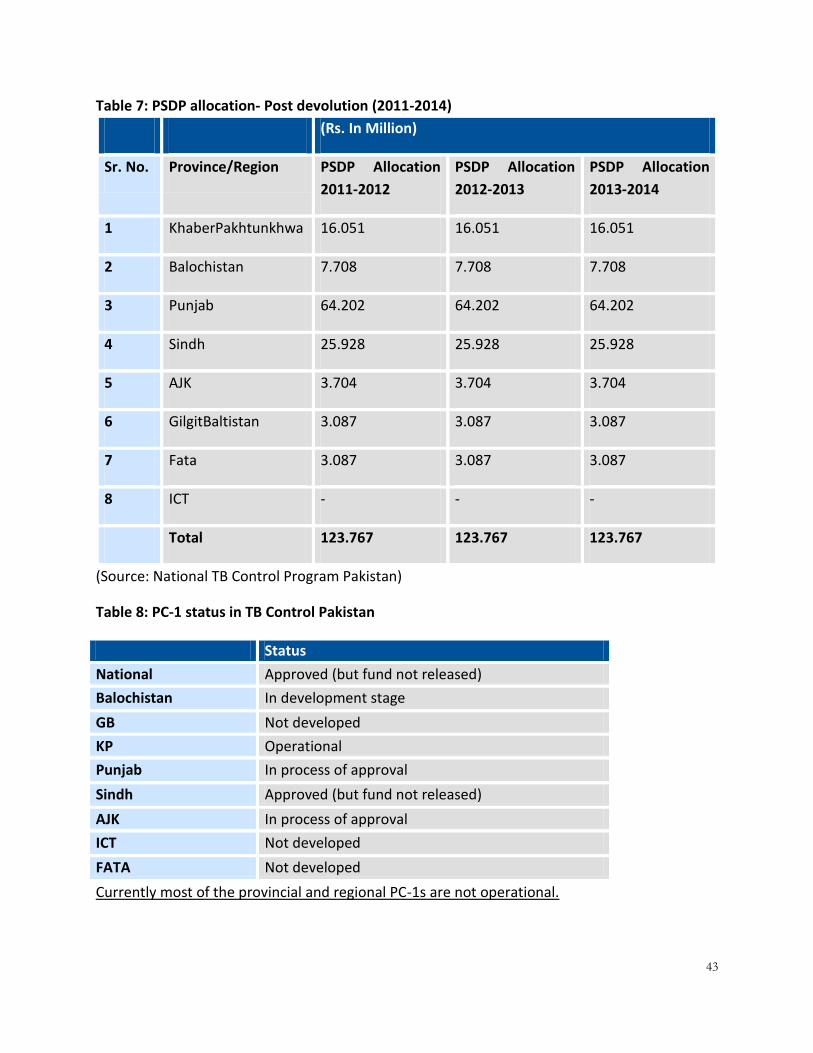
43
Table 7: PSDP allocation- Post devolution (2011-2014)
(Rs. In Million)
Sr. No. Province/Region PSDP Allocation
2011-2012
PSDP Allocation
2012-2013
PSDP Allocation
2013-2014
1 KhaberPakhtunkhwa 16.051 16.051 16.051
2 Balochistan 7.708 7.708 7.708
3 Punjab 64.202 64.202 64.202
4 Sindh 25.928 25.928 25.928
5 AJK 3.704 3.704 3.704
6 GilgitBaltistan 3.087 3.087 3.087
7 Fata 3.087 3.087 3.087
8 ICT - - -
Total 123.767 123.767 123.767
(Source: National TB Control Program Pakistan)
Table 8: PC-1 status in TB Control Pakistan
Status
National Approved (but fund not released)
Balochistan In development stage
GB Not developed
KP Operational
Punjab In process of approval
Sindh Approved (but fund not released)
AJK In process of approval
ICT Not developed
FATA Not developed
Currently most of the provincial and regional PC-1s are not operational.

44
Figure 6: Contribution to TB control activities by funding source5: 2012-13
In recent years the confidence and commitment of the partners/donors has been increasing.
This is mainly because of transparent decision-making at the National level with involvement of
all stakeholders, demonstrated success endorsed by national and international missions, and
continued encouragement/ facilitation of all program partners. This high dependence on donor
inputs (85%) is a caution to NTP/PTPs to work in parallel and access an equitable contribution
from the public sector funding.
5.2 TB CASE NOTIFICATION
5.2.1 TB burden analysis
Steady progress can be witnessed during the last decade to improve the case detection and
treatment success rate by emphasizing quality assurance of smear microscopy, drug
management, community mobilization, involving tertiary care hospitals, NGOs, and inter-
sectoral organizations and, above all, involving private sector for service delivery. Between
2001 and 2012, 2.14 Million TB patients have been diagnosed and treated free of cost under
the National TB Control Program. With reference to expansion, 141 districts were detecting TB
cases from five provinces [Balochistan, GilgitBaltistan (GB), Khyber Pakhtunkhwa, Punjab and
Sindh] and three regions (ICT, FATA and AJ&K) in the country with a network of 1,230 public
sector Basic Management Units (BMUs).

45
Table 9:Year-wise notified TB cases and NSS+ Pakistan
Year Estimated TB Case
Burden in Pakistan
Case detection NSS+ Re-treatment
2001 259,886 20,707 6,703 702 (3%)
2002 263,505 49,186 15,446 2,952 (4%)
2003 269,033 75,528 21,033 4,449 (6%)
2004 274,184 97,245 31,557 4,890 (5%)
2005 279,667 144,771 48,220 5,425 (4%)
2006 285,260 179,780 65,711 5,565 (3%)
2007 290,792 234,100 88,747 7,738(3%)
2008 296,779 248,678 100,103 7,982(3%)
2009 302,767 267,451 101,887 9,200(3%)
2010 317,607 269,290 104,263 10,805 (4%)
2011 413,450 270,422 105,733 11,417 (4%)
2012 416,000 285,410 110,545 11,717 (4%)
The table above shows that the case detection has increased in initial years, as has the number
of NSS+ and re-treatment cases. Since 2008, case reporting has remained stagnant (2-3%
annual increase seen in the country).

46
Table 10: Estimates of TB burden 201215
Impact Rate (per 100000 population)
Mortality 34 (15-61)
Prevalence 348 (287-409)
Incidence 276 (158-424)
Figure 7: Provincial TB Case notification and population proportion
Case notification (%) – All Provinces and regions – 2012
Population (%) – All Provinces and regions – 2012
The figure above shows that the most populous province i.e. Punjab is providing the greatest
proportion of notified cases (62.2%) in the country, where as Sindh and KPK contribute 19.4%
and 11.9% of the total notified cases respectively. Smaller provinces and regions have a joint
contribution of 6.5%.
15
National TB Prevalence Survey Report, NTP Pakistan , 2012-13
AJK 1.8%
B'TAN 2.4%
FATA 1.3%
GB 0.5%
KPK 11.9%
PJB 62.2%
SINDH 19.4%
ICT 0.5%
AJK B'TAN FATA GB KPK PJB SINDH ICT
PJB 54%
Sindh 22%
B'TAN5%
KPK 13%
GB 0.70%
AJK 2%
FATA 2%
ICT 0.60%
PJB Sindh B'TAN KPK GB AJK FATA ICT

47
Figure 8: Case notification by age (%) – National – 2012
(Source: National TB Control Program)
The majority of the cases reported are in the age group 15-24 years. However, also around 10%
of the total notified cases are being reported in adults above 65 years.
5.2.2 Re-treatment cases
The table below shows that, at the national level in 2012, the overall number of re-treatment
cases reported was 15,688 (4%) i.e. the number of re-treatment cases, including other re-
treatment SS+ cases, was 11,717 and the number of other re-treatment SS- and EP cases was
3,971. The low proportion of re-treatment cases shows that program implementation is not at
the desired level. The highest proportion (7%) of re-treatment cases has been reported from
the province of Sindh, followed by Punjab, KP and AJK (each 3%).
According to WHO (2013 report) it is estimated that 3.5% and 32% of the new and re-treatment
cases, respectively, will be potential DR-TB cases in Pakistan. According the preliminary results
of the DRS, completed in 2013, the prevalence of drug resistance in new and retreatment cases
is 4.3% and 19.4% respectively.
4% 5% 4% 4% 4% 4% 4% 4% 4% 5%
4% 4% 4%
28% 28% 26% 26%
24% 24% 24% 23% 24% 25% 25% 25% 26%
5% 6% 6%
8% 8% 8% 9% 9% 9% 10% 9% 10% 10%
0%
5%
10%
15%
20%
25%
30%
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 Q1-13
0-14 15-24 65 OR >

48
Table 11: Proportion of re-treatment cases reported
(Province/Region/National 2001- 2012)
20
01
20
02
20
03
20
04
20
05
20
06
20
07
20
08
20
09
20
10
20
11
20
12
AJK 3% 3% 5% 4% 3% 4% 4% 3% 3% 4% 2% 3%
B'tan 1% 2% 2% 2% 1% 2% 2% 2% 2% 3% 3% 2%
FATA 1% 4% 4% 4% 2% 2% 2% 3% 5% 6% 2% 2%
GB 1% 0% 0% 0% 0% 0% 0% 1% 0% 1% 1% 1%
KPK 4% 4% 5% 5% 4% 3% 3% 4% 3% 3% 3% 3%
PJB 3% 3% 6% 3% 3% 2% 3% 3% 3% 3% 3% 3%
SINDH 4% 8% 10% 9% 6% 6% 5% 5% 6% 8% 7% 7%
ICT 1% 3% 3%
PAKISTA
N
3% 4% 6% 5% 4% 3% 3% 3% 3% 4% 3% 4%
5.2.3 TB care facilities in Pakistan
The table below reflects the current status of TB care facilities in the public and private sectors.
This reflects that public sector facilities (TCH/DHQ/THQ and RHC) are almost 100% covered for
TB case management as per NTP protocols and guidelines. A large number of BHUs in the
country (up to 50%) are managed by NGOs (PRSP/PPHI) and, among them, a significant number
of BHUs have the potential to be strengthened for TB diagnostic services.
Similarly, many health facilities under the public sector (Army, Social Security, Railway, Mining
department, etc.) are currently not fully involved in TB case management as per the NTP
protocols and guidelines but have the potential to be involved as BMUs.
As far as the private sector is concerned a large number of GPs and laboratories in the country
are not in partnership with the NTP. Similarly many NGO run clinics and private hospitals (PATA,
AKF, MALC, etc) are not in full partnership with the NTP, while others are not partnering at all.
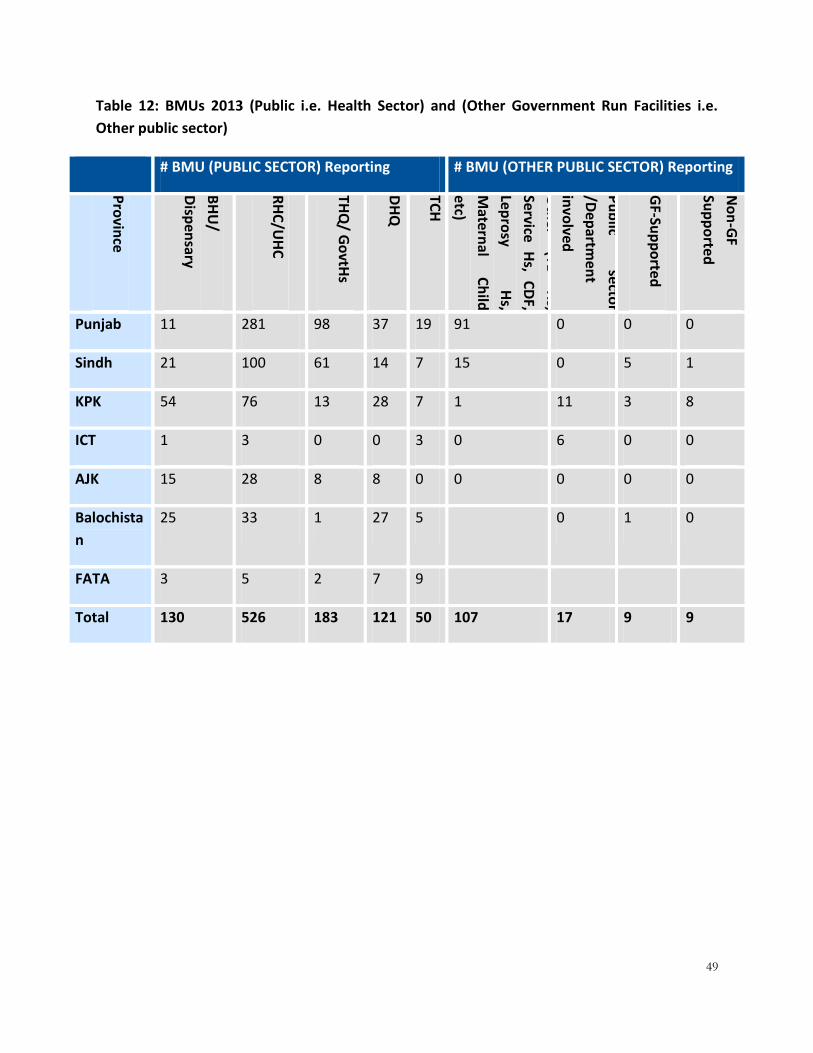
49
Table 12: BMUs 2013 (Public i.e. Health Sector) and (Other Government Run Facilities i.e.
Other public sector)
# BMU (PUBLIC SECTOR) Reporting # BMU (OTHER PUBLIC SECTOR) Reporting
Pro
vince
BH
U/
Disp
ensary
RH
C/U
HC
THQ
/ Go
vtHs
DH
Q
TCH
Oth
er (TB
H
s,
Service H
s, C
DF,
Lepro
sy H
s,
Mate
rnal
Ch
ild
etc)
Pu
blic
secto
r
/Dep
artmen
t
invo
lved
GF-Su
pp
orte
d
No
n-G
F
Sup
po
rted
Punjab 11 281 98 37 19 91 0 0 0
Sindh 21 100 61 14 7 15 0 5 1
KPK 54 76 13 28 7 1 11 3 8
ICT 1 3 0 0 3 0 6 0 0
AJK 15 28 8 8 0 0 0 0 0
Balochista
n
25 33 1 27 5 0 1 0
FATA 3 5 2 7 9
Total 130 526 183 121 50 107 17 9 9

50
Table 13: BMUs 2013 by source of funding (Private) and (GP clinics)
PRIVATE
GF SUPPORTED GP CLINICS/OTHER
PUBLIC SECTOR HOSPITALS
Non-GF SUPPORTED
GP CLINICS
Pro
vince
# o
f N
GO
s
invo
lved
# R
epo
rting
BM
U in
review
qu
arter
Imp
lemen
ting
partn
er (SR)
# R
epo
rting
in
review
qu
arter
PP
M lab
s
Oth
er P
ub
lic
Sector
Ho
spitals
Imp
lemen
ting
Partn
ers (SR)
# R
epo
rting in
review
qu
arter
Punjab 0 0 3 1,130 125 10 0 0
Sindh 0 41 4 669 57 5 0 2
KPK 28 28 3 213 37 7 4 48
ICT 0 1 1 22 3 0 0 0
AJK 0 0 1 52 9 0 0 0
Balochistan 0 2 3 124 13 2
GB 1 34 1
FATA
Total 28 72 6* 2,24 245 24 4 50
*The total number of SR is 6 (including MC-PIU). Some SRs are working in more than one
province/region.

51
Table 14: Districts with urban/sub-urban population ≥ one million
Province/Regions
Districts with populous
cities with overcrowded
suburban areas
Population
TB cases (all
age, all forms),
2013
Balochistan Quetta 963,104 2,134
GB -
KP Peshawar 2,555,389 5,869
Punjab
Lahore 8,383,436 7,397
Faisalabad 6,448,816 3,124
Multan 3,798,438 6,336
Gujranwala 4,203,123 11,932
Rawalpindi 4,109,112 13,490
Sindh Karachi 13,230,747 18,029
Hyderabad 1,971,189 2,623
AJK -
ICT Islamabad 1,054,430 1,597
FATA - 46.7 million 72,531
TOTAL
It is estimated based on the incidence figure that there are about 130,000 TB cases which needs
to be detected and treated. In 2013, 72531 (56%) case were reported from these district/cities.
There is a huge potential in these mega cities to capture additional TB cases through active case
finding approaches.

52
5.2.4 TB Control service delivery in districts
The delivery and management of TB care has been integrated within district healthcare services
so that continuing care can be provided close to the patient's home. TB care has become an
integral part of healthcare at all levels starting from district hospitals to primary healthcare
facilities to community health workers. This integration has made it possible to plan and carry
out TB control in a district without the addition of a TB-specific care delivery staff. In the
context of devolution, the district health authorities i.e. Executive District Officer Health (EDO),
District Health Officer (DHO), Medical Superintendent of District Head Quarter Hospital, District
TB Coordinator (nominated person), In-charge doctors, DOTS facilitators and Laboratory
technician of Rural Health Centers, Basic Health Units, and the District Laboratory Supervisor
are the key district personnel that are involved in TB control activities at the district level. The
district EDO-H/DHO and the DTC are primarily responsible for advocating, planning, financing,
implementing, and monitoring TB care services in their respective districts.
The district and sub-district hospitals, the rural health centers and selected BHUs (where
needed) in public health /other health sector works as BMUs. A BMU has a laboratory with
laboratory staff and a doctor/qualified medical staff who is trained to diagnose and initiate
treatment. The BMU is also a facility where patients return for re-examination and confirmation
of cure. The BMU maintains record on standard formats and provides periodic reports to the
district coordinator including report on treatment outcome.
Role of BMU
Screen people with respiratory symptoms (suspected as TB patient) by sputum smear
examination
Diagnose and prescribe drugs to confirmed TB patients
Register TB patients, and identify suitable treatment center, and refer the patient
Do follow up smear examinations
Prepare quarterly reports on case finding, smear conversion and treatment outcome
Maintain patients record, and stock books for drugs and materials
Provide patient and family education, both pre-treatment and during treatment
Act as a treatment center for those living nearby
a) The primary healthcare facilities such as basic health units and dispensaries work as
treatment centers. The treatment center is the nearest or most convenient health
53
facility for the patient to continue the treatment. The health facility supplies anti-TB
drugs and ensures that the "direct observation" is carried out through appropriately
selected supporter. Some patients who live close to a diagnostic center may prefer to
avail all the TB care including periodic collection of drugs, supervised drug
administration etc. at the BMU. If this is the case, then the BMU also becomes a
treatment center.
Treatment Centers: Role
Refer people with respiratory symptoms (suspected as TB patient) to the BMU
Provide or arrange community-based observation of treatment
Supply anti-TB drugs to the patients
Maintain patients record
Refer patients with drug reaction to district hospital
Refer patients to BMU for follow up examination
Identify and arrange retrieval of patients showing delay/interruption in drug
intake/collection.
Maintain the stock register for drugs and materials
Provide patient and family education, both pre-treatment and during treatment
The tertiary/specialized hospitals, district and sub-district hospitals and TB clinics offer TB
services as diagnostic centers. The district, teaching and specialized hospitals also provide care
to difficult to diagnose and manage adult TB cases as well as childhood TB cases. Selected
teaching, specialized and district hospitals also offer diagnosis and case management of MDR-
TB cases (with capacity enhancement and support from the program). The medical schools and
post-graduate training institutions would continue contributing in the under-graduate and post-
graduate training of doctors and chest specialists as well as TB related research.
TB care diagnostic and treatment facilities in private sector settings includes a variety of
implementing models (see relevant section on PPM).

54
5.2.5 Diagnostic algorithms
The diagnostic algorithm is as follows:
Figure 9: Diagnostic procedure for suspected pulmonary TB
(Source: Guidelines for Diagnosis and Management of Tuberculosis in Pakistan, NTP 2012)
*New TB cases, started on FLD, who report smear positive at the end of month 2 should be
referred for Xpert testing.
**Retreatment/Other Positive cases on FLDs, reported smear positive at the end of month 3
should be referred for Xpert testing.
TB suspect
( cough >2wks)
2-Sputum smear for AFB
1 or >1 AFB smear +ve
NEW TB Case
Register start FLD*
Retreatment + Other Case
Xpert-MTB/RIF assay
MTB+ RR+
Refer TO MDR MU
MTB+RR-ve
Regsiter start FLD(re-treatment
regimen)**
Two AFB Sm -ve
Broad spectrum antibiotics (clinician
decision)
Chest X-ray
Consistent with TB
Retreatment case +OTHER neg**
Xpert MTB/RIF
MTB+ RR+
Refere to MDR MU
MTB+RR-ve
Register start FLS(re-tr regimen)
MTB-ve
Culture /clinical evaluation
NEW SM -ve TB Case
Register Start FLD

55
Currently the NTP policy is to diagnose and treat TB through the passive case finding approach.
Passive case finding focuses on:
- TB suspects with relevant symptoms who present themselves at health facilities
- A patient who for any reason has had a radiological examination of the chest showing an
abnormality consistent with TB.
There are several challenges which have led to stagnant case notification over the past several
years. The national TB prevalence survey showed that patient diagnostic rate of 41.5% and case
detection rate of 45.4% suggest that high proportion of cases present in the community is being
missed. The limitation of screening algorithm (cough for more than 2 weeks is the TB suspect
identification) whereas research has shown that only 30% patients present with a cough for
more than 2 weeks or hemoptysis; TB is concentrated more and more among high risk groups;
active-case finding carried out on limited scale, and passive v/s active creates provider pushed
to create demand are the factors which requires special focus.
Experience suggests that passive case finding is likely to delay diagnosis and treatment of TB
and increase M. tuberculosis transmission. Therefore, strategies like active and systematic
screening need to be considered.
5.3 TB TREATMENT AND CASE HOLDING Treatment
TB patients must be treated with the anti-tuberculosis drug regimens recommended by NTP
Pakistan. It is the responsibility of the medical officer at the BMU to prescribe the standardized
drug regimen according to the category of a diagnosed patient. The NTP recommended drug
regimens are very effective and can successfully treat almost all cases of tuberculosis if used in
the right dosage and for the right duration. Currently the treatment period for new TB cases
lasts 6 months. The five essential anti-TB drugs used in the NTP Pakistan, with their mode of
action and dosage (in mg per kg body weight), are given in the table below.
Table 15: Characteristics of essential Anti-TB drugs
Essential anti-TB drugs (Abbreviation)
Mode of action Dosage
(mg/ kg) Common drug preparations
Isoniazid (H) Bactericidal 5 (4-6) Tab: 100mg
Rifampicin (R)* Bactericidal 10 (8-12) Tab: 150, 300, 450mg
Pyrazinamide (Z) Bactericidal 25 (20-30) Tab: 500mg

56
Streptomycin (S) Bactericidal 15 (12-18) Amp: 1000mg
Ethambutol (E) Bacteriostatic 15 (15-20) Tab: 400mg
The TB Control Program strongly recommends the use of FDC drugs for the treatment of all
types of TB cases. The recommended formulations currently used are shown in the table below:
Table 16: Type of FDCs recommended by NTP
Drug Combination Strength for daily use
Isoniazid+ Rifampicin (HR) 100+150mg
Isoniazid+ Rifampicin+ Pyrazinamide+ Ethambutol (HRZE) 75+150+400+275mg
The table below summarizes the drugs and the duration of intensive and continuation phase in
two categories of TB patients.
Table 17: FLDs prescription schedule
Category Intensive Phase Continuation Phase
Duration in month Drugs Duration in month Drugs
CAT-I 2 HRZE 4 RH
CAT-II 3 HRZE +S* 5 RHE
*Streptomycin is used only for two months during intensive phase of Cat-II
Case holding
Directly Observed Treatment (DOT) ensures that TB drugs are taken and prevents the
development of resistance to Rifampicin. The risk of drug resistance is higher during the early
stages of anti-TB drug treatment when there are more TB bacilli. According to the WHO, there
can be flexibility and innovation in observing treatment, if the treatment supporter is
accountable to the health services and accessible to the patient.
Based on National and International experiences, the NTP Pakistan has recommended the
following types of treatment supporters for TB patients.
o Health facility based worker i.e. health staff member at the selected treatment
center
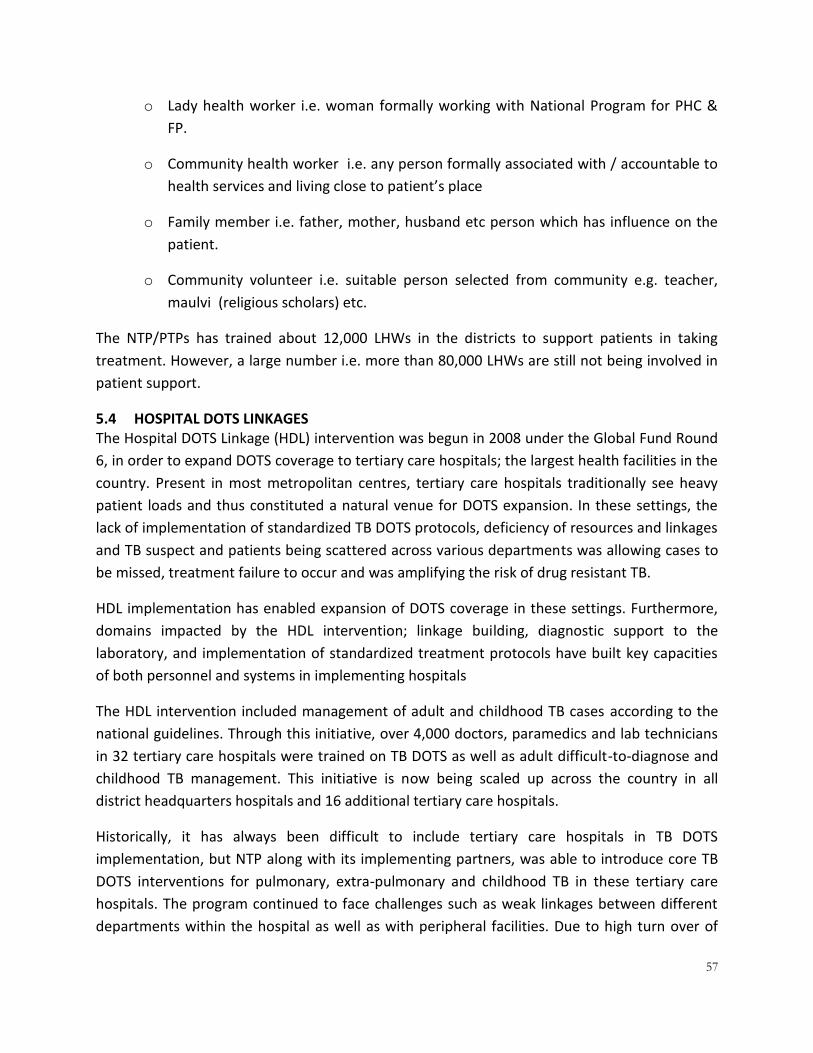
57
o Lady health worker i.e. woman formally working with National Program for PHC &
FP.
o Community health worker i.e. any person formally associated with / accountable to
health services and living close to patient’s place
o Family member i.e. father, mother, husband etc person which has influence on the
patient.
o Community volunteer i.e. suitable person selected from community e.g. teacher,
maulvi (religious scholars) etc.
The NTP/PTPs has trained about 12,000 LHWs in the districts to support patients in taking
treatment. However, a large number i.e. more than 80,000 LHWs are still not being involved in
patient support.
5.4 HOSPITAL DOTS LINKAGES The Hospital DOTS Linkage (HDL) intervention was begun in 2008 under the Global Fund Round
6, in order to expand DOTS coverage to tertiary care hospitals; the largest health facilities in the
country. Present in most metropolitan centres, tertiary care hospitals traditionally see heavy
patient loads and thus constituted a natural venue for DOTS expansion. In these settings, the
lack of implementation of standardized TB DOTS protocols, deficiency of resources and linkages
and TB suspect and patients being scattered across various departments was allowing cases to
be missed, treatment failure to occur and was amplifying the risk of drug resistant TB.
HDL implementation has enabled expansion of DOTS coverage in these settings. Furthermore,
domains impacted by the HDL intervention; linkage building, diagnostic support to the
laboratory, and implementation of standardized treatment protocols have built key capacities
of both personnel and systems in implementing hospitals
The HDL intervention included management of adult and childhood TB cases according to the
national guidelines. Through this initiative, over 4,000 doctors, paramedics and lab technicians
in 32 tertiary care hospitals were trained on TB DOTS as well as adult difficult-to-diagnose and
childhood TB management. This initiative is now being scaled up across the country in all
district headquarters hospitals and 16 additional tertiary care hospitals.
Historically, it has always been difficult to include tertiary care hospitals in TB DOTS
implementation, but NTP along with its implementing partners, was able to introduce core TB
DOTS interventions for pulmonary, extra-pulmonary and childhood TB in these tertiary care
hospitals. The program continued to face challenges such as weak linkages between different
departments within the hospital as well as with peripheral facilities. Due to high turn over of

58
staff and resistance from consultants and hospital administration, uniform implementation of
national TB guidelines is still a challenge.
The teaching hospitals, at the tertiary care level, are mainly located in major and all
metropolitan cities of the country. They have a catchment population of their own district and,
in some cases, patients are also referred from adjacent districts. There are about thirty-five
teaching and specialized hospitals in Pakistan. Most of the teaching and specialized TB hospitals
are in the public sector whereas as few are in the private sector.
Below are the public sector hospitals which have own management authority.
Existing partners
Various types of stakeholders exist under this partnership. It mainly includes 27 Public Sector
and more than 10 Private Sector teaching hospitals under the Hospital DOTS Linkage (HDL)
initiative:
Punjab: LGH, Services, Jinnah, Mayo, Ganga Ram, BBH, Holy Family, DHQ Rawalpindi, Nishtar,
SheikZaid, Allied Hospital,
Sindh:Ojha Institute of Chest Diseases, Indus Hospital, Aga Khan
Balochistan: Bolan Medical Complex
KPK: LRH Pesh, HMC Pesh, AMC Abbott, King Abdullah Hospital
ICT: PIMS, FGSH
Arrangements
Through Global Fund support, the Hospital DOTS Linkage (HDL) model was implemented in
2008 teaching/specialized hospitals in the country. This includes: an advocacy and
implementation planning events, provision of anti-TB medicine and laboratory strengthening,
intra-hospital linkages and monitoring, and external linkages with district health services. In
addition, an HDL mobilizer was also made available through GF support in each hospital to
support the working of DOTS facilitator. Several other components of the TB program have
been added to the ongoing DOTS implementation in teaching and specialized hospitals include
the management of; difficult to diagnose and treat TB patients, TB-HIV co-infection, and
childhood TB (the details are described in relevant sections). Recently the support for this
implementation through GF has completed and there is a need to sustain the activities in these
hospitals.

59
Contribution
The table below provides an overview of the contribution of the HDL component in routine TB
care in year 2012.
Table 18: Contribution of HDL in core TB DOTS, 2012
Province Annual NSS+ % of Annual Provincial
Registration
% of Annual National
Registration
NSS+ All types
Punjab 3400 -
Balochistan 200 -
Sindh 3600 -
KPK 400 -
GB - -
AJK - -
ICT - -
FATA - -
Total 7600 - 7.5% 11%
5.5 EXTRA-PULMONARY TB DIAGNOSIS The current NTP arrangements have limited emphasis on the diagnostic arrangement for extra-
pulmonary TB, which accounts for a substantial proportion (30%) of all types of TB cases
diagnosed in a year. Aspirates or tissues requiring histopathology/ cytology can only be
examined in laboratories where a pathologist is available, which are mainly at the DHQ or
tertiary hospitals. There is almost no facility available at the primary health care level to
support the diagnosis of extra-pulmonary TB cases, which results in under diagnosis of smear-
negative TB.

