Embed Size (px)
Citation preview

SPECIAL SITUATIONS
Venomous bites and stingsDavid Lalloo
AbstractBites and stings are common in many tropical countries. Snakebite
predominantly affects the rural poor and causes both morbidity and
mortality. The clinical features of snake envenoming depend upon the
species: both local and systemic envenoming can occur. Spider bites
and scorpion, fish and jellyfish stings can all cause significant morbidity,
and occasional mortality.
Keywords antivenom; envenoming; snakebite
Epidemiology
Bites and stings from venomous animals occur throughout the
world, but are particularly important in tropical and subtropical
regions, where the large number of venomous species and the
rural activity of the population lead to significant morbidity and
mortality. In some countries, envenoming is one of the principal
causes of death in adults; annual mortality rates from snakebite
of 5e15/100,000 population have been reported in countries
such as Myanmar and Sri Lanka. Recent estimates suggest that
there are between 20,000 and 100,000 deaths and at least 420,000
envenomings annually worldwide. The sequelae of envenoming
can also be severe; disability from a severely damaged limb
following snakebite is particularly problematic in the tropics.
Furthermore, antivenom and the intensive treatment needed by
victims increase health costs in tropical countries with limited
health budgets.
Envenoming can be caused by a large variety of terrestrial and
marine animals. The most important are species of snake, scor-
pion, spider and jellyfish. Bee and wasp stings and marine
animals also cause problems in some parts of the world.
Snakebites
Venomous snakes are found throughout the world. Most patients
are bitten on the lower limb after disturbing snakes, often while
working in fields or hunting; snakes seldom attack humans
spontaneously. Some bites occur through handling of snakes,
and envenoming can occur even after a snake has been killed.
Venom is deposited subcutaneously by the hollow fangs of the
snake. Components of venom usually reach the circulation via
the lymphatics, although low-molecular-weight components may
be absorbed directly into capillaries.
Most venoms are complex mixtures of many different toxins:
� Proteinases act as cytotoxins, causing severe local swelling and
tissue damage in the region of the bite.
David Lalloo MD FRCP is a Professor of Tropical Medicine and Director of
the Wellcome Trust Tropical Centre at the Liverpool School of Tropical
Medicine, Liverpool, UK. Competing interests: none declared.
MEDICINE 38:1 52
� Neurotoxins interfere with neuromuscular transmission. Some
phospholipase A2 toxins also damage myocytes directly.
� Some venoms contain haemorrhagins (metalloproteinases that
damage vascular endothelium, causing bleeding).
� Components of venom can act at many different sites in the
coagulation pathway, causing anticoagulant or procoagulant effects
leading to a state resembling disseminated intravascular
coagulation. Components also act directly on platelets.
Clinical features of envenoming depend on the species;
accurate identification, ideally by examination of the dead snake,
is crucial. Careful clinical evaluation is necessary before treat-
ment is administered, because bites by a venomous species do
not always result in envenoming.
The bite of elapid snakes (kraits, cobras) most commonly
causes neurotoxicity, whereas viperine snakes (vipers, pit vipers,
rattlesnakes, British adder) cause local tissue damage, shock and
coagulopathies. However, this distinction is somewhat blurred;
for example, Australasian elapids can cause both neurotoxicity
and coagulopathies.
Envenoming causes both local and systemic effects. Symp-
toms of systemic envenoming (headache, lymph node pain and
collapse) often occur within several minutes of the bite. Most
signs of envenoming develop within the first few hours, though
neurotoxicity can occasionally take more than 12 hours.
� Fang marks are usually visible at the site of the bite.
� Following bites from some species, oedema (Figure 1) can
occur at the site of the bite and progress to involve the whole
limb. Some species cause tissue necrosis at the site of the bite.
� Painful regional lymph node enlargement is a common early
sign of envenoming.
Figure 1 Severe local oedema, blistering, bruising, bleeding and early
necrosis in a Thai boy bitten on the shin 3 days earlier by a Malayan pit
viper (Calloselasma rhodostoma). � 1997 Professor DA Warrell.
� 2009 Elsevier Ltd. All rights reserved.

Figure 2 Spontaneous bleeding from the gums in a patient bitten by
a Papuan taipan (Oxyuranus scutellatus canni). � 1997 Professor DA
Warrell.
SPECIAL SITUATIONS
� Venom haemorrhagins act on endothelium, causing bleeding
from the gums (Figure 2) and other sites (e.g. old sores).
Coagulopathies can exacerbate this effect, and occasionally lead to
life-threatening bleeding.
� Shock can occur as a result of loss of fluid into a limb or
haemorrhage.
� Neurological involvement classically causes progressive
paralysis. Ptosis occurs initially; this progresses to involvement of
the bulbar muscles (Figure 3) and, ultimately, paralysis of the
diaphragm.
� Destruction of skeletal muscle, following envenoming by species
such as sea snakes, leads to painful myopathy and paralysis.
� Renal failure complicates envenoming by several species.
