Embed Size (px)
Citation preview

I. Introduction
Uterine Myoma are among the most frequent entities encountered in
the practice of gynecology, occurring in 20–40% of women during their
reproductive years. It is the most common pelvic neoplasm of gynecologic
origin, as well as the most frequently occurring tumor of the uterus. They are
benign and account for the single largest indication for hysterectomy.
Myomas range in size from seedlings to large uterine tumors. They are
round, firm, benign lumps of the muscular wall of the uterus, composed of
smooth muscle and connective tissue, and are rarely solitary. Usually as
small as a hen's egg, they commonly grow gradually to the size of an orange
or grapefruit. On cutting into such a tumor, its surface is seen to be glistening
white color, with characteristic whorl-like trabeculation so that it stands out in
sharp contrast to the surrounding muscularies.
A diagnosis of uterine myoma is the most common indication for
hysterectomy. Many surgical procedures other than hysterectomy are also
commonly performed because of myomas. Women with symptoms like heavy
bleeding and pain may need surgery. If the woman is not planning to have
any more children, a hysterectomy may be recommended. This is surgery to
remove the uterus. If the woman would like to become pregnant in the
future, a myomectomy may be done instead. This is surgery to remove only
the fibroid. The uterus is left intact.
A. Current Trends
‘Young Early Stage Ovarian Cancer Patients Can Preserve Fertility’ScienceDaily (Aug. 10, 2009) — A new study finds that young women with early-stage ovarian cancer can preserve future fertility by keeping at least one ovary or the uterus without increasing the risk of dying from the disease.
The study is published in the September 15, 2009 issue of Cancer, a peer-reviewed journal of the American Cancer Society.Most cases of ovarian cancer are diagnosed at later stages and in older women. However, up to 17 percent of ovarian tumors occur in women 40 years of age or younger, many of whom have early stage disease. Surgery for ovarian cancer usually involves complete removal of the uterus (hysterectomy) and ovaries, which not only results in the loss of fertility, but also subjects young women to the long-term consequences of estrogen deprivation.
Researchers led by Jason Wright, M.D., of Columbia University College of Physicians and Surgeons in New York City conducted a study to examine

the safety of fertility-conserving surgery in premenopausal women with ovarian cancer. This type of surgery conserves at least one ovary or the uterus.
The investigators analyzed data from women 50 years of age or younger who were diagnosed with early stage (stage I) ovarian cancer between 1988 and 2004 and who were registered in the National Cancer Institute's Surveillance, Epidemiology and End Results database, a population-based cancer registry that includes approximately 26 percent of the US population. Patients who had both of their ovaries removed were compared with those who had only the cancerous ovary removed. A second analysis examined uterine conservation vs hysterectomy.For their first analysis, the researchers identified 1,186 ovarian cancer patients. While most had both ovaries removed, about one in three (36 percent) had one ovary conserved. They found those in whom one ovary was saved had similar survival for up to at least five years.To examine the effect of uterine preservation, the investigators studied a total of 2,911 women. While most of the women underwent hysterectomy, about one in four (23 percent) had uterine preservation. Uterine preservation also had no effect on survival.Women who were younger, who were diagnosed in more recent years, and who resided in the eastern or western United States were more likely to undergo ovarian or uterine conservation.These results are promising for the many young women who are diagnosed with ovarian cancer each year. An estimated 21,650 women in the United States were diagnosed with the disease in 2008. "Given the potential reproductive and nonreproductive benefits of ovarian and uterine preservation, the benefits of conservative surgical management should be considered in young women with ovarian cancer," the authors concluded.
Article Date: Aug. 10, 2009
Source: http://www.sciencedaily.com/releases/2009/08/090810024819.htm
Prevalence/incidence of myoma
Every 10 minutes, 12 hysterectomies are performed. According to a
report published by Obstetrics and Gynecology, 9 of them probably didn't
meet the guidelines set out by the American College of Obstetricians &
Gynecologists for hysterectomy.
*Over 5 billion dollars spent annually on hysterectomies (medical
expense of procedures only)
*Average time off from work to recover from a hysterectomy is 6
weeks (~144 million lost work hours)

*60% of all women undergoing hysterectomy have their ovaries
removed (castration)
* 37% of all women undergo hysterectomy by age 60
*Myomectomy is performed less than 40,000 times a year
*Over 25,000 uterine artery embolizations have been performed
worldwide since 1996.
*For every 10,000 hysterectomies performed, 11 women die.
(Approximately 660 women die each year from complications of
hysterectomy.)
Possibly as many as 80% of all women have uterine fibroids while the
majority usually have no symptoms, 1 in 4 end up with symptoms severe
enough to require treatment.
B. Reasons of choosing the case
The researchers chose the case of uterine myoma due to favorable
suggestions because as they had their duty at the Balitucan District Hospital
most of the OB cases were normal deliveries or caesarean section so the
researchers took the case as it came, grabbing the chance to learn more
about uterine myoma.
II. NURSING PROCESS
a. Assessment
1. PERSONAL DATA
A. Socio-economic and cultural factors
This includes the relationship of people with others, superstitious
beliefs related to health, religious affiliations, financial status, occupation,
income and vices. Culture encompasses the set of beliefs, moral values,
traditions, language, and laws held in common by a nation, a community, or
other defined group of people.
Early detection of diseases or any other abnormalities within the body
such as myoma uteri is very important to make necessary interventions. In
this way there is much chance to prevent further complications to occur. But
in reality a lot of people suffer from it without even having doctor

consultations due to lack of money to pay their professional fee. In addition,
once a person is diagnosed with such, screening tests will be done and it’s
quite expensive as it was expected.
Finally, patients tend to seek for more guidance to God to endure
myoma that they will be facing. Through the help and guidance of Him, the
belief that He will be the one to heal the tumor with the aid of the
professionals.
2. History of Past Illness
This includes the illnesses that the patient experienced which has no
relation to the present illness. The past medical history is essential
background information related to the patient’s health and well being. A brief
past medical and social history often includes these elements:
1. Allergies and reactions to drugs
2. Current medications
3. Medical or psychiatric illnesses (DM, Hypertension, Depression, etc.)
4. Surgeries or injuries or hospitalizations (appendectomy, car
accidents, etc.)
5. Immunizations
6. Tobacco, alcohol or drug use
7. Reproductive status for females
a. LMP
b. Last pelvic exam/pap smear
c. Pregnancies /births/contraception
8. Birth history/developmental milestones for children
9. Marital/family status
10. Occupation/Exposures
3. History of Present Illness
Medical practice a chronological description of the development of the
patient’s present illness, from the first sign and symptoms from the previous
encounter to the present; HPI includes location, quality, severity, duration,
timing, context, modifying factors and associated signs and symptoms.