60
5.6 CHILDHOOD TUBERCULOSIS Overview
Data about prevalence and incidence of TB in children is lacking. WHO estimates are that
children may comprise 3-23 % of the disease burden in high TB burden countries. However
globally, of the estimated 8.8 million new cases of TB that occurred in 2010, about 11%
occurred in children (<15 years of age). It is estimated, that with accurate diagnosis and good
reporting systems, children are likely to contribute 10-20% of the disease burden in areas
where TB is poorly controlled.
In Pakistan, the National Institute of Population Studies projects that, by 2020, there will be
about 67 million children (35% of the population) between ages 0-14 year in the country. The
exact proportion of children with TB in Pakistan is unknown. NTP surveillance data did not
differentiate age category of all registered child TB cases until 2010. Childhood TB case
reporting comprised of about 4% of all cases from 2002 to 2009. The reporting was of only
sputum smear positive cases. The incidence of pediatric TB provides an accurate measure of
ongoing transmission within communities, which is a key indicator of epidemic control.
After the revision of NTP reporting tools in 2010, the number of child cases notified was 25,737
(12%) in 2011. However, based on field experience, high smear positivity rate among adult TB
cases and limited contact screening it is expected that childhood TB cases may be much higher
than currently notified.
Through Global Fund support childhood TB interventions were implemented in a phased
manner:
• First phase
• 2004- 2008
• GF R2 support
• Guideline developed
• 42 districts
• Second phase
• 2009-2010
• GF R6 support
• Guidelines revised

61
• 27 TCHs
• Third phase
• 2011
• CG support
• 32 TCHs
• 30 Districts
• 25,737childhood TB cases notified in country from Jan-Dec 2011
• Fourth phase
• 2013- onward
• Scaling up of Childhood TB intervention in 141 DHQ Hospitals across the country
Childhood TB guidelines and materials
In the last few years the NTP has developed a comprehensive set of guidelines and training
materials for standardizing the management of childhood TB cases. Moreover, the new
recording and reporting tools have also incorporated key variables required to monitor
childhood TB care services. The materials developed include:
- Childhood Technical Guidelines
- Childhood TB case management desk guide
- Childhood TB training materials
The paediatricians involved in childhood TB case management receive a three-day training on
NTP childhood TB materials.
5.7 TB/HIV Pakistan is a low prevalence country for HIV (ANC prevalence 0.045%), however, recent
surveillance data (HASP Round 4, 2011) shows that Pakistan has a concentrated epidemic of HIV
with HIV prevalence rates higher than 5% in most-at-risk populations including injecting drug
users and transgendered sex workers. The prevalence among the Injecting Drug Users (IDUs) is
37.5%, and in transgendered sex workers, it is 7.2%. The prevalence of HIV among female sex
workers (FSWs) in Pakistan is 0.8%, and among male sex workers, it is 3.2%. Behavioral data
shows significant overlaps between different key populations, which provide a possible conduit

62
of spread of infection between these populations, and eventually into the general population
through a large bridging group (clients of sex workers). The National AIDS Control Program
(NACP) Pakistan has established 18 HIV Treatment and Care centers nationwide. These Centers
provide comprehensive HIV care services including free antiretroviral therapy, HIV counseling
and testing, care and treatment for opportunistic infections, acute and chronic HIV care, in-
patient admissions, linkages with social support NGOs, and advanced HIV diagnostic testing to
people infected or affected by HIV/AIDS and their families. Currently 7,568 known HIV cases are
registered with these 18 centers, about half of which (4,391) are on anti-retroviral therapy
(NACP 2014). From November 2007 to December 2012, NTP and its implementing partners
under the Global Fund-funded TB/HIV co-infection interventions screened 1,054 PLHIV for TB,
out of which 61 were diagnosed with TB (less than 6%).
The NTP is coordinating with the NACP for providing quality care to those suffering from TB/HIV
co-infection. A national level TB/HIV Board has been constituted to steer the two programs’
coordinated work for TB/HIV co-infection and MDR-TB. The existing HIV Treatment and Care
centers have been strengthened through the Global Fund Round 6 support to manage TB
screening and care for TB-HIV co-infected cases. The strengthening of these centers includes:
staff training, infection control measures, provision of materials, referral linkages, and
monitoring support to provide quality counseling and testing, and referral services.
Operational arrangements
A joint collaborating board for MDR-TB and TB/HIV, and a national technical working group for
TB/HIV have been constituted. The NTP/PTPs are following a policy of Intensified Case Finding
(ICF) – active TB case detection among PLHIV. It is recommended that Isoniazid (INH) Preventive
Therapy (IPT) should be administered to HIV patients after excluding active TB. The screening of
TB infection among HIV patients is also carried out.
Those found co-infected with TB and HIV is managed for TB/HIV co-infection at the nearest HIV
Treatment and Care Center. Active TB case finding among people living with HIV/AIDS at ARV
treatment centers is also carried out. To standardize care delivery, National guidelines were
developed and introduced for screening of TB patients for HIV. To date, 49,039 TB patients have
been counseled and screened for HIV. 160 HIV cases were detected among these TB patients.
Moreover, 1,054 People Living with HIV/AIDS (PLHIVs) were screened for TB among, out of
which 61 TB cases were detected and registered for treatment. 45 People Living with HIV/AIDS
(PLHIVs) diagnosed with latent TB were also put on INH prophylaxis.
There are 16 NTP Sentinel sites operating in Pakistan. The majority of the ART/ DOTS/ Sentinel
facilities are in same facility. The current situation, including proposed sites, is shown in the
table below.
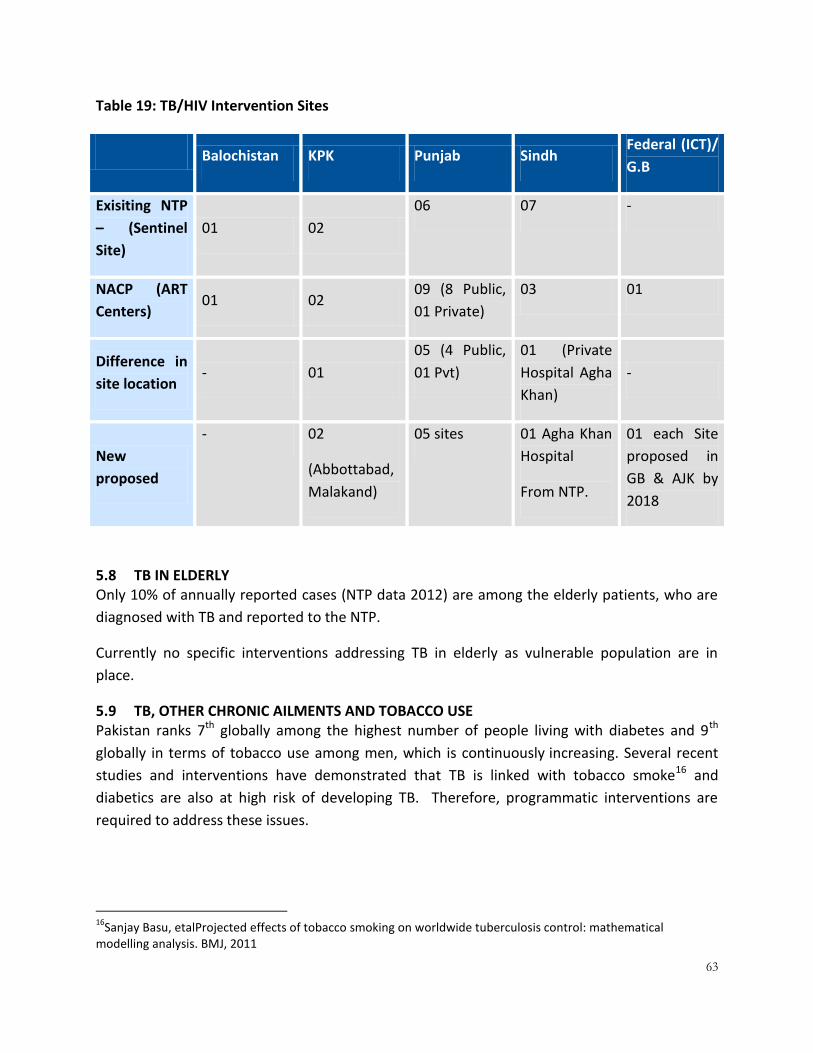
63
Table 19: TB/HIV Intervention Sites
Balochistan KPK Punjab Sindh
Federal (ICT)/
G.B
Exisiting NTP
– (Sentinel
Site)
01 02
06 07 -
NACP (ART
Centers) 01 02
09 (8 Public,
01 Private)
03 01
Difference in
site location - 01
05 (4 Public,
01 Pvt)
01 (Private
Hospital Agha
Khan)
-
New
proposed
- 02
(Abbottabad,
Malakand)
05 sites 01 Agha Khan
Hospital
From NTP.
01 each Site
proposed in
GB & AJK by
2018
5.8 TB IN ELDERLY Only 10% of annually reported cases (NTP data 2012) are among the elderly patients, who are
diagnosed with TB and reported to the NTP.
Currently no specific interventions addressing TB in elderly as vulnerable population are in
place.
5.9 TB, OTHER CHRONIC AILMENTS AND TOBACCO USE Pakistan ranks 7th globally among the highest number of people living with diabetes and 9th
globally in terms of tobacco use among men, which is continuously increasing. Several recent
studies and interventions have demonstrated that TB is linked with tobacco smoke16 and
diabetics are also at high risk of developing TB. Therefore, programmatic interventions are
required to address these issues.
16
Sanjay Basu, etalProjected effects of tobacco smoking on worldwide tuberculosis control: mathematical modelling analysis. BMJ, 2011

64
5.10 TB and diabetes Diabetes, a chronic metabolic disease is increasing globally, including in settings with high
burden of tuberculosis (TB) such as Pakistan. It is associated with higher risks of TB17 and
adverse TB treatment outcomes18. The increase in the number of people with diabetes may
further complicate control of TB, especially in population with high burden of both diseases19’20.
Diabetes can pose a challenge for the management of TB, and TB can worsen glycaemic control
in people with diabetes. Individuals with both conditions thus require careful clinical
management. Currently limited experience is available in Pakistan regarding TB-Diabetes joint
management. Strategies are needed to ensure that optimal care is provided to patients with
both diseases.
5.11 MANAGEMENT OF CONTACTS In year 2012, the total number of contacts screened were 143,667 and 4,504 TB cases were
diagnosed among them i.e. 32 contacts per TB case, which is a reasonable performance. This
shows that only 3% of contacts have been diagnosed.
For tuberculosis, a contact is defined as a person who shares the air with a known infectious TB
case. Close contacts, particularly household and workplace contacts, are considered to be at
high risk of contracting TB infection and disease. In low-incidence settings an average of 5–10
contacts are identified for each incident tuberculosis case. In high-prevalence countries, about
50% of household contacts have latent infection, and about 10–20% have active tuberculosis at
the time of initial investigation. Evidence suggests that contact investigation in high incidence
settings is a high-yield strategy for case finding. Contact management is therefore a tool for
early and active case finding and for reducing the duration of infectiousness of the case i.e. to
reduce TB transmission and burden.
High-risk contacts are contacts that are at a particularly high risk of developing TB disease if
they are exposed to an index case with smear positive tuberculosis. These are:
- Children under 5 years of age with no symptoms or above 5 years of age with symptoms
- HIV/AIDS patients
- People exposed to Silica
17
Jeon CY, et al. Diabetes mellitus increases the risk of active tuberculosis: a systematic review of 13 observational studies. PLoS Medicine, 2008, 5:e152. 18
Baker MA, et al. Systematic review: the impact of diabetes on tuberculosis treatment outcomes BMC Medicine accepted 2011, 9: 81. 19
Goldhaber-Fiebert JD, et al. Diabetes mellitus and tuberculosis in countries with high tuberculosis burdens: individual risks and social determinants. International Journal of Epidemiology, 2011, 40:417–428. 20
Dye C et al. Nutrition, Diabetes and Tuberculosis in the Epidemiological Transition. PLoS ONE, 2011, 6(6):e21161 (doi:10.1371/journal.pone.0021161).
65
In additional there are also certain groups which can be at a higher risk than the general
population for developing TB; thisincludes people with diabetes mellitus, COPD and smokers.
Contact management is one of the main strategies for TB elimination. The National TB control
program has declared contact tracing as integral part of the program and recommends
screening of close contacts of all infectious TB cases. The objective is to identify the people
suffering from TB disease at an early stage and stop TB transmission by treating identified TB
cases amongst contacts.
5.12 QUALITY ASSURED BACTERIOLOGY
Overview
The laboratory network established by the TB control Program in Pakistan to support the
diagnosis and quality of services has evolved over the years. The basic microscopy network in
the public sector, which is performing AFB microscopy, is established at RHCs, THQ/DHQ
hospital and tertiary care hospitals. It has also been extended into the private sector, under the
PPM model, and is also involved in DR-TB care based on standardized criteria.
There are about 1,230 microscopy centres in 141 districts of Pakistan which have been
strengthened with the provision of a light microscope, slides and reagents, sputum cups and
print materials and training for a microscopist who performs sputum smear microscopy. Only a
few BHUs also have these arrangements and, to a certain extent, are performing AFB
microscopy. On average, at the end of 2012, one microscopy laboratory was serving a
population of 131,421 population country wide; this varies from province to province /region
depending on population density and geographical terrain which ranges from 54,254 in GB to
164,791 in Punjab.

66
Table 20: Milestones achieved by the laboratory network
Year Situation/ Milestones
2000 >50 microscopy lab / No network/ No NRL/ No IDL
2001 NRL/PRL designated
2005 Microscopy network coverage in entire public sector
2005-06 EQA piloted in one district
2006-09 EQA implemented to cover >90% of centers. IDL established
2009 NRL started culture +DST services
2009-13 Expansion of TB culture and DST services
2010-11 TB disease prevalence survey
2011-13 Early implementation and expansion of XPERT
2012-13 Drug Resistance Survey
5.12.1 Organization of laboratory network
Pakistan’s TBC TB laboratory network has evolved over years. It is now arranged at four tiers
and is comprised of one National Reference Laboratory, 4 Provincial Reference Laboratories,
115 district laboratories and > 1400 peripheral laboratories (inclusive of the private sector)
Table 21: Functional level /location and current defined responsibilities are as follows
Level Location Main Responsibilities
National reference
laboratory
Federal
Capital
All technical functions +Policy guideline, SOP, TOT
and Monitoring, Surveys
Provincial reference
laboratory
Provincial HQ All technical functions +Planning ,Training
,supervision, monitoring of District lab network
67
District TB laboratory DHQ, DTO,
EDO-office
AFB microscopy + EQA implementation,
supervision, stain preparation lab supply
management
AFB Microscopy
Laboratories
DHQ, THQ,
RHC, TCH
AFB microscopy
The key set of indicators which the NTP is currently monitoring under core laboratory network
includes:
- Suspect positivity rate
- Follow-up smear positivity rate
- Proportion false positive
- Proportion false negative
- Efficiency of microscopy (agreement rate)
5.12.2 Diagnostic services and coverage
5.12.2.1 AFB microscopy services
The NTP guidelines recommend AFB microscopy as the initial diagnostic tool for screening of TB
suspects. Direct smear, ZN staining technique and Bright field microscopes are used. Two
specimens are examined for diagnosis of pulmonary TB and, for treatment monitoring, one
specimen is examined for AFB smear at the end of 2, 4 and 6 months of treatment.
The initially recommended policy for three sputum specimens was replaced with two sputum
specimens for diagnosis of TB in 2012 as the EQA coverage expanded.
Introduction of LED FM: The Program plans to phase in LED fluorescent microscopy in high
workload laboratories. Support available include 200 LED microscopes through USAID funding,
36 microscopes through Global fund round 9, and 250 microscopes through KFW for KP
province. Training of trainers (TOT) was organized at the NTRL and training is currently in
process at the provincial level.
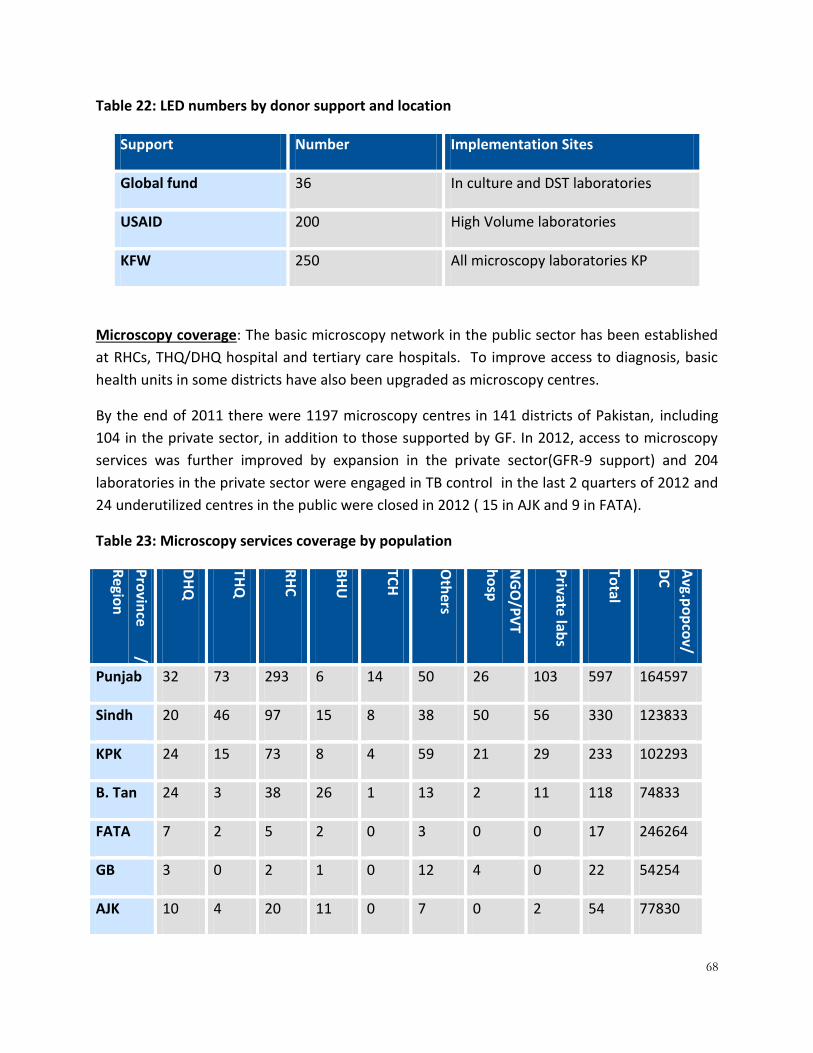
68
Table 22: LED numbers by donor support and location
Support Number Implementation Sites
Global fund 36 In culture and DST laboratories
USAID 200 High Volume laboratories
KFW 250 All microscopy laboratories KP
Microscopy coverage: The basic microscopy network in the public sector has been established
at RHCs, THQ/DHQ hospital and tertiary care hospitals. To improve access to diagnosis, basic
health units in some districts have also been upgraded as microscopy centres.
By the end of 2011 there were 1197 microscopy centres in 141 districts of Pakistan, including
104 in the private sector, in addition to those supported by GF. In 2012, access to microscopy
services was further improved by expansion in the private sector(GFR-9 support) and 204
laboratories in the private sector were engaged in TB control in the last 2 quarters of 2012 and
24 underutilized centres in the public were closed in 2012 ( 15 in AJK and 9 in FATA).
Table 23: Microscopy services coverage by population
Pro
vince
/
Regio
n
DH
Q
THQ
RH
C
BH
U
TCH
Oth
ers
NG
O/P
VT
ho
sp
Private
labs
Total
Avg.p
op
cov/
DC
Punjab 32 73 293 6 14 50 26 103 597 164597
Sindh 20 46 97 15 8 38 50 56 330 123833
KPK 24 15 73 8 4 59 21 29 233 102293
B. Tan 24 3 38 26 1 13 2 11 118 74833
FATA 7 2 5 2 0 3 0 0 17 246264
GB 3 0 2 1 0 12 4 0 22 54254
AJK 10 4 20 11 0 7 0 2 54 77830
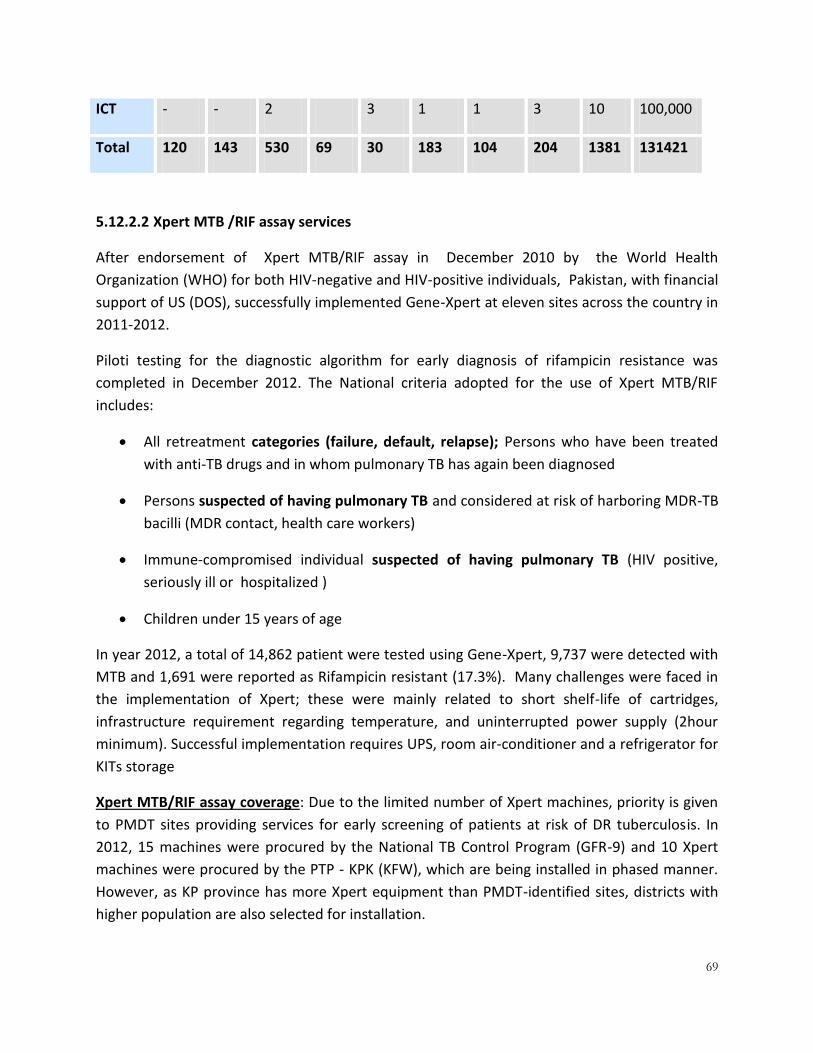
69
ICT - - 2 3 1 1 3 10 100,000
Total 120 143 530 69 30 183 104 204 1381 131421
5.12.2.2 Xpert MTB /RIF assay services
After endorsement of Xpert MTB/RIF assay in December 2010 by the World Health
Organization (WHO) for both HIV-negative and HIV-positive individuals, Pakistan, with financial
support of US (DOS), successfully implemented Gene-Xpert at eleven sites across the country in
2011-2012.
Piloti testing for the diagnostic algorithm for early diagnosis of rifampicin resistance was
completed in December 2012. The National criteria adopted for the use of Xpert MTB/RIF
includes:
All retreatment categories (failure, default, relapse); Persons who have been treated
with anti-TB drugs and in whom pulmonary TB has again been diagnosed
Persons suspected of having pulmonary TB and considered at risk of harboring MDR-TB
bacilli (MDR contact, health care workers)
Immune-compromised individual suspected of having pulmonary TB (HIV positive,
seriously ill or hospitalized )
Children under 15 years of age
In year 2012, a total of 14,862 patient were tested using Gene-Xpert, 9,737 were detected with
MTB and 1,691 were reported as Rifampicin resistant (17.3%). Many challenges were faced in
the implementation of Xpert; these were mainly related to short shelf-life of cartridges,
infrastructure requirement regarding temperature, and uninterrupted power supply (2hour
minimum). Successful implementation requires UPS, room air-conditioner and a refrigerator for
KITs storage
Xpert MTB/RIF assay coverage: Due to the limited number of Xpert machines, priority is given
to PMDT sites providing services for early screening of patients at risk of DR tuberculosis. In
2012, 15 machines were procured by the National TB Control Program (GFR-9) and 10 Xpert
machines were procured by the PTP - KPK (KFW), which are being installed in phased manner.
However, as KP province has more Xpert equipment than PMDT-identified sites, districts with
higher population are also selected for installation.

70
Table 24: Gene-Xpert Expansion Plan
5.12.2.3 TB Culture & DST services
Through GFR-6 and 9 grant resources were secured to establish 6 TB Culture + DST and 16 TB
culture laboratories to provide equal access population in different geographical areas of
Pakistan.
Laboratories are being established by upgrading existing structure to improve bio-safety
conditions and workflow. TB culture and DST laboratories expansion were delayed due to
procedural complexities, and limited technical capacity. Civil work has now been recently
completed in one DST lab (PRL Karachi) and 3 Culture lab including one in Sindh (ICD) one in
Punjab (AHF) one in KP (ATH). TB laboratories performing culture and DST have been
established in the in Private sector. Two main Private laboratories, providing TB culture and
DST services for PMDT program, are located in Karachi i.e TB laboratory in Agha Khan Hospital
Indus Hospital.
5.12.3 TB culture services
TB culture policy: Services are required for bacteriological diagnosis of tuberculosis in smear
negative and extra-pulmonary tuberculosis and monitoring of treatment of patient on second
line treatment.
Diagnosis of smear negative and EPTB cases: There is no clear guideline /diagnostic algorithm
on use of culture for bacteriological diagnosis of smear negative and extra-pulmonary
tuberculosis. Introduction of Xpert MTB /Rif assay has largely reduced the need of culture
laboratories for diagnosis of Tuberculosis.
Nat
ion
al
Pu
nja
b
Sin
dh
KP
K
Bal
uch
ista
n
FATA
AJK
GB
Tota
l
2011 1 5 3 1 1 0 0 0 11
2012 1 6 3 4 1 0 0 0 15
2013/
2014 2 12 8 10 3 6 1 1 43
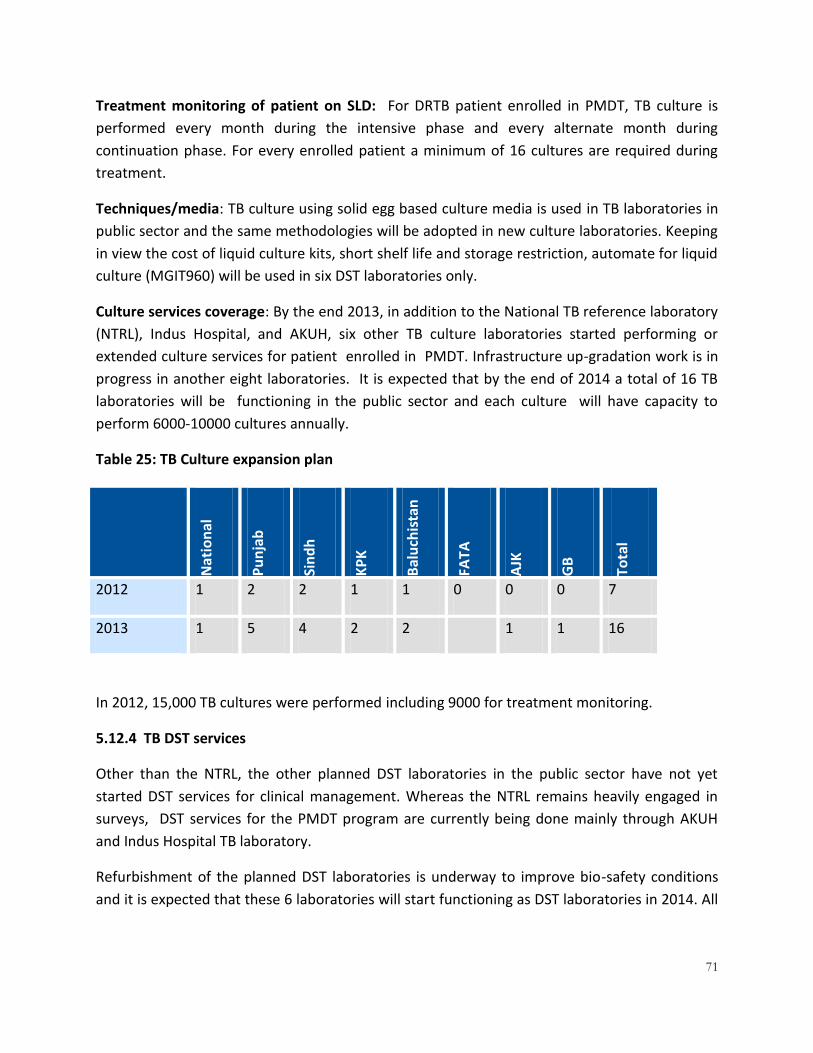
71
Treatment monitoring of patient on SLD: For DRTB patient enrolled in PMDT, TB culture is
performed every month during the intensive phase and every alternate month during
continuation phase. For every enrolled patient a minimum of 16 cultures are required during
treatment.
Techniques/media: TB culture using solid egg based culture media is used in TB laboratories in
public sector and the same methodologies will be adopted in new culture laboratories. Keeping
in view the cost of liquid culture kits, short shelf life and storage restriction, automate for liquid
culture (MGIT960) will be used in six DST laboratories only.
Culture services coverage: By the end 2013, in addition to the National TB reference laboratory
(NTRL), Indus Hospital, and AKUH, six other TB culture laboratories started performing or
extended culture services for patient enrolled in PMDT. Infrastructure up-gradation work is in
progress in another eight laboratories. It is expected that by the end of 2014 a total of 16 TB
laboratories will be functioning in the public sector and each culture will have capacity to
perform 6000-10000 cultures annually.
Table 25: TB Culture expansion plan
Nat
ion
al
Pu
nja
b
Sin
dh
KP
K
Bal
uch
ista
n
FATA
AJK
GB
Tota
l
2012 1 2 2 1 1 0 0 0 7
2013 1 5 4 2 2
1 1 16
In 2012, 15,000 TB cultures were performed including 9000 for treatment monitoring.
5.12.4 TB DST services
Other than the NTRL, the other planned DST laboratories in the public sector have not yet
started DST services for clinical management. Whereas the NTRL remains heavily engaged in
surveys, DST services for the PMDT program are currently being done mainly through AKUH
and Indus Hospital TB laboratory.
Refurbishment of the planned DST laboratories is underway to improve bio-safety conditions
and it is expected that these 6 laboratories will start functioning as DST laboratories in 2014. All

72
these DST laboratories will be equipped with Liquid Culture (MGIT) and molecular diagnosis of
MDR using line probe assay technique.
5.12.5 National Reference Laboratory
The TB laboratory in the federal TB center of Rawalpindi was designated as the National
Reference laboratory in 2002. While in the struggling phase to develop its technical capacity,
its structure was demolished on administrative grounds in 2005. While the national reference
laboratory played a key role in strengthening the microscopy network and implementation of
EQA, technical functions related to culture and DST remained suspended for four years due to a
lack of space. In 2009 the building was allocated in the premises of the federal general hospital
near NIH. After up-gradation the NTRL started functioning and soon achieved 100% proficiency
for First line DST (16th round of panel testing coordinated by SNRL Antwerp Belgium) and in the
subsequent year achieved proficiency for second line DST as well in the 17th Round. The NRL
maintained its proficiency in subsequent years.
A major accomplishment in 2012 was completion of the Prevalence survey, and the start of the
FIRST NATIONAL DRUG RESISTANCE SURVEY. Currently the DRS survey is in progress, field
work was completed in September 2013 and the interim report will be available by the second
quarter of 2014.
Table 26: Drug resistance pattern at NRL 2012
NEW Cases Retreatment Cases
2009
(Q-4) 2010 2011 2012
2009
(Q-4) 2010 2011
2012
Available DST for
H & R
112 252 186 461 23 118 109 154
Resistant to H
but not R
8 14 13 37 4 10 11 9
Resistant to R
but not H
1 1 0 2 1 3 1 2
Resistant to R+H
(%)
5
(4 %)
8
(3 %)
11
(5.9%)
19
(4.1%)
7
(30 %)
39
(33 %)
28
(25.6%)
55
(35.7%)
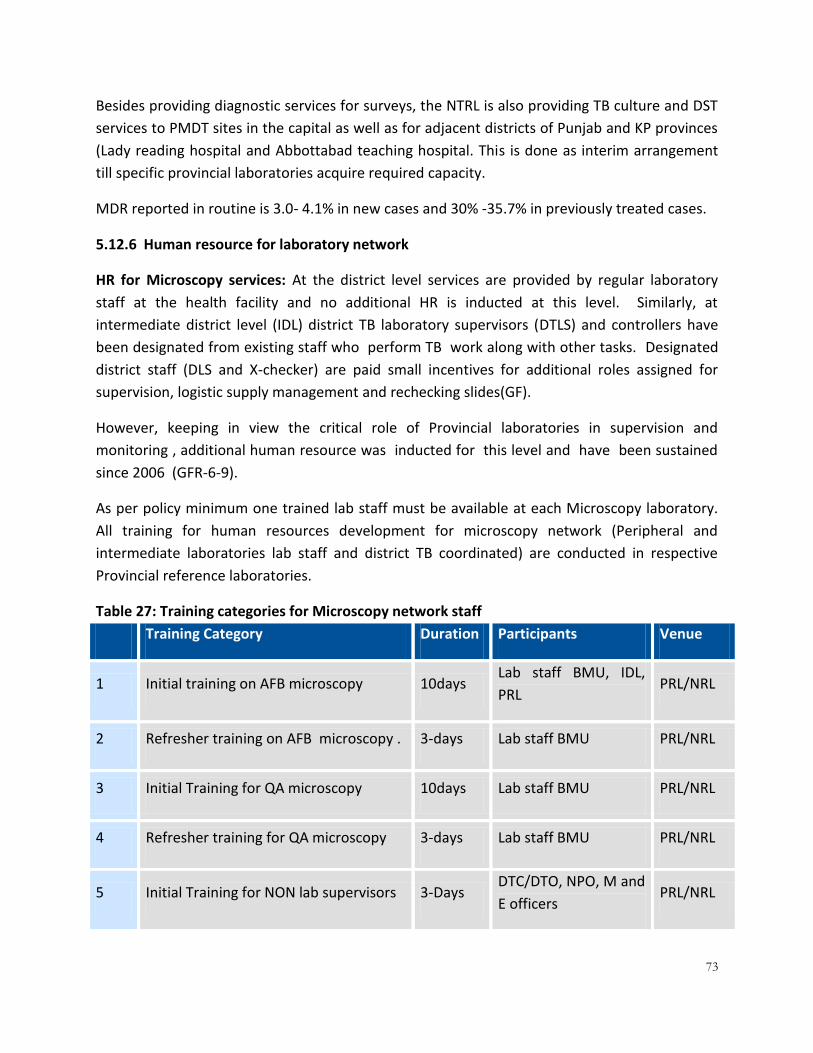
73
Besides providing diagnostic services for surveys, the NTRL is also providing TB culture and DST
services to PMDT sites in the capital as well as for adjacent districts of Punjab and KP provinces
(Lady reading hospital and Abbottabad teaching hospital. This is done as interim arrangement
till specific provincial laboratories acquire required capacity.
MDR reported in routine is 3.0- 4.1% in new cases and 30% -35.7% in previously treated cases.
5.12.6 Human resource for laboratory network
HR for Microscopy services: At the district level services are provided by regular laboratory
staff at the health facility and no additional HR is inducted at this level. Similarly, at
intermediate district level (IDL) district TB laboratory supervisors (DTLS) and controllers have
been designated from existing staff who perform TB work along with other tasks. Designated
district staff (DLS and X-checker) are paid small incentives for additional roles assigned for
supervision, logistic supply management and rechecking slides(GF).
However, keeping in view the critical role of Provincial laboratories in supervision and
monitoring , additional human resource was inducted for this level and have been sustained
since 2006 (GFR-6-9).
As per policy minimum one trained lab staff must be available at each Microscopy laboratory.
All training for human resources development for microscopy network (Peripheral and
intermediate laboratories lab staff and district TB coordinated) are conducted in respective
Provincial reference laboratories.
Table 27: Training categories for Microscopy network staff
Training Category Duration Participants Venue
1 Initial training on AFB microscopy 10days Lab staff BMU, IDL,
PRL PRL/NRL
2 Refresher training on AFB microscopy . 3-days Lab staff BMU PRL/NRL
3 Initial Training for QA microscopy 10days Lab staff BMU PRL/NRL
4 Refresher training for QA microscopy 3-days Lab staff BMU PRL/NRL
5 Initial Training for NON lab supervisors 3-Days DTC/DTO, NPO, M and
E officers PRL/NRL
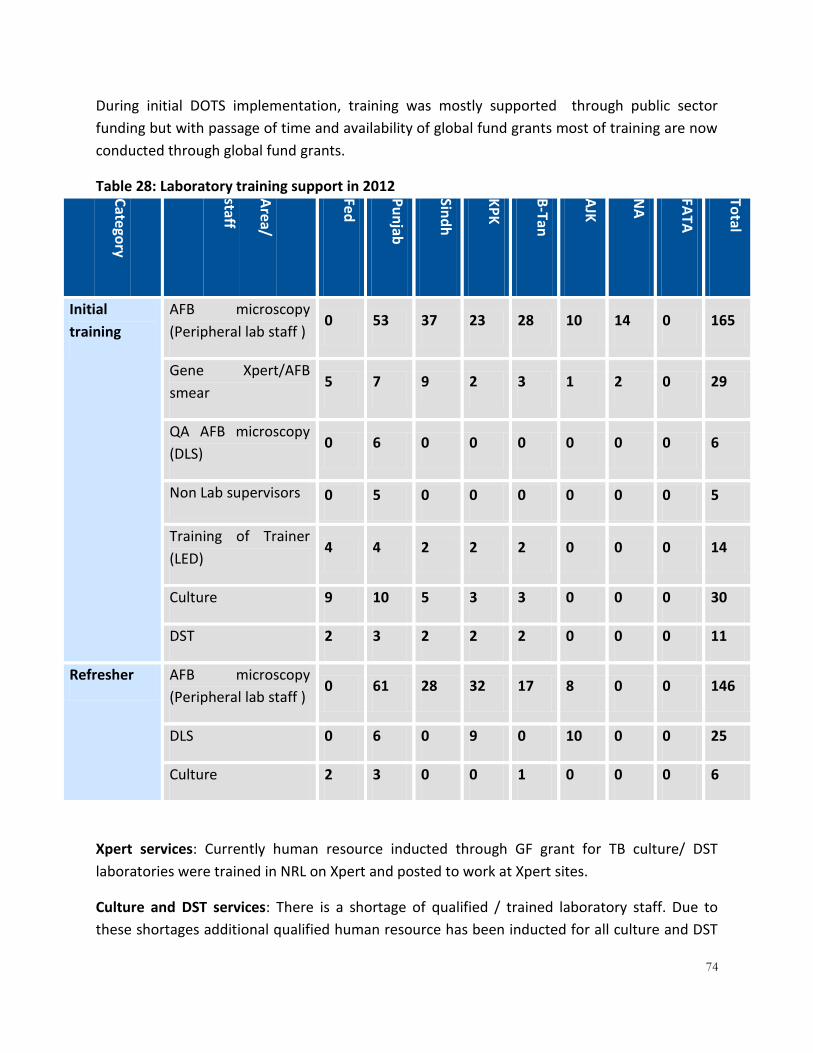
74
During initial DOTS implementation, training was mostly supported through public sector
funding but with passage of time and availability of global fund grants most of training are now
conducted through global fund grants.
Table 28: Laboratory training support in 2012 Cate
gory
Area/
staff
Fed
Pu
njab
Sind
h
KP
K
B-Tan
AJK
NA
FATA
Total
Initial
training
AFB microscopy
(Peripheral lab staff ) 0 53 37 23 28 10 14 0 165
Gene Xpert/AFB
smear 5 7 9 2 3 1 2 0 29
QA AFB microscopy
(DLS) 0 6 0 0 0 0 0 0 6
Non Lab supervisors 0 5 0 0 0 0 0 0 5
Training of Trainer
(LED) 4 4 2 2 2 0 0 0 14
Culture 9 10 5 3 3 0 0 0 30
DST 2 3 2 2 2 0 0 0 11
Refresher AFB microscopy
(Peripheral lab staff ) 0 61 28 32 17 8 0 0 146
DLS 0 6 0 9 0 10 0 0 25
Culture 2 3 0 0 1 0 0 0 6
Xpert services: Currently human resource inducted through GF grant for TB culture/ DST
laboratories were trained in NRL on Xpert and posted to work at Xpert sites.
Culture and DST services: There is a shortage of qualified / trained laboratory staff. Due to
these shortages additional qualified human resource has been inducted for all culture and DST