Figure 3 Severe ptosis and bulbar palsy requiring intubation in a patient
bitten by a Papuan taipan.
MEDICINE 38:1 53
Investigations e the white blood cell count is commonly
elevated and thrombocytopenia often occurs, particularly in
patients with coagulopathy. Renal function should be checked.
Creatine kinase elevation occurs in myotoxicity.
The whole-blood clotting test is an important bedside indi-
cator of envenoming by species that cause coagulopathy. Blood
left in a clean, dry glass tube is examined after 20 minutes to see
whether clotting has occurred. In some cases, the test can also be
used to follow the response to antivenom. If available, standard
clotting assays. (prothrombin time (PT), activated partial
thromboplastin time (APTT), fibrinogen) are sensitive indicators
of a coagulopathy.
Management e most traditional first aid procedures (e.g.
incision, suction) are more harmful than beneficial. Immobili-
zation of the bitten limb and compression bandaging, when
properly applied, appear to be helpful in slowing lymphatic
spread of venom. It should be used for bites by species that do
not cause local tissue necrosis, to allow time for transport of the
victim to hospital. Intramuscular injections and aspirin should be
avoided in patients with coagulopathy.
Antivenom is indicated for the treatment of systemic or severe
local envenoming. A delay in administration reduces the efficacy,
but antivenom can remain useful as long as signs of systemic
envenoming persist. The antivenom used depends on the biting
species; in many parts of the world, polyspecific antivenoms
covering the commonly occurring species are available.
Antivenom should be given by slow intravenous infusion. The
appropriate dose is dictated by local experience. Children require
the same dose as adults. Test doses have no role in predicting
antivenom reactions. In some countries, antihistamine or
adrenaline (epinephrine) is given as routine prophylaxis against
reactions. Most evidence suggests that there is no role for routine
prophylaxis but adrenaline (epinephrine) should always be
available for treatment of reactions.
Effective antivenom treatment should halt local oedema and
reverse coagulopathy within 6e12 hours. The whole-blood
clotting test 6 hours after administration of antivenom, or
measurement of PT or APTT after 6 hours can help to determine
whether further doses are necessary.
Most toxins acting postsynaptically are reversed by anti-
venom, but presynaptic neurotoxicity is less responsive;
supportive therapy may be needed until spontaneous recovery
occurs.
Delayed absorption of venom from a depot at the bite site can
occur. Repeated doses of antivenom may be needed after initial
therapy if coagulopathy redevelops, neurological deterioration
occurs or limb oedema progresses.
Care of the airway is critical in severe neurotoxicity. Bulbar
involvement (demonstrated by inability to swallow secretions) is
an indication for early intubation and mechanical ventilation if
facilities are available; patients have been ventilated successfully
by hand for several days. Hypotension requires appropriate
management with fluids. Peritoneal dialysis can be instituted in
many tropical regions and can be life-saving.
Fasciotomy is seldom, if ever, necessary, even in severe
oedema. The only indication is raised intracompartmental pres-
sure. Surgery should not be performed until coagulopathy has
been corrected.
� 2009 Elsevier Ltd. All rights reserved.

SPECIAL SITUATIONS
Anticholinesterases are effective in some patients with
neurotoxic envenoming; the therapeutic response may be
dramatic. A trial of a short-acting anticholinesterase such as
neostigmine or edrophonium should be performed in such cases;
in the absence of antivenom, it can be life-saving.
Plasma or clotting factors are seldom needed unless life-
threatening haemorrhage occurs, and should not be given until
adequate doses of antivenom have been administered.
Scorpion stings
Venomous scorpion stings are a major problem in the Americas,
North Africa, the Middle East and South Asia. Scorpion venoms
are usually less complex than snake venoms; most components
are peptides that affect sodium and potassium channels. The
severity of envenoming varies between species.
Clinical features e severe pain in the region of the sting is
common. A small proportion of patients, particularly children,
develop signs and symptoms caused by the action of scorpion
venom on the autonomic nervous system. Hyperexcitability,
sweating, lacrimation, excessive salivation and tachypnoea may
occur. In severe envenoming, catecholamine release causes hyper-
tension, cardiac arrhythmias, myocardial failure and pulmonary
oedema. Skeletal muscle stimulation can lead to muscular spasms.
Management e antivenom therapy is the mainstay of therapy,
with supportive medical treatment. Atropine may be required in
patients with severe bradyarrhythmia, but has no other proven
value. Vasodilator therapy (particularly prazosin) can be useful
in the treatment of cardiovascular manifestations of envenoming.
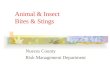
Figure 4 Box jellyfish, Chironex fleckeri.
Spider bites
Species of venomous spiders are found throughout the world, in
temperate and tropical regions.
Clinical features e the most common venomous spiders are
the widow spiders (Latrodectus spp.): their venom stimulates
transmitter release from neurones throughout the nervous system,
causing severe local and generalized pain, muscle cramps and
spasms, sweating, and occasionally severe hypertension.