4. Physical examination
During a physical examination, a health care provider studies a patient's
body to determine the presence or absence of physical problems.
Head – no presence of lumps and there’s no pain in palpation
Hair – equally distributed, no loosing, (-) dandruff or lice
Neck – no deformities noted, neck movements within normal, no pain
presented
Eyes- pale conjunctiva, pupil equally round reactive to light and
accommodation
Nose – sense of smell functioning well, (-) obstruction, (-) sinus pain
Mouth- no dental caries, no dentures, (-) soreness of mouth and tongue
Integumentary – no acne, no rashes, (-) cyanosis, (+) sweating
Respiratory – (-) dyspnea, (-) rales noted upon auscultation
GIT – (-) nausea and vomiting, tender abdomen upon palpation, abdominal
discomfort or bloating
Genital – (+) vaginal bleeding with onset of pain, onset of menarche 14y/o,
Uterus – soft with palpable nodules and firm masses and accompanied with
pain
Reproductive problems - such as infertility, multiple miscarriages or early
labor
Menorrhagia, Pain during sex
Bladder – distended, (+) urination, 10 cc, 20x a day urinary frequency or
retention
Breast- (-) inflammation and swelling, inverted nipple
Nervous system – (-) seizures, (-) paresthesia and paralysis, no speech
deformities
GUT- painful defecation
III. Anatomy and Physiology
FEMALE REPRODUCTIVE SYSTEM

The female reproductive system is designed to carry out several
functions. It produces the female egg cells necessary for reproduction, called
the ova or oocytes. The system is designed to transport the ova to the site of
fertilization. Conception, the fertilization of an egg by a sperm, normally
occurs in the fallopian tubes. The next step for the fertilized egg is to implant
into the walls of the uterus, beginning the initial stages of pregnancy. If
fertilization and/or implantation do not take place, the system is designed to
menstruate (the monthly shedding of the uterine lining). In addition, the
female reproductive system produces female sex hormones that maintain the
reproductive cycle.
During menopause the female reproductive system gradually stops. It
makes the female hormones necessary for the reproductive cycle to work.
When the body no longer produces these hormones a woman is considered to
be menopausal.
Female Anatomy
The female reproductive anatomy includes internal and external structures.
The function of the external female reproductive structures (the
genital) is twofold: To enable sperm to enter the body and to protect the
internal genital organs from infectious organisms. The main external
structures of the female reproductive system include:

Labia majora: The labia majora enclose and protect the other
external reproductive organs. Literally translated as "large lips," the
labia majora are relatively large and fleshy, and are comparable to the
scrotum in males. The labia majora contain sweat and oil-secreting
glands. After puberty, the labia majora are covered with hair.
Labia minora: Literally translated as "small lips," the labia minora can
be very small or up to 2 inches wide. They lie just inside the labia
majora, and surround the openings to the vagina (the canal that joins
the lower part of the uterus to the outside of the body) and urethra
(the tube that carries urine from the bladder to the outside of the
body).
Bartholin's glands: These glands are located next to the vaginal
opening and produce a fluid (mucus) secretion.
Clitoris: The two labia minora meet at the clitoris, a small, sensitive
protrusion that is comparable to the penis in males. The clitoris is
covered by a fold of skin, called the prepuce, which is similar to the
foreskin at the end of the penis. Like the penis, the clitoris is very
sensitive to stimulation and can become erect.

The internal reproductive organs:
Vagina: The vagina is a canal that joins the cervix (the lower part of
uterus) to the outside of the body. It also is known as the birth canal.
Ovaries: The ovaries are small, oval-shaped glands that are located
on either side of the uterus. The ovaries produce eggs and hormones.
Fallopian tubes: These are narrow tubes that are attached to the
upper part of the uterus and serve as tunnels for the ova (egg cells) to
travel from the ovaries to the uterus. Conception, the fertilization of an
egg by a sperm, normally occurs in the fallopian tubes. The fertilized
egg then moves to the uterus, where it implants to the uterine wall.
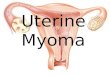
Uterus (womb): The uterus is a hollow, pear-shaped organ that is the
home to a developing fetus. The uterus is divided into two parts: the
cervix, which is the lower part that opens into the vagina, and the main
body of the uterus, called the corpus. The corpus can easily expand to
hold a developing baby. A channel through the cervix allows sperm to
enter and menstrual blood to exit.
Sagittal section of the lower part of a female trunk, right segment.
The uterus is a hollow, thick-walled, muscular organ situated deeply in
the pelvic cavity between the bladder and rectum. Into its upper part the
uterine tubes open, one on either side, while below, its cavity communicates