75
laboratories. Newly inducted staff is then trained in NRL. All training for culture and DST
laboratories is centralized and is organised at NTRL.
5.12.7 Quality management systems within the laboratory network
Quality assurance of microscopy services: The external quality assurance (EQA) by blinded
rechecking remains the corner stone for quality assured microscopy services. The intermediate
laboratory at the district level plays a critical role in EQA activities, preparation and distribution
of lab supplies. Every quarter sample of slides are collected for rechecking during intra-district
meeting
In 2012, 1,179 DCs (including 84 DCs of PPM-GF) in 127 districts were covered by EQA.
Continued support was provided for quality assured microscopy services including human
resource development, participation of laboratory staff in quarterly surveillance meeting and
provision of laboratory supplies.
Figure 10: Microscopy EQA coverage and performance
Table 29: Diagnostic network in Pakistan
1026
1131 1148 1159 1181 1187
1381
324 360
940 1005
1106 1097 1179
95 188
570 640
749 827 840
0
200
400
600
800
1000
1200
1400
1600
2006 2007 2008 2009 2010 2011 2012
# DC # DC under EQA # acceptable performance

76
Mic
rosc
op
y N
etw
ork
Year
Pu
njab
Sind
h
KP
B.T
AN
AJK
GB
FATA
ICT
Total
2005 445 237 163 63 35 11 28 - 982
2006 445 237 181 80 35 18 28 - 1026
2007 472 259 199 102 57 18 24 - 1131
2008 473 262 203 102 62 22 24 - 1148
2009 473 264 199 108 67 22 26 - 1159
2010 486 270 202 108 67 22 26 - 1181
2011 487 274 203 108 67 22 26 - 1187
2012 494 274 204 107 52 22 17 7 1177
2012(PPM-GF)
103 56 29 11 2 0 0 3 204
EQA
co
vera
ge
2006 111 84 71 29 18 11 0 - 324
2007 118 91 81 40 18 12 0 - 360
2008 420 234 200 57 13 2 14 - 940
2009 441 262 191 91 0 0 20 - 1005
2010 482 268 200 93 48 0 15 - 1106
2011 480 268 199 98 53 0 14 - 1112
2012 491 270 201 89 53 0 17 3 1124
2012(PPM-GF)
33 45 5 0 1 0 0 0 84
# o
f C
en
ters
w
ith
ac
cep
tab
le
resu
lt
2006 20 15 31 22 2 5 0 - 95
2007 42 61 49 21 4 11 0 - 188
2008 257 125 124 43 7 2 12 - 570
2009 282 138 127 75 0 0 18 - 640
2010 319 149 149 85 34 0 13 - 749
2011 361 167 133 89 25 NA 13 - 788
2012 368 165 132 74 38 NA 17 3 797
2012(PPM-GF)
28 36 4 NA 1 NA NA NA 69
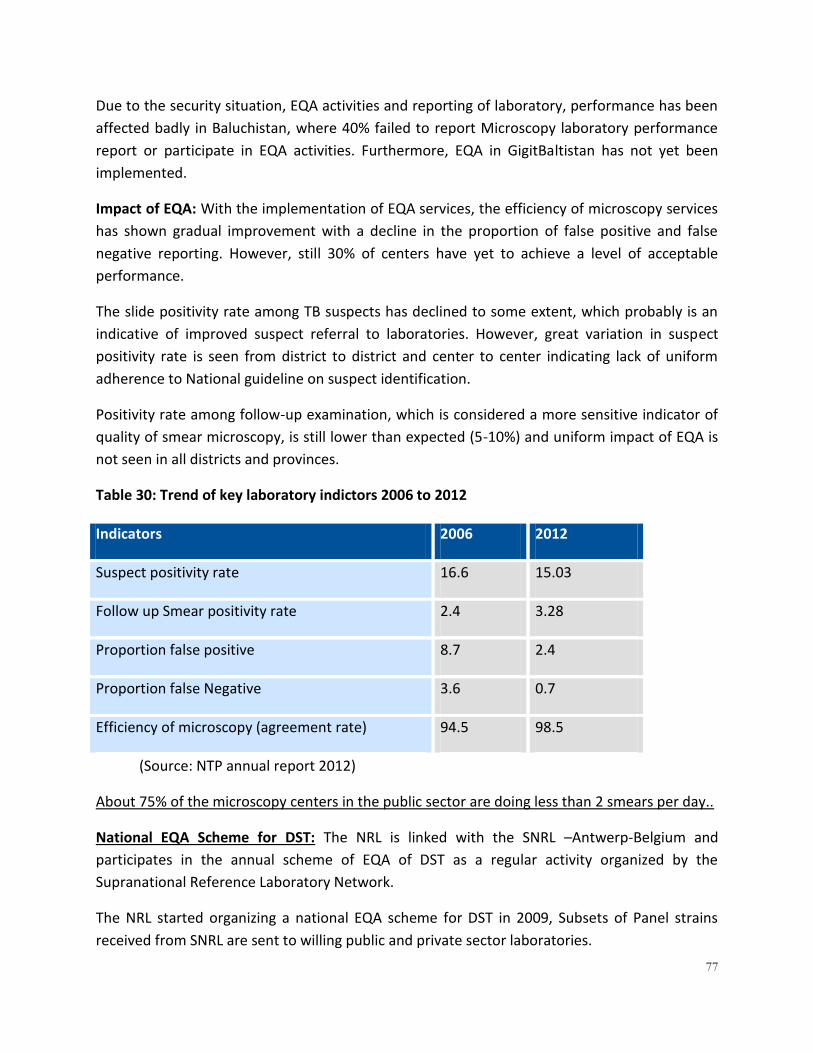
77
Due to the security situation, EQA activities and reporting of laboratory, performance has been
affected badly in Baluchistan, where 40% failed to report Microscopy laboratory performance
report or participate in EQA activities. Furthermore, EQA in GigitBaltistan has not yet been
implemented.
Impact of EQA: With the implementation of EQA services, the efficiency of microscopy services
has shown gradual improvement with a decline in the proportion of false positive and false
negative reporting. However, still 30% of centers have yet to achieve a level of acceptable
performance.
The slide positivity rate among TB suspects has declined to some extent, which probably is an
indicative of improved suspect referral to laboratories. However, great variation in suspect
positivity rate is seen from district to district and center to center indicating lack of uniform
adherence to National guideline on suspect identification.
Positivity rate among follow-up examination, which is considered a more sensitive indicator of
quality of smear microscopy, is still lower than expected (5-10%) and uniform impact of EQA is
not seen in all districts and provinces.
Table 30: Trend of key laboratory indictors 2006 to 2012
Indicators 2006 2012
Suspect positivity rate 16.6 15.03
Follow up Smear positivity rate 2.4 3.28
Proportion false positive 8.7 2.4
Proportion false Negative 3.6 0.7
Efficiency of microscopy (agreement rate) 94.5 98.5
(Source: NTP annual report 2012)
About 75% of the microscopy centers in the public sector are doing less than 2 smears per day..
National EQA Scheme for DST: The NRL is linked with the SNRL –Antwerp-Belgium and
participates in the annual scheme of EQA of DST as a regular activity organized by the
Supranational Reference Laboratory Network.
The NRL started organizing a national EQA scheme for DST in 2009, Subsets of Panel strains
received from SNRL are sent to willing public and private sector laboratories.
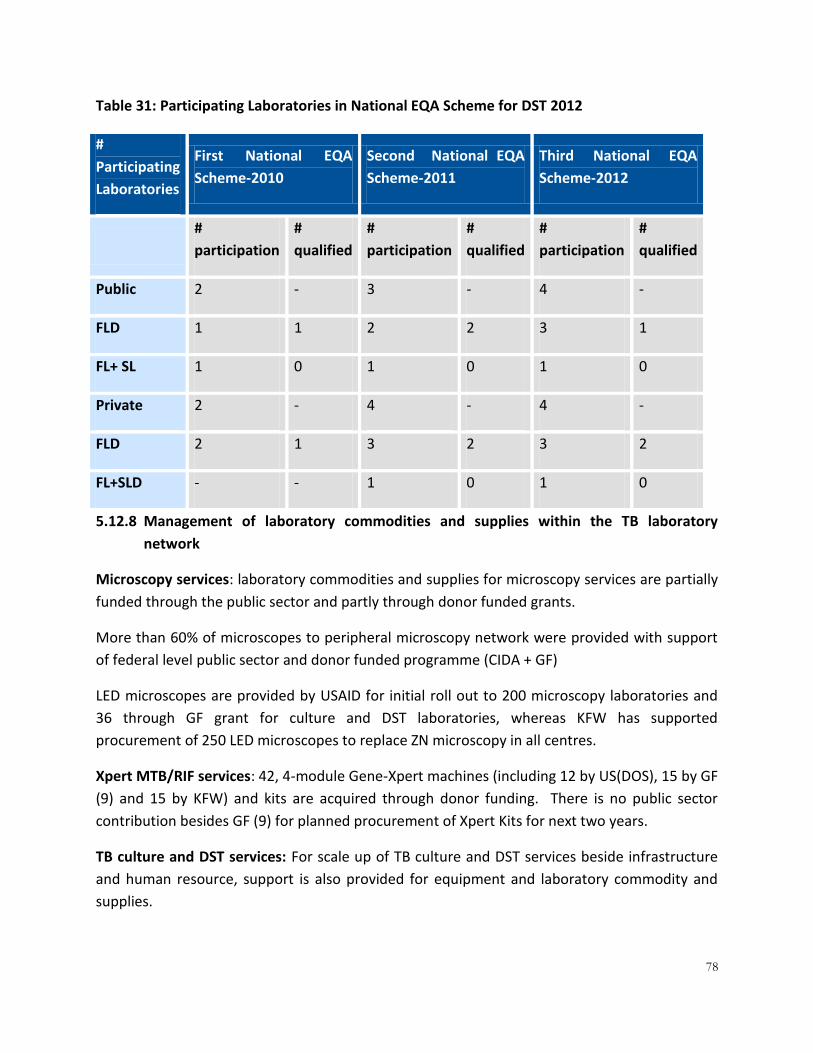
78
Table 31: Participating Laboratories in National EQA Scheme for DST 2012
#
Participating
Laboratories
First National EQA
Scheme-2010
Second National EQA
Scheme-2011
Third National EQA
Scheme-2012
#
participation
#
qualified
#
participation
#
qualified
#
participation
#
qualified
Public 2 - 3 - 4 -
FLD 1 1 2 2 3 1
FL+ SL 1 0 1 0 1 0
Private 2 - 4 - 4 -
FLD 2 1 3 2 3 2
FL+SLD - - 1 0 1 0
5.12.8 Management of laboratory commodities and supplies within the TB laboratory
network
Microscopy services: laboratory commodities and supplies for microscopy services are partially
funded through the public sector and partly through donor funded grants.
More than 60% of microscopes to peripheral microscopy network were provided with support
of federal level public sector and donor funded programme (CIDA + GF)
LED microscopes are provided by USAID for initial roll out to 200 microscopy laboratories and
36 through GF grant for culture and DST laboratories, whereas KFW has supported
procurement of 250 LED microscopes to replace ZN microscopy in all centres.
Xpert MTB/RIF services: 42, 4-module Gene-Xpert machines (including 12 by US(DOS), 15 by GF
(9) and 15 by KFW) and kits are acquired through donor funding. There is no public sector
contribution besides GF (9) for planned procurement of Xpert Kits for next two years.
TB culture and DST services: For scale up of TB culture and DST services beside infrastructure
and human resource, support is also provided for equipment and laboratory commodity and
supplies.

79
In KP, laboratory commodities and supplies are supported through KFW (PRL in Peshawar),
however besides this only a very small fraction of equipment has been provided by provincial
programme in Sindh province. All other laboratories are supported through Global Fund grants.
5.12.9 Laboratory information and data management for the TB laboratory network
Microscopy services: recording and reporting tools are developed for microscopy as well as for
the QA programme; reporting is done on paper form at the district and sub districts level
whereas paper reports are consolidated at the provincial level and entered in a data base
developed in access
A web-based system for collecting TB Laboratory data has been introduced and is managed on-
line www.ntp.gov.pk. The new system allows the NRL as well as the PRL staff to complete the
quarterly routine performance and EQA data collection forms online.
Laboratory staff regularly participate in quarterly meetings held at the district level while the
DLS attend quarterly meetings organized by provincial labs.Xpert Services: specimen request
forms and recording and reporting tools have been developed and are used by staff working at
Xpert sites. Data is maintained in an excel file and shared regularly with the PTP and the NTRL.
Revised reporting and recording (2013) are not yet implemented.
Xpert data is regularly submitted to WHO.
TB culture and DST services: recording and reporting forms are developed and paper forms are
used in established culture and DST laboratories. An electronic recording and reporting system
is not yet developed.
5.12.10 Sample referral system for the TB laboratory network
Although specimen transport has been successfully used in the TB disease prevalence survey
and ongoing drug resistance survey and, to some extent, is now also used for transportation of
specimens from PMDT sites to culture laboratories. However, the transport system is not yet
established for transportation of specimens from BMUs to either Xpert sites or culture and DST
laboratories.
5.13 DRUG-RESISTANT (DR) TB 5.13.1 Overview
Drug resistance tuberculosis (DR-TB) is caused by organisms that are resistant to a first-line or
second-line anti-TB drug. The term DR-TB is used as it covers, in addition to MDR-TB, other
different types of drug resistant TB. Multi-Drug Resistant tuberculosis (MDR-TB) which is the
most common form of DR-TB, is caused by organisms that are resistant to Isoniazid and

80
Rifampicin (two first-line anti-TB drugs). According to Global TB Report 2013, there were
estimated 450,000 New MDR cases in the world in 2012 (range 300,000-600,000). The DR-TB is
a continued threat to the progress that Pakistan has made in controlling TB21.
Pakistan ranks 4th among 27 MDR-TB high burden countries in the world22. According to WHO
Global Report 2013, the 2012 estimated incidence for DR-TB was 3.5% among new TB cases and
32% among retreatment cases. At the same time, the NTP thorough GF support has conducted
and Drug Resistance Survey in 2012-2013; the preliminary results are 4.3% among new cases
and 19.4% among retreatment cases.
Since the Beijing’s call for action in April 2009, the NTP Pakistan has shown its commitment to
address MDR-TB through a structured and comprehensive approach, which includes developing
policies, strategies, guidelines and phased expansion of implementation activities. The NTP has
acted in accordance with the Beijing call to establish a comprehensive MDR-TB programme,
based on the recommendations of the call.
5.13.1 DR-TB estimates in Pakistan
Based on the 2012 National TB Data, using the WHO percentage of TB cases with MDR –TB, the
following table presents the estimates of DR-TB cases in the country:
Based on the National TB Data, using the preliminary results of DRS percentage of Pulmonary
TB cases with MDR-TB, the following table presents the estimates of DR-TB cases in the
country:
Table 32: Estimates of DR-TB in Pakistan 2012 based on WHO estimates
Year New Pul (B+,B-)
Retreatment cases
MDR-TB among notified TB case (using DRS preliminary estimates)
Total MDR estimates
Among New (4.3%)
Among Retreatment (19.4%)
2012 219970 11717 9459 2273 11732
2013 230496 10997 9911 2133 12044
5.13.2 Diagnostic approach to DR-TB
The use of Gene Xpert has been recommended as a first step testing to the following high risk
groups (DR-TB suspects) followed by routine culture and DST for all rifampicin resistant cases.
21
National Guidelines for PMDT, 2011, NTP-Pakistan 22
http://www.who.int/tb/publications/global_report

81
The NTP has recommended that the screening of DR-TB (presumptive TB cases) suspects
should be based on the following criteria (in order of priority):
GROUP I: TB PATIENT / Symptomatic at risk of DR-TB
A. ALL RETREATMENT TB CASES: All TB cases (AFB SS+ve or negative) with history of
previous ATT should be tested for Xpert at month zero of enrolment. This includes:
• Treatment Failure Cat-I (F-1)
• Treatment Failure Cat-II (F-2)
• Relapse after Cat-I (R-1)
• Relapse after Cat-II (R-2)
• Treatment after loss to follow up Cat-1(D-1)
• Treatment after loss to follow up Cat-II (D-2)
• Other Retreatment
B. SYMPTOMATIC CONTACTS OF DR-TB PATIENT:
All household and workplace symptomatic contacts of DR-TB patients should be screed for
RRTB. Specimen from these individuals should be processed for AFB smear and then the
specimen is referred for Xpert MTB/RIF assay irrespective of smear results.
C. TB PATIENTS UNDER TREATMENT WHO FAIL TO CONVERT AT THE END OF INTENSIVE
PHASE
• AFB smear +ve patient on Cat-1 who fail to convert at the end of month #2 of
treatment.
• AFB smear +ve patient on Cat- II who fail to convert at the end of 3 months.
• AFB smear negative Patient who is reported AFB smear positive at the end of intensive
phase
GROUP II: TB Symptomatic among vulnerable population
Screening of RRTB, for early diagnosis and management, is important to all individuals who are
potentially at risk of DR-TB and belong to vulnerable population. The specimen from these
individuals should be processed for AFB smear and then is referred for Xpert MTB/RIF assay
irrespective of Smear results. This group includes:

82
• Children under 15 years of age
• HIV positive
• Other immune-compromised (Diabetic, on immunosuppressive or chemotherapy)
• Injecting drug users
• Contact of TB
• Health Care workers including laboratory workers
• Hospitalized
• Prisoners
Group III: Individual suffering from a Life threatening disease or having difficulty in clinical
diagnosis
• Specimen from individuals suffering from life threatening illness, and at risk of TB,
should be tested with Xpert/MTB Rif assay (eg.CSF).
GROUP IV: AFB Smear Negative Clinically Diagnosed TB cases Not at risk of DR-TB:-
If not listed in any of the groups group mentioned above you may follow the program guidance
on Xpert testing on this group. Program may formulate new or revised policies for this group
based on resources.
The following groups are eligible to be enrolled on DR-TB treatment:
a) Patients detected as Rifampicin resistant on Gene Xpert.
b) Patients who have been confirmed to have DR-TB by DST
c) Patients with strong suspicion (high likelihood) of DR-TB (in absence of Gene-Xpert, the
patient might be enrolled on treatment while waiting for DST results).
83
5.13.3 Procedures for DR-TB enrolment, and follow-up management
The following procedures are used for enrolment of DR-TB on treatment:
a- An Initial meeting at the PMDT site with the DR-TB treatment coordinator
and management team to review all referring documents, laboratory and
radiological testing, perform all the clinical and laboratory examinations, fill
out all the necessary forms for enrolment and registry, evaluate the medical
conditions of the patient and decide on the best mode of care (Ambulatory
vs Hospitalized based), educate the patient about DR-TB treatment and care
and write a prescription order to the pharmacy to prepare for drugs. This
initial meeting will be followed by another visit after 2 weeks to ensure that
all elements of DR-TB management are taken care of and to make sure that
patient is doing well. The PMDT treatment site, along with PTP, DTC and DTO
will work together to identify the nearest DOT center (BMU), the treatment
supporter for DOT and monitoring & evaluation.
b- Patient’s Follow Up schedule at Month 1 – 8 of treatment after Enrolment
(Intensive Phase management):
The DR-TB patient, accompanied by treatment supporter, is expected to visit the nearest DOTS
center or PHC on a weekly basis during the Intensive Phase of treatment for early detection and
management of any adverse reaction and drugs replenishment, if applicable. The treatment
supporter administers each dosage under strict DOT.
On the other hand, the patient and treatment supporter are instructed to visit the PMDT site on
a monthly basis during the Intensive Phase of treatment for comprehensive review, laboratory
testing including monthly sputum for smear microscopy and culture, detection and
management of any adverse reaction and replenishment of drugs on a monthly basis.
c- Evaluation of DR-TB Patient’s Progress at the end of Month-8 of treatment:
At the end of Month-8 of treatment, the patient meets with the DR-TB clinician to review
eligibility for switching from the Intensive Phase to Continuation Phase management if the
patient has completed at least 8 months of injectable with at least 6 months of treatment after
culture conversion. If the patient did not meet the above criteria then the intensive phase will
be expanded until such a time when the patient meets the recommended criteria.
d- Patient’s Follow Up Visits to the PMDT site after the discontinuation of
Injectable (Continuation Phase management):
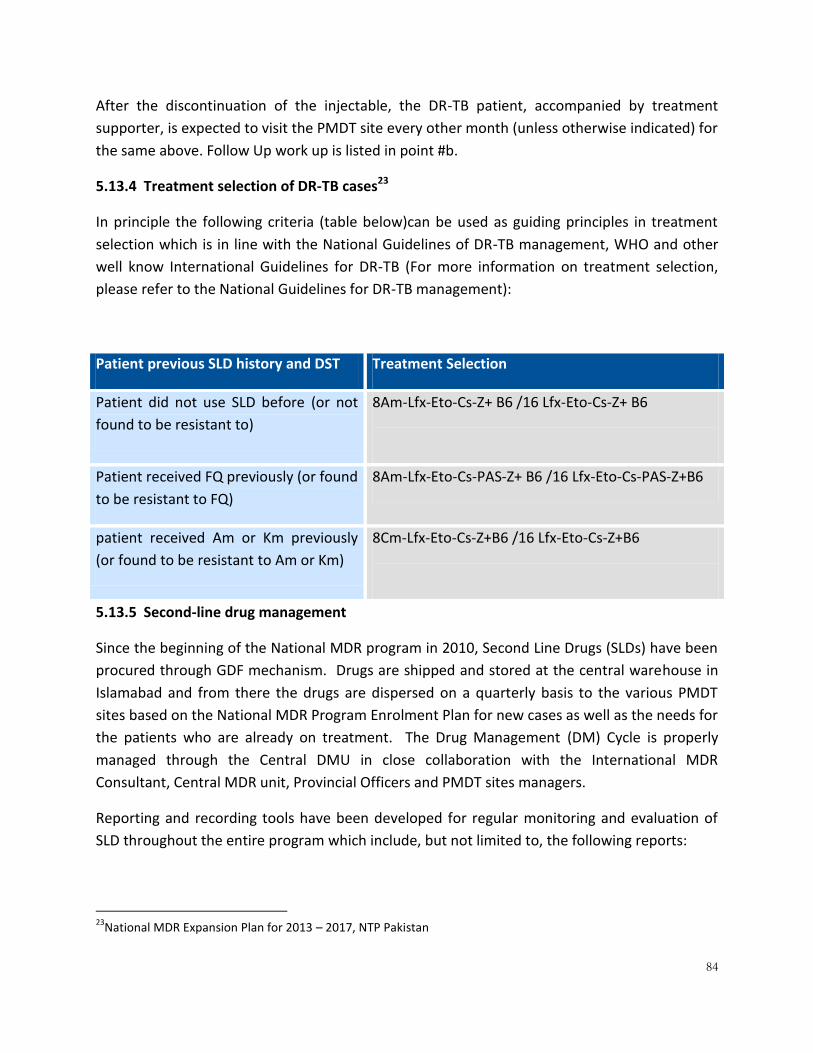
84
After the discontinuation of the injectable, the DR-TB patient, accompanied by treatment
supporter, is expected to visit the PMDT site every other month (unless otherwise indicated) for
the same above. Follow Up work up is listed in point #b.
5.13.4 Treatment selection of DR-TB cases23
In principle the following criteria (table below)can be used as guiding principles in treatment
selection which is in line with the National Guidelines of DR-TB management, WHO and other
well know International Guidelines for DR-TB (For more information on treatment selection,
please refer to the National Guidelines for DR-TB management):
Patient previous SLD history and DST Treatment Selection
Patient did not use SLD before (or not
found to be resistant to)
8Am-Lfx-Eto-Cs-Z+ B6 /16 Lfx-Eto-Cs-Z+ B6
Patient received FQ previously (or found
to be resistant to FQ)
8Am-Lfx-Eto-Cs-PAS-Z+ B6 /16 Lfx-Eto-Cs-PAS-Z+B6
patient received Am or Km previously
(or found to be resistant to Am or Km)
8Cm-Lfx-Eto-Cs-Z+B6 /16 Lfx-Eto-Cs-Z+B6
5.13.5 Second-line drug management
Since the beginning of the National MDR program in 2010, Second Line Drugs (SLDs) have been
procured through GDF mechanism. Drugs are shipped and stored at the central warehouse in
Islamabad and from there the drugs are dispersed on a quarterly basis to the various PMDT
sites based on the National MDR Program Enrolment Plan for new cases as well as the needs for
the patients who are already on treatment. The Drug Management (DM) Cycle is properly
managed through the Central DMU in close collaboration with the International MDR
Consultant, Central MDR unit, Provincial Officers and PMDT sites managers.
Reporting and recording tools have been developed for regular monitoring and evaluation of
SLD throughout the entire program which include, but not limited to, the following reports:
23
National MDR Expansion Plan for 2013 – 2017, NTP Pakistan

85
A monthly Computerized Central Warehouse inventory, bin card and stock balance
report.
A monthly PMDT Stock balance and matrix reports reflecting the monthly
consumption rate and stock balance at each treatment site.
A monthly update of the DR-TB Register (ENRS) for monitoring and evaluation new
and current enrolled patients’ treatment and follow up progress.
the NTP receives these reports on a monthly basis for proper analysis, verification, early
detection and immediate management of any possible stock out or drugs with short expiry
dates.
The NTP uses the following combined SLD procurement methods:
1- An Excel based calculated sheet reflecting the various treatment regimens and the
percentage of the new cohort using these regimens.
Table 33: SLDs for DR-TB patients recommended by NTP
Treatment regimen percentage of the
cohort using this
regimen
8 Am-Lfx-Cs-Eto-(PAS)+Z / 16 Lfx-Cs-Eto-(PAS)+Z. 85%
8 Cm-Lfx-Cs-Eto-(PAS)+Z /16Lfx-Cs-Eto-(PAS)+Z. 10%
Number of patients will need PAS 75%
8 Cm-Mfx-Cs-Eto-PAS + Z + Clr +Clo+Amo-Clav / 16Mfx-
Cs-Eto-PAS+ Z+ Clr+ Clo +Amo-Clav. 5%
2- An estimated SLD needs for the patients who are already on treatment at the time of
placing a SLD order request.
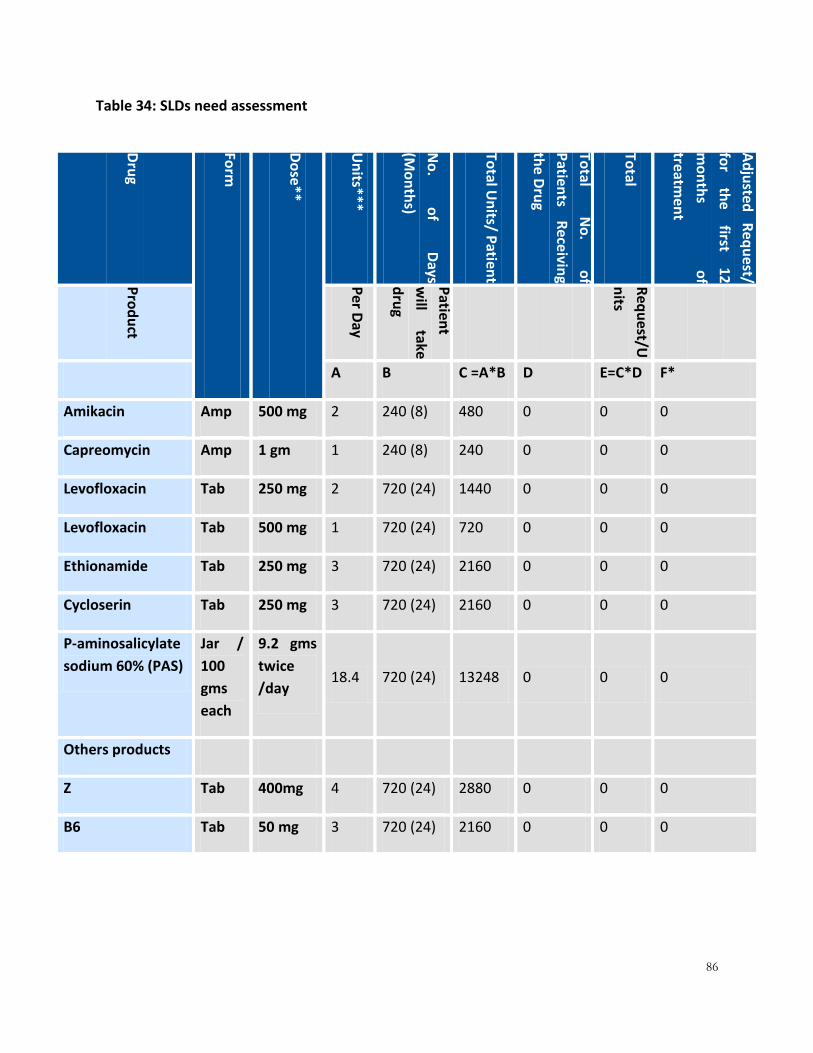
86
Table 34: SLDs need assessment
Dru
g
Form
Do
se**
Un
its***
No
. o
f D
ays
(Mo
nth
s)
Total U
nits/ P
atient
Total
No
. o
f
Patien
ts R
eceivin
g
the D
rug
Total
Ad
justed
R
equ
est/
for
the
first 12
mo
nth
s o
f
treatmen
t
Pro
du
ct
Per D
ay
Patien
t
will
take
dru
g
Req
uest/U
nits
A B C =A*B D E=C*D F*
Amikacin Amp 500 mg 2 240 (8) 480 0 0 0
Capreomycin Amp 1 gm 1 240 (8) 240 0 0 0
Levofloxacin Tab 250 mg 2 720 (24) 1440 0 0 0
Levofloxacin Tab 500 mg 1 720 (24) 720 0 0 0
Ethionamide Tab 250 mg 3 720 (24) 2160 0 0 0
Cycloserin Tab 250 mg 3 720 (24) 2160 0 0 0
P-aminosalicylate
sodium 60% (PAS)
Jar /
100
gms
each
9.2 gms
twice
/day 18.4 720 (24) 13248 0 0 0
Others products
Z Tab 400mg 4 720 (24) 2880 0 0 0
B6 Tab 50 mg 3 720 (24) 2160 0 0 0
87
5.13.6 Criteria to establish a programmatic management of DR-TB (PMDT) treatment site
The NTP Pakistan has established standard criteria for a DR-TB site:
a) Functional Gene-Xpert machine or access to the machine for testing suspected DR-TB
cases.
b) Establish TB culture and DST services or access to the services.
c) Infection control for outpatients, inpatients and community care of DR-TB cases in
place.
d) Access and ability to manage second line drugs.
e) Senior and mid-level doctors, paramedics and laboratory staff with role-specific training
and tools for delivering care as per national guidelines.
f) Arrangements to deliver Ambulatory based Model of Care of DR-TB care and established
linkage with a strong network of functioning DOTS clinics in public as well as private
sector.
g) Social support arrangements for patients and treatment supporters.
5.13.7 DR-TB guidelines and materials
The NTP has developed a set of materials and guidelines to structure the delivery of DR-TB care
through public and private sector hospitals. The materials include;
- National Guidelines on PMDT
- National TB Infection Control Guidelines
- Guidelines for management of second-line drugs
- DR-TB Recording and Reporting Tools (17 tools)
5.13.8 NTP/PTP arrangement for management of DR-TB initiative
The NTP has a fully established unit to manage the MDR-TB initiative at the national level.
Under the overall management of the National Manager, the MDR-TB unit is led by a National
MDR-TB coordinator supported by an international consultant. MDR-TB management is
implemented throughout the country with 5 sub recipient to the Global Fund grant. These
recipients are responsible for establishment and preparation of the MDR-TB management unit
(HR, training and logistics etc).
88
The provincial TB control programs, with the support of Global Fund grants, have been provided
with Provincial MDR-TB Coordinators and office assistants. The responsibility of the PTP is to
ensure the proper implementation of DR-TB programme.
5.13.9 Contribution of PMDT sites: National
By the end of 2013 18 PMDT treatment sites have been functional in the tertiary care hospitals
in the country whereas by September of 2014, 12 more PMDT sites are scheduled to be
prepared to begin enrollment of DR-TB case in different provinces of the country. Eighteen
additional PMDT sites, 12 in 2016 and 6 in 2017, are required for the MDR Expansion plan. The
current intervention is supported by the TGF Round 9 grant until mid 2015.

89
Table 35: Province wise PMDT sites and cases (2012)
S.# Province SR PMDT Sites / Hospitals Public/ Private
Status Date PMDT Started
1 ICT ASD PIMS Hospital, Islamabad Public Functional Nov-2013
2 Sindh IHK Indus Hospital, Karachi Private Functional June 2010
3 Sindh NTP/PTP Ojha Hospital, Karachi Public Functional June 2010
4 Sindh IHK Institute of Chest Diseases, Kotri
Public Functional Q1 2013
5 Sindh IHK Civil Hospital, Sukkur Public Functional Q1 2013
6 Sindh IHK JPMC Hospital, Karachi Public Functional June-2013
7 Sindh IHK DHQ Hospital, Nawabshah Public Q-3, 2013 Non-Functional
8 Sindh IHK CMC Hospital, Larkana Functional June-2013
9 Sindh IHK DHQ Hospital, MirpurKhas Public Q-3, 2014 Non-Functional
10 Punjab NTP/PTP Gulab Devi Hospital, Lahore Private Functional June 2010
11 Punjab ASD Leprosy Hospital, Rawalpindi Private Functional June 2011
12 Punjab ASD Nishtar Hospital, Multan Public Functional Q1 2013
13 Punjab ASD Mayo Hospital, Lahore Public Functional Q1 2013
14 Punjab ASD Samli Sanatorium, Murree Public Functional Q1 2013
15 Punjab ASD Jinnah Hospital, Lahore Functional June-2013
16 Punjab ASD Allied Hospital, Faisalabad Q-2, 2013 Non-Functional
17 Punjab ASD DHQ Hospital, Sargodha Public Functional Sept-2013
18 Punjab ASD DHQ Hospital, Bahawalpur Public Q-1, 2014 Non-Functional
19 Punjab ASD DHQ Hospital, Sialkot Public Q-2, 2014 Non-Functional
20 Punjab ASD Holy Family Hospital, Rawalpindi
Q-2, 2014 Non-Functional
21 Punjab ASD Sheikh Zaid Hospital, Rahim Yar Khan
Q-3, 2014 Non-Functional
22 Azad Kashmir ASD District Head Quarter, Muzaffarabad
Public Q-3, 2014 Non-Functional
23 KPK ACD Lady Reading Hospital, Peshawar
Public Functional March 2012
24 KPK ACD Ayub Teaching Hospital, Abbottabad
Public Functional Q1 2013

90
Note:As of end of July 2013, the total number of enrolled cases was 2,210.
5.13.10 DR-TB culture services
In 2012, 6 laboratories in the country were performing DR-TB culture services. So far 15,260
cultures were performed for patients in culture facilities linked with PMDT sites. It is expected
that 15 more will be operational in 2013, and 23 laboratories in 2015, with the support of GF.
Table 36: Province wise TB culture sites and diagnosis and follow-up performance
Sr.# Site/ Hospital Culture Performance
Total Diagnosis Follow-up
National
1. NRL 2233 2218 4451
Punjab
2. PRL-Punjab 1337 404 1741
3. GDH 1025 1313 2338
Sindh
4. PRL-Sindh 1005 4531 5536
25 KPK ACD DHQ Hospital, Swat Public Q-2, 2014 Non-Functional
26 KPK ACD DHQ Hospital, DI Khan Public Functional Sept-2013
27 GilgitBaltistan ACD District Head Quarter, Gilgit Public Q-3, 2014 Non-Functional
28 Baluchistan IHK Fatima Jinnah Hospital, Quetta Public Functional Q1 2013
29 Baluchistan IHK DHQ Hospital, Turbat Public Q-1, 2014 Non-Functional
30 Baluchistan IHK DHQ Hospital, Khuzdar Public Q-3, 2014 Non-Functional

91
KPK
5. PRL-KPK 540 279 819
Balochistan
6. PRL-Balochistan 86 289 375
Grand Total 6226 9034 15260
5.13.11 TB drug susceptibility testing laboratories
Currently, 7 laboratories are providing TB drug susceptibility testing services (BSL-3 level) in the
country. There are plans to upgrade 8 more laboratories to BSL-3 in 2013.
Table 37: TB DST expansion plan 2013
Provinces/ Regions 2012 2013 Total 2013
Federal/National 1 - 1
Punjab 2 2 4
Sindh 2 2 4
KPK 1 1 2
Balochistan 1 1 2
AJK - 1 1
GB - 1 1
TOTAL 7 8 15
(Source: NTP Draft Annual Report, 2012)
5.13.12 XPERT sites
Currently Xpert services are available at 11 (2011) and 15 (2012) sites/hospital in the country.
NTP is planning to extend these services in 42 labs in 2013.