The predominant feature of envenoming by recluse spiders
(Loxosceles spp.) is severe, slowly-evolving local necrosis. The
Australian funnel web spider (Atrax robustus) releases a presyn-
aptic neurotoxin that can stimulate the autonomic and peripheral
nervous system and can cause cardiovascular instability and
severe pulmonary oedema.
Management e pressure immobilization is recommended for
funnel web spider bites, but is not used for other species. The
availability of antivenom depends on the species and the
geographical location. Antivenom should be used for significant
systemic envenoming.
Venomous fish
Many different venomous fish sting if they are stood on or
touched. Systemic envenoming is rare. Excruciating pain at the
site of the sting is the major effect. Regional nerve blocks and
MEDICINE 38:1 54
local infiltration of lidocaine can be effective, but most marine
venoms are heat labile. Immersing the stung part in hot water is
extremely effective in relieving pain. Care should be taken to
avoid scalding; the envenomed limb may have abnormal
sensation.
Coelenterate stings
Venomous jellyfish occur throughout the world, but are partic-
ularly common in the tropical waters of the Indo-Pacific region. A
mechanical stimulus causes nematocysts on the tentacles to
discharge, injecting venom subcutaneously.
Clinical features depend on the species. Most cause imme-
diate pain at the site of contact and an acute local inflammatory
response. The box jellyfish, Chironex fleckeri (Figure 4), can
cause full-thickness skin damage and systemic involvement;
death can occur rapidly from myocardial toxicity. Some tiny
carybdeid jellyfish stings cause Irukandji syndrome, often in the
absence of skin lesions. Pain, hypertension and cardiopulmonary
decompensation can occur 30e40 minutes after the sting.
Management e undischarged nematocysts adherent to the
skin should be prevented from firing; vinegar is effective on
stings from the box jellyfish found in Pacific and Australasian
regions. Stings from hydroids (e.g. Portuguese man-of-war),
should be washed with fresh sea-water and adherent tentacles
picked off.
In patients with box jellyfish stings, compression bandaging
can reduce systemic absorption of venom. In severe envenoming,
collapse may occur on the beach. Cardiopulmonary resuscitation
may be life-saving.
Antivenom is not available for hydroid stings or Irukandji
syndrome. Pain relief can be achieved by the use of ice and
� 2009 Elsevier Ltd. All rights reserved.

SPECIAL SITUATIONS
opioids: immersion in hot water is also effective for some
species. Supportive therapy is necessary for the management of
cardiovascular manifestations. A
Vipera berus (adder)
The adder inflicts about 50e100 bites each year in the UK. Most
patients present with minimal symptoms and signs; serious
envenoming is rare and death extremely uncommon.
In most cases, symptoms develop within 6 hours of the bite.
The most common local features are pain and swelling that may
spread to involve the whole limb. Gastrointestinal disturbances,
abdominal pain, vomiting and diarrhoea may be prominent if
systemic absorption of venom occurs. Severe systemic enve-
noming causes circulatory disturbances with tachycardia, hypo-
tension and shock; these can occur within minutes of the bite or
be delayed for hours. Bleeding and coagulopathy are rare. Leu-
cocytosis, metabolic acidosis or raised creatine phosphokinase
may indicate systemic envenoming.
Antivenom should be given to patients with severe local
envenoming or evidence of systemic envenoming, particularly
shock, or protracted gastrointestinal symptoms.
Indication for antivenom
C Severe local envenoming (oedema extending over more than
half the bitten limb or necrosis)
C Coagulopathy
C Bleeding
C Shock
C Neurotoxicity
C Myotoxicity
C Renal failure
MEDICINE 38:1 55
FURTHER READING
Kasturiratne A, Wickremasinghe AR, de Silva N, et al. The global
burden of snakebite: a literature analysis and modelling based on
regional estimates of envenoming and deaths. PLoS Med 2008; 5:
e218. doi:10.1371/journal.pmed.0050218.
Sano-Martins IS, Fan HW, Castro SC, et al. Reliability of the simple 20
minute whole blood clotting test (WBCT20) as an indicator of low
plasma fibrinogen concentration in patients envenomed by Bothrops
snakes. Toxicon 1994; 32: 1045e50.
Theakston RDG, Lalloo DG. Venomous bites and stings. In: Zuckerman J,
ed. Principles and practice of travel medicine. Chichester: John Wiley
and Sons, 2001.
Warrell DA. Treatment of bites by adders and exotic venomous snakes.
BMJ 2005 Nov 26; 331: 1244e7.
Practice points
C Not all patients bitten by a venomous snake are envenomed
C The 20-minute whole-blood clotting test is a rapid, easy test
for envenoming following bites by some species
C Antivenom should be given only when there are clear signs of
envenoming
C Doses of antivenom are the same for children and adults
C Observe patients carefully after administration of antivenom,
to detect reactions and to monitor the need for further
treatment
Acknowledgement
We are grateful to Professor DA Warrell for granting permission to
use his photographs for Figures 1 and 2.
� 2009 Elsevier Ltd. All rights reserved.