with that of the vagina. When the ova are discharged from the ovaries they
are carried to the uterine cavity through the uterine tubes. If an ovum be
fertilized it imbeds itself in the uterine wall and is normally retained in the
uterus until prenatal development is completed, the uterus undergoing
changes in size and structure to accommodate itself to the needs of the
growing embryo.
After parturition the uterus returns almost to its former condition, but
certain traces of its enlargement remains. It is necessary, therefore, to
describe as the type-form the adult virgin uterus, and then to consider the
modifications which are effected as a result of pregnancy.
In the virgin state the uterus is flattened antero-posteriorly and is
pyriform in shape, with the apex directed downward and backward. It lies
between the bladder in front and the pelvic or sigmoid colon and rectum
behind, and is completely within the pelvis, so that its base is below the level
of the superior pelvic aperture. Its upper part is suspended by the broad and
the round ligaments, while its lower portion is imbedded in the fibrous tissue
of the pelvis.
The long axis of the uterus usually lies approximately in the axis of the
superior pelvic aperture, but as the organ is freely movable its position varies
with the state of distension of the bladder and rectum. Except when much
displaced by a fully distended bladder, it forms a forward angle with the
vagina, since the axis of the vagina corresponds to the axes of the cavity and
inferior aperture of the pelvis. The uterus measures about 7.5 cm. in length,
5 cm. in breadth, at its upper part, and nearly 2.5 cm. in thickness; it weighs
from 30 to 40 gm. It is divisible into two portions.
On the surface, about midway between the apex and base, is a slight
constriction, known as the isthmus, and corresponding to this in the interior is
a narrowing of the uterine cavity, the internal orifice of the uterus. The
portion above the isthmus is termed the body, and that below, the cervix.
The part of the body which lies above a plane passing through the points of
entrance of the uterine tubes is known as the fundus. Body (corpus uteri).—
The body gradually narrows from the fundus to the isthmus.
The vesical or anterior surface (facies vesicalis) is flattened and
covered by peritoneum, which is reflected on to the bladder to form the

vesicouterine excavation. The surface lies in apposition with the bladder.
The intestinal or posterior surface (facies intestinalis) is convex transversely
and is covered by peritoneum, which is continued down on to the cervix and
vagina. It is in relation with the sigmoid colon, from which it is usually
separated by some coils of small intestine. The fundus (fundus uteri) is
convex in all directions, and covered by peritoneum continuous with that on
the vesical and intestinal surfaces. On it rest some coils of small intestine,
and occasionally the distended sigmoid colon. The lateral margins (margo
lateralis) are slightly convex.
At the upper end of each the uterine tube pierces the uterine wall.
Below and in front of this point the round ligament of the uterus is fixed,
while behind it is the attachment of the ligament of the ovary. These three
structures lie within a fold of peritoneum which is reflected from the margin
of the uterus to the wall of the pelvis, and is named the broad ligament.
Cervix
The cervix is the lower constricted segment of the uterus. It is
somewhat conical in shape, with its truncated apex directed downward and
backward, but is slightly wider in the middle than either above or below.
Owing to its relationships, it is less freely movable than the body, so that the
latter may bend on it. The long axis of the cervix is therefore seldom in the
same straight line as the long axis of the body. The long axis of the uterus as
a whole presents the form of a curved line with its concavity forward, or in
extreme cases may present an angular bend at the region of the isthmus.
The cervix projects through the anterior wall of the vagina, which
divides it into an upper, supravaginal portion, and a lower, vaginal portion.
The supravaginal portion (portio supravaginalis [cervicis]) is separated in
front from the bladder by fibrous tissue (parametrium), which extends also on
to its sides and lateralward between the layers of the broad ligaments. The
uterine arteries reach the margins of the cervix in this fibrous tissue, while on
either side the ureter runs downward and forward in it at a distance of about
2 cm. from the cervix. Posteriorly, the supravaginal cervix is covered by
peritoneum, which is prolonged below on to the posterior vaginal wall, when

it is reflected on to the rectum, forming the rectouterine excavation. It is in
relation with the rectum, from which it may be separated by coils of small
intestine.
The vaginal portion (portio vaginalis [cervicis]) of the cervix projects
free into the anterior wall of the vagina between the anterior and posterior
fornices. On its rounded extremity is a small, depressed, somewhat circular
aperture, the external orifice of the uterus, through which the cavity of the
cervix communicates with that of the vagina. The external orifice is bounded
by two lips, an anterior and a posterior, of which the anterior is the shorter
and thicker, although, on account of the slope of the cervix, it projects lower
than the posterior. Normally, both lips are in contact with the posterior
vaginal wall. Interior of the Uterus
The cavity of the uterus is small in comparison with the size of the
organ. The Cavity of the Body (cavum uteri) is a mere slit, flattened antero-
posteriorly. It is triangular in shape, the base being formed by the internal
surface of the fundus between the orifices of the uterine tubes, the apex by
the internal orifice of the uterus through which the cavity of the body
communicates with the canal of the cervix. The Canal of the Cervix (canalis
cervicis uteri) is somewhat fusiform, flattened from before backward, and
broader at the middle than at either extremity. It communicates above
through the internal orifice with the cavity of the body, and below through
the external orifice with the vaginal cavity. The wall of the canal presents an
anterior and a posterior longitudinal ridge, from each of which proceed a
number of small oblique columns, the palmate folds, giving the appearance
of branches from the stem of a tree; to this arrangement the name arbor vitæ
uterina is applied. The folds on the two walls are not exactly opposed, but fit
between one another so as to close the cervical canal.

Posterior half of uterus and upper part of vagina.
The total length of the uterine cavity from the external orifice to the fundus
is about 6.25 cm.
Ligaments
The ligaments of the uterus are eight in number: one anterior; one
posterior; two lateral or broad; two uterosacral; and two round ligaments.
The anterior ligament consists of the vesicouterine fold of peritoneum, which
is reflected on to the bladder from the front of the uterus, at the junction of
the cervix and body. The posterior ligament consists of the rectovaginal fold
of peritoneum, which is reflected from the back of the posterior fornix of the
vagina on to the front of the rectum. It forms the bottom of a deep pouch
called the rectouterine excavation, which is bounded in front by the posterior
wall of the uterus, the supravaginal cervix, and the posterior fornix of the
vagina; behind, by the rectum; and laterally by two crescentic folds of
peritoneum which pass backward from the cervix uteri on either side of the
rectum to the posterior wall of the pelvis.
These folds are named the sacrogenital or rectouterine folds. They
contain a considerable amount of fibrous tissue and non-striped muscular
fibers which are attached to the front of the sacrum and constitute the
uterosacral ligaments. The two lateral or broad ligaments (ligamentum
latum uteri) pass from the sides of the uterus to the lateral walls of the pelvis.
Together with the uterus they form a septum across the female pelvis,