92
Table 38: Status Gene Xpert tests (2012) and expansion plan (2013)
Sr.# Name of site/
hospital (2012) Public/private Gene Xpert performance 2012 Planned
sites 2013 # tests # RR %RR
Federal/National 2
1. NRL (NIH) Public 3161 321 10%
2. PMRC Public 6 4 67%
Punjab 12
3. RYK Public 148 16 11%
4. NMC-Multan Public 272 97 36%
5. Allied Hospital-
Faisalabad Public 120 19 16%
6. GDH- Lahore Private 810 289 36%
7. Jinnah Hospital
Lahore Public 112 13 12%
Sindh 8
8. PRL Karachi- Ojha
Institute Public 2496 278 11%
9. Kotri Public 578 200 35%
10. Larkana Public 344 85 25%
KPK 10
11. LRH Public 705 208 30%
12. PRL KP Public 306 53 17%
13. MMC Public 48 8 17%
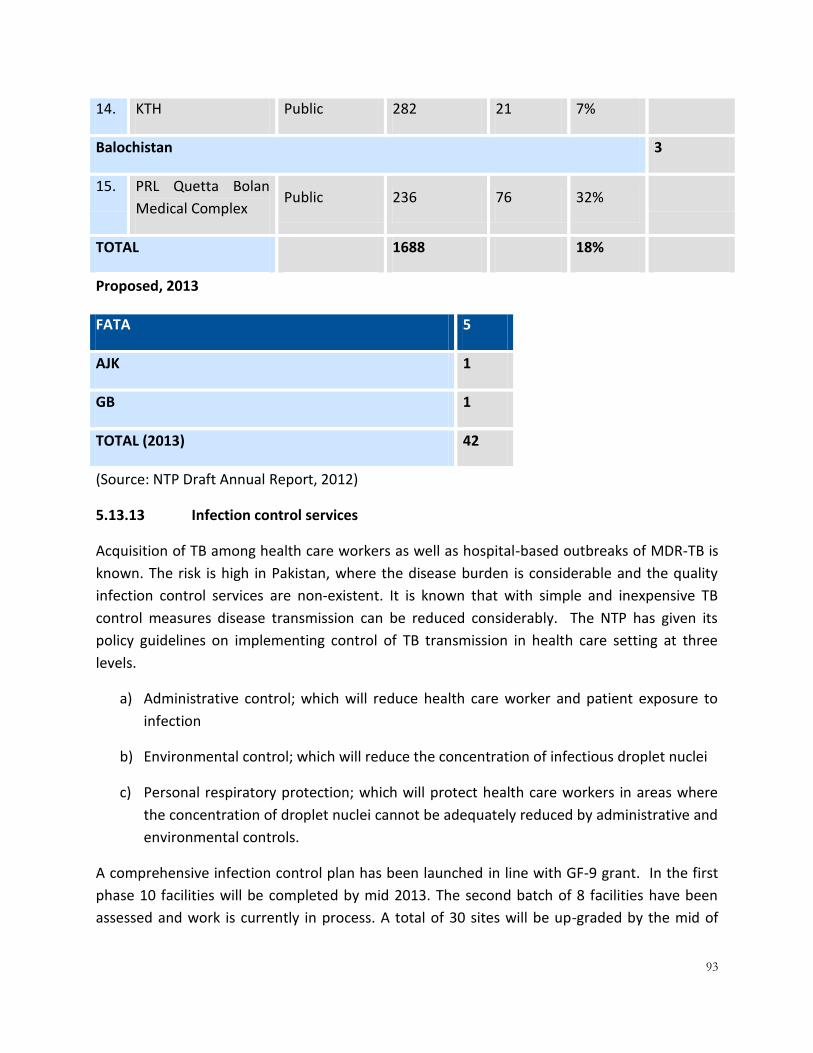
93
14. KTH Public 282 21 7%
Balochistan 3
15. PRL Quetta Bolan
Medical Complex Public 236 76 32%
TOTAL 1688 18%
Proposed, 2013
FATA 5
AJK 1
GB 1
TOTAL (2013) 42
(Source: NTP Draft Annual Report, 2012)
5.13.13 Infection control services
Acquisition of TB among health care workers as well as hospital-based outbreaks of MDR-TB is
known. The risk is high in Pakistan, where the disease burden is considerable and the quality
infection control services are non-existent. It is known that with simple and inexpensive TB
control measures disease transmission can be reduced considerably. The NTP has given its
policy guidelines on implementing control of TB transmission in health care setting at three
levels.
a) Administrative control; which will reduce health care worker and patient exposure to
infection
b) Environmental control; which will reduce the concentration of infectious droplet nuclei
c) Personal respiratory protection; which will protect health care workers in areas where
the concentration of droplet nuclei cannot be adequately reduced by administrative and
environmental controls.
A comprehensive infection control plan has been launched in line with GF-9 grant. In the first
phase 10 facilities will be completed by mid 2013. The second batch of 8 facilities have been
assessed and work is currently in process. A total of 30 sites will be up-graded by the mid of

94
2014. At the meantime, DR management has already started in some of these sites while
infection control upgrading is going on.
The hospital facilities shall be upgraded keeping Infection Control Principals in view and this
process includes establishing waiting areas separately for MDR Patients, improvements in
Milieu Interior of hospitals including Out-patient departments, MDR wards, X-ray department,
Procedure & Bronchoscopy suites, XDR rooms with Installations of HVAC units where ever
required.
5.13.14 Social support services
TB patient compliance to treatment both in sensitive and drug-resistant TB is a known problem.
In the case of treatment for DR-TB the patient has to take the medicine and injectables for two
years which is a significant challenge, not only for the patient but also for the care
givers/families who are supporting him/her in this treatment. Keeping in view the above stated
factors, and to enhance the compliance of patient to treatment, the NTP is offering social
support to DR-TB patients as well as their treatment supporters.
Each DR-TB patient is provided with a “food basket coupon” and “travel reimbursement” on
his/her monthly follow-up visit to the hospital. The patient is initially hospitalized for 1-2 weeks
if indicated and after that the patient is managed on an ambulatory base with the help of a
treatment supporter and visits the hospital for follow up (clinical & lab evaluation and provision
of medicine) on monthly basis. The NTP is providing social support package (essential food
items) to patient and treatment supporter on their monthly visit to treating hospital. In addition
to the social support package, the DR-TB patient is also provided with travel expenses. The
social support packages are procured from utility stores and provided to patients and treatment
supporters through peripheral outlets.
The social support provision has definitely enhanced treatment adherence and reduced the
number of “lost to found” cases. In view of this, NTP plans to continue this support to DR TB
patients in future also.
Currently, the social support program in Pakistan contains:
a) Each patient receives a monthly food basket, which costs today $22.88, and travel
incentive of $6.53.
b) Each Treatment Supporter receives also a monthly food basket (same value as above)
with no travel incentive.

95
5.13.15 MDR- training
The NTP has currently conducting training for the following categories at various PMDT sites
and districts through the implementing SRs. The NTP has initially trained master trainers from
the national and provincial programs and partners who are responsible for scale-up trainings.
Table 39:Category and training days for DR-TB
Sr.No. Category of training Training Days Average Batch size
1. Professors, senior registrar and registrar 2 5 participants
2. Doctors 6 10
3. Paramedics 4 15
4. Treatment Supporter 2 15
5. Data Management 4 10
6. SLD Management and Warehousing 4 25
5.14 PUBLIC-PRIVATE MIX 5.14.1 Overview
In most resource-poor countries with a high TB-burden, patients with symptoms suggestive of
tuberculosis (TB) seek care from a wide array of health-care providers. These care providers,
often not linked to National Tuberculosis (NTP), serve a large proportion of TB suspects. The
size, types and roles of these care providers vary greatly within and across countries. In some
settings, there is a large private commercial sector and numerous non-governmental
organizations (NGOs) while in others there are public sector providers (such as general and
specialized hospitals) that operate outside the scope of NTPs. Evidence suggests that failure to
involve all care providers used by TB suspects and patients hampers case detection, delays
diagnosis, leads to inappropriate and incomplete treatment, contributes to increasing drug
resistance and places an unnecessary financial burden on patients. Engaging all relevant health
care providers in TB care and control through public-private mix approaches is an essential
component of the World Health Organization's (WHO's) Stop TB Strategy. Currently, nearly all
high TB burden countries are implementing PPM activities and it is one of the priority strategic
areas of Stop TB plan 2006-2015.

96
Reports from countries and several project evaluations have shown that PPM has supported in
increasing case detection (between 10% and 60%), improving treatment outcomes (over 85%),
reaching the poor and saving costs. Effective PPM could help NTP in detecting and curing all TB
cases, not just 70/85 and progressing from "care" to "cutting transmission".
Tremendous progress has been made in Pakistan for tuberculosis control in recent years
through implementation of DOTS. It has been acknowledged that TB control efforts are
impressive but, not sufficient. The CDR remains 63% means missing at least 37% of the patients.
As in most countries with a significant burden of TB, DOTS implementation is limited largely to
public sector services under national tuberculosis programs (NTPs). In reality, however, many
patients with symptoms of TB, including the very poor, do seek and receive care from a wide
variety of health care providers outside the network of NTP services mostly not following
National Guidelines. Thus the TB patients they serve are deprived of the benefits of DOTS and
poses an obvious risk of drug resistant TB.
5.14.2 NTP/PTP model of PPM
Since 2010, the NTP/PTPs, in collaboration with its partners, are implementing a district led
model of PPM in almost 50% of Pakistan i.e. 62/133 districts in five provinces of Pakistan, AJK
and ICT. This initiative is supported by the Global Fund, with Mercy Corps as the Principal
Recipient. The NTP/PTPs are planning to expand the model of PPM to the entire country by
strengthening current partners and bringing more partners into PPM. The figure below
presents the key features of the NTP/PTP model of PPM.
There are basic six types of models24 which exist currently under the PPM and are contributing
in increasing case notification and treatment success.
1. District led model: The model has the main stewardship with the district health
authorities, District TB coordinator has a pivotal role . All the TB related activities and
implementation is done through the public sectors. The NGO supporting the project has
mainly a role of coordination between the GPs and the Public sector, providing logistics
for the project and organizing community awareness activities.
2. NGO led model: The model is experienced mainly in Punjab where Pakistan Anti TB
association has a large network which mainly provide TB care, self operated , supported
by local philanthropists. The AKHSP is working in GB and MALC is operational with few
centers in Sindh.
24
NTP Pakistan, National Guidelines for Public Private Mix in TB-DOTS
97
3. Social franchising: Franchise network of Green Star Social Marketing and 1000 GPs are
engaged mainly in five metropolitan cities.
4. Large private hospitals: Includes large private hospitals and private Tertiary Care
Hospitals e.g (Gulab Devi and Indus). The large private hospitals are engaged with PTPs
which directly supervises the TB DOTS implementation, provides drugs & trainings, and
generates quarterly reports e.gGhurki trust hospital, Bethania hospital etc
5. Parastatal Model: Includes Social Security, Faujifoundation ,Wapda, Railways
Cantonment hospitals and other Parastatal in all the four provinces of Pakistan
6. Engagement of Pharmacies in TB control : This has been piloted in four large urban cities
of Pakistan to develop referral linkages between pharmacies and service delivery points.
For the purpose of this document, the six models are grouped as:
a) Public- private i.e. between NTP/PTP and the private sector (mainly non-government
organizations ‘NGOs’ hospitals, private hospitals, GPs and private hospitals and health
centers)
b) Public-public i.e. between NTP/PTP and other public sector hospitals (Teaching/Tertiary
and general hospitals, prison and social security organizations)
There are other key organizations and settings in the country which can play a potentially
significant role in fight against TB both in urban and rural settings. This includes;
- Armed forces hospitals
- PRSP/PPHI (managed primary health care facilities in the rural settings)
- Pharmacies
- Workplace TB care
PPM also implies engaging relevant care providers in prevention and management of MDR-TB
and in the implementation of TB/HIV collaborative activities, which the NTP is considering to
implement. The potential role of PPM in MDR and TB/HIV is discussed in the relevant sections.
5.14.3 PPM guideline and materials
The NTP has developed a set of materials and guidelines to structure the delivery of TB care
through PPM. The materials include;
- National Guidelines for Public Private Mix in TB-DOTS
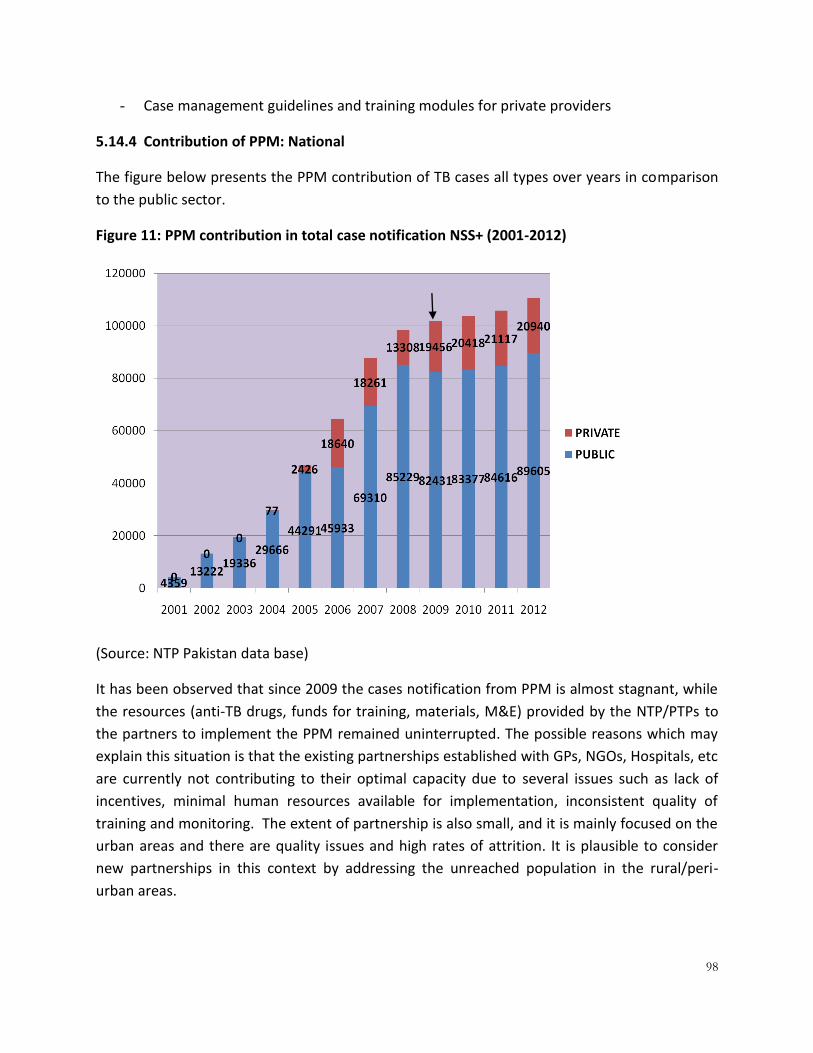
98
- Case management guidelines and training modules for private providers
5.14.4 Contribution of PPM: National
The figure below presents the PPM contribution of TB cases all types over years in comparison
to the public sector.
Figure 11: PPM contribution in total case notification NSS+ (2001-2012)
(Source: NTP Pakistan data base)
It has been observed that since 2009 the cases notification from PPM is almost stagnant, while
the resources (anti-TB drugs, funds for training, materials, M&E) provided by the NTP/PTPs to
the partners to implement the PPM remained uninterrupted. The possible reasons which may
explain this situation is that the existing partnerships established with GPs, NGOs, Hospitals, etc
are currently not contributing to their optimal capacity due to several issues such as lack of
incentives, minimal human resources available for implementation, inconsistent quality of
training and monitoring. The extent of partnership is also small, and it is mainly focused on the
urban areas and there are quality issues and high rates of attrition. It is plausible to consider
new partnerships in this context by addressing the unreached population in the rural/peri-
urban areas.

99
Figure 12: Case notification: Public - Private 2012
(Source: NTP data base)
Figure 13:PPM CONTRIBUTION NSS+ –ALL PROVINCES (Q1 2013)
5.14.5 Contribution of PPM: Province wise
The figure below presents the province wise contribution of PPM. It has been observed that
most of the case notification is coming from the province of Punjab where the most number of
partnerships currently exits whereas, the contribution from Balochistan is almost negligible
18%
67%
2%
13% 17%
74%
1%
8%
0%
20%
40%
60%
80%
KPK Punjab B,Tan Sindh
NSS+ All
Public 89605 (81%)
Private 20940 (19%)
NSS+
Public Private
Public 228122 (80%)
Private 57288 (20%)
All Type
Public Private

100
where the partnerships are also few. One possible reason for limited partnerships in
Balochistan is due to its geography, which is mostly rural and difficult to access areas.
Innovations are required in Balochistan to increase the number of partnerships so that PPM
contributions to increase the case notification can get visible.
Figure 14: Province wise PPM contribution: TB new sputum smear positive cases/ all types
(Source: NTP Pakistan data base)
5.14.5.1 Public- Private
The partnership is between NTP/PTPs and the private sector. This constitutes those health
centres which are either private sector owned or public sector health centres being managed
by the NGOs. These are mainly outdoor facilities, but few centres also have admission facilities
available. Moreover, it constitutes private hospitals most of which are specialized TB hospitals
or have a TB unit with both indoor and outdoor facilities and General practitioners (GPs)
Existing partners:
Four main networks of non-government partners ‘NGOs’ which are currently offering TB
services under NTP/PTP partnership are:
- Pakistan Anti-TB Association (PATA)
- Aga Khan Health Services Pakistan (AKHSP)
- Marie Adelaide Leprosy Center (MALC)
- Private sector hospitals

101
Punjab (6):GulabDavi, Marie Adelaide Leprosy Hospital, GTH, FMH, AllamaIqbal Memorial
Hospital, Bethania Hospital
Sindh (7):FatemaBaqai Hospital, Shoukat U Hospital, Sir Syed Medical University & Hospital,
Indus Hospital, Bantwa Hospital, Murshid Hospital, Kharadar Hospital
Balochistan (1):Al Shifa Hospital
KPK(4): Mission hospital (2), Kuwait Hospital, Kai Hospital,
(Source: NTP consolidated data, 2012)
- Clinics run by General Practitioners (GPs)
- Laboratories in major cities
Number of GPs
The table below shows the number of GPs involved in each province and regions of Pakistan.
Table 40: GPs involved in TB care by province, 2013
PROVINCE GPs
ENGAGED REPORTING
AJK 52 8
BALOCHISTAN 124 28
FATA (FR/AGENCY) - -
GB 34 -
KPK 213 160
PUNJAB 1130 527
SINDH 669 442
ICT 22 14
PAKISTAN 2244 1179

102
Arrangements:
The PATA has a countrywide network of 83 diagnostic centers (basic TB management unit),
whereas AKHSP runs a network of 24 diagnostic and 48 treatment centers in various parts of
the country. The MALC has about 15 centers, mainly in Karachi and Sindh. In addition, MALC
also supports DOTS in about 140 public sector centers mainly in Azad Jammu Kashmir and
Northern areas of Pakistan. The NGO partners manage staff inputs as well as facility operations
for TB care through their own resources which includes anti-TB medicines and microscopy. The
NTP/PTP contributes by supplementing anti-TB medicines for routine cases and laboratory
supplies, print materials and monitoring support. The non-government partners do face
challenges in sustaining the inputs and operations in the absence of additional project
resources.
For GPs: The NTP/PTPs are providing anti-TB drugs, trainings and monitoring and surveillance
support. The private partners are managing their centres with their human resource,
infrastructure and laboratory equipment and supplies. They are in compliance with the NTP
policy of providing free drugs and sputum smear microscopy to TB patients.
Through support from the Global Fund under the SSF grant, the PPM model is currently being
implemented in 62 districts including 5 metropolitan cities. Mercy Corps is the principal
recipient for this grant with six NGOs implementing the PPM model in these districts which
include; Green Star Marketing (GSM), Bridge, PYLC, Association for Community Development
(ACD), Association for Social Development (ASD) and Mercy Corp (MC).
In the PPM model there are solo laboratories attached with the private hospitals, which are
strengthened to support the GPs in diagnosing TB. The Private labs are enabled through GF
support and are linked with GPs to provide diagnostic support at subsidized rates.
Contribution:
The PATA is currently reporting from its 51/83 health centers [Punjab (34), Sindh (5), KPK PATA
(12) and Anti-TB association Geneva (3)] whereas, AKHSP is reporting from 21 of its health
centers [(Punjab (4), Sindh (9), KPK (8)]. The annually register about 11,000 and 500 smear-
positive TB cases, with treatment success rate of 90% or more (i.e. about 11% and 0.5% of
national registration respectively). MALC centers [(Sindh (11), KPK (2)], Dioces of Hyderabad [(
Sindh (4)], Bahbood Association [(Sindh (2)], register and treat about 3,500 new smear-positive
cases each year (i.e. about 3.5% of national registration). Based on the ongoing experience, this
sector is currently managing about 15% of the registered new smear-positive TB patients (NSS+)
in the country.
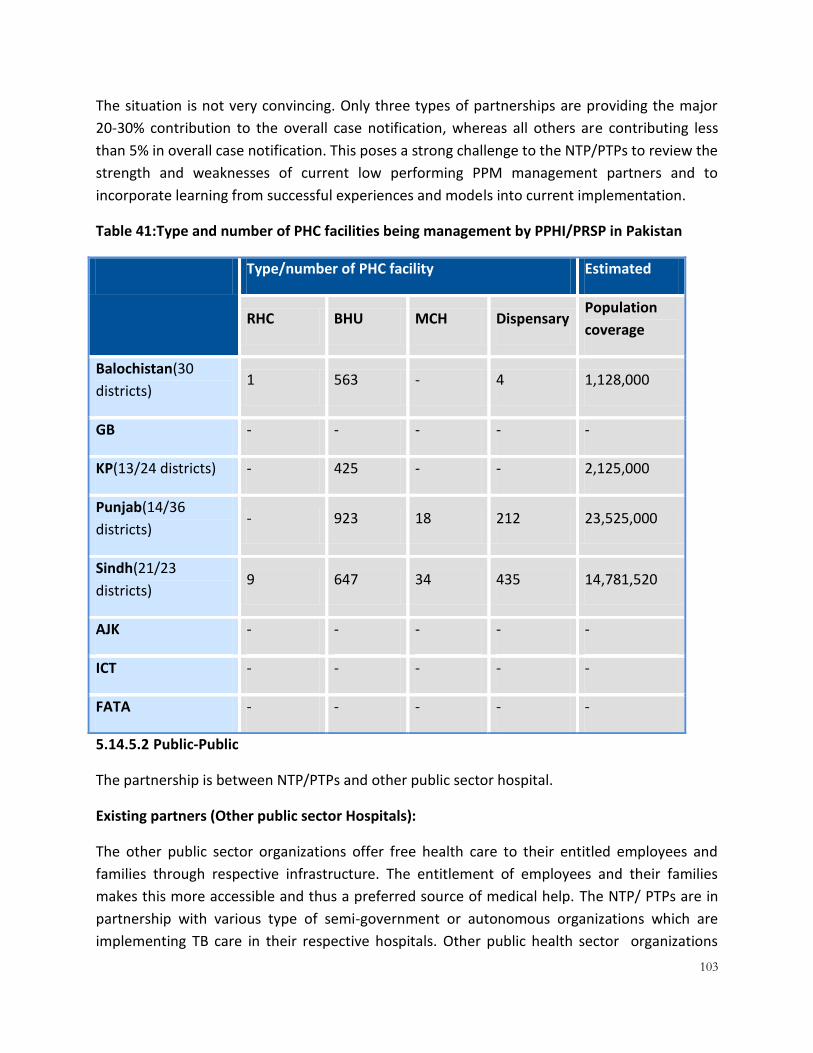
103
The situation is not very convincing. Only three types of partnerships are providing the major
20-30% contribution to the overall case notification, whereas all others are contributing less
than 5% in overall case notification. This poses a strong challenge to the NTP/PTPs to review the
strength and weaknesses of current low performing PPM management partners and to
incorporate learning from successful experiences and models into current implementation.
Table 41:Type and number of PHC facilities being management by PPHI/PRSP in Pakistan
Type/number of PHC facility Estimated
RHC BHU MCH Dispensary Population
coverage
Balochistan(30
districts) 1 563 - 4 1,128,000
GB - - - - -
KP(13/24 districts) - 425 - - 2,125,000
Punjab(14/36
districts) - 923 18 212 23,525,000
Sindh(21/23
districts) 9 647 34 435 14,781,520
AJK - - - - -
ICT - - - - -
FATA - - - - -
5.14.5.2 Public-Public
The partnership is between NTP/PTPs and other public sector hospital.
Existing partners (Other public sector Hospitals):
The other public sector organizations offer free health care to their entitled employees and
families through respective infrastructure. The entitlement of employees and their families
makes this more accessible and thus a preferred source of medical help. The NTP/ PTPs are in
partnership with various type of semi-government or autonomous organizations which are
implementing TB care in their respective hospitals. Other public health sector organizations

104
offering health services include: railways, social security, Fauji Foundation, army, police, prisons
etc. About 10 million (i.e. 6%) of the country population is covered through other public sector
health services.
The National TB Control Program has already established partnership with four other public
sector institutions i.e. Social Security, Railways, Fauji Foundation and prisons. In first phase,
total 29 hospitals run by three institutions and a network of prison health facilities in all parts of
the country are enabled to provide quality care to the population of about 8.5 million people.
This has improved the access to quality DOTS care for about 5% of the country population,
benefiting about 10,000 TB patients each year. In subsequent years, further expansion will be
planned in light of these experiences.
Currently following other public sector hospitals are working under PPM model in various
provinces:
Punjab (8): Railway Hospital Lahore, SSH Shadara Lahore, SSH Rawalpindi, Railway Hospital
Rawalpindi, SSH Sialkot, SSH Gujranwala, SSH Multan, PESSI Lahore
Sindh (4): Railway H Kch, Railway H Sukkur, SESSI ValikaKch, SESSILandhiKch
Balochistan:
KPK: (10): Cant General, F.GovtHospt, Jail Haripur, Jail Peshawar, Police Hosp, Railway Hosp,
SS Hosp, WapdaHosp, PTCL, Fouji Foundation
Table 42: Type and number of facilities: Armed Forces
Type/number of Hospitals Estimated
CMH PAF PNS MH Population coverage
Balochistan 4 - - -
GB 2 - - -
KP 12 - - -
Punjab 14 2 - 1
Sindh 6 2 2 -

105
AJK 2 - - -
ICT - 1 1 -
FATA - - - -
National (TOTAL) 40 5 3 1 620,000 (active
personnel)
Table 43: Type and number of facilities: Fauji Foundation
Type/number of Hospitals/H.F OPD cases
Urban Semi-
Urban Rural
Medical
centers/Disp
Outdoor patients
(2012)
Balochistan - - - 2 47,292
GB - - - 2 34,344
KP 1 - 1 10 236,033
Punjab 2 5 1 29 1,377,893
Sindh 1 - 1 11 415,969
AJK - - - 2 21,936
ICT - - - - -
FATA - - - - -
National (TOTAL) 2,133,467

106
Table 44: Type and number of facilities: Social Security
Hospitals Medical centers/other
Balochistan - -
GB - -
KP 1 28
Punjab 11 -
Sindh 4 5
AJK - -
ICT 1 -
FATA - -
National (TOTAL) 17 33
5.15 DRUG MANAGMENT The National and Provincial TB Control Programs provide uninterrupted, quality-assured, and
free of cost anti-TB drugs to every enrolled patient in the county. The NTP with the support of
the Global Fund is implementing a multi-dimensional program to procure essential anti-TB
drugs, upgrade and refurbish national, provincial and district warehouses, train public and
private healthcare providers on TB Drug management and strengthen the drug management
information system for TB across the country.
5.15.1 Operational Arrangements
At NTP, a Drug Management Unit has been established looking after all anti-TB drugs (FLDs,
SLDs, Ancilliary drugs) management related issues including procurement and storage,
distribution, correspondence with partners and implementers, monitoring & implementation of
TB-DMIS and developing and implementing drug management guidelines across the country.
Drug Management Unit ensures the implementation of a TB pharmaceutical management
system which involves four basic functions: selection, procurement, distribution, and use.
107
5.15.2 TB Pharmaceutical Management (Drug Management) Cycle:
Selection involves choosing high-quality TB medicines, appropriate dosage forms (e.g., fixed-
dose combination [FDC] medicines) and appropriate packaging, such as patient kits. The TB
drugs are included in the Pakistan national essential medicine list and registered in the country.
ATT medicines are selected in accordance with the latest National Model List of Essential
Medicines, particularly in the form of FDCs, and the latest TB treatment guidelines for National
TB Control Program.
Quantification and forecasting of ATT drugs is based on case notification. However, other
factors are also taken into consideration like available stock position, consumption pattern,
expiry of the drugs and supplies in pipeline.
Procurement of ATT medicine are ensured through selecting appropriate procurement
methods, managing tenders, establishing contract terms, ensuring adherence to those terms,
and assuring pharmaceutical quality. At federal level through donor supports NTP procures
selected medicines through WHO / GDF mechanism from manufacturers and suppliers whose
products meet the WHO prequalification program standards to ensure transparent and cost-
effective procurement of quality goods and services. Provinces procure ATT drugs from their
provincial allocations as per the rules set forth by Provincial Procurement Committee.
Storage & Distribution: The procured medicines are distributed to the service delivery points on
time and in the right quantity, to ensure proper inventory control, and stored under the
recommended storage conditions.
Storage: One of the considerable achievements of the NTP, under Round-8 GF Grant, was a
successful refurbishment of its warehouses and stores across the supply chain. To achieve
optimal storage conditions, the NTP has provided and installed the supplies mandatory for a
warehouse or a store’s conducive environment i.e. Air-Conditioner, Pallets, Racks, Exhaust Fans,
Hygrothermometer, fire-extinguisher etc. to all the 141 warehouses across the country (that
include central, provincial/ regional and district stores).
Currently all the drugs (FLDs, SLDs, Ancillary & Pediatric) and laboratory supplies are stored at
the central, provincial, district and MDR sites’ warehouses/ stores. At the Central level, the NTP
has leased a warehouse, with sufficient storage space up to ten thousand square feet and
where WHO recommended good storage practices are being followed, to house all TB Drugs.
Distribution and supply mechanism:
The FLDs are supplied with standard blister and defined pack size hence does not require any
re-packaging while distributing further to provinces/ districts.