dividing that cavity into two portions. In the anterior part is contained the
bladder; in the posterior part the rectum, and in certain conditions some coils
of the small intestine and a part of the sigmoid colon.
Between the two layers of each broad ligament are contained: (1) the
uterine tube superiorly; (2) the round ligament of the uterus; (3) the ovary
and its ligament; (4) the epoöphoron and paroöphoron; (5) connective tissue;
(6) unstriped muscular fibers; and (7) bloodvessels and nerves. The portion of
the broad ligament which stretches from the uterine tube to the level of the
ovary is known by the name of the mesosalpinx. Between the fimbriated
extremity of the tube and the lower attachment of the broad ligament is a
concave rounded margin, called the infundibulopelvic ligament.
The round ligaments (ligamentum teres uteri) are two flattened bands
between 10 and 12 cm. in length, situated between the layers of the broad
ligament in front of and below the uterine tubes. Commencing on either side
at the lateral angle of the uterus, this ligament is directed forward, upward,
and lateralward over the external iliac vessels. It then passes through the
abdominal inguinal ring and along the inguinal canal to the labium majus, in
which it becomes lost.
The round ligaments consists principally of muscular tissue, prolonged
from the uterus; also of some fibrous and areolar tissue, besides
bloodvessels, lymphatics; and nerves, enclosed in a duplicature of
peritoneum, which, in the fetus, is prolonged in the form of a tubular process
for a short distance into the inguinal canal. This process is called the canal of
Nuck. It is generally obliterated in the adult, but sometimes remains pervious
even in advanced life. It is analogous to the saccus vaginalis, which precedes
the descent of the testis. In addition to the ligaments just described, there is
a band named the ligamentum transversalis colli (Mackenrodt) on either side
of the cervix uteri.
It is attached to the side of the cervix uteri and to the vault and lateral
fornix of the vagina, and is continuous externally with the fibrous tissue
which surrounds the pelvic bloodvessels. The form, size, and situation of the
uterus vary at different periods of life and under different circumstances.

Sagittal section through the pelvis of a newly born female
Structure
The uterus is composed of three coats: an external or serous, a middle
or muscular, and an internal or mucous. The serous coat (tunica serosa) is
derived from the peritoneum; it invests the fundus and the whole of the
intestinal surface of the uterus; but covers the vesical surface only as far as
the junction of the body and cervix. In the lower fourth of the intestinal
surface the peritoneum, though covering the uterus, is not closely connected
with it, being separated from it by a layer of loose cellular tissue and some
large veins.
The muscular coat (tunica muscularis) forms the chief bulk of the
substance of the uterus. In the virgin it is dense, firm, of a grayish color, and
cuts almost like cartilage. It is thick opposite the middle of the body and
fundus, and thin at the orifices of the uterine tubes. It consists of bundles of
unstriped muscular fibers, disposed in layers, intermixed with areolar tissue,
bloodvessels, lymphatic vessels, and nerves. The layers are three in number:
external, middle, and internal. The external and middle layers constitute the
muscular coat proper, while the inner layer is a greatly hypertrophied
muscularis mucosæ.

During pregnancy the muscular tissue becomes more prominently
developed, the fibers being greatly enlarged. The external layer, placed
beneath the peritoneum, is disposed as a thin plane on the vesical and
intestinal surfaces. It consists of fibers which pass transversely across the
fundus, and, converging at each lateral angle of the uterus, are continued on
to the uterine tube, the round ligament, and the ligament of the ovary: some
passing at each side into the broad ligament, and others running backward
from the cervix into the sacrouterine ligaments. The middle layer of fibers
presents no regularity in its arrangement, being disposed longitudinally,
obliquely, and transversely.
It contains more bloodvessels than either of the other two layers. The
internal or deep layer consists of circular fibers arranged in the form of two
hollow cones, the apices of which surround the orifices of the uterine tubes,
their bases intermingling with one another on the middle of the body of the
uterus. At the internal orifice these circular fibers form a distinct sphincter.
The mucous membrane (tunica mucosa) is smooth, and closely adherent to
the subjacent tissue. It is continuous through the fimbriated extremity of the
uterine tubes, with the peritoneum; and, through the external uterine orifice,
with the lining of the vagina.
In the body of the uterus the mucous membrane is smooth, soft, of a
pale red color, lined by columnar ciliated epithelium, and presents, when
viewed with a lens, the orifices of numerous tubular follicles, arranged
perpendicularly to the surface. The structure of the corium differs from that
of ordinary mucous membranes, and consists of an embryonic nucleated and
highly cellular form of connective tissue in which run numerous large
lymphatics. In it are the tube-like uterine glands, lined by ciliated columnar
epithelium. They are of small size in the unimpregnated uterus, but shortly
after impregnation become enlarged and elongated, presenting a contorted
or waved appearance. In the cervix the mucous membrane is sharply
differentiated from that of the uterine cavity. It is thrown into numerous
oblique ridges, which diverge from an anterior and posterior longitudinal
raphé.
In the upper two-thirds of the canal, the mucous membrane is provided
with numerous deep glandular follicles, which secrete clear viscid alkaline

mucus; and, in addition, extending through the whole length of the canal is a
variable number of little cysts, presumably follicles which have become
occluded and distended with retained secretion. They are called the ovula
Nabothi. The mucous membrane covering the lower half of the cervical canal
presents numerous papillæ. The epithelium of the upper two-thirds is
cylindrical and ciliated, but below this it loses its cilia, and gradually changes
to stratified squamous epithelium close to the external orifice. On the vaginal
surface of the cervix the epithelium is similar to that lining the vagina, viz.,
stratified squamous.
Vertical section of mucous membrane of human uterus. (Sobotta.)
The arteries of the internal organs of generation of the female, seen from
behind.
Vessels and Nerves.