108
These TB drugs are then distributed to each Provincial and Regional TB Control Program
according to the need communicated by the respective PTPs/ RTPs to NTP.
The consignment from supplier arrives at the NTP central warehouse, where physical inspection
is done; quantities are verified and recorded for inventory management. All relevant
information like supplier name, quantity, batch wise information, shelf life etc are properly
entered in store stock register and samples are collected for quality testing. The stock is then
delivered to the Provincial and Regional warehouses, as per their requirements where the
drugs are stored and distributed to districts based on their consumption pattern along with
observance of case notification and stock positions. District stores followthe same practice of
supply to Basic Management Units (BMUs), both in public and private sectors. However, to
cater the special needs of those private sector providers which are linked with some network
like Greenstar’sGoodLife program, the drugs are provided to the organization for onward
distribution to its network providers.
Flow chart showing distribution of drugs from Central Warehouse up to the end user:
From Central warehouse to provinces/ districts the drugs are distributed /supplied by road;
however, quite a few items (SLDs) are distributed by air. The drugs are then transported
through official vehicles from districts to SDPs.
For the transportation of commodities, NTP on annual basis solicits bids from Goods
Forwarding Agencies, through open competitive bidding procedure and in the bid document it
is clearly outlined that, “complete and secure transportation of commodities is the
NTP
Central
warehous
e
Provincial/
regional
Warehouses’
Districts Drug stores
Public Health Facilities
Private Care Providers and institutions(e.g. GS)
TB Patients

109
responsibility of Goods Forwarding Agency, failing to which the agency is liable to reimburse
NTP for the total cost of commodity (s) in case of damage, theft or loss”.
Also NTP has procured 5 mini loader trucks installed with special containers for transportation
of program drugs and other commodities. The truck at Central Warehouse would be used for
transportation to Provincial / Regional Warehouses of KP, AJK and FATA, whereas,
transportation to Punjab, Sindh, GB and Balochistan would be done through hiring of services
of GFA. Keeping in view the large quantities of ATT drugs to be transported and large
geographical spread, NTP would need more such loader trucks for transportation both at
central as well as provincial level.
Usage includes diagnosing, prescribing, dispensing, administration, and proper consumption by
the patient. Each function builds on the next, forming the pharmaceutical management cycle.
Then, correct medicines are ensured to be given to TB patients in correct dosages to maximize
their efficacy. TB patients are encouraged to take their medicines for the prescribed periods
through direct observation to achieve cure by adhering to the treatment protocol and to
prevent the development of multidrug-resistant tuberculosis.
5.15.3 Securing Funding for ATT Drugs Up till 2015:
NTP is detecting and treating about 274,000 cases annually. NTP as a regulatory body is
mobilizing resources for the provision of quality assured drugs free of cost to the patients.
Global Fund has been supporting NTP Pakistan to bridge the financial gaps through R-2, 3, 6, 8
&9 grants. R-8 grant primarily has been awarded to bridge the funding gap of first line drugs
(FLDs). GF commitment for FLDs through R-8 grant had been for 50% of country needs. The
contribution reduced to a cumulative of 33% during phase-2 approval (year 2011-2014) with
the understanding that this gap will be addressed while consolidating the TB grants in the
country. Based on successful implementation of the R-8 grant NTP is able to secure more than
60 Million USD for the procurement of FLDs and SLDs in SSF budget.
FLDs additional support of 8 Million:
As per WHO guidelines to avail 100 buffer stocks of FLDs across the supply chain; Drug
Management Unit has done a comprehensive gap analysis of FLDs in country and on the basis
of this gap analysis successfully able to get additional grant of 8 million USD from Global Fund
and became the first country to get GF interim funding.
WHO Emergency Grant of 7 Million:
In collaboration with World Health Organization and Stop TB Partnership Geneva, NTP / DMU
has conducted a GDF review mission in year 2013 to assess the activities of Drug Management.
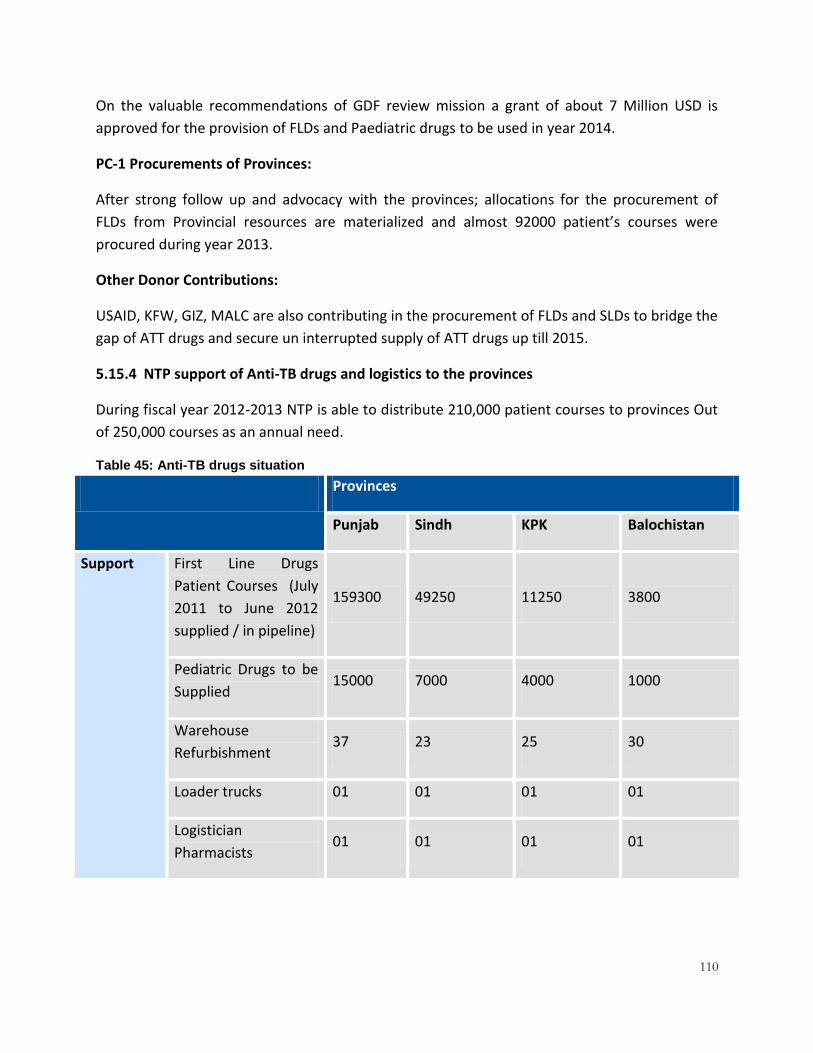
110
On the valuable recommendations of GDF review mission a grant of about 7 Million USD is
approved for the provision of FLDs and Paediatric drugs to be used in year 2014.
PC-1 Procurements of Provinces:
After strong follow up and advocacy with the provinces; allocations for the procurement of
FLDs from Provincial resources are materialized and almost 92000 patient’s courses were
procured during year 2013.
Other Donor Contributions:
USAID, KFW, GIZ, MALC are also contributing in the procurement of FLDs and SLDs to bridge the
gap of ATT drugs and secure un interrupted supply of ATT drugs up till 2015.
5.15.4 NTP support of Anti-TB drugs and logistics to the provinces
During fiscal year 2012-2013 NTP is able to distribute 210,000 patient courses to provinces Out
of 250,000 courses as an annual need.
Table 45: Anti-TB drugs situation
Provinces
Punjab Sindh KPK Balochistan
Support First Line Drugs
Patient Courses (July
2011 to June 2012
supplied / in pipeline)
159300 49250 11250 3800
Pediatric Drugs to be
Supplied 15000 7000 4000 1000
Warehouse
Refurbishment 37 23 25 30
Loader trucks 01 01 01 01
Logistician
Pharmacists 01 01 01 01
111
5.15.5 Guidelines and materials
NTP Drug Management Unit has developed the following guidelines providing details of
selection of medicines, their quantification, procurement, storage, distribution and usage
across the supply chain:
1st line and 2nd line anti-TB Drug management guidelines
Drug dispensing manual
Standard operating procedures (SOPs) for pharmaceutical management
Quality assurance plan
5.15.6 Drug Management Information System:
The Drug management information system (DMIS) serves as the engine for supply chain
management programs. A functioning DMIS is the key to programmatic success. Accessing web-
based technology to enhance DMIS timely reporting and accuracy creates the ability to make
prompt supply decisions using accurate data.
Fully functional and developed TB DMIS is being developed and handed over to NTP by Green
Star through GF funding; TB DMIS training across the country and accordingly implementation
national/provincial/district level are in progress to develop a pool of skilled personnel for
smooth functioning and execution of this task.
NTP management is confident that with the implementation of TB DMIS, robust analysis of
inventory management, consumptions patterns of drugs, monitoring stock outs, over stocking
and timely availability of precious drugs to patients will be done on regularly basis.
5.16 ACSM Government of Pakistan declared Tuberculosis as National emergency in year 2001. National TB
Control program piloted and started implementation of DOTS strategy across the country
through public sector health facilities. ACSM has been an integral component of the TB control
program right from the beginning of the program but gained momentum in year 2005 when
100% DOTS coverage in public sector was in place. NTP secured funding from Global Fund
through R-2 grant and a full fledge ACSM component was implemented in selected districts of
the country which included development of Behaviour change strategy (BCC). Latter in R-6
funding from GF was secured for ACSM strategywhich included mass media communication,
social mobilization and public relations.
The strategy primarily addressed following areas:

112
Public awareness regarding sign and symptoms of TB through mass media and inter-
personal communication
Public awareness regarding availability of TB management services highlighting TB brand
Advocacy with policy makers including parliamentarians
Establishing consistent brand identity of NTP and engaging a celebrity as TB
ambassador.
Installation of billboards in cities promoting NTP brand
Patient empowerment by establishing patient groups in the districts
Establishment of NTP resource centre
NTP, Pakistan is being recognized as a leader on producing high quality advocacy,
communication and social mobilization products. NTP/ACSM Unit has further modeled Public-
Public and Public-Private partnerships with a number of institutions related to health sector in
the country. The activities conducted in last two years with the support of GF are as under:
Table 46: ACSM activities status Serial # Activity Total conducted/
trained
1 Number of community based ACSM events (theatre, music, drama, etc) conducted
7,694
2 Number of Journalists oriented/ trained 29,195
2.1 Articles published/ ACSM activities coverage 2,263
3 Orientation of Advocates (policy makers, opinion leaders, key influencers)
81,544
4 No. of Community coalitions meetings held 1,945
5 No. of service providers trained in inter-personnal communication (including district level health care providers i.e. LHWs, DOTS facilitators)
81,808
6 Number of healthcare providers trained on quality assurance for interpersonal communication
61,516
7 Number of National Steering Committee meetings conducted
11
8 Number of Provincial Steering Committee meetings conducted
10
9 Number of capacity building session with TB Patients at Provincial level
25
113
10 Number of quarterly meetings with EDOs & NPOs 4
11 Number of TV spots aired 1,759
12 Number of Radio spots aired 2,384
13 Capacity building workshops As per requirements
In addition, NTP ACSM Unit as well as Principal Recipient and implementing partners have
conducted several capacity building workshops, and advocacy meetings and seminars with
media and other stakeholders.
5.16.1 Stop TB Partnership Pakistan
Stop TB Partnership Pakistan, established with the assistance of Stop TB Partnership EMRO, is
chaired by the Vice Chancellor, Dow University of Medical Sciences, Karachi. The partnership is
holding meetings at regular intervals.
5.16.2 World TB Day
World TB Day has been commemorated every year on March 24th. Every year National TB
Control Program (NTP) designs and implements a number of activities to commemorate World
TB Day on March 24 in line with Stop TB Partner Ship theme.
5.16.3 Results of the mid-term evaluation of ACSM
Independent international and national consultants were commissioned to conduct a mid-term
evaluation of the Mercy Corps intervention districts. Empirical results from a multistage,
random sample of populations in the intervention districts identified a number of significant
findings. Participant recall of TB was considerable with 64.6% recalling any TB information
without prompts, while 31.4% specifically recalled the TB brand following prompting.
Comparisons of knowledge, attitudes and practices (KAP) of participants aware of TB
information (AwareTBinfo) vs. those that were unaware of TB information (UnawareTBinfo)
found AwareTBinfo participants to have significantly better knowledge than their
UnawareTBinfo counterparts (p< .01).
5.17 MONITORING, EVALUATION, RESEARCH AND LEARNING (MERL) 5.17.1 Overview of M&E
The NTP/PTPs has an efficient M & E and supervision system in place, which is the backbone to
maintain the quality of TB services in the country. The NTP has developed structured approach
to M & E by developing monitoring and supervision module/ tools. They are conducting regular
surveillance meetings at national, provincial and district levels. In additional there are annual

114
program reviews, internal and third party evaluations, online laboratory data management
system and electronic reporting system – piloting started, followed by countrywide expansion.
The human resource to perform the M & E function at National level it includes; Full-time M & E
officers/ filed officers/ program officers, National Program Officers (NPOs) at regional level and
Senior Laboratory Supervisor (SLS) at regional level. At the provincial level it includes; Full-time
Provincial Program Officers and Medical Officers and Laboratory Supervisors and at district level
it includes; Designated District TB Coordinator (DTC) and Full-time District Laboratory
Supervisor (DLS).
Except the DTC, all other M& E staff is supported from donor supports in which Global Fund has
the major contribution.
Figure 15: System of M&E operations in the country LEVEL ACTIVITY
NTP
PTPs
DISTRICTS
BMUs
The above system is all based on the donor support mainly from Global Fund.
Note: The other Components i.e. Effective Drug Supply and Management, Childhood TB,
Difficult to Diagnose TB, TB-HIV Co-infection and ACSM are covered as separate sections.
5.18 OPERATIONAL RESEARCH Research is a key strategic area identified in the National strategic and operational (PC1) plans
as well as the new stop TB strategy. The strategy describes operational research as a core
component of NTP work. Designing and conducting locally relevant operational research can
help in identifying problems and workable solutions, testing them in the field and planning for
the scaling up of activities.
Inter-Provincial Meeting held by 07th day of the SECOND
month following end of Qtr.
Inter-District Meeting of all DOTS Districts of the Province held
by 25th day of the month following end of Qtr.
Intra-District Meeting of BMUs held by the 15th day of the
month following end of a Qtr.
BMU record data in TB Register. At the end of the Qtr. compile
& complete Forms 07,08& 09

115
There are several objectives which include:
- To provide research leadership to establish National research/development
agendas, attracts resources, new researchers and research groups, and develops
Institutional networks.
- Provide management capacity for carrying out specific research projects to ensure
relevance, quality, timeliness, efficiency and accountability.
- Develop critical mass of personnel with up-to-date R&D skills.
- Enable the means and opportunities for participating in international R&D.
- Develop road maps for new researches based on need and priority of NTP.
- Develop collaborations with international academic institutes to perform
international standard quality research.
Arrangements
The NTP has a well organized Research Unit in place. In last few years NTP has designed and
implemented several OR projects and national level surveys on priority program needs.
Contribution
Below is the list of few significant contributions of Research Unit in last few years.
5.18.1.1 National TB prevalence survey
The National TB prevalence survey was completed in Dec 2011/12. The final report has been
published and shared with stakeholders on the 24thMarch, 2014.
5.18.1.2 Capture re-capture project
Between 1st January 2012 and 31st March 2012 a capture re-capture project was carried out by
NTP. The study aim was to determine TB Disease Burden and to observe TB case management
practices of public and private non-NTP providers in the 12 selected districts as part of a
strategy of the National TB Control Program to create additional data sources for improving
case notification. The study was done in parallel to the Disease Prevalence survey and was of
tremendous importance which showed 28% under-reporting in the study only 32% of cases
were found registered with the NTP which opened up the need to engage private providers on
priority with the program to enhance TB case notifications. The results of the study are will be
published in international Journal.

116
5.18.1.3 TB REACH Wave 1
The project was completed in 2011-12 and a total of 3117 tuberculosis positive cases were
detected; 1707 through chest camps and 1410 from GPs clinics. During the project, the total
number of smear positive TB notification rate increased 226% progressively from chest camp
intervention over the intervention period. The project was proven to be very successful
receiving an A Grade in international monitoring and it is has been recommended that these
same activities be replicated in other hard to reach areas of the country.
5.18.1.4 TB REACH Wave 2
Recently a study to test the “Effectiveness of widening the circle of contact screening from
within the household to 100 m around the house of index case on case finding through
outreach using GIS” has been launched. The project introduces active contact investigation in
four cities. Household contacts, i.e. those normally resident or sharing the same airspace, will
initially be verbally screened, followed by screening of a wider circle of close community
contacts. The project will use Gene-Xpert among smear negatives TB cases and chest X-ray
suggestive of TB.
5.18.1.5 Indus hospital project TB REACH
In Karachi Indus Hospital used community laypeople, mobile phones, and awareness campaigns
to screen ~500K people at 54 private clinics and a large hospital. The results demonstrated that
case detection doubled in one year and the Indus hospital became the second largest reporting
center in Pakistan. The control area saw no significant change in TB case notifications.
(Source: Aamir J Khan, et al; Engaging the private sector to increase tuberculosis case detection:
an impact evaluation study)
5.18.1.6 Enabling pharmacies in TB control
Private sector pharmacists are a crucial partner in increasing the number of people who are
properly diagnosed and treated for tuberculosis (TB). Pharmacists often have close ties to the
community and frequently serve as the first point of contact with the health system. It has been
reported that private markets in four countries i.e. Pakistan, the Philippine, Indonesia and India
had the largest relative sales volumes; annually, they sold enough first line TB drugs to provide
65-117% of the respective countries annual incident cases with a standard 6-8 months regimen
(Source: William.A.Wells, et al; Size and usage pattern of private TB drug market in the high
burden countries). This calls for appropriate policy and market response i.e. expansion of PPM,
greater reach, flexibility, regulatory and quality enforcement, etc. The figure below presents the
percentage of anti-TB drugs sold in the private market.

117
Figure 16: Percentage of anti-TB drugs sold in private market
(Source: Global Alliance for TB Drug Development, Annual Report, 2009)
Recently the NTP, in collaboration with Pakistan Pharmacists Association and DEV-NET,
supported by USAID-funded initiative of “Engaging Pharmacists in TB Care and Control in
Pakistan”. Pharmacists have historically been underutilized in TB prevention and care. An
impact evaluation study in Pakistan found that training laypeople in the community to screen
for TB in private clinics and then linking patients to free diagnosis and treatment from a NTP
approved private facility was one of several interventions that increased case detection two-
fold over that observed in the control area. However, Pakistan cannot afford to ignore retail
pharmacies in TB control, given their ease of accessibility, presence of few qualified staff, and
lack of knowledge of both TB and the NTP. The NTP can benefit from engaging private
pharmacies for rationale use of drugs (good prescribing habits), screening & referrals (case
detection), supervised treatment, counseling, education and awareness.
0
20
40
60
80
100
120
140
Drugs sold in the private market
65
%

118
5.19 HUMAN RESOURCE DEVELOPMENT Health services cannot be delivered effectively and efficiently without trained human
resources. Attaining, training and retaining of human resource are challenges in developing
countries.
The table below presents the NTP/PTPs recommended category of core staff in each district to
be involved in core TB service delivery and the guidelines and materials to be used. The training
of health care providers is an on-going process including refresher courses. Moreover, in order
to incorporate new interventions and recommendation in TB control, updating of the training
modules and guidelines is also an on-going process.
Table 47: Recommended staff training in NTP/PTPs
Staff Category
Training
Participants Duration (Days)
Material Location
Doctors 6 NTP Doctors Module District Hospital and PHC Doctors
Paramedics (all) 3 NTP Paramedic’s Module District Hospital and PHC paramedics
Paramedic (BMUs only)
1 NTP Quarterly Reporting Module
District 1 paramedic per BMU
Laboratory staff 10 NTP laboratory staff module
Province Prefer: Provincial Reference laboratory
District laboratory supervisor
10 NTP Province Prefer: Provincial Reference laboratory
Lady Health Worker 1 NTP LHW Module Facility Prefer: Associated health facility
District Managers 2 NTP Planning/ Review Guide
District
District manager include: EDO, DOH, DTC, In-charge DHDC, MS DHQ/THQ Product: District TB plan
119
SECTION A2 –
A2/2: SWOT ANALYSIS
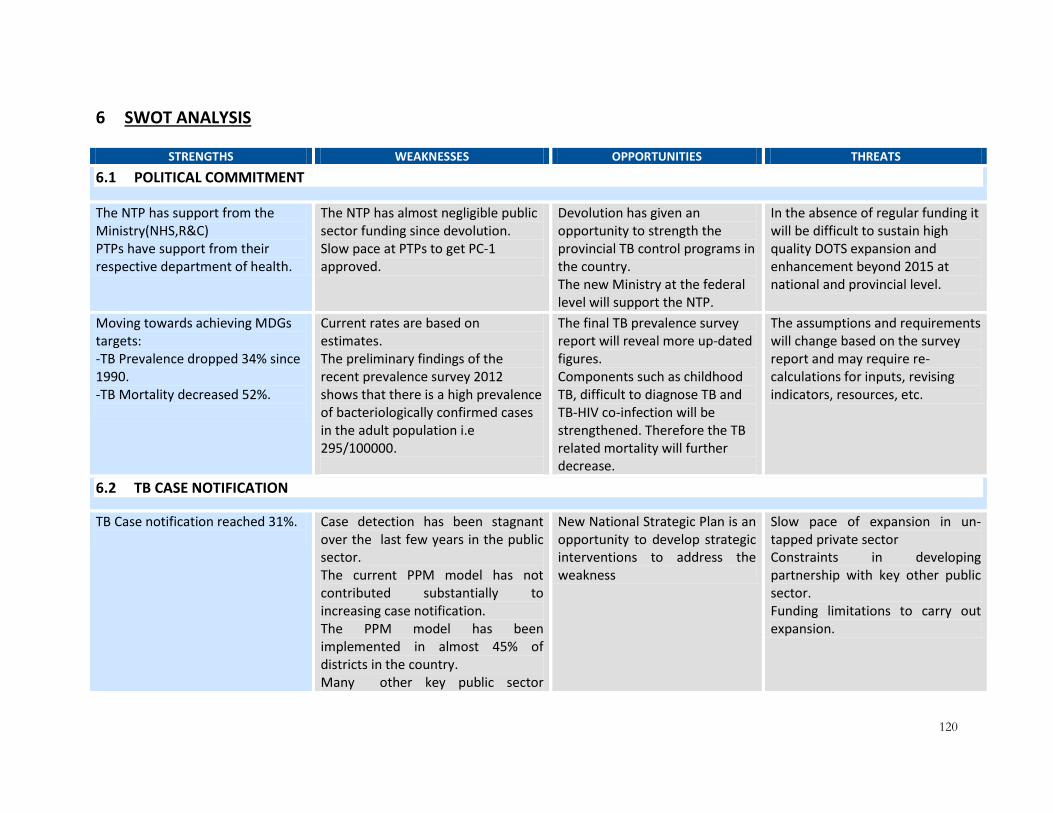
120
6 SWOT ANALYSIS
STRENGTHS WEAKNESSES OPPORTUNITIES THREATS
6.1 POLITICAL COMMITMENT
The NTP has support from the Ministry(NHS,R&C) PTPs have support from their respective department of health.
The NTP has almost negligible public sector funding since devolution. Slow pace at PTPs to get PC-1 approved.
Devolution has given an opportunity to strength the provincial TB control programs in the country. The new Ministry at the federal level will support the NTP.
In the absence of regular funding it will be difficult to sustain high quality DOTS expansion and enhancement beyond 2015 at national and provincial level.
Moving towards achieving MDGs targets: -TB Prevalence dropped 34% since 1990. -TB Mortality decreased 52%.
Current rates are based on estimates. The preliminary findings of the recent prevalence survey 2012 shows that there is a high prevalence of bacteriologically confirmed cases in the adult population i.e 295/100000.
The final TB prevalence survey report will reveal more up-dated figures. Components such as childhood TB, difficult to diagnose TB and TB-HIV co-infection will be strengthened. Therefore the TB related mortality will further decrease.
The assumptions and requirements will change based on the survey report and may require re-calculations for inputs, revising indicators, resources, etc.
6.2 TB CASE NOTIFICATION
TB Case notification reached 31%.
Case detection has been stagnant over the last few years in the public sector. The current PPM model has not contributed substantially to increasing case notification. The PPM model has been implemented in almost 45% of districts in the country. Many other key public sector
New National Strategic Plan is an opportunity to develop strategic interventions to address the weakness
Slow pace of expansion in un-tapped private sector Constraints in developing partnership with key other public sector. Funding limitations to carry out expansion.

121
organizations are not currently in partnership with NTP.
Diagnosis is based on passive case finding.
New diagnostic algorithms are not in place in which active TB disease will be detected through passive, active and enhanced case finding approaches. Care providers will require training on new algorithms.
New plans at the National and provincial levels will include requirement to introduce new TB diagnostic algorithms in the country.
Enhanced case finding will increase the load on the laboratories and care provides, which may affect quality of care.
6.3 CONTACT INVESTIGATION
TB contact investigation is part of the National TB policy
Implementation is not as per the required pace
Guidelines need to be refined and properly implemented.The strategy will incorporate the activities which will require addressing the issues around TB contact investigation.
Expansion of services implies stringent quality assurance.
6.4 CHILDHOOD TB
- 32 TCHs - 30 Districts - 25,737childhood TB cases
notified in country from Jan-Dec 2012
-Accuracy in diagnosis- more dependency on laboratory tests -Non-Involvement of the private sector -Adequate knowledge, skills on diagnostic tools -Shortage of trained healthcare staff for Childhood TB Case Management -TB cases are not reported separately in National data. -Non-availability of Child friendly ATT (FLD/SLD) -PPD-procurement, transportation (high wastage, cold chain
The strategy will incorporate activities which will require addressing the issues around childhood TB case management.
Expansion of services implies stringent quality assurance.

122
maintenance) and distribution issues. -Poor childhood TB case management at peripheral levels (THQs/RHCs/BHUs) -No ACSM strategy
6.5 HOSPITAL DOTS LINKAGE (HDL) i.e. TEACHING HOSPITAL
Experience of implementation of TB DOTS in tertiary care hospitals Collaboration with Pakistan Chest Society and Pakistan Paediatric Association in the development and endorsement of Adult and childhood TB management guidelines
Weak linkages within the tertiary care hospitals ACSM activities were not appropriately targeting the TCH settings Weak M&E of HDL component Weak external linkages with peripheral facilities
Rapid turnover of trained staff
Staff capacity and motivation
High clientele at TCH
Legislation to make TB a notifiable disease
Lack of ownership of hospital management
Continued lack of communication between departments within the hospital
Lack of integration of TB data in
the hospital’s medical records
system
6.6 ACSM
Key ACSM activities has been carried out including; -Community awareness -Community coalitions -Involvement of electronic and print media -Patient empowerment interventions, etc -ACSM resource materials were produced and distributed
-Highly dependent on GF and other donor support and since the completion of funding the ACSM activities almost stopped. -Public sector support is negligible.
New national and provincial plan will incorporate sustaining key ACSM interventions.
6.7 DRUG MANAGEMENT
Using FDCs proven bioavailability as first line anti-TB.
Procurement of quality FDCs at the local level is a challenge.
The local pharmaceutical industry is becoming sensitized
Process of approvals will take time.
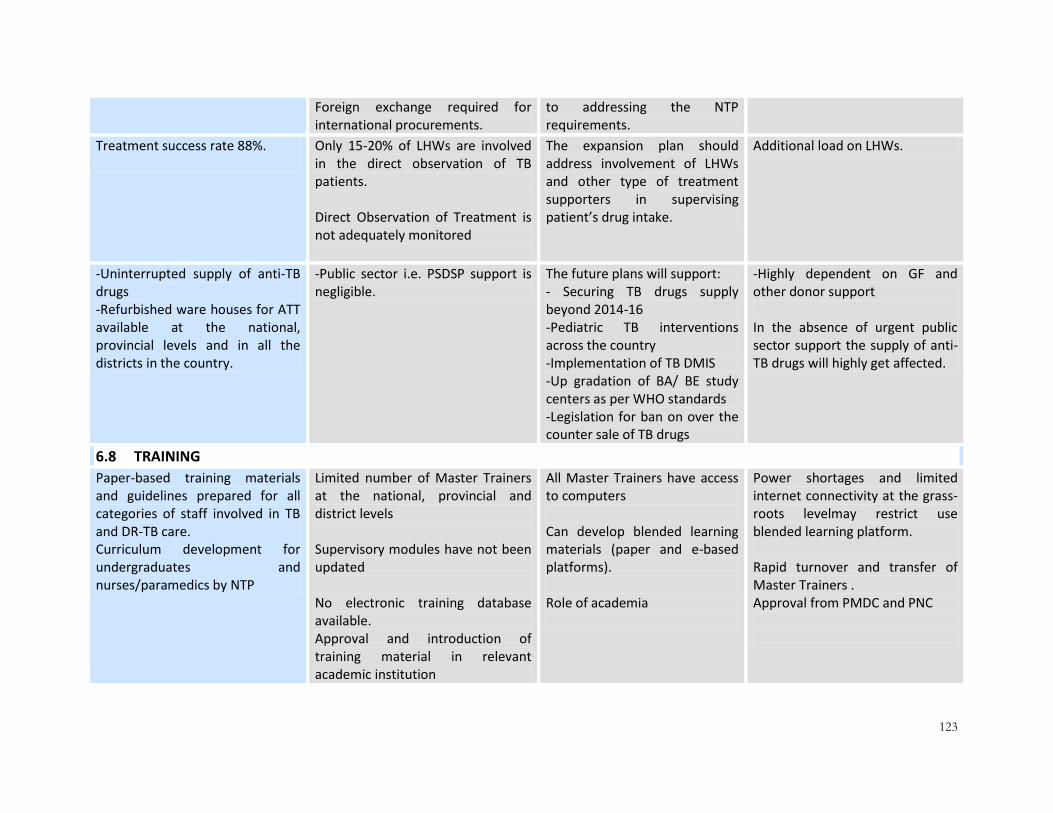
123
Foreign exchange required for international procurements.
to addressing the NTP requirements.
Treatment success rate 88%.
Only 15-20% of LHWs are involved in the direct observation of TB patients. Direct Observation of Treatment is not adequately monitored
The expansion plan should address involvement of LHWs and other type of treatment supporters in supervising patient’s drug intake.
Additional load on LHWs.
-Uninterrupted supply of anti-TB drugs -Refurbished ware houses for ATT available at the national, provincial levels and in all the districts in the country.
-Public sector i.e. PSDSP support is negligible.
The future plans will support: - Securing TB drugs supply beyond 2014-16 -Pediatric TB interventions across the country -Implementation of TB DMIS -Up gradation of BA/ BE study centers as per WHO standards -Legislation for ban on over the counter sale of TB drugs
-Highly dependent on GF and other donor support In the absence of urgent public sector support the supply of anti-TB drugs will highly get affected.
6.8 TRAINING
Paper-based training materials and guidelines prepared for all categories of staff involved in TB and DR-TB care. Curriculum development for undergraduates and nurses/paramedics by NTP
Limited number of Master Trainers at the national, provincial and district levels Supervisory modules have not been updated No electronic training database available. Approval and introduction of training material in relevant academic institution
All Master Trainers have access to computers Can develop blended learning materials (paper and e-based platforms). Role of academia
Power shortages and limited internet connectivity at the grass-roots levelmay restrict use blended learning platform. Rapid turnover and transfer of Master Trainers . Approval from PMDC and PNC

124
6.9 TB CARE IN ELDERLY AND HIGH RISK GROUPS
TB care includes services for the elderly patients and other risk groups
Utilization of services is low among the elderly and high risk groups
Availability of global strategic guidelines to address TB in elderly and high risk groups
Stigmatization of high risk groups deters care seeking
6.10 TB-HIV CO-INFECTION
The program has six years of experience implementing TB/HIV co-infection interventions There at least 19 sites across Pakistan where counseling and testing for TB and HIV has been made available through TB/HIV collaboration National TB/HIV Collaborating Boards and provincial coordination committees have been formed
- Interventions implemented so far are not specifically targeting key populations where risk of infection (both TB and HIV) is higher
- Coordination between TB and HIV programs has been sub-optimal
- Low coverage of sentinel sites -Private sector healthcare providers not engaged in TB/HIV co-infection - Lack of innovations and Operations Research
- Addressing TB/HIV co-infection is an international priority - Engagement of private sector healthcare providers and facilities provides an opportunity to include TB/HIV interventions - Data on prevalence of HIV in key populations is available through HASP Round 4 conducted in 2011 - Opportunities exist to enhance collaboration between TB and HIV programs
- Socio-cultural stigma - HIV is a low priority
6.11 TB AND CHRONIC AILMENTS AND TOBACCO SMOKING
The NTP has demonstrated successful implementation of new initiatives
No policy and guidelines at the national level
New strategic plan will provide strategic interventions to address these areas
Strong lobbying by the tobacco manufacturers
6.12 LABORATORY NETWORK
-Microscopy Network functional
in all 141 districts.
-Access to microscopy services is
not uniform in all settings.
-To improve access by
establishing diagnostic facilities
-High cost implication on DOH for new induction of HR.
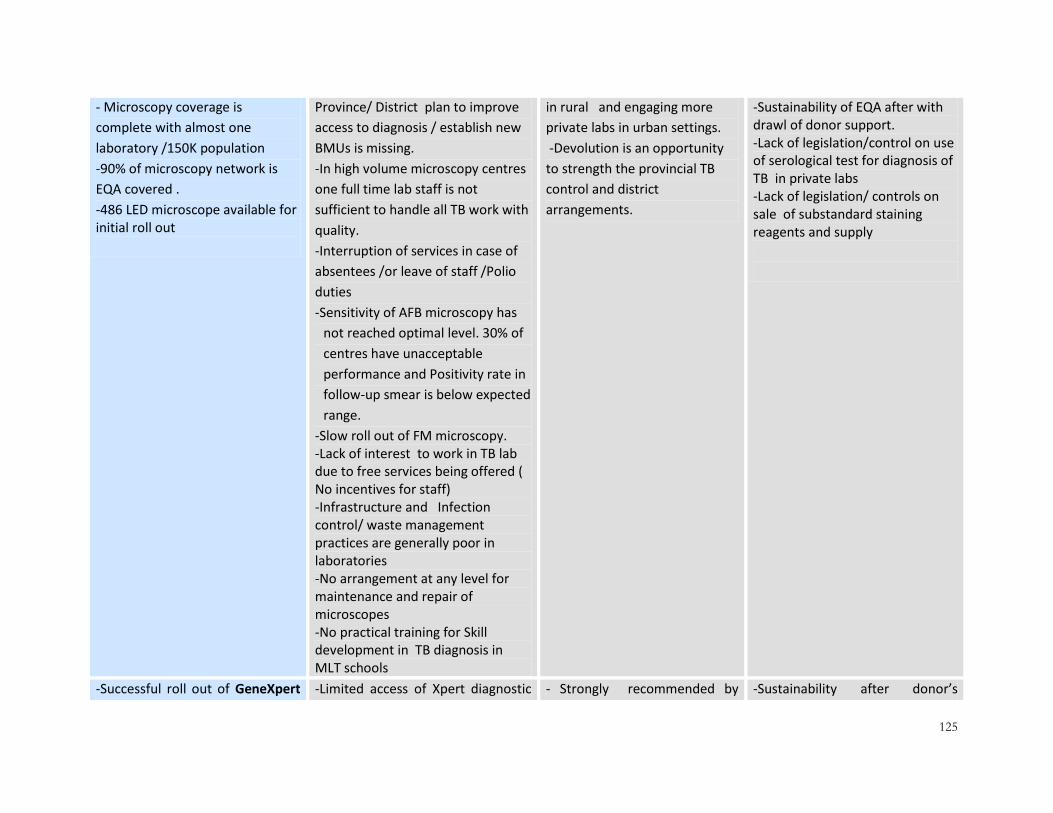
125
- Microscopy coverage is
complete with almost one
laboratory /150K population
-90% of microscopy network is
EQA covered .
-486 LED microscope available for initial roll out
Province/ District plan to improve
access to diagnosis / establish new
BMUs is missing.
-In high volume microscopy centres
one full time lab staff is not
sufficient to handle all TB work with
quality.
-Interruption of services in case of
absentees /or leave of staff /Polio
duties
-Sensitivity of AFB microscopy has
not reached optimal level. 30% of
centres have unacceptable
performance and Positivity rate in
follow-up smear is below expected
range.
-Slow roll out of FM microscopy. -Lack of interest to work in TB lab due to free services being offered ( No incentives for staff) -Infrastructure and Infection control/ waste management practices are generally poor in laboratories -No arrangement at any level for maintenance and repair of microscopes -No practical training for Skill development in TB diagnosis in MLT schools
in rural and engaging more
private labs in urban settings.
-Devolution is an opportunity
to strength the provincial TB
control and district
arrangements.
-Sustainability of EQA after with drawl of donor support. -Lack of legislation/control on use of serological test for diagnosis of TB in private labs -Lack of legislation/ controls on sale of substandard staining reagents and supply
-Successful roll out of GeneXpert -Limited access of Xpert diagnostic - Strongly recommended by -Sustainability after donor’s

126
with installation at 18 sites.
-Piloting done for early diagnosis
of rifampicin resistance
services to all patient at risk of
MDR.
- Lack of specimen referral and
transport mechanism.
Weak logistic and supply systems
for effective storage and
transportation of kits at provincial
level.
New R and R tool (2013) not yet
implemented.
Delay in procurement and
calibration of equipment
- Minimal contribution of domestic
funding in Xpert implementation.
WHO as initial test in Patient at
risk of MDR
GF support available for Xpert
KITs to support initial scale up
of PMDT programme
withdrawal.
-Challenges of Int. Procurement
from public sector finances..
-Resources available for
establishing 16 culture
laboratories
-6 culture laboratories established
and offering services for PMDT.
-Limited access to culture services
due to low coverage and lack of
specimen referral and transport
mechanism.
-No policy on use of culture for
confirmation of AFB smear negative
and EPTB cases.
-Weak infrastructure, low
counterpart funding for overheads
and maintenance cost.
-Limited in country capacity
maintenance/ repair of equipment.
-Paper based recording and
-WHO guidance on need and
coverage of TB culture and DST
services.
-Initial capital investment for
establishing 16 culture facilities
available through GF.
-Failure to enhance domestic
funding for TB diagnostic.
-Sustainability on withdrawal of
donors (services ,
infrastructure , supplies,
maintenance)
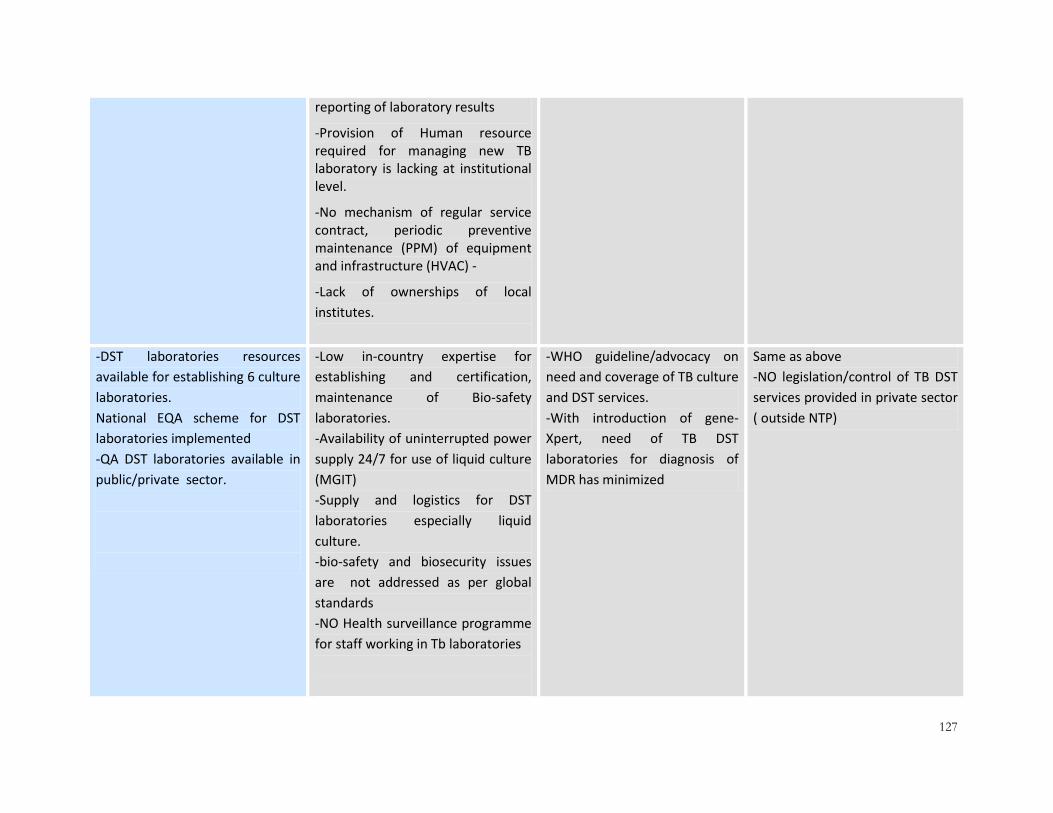
127
reporting of laboratory results
-Provision of Human resource required for managing new TB laboratory is lacking at institutional level.
-No mechanism of regular service contract, periodic preventive maintenance (PPM) of equipment and infrastructure (HVAC) -
-Lack of ownerships of local
institutes.
-DST laboratories resources
available for establishing 6 culture
laboratories.
National EQA scheme for DST
laboratories implemented
-QA DST laboratories available in
public/private sector.
-Low in-country expertise for
establishing and certification,
maintenance of Bio-safety
laboratories.
-Availability of uninterrupted power
supply 24/7 for use of liquid culture
(MGIT)
-Supply and logistics for DST
laboratories especially liquid
culture.
-bio-safety and biosecurity issues
are not addressed as per global
standards
-NO Health surveillance programme
for staff working in Tb laboratories
-WHO guideline/advocacy on
need and coverage of TB culture
and DST services.
-With introduction of gene-
Xpert, need of TB DST
laboratories for diagnosis of
MDR has minimized
Same as above
-NO legislation/control of TB DST
services provided in private sector
( outside NTP)
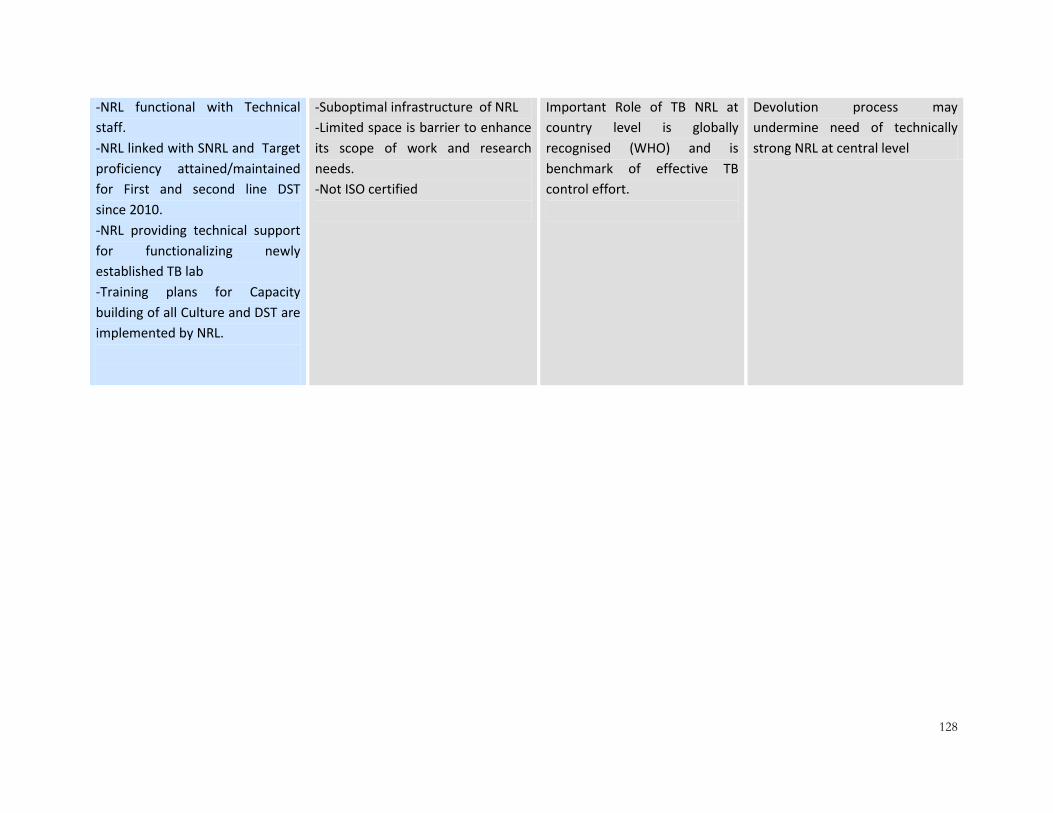
128
-NRL functional with Technical
staff.
-NRL linked with SNRL and Target
proficiency attained/maintained
for First and second line DST
since 2010.
-NRL providing technical support
for functionalizing newly
established TB lab
-Training plans for Capacity
building of all Culture and DST are
implemented by NRL.
-Suboptimal infrastructure of NRL
-Limited space is barrier to enhance
its scope of work and research
needs.
-Not ISO certified
Important Role of TB NRL at
country level is globally
recognised (WHO) and is
benchmark of effective TB
control effort.
Devolution process may
undermine need of technically
strong NRL at central level

129
6.13 DRUG RESISTANT-TB
NTP has a DR-TB structure: Full-
time MDR-TB unit with logistics.
-Although budgets and posts have been initiated, yet PTP structure and management capacity have yet to be strengthened.
-NTP MDR-TB unit needs
strengthening to address the
expansion phase.
-Devolution has given an
opportunity to strength the
provincial TB control programs
in the country.
-New Ministry formulated in
Islamabad.
Without additional National and
International financial resources it
will be difficult to sustain MDR-TB
programmatic activities beyond
2015 in the country.
84% of the 2013 target of
enrollment has been achieved.
-High DR-TB incidence among new
(4.3%) and re-treatment TB cases
(19.4%).
-16% of the 2013 target of
enrollment has been missed.
-Following a passive approach to
case detection.
-Private sector not fully onboard in
DR-TB care.
- Other public sector health care
providers as well as parastatal are
not fully involved in DR-TB care.
-Revised case finding strategy
has been established to
increase case enrollment
-MDR-TB expansion plan has
been developed.
Without the full implementation
of the revised case finding
strategy and active involvement
of PPM, it will be very difficult to
achieve the target.
-18 PMDT sites functional in four
provinces till the end of
December 2013
-Infection control arrangement in
place.
-Human resource trained.
-Funding is available
-Expansion of PMDT sites not in full
accordance with the work plan.
- Delays in infection control
arrangements
-12 more PMDT sites will be
established in 2014.
-Expansion plan which will be
reflected in National and
Provincial Strategic Plans will
accommodate the
establishment of more PMDT
-Lack of adequate Funding for
expansion and sustainability of
the PMDT.
-Lengthy procurement processes
delay the establishment of PMDT
sites and consumables.
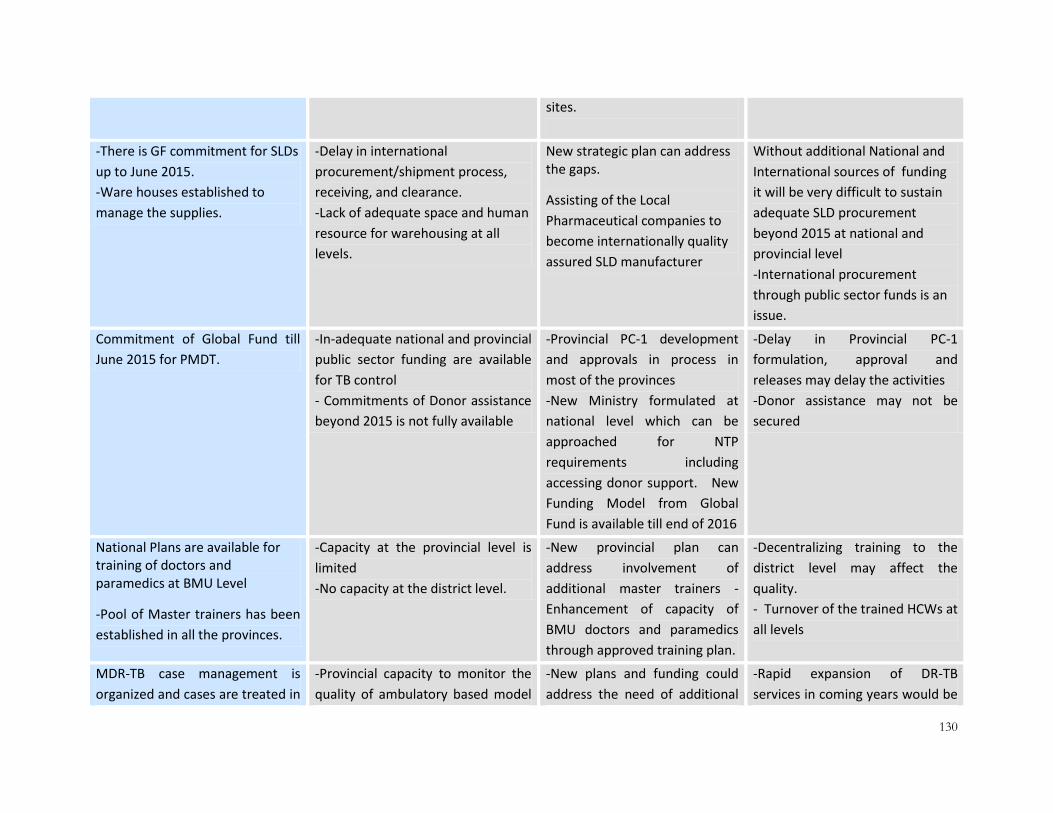
130
sites.
-There is GF commitment for SLDs
up to June 2015.
-Ware houses established to
manage the supplies.
-Delay in international
procurement/shipment process,
receiving, and clearance.
-Lack of adequate space and human
resource for warehousing at all
levels.
New strategic plan can address the gaps.
Assisting of the Local
Pharmaceutical companies to
become internationally quality
assured SLD manufacturer
Without additional National and
International sources of funding
it will be very difficult to sustain
adequate SLD procurement
beyond 2015 at national and
provincial level
-International procurement
through public sector funds is an
issue.
Commitment of Global Fund till
June 2015 for PMDT.
-In-adequate national and provincial
public sector funding are available
for TB control
- Commitments of Donor assistance
beyond 2015 is not fully available
-Provincial PC-1 development
and approvals in process in
most of the provinces
-New Ministry formulated at
national level which can be
approached for NTP
requirements including
accessing donor support. New
Funding Model from Global
Fund is available till end of 2016
-Delay in Provincial PC-1
formulation, approval and
releases may delay the activities
-Donor assistance may not be
secured
National Plans are available for training of doctors and paramedics at BMU Level
-Pool of Master trainers has been
established in all the provinces.
-Capacity at the provincial level is
limited
-No capacity at the district level.
-New provincial plan can
address involvement of
additional master trainers -
Enhancement of capacity of
BMU doctors and paramedics
through approved training plan.
-Decentralizing training to the
district level may affect the
quality.
- Turnover of the trained HCWs at
all levels
MDR-TB case management is
organized and cases are treated in
-Provincial capacity to monitor the
quality of ambulatory based model
-New plans and funding could
address the need of additional
-Rapid expansion of DR-TB
services in coming years would be

131
line with WHO and national
guidelines.
of care in DR-TB services is not
adequate.
-Inadequate HR at all levels to
monitor PMDT
trained human resource and
logistics.
a challenge for TB control
programs.
- Social Support that is provided
to Patient and Treatment
supporter enhance case holding
among DR-TB cases.
-Costly.
- No public sector funding for social support
New plans for funding including
PC-1 could address the social
support.
-Difficult to sustain
-Public sector has limited
precedence
Technical assistance currently
available at national level through
GF and donor agencies
Limited technical assistance
available at provincial level
-New plans and funding could
address the national and
provincial TA needs.
-Post devolution situation can
provide opportunity to
strengthen the provincial
programmes
Sustainability for long term
technical assistance
6.14 PUBLIC PRIVATE MIX (PPM)
TB case contribution from PPM is 20% of the overall national case notification.
Case detection has been stagnant over the last few years. The current PPM model has not contributed substantially in increasing the case notification.
New plans can incorporate interventions to strengthen the existing model.
High cost initiative and difficult to get support from public sector finances.
Diagnosis is based on passive case finding.
New diagnostic algorithms are not in place in which active TB disease will be detected through passive, active and enhanced case finding approaches. Care providers will require training on new algorithms.
New plans at National and provincial levels will include the requirement to introduce new TB diagnostic algorithms in the country.
Enhanced case finding will increase the load on the laboratories and care provides which may affect quality of care.
About 200 NGO managed clinics Key NGO set-up is not in current About 10% of PHC facilities

132
involved in PPM model (PATA, AKHSP, MALC, etc)
partnership such as PPHI/PRSP. managed by PPHI/PRSP can contribute to case detection and the remaining in suspect screening and referral. About 30 million population with expected 68,000 cases can be addressed.
About 18 large hospitals managed by private sector/NGOs in major cities are involved in PPM model.
Still many private sector hospitals in big cities need to be brought in to partnership.
New plans can incorporate involving additional private hospitals in TB care.
Without rigorous monitoring the quality of service will be compromised.
About 10 million population are provided TB services through other public sector facilities. About 30 other public sector hospitals in big cities under the PPM model.
Many key other public sector organizations are not currently in partnership with NTP. Expansion is very slow.
Expanding the PPM initiative by involving currently un-tapped private sector and involving key other public sector organizations.
Slow pace of expansion in un-tapped private sector Constraints in developing partnership with key other public sector. Funding limitations to carry out expansion.
2300 GPs involved in current PPM model implemented in 45% of districts in the country.
Slow implementation. High attrition rate among GPs. Coverage in the private sector is not 100%. Chest specialists and medical specialist are not involved in PPM model. Involvement of PMA and PSS not significant. No involvement of Society of family physicians.
Devolution has given an opportunity to strength the provincial TB control programs in the country to monitor PPM activities. Opportunity to expand the current model in 100% district involving 5,000 GPs.
Sustaining quality of services will be a challenge.
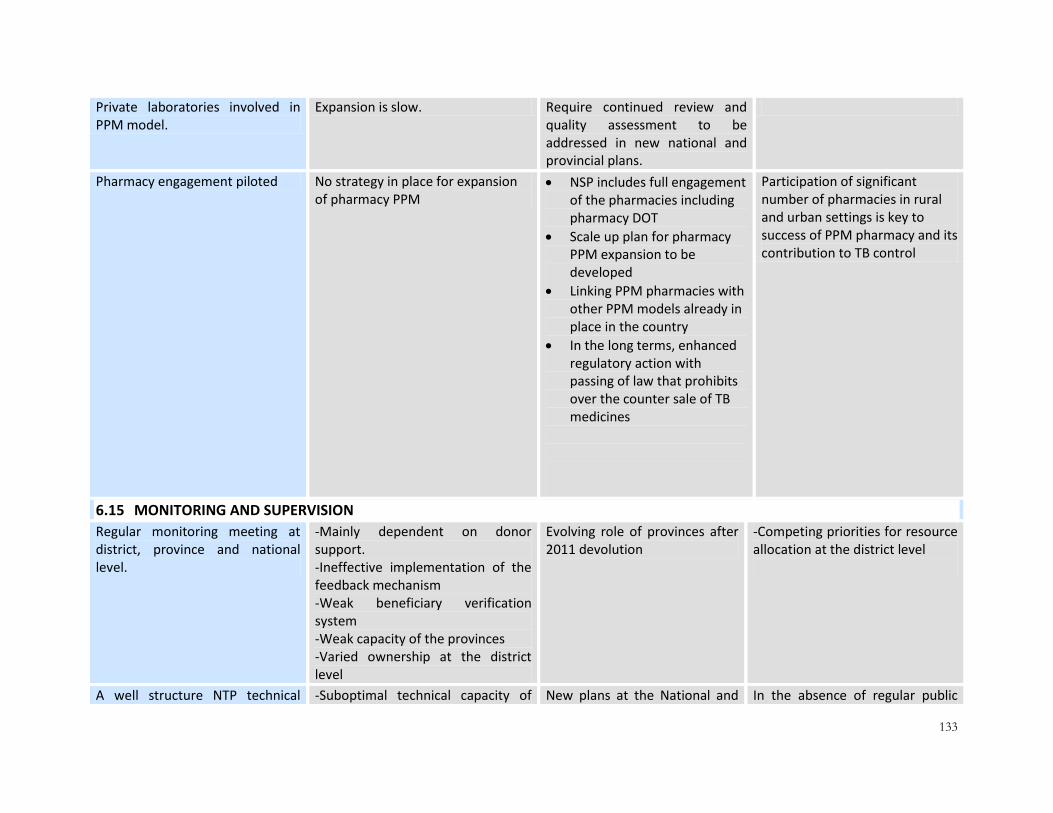
133
Private laboratories involved in PPM model.
Expansion is slow. Require continued review and quality assessment to be addressed in new national and provincial plans.
Pharmacy engagement piloted No strategy in place for expansion of pharmacy PPM
NSP includes full engagement of the pharmacies including pharmacy DOT
Scale up plan for pharmacy PPM expansion to be developed
Linking PPM pharmacies with other PPM models already in place in the country
In the long terms, enhanced regulatory action with passing of law that prohibits over the counter sale of TB medicines
Participation of significant number of pharmacies in rural and urban settings is key to success of PPM pharmacy and its contribution to TB control
6.15 MONITORING AND SUPERVISION
Regular monitoring meeting at district, province and national level.
-Mainly dependent on donor support. -Ineffective implementation of the feedback mechanism -Weak beneficiary verification system -Weak capacity of the provinces -Varied ownership at the district level
Evolving role of provinces after 2011 devolution
-Competing priorities for resource allocation at the district level
A well structure NTP technical -Suboptimal technical capacity of New plans at the National and In the absence of regular public

134
unit in place the provincial units. Dependent on donor funding which is available up to 2015.
provincial levels will include requirements to sustain the current technical unit at NTP/PTPs
and donor funding it will be difficult to sustain.
Arrangements in place to coordinate TB control activities in districts.
District TB Coordinator (DTC) is a designated officer from the district health office and has additional responsibilities.
New plans at the National and provincial levels may include a dedicated DTC in all 141 districts.
Shortage of staff in the districts. Additional recruitment implies high cost.
6.16 OPERATIONAL RESEARCH
-National Prevalence Survey conducted -OR projects of significant importance conducted
-Operational difficulties in implementing surveys in areas with natural disasters and effected with law and order situation.
Identified priority research areas i.e. MDR default tracing mechanism (e DOTS), Community management of MDR, Infection control of MDR patients once released in community, contact screening among sensitive and resistant TB.
- High MDR Defaults because of poor linkages with the district health system -Weak involvement of treatment center in treatment support of MDR Patients. -Poor infection control at household and community levels may lead to MDR among contacts and disease progression -Current program routine data shows poor yield from contact tracing interventions among sensitive and resistant TB
-Pilot of GIS based-DOTS and scale up -OR on the diagnostic center and treatment center link model to improve community management of MDR -Pilot of infection control strategies at the household and community level s and then scale up -Innovative strategies to enhance yields from contact tracing among sensitive and resistant TB
New Survey to estimate disease burden and under-reporting
Huge private sector in the country , the under-reporting involving Non NTP private and public sector need
Inventory study will be done in 2016 again to re-estimate the disease burden in the country

135
to be done
Established linkages with international academic institutions
The national academia is not engaged
The national academia can support many community activities. Sustain and expand linkages with other international institutions.
6.17 STOP TB PARTNERSHIP
Basic structure is available Not fully organized and not operational
Stop TB coalition at district level may provide a community level structure New innovation required strong STOP TB partnership in the country
6.18 TRANS-BORDER TB
Initial implementation started Not fully opertionalized New strategic plan will address this innovation
Geo political and security situation poses an obvious threat
6.19 TB AND POVERTY
Social support initiative for DR-TB patients
Limited experience New strategic plan will address this innovation
Multi-disciplinary involvement may result in difficulties mainly not in purview of the NTP

SECTION A2 –
A2/3: GAP ANALYSIS

137
7 GAP ANALYSIS
7.1 FUNDING MAINLY DEPENDS ON EXTERNAL SUPPORT 7.1.1. Even though TB control is organized in the framework of a well-structured national
program
7.1.2. Ongoing devolution process
7.1.3. Coordination between the NTP and International technical and donor agencies exists
7.1.4. TB control is a health priority for health department of the provinces
7.1.5. Not enough public sector funds are allocated in the provinces and, if allocated, there are
not enough released to cover all the needs of TB control
7.1.6. PC-1 are either newly developed and releases are not timely or are in the process of
being developed
7.1.7. Limited public sector funds are allocated from the federal level to implement TB control
activities in the provinces
7.1.8. Many components of TB control are dependant on international funding. For instance,
the implementation of MDR-TB case management activities are fully financed by GF.
7.2 LOW TB CASE NOTIFICATION 7.2.1. According to the last WHO estimate, 64% of smear-positive TB cases are being detected.
However, based on the preliminary results of the last TB prevalence survey, which shows
that prevalence of bacteriologically confirmed TB is about 295/100000 among adult
population, in fact the TB case notification is much lower i.e. 31%.
7.2.2. Passive case finding has been implemented and there is no national policy on active and
enhanced case finding.
7.2.3. A significant proportion of the rural population has limited access to screening services,
or are not screened for TB
7.2.4. In major cities (10) of the country, a significant proportion of the population is poor and
live in overcrowded downtown and suburban/slum areas and therefore have limited
access to TB diagnostic services.
7.2.5. A significant proportion of patients who seek care for a 2-week cough in health facilities
are not screened for TB. Data suggest that respiratory patients that are evaluated for TB
are those who have symptoms that heavily suggest TB. For example, data from TB
laboratory registers point out that 15% of TB suspects are smear-positive in Pakistan.
7.2.6. It is believed that a non-negligible number of TB patients who have been identified
through sputum smear examination are neither registered nor notified. For instance, in
Sindh Province, 9% of smear-positive TB cases detected in2012 were not registered nor
notified and therefore not promptly treated.
138
7.3 LOW PROPORTION OF TB CONTACT ARE INVESTIGATED FOR TB 7.3.1. TB contact investigation is included in the national strategy to control TB. There is no
specific national guide for contact investigation, but guidance is provided in the
national TB treatment guidelines’ document and in MDR-TB case management guide.
7.3.2. The definitions of TB index case and contact are not quite in line with the WHO
recommendations and the algorithm and SOPs need further specifications.
7.3.3. There is an information system that generates some data on TB contact investigation
activities. These data suggest that TB contact investigation is far from being fully
implemented. It seems that only 1% of the identified contacts are screened for TB.
7.4 CHILDHOOD TB CASES NOT FULLY REPORTED TO NTP 7.4.1. Out of 110,000 SS+ all age groups diagnosed in 2012, childhood SS+ TB cases were 4,400
(4%).
7.4.2. Out of 285,410 total cases in 2012, children were 25,737 (9%).
7.4.3. About 40% of the district hospitals in the country are currently not implementing
childhood TB as per NTP protocols.
7.4.4. It is expected that with the high prevalence of bacteriologically confirmed TB among
adults 295/100000, there will be more children who will be in contact of these cases, are
getting TB, and need to be diagnosed and managed.
7.5 HOSPITAL DOTS LINKAGE (HDL) NOT FULLY OPERATIONAL A significant proportion of TCH are not linked to NTP. This minimizes the opportunity to reach a
large volume of presumptive TB patients that seek services at TCHs.
Effective referrals systems between periphery and TCH have not been established, leading to
weak implementation of TB DOTS in these settings
Sub-optimal inter-departmental coordination in the hospitals
Lack of integration of TB data into the hospital’s medical records system
7.6 ACSM STRATEGY NOT ABLE TO CREATE AN IMPACT ON INCREASING CASE FINDING 7.6.1. The prevalence survey has indicated that about 60% of TB patients have not visited any
health facility for their symptoms.
7.6.2. Huge gaps exits in term of providing information and mobilizing the patients who are
symptomatic to health facilities.
7.6.3. Involvement of community health workers (Lady Health Workers, Community Mid Wives,
mobile vaccinators, etc) in suspect identification and referral are almost non-existent
7.6.4. Although extensive ACSM activities have been implemented at the national, provincial
and district level in recent years, they have shown almost no effect in increasing case
detection in the districts. For example in the province of Punjab the ACSM districts when
139
compared with non-ACSM districts shows either static or decreases in case notification
over time.
7.6.5. ACSM policy, strategy and operations need significant revision.
7.7 SIGNIFICANT ISSUES IN DRUG MANAGEMENT 7.7.1. Currently the major proportion of FLDs and all SLDs procured at the National level are
being provided from the GDF through the NTP, which will continue up to 2015-16. Beyond
that, no plan exists to sustain procurement at the National level.
7.7.2. The current procurement procedure does not address the issues related to availability of
quality assured drugs at the national and provincial levels, especially SLDs.
7.7.3. Even though, there are clearly defined procedures to manage TB drugs at the district and
BMU levels, these procedures are usually not respected by the staff at these levels; this
results in overstocking, a stock of TB drugs that remain beyond their shelve life and
simply a waste of TB drugs. In contrast, stock out of TB drugs occasionally occurs in some
BMUs.
7.7.4. In addition, the level of buffer stock, as required in the national guidelines on TB drug
management is not always maintained.
7.7.5. Many districts do not receive their stocks of TB drugs on time as planned because of the
limited availability of appropriate transportation system between the province and
district levels.
7.8 SIGNIFICANT ISSUES IN TRAINING IN TB CONTROL 7.8.1. The management of training activities is still quite under the leadership of the NTP
Central Unit. The national training modules and programs are well established for the
different areas of TB control and for the various categories of health professionals.
7.8.2. The training agendas of the provinces are often established by the NTP focal point for
training in coordination with the provincial manager for TB program. Planning of training
activities is not pro-actively shared with the PTP and is not always based on provincial
training needs and is not a bottom-up approach.
7.8.3. No core of national and/or provincial trainers have been established. The trainers that
need to be involved in training activities are identified on ad hoc basis.
7.9 NO SPECIFIC ACTIONS HAVE BEEN ESTABLISHED TO TARGET ELDERLY 7.9.1. The recent TB prevalence survey has reported that the prevalence of TB among people
aged 65 years and over is approximately 1.2% and 6.7 times higher than TB prevalence in
those aged 15-24 years.
7.9.2. To date, no specific strategy has been defined to actively screen elderly for TB and
establish appropriate mechanisms to manage patients with TB belonging to this age
group in Pakistan.

140
7.10 LIMITED IMPLEMENTATION OF TB/HIV COLLABORATIVE ACTIVITIES 7.10.1. The prevalence of HIV in the general population is less than 0.1%. The sentinel
surveillance system for TB/HIV, established by the NTP and involving 16 sites throughout
Pakistan, reported that the prevalence HIV infection among TB patients was 0.3% in
2012.Less robust data showed that the prevalence of TB in HIV-positive persons was 5.6%
for the same year. There is at present no robust system of data collection to establish
national and provincial prevalence of TB among HIV positive persons and vice versa.
7.10.2. There is Joint Coordination Board (JCB) for TB/HIV at the national level and in each
province. These JCBs include clearly identified members and have well defined terms of
reference. However, they do not meet on a regular basis.
7.10.3. The national guidelines for TB/HIV and training materials have not been updated in light
of the latest HASP data, and guidelines for targeting key populations have not been
developed.
7.10.4. No strategy has been designed and implemented to address needs of the key
populations.
7.10.5. As TB/HIV has been a low priority, domestic resources have been minimal for these
interventions.
7.11 NOSPECIFIC INTERVENTION HAS BEEN ESTABLISHED TO ADDRESS TB & CHRONIC AILMENTS AND TB &TOBACCO USE
7.11.1. No specific strategy has been defined or operationalized to address TB and Poverty
7.11.2. No specific strategy has been defined or operationalized to address TB in context of
Chronic ailments such as Diabetes and COPD
7.11.3. No specific strategy has been defined or operationalized to address TB control among
Tobacco Smokers
7.12 TB LABORATORY NETWORK NOT FULLY OPTIMIZED The National TB laboratory network includes 1381 microscopy laboratories, seven culture
laboratories among which three are performing DST and 22 laboratories were equipped with
Xpert machines by the end of 2013.
7.12.1: Microscopy Network for diagnosis of smear positive TB cases
Coverage: Distribution of Microscopy laboratories and catchment population varies from
province to province (due to variation in density population) between districts and also with in
districts. Mapping of functioning microscopy centres and accessibility of catchment population
to a diagnostic facility is not done. Plans to improve access by establishing more diagnostic
facilities engaging private sector laboratories or using specimen transport mechanism (sputum
or smeared slides) do not exist. Involvement of community health workers in suspect
identification and referral is minimal.
AFB smear microscopy is not done as a routine test in most private laboratories, rather all sorts
of serological test are being offered for TB diagnosis in private sector.

141
Infrastructure:- Microscopy services are integrated within multipurpose routine laboratories in
most of health facilities. Infrastructure of laboratories is mostly suboptimal in terms of space,
ventilation and infectious waste disposal arrangement. Infection control issues are not
addressed (improper place for specimen reception, specimen collection and waste
management).
Workload: Tb suspect identification is low furthermore TB services are not yet fully
decentralized. As a consequence workload in microscopy network is unevenly distributed, most
of peripheral microscopy laboratories ( RHC) have very low workload (<2 sm/day) in contrast to
laboratories at secondary level (DHQ,THQ) with workload exceeding 30 or more smears per
day.
Human resource for TB laboratories:- There is high staff turnover as result of contractual
appointment or transfer and posting which sometime reaches up to 40% in a year leading to
long queue of staff in waiting for formal training. System for on-job training or training on
induction at the district level is not in place and, as a result, a considerable number of
microscopy laboratories are functioning with untrained staff.
As TB microscopy services are offered FREE to patient with no incentive to Lab staff whom
otherwise likely to receive some incentive from other lab tests done. Therefore, lab staff is
more interested in doing non TB work due to financial benefit. Staff turnover is more
pronounced in private laboratories as service structure do not exist and salary scale are very
low in most of small scale laboratories.
There is a lack of dedicated TB Laboratory supervisors. Although District TB laboratory
supervisors have been identified in all districts, staff have been designated to perform these
additional TB laboratory duties besides their own routine tasks; as a result the commitment and
quality of work varies a great deal from district to district.
Trainings are conducted at the provincial level but no follow up is done of the human resources
trained. The database of HR working in TB laboratories is not maintained on a regular basis and
HR cannot be located if transferred from one health facility to another.
Training curriculum and practical facilities for TB diagnosis are inadequate in laboratory
technician schools and there is limited capacity of tutors. Graduates from these schools often do
not have any practical exposure to TB diagnosis.
Equipment for Microscopy services: Good quality microscopes are available in most health
facilities but there is no established system for regular servicing and repair of equipment.
There is no documented policy for the procurement and frequency of replacing and servicing
microscopes.
400 LED microscopes, distributed to the provinces for the introduction of FM microscopy in high
volume laboratories, have not yet been implemented at most of sites. Availability of resources
for LED microscopes varies from province to province and is not proportional to the number of
high volume laboratories.
142
Laboratory staining reagents and chemicals: There are significant barriers to the
implementation of policy guidelines for laboratory staining reagents and chemicals required for
TB diagnosis. The quality of reagents procured is not uniform.
The guidelines for the contribution to the logistics of the microscopy network do not exist at
various levels.
Quality assurance: External quality assessment by blinded re-checking is implemented in 90% of
the TB microscopy laboratories but its quality and outcome varies from district to district. Weak
monitoring (onsite and desk) and on-the-job training and feedback is not optimal at all levels.
7.12.2: Culture/Xpert laboratory for diagnosis of smear negative tuberculosis
Approximately half of all pulmonary TB cases are smear negative in Pakistan and these are not
bacteriologically confirmed due to a lack of resources, limited capacity, and absence of policy
guidelines.
The culture and GeneXpert laboratory network is expanding, but optimal utilization of these
services cannot be achieved without an effective specimen transport and referral mechanism.
7.12.3: Culture and DST laboratories for management of DR-TB:
Coverage:- Currently resources are available for establishing one DST laboratory for 25 Million
population. With the expected revision in guidelines, in light of Xpert rollout, this number will
need to be reviewed.
Infrastructure:- Upgrading the infrastructure of the planned laboratories is in process through
global fund but there are serious concerns regarding sustained maintenance and overhead costs
of the established laboratories after close out of the project.
There is a power crisis in the country and most institutes are facing power outages. Provision of
uninterrupted power supply to run the equipment (especially MGIT for liquid DST) requires high
capacity generators and regular funding for fuel charges.
Equipment:- Maintenance of the equipment, including the national TB laboratory, is a
continuous and major problem. Additionally, in-country capacity for certification of BSC and
repair of equipment in very limited.
Funding to sustain these services has not been secured after 2015.
New diagnostic tools Infrastructure requirements and short shelf life are the main challenges for
rolling out new technologies.
Harsh environmental conditions (temperature >400C in most part of country for most part of
year), compounded by the prevailing power crises, is one of major challenges to ensuring
uninterrupted functioning of Xpert and MGIT.
There is limited funding contribution from the public sector for introduction/maintenance or
supply of Kits for running new diagnostic tools.
Human resources: All technical staff are funded through GF for new TB culture and DST
laboratories including both the national and provincial reference laboratories, however there is

143
still a shortage of trained staff because the public sector has not been able to provide the
required staff due to gaps in HR.
As a result continuity of services beyond 2015 will be a challenge.
There is lack of dedicated full time TB Laboratory managers at the provincial levels, as currently
TB in-charges at the provincial levels have many other assigned tasks which limits their
commitment for TB.
TB Laboratory supplies and management: Most laboratory supplies are provided to all TB
culture and DST laboratories through donor funding with little contribution from the provinces
or host health institutes.
7.12.4: National TB Reference laboratory
The NTRL is providing services for PMDT and handling large numbers of highly infectious
specimens (11 XDR reported in 2013) but weak infrastructure and bio-safety standards pose a
risk to laboratory staff. Issues pertaining to Biosafety and bio-security are not addressed.
The NTRL is a central place for HRD of TB culture and DST laboratory networks but due to small
space, it is difficult to implement training and routine services simultaneously; therefore training
quality or routine services are compromised.
The national EQA scheme for DST has been established but there is a need for capacity building
to implement a quality management system.
There is need to properly manage and analyze, on a regular basis, data generated both at the
NTRL and National laboratory network levels. Capacity of the NTRL to conduct operational
research, based on program needs, and publish in international peer reviewed journals is
limited.
The molecular section of the NTRL is not yet fully established.
Gaps in reaching ISO laboratory accreditation /certification include infrastructure, bio- safety,
equipment maintenance, training, recording and reporting.
There is need to establish one centre of excellence in the country with the capacity to train ,
conduct research and address the need for advanced tuberculosis diagnostics.
7.13 MANY CARE PROVIDERS OUTSIDE THE NTP NETWORK ARE NOT INVOLVED IN TB CARE AND CONTROL EFFORTS
7.13.1. Pakistan has a wide and unregulated health sector and includes many varieties of
care providers, including a significant number of traditional healers.
7.13.2. Moreover, not all health facilities and type of health care providers are
appropriately linked with the existing TB diagnostic and referral services.
7.13.3. There are approximately 5,000 basic health units (BHU) and each of them covers
2,000 to 25,000 population. The daily attendance in each BHU ranges from 2 to 50
patients. Nearly all the BHUs are not under the responsibility of the District health
Authorities but under that of NGOs (PPHI, PRSP), therefore, they have quasi or no