The arteries of the uterus are the uterine, from the hypogastric; and
the ovarian, from the abdominal aorta. They are remarkable for their tortuous
course in the substance of the organ, and for their frequent anastomoses.
The termination of the ovarian artery meets that of the uterine artery, and
forms an anastomotic trunk from which branches are given off to supply the
uterus, their disposition being circular. The veins are of large size, and
correspond with the arteries. They end in the uterine plexuses. In the
impregnated uterus the arteries carry the blood to, and the veins convey it
away from, the intervillous space of the placenta. The nerves are derived
from the hypogastric and ovarian plexuses, and from the third and fourth
sacral nerves.
Puberty
Puberty is the time at which a growing boy or girl begins the process of
sexual maturation. Puberty involves a series of physical stages or steps that
lead to the achievement of fertility and the development of the so-called
secondary sex characteristics, the physical features associated with adult
males and females (such as the growth of pubic hair). While puberty involves
a series of biological, or physical, transformations, the process can also have
an effect on the psychosocial and emotional development of the adolescent.
The onset of puberty varies among individuals. Puberty usually occurs
in girls between the ages of 10 and 14. In some African American girls,
puberty begins earlier, at about age 9, meaning that puberty occurs from
ages 9 to 14.
Adolescent girls reach puberty today at earlier ages than were ever
recorded previously. Nutritional and other environmental influences may be
responsible for this change. For example, the average age of the onset of
menstrual periods in girls was 15 in 1900. By the 1990s, this average had
dropped to 12 and a half years of age.
The timing of the onset of puberty is not completely understood and is
likely determined by a number of factors. One theory proposes that reaching

a critical weight or body composition may play a role in the onset of puberty.
It has been proposed that the increase in childhood obesity may be related to
the overall earlier onset of puberty in the general population in recent years.
Leptin, a hormone produced by fat cells (adipocytes) in the body, has
been suggested as a possible mediator of the timing of puberty. In studies,
animals deficient in leptin did not undergo puberty, but puberty began when
leptin was administered to the animals. Further, girls with higher
concentrations of the hormone leptin are known to have an increased
percentage of body fat and an earlier onset of puberty than girls with lower
levels of leptin. The concentration of leptin in the blood is known to increase
just before puberty in both boys and girls.
Leptin likely is one of multiple influences on the hypothalamus, an area
of the brain that releases a hormone known as gonadotropin-releasing
hormone (GnRH), which in turn signals the pituitary gland to release
leutinizing hormone (LH) and follicle-stimulating hormone (FSH). LH and FSH
secretion by the pituitary is responsible for sexual development.
A gene has been identified that appears to be critical for the normal
development of puberty. The gene, known as GPR54, encodes a protein that
appears to have an effect on the secretion of GnRH by the hypothalamus.
Menstrual Cycle
Females of reproductive age experience cycles of hormonal activity
that repeat at about one-month intervals. (Menstru means "monthly"; hence
the term menstrual cycle.) With every cycle, a woman's body prepares for a
potential pregnancy, whether or not that is the woman's intention. The term
menstruation refers to the periodic shedding of the uterine lining.
The average menstrual cycle takes about 28 days and occurs in
phases: the follicular phase, the ovulatory phase (ovulation), and the luteal
phase. There are four major hormones (chemicals that stimulate or regulate

the activity of cells or organs) involved in the menstrual cycle: follicle-
stimulating hormone, luteinizing hormone, estrogen, and progesterone.
Follicular Phase
This phase starts on the first day of your period. During the follicular phase of
the menstrual cycle, the following events occur:
Two hormones, follicle stimulating hormone (FSH) and luteinizing
hormone (LH) are released from the brain and travel in the blood to the
ovaries.
The hormones stimulate the growth of about 15-20 eggs in the ovaries
each in its own "shell," called a follicle.
These hormones (FSH and LH) also trigger an increase in the
production of the female hormone estrogen.
As estrogen levels rise, like a switch, it turns off the production of
follicle-stimulating hormone. This careful balance of hormones allows
the body to limit the number of follicles that complete maturation, or
growth.
As the follicular phase progresses, one follicle in one ovary becomes
dominant and continues to mature. This dominant follicle suppresses
all of the other follicles in the group. As a result, they stop growing and
die. The dominant follicle continues to produce estrogen.
Ovulatory Phase
The ovulatory phase, or ovulation, starts about 14 days after the follicular
phase started. The ovulatory phase is the midpoint of the menstrual cycle,
with the next menstrual period starting about 2 weeks later. During this
phase, the following events occur:
The rise in estrogen from the dominant follicle triggers a surge in the
amount of luteinizing hormone that is produced by the brain.
This causes the dominant follicle to release its egg from the ovary.

As the egg is released (a process called ovulation) it is captured by
finger-like projections on the end of the fallopian tubes (fimbriae). The
fimbriae sweep the egg into the tube.
Also during this phase, there is an increase in the amount and a
change in the consistency of mucus produced by the cervix (lower part
of the uterus.) If a woman were to have intercourse during this time,
this receptive mucus captures the man's sperm, nourishes it, and helps
it to move towards the egg for fertilization.
Luteal Phase
The luteal phase begins right after ovulation and involves the following
processes:
Once it releases its egg, the empty follicle develops into a new
structure called the corpus luteum.
The corpus luteum secretes the hormone progesterone. Progesterone
prepares the uterus for a fertilized egg to implant.
If intercourse has taken place and a man's sperm has fertilized the egg
(a process called conception), the fertilized egg (embryo) will travel
through the fallopian tube to implant in the uterus. The woman is now
considered pregnant.
If the egg is not fertilized, it passes through the uterus. Not needed to
support a pregnancy, the lining of the uterus breaks down and sheds,
and the next menstrual period begins.
During fetal life, there are about 6 million to 7 million eggs. From this
time, no new eggs are produced.
The vast majority of the eggs within the ovaries steadily die, until they are
depleted at menopause. At birth, there are approximately 1 million eggs; and
by the time of puberty, only about 300,000 remain. Of these, 300 to 400 will
be ovulated during a woman's reproductive lifetime. The eggs continue to
degenerate during pregnancy, with the use of birth control pills, and in the
presence or absence of regular menstrual cycles.

Menopause
Menopause is the absence of menstrual periods for 12 months. The
menopausal transition starts with varying menstrual cycle length and ends
with the final menstrual period. Perimenopause means "the time around
menopause" and is often used to refer to the menopausal transitional period.
It is not officially a medical term, but is sometimes used to explain certain
aspects of the menopause transition in lay terms. Postmenopause is the
entire period of time that comes after the last menstrual period.
Menopause is the time in a woman's life when the function of the
ovaries ceases. The ovary, or female gonad, is one of a pair of reproductive
glands in women. They are located in the pelvis, one on each side of the
uterus. Each ovary is about the size and shape of an almond. The ovaries
produce eggs (ova) and female hormones such as estrogen.
During each monthly menstrual cycle, an egg is released from one
ovary. The egg travels from the ovary through a Fallopian tube to the uterus.
The ovaries are the main source of female hormones, which control the
development of female body characteristics such as the breasts, body shape,
and body hair. The hormones also regulate the menstrual cycle and
pregnancy. Estrogens also protect the bone. Therefore, a woman can develop
osteoporosis (thinning of bone) later in life when her ovaries do not produce
adequate estrogen.
IV. THE PATIENT’S ILLNESS
Synthesis of the disease
1. Definition

A Myoma is a solid tumor made of fibrous tissue; hence it is often
called a 'fibroid' tumor. Myomas may grow as a single nodule or in clusters
and may range in size from 1 mm to more than 20 cm in diameter. Myomas
are the most frequently diagnosed tumor of the female pelvis and the most
common reason for a woman to have a hysterectomy. Although they are
often referred to as tumors, they are not cancerous. Myomas start as small as
a pea but can grow to fill the pelvis and they are often small and
asymptomatic. Symptomatic fibroids occur in 25% of white women and 50%
of black women. Their growth is variable and not predictable.
2. Predisposing/Precipitating Factors
The cause is unknown as yet. It is usually an inherited condition. For
some reason, it is more common in black women.
Risk factors include:
a. Race
Although the basis for the higher prevalence among black women is
unknown, ethnic differences have been found in circulating estrogen levels
while on control diets, and differences in estrogen metabolism have been
noted. In control groups of healthy, premenopausal women placed on a high-
fat, low-fiber diet similar to their usual diet, African-American women had
significantly higher serum levels of estrone, estradiol, and free estradiol than
Caucasian women.
b. Obesity and overweight
Estrogen can increase for a number of reasons; including excessive
weight gain (estrogen is stored in adipose (fat) tissue and the use of estrogen
replacement therapy during menopause. being overweight increases the

amount of natural estrogen formed in the body's fat cells. Since fat cells
produce estrogen, overweight can lead to overproduction of estrogen.
c. Early menarche
There is a suggestion of slightly increased risk of fibroids associated
with early menarche, although the risk has often not been statistically
significant (Cramer et al. 1995; Parazzini et al. 1988; Samadi et al. 1996).
Recently, a significant inverse association between risk of fibroids and age at
menarche was reported; that is, compared with women who were 12 years of
age at menarche, those who were ¾ 10 years of age at menarche were at
increased risk [relative risk (RR) 1.24], whereas women who were age >= 16
years of age at menarche were at lower risk (RR 0.68) (Marshall et al. 1998a).
Sato et al. (2000b) found that women with uterine leiomyomas more often
exhibited an early normal menstrual cycle pattern, and concluded that early
menstrual regularity may enhance leiomyoma growth in early reproductive
life.
The early onset of menstrual cycles may increase the number of cell
divisions that the myometrium undergoes during the reproductive years,
resulting in an increased chance of mutation in genes controlling myometrial
proliferation (Marshall et al. 1998a).
d. Age
Studies that define cases by pathologic diagnosis, thus restricting
cases to those having surgery (Ross et al. 1986), have shown a rapid increase
in fibroid diagnoses among women in their forties. Whether the risk of new
fibroids actually increases rapidly in women during their forties is not known.
The observed increase could also result from increased growth of or
increased symptomatology from, already existing fibroids, as well as from a
greater willingness of women in the later reproductive years to have
gynecologic surgery. If the likelihood of fibroid development and growth
actually accelerates during the late reproductive years, hormonal factors
associated with perimenopause may be important modulators; alternatively,

the apparent increase in the late reproductive years may simply represent
the cumulative culmination of 20-30 years of stimulation by estrogen and
progesterone.
Myomas are estrogen-dependent tumors
• Growth is associated with exposure to circulating estrogen, the main female
hormone.
• Thus, maximum growth is during the reproductive years, when a woman
produces high concentrations of estrogen regularly. There is a growth spurt
in the decade before menopause.
• They can grow in pregnancy, not just because of high estrogen, but
because of increased blood flow to the - uterus.
• Predictably, they decrease in size after menopause, or other conditions of
low estrogen.
The cause of myomas has not actually been determined, but most
myomas develop in women during their reproductive years. Myomas do not
develop before the body begins producing estrogen. Myomas tend to grow
very quickly during pregnancy when the body is producing extra estrogen.
Once menopause has begun, myomas generally stop growing and can begin
to shrink due to the loss of estrogen.
3. Signs and Symptoms
Most fibroids, even large ones, produce no symptoms. These masses
are often found during your regular pelvic examination.
When you do experience symptoms, the most common are these:
Irregular vaginal bleeding or an increase in menstrual bleeding, known
as menorrhagia, sometimes with blood clots