144
linkages with the NTP. The available information suggests that very few patients
are referred from the BHU setting to the BMU network.
7.13.4. According to the National Health Accounts of 2009, there are about
100,00qualified general practitioners (GP) in Pakistan. Significant efforts have
been made to link them to NTP network. At present, roughly 2,500 GPs are
collaborating with the NTP/PTPs. A significant proportion of the GPs have never
notified any TB case or stopped notification. It is estimated that around 5% of TB
cases are notified by the GPs with some provincial variation. The NTP has not yet
initiated any action to involve the private chest specialists and professionals,
medical associations such as Pakistan Medical Association (PMA), Pakistan Chest
Society (PCS), Society of General Practitioners and Family Medicine, Pakistan
Pediatric Association (PPA) and others. The policy, strategy and operations of
involving and sustaining GPs in TB control activities need significant revision.
7.13.5. There are more informal and unqualified private care providers than qualified
care providers particularly in rural areas and poor urban settings where TB is
usually highly prevalent. To date, no strategy has been established by the NTP to
explore how these informal and unqualified health workers can be linked to TB
control network. In addition, care services are provided in comparable number of
medicine stores without any regulation.
7.13.6. There are many private retail pharmacies in rural areas and poor urban setting
where clients with TB like symptoms seek care first. To date, no strategy has been
put in place how to engage the retail pharmacies to contribute to early case
detection, referral and pharmacy DOTS where TB treatment can be appropirately
dispensed accroding to national treatment guidelines. In addition, lack of of
regulatory enforcement to ensure that TB medicines are not freely sold in the
retail pharmacies has contributed to inappropriatness of TB management and
potentially contributed to increased resistance to TB medicines.
7.13.7. In Pakistan, there are many health services provided by other public sector
(corporate) sector such as the social security, army forces, Pakistan Railways,
mining societies and others. To date, limited linkages have been established
between the NTP and this sector.
TB in penitentiary system
7.13.8. TB control in prison system is included in the national policy to control TB. This
intervention was implemented in all 32 prisons of Punjab Province through the
TBREACH Project. To make this experience successful specific SOPs have been
developed. The data generated through this project suggest that the prevalence
of TB in prison is 1.3%.
145
7.13.9. The TBREACH Project was over at the end 2012 and TB control activities were
maintained in the 32 prisons.
7.13.10. The SOPs used for the TBREACH Project have not been yet adopted at
national level and no other TB control activities have been implemented outside
the prisons of Punjab Province.
TB in mining settings
7.13.11. There is no national policy for TB control in mining settings. There is no
collaboration established between the NTP and the health services of mining
corporations. The NTP has no information on TB burden and TB control in these
settings. There is no specific system generating such information.
7.14 A HIGH PROPORTION OFDR-TB PATIENTS ARE NOT DETECTED 7.14.1. A high proportion of DR-TB patients are not detected.
7.14.2. The annual estimate of DR-TB cases in Pakistan is 12044. At the same time our GF
based target for 2014 is 4518. Our current projected rate is at 42% of the GF
target
7.14.3. It is expected with new strategy in place, the DR-TB case finding will increase
proportionately which will require more material and logistic support to manage
these cases
7.14.4. Appropriate guidelines for PMDT are in place and operational plan has been
established for expansion with substantial funding mobilized from Global Fund.
However, diagnostic and follow-up laboratory facilities are limited.
7.14.5. Management of DR-TB cases is established through PMDT treatment sites which
are located throughout the country focusing primarily on Ambulatory Based
Model of care. However other health care system (i.e. BMUs, National
Programme, NRSP and PRSP, PPHI etc) are not fully involved yet in Ambulatory
based model of care.
7.14.6. Infection Control measures are generally in place in PMDT sites. However there
have been delays in the implementation of the plan among some PMDTs.
Infection control measures at the community level is inadequate
7.14.7. Lack of adequate administration and monitoring of social support component.
7.14.8. National guidelines on TB infection control are available. Infection control has
been implemented in 6 PMDTS with trained staff in line with the international
standards.
146
7.14.9. There is an operational plan to expand TB infection control in 30 PMDTS; funding
from GF is available for the procurement of the required supplies and to print
training modules and guidelines. But, there is no funding to organize training
sessions of the staff of these PMDTS.
7.14.10. No TB infection control has been implemented in HIV care facilities and in
health centres ensuring TB/HIV collaborative activities.
7.14.11. No clear approach has been defined for TB infection control in the BMUs
dealing with the majority of routine TB patients among which many will be
potential M/XDR-TB.
7.14.12. No system has been implemented to monitor and evaluate TB infection
control measures. There is no information system monitoring the health workers
who are affected with TB.
7.15 ISSUES IN OPERATIONALIZING MONITORING, SUPERVISION AND EVALUATION AT PROVINCIAL AND DISTRICT LEVELS
7.15.1. The monitoring and evaluation system is not properly structured at all the administrative
levels therefore; the quality of supervision is sub-optimal.
7.15.2. The M&E activities are the responsibility of both district (DHO/DTC), regional (NPOs) and
provincial staff (PTP). The NTP has provided PTO, NPOs and M&E officers to look after a
cluster of districts in the province but there are usually delays in recruitment and attrition
of staff is often so most of the regions were not supervised on a regular basis due to
shortage of NPOs.
7.15.3. At the regional level (divisional) there is no arrangement to monitor and evaluate TB
activities.
7.15.4. At the district level there is no formal arrangement to monitor and evaluate routine TB
activities. Additional case finding activities would demand more strong human resource
arrangement at district level.
7.15.5. The surveillance activities, data validation and analysis is sub-optimal. The data
generated by the monitoring and evaluation system in not analysed for decision making
at the provincial and district levels.
7.15.6. The supervision of TB control activities is well structured and its proceeding is well
established. The Central Unit supervises the province which supervises the district which
supervises BMUs. The three levels establish supervision agendas for one or three
months. The district level usually informs the province level on the supervision that will
be undertaken at its level and does not submit any supervision report.
Weak managerial capacities at district level
147
7.15.7. The NTP is well structured with a Central Unit and Managerial units at the province and
district levels. The mission of the Central Unit is well defined and includes sufficient
number of staff. All the interventions defined in the national strategy to control TB are
covered by appropriate staff.
7.15.8. The ongoing process of devolution constitutes an opportunity to improve the capacities
of the NTP through the decentralization of many managerial responsibilities at province
level.
7.15.9. This process of decentralization needs to be appropriately defined, established and
technically assisted, especially at province level.
7.15.10. The capacities of the managerial units of the provinces need to be developed; to
adapt the national policy for TB control, to establish strategic plans for the province, to
set mechanisms for the organization of the supervision and training activities in the
provinces, to ensure appropriate TB surveillance, the monitoring of the TB control
activities implementation as well as TB care and control services delivery, the evaluation
of TB control outcome and to organize and develop the managerial capacities at district
level.
7.15.11. Significant weaknesses are identified at the district level in terms of management
of the TB control program.
7.16 TB CONTROL PROBLEMS NOT ADDRESSED THROUGH OPERATIONAL RESEARCH 7.16.1. Data collected from the NTP system is not fully analyzed to hypothesize for issues to be
addressed through operational research
7.16.2. There is no up-dated agenda for operational research at the national and provincial levels
7.16.3. Academic institutions are not fully collaborating with the NTP in operational research
7.16.4. The Operational Research which is done is inadequately translated into practice
7.16.5. Provincial and district capacity is limited to design and conduct of operational research
7.16.6. There is no comprehensive policy on operational research
7.17 NON FUNCTIONING NATIONAL STOP TB PARTNERSHIP 7.17.1. The National Stop TB Strategy for Pakistan was created in 2004. An executive secretariat
was established with clear terms of reference. But since that time, no action has been
undertaken by this partnership, especially to raise funds within country.
7.18 TB IN TRANS-BORDER POPULATIONS NOT OPERATIONAL 7.18.1. The province of KP and Balochistan has a border with Afghanistan and Iran from where
trade and refugee movement is frequent. To date, no specific strategy has been
defined to operationalize TB in trans-border population.
7.19 NOSPECIFIC INTERVENTION HAS BEEN ESTABLISHED TO ADDRESS TB &POVERTY, Legislation on drug sale, declaring TB as notifiable disease
7.19.1. No specific strategy has been defined or operationalized to address TB and Poverty

148
7.19.2. No current legislation on the sales of Anti-TB drugs in the market
7.19.3. No current legislation to declare TB a notifiable disease

149
SECTION A3 –
STRATEGIC GOALS, OBJECTIVES, INTERVENTIONS
& ACTIVITIES

150
8 STRATEGIES AND ACTIVITIES: TB CONTROL “VISION 2020”
8.1 OVERVIEW: NATIONAL TB STRATEGIC PLAN “VISION 2020” TB Control at the National, Provincial and Regional levels is currently going through a
rejuvenating phase of program development due to several reasons, including;
i) Health sector devolution;
ii) Limited public sector financing for TB control and shrinking donor assistance;
iii) Stagnant TB case notification over the last several years;
iv) High number of TB cases undetected in the community;
v) Effect of social determinants such as increasing poverty and societal inequalities;
vi) Global innovations in TB diagnosis and management;
vii) Increasing drug resistant TB;
viii) Managerial and governance issues;
ix) High risk behaviors such as increased use of tobacco;
x) Increase in the occurrence of COPD, diabetes and HIV/AIDS, etc.
This implies strategic thinking at all levels to address the challenges faced today by the TB
control program in Pakistan. The National TB Strategic Plan (NSP) “Vision 2020” is drawn from
provincial and regional strategic plans and consists of strategic interventions that will be
implemented under the purview of the NTP, in the context of the devolved health sector and in
the wake of the national TB prevalence survey.
The National TB Strategic Plan “Vision 2020” entails developing innovative strategies that will:
1- Improve the performance and impact of TB control by maximizing public sector investment
and accountability in TB control activities.
2- Address sensitive and drug resistant TB by: (a) reducing diagnostic delays, (b) reducing the
duration and improving the efficacy of treatment, (c) preventing disease, and (d) increasing
access to DOTS and DR-TB treatment, etc.
3- Invest in new diagnostic and TB management tools and approaches that are less labor
intensive, more cost-effective, and can be delivered close to patients to minimize the health
workforce burden and help improve patient access, thereby increasing case detection and
enhance treatment success rates.
4- Universal access to TB services, which implies expanding TB DOTS through all types of
healthcare providers including the large and currently unregulated private sector
151
5- Prioritize research that has the potential to change policy and practice in TB care in the
country.
The NSP vision 2020 entails achieving the following:
Vision: TB Free Pakistan
Mission: To ensure universal access to quality diagnosis and treatment for people with TB.
8.2 GOAL AND OBJECTIVES: Goal: To reduce 50%, the prevalence of TB by 2025 in comparison to 2012.
Objectives:
i) To increase the number of notified TB cases from 298,981 in 2013 to at least 420,000 by
2020 while maintaining the treatment success rate above 90%;
ii) To reduce, by at least 5% per year by 2020, the prevalence of MDR-TB among TB patients
who have never received any TB treatment
iii) Strengthen programmatic and operational management capacity of the TB Control Program
while enhancing public sector support for TB control by 2020;
8.3 PRIORITY PROGRAM AREAS:
For objective 1, the priority program areas are:
Increase gradually the number of suspects evaluated for TB from 839,371 in 2013 to
3,320,000 in 2020; the ratio number of suspects evaluated to identify 1 bacteriologically
confirmed pulmonary TB case was 7.5 in 2013; this ratio will progressively increase to 8 in
2014, 10 to 2015, 12 in 2016, 15 in 2017, 2018 and 2019 and 16 in 2020
Increase the number of bacteriologically confirmed TB cases who are notified from
111,916 in 2013 to 208,000 in 2020; the proportion of bacteriologically confirmed
pulmonary TB cases among all notified new pulmonary TB cases is 48% in 2013; in order
to improve the quality of TB diagnosis this proportion will gradually increase to reach at
least 70% from 2017 onwards (72% in 2020)
Ensure uninterrupted TB drug supplies through the improvement of TB drug
management at national, provincial and district levels
Enhance case-holding when TB patients are on treatment
152
Improve and expand TB contact investigation
Expand childhood TB case management
Improve the organization of TB care and control services within tertiary care level
hospitals as well as their linkages with their external health environment
Design and implement advocacy and awareness activities for policy makers, communities
and TB patients and their families
Improve training capacity and develop human resource development at national,
provincial and district level
Improve TB detection in elderlies
Improve TB detection and management in coal miners
Improve TB care and control services in vulnerable populations: slums’ dwellers,
internally displaced people/refugees and brick kiln workers
Strengthen and scale up TB/HIV collaborative activities
Improve co-management of TB and chronic conditions (diabetes and tobacco smoking)
Implement PAL
Optimizing and enhancing TB laboratory network: from 1,365 in 2013 to
1,953 AFB microscopy laboratories in 2020
Increase the number of Xpert machines from 43 in 2013 to 70 in 2020
Increase the number of laboratories performing culture from 10 in 2013 to 30in 2020 and
the number de DST sites from 2 in 2013 to 15 in 2020
Expand partnerships with private sector in an effort to engage all health care providers in
delivering quality diagnostic and treatment services for TB control in Pakistan; the
contribution of the private health sector in TB notification is expected to increase from
20% in 2013 to at least 35% in 2017onwards.
153
For objective 2, the priority program areas are:
Optimizing drug-resistant (DR) TB management by increasing the number of MDR-TB
cases to be detected and managed from 1,560 MDR-TB cases in 2013 to 14,316in 2020
Sustaining 30 PMDT sites in the country
Strengthen and expand TB infection control
Ensure social support for MDR-TB patients
Establish a sentinel surveillance system in 2018 to monitor the trend over time of MDR-
TB prevalence among TB cases who has never received any TB treatment
For objective 3, the priority program areas are:
Revitalization of the National Stop TB Partnership Pakistan (created in 2006)
Mobilization of public funding for TB control included as a top priority in the agenda of
National Stop TB Partnership Pakistan including formulation of respective provincial and
regional PC-1s.
Advocacy by National Stop TB Partnership Pakistan for increasing public TB funding in the
sub-committees for Health of the Senate and the National Assembly of Pakistan; this will
enhance at federal level the allocation by the Council of Common Interest for TB control
funding
Advocacy by National Stop TB Partnership Pakistan for increasing public TB funding
through the 60 medical doctors who are members of the Senate and the National
Assembly; this will contribute to sensitizing the members of the sub-Committees for
Health of the Senate and the National Assembly of Pakistan as well as the members of
the Council of Common Interest
Advocacy by National Stop TB Partnership Pakistan for increasing public TB funding in the
sub-committees for Health of the Provincial and Regional Assemblies; this will help
improve the funding allocation for TB control in the provinces and regions.
Strengthen the managerial capacities at national, provincial and regional levels, including
of recruitment of technical and operational staff (coordination of various program
components, finance, administration, etc)
Development of operational research activities to address programmatic needs
Staff coordination meetings on quarterly basis at all levels
Organize the supervision of TB control activities
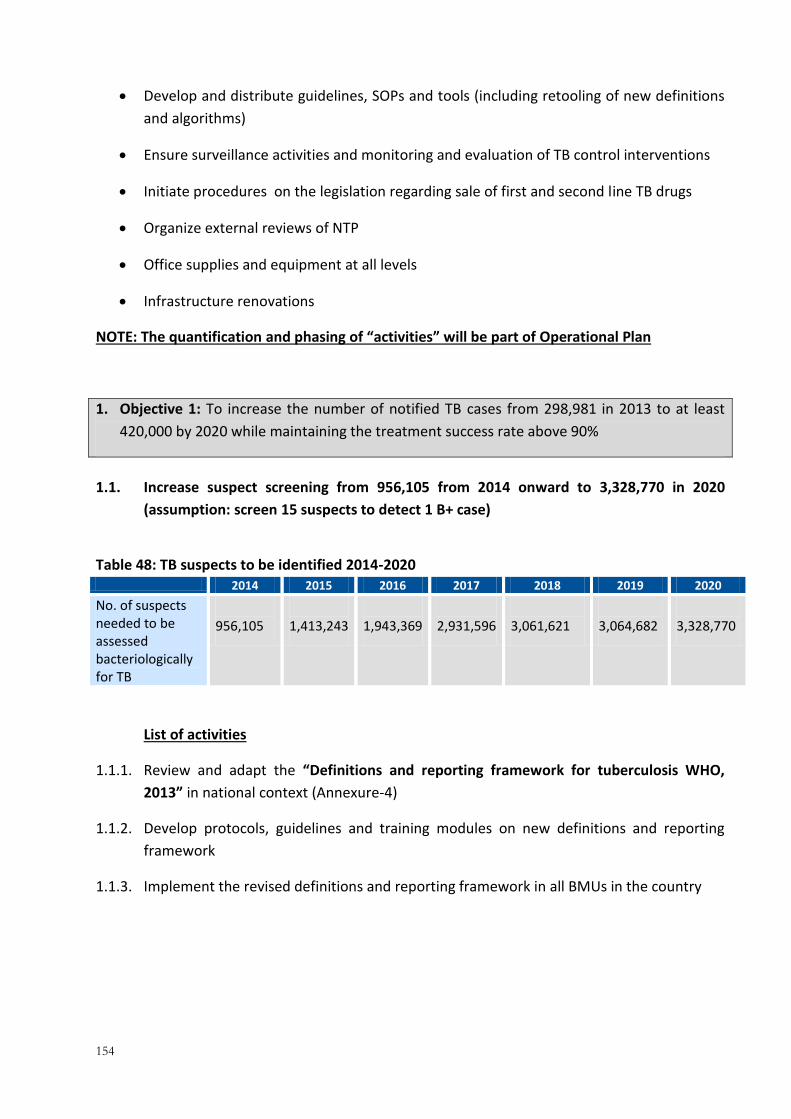
154
Develop and distribute guidelines, SOPs and tools (including retooling of new definitions
and algorithms)
Ensure surveillance activities and monitoring and evaluation of TB control interventions
Initiate procedures on the legislation regarding sale of first and second line TB drugs
Organize external reviews of NTP
Office supplies and equipment at all levels
Infrastructure renovations
NOTE: The quantification and phasing of “activities” will be part of Operational Plan
1. Objective 1: To increase the number of notified TB cases from 298,981 in 2013 to at least
420,000 by 2020 while maintaining the treatment success rate above 90%
1.1. Increase suspect screening from 956,105 from 2014 onward to 3,328,770 in 2020
(assumption: screen 15 suspects to detect 1 B+ case)
Table 48: TB suspects to be identified 2014-2020 2014 2015 2016 2017 2018 2019 2020
No. of suspects needed to be assessed bacteriologically for TB
956,105
1,413,243
1,943,369
2,931,596
3,061,621
3,064,682
3,328,770
List of activities
1.1.1. Review and adapt the “Definitions and reporting framework for tuberculosis WHO,
2013” in national context (Annexure-4)
1.1.2. Develop protocols, guidelines and training modules on new definitions and reporting
framework
1.1.3. Implement the revised definitions and reporting framework in all BMUs in the country

155
1.2. Increase bacteriologically confirmed case notification of pulmonary TB cases from
119,513 in 2012 to at least 208,048 in 2020 (assumption: average annual increase of
7.5%)
Table 49: TB cases projection 2014-2020
2014 2015 2016 2017 2018 2019 2020
Population (Projected, million)
185 188 191 193 197 200 203
All Type Cases Notified
313,930 337,475 362,785 377,297 382,956 383,339 379,506
Pulmonary TB cases
Total number of new pulmonary TB cases bacteriologically confirmed
119,513 141,324 161,947 195,440 204,108 204,312 208,048
Total number of new pulmonary TB cases clinically diagnosed
119,513 115,629 107,965 83,760 87,475 87,562 80,908
EPTB cases
Total new extra-pulmonary cases notified
56,068 60,273 67,478 69,800 68,396 68,464 67,780
List of activities
1.2.1. Review and adapt the approaches and algorithms “Systematic screening for active
tuberculosis: Principles and recommendation WHO, 2013” in the national context
(Annexure-5)and “Improving the diagnosis of smear negative and extra-pulmonary TB
among adults and adolescents, WHO”.(Annexure -11)
1.2.2. Re-design roles of various care providers in implementing new approaches and
algorithms
1.2.3. Develop protocols, guidelines and training modules on new approaches and algorithms
1.2.4. Implement the adapted version of algorithms in all BMUs in the country
1.2.5.
1.3. Increase the treatment success rate from 92% in 2014 while maintaining it to 93%in
2020

156
Table 50: TB treatment success projection 2014-2020
2014 2015 2016 2017 2018 2019 2020
Treatment success rates among new smear positive cases and/or culture-positive (%)
92% 92% 93% 93% 93% 93% 93%
List of activities
1.3.1. Develop innovative approaches to improve treatment success rate
1.3.2. Develop protocols, guidelines and tool to implement innovative approaches to increase treatment success
1.3.3. Train 80,000 LHWs in offering treatment support arrangement in all over the country.
1.3.4. Develop mechanism and guidelines to monitor treatment support activities.
1.3.5. Implement treatment support protocols in 141 districts in the country in both the public as well as the private sector.
1.3.6. Consider other types of treatment support arrangement such as family DOT, etc.
1.3.7. Consider incentives for patients especially sputum smear positive cases in intensive phase of treatment.
1.3.8. Involve high school students in patient support
1.3.9. Involve community volunteers in patient support
1.4. Increase contact management from 246,989 in 2014 to 1,156,973 2020 (assumption:
with annual increases in proportion of index case to be investigated from 0.3 in 2014 to
0.8 in 2020)
Table 51: Contact management projection 2014-2020
2014 2015 2016 2017 2018 2019 2020
Proportion of Index cases to be investigated
30
50
60
70
80
80
80
No. of HH contacts eligible for screening
823,297
979,503
1,148,132
1,390,590
1,419,276
1,420,695
1,446,216
No. of HH contacts to be screened (6 contacts/HH)
246,989
489,751
688,879
973,413
1,135,421
1,136,556
1,156,973
No. of HH contacts less than 5 years eligible for IPT
30,874
61,219
86,110
121,677
141,928
142,070
144,622
No. of HH contacts <5 years that need to be treated by IPT
30,565
60,607
85,249
120,460
140,508
140,649
143,175
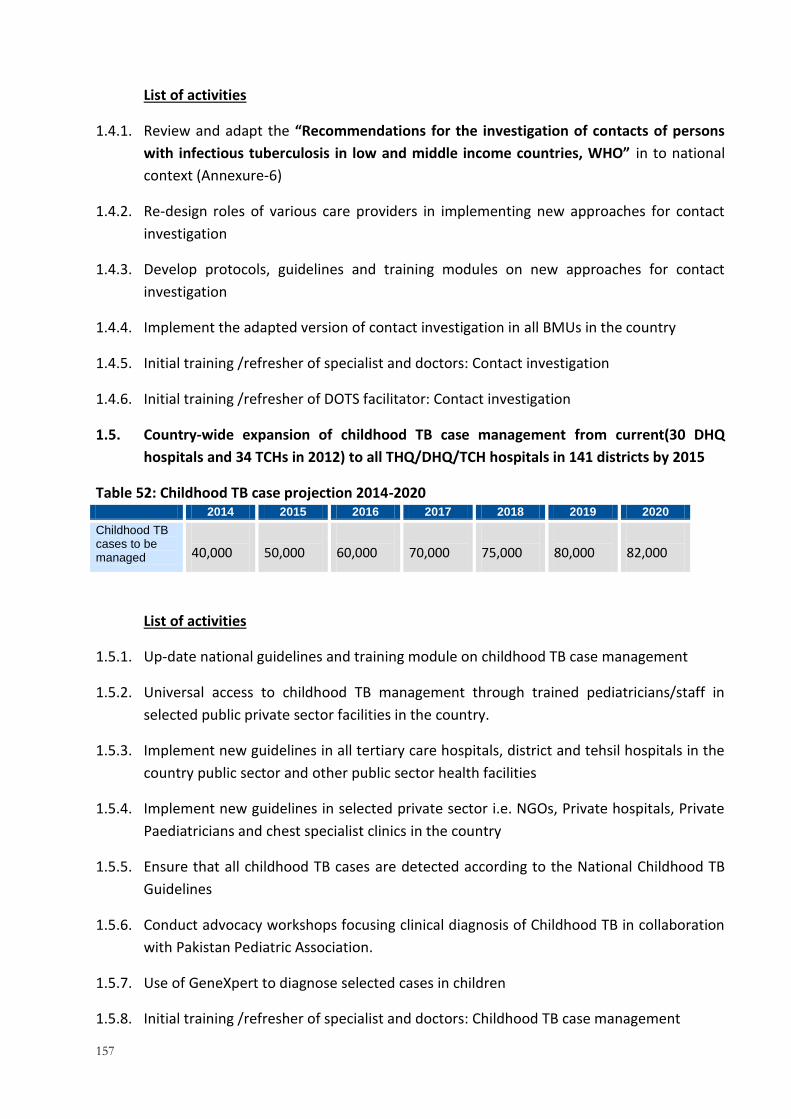
157
List of activities
1.4.1. Review and adapt the “Recommendations for the investigation of contacts of persons
with infectious tuberculosis in low and middle income countries, WHO” in to national
context (Annexure-6)
1.4.2. Re-design roles of various care providers in implementing new approaches for contact
investigation
1.4.3. Develop protocols, guidelines and training modules on new approaches for contact
investigation
1.4.4. Implement the adapted version of contact investigation in all BMUs in the country
1.4.5. Initial training /refresher of specialist and doctors: Contact investigation
1.4.6. Initial training /refresher of DOTS facilitator: Contact investigation
1.5. Country-wide expansion of childhood TB case management from current(30 DHQ
hospitals and 34 TCHs in 2012) to all THQ/DHQ/TCH hospitals in 141 districts by 2015
Table 52: Childhood TB case projection 2014-2020 2014 2015 2016 2017 2018 2019 2020
Childhood TB cases to be managed
40,000
50,000
60,000
70,000
75,000
80,000
82,000
List of activities
1.5.1. Up-date national guidelines and training module on childhood TB case management
1.5.2. Universal access to childhood TB management through trained pediatricians/staff in
selected public private sector facilities in the country.
1.5.3. Implement new guidelines in all tertiary care hospitals, district and tehsil hospitals in the
country public sector and other public sector health facilities
1.5.4. Implement new guidelines in selected private sector i.e. NGOs, Private hospitals, Private
Paediatricians and chest specialist clinics in the country
1.5.5. Ensure that all childhood TB cases are detected according to the National Childhood TB
Guidelines
1.5.6. Conduct advocacy workshops focusing clinical diagnosis of Childhood TB in collaboration
with Pakistan Pediatric Association.
1.5.7. Use of GeneXpert to diagnose selected cases in children
1.5.8. Initial training /refresher of specialist and doctors: Childhood TB case management
158
1.5.9. Initial training /refresher of DOTS facilitator: Childhood TB case management
1.5.10. Ensure availability of simple drug dosages according to pediatric formulations.
1.5.11. Effective supply chain management for PPD(Despite poor diagnostic value, PPD is still
recommended by WHO as initial tool and should continue as such; Positive test HELPS
but negative does not exclude)
1.6. Strengthen Hospital DOTS internal and external linkage in all tertiary care hospitals by
2015
1.6.1. Scale up TB DOTS implementation including pulmonary and extra-pulmonary and
childhood TB management in TCHs and DHQs
1.6.2. Strengthen bacteriological diagnosis of extra-pulmonary and childhood TB at the TCH and
DHQs
1.6.3. Implement ACSM interventions in the TCH and DHQ settings
1.6.4. Streamline external linkage mechanisms with public and private peripheral TB care
services, including strengthening of pre-registration referral to the BMU nearest to the
patient residence
1.6.5. Advocacy with the provincial Department of Health, hospital management, senior
consultants and specialists
1.6.6. Build capacity of staff of relevant departments within the hospital
1.6.7. Implement strong M&E systems to measure performance, identify challenges and
implement solutions
1.7. ACSM strategy to be re-designed and require focused implementation
List of activities
1.7.1. Review and refine the current model of ACSM in country
1.7.2. Implement focused ACSM intervention for TB patients including DR-TB cases
1.7.3. Involve electronic and print media in advocacy
1.7.4. Community events in mobilizing TB patients
1.7.5. National level events: high-level discussions around TB
159
1.7.6. Field visits for high-level officials or journalists
1.7.7. Production of IEC materials to improve knowledge of TB in the general population
1.7.8. Mass media campaigns: Broadcast materials (Public Service Announcement)
1.7.9. Initial training /refresher of specialist and doctors: ACSM
1.7.10. Initial training /refresher of DOTS facilitator: Community involvement
1.7.11. Initial training /refresher of DOTS facilitator: Advocacy and Communication
1.7.12. Initial training /refresher of community health workers/volunteers: Community
involvement
1.7.13. Initial training /refresher of community health workers/volunteers: Advocacy and
Communication
1.8. Improve drug management at national, provincial and district levels
List of activities
1.8.1. First-line drug procurement and management
1.8.2. Second-line drug procurement and management. “The use of bedaquiline in the
treatment of MDR-TB, WHO 2012”. (Annexure-12)
1.8.3. Strengthen and sustain the national, provincial and district capacity to store drugs (FLDs
and SLDs)
1.8.4. Strengthen and sustain the logistics for transporting drugs to all BMUs and PMDT sites in
the country
1.8.5. Up gradation of BA/BE study center as per WHO standards “A practical handbook on the
pharmaco-vigilance of medicines used in the treatment of Tuberculosis enhancing the
safety of the TB patient-WHO, 2012”.Annexure 7
1.8.6. Support PTPs to develop their BA/BE stud centers.
1.8.7. Monitor and evaluate the implementation.
1.8.8. Initial training /refresher of managers and TB coordinators at all level: drug management
1.9. Improve training capacity and develop human resource development (HRD) at national,
provincial and district
List of activities
1.9.1. Training (at national and international level) of managers and coordinators at national,
provincial and district level: Program management and operational research on technical
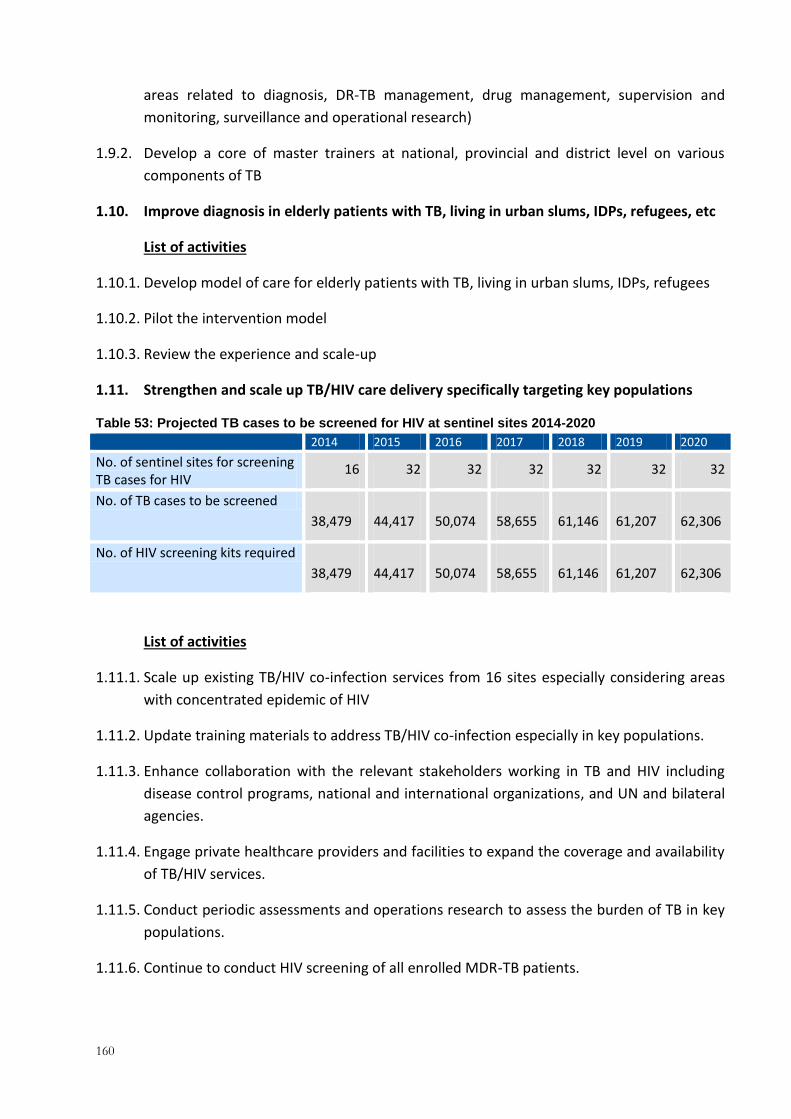
160
areas related to diagnosis, DR-TB management, drug management, supervision and
monitoring, surveillance and operational research)
1.9.2. Develop a core of master trainers at national, provincial and district level on various
components of TB
1.10. Improve diagnosis in elderly patients with TB, living in urban slums, IDPs, refugees, etc
List of activities
1.10.1. Develop model of care for elderly patients with TB, living in urban slums, IDPs, refugees
1.10.2. Pilot the intervention model
1.10.3. Review the experience and scale-up
1.11. Strengthen and scale up TB/HIV care delivery specifically targeting key populations
Table 53: Projected TB cases to be screened for HIV at sentinel sites 2014-2020 2014 2015 2016 2017 2018 2019 2020
No. of sentinel sites for screening TB cases for HIV
16 32 32 32 32 32 32
No. of TB cases to be screened
38,479
44,417
50,074
58,655
61,146
61,207
62,306
No. of HIV screening kits required
38,479
44,417
50,074
58,655
61,146
61,207
62,306
List of activities
1.11.1. Scale up existing TB/HIV co-infection services from 16 sites especially considering areas
with concentrated epidemic of HIV
1.11.2. Update training materials to address TB/HIV co-infection especially in key populations.
1.11.3. Enhance collaboration with the relevant stakeholders working in TB and HIV including
disease control programs, national and international organizations, and UN and bilateral
agencies.
1.11.4. Engage private healthcare providers and facilities to expand the coverage and availability
of TB/HIV services.
1.11.5. Conduct periodic assessments and operations research to assess the burden of TB in key
populations.
1.11.6. Continue to conduct HIV screening of all enrolled MDR-TB patients.
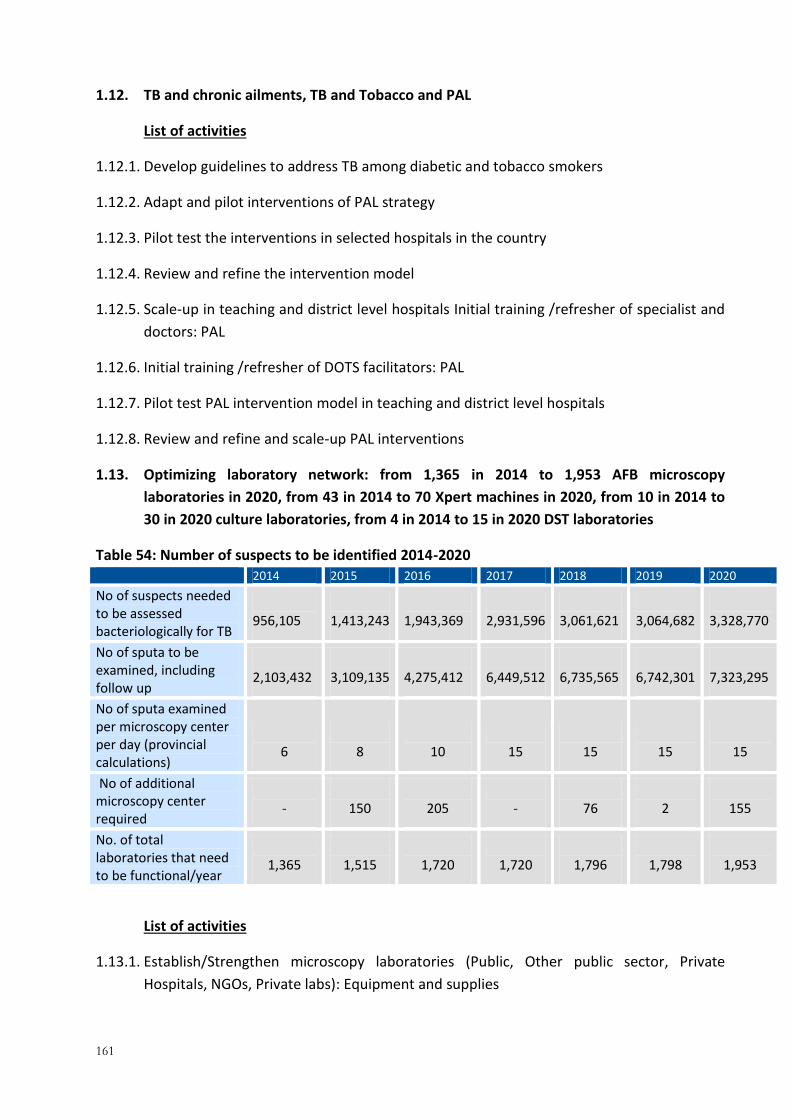
161
1.12. TB and chronic ailments, TB and Tobacco and PAL
List of activities
1.12.1. Develop guidelines to address TB among diabetic and tobacco smokers
1.12.2. Adapt and pilot interventions of PAL strategy
1.12.3. Pilot test the interventions in selected hospitals in the country
1.12.4. Review and refine the intervention model
1.12.5. Scale-up in teaching and district level hospitals Initial training /refresher of specialist and
doctors: PAL
1.12.6. Initial training /refresher of DOTS facilitators: PAL
1.12.7. Pilot test PAL intervention model in teaching and district level hospitals
1.12.8. Review and refine and scale-up PAL interventions
1.13. Optimizing laboratory network: from 1,365 in 2014 to 1,953 AFB microscopy
laboratories in 2020, from 43 in 2014 to 70 Xpert machines in 2020, from 10 in 2014 to
30 in 2020 culture laboratories, from 4 in 2014 to 15 in 2020 DST laboratories
Table 54: Number of suspects to be identified 2014-2020 2014 2015 2016 2017 2018 2019 2020
No of suspects needed to be assessed bacteriologically for TB
956,105
1,413,243
1,943,369
2,931,596
3,061,621
3,064,682
3,328,770
No of sputa to be examined, including follow up
2,103,432
3,109,135
4,275,412
6,449,512
6,735,565
6,742,301
7,323,295
No of sputa examined per microscopy center per day (provincial calculations)
6
8
10
15
15
15
15
No of additional microscopy center required
-
150
205
-
76
2
155
No. of total laboratories that need to be functional/year
1,365
1,515
1,720
1,720
1,796
1,798
1,953
List of activities
1.13.1. Establish/Strengthen microscopy laboratories (Public, Other public sector, Private
Hospitals, NGOs, Private labs): Equipment and supplies