Pressure on the bladder, which may cause you to urinate often and feel
a sense of urgency to urinate and, rarely, the inability to urinate
Pressure on the rectum, resulting in constipation
Pelvic pressure, "feeling full" in the lower abdomen, lower abdominal
pain
Increase in size around your waist and change in abdominal contour
(You may need to increase your clothing size but not because of a
significant weight gain.)
Infertility, which is defined as an inability to become pregnant after 1
year of attempting to get pregnant
A pelvic mass discovered by your health care provider during a
physical examination
Excessive menstrual bleeding is often the only symptom. This is due
to several factors:
• Increased blood supply to the myomas also brings increased blood supply
to the uterine lining (endometrium) which is shed at menses.
• Fibroids usually increase the size of the uterine cavity, therefore , there is
an increased surface area of the lining.
• Bleeding could also be aggravated by endometritis (inflammation of the
lining) which is frequently observed in the endometrial tissue overlying
submucosal tumors.
• Degeneration of the myoma
Excessive bleeding can lead to anemia, usually manifested in fatigue,
headaches and lightheadedness. Degeneration results because of infection or
when the myoma loses its blood supply. The muscle cells and connective
tissues are replaced by fat, cysts, calcification, and/or granular, hyaline or
mucoid material characteristic of necrotic (dying) cells. This often leads to

excessive menstrual bleeding. It can also affect your quality of life, if the
bleeding interferes with your regular activities.
Pain as a symptom is infrequent. It is usually associated with:
• Twisting(tortion) of a fibroid stalk
• Cervical dilatation, if a myoma protrudes through the lower uterine
segment
• Carneous degeneration, often associated with pregnancy.
• Adenomyosis (presence of endometrial glands in the uterine muscle) is
usually associated with myomas, and may also cause pain.
Myomas can cause acute severe pain, due to torsion of the stalk or
degeneration. In such cases, the pain will be localized to the specific area
that is affected. This can usually improve with pain relievers and go away
after two-three weeks. Obviously, if the pain is unbearable, it is best to see a
doctor right away.
Chronic pelvic pain, which is mild but persistent, can also occur. Again,
this is generally localized to a specific area. Low back pain may be
experienced, when the fibroids can press against the nerves of the lower
back.
Pain or discomfort during sexual intercourse (dyspareunia) may also be
experienced. This may be associated only with certain positions, or with the
beginning or middle (around ovulation) of your menstrual cycle.

Possible complications from myomas:
• Stemmed fibroids may twist, causing pain, nausea and fever.
• Infection may lead to degeneration, causing bleeding and other discharge
• Rarely, very rapid growth may be observed. Cancer must then be ruled out.
• Infertility
Health Promotion and Preventive Aspects of the Disease
Avoid weight gain after age 18 and maintain a normal body weight
compared to your height. Body weight tends to increase estrogen production,
thus aggravating fibroid growth. Exercise can help control your weight and
additionally decrease hormone production that stimulates fibroid growth.
Tobacco use has not been proven to be linked to an increase in
fibroids. But quitting smoking will improve general health and well being if
you have fibroids.
Fibroids can make it difficult to conceive a baby. During pregnancy, a
fibroid can cause a miscarriage or difficulty with delivery. A fibroid can also
become twisted and need emergency surgery. Although rare, it is possible for
a fibroid to become cancerous. Fibroids are not contagious. A fibroid may
pose a risk to the fetus during pregnancy.
Most fibroids do not cause symptoms and don't need treatment.
Sometimes, medicines are used to shrink the tumor by decreasing the level
of estrogen in the blood.
A procedure that may be performed is an arterial embolization. A tube
is threaded into a uterine artery. Small beads are injected into the artery
leading to the tumor. This blocks the blood flow to the artery, shrinking the
fibroid.
Laser treatment, called myolysis, is another procedure used to destroy
fibroids. The woman takes medication for 3 to 4 months to shrink the tumor

before the laser treatment is done. Surgery carries a risk of bleeding,
infection, and allergic reaction to anesthesia. If a hysterectomy was done, no
more fibroids can develop. If the ovaries were removed with the uterus,
hormone replacement therapy may be necessary. Fibroids do grow back
about 10% of the time after a myomectomy.
Women with fibroids should be examined every 6 months to monitor
the size of the fibroid. Any unusual symptoms or concerns should be reported
to the healthcare provider. Fibroids are very common, especially in women
older than 35 years of age. They rarely become malignant or cancerous.
Fibroids that grow near the outer surface of the uterus can be felt as lumps
during a pelvic exam. Fibroids growing in the lining of the uterus may be
harder to detect during a pelvic exam.
The diagnosis can be confirmed by an ultrasound. Sometimes a dilation
and curettage, or D & C, will be performed. This is a minor surgical procedure
in which tissue is scraped from the inside of the uterus. A hysteroscopy, in
which a fiberoptic tube is used to examine the inside of the uterus, may also
be done. These procedures may be ordered to rule out other problems, such
as uterine cancer or polyps. Schedule routine health visits with your provider
to allow for early detection.
3. NURSING MANAGEMENT
A. MEDICAL MANAGEMENT
a. IVFs
Medical
Managemen
Date
Ordered
General
Descriptio
Indication(
s)
Clients
Response

t/
Treatment
Date
Performed
Date
Changed
n Or Purpose to
Treatment
-no insertion
of IVF
Nursing Responsibilities
Check the doctor’s order.
b. Drugs
Name of
Drug:
Generic
Name
Brand
Date
Order
ed
Date
Perfor
Route
of
Admin.
Dosage
&
General
Action
Classificatio
n
Mechanism
Indicati
on(s)
or
Purpos
es
Clients
Respon
se to
the
Meds

Name med
Date
Chang
ed
Freque
ncy of
admin.
of Action with
actual
Side-
effects
Generic
Name:
Brand
Name:
DO:
DP:
General
Action:
Classification
:
Mechanism
of Action:
Nursing Responsibilities
Diet
Type of
Diet
Date
Ordered
Date
Performed
Date
Changed
General
Descriptio
n
Indication(
s)
Or Purpose
Clients
Response
and
Reaction
to the Diet

DO:
DP:
DO:
DP:
Nursing Responsibilities
▷ Check the doctor’s order.
Activity and Exercise
Type of
Exercise
Date
Ordered
Date
Performed
Date
Changed
General
Description
Indication
(s)
Or
Purpose
Clients
Response
and
Reaction
to the
Activity
Stretching
of Arms and
Dangling of
Legs
DO:
DP:
ROM (Range
of Motion)
To improve
blood
circulation.
She
followed the
instructions
given; she
does this
before
getting up in
bed.
Deep DO:

Breathing
Exercise DP:
For Full Lung
Expansion.
For airway
clearance
and proper
blood
circulation.
This
exercise
made her
feel relax.
Ambulation DO:
DP:
ROM (Range
of Motion)
To improve
blood
circulation
Gradual
Walking and
Standing,
the patient
feeling
better.
Nursing Responsibilities
▷ Check the doctor’s order.
▷ Instruct patient about the prescribed activity as ordered by the
doctor.
VII. CONCLUSION
Leiomyomas arise from the overgrowth of smooth muscle and connective tissue in the uterus. A genetic predisposition exists. Histologically, a monoclonal proliferation of smooth muscle cells occurs. It is the most frequently diagnosed gynecologic tumor, occurring in 20-50% of women older than 30 years.
Rarely, uterine leiomyoma may undergo malignant degeneration to become a sarcoma. The true incidence of malignant transformation is difficult to determine, because leiomyomas are common, whereas malignant leiomyosarcomas are rare and can arise de novo. The incidence of malignant degeneration is less than 1.0% and has been estimated to be as low as 0.2%.

Infertility may occur as a result of narrowing of the isthmic portion of the fallopian tube or as a consequence of interference with implantation, especially inference caused by submucosal fibroids.
Complications during pregnancy include spontaneous abortion, intrauterine growth retardation, preterm labor, uterine dyskinesia or inertia during labor, obstruction of the birth canal, postpartum hemorrhage, and hydronephrosis. Most leiomyomas occur in the fundus and body of the uterus; only 3% occur in the cervix. The fibroids may be solitary, multiple, or diffuse.
Most fibroids (95%) are intramural, being located in the middle of the myometrium. Subserosal, or exophytic, fibroids are located in the subserosal layer and tend to cause a focal bulge in the exterior surface of the uterus; they can become pedunculated. Rarely, subserosal fibroids occur in the broad ligament. Submucosal, or subendometrial, fibroids are the least common. They distort the overlying endometrium and can become extruded or pedunculated (ie, fibroid polyps) in the endometrial canal.
Calcified fibroids are often depicted on conventional radiographs of the pelvis. In some patients, magnetic resonance imaging (MRI) provides additional information. The role of computed tomography (CT) scanning is limited. Calcifications may be more visible on CT scans than on conventional radiographs because of the superior contrast differentiation achieved with CT scanning.
Recommendation:
The following information was prepared to provide background information on fibroid tumors and some of the treatment options available, including a relatively new procedure that allows women to avoid surgery.Methods of treatment depend on the severity of symptoms, the patient's age, her pregnancy status, her possible desire for future pregnancies, her general health, and characteristics of the fibroids. Treatment may consist of simply monitoring the rate of growth of the fibroids with periodic pelvic exams or ultrasound.
Nonsteroidal anti-inflammatory medications like ibuprofen or naprosyn may be recommended for lower abdominal cramping or pain with menses. Iron supplementation will help to prevent anemia in women with heavy periods. These methods are usually sufficient in premenopausal women. Hormonal treatment, involving drugs such as injectable Depo Leuprolide, causes fibroids to shrink, but can also cause significant side effects. This method is sometimes used for short treatment periods before surgical procedures or when menopause is imminent.
Learning derived:

Handling this kind of patient is interesting. Although it’s quite difficult for the researchers, but it has a purpose to the researching to gain more experience in the field of nursing. At first the researchers did not know what to do in this case, because we have no background about it. But when the researchers did this case study about myoma we were challenge to do it.
Such a wonderful opportunity to be exposed in the ward of ob-gyne. And the researchers are thankful of C.I ma’am Marilou Limiac for being supportive and having a long patience with group 50 whenever a mistake is done.
VIII. BIBLIOGRAPHY
Internet resources:
http://www.sciencenews.org/search/seek?for=uterine+myoma
http://www.sciencedaily.com/releases/2009/08/090810024819.htm
Books:
Nurse’s Pocket Guide, Edition 11, F.A Davis Company
Diseases: A Nursing Process Approach to Excellent Care, Lippincott Williams
& Wilkins Fourth Edition
Anatomy Demystified, Dr. Dale Pierre Layman, Ph.D., McGraw-Hill
l

TABLE OF CONTENTS
I. INTRODUCTION
II. NURSING PROCESS
A. ASSESSMENT
1. Personal Data
a. Demographic Data
b. Socio-economic and Cultural Factors
c. Environmental Factors
2. Personal History
a. Maternal-Obstetric Record
b. Antepartal or Prenatal Preparation
c. Significant Trimestral Changes
3. Family Health – Illness History
4. History of Past Illness
5. History of Present Illness
6. Physical Examination
7. Diagnostic and Laboratory Procedures
III. ANATOMY AND PHYSIOLOGY
IV. PATIENT’S ILLNESS
SYNTHESIS OF THE DISEASE

1. Definition of the Disease
2. Predisposing/Precipitating Factors
3. Pathophysiology
a. Client-Centered
b. Schematic Diagram
4. Signs and Symptoms
5. Health Promotion and Preventive Aspects
V. THE PATIENT AND HER CARE
A.MEDICAL MANAGEMENT
1. IVF
2. Drugs
3. Diet
4. Activity/Exercise
B.NURSING CARE MANAGEMENT
1. Nursing Care Plan
2. Actual SOAPIER
VI. CLIENT’S DAILY PROGRESS IN THE
HOSPITAL
A. CLIENT’S DAILY PROGRESS CHART
VII. CONCLUSION
VIII. BIBLIOGRAPHY

ANGELES UNIVERSITY FOUNDATIONAngeles City
COLLEGE OF NURSING

A Case Study
Presented to the Faculty of theCollege of Nursing
In Partial Fulfillment of the Requirements for the Degree ofBACHELOR OF SCIENCE IN NURSING
Presented by:
Baysa III, CarlosCapitly, Ellaine
Pineda, Janine Snay, Liza Marie
Marilou S. Limiac, RNClinical Instructor
November 26, 2009