162
1.13.2. Establish/ Strengthen LED microscopy laboratories (Public, Other public sector, Private
Hospitals, NGOs, Private labs): Equipment and supplies
1.13.3. Initial training/refresher of laboratory technicians (Public Sector): AFB microscopy
1.13.4. Initial training/refresher of laboratory technicians (Other public sector Sector): AFB
microscopy
1.13.5. Initial training/refresher of laboratory technicians (Private Hospitals): AFB microscopy
1.13.6. Initial training/refresher of laboratory technicians (NGOs): AFB microscopy
1.13.7. Initial training/refresher of laboratory technician (Private labs)s: AFB microscopy
1.13.8. Initial training/refresher of laboratory technicians (Public Sector): LED microscopy
1.13.9. Initial training/refresher of laboratory technicians (Other public sector): LED microscopy
1.13.10. Initial training/refresher of laboratory technicians (Private Hospitals): LED
microscopy
1.13.11. Initial training/refresher of laboratory technicians (NGOs ): LED microscopy
Table 55: Number of GeneXpert machines required 2014-2020 2014 2015 2016 2017 2018 2019 2020
No. of tests to be done on GeneXpert
59,612
92,849
148,801
206,448
208,771
208,979
213,004
No. of total GeneXpert machines required
20
31
50
69
70
70
71
No. of GeneXert machines available
43
43
43
50
69
70
70
No. of additional GeneXpert machines needed
0 0 7 19 1 0 1
1.13.12. Establish/strengthen Xpert sites (Public, Other public sector, Private Hospitals,
NGOs):
1.13.13. Structure enhancement, equipment and suppliesPurchase additional Gene-Xpert
machines to implement in the selected centers by 2020 .
1.13.14. Purchase cartridges for Xpert machines for continued DR-TB care. Purchase
additional equipment and materials to establish sites.
1.13.15. Train human resource to conduct Xpert tests.

163
Table 56: Number of culture laboratories required 2014-2020 2014 2015 2016 2017 2018 2019 2020
No. of cultures to be done
79,517
118,619
160,019
230,937
239,299
239,538
251,964
No. of laboratories required for culture (8,000 cultures/lab/year)
10
15
20
29
30
30
31
No. culture laboratories available
10
23
23
23
29
30
30
No. of additional culture laboratories needed
0 0 0 6 1 0 1
1.13.16. Establish/strengthen culture laboratories (Public, Other public sector, Private
Hospitals, NGOs): Structural enhancement, equipment and supplies
1.13.17. Purchase equipment and supplies to establish culture laboratories in the selected
centers by 2020
1.13.18. Infrastructure enhancement for new culture laboratories
1.13.19. Initial training/refresher of laboratory technicians (Public Sector): Culture
1.13.20. Initial training/refresher of laboratory technicians (Other public sector): Culture
1.13.21. Initial training/refresher of laboratory technicians (Private Hospitals): Culture
1.13.22. Initial training/refresher of laboratory technicians (NGOs): Culture
Table 57: Number of DST laboratories required 2014-2020 2014 2015 2016 2017 2018 2019 2020
No. of DST to be carried out
4,970 7,414 10,001 14,434 14,956 14,971 15,748
No. of DST laboratories required
5 7 10 14 15 15 16
No. DST laboratories available
4 5 7 10 14 15 15
No. of additional DST laboratories needed
1 2 3 4 1 0 1
1.13.23. Establish/strengthen laboratories performing molecular tests (Public, Other public
sector, Private Hospitals): Structural enhancement, equipment and supplies
1.13.24. Infrastructure enhancement for new culture laboratories

164
1.13.25. Purchase equipment and supplies to establish DST laboratories in the selected
centers by 2020
1.13.26. Initial training/refresher of laboratory technicians (Public Sector): DST
1.13.27. Initial training/refresher of laboratory technicians (Other public sector): DST
1.13.28. Initial training/refresher of laboratory technicians (Private Hospitals): DST
1.13.29. Initial training/refresher of laboratory technicians (NGOs): DST
1.13.30. Initial training/refresher of laboratory technicians (Public Sector): molecular test
1.13.31. Establish/strengthen EQA for microscopy, LED, Xpert, culture, DST, molecular
testing (Public, Other public sector, Private Hospitals, NGOs, Private labs): Human
Resource, Logistics, Equipment and supplies
1.14. Expand partnerships with private sector in an effort to engage all healthcare providers
in delivering quality diagnostic and treatment services for TB control in Pakistan;
increasing contribution in total national TB case notification from 20% in 2012 to 32% in
2020
1.14.1. Policy advocacy at national and provincial level for appropriate policies, legislation and
regulatory framework for involving private sector providers
Table 58: Contribution projected for PPM in country 2014-2020 2014 2015 2016 2017 2018 2019 2020
TB Case notification (all ages, all forms)
313,930 337,475 362,785 377,297 382,956 383,339 379,506
Number of TB case notification from PPM intervention
69,065
84,369
108,836
120,735
122,546
122,669
121,442
Proportion of TB case notification from PPM intervention
22% 25% 30% 32% 32% 32% 32%
1.14.2. Establish and implement standardized training and quality assurance mechanisms
including ISTC through a central PPM Unit and provincial steering committees
Target audience: Private sector healthcare providers, NGO clinics and hospitals, pharmacies,
professional bodies, small and large private laboratories, corporate sector, philanthropy,
other public sector healthcare providers, Hakims and homeopaths, and informal healthcare
providers.

165
1.14.3. Implement ‘hard’ contracts with collaborating private sector providers/hospitals/NGO
clinics/other public sector organizations
1.14.4. Establish and implement accreditation and certification mechanisms
1.14.5. Incentivize collaboration of private providers and TB patients in TB control activities
1.14.6. Implement a robust system of monitoring and evaluation that employs modern
technology including m-Health for data recording and reporting in simplified formats, and
follow up and tracking of TB patients.
1.14.7. Address urban DOTS and TB in key populations (including urban slums, drug users, street
children, migrants and Madrassasetc.) through active case finding
1.14.8. Establish referral linkages with Xpert and PMDT sites
1.14.9. Engage pharmacies in identification and referral of presumptive TB cases and treatment
support
1.14.10. Support PPM interventions with a comprehensive and strategic advocacy and
communication campaign
1.14.11. Advocacy at the provincial level with the policy makers, policy implementers and
media
1.14.12. Awareness raising and advocacy with key stakeholders at the provincial and
national levels including professional bodies, specialists, hospitals, NGOs, corporate
sector companies, philanthropy, media etc.
1.14.13. Stop TB Coalitions at the district level
1.14.14. Communication at the local level about availability of services through
community-based media and local mass media
1.14.15. Use of mobile phones for raising awareness and ensuring adherence of the TB
patients to treatment
1.14.16. Conduct operations research to inform the design and implementation of the
PPM interventions, make course correction, and document and disseminate the results
166
2. Objective 2:To reduce, by at least 5% per year from 2018 onwards, the prevalence of MDR-
TB among New Pulmonary TB patients (who have never received any TB treatment)
2.1. Optimizing DR-TB management by detecting and managing 1,570 DR-TB cases from
2013 to 14,316 DR-TB cases in 2020
Based on the international recommendations of the Global Plan Every DR-TB case should have access to treatment by 2015 However, keeping the country situation and provincial caseload, the strategy For DR-TB case detection and management will be phased gradually to reach 100% by 2020. NTP will be using the following revised case finding strategies:
GROUP I: TB PATIENT / Symptomatic at risk of DR-TB
A. ALL RETREATMENT TB CASES: All TB cases (AFB SS+ve or negative) with history of previous ATT should be tested for Xpert at month zero of enrolment. This includes:
• Treatment Failure Cat-I (F-1)
• Treatment Failure Cat-II (F-2)
• Relapse after Cat-I (R-1)
• Relapse after Cat-II (R-2)
• Treatment after loss to follow up Cat-1(D-1)
• Treatment after loss to follow up Cat-II (D-2)
• Other Retreatment
B. SYMPTOMATIC CONTACTS OF DR-TB PATIENT:
All household and workplace symptomatic contacts of DR-TB patients should be screed for RRTB. Specimen from these individuals should be processed for AFB smear and then the specimen is referred for Xpert MTB/RIF assay irrespective of smear results.
C. TB PATIENTS UNDER TREATMENT WHO FAIL TO CONVERT AT THE END OF INTENSIVE PHASE
• AFB smear +ve patient on Cat-1 who fail to convert at the end of month #2 of treatment.
• AFB smear +ve patient on Cat- II who fail to convert at the end of 3 months.
• AFB smear negative Patient who is reported AFB smear positive at the end of intensive phase
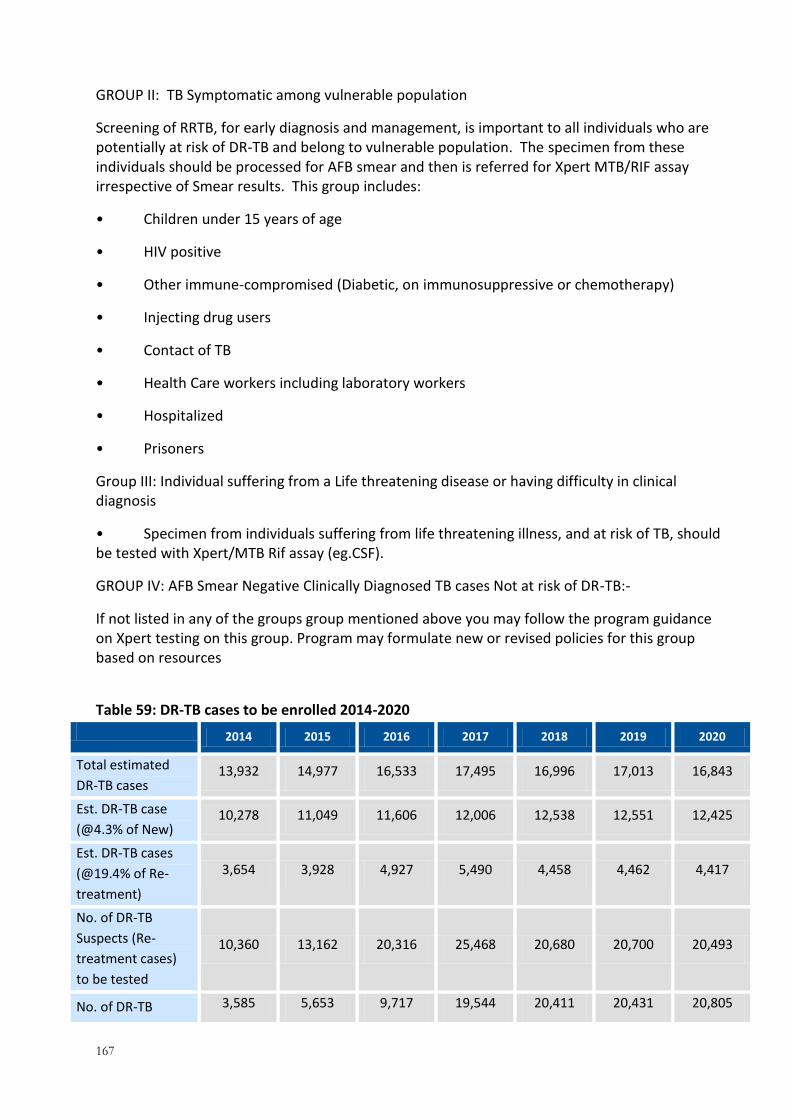
167
GROUP II: TB Symptomatic among vulnerable population
Screening of RRTB, for early diagnosis and management, is important to all individuals who are potentially at risk of DR-TB and belong to vulnerable population. The specimen from these individuals should be processed for AFB smear and then is referred for Xpert MTB/RIF assay irrespective of Smear results. This group includes:
• Children under 15 years of age
• HIV positive
• Other immune-compromised (Diabetic, on immunosuppressive or chemotherapy)
• Injecting drug users
• Contact of TB
• Health Care workers including laboratory workers
• Hospitalized
• Prisoners
Group III: Individual suffering from a Life threatening disease or having difficulty in clinical diagnosis
• Specimen from individuals suffering from life threatening illness, and at risk of TB, should be tested with Xpert/MTB Rif assay (eg.CSF).
GROUP IV: AFB Smear Negative Clinically Diagnosed TB cases Not at risk of DR-TB:-
If not listed in any of the groups group mentioned above you may follow the program guidance on Xpert testing on this group. Program may formulate new or revised policies for this group based on resources
Table 59: DR-TB cases to be enrolled 2014-2020
2014 2015 2016 2017 2018 2019 2020
Total estimated
DR-TB cases 13,932 14,977 16,533 17,495 16,996 17,013 16,843
Est. DR-TB case
(@4.3% of New) 10,278 11,049 11,606 12,006 12,538 12,551 12,425
Est. DR-TB cases
(@19.4% of Re-
treatment)
3,654 3,928 4,927 5,490 4,458 4,462 4,417
No. of DR-TB
Suspects (Re-
treatment cases)
to be tested
10,360 13,162 20,316 25,468 20,680 20,700 20,493
No. of DR-TB 3,585 5,653 9,717 19,544 20,411 20,431 20,805
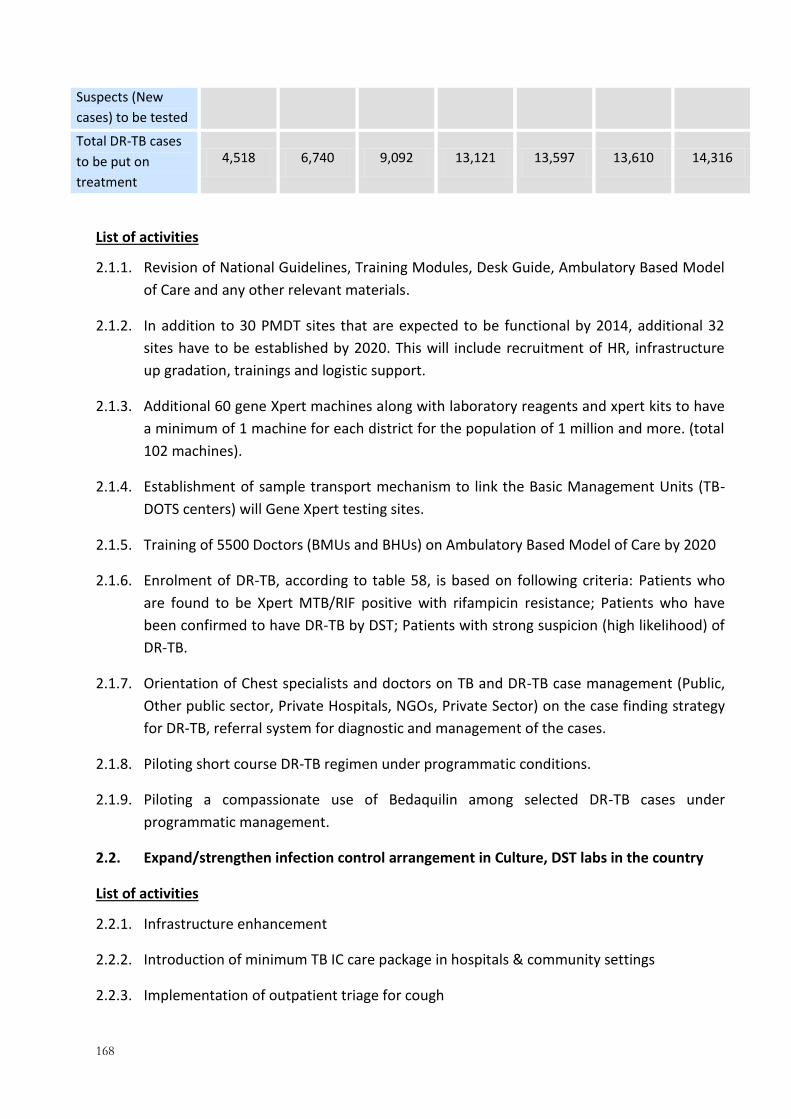
168
Suspects (New
cases) to be tested
Total DR-TB cases
to be put on
treatment
4,518 6,740 9,092 13,121 13,597 13,610 14,316
List of activities
2.1.1. Revision of National Guidelines, Training Modules, Desk Guide, Ambulatory Based Model
of Care and any other relevant materials.
2.1.2. In addition to 30 PMDT sites that are expected to be functional by 2014, additional 32
sites have to be established by 2020. This will include recruitment of HR, infrastructure
up gradation, trainings and logistic support.
2.1.3. Additional 60 gene Xpert machines along with laboratory reagents and xpert kits to have
a minimum of 1 machine for each district for the population of 1 million and more. (total
102 machines).
2.1.4. Establishment of sample transport mechanism to link the Basic Management Units (TB-
DOTS centers) will Gene Xpert testing sites.
2.1.5. Training of 5500 Doctors (BMUs and BHUs) on Ambulatory Based Model of Care by 2020
2.1.6. Enrolment of DR-TB, according to table 58, is based on following criteria: Patients who
are found to be Xpert MTB/RIF positive with rifampicin resistance; Patients who have
been confirmed to have DR-TB by DST; Patients with strong suspicion (high likelihood) of
DR-TB.
2.1.7. Orientation of Chest specialists and doctors on TB and DR-TB case management (Public,
Other public sector, Private Hospitals, NGOs, Private Sector) on the case finding strategy
for DR-TB, referral system for diagnostic and management of the cases.
2.1.8. Piloting short course DR-TB regimen under programmatic conditions.
2.1.9. Piloting a compassionate use of Bedaquilin among selected DR-TB cases under
programmatic management.
2.2. Expand/strengthen infection control arrangement in Culture, DST labs in the country
List of activities
2.2.1. Infrastructure enhancement
2.2.2. Introduction of minimum TB IC care package in hospitals & community settings
2.2.3. Implementation of outpatient triage for cough
169
2.2.4. Arrangement for collection of sputum outdoors or in separate, sufficiently ventilated
rooms
2.2.5. Arrangement for adequate ventilation in other consultation/examination areas, waiting
areas and TB wards
2.2.6. Isolation of TB patients in separate inpatient TB wards
2.2.7. All-staff training about TB, TB infection control, and the clinic’s TBIC implementation plan
2.2.8. Development of TB IC software to monitor monthly implementation of TB IC practices
including; For IC M&E of clinical sites, administrative/ environmental controls & PPE
usages (Hand Hygiene Survey , Staff Risk Assessment Log), and to Measure and Compare
Quality of Services / Time Spent in the Facility
2.2.9. Monitoring of health facilities implementing infection control intervention and
surveillance of HCWs
2.2.10. Data verification form HCFs on quarterly basis
2.2.11. Develop a confidential data collection system for TB disease among staff and a means to
share the aggregate data with the workers.
2.2.12. Develop a case notification & data collection system and tools i.e. TB registry, staff risk
assessment forms, analysis reports.
2.2.13. Identify and train persons responsible for confidential recording, collecting and reporting,
importance of prompt disease notification, stigma reduction and support for their ill
colleague(s).
2.2.14. Identify role-models to give talks to others.
2.2.15. Evaluate the impact of control measures and if needed re-adjust interventions.
2.2.16. Identify and plan technical assistance priorities in DR-TB control.
2.2.17. Identify and arranging financial resources for provision of technical assistance in priority
areas
2.2.18. Initial training /refresher of specialist and doctors: Infection control
2.2.19. Initial training /refresher of DOTS facilitator: Infection control
2.2.20. Initial training /refresher of Laboratory technician at microscopy centres: Infection
control
2.2.21. Initial training /refresher of Laboratory technician at culture laboratories: Infection
control
170
2.2.22. Initial training /refresher of Laboratory technician at DST laboratories: Infection control
2.3. Increase and improve social support/incentives for patients and care provides 1,570 DR-
TB cases from 2013 to 14,316 DR-TB cases in 2020
List of activities
2.3.1. Conduct situational analysis to assess the quality of services and delivery mechanism of
social support needs to be developed
2.3.2. Qualitative research, involving focus groups, is needed to identify gaps and needs of the
patients and care/service providers in order to assess their needs and jointly plan
support
2.3.3. Development of operational guidelines/SOPs, on the basis of identified gaps, is needed in
order to improve quality of services of social support.
2.3.4. Secure additional funds to bring required changes and improvement in the incentives and
food basket items (by revising the budget of social support in line with agreement of GF)
3. Objective 3: To optimize and sustain the programmatic deliverables (technical and
managerial) at operational level by 2018
3.1. Recruitment of technical and operational staff (coordination of various program
components, finance, administration etc)
3.2. NTP to secure public sector support through PC-1
List of activities
3.2.1. Develop PC-1 to support development, implementation and research activities
3.2.2. Advocacy with key stakeholders to sensitize them for approval and release of PC-1 funds
3.2.3. Effective implementation of the operational plan through PC-1 support

171
3.3. NTP to secure support from international donors
3.4. Coordinate with international technical and donor agencies (Global Fund, USAID, DFID,
KFW, etc)
3.5. Increase international technical and donor assistance to meet the financial gaps for TB
control activities at all levels
3.6. Provincial and Regional TB control programs to develop and operationalize PC-1s in
context of devolution context
3.7. Develop PC-1 to support development, implementation and research activities
3.8. Advocacy with key stakeholders to sensitize them for approval and release of PC-1
funds
3.9. Effective implementation of operational plan through PC-1 support
3.10. District health authorities to delegate funds for TB control activities in districts
3.11. Secure 5-10% of the total budgetary allocation for procurement of quality assured ATT
drugs
3.12. Adequate support to the district TB team (EDO/MS/DoH/DDoH/DTC/DLS/Cross-
checker) for monitoring and supervision
3.13. Design and implement operational research activities i.e. at least 2 operational
research projects at national and same number in each province every year
List of activities
3.13.1. Develop national TB policy on operation research. “Priorities for Tuberculosis Research,
WHO”. (Annexure-7)
3.13.2. Develop and implement operational research projects
3.13.3. Strengthen provincial TB control staff in implementing operational research projects
3.13.4. Establish partnerships with research academic institution nationally and internationally
3.14. Staff coordination meetings on quarterly basis at all levels including supervision,
monitoring and evaluation
List of activities
3.14.1. Sustain the functions of the National and Provincial Technical Unit to manage M&E
activities in the country

172
3.14.2. Sustain IACC meetings.
3.14.3. Plan and arrange for timely preparation and dissemination of annual provincial and
national progress reports.
3.14.4. Sustain the support for field monitoring activities of the program and the district staff.
This also includes mobility support, staff training, and technical assistance.
3.14.5. National level (Quarterly Inter-Provincial Meetings)
3.14.6. Provincial level (Quarterly Inter-District Meetings)
3.14.7. District level(Quarterly Intra-District Meetings)
3.15. Development, production and distribution of guidelines and tools(including retooling of
new definitions/algorithms)
List of activities
3.15.1. Guidelines development - consultations and/or workshops
3.16. Design and implement operational research on priority program needs.
List of activities
3.16.1. Pilot of GIS based e DOTS and scale up
3.16.2. Operational Research on the diagnostic centre and treatment centre link model to
improve community management of MDR
3.16.3. Pilot of infection control strategies in household and community level and then scale up.
3.16.4. Innovative strategies to enhance yield from contact tracing among sensitive and resistant
TB.
3.16.5. Inventory study will be done in 2016 again to re-estimate the disease burden in the
country
3.16.6. Operational research on involvement of Pharmacies in TB control
3.16.7. Sustain and expand linkages with other international institutions
3.17. Surveillance activities
List of activities
3.17.1. Integrate e-surveillance with current paper based system in all BMUs in the country.
“Electronic recording and reporting for TB care and control, WHO 2012”. Annex-8
3.17.2. Train human resource in BMUs in all 141 districts on e-surveillance
173
3.17.3. Train human resource in all 141 districts in the country.
3.17.4. Build provincial level capacity in DMIS.
3.17.5. Monitor the quality of implementation.
3.18. Legislation for ban over the counter sale of anti-TB drugs both FLD and SLD.
List of activities:
3.18.1. Develop plan of action to ban counter sale of anti-TB drugs with the pharmaceutical
society
3.18.2. Advocacy with key stakeholders
3.18.3. Develop counter sale ban policy in collaboration with stakeholders.
3.18.4. Implement ban policy.
3.19. Review by third party
3.20. Transportation (New vehicles, maintenance i.e. old and new, fuel i.e. old and new)
3.21. Office supplies and equipment at all levels
List of activities
3.21.1. Procurement/provision at National level
3.21.2. Procurement/provision at Provincial level
3.21.3. Procurement/provision at District level including BMUs
3.22. Infrastructure new and renovations
List of activities
3.22.1. National level (DST/Culture/Gene-Xpert/Drugs)
3.22.2. Provincial level (DST/Culture/Gene-Xpert/Drugs)
3.22.3. District level/BMUs (Gene-Xpert/Drugs)

174
9 LIST OF LITERATURE REVIEWED (REFERENCES AND ANNEXURES)
1. United Nations Development Program, HDI report 2007-08
2. National Health Accounts 2009-2010, Pakistan Bureau of Statistics, Government of Pakistan
3. Eliminating the financial hardship of TB via universal health coverage and other social
protection measures: WHO, 2013.
4. National Institute of Population Studies, Government of Pakistan, 2012
5. Pakistan Health Profile, WHO, 2013
6. Ministry of Health, Government of Pakistan, Year book 2009
7. Nishtar, S 2006, p s61
8. WHO Global Tuberculosis Report 2012
9. WHO. Global Tuberculosis Control; WHO Report 2013
10. WHO. Tuberculosis Profile, Pakistan 2011
11. Sanjay Basu, etal.Projected effects of tobacco smoking on worldwide tuberculosis control:
mathematical modeling analysis. BMJ, 2011
12. National TB Control Pakistan, Data base 2011
13. Third-party evaluation of NTP, TRF 2011
14. Pakistan TB ACSM mid-term evaluation report , Mercy Corps, 2011
15. ACSM National Strategy and Operational Guidelines, NTP-MoH, 2010
16. National Guidelines for PMDT, 2011, NTP-Pakistan
17. Gesine Meyer-Rath, etal. The Impact and Cost of Scaling up GeneXpert MTB/RIF in South
Africa, PloS 2012
18. MDR-TB fact sheet, WHO, 2013
19. Ejaz M et al, Prevalence of multi-drug resistant tuberculosis in Karachi, Pakistan:
identification of at risk groups. Trans R Soc Trop Med Hyg 2010
20. H.K.Khoharo, et al, Drug resistance patterns in pulmonary tuberculosis, JPMA, 2011
21. National MDR Expansion Plan for 2013 – 2017, NTP Pakistan
22. NTP Pakistan, National Guidelines for Public Private Mix in TB-DOTS
23. SamiaIqbal, etal, Challenges faced by general practitioners in Pakistan in management of
tuberculosis: a qualitative study. Rawal Medical Journal, 2013
24. Sven GudmundHinderaker, Razia Fatima, Lost in time and space: the outcome of patients
transferred out from large hospitals, Public Health Actions, 2013
25. DOTS Expansion Working Group Strategic Plan 2 0 0 6 – 2 0 1 5, WHO/STOP TB partnership
175
26. Joint Review of Global Fund Grants 6 & 9 in Pakistan, July 2012
27. German - Pakistan Technical Cooperation Support for Tuberculosis Control - GIZ/AGEG PPM
Situation Analysis, 2013
28. Strategic plan for the prevention and control of multidrug-resistant and extensively drug-
resistant tuberculosis in the Eastern Mediterranean Region (2010–2015) , WHO
29. Narrowing the gap: Expanding access to new diagnostics for patients at risk of multi-drug
resistant tuberculosis (MDR-TB), World Health Organization, Global Laboratory Initiative
Foundation for Innovative New Diagnostics, Global Drug Facility, 2012
30. Multi-Drug Resistant Tuberculosis (MDR-TB) Indicators.A minimum set of indicators for the
programmatic management of MDR-TB in national tuberculosis control programs, WHO 2010
31. Management of Multidrug-Resistant Tuberculosis in Children: A Field Guide. USAID, TB Care
II, 2012
32. Definitions and reporting framework for tuberculosis WHO, 2013
33. Systematic screening for active tuberculosis: Principles and recommendation WHO, 2013
34. Improving the diagnosis of smear negative and extra-pulmonary TB among adults and
adolescents, WHO
35. Recommendations for the investigation of contacts of persons with infectious tuberculosis in
low and middle income countries, WHO
36. The use of bedaquiline in the treatment of MDR-TB, WHO 2012
37. A practical handbook on the pharmaco-vigilance of medicines used in the treatment of
Tuberculosis enhancing the safety of the TB patient-WHO, 2012
38. National Guidelines for PPM-NTP Pakistan
39. Guidelines for the programmatic management of DR-TB, WHO 2011
40. Priorities for Tuberculosis Research, WHO
41. Electronic recording and reporting for TB care and control, WHO 2012
42. Guidelines for clinical and operational management of DR-TB, Union.2013
176
SECTION B –
BUDGET SUMMARY

2014 2015 2016 2017 2018 2019 2020 Total
1. Improving diagnosis $
7,952,543 $
9,603,232 $
12,860,708 $
20,579,485 $
18,653,639 $
18,148,021 $
20,002,247 $
107,799,875
2. Patient support $
6,375,802 $
9,511,121 $
12,830,630 $
18,516,977 $
19,187,439 $
19,206,626 $
20,202,970 $
105,831,565
3. First-line drugs procurement and management
$ 8,565,633
$ 9,278,683
$ 10,295,749
$ 10,928,927
$ 10,711,747
$ 10,722,459
$ 10,625,245
$ 71,128,443
4. M&E $
1,134,590 $
1,254,590 $
1,144,590 $
1,154,590 $
1,144,590 $
1,154,590 $
1,144,590 $
8,132,133
5. Programme management and supervision
$ 960,816
$ 1,042,764
$ 623,539
$ 684,545
$ 698,733
$ 625,467
$ 654,285
$ 5,290,148
6. HRD: Staff $
6,516,676 $
7,200,024 $
7,912,597 $
8,703,851 $
10,030,154 $
11,033,177 $
12,136,481 $
63,532,959
7. HRD: International technical assistance
$ -
$ 106,000
$ 160,000
$ 191,000
$ -
$ -
$ -
$ 457,000
8. HRD: Training $ -
$ 5,228,966
$ 192,683
$ 1,850,899
$ 1,002,333
$ 2,043,582
$ 7,399,032
$ 17,717,495
9. Collaborative TB/HIV activities $
523,567 $
604,372 $
681,335 $
798,095 $
831,989 $
832,820 $
847,776 $
5,119,954
10. MDR-TB $
27,756,920 $
41,084,344 $
55,399,740 $
79,911,265 $
82,751,354 $
82,834,063 $
87,128,895 $
456,866,581
11. High risk groups $ -
$ 1,387,500
$ 137,500
$ 137,500
$ 137,500
$ 137,500
$ 137,500
$ 2,075,000
12. Infection control $
822,463 $
981,080 $
1,132,718 $
1,380,362 $
1,440,708 $
1,442,145 $
1,471,462 $
8,670,938
13. Involving all care providers: PPM/ISTC
$ 11,741,050
$ 14,342,730
$ 18,502,120
$ 20,524,950
$ 20,832,820
$ 20,853,730
$ 20,645,140
$ 127,442,540
14. Partnering initiatives $
96,448 $
213,933 $
96,448 $
213,933 $
96,448 $
213,933 $
96,448 $
1,027,590
15. Community involvement $
910,519 $
978,808 $
1,052,218 $
1,094,307 $
1,110,722 $
1,111,832 $
1,100,714 $
7,359,121
16. Operational research $ -
$ 293,580
$ 171,080
$ -
$ -
$ 4,574,846
$ -
$ 5,039,506
Total costs for TB control
$ 73,357,026
$ 103,111,726
$ 123,193,656
$ 166,670,685
$ 168,630,177
$ 174,934,792
$ 183,592,785
$ 993,490,848

SECTION C –
TECHNICAL ASSISTANCE PLAN (attached)